
Abstract
Aims/hypothesis
Diabetes is associated with an increased risk of atherosclerotic cardiovascular disease, but whether there is a direct and independent role for impaired glucose control in atherogenesis remains uncertain. We investigated whether diabetes with poor glycaemic control would accelerate atherogenesis in a novel pig model of atherosclerosis, the D374Y-PCSK9 + transgenic minipig.
Methods
Nineteen minipigs were fed a cholesterol-enriched, high-fat diet; ten of these pigs were injected with streptozotocin to generate a model of diabetes. Restricted feeding was implemented to control the pigs’ weight gain and cholesterol intake. After 49 weeks of high-fat feeding, the major arteries were harvested for a detailed analysis of the plaque burden and histological plaque type.
Results
Stable hyperglycaemia was achieved in the diabetic minipigs, while the plasma total and LDL-cholesterol and creatinine levels were unaffected. Diabetes failed to increase atherosclerosis in any of the vessels examined. The plaque burden in the aorta and right coronary artery was comparable between the groups, and was even reduced in the left anterior descending (LAD) coronary and iliofemoral arteries in the diabetic pigs compared with the controls. The distribution of plaque types and the collagen and macrophage contents were similar between the groups, except for a reduced infiltration of macrophages in the LAD arteries of the diabetic pigs.
Conclusions/interpretation
Poorly controlled diabetes with no alterations in plasma cholesterol or creatinine concentrations did not augment the plaque burden or promote the development of more advanced lesions in this large-animal model of human-like atherosclerosis. This is consistent with clinical studies in patients with type 1 diabetes, indicating that hyperglycaemia per se is not an independent promoter of atherosclerotic disease, but that other diabetes-associated risk factors are important.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Type 1 diabetes is associated with a substantially increased risk of atherosclerotic cardiovascular disease and cardiovascular mortality [1–5]. Several factors may explain this excess risk, including hyperglycaemia, renal dysfunction, hypertension and dyslipidaemia, but the potential impact of each factor and the evidence for the underlying mechanism remain disputed [1, 6, 7]. The association between diabetic hyperglycaemia and other diabetes-associated risk factors, for example kidney damage [8, 9], complicates the analysis of human data. The direct effect of poor glycaemic control on atherogenesis is thus subject to debate, with some studies [10–12] pointing to hyperglycaemia as an independent predictor of subclinical and clinical atherosclerosis in diabetic patients, but others [3, 13] failing to detect such an association, especially after controlling for competing risk factors.
Animal experiments may suffer from similar limitations. In most studies of wild-type and genetically modified mice used as a model of diabetes, type 1 diabetes has been reported to boost plasma cholesterol concentrations [14–21], making it difficult to isolate the effect of glucose dysregulation on atherogenesis. Similarly, diabetes has been reported to augment cholesterol levels in Yucatan and Sinclair minipigs [22, 23]. In the widely used Yorkshire pig model of diabetes, inconsistent results have been obtained regarding the effect of diabetes on atherosclerosis and cholesterol level [24–26]. Impairment of kidney function and severe weight faltering in animal models of diabetes may further obscure the link between hyperglycaemia and atherosclerosis.
Proprotein convertase subtilisin/kexin type 9 (PCSK9) is a protein that binds to the LDL receptor and facilitates its degradation in hepatocytes. By overexpressing a hyperactive (D374Y) human form of PCSK9 in the hepatocytes of Yucatan minipigs (D374Y-PCSK9 + minipigs), we recently created a model of hypercholesterolaemia and accelerated human-like atherosclerosis [27]. In the current study, we present methods for controlled induction and management of hyperglycaemia in D374Y-PCSK9 + minipigs, to generate a model of type 1 diabetes. Furthermore, we report the effect of impaired glycaemic control on the development of atherosclerosis in the absence of diabetes-associated changes in plasma cholesterol or creatinine concentrations, and while maintaining steady body growth.
Methods
Animals
Yucatan minipigs were obtained from breeding colonies maintained at Aarhus University and housed in specific pathogen-free stable facilities. Transgenic minipigs were bred by mating wild-type sows with two cloned, genetically identical boars harbouring transgene insertions on chromosomes X and 9 [27]. Male transgenic offspring with the chromosome 9 transgene and females offspring with the chromosome X transgene were randomly assigned to either a control group (four females and five males) or a diabetes model group (DM; five females and seven males). The animals in the control group were also part of a concurrent study that was recently published [27] in which the phenotype was described in detail. A high-fat, high-cholesterol (HFHC) diet was mixed by adding 20% (wt/wt) of lard and 2% cholesterol (Sigma-Aldrich, Brøndby, Denmark) to standard pig chow. All the pigs were started on the HFHC diet at 8–9 weeks of age and fed ad libitum until they reached a weight of 20 kg, after which feeding was restricted to 700 g divided into two daily portions, which were completely consumed by the pigs without wastage. Restricted feeding was implemented to control the pigs’ weight gain and to ensure an equal cholesterol intake in all the animals. The principles of laboratory animal care (NIH publication no. 85–23) were followed. The Danish Animal Experiments Inspectorate approved all the experimental procedures.
Induction of diabetes
Doses of streptozotocin (STZ; Sigma-Aldrich) were calculated based on body weight (110 mg/kg), and the first injection was carried out 2–4 weeks after the start of the HFHC diet. Prior to STZ injection, animals in the DM group were fasted for 16 h and sedated as detailed in the electronic supplementary material (ESM) Methods. STZ (100 mmol/l) was dissolved in sodium citrate buffer (100 mmol/l, pH 4.5) as previously described [24] and immediately injected over 2–3 min through sterile filters into an ear vein.
Fasting plasma glucose (FPG) in the DM group of pigs was monitored twice a week using a hand-held glucometer (Accu-Check Compact Plus; Roche, Basel, Switzerland). If the average FPG dropped below 10 mmol/l for 2 consecutive weeks, the STZ injection was repeated. Insulin treatment (isophane insulin; Novo Nordisk, Bagsværd, Denmark) was initiated if the FPG increased to above 20 mmol/l on two successive measurements within a week, and was continued until the animals were killed. Insulin was injected subcutaneously once daily, and the dose was adjusted to keep the FPG at 12–17 mmol/l as detailed in ESM Table 1. When the animals received insulin, the FPG was measured immediately prior to that day’s insulin administration, i.e. 24 h after the last insulin administration. One DM pig (male) was killed after the development of plasma acidosis and ketonuria. Another DM pig (female) was killed due to the development of a cataract. Thus, in the DM group, ten pigs (four females, six males) completed the study. Fasting blood samples were drawn from the jugular vein at the time points indicated. For details on plasma analysis, see the ESM Methods.
Tissue analysis
The control pigs were killed 46 (range 43–48) weeks and the diabetic pigs 49 (range 42–51) weeks after initiation of the HFHC diet. The procedures for killing the animals and analysing the tissues were followed as previously described [27]. In brief, after the pigs had been sedated, a lethal dose of pentobarbital (Lundbeck, Copenhagen, Denmark) was injected and the heart and major arteries were extracted. All the tissues were immersion-fixed in 4% formaldehyde for 6 h. The aorta, right iliofemoral artery (proximal 10 cm) and right coronary artery (RCA; proximal 6 cm) were stained en face through immersion in Sudan IV solution (Sigma-Aldrich; 5 g/l in 96% ethanol) for 5 min, followed by 90 s of wash-out in 96% ethanol. Digital images of the stained intimal surfaces were analysed with custom-made computer software.
The proximal 1.5 cm of the left anterior descending (LAD) coronary artery was cross-sectioned at 3 mm intervals. The largest raised plaque in the abdominal aorta, typically situated within 3 cm of the renal arteries, was identified by macroscopic inspection and excised for histological analysis. A longitudinal slice from the aortic root to the branching point of the upper body vasculature was obtained from the major curvature of the ascending aorta. The aortic and coronary slices were embedded in paraffin, sectioned (3 μm sections) and stained with haematoxylin and eosin using routine methods. The intimal and medial areas of the coronary sections were quantified using ImageJ software (National Institutes of Health, Bethesda, MD, USA) and the mean values were calculated for each vessel. The classification of histological lesion type proposed by Virmani et al [28] was performed in a blind approach by two observers, with intra- and inter-observer Cohen’s weighted κ values of 0.86 and 0.79, respectively. In the LAD arteries, the most advanced plaque was selected for a between-groups comparison of plaque type.
Plaque macrophages were detected by immunohistochemical staining using rabbit anti-muramidase primary antibody (1:500, A0099; Dako, Glostrup, Denmark), biotinylated secondary antibody (E0453; Dako), alkaline phosphatase-conjugated streptavidin (SA-5100; Vector Labs, CA, USA) and Liquid Permanent Red (K0640; Dako). To quantify the collagen, sections were stained with Sirius Red and analysed under polarised light. The stained areas were measured in ImageJ using the Threshold tool.
Statistical analysis
Statistical analyses were performed using Prism software (GraphPad Software, La Jolla, CA, USA). Normally distributed data are presented as means ± SEM and non-normal data are displayed as the median and interquartile range (IQR). Group comparisons were made using an unpaired Student’s t test, Welch’s t test or Mann–Whitney U test as appropriate. Differences in time series measurements were assessed by comparing the AUCs. Plaque types were grouped into early lesions (intimal thickening or xanthomas) and progressive lesions (pathological intimal thickening or fibroatheromas) in contingency tables, and Fisher’s exact test was used to assess the differences. The data were initially analysed separately for each sex, but no sex differences were detected for any of the measures of atherosclerosis or plasma metabolites. Therefore the data for male and female pigs were combined to increase the statistical power. The significance level was set to <0.05 and p values are presented for significant results.
Results
Induction of diabetes
The level of hyperglycaemia following the first injection of STZ varied, which is a known issue with standard weight-adjusted dose administration regimens. However, by using an algorithm with repeated STZ injections (1–4 injections, median 2.5 injections per pig), diabetes was achieved in all the pigs. A stable FPG >10 mmol/l was reached at a median of 9 (IQR 2–12) weeks after the start of the HFHC diet. Insulin therapy was initiated at a median of 19 (IQR 18–23) weeks after the start of the HFHC diet, which restricted the FPG to below 20 mmol/l (Fig. 1a). The pigs injected with STZ showed a significantly higher cumulative FPG load (a 3.3-fold increase in the AUC) compared with the control pigs (p < 0.0001), in which the FPG remained stable at approximately 5 mmol/l.

Characteristics of the development of diabetes. (a) FPG levels, p < 0.0001. The shaded areas show the periods of STZ and insulin administration. The left boxplot (showing the median, IQR and range) shows the time of final STZ injection. The right boxplot shows the initiation of insulin therapy. (b) Plasma fructosamine levels, p < 0.0001. (c) AUC for plasma fructosamine, indicating the total glycaemic load during the study period, p < 0.0001. (d) Plasma C-peptide levels, p < 0.005. The horizontal line represents the limit of detection of the assay. (e) Body weight, p < 0.05. (f) Plasma creatinine levels. Black circles, diabetic pigs; white circles, controls. Error bars indicate ± SEM. p values determined by t test were calculated by comparing AUCs (a–d, f) or final weight (e) for DM vs control pigs
Due to the limited transmembrane glucose permeability of porcine erythrocytes, fructosamine rather than glycated haemoglobin reflects long-term glycaemic levels in pigs [29]. Fructosamine levels paralleled glucose levels after the STZ injections in the DM pigs (Fig. 1b). Insulin therapy triggered a transient decline in fructosamine levels, but the high levels were re-established after adjustment of the insulin doses. The AUC for fructosamine correlated well with the AUC for FPG prior to insulin administration (p < 0.0001, r 2 = 0.95) and during insulin therapy (p < 0.0001, r 2 = 0.96) (ESM Fig. 1a). The AUC for fructosamine was higher in the diabetic pigs than in the controls (p < 0.0001), and all the DM pigs achieved a fructosamine AUC of at least 6 SD above the mean of the control group (Fig. 1c). The fructosamine measurements thus further confirmed that increased glycaemic load was successfully achieved in all the STZ-treated animals.
Levels of C-peptide, which is derived from endogenous insulin production, initially declined on the HFHC diet for the pigs in both groups, but it was maintained at much lower levels in the STZ-injected than in the control pigs (p < 0.005 for difference in AUC). In the DM group, several pigs had C-peptide levels towards the end of study that were the same as or lower than the reported detection limit of the assay (0.033 nmol/l) (Fig. 1d).
The body weights were not significantly different between the two groups at the start of the experiment, and both groups gained weight steadily, although the DM pigs trailed 11% behind the control group at the end of the experiment (p < 0.05; Fig. 1e). No differences were detected in renal (creatinine) or hepatic (alanine aminotransferase) markers (Fig. 1f and ESM Fig. 1b).
Effects on plasma lipids
Levels of total cholesterol, LDL-cholesterol and HDL-cholesterol increased in all the animals following the initiation of the HFHC diet. The increase in HDL-cholesterol was modest and ceased after 4 weeks, whereas total cholesterol and LDL-cholesterol concentrations continued to rise, reaching approximately 20 mmol/l and approximately 12 mmol/l, respectively (Fig. 2a–c). No differences were detected between the groups, indicating that diabetes did not modulate the cholesterol levels. Size exclusion chromatography of the pooled plasma samples was consistent with these measurements and further revealed a steady increase in the cholesterol carried by VLDL-sized particles in both groups (Fig. 2d–f). The lipoproteins were of similar size, but the fraction of cholesterol carried by the VLDL-sized particles was lower in the DM group at week 20 compared with the control animals. Plasma levels of human PCSK9 were similar in both groups (ESM Fig. 1c).

Plasma cholesterol levels. (a) Total cholesterol. (b) LDL-cholesterol. (c) HDL-cholesterol. (d–f) Size exclusion chromatography on pooled plasma samples conducted prior to placing the pigs on the HFHC diet (d) and after 20 (e) and 42 (f) weeks on the diet. Black circles, diabetic pigs; white circles, controls. No significant differences were found (a–c). Error bars indicate ± SEM
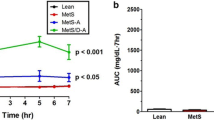
Baseline triacylglycerol levels were higher in the DM group compared with the control group, but this was mainly driven by two data points and was not statistically significant. During the study, the triacylglycerol levels were higher on average in the diabetic group (p < 0.001 for AUC; Fig. 3a). This link between diabetes and increased plasma triacylglycerol concentrations was further corroborated by a significant correlation between the AUC for triacylglycerol and the AUC for fructosamine (exponential growth correlation, r 2 = 0.83, p < 0.0005; Fig. 3b). Size fractioning revealed, as expected, that triacylglycerol was mainly stored in VLDL-sized particles (Fig. 3c–e).

Plasma triacylglycerol levels. (a) Plasma triacylglycerol, p < 0.001 determined by t test comparing AUCs for DM vs control pigs. (b) Exponential growth correlation between the AUCs for triacylglycerol and fructosamine. p < 0.0005 for power coefficient. (c–e) Size fractioning of pooled plasma samples showing the distribution of triacylglycerol in lipoprotein particles and glycerol data prior to placing the pigs on the HFHC diet (c) and after 20 (d) and 42 (e) weeks on the diet. Black circles, diabetic pigs; white circles, controls. Error bars indicate ± SEM
Effects on atherosclerosis
Atherosclerotic lesions in the thoracic aorta of all the pigs were predominantly confined to the aortic root and arch. Raised lesions were found solely in the abdominal part. The areas of the atherosclerotic lesions in the aorta expressed as a percentage of the total surface area were 40.3% (±4.7% SEM) in the control pigs and 30.9% (±2.8% SEM) in the diabetic pigs, and the difference was not significant (Fig. 4a). Lesions in the iliofemoral arteries were more extensive in control pigs (47.2% ± 11.4% SEM) than diabetic pigs (10.7 ± 2.4% SEM, p < 0.05; Fig. 4b). En face analysis revealed no significant differences in the coverage of RCA lesions (Fig. 4c), but there was a significant decrease in the absolute cross-sectional area of the lesions in the LAD arteries of the diabetic pigs (p < 0.05; Fig. 4d). The latter result may be influenced by a smaller LAD artery in diabetic pigs, as measured by a 19% reduction in the area of the media (p < 0.05; ESM Fig. 2a); this may reflect, at least in part, the lower body weight. The ratio of intima/media area in the LAD arteries was not significantly different between the groups (ESM Fig. 2b).

Atherosclerosis data. (a–c) Percentage of the total vessel area covered by atherosclerosis in the aorta (a), iliofemoral arteries (b) and RCA (c). (d) The cross-sectional plaque area in the proximal LAD artery. *p < 0.05 determined by t test (b) or Mann–Whitney U test (d). Error bars are ± SEM (a, b) and median with IQR (c, d). C, control
Group-wise correlation analysis revealed that neither body weight (data not shown) nor the total dose of injected insulin (ESM Fig. 3) in the DM pigs correlated significantly with the atherosclerotic burden in any of the vessels examined.
The classification of LAD artery, thoracic aortic and abdominal aortic lesions, based on the scheme proposed by Virmani et al [28], revealed that the lesions were mostly pathological intimal thickenings in the LAD arteries and thoracic aorta, but the abdominal aorta contained more fibroatheromas (Fig. 5a–f). Importantly, no significant group differences in the distribution of lesion types were detected (Fig. 5g–i). No differences in collagen content, measured as the percentage of the area stained with Sirius Red, were detected in the vessels examined (Fig. 6d–f). The macrophage content, measured as the percentage of the area that was muramidase positive, was reduced in LAD artery lesions in diabetic pigs compared with controls, consistent with the smaller lesion size, but otherwise no differences in macrophage content were detected (Fig. 6g–i).

Histology and classification of plaques. (a, b) Sections from the LAD artery of a control (a) and a diabetic (b) pig showing pathological intimal thickening containing foam cells and extracellular lipid pools (LP). (c, d) Fibroatheromas from abdominal aortas of a control (c) and a diabetic (d) pig containing calcium deposits (C), necrotic core development (NC) and a fibrous cap (F). (e, f) Sections from the thoracic aorta of a control (e) and a diabetic (f) pig showing pathological intimal thickening. Scale bars, 0.5 mm. L, lumen; M, media. (g–i) Distribution of plaque types in the thoracic aorta, abdominal aorta and proximal LAD artery. White bars, normal or intimal thickening; grey bars, xanthoma; striped bars, pathological intimal thickening; black bars: fibroatheroma; (g–i) C, control

Plaque collagen and macrophage content. (a, b) Sirius Red staining of an abdominal aortic lesion seen under normal (a) or polarised light (b), showing the accumulation of collagen. (c) Immunohistochemical staining for muramidase to reveal plaque macrophages (red). L, lumen; C, calcification; F, fibrous cap; M, media. (d–i) Quantification of collagen-rich and macrophage-rich areas in lesions from the thoracic aorta, abdominal aorta and LAD artery. *p < 0.05 determined by t test. Error bars are ± SEM; (d–i) C, control
Discussion
In the current study, we established a protocol for the induction and management of diabetes in a novel atherosclerosis-prone pig model. In contrast to many previous studies, we found no effects of diabetes on the level of total or LDL-cholesterol, and no signs of kidney function impairment. We conducted analyses of atherosclerosis in several clinically relevant vascular beds and found no aggravating effect of impaired glucose control on the amount or type of atherosclerotic lesions. On the contrary, diabetes was associated with a reduced burden of atherosclerosis in the proximal LAD and iliofemoral arteries.
Animal models of diabetes and atherosclerosis
Animal models potentially hold the key to testing the isolated effect of hyperglycaemia on atherogenesis, but animal models that combine type 1 diabetes and atherosclerosis have generally suffered from concurrent effects on plasma cholesterol.
In mice of various genetic backgrounds, type 1 diabetes has been reported to increase atherosclerosis, but this has often been accompanied by a marked diabetes-induced elevation in plasma cholesterol concentrations [14–21]. When cholesterol levels were not significantly altered by diabetes, inconsistent results were observed and atherosclerosis was augmented [20, 30], unmodified [21, 31, 32] or even reduced [33]. Interestingly, in one study, when diabetic and control mice were matched based on cholesterol levels, the initially significant difference between the two groups disappeared [20].
Pigs provide models of atherosclerosis that are close to the human pathology with respect to the size and composition of the plaques, and unlike mice, the disease is initiated in an arterial intima that already contains various amounts of cells and extracellular matrix [34]. This is particularly relevant for studies on diabetes because the alteration in the composition of the arterial matrix that is seen in diabetes has been hypothesised to increase the susceptibility to atherosclerotic lesion formation [35]. Relatively few studies have examined the atherogenic effect of hyperglycaemia in pigs (Table 1). In a small study of wild-type Yucatan minipigs in which they examined one section of 0.75–2 mm from each vessel, Wang et al detected an increase in intima/media thickness in two out of six vascular beds examined [22]. Dixon et al found increased sudanophilia in the carotid artery of diabetic Sinclair minipigs [23]. In both studies, however, the results were potentially confounded by a near doubling of LDL-cholesterol concentration [22, 23]. Dixon et al also examined Yucatan minipigs and reported vascular changes on intravascular ultrasound (a raised endothelium) in a higher number of diabetic coronary segments compared with controls, but it is not known whether this represented atherosclerosis because tissue analysis, including histology, was not performed [36].
In a seminal paper, Gerrity et al showed increased aortic atherosclerosis and coronary luminal stenosis in diabetic Yorkshire pigs as early as 20 weeks into the study, without concomitant changes in total cholesterol levels [24]. However, in two subsequent studies in Yorkshire × Landrace and Yorkshire pigs, respectively, diabetes was accompanied by augmented hypercholesterolaemia. In the first of these studies, van den Heuvel et al reported increased atherosclerosis in abdominal aortas [26], but in the other, Hamamdzic et al observed no effect on intimal area, intima/media ratio or the degree of stenosis of the coronary arteries, although the lesions were reported to be more complex in diabetic compared with control animals [25]. In the latter study, an approximately 50% reduction in body weight was also reported for the diabetic pigs compared with the controls.
Since combined insulin deficiency and hyperglycaemia has been documented in all of the reports in pigs (Table 1) and mice [14–21, 30–33], the failure to consistently augment atherosclerosis suggests that impaired glycaemic control per se may not accelerate atherogenesis, but that other factors that are variably present in diabetic animal models, including elevated cholesterol and kidney damage, may play an important role. The lack of an atherogenic effect of diabetes in this study supports this interpretation.
Effect of diabetes on plasma lipids
The lack of diabetes-associated hypercholesterolaemia in D374Y-PCSK9 + transgenic minipigs is an important strength compared with many previous animal studies. Insulin has been shown to upregulate the expression of the LDL receptor [37], and reduced hepatic LDL uptake due to insulin deficiency may be one mechanism underlying hypercholesterolaemia in diabetes [38]. Recent work in mice has shown that the restriction of PCSK9 expression by insulin plays a major role in mediating this effect [38]. In our transgenic minipigs, human D374Y-PCSK9 is expressed under a constitutively active liver-specific promoter [27] rather than the native insulin-controlled PCSK9 promoter. Furthermore, the high expression level of D374Y-PCSK9 overwhelms the effect of any changes in endogenous porcine PCSK9. Thus, the regulatory link between insulin and LDL receptor levels may be effectively disrupted, which may explain the lack of diabetes-induced hypercholesterolaemia in D374Y-PCSK9 + minipigs. A reduced binding of apoB48-containing remnants to hepatic proteoglycans has been suggested to cause cholesterol accumulation in diabetic LDL-receptor-deficient mice [39], but this mechanism is probably of less relevance in pigs (or humans), where the bulk of the cholesterol is carried in apoB100-containing LDL/VLDL particles. Furthermore, diabetic hyperphagia [39, 40], with an increased dietary cholesterol intake in animals fed ad libitum, has been shown to contribute to diabetic hypercholesterolaemia [41, 42]. To counteract this effect, we secured a uniform intake of the HFHC diet by using a restricted feeding regimen.
An increased AUC for triacylglycerol was seen in the diabetic group, which is consistent with observations in type 1 diabetic patients, but, importantly, our diabetic pigs did not develop the kinds of giant lipoproteins that have previously been found to reduce atherogenesis in diabetic rabbits [43].
Hyperglycaemia and coronary heart disease
Although studies have reported that individuals with type 1 diabetes suffer from an increased risk of atherosclerosis [3, 4] and cardiovascular mortality [1, 2], the direct and independent contribution of glycaemic dysregulation to this excess risk remains to be proven. Table 2 provides a summary of human studies that have been conducted on major cohorts of patients with type 1 diabetes in recent years. As depicted, the studies are not unanimous in identifying hyperglycaemia as an independent predictor of subclinical atherosclerosis or ischaemic coronary events when competing risk factors are controlled for.
The Wisconsin Epidemiologic Study of Diabetic Retinopathy [44] and two follow-up studies on patients from the DCCT [10, 11, 45] all identified hyperglycaemia as an independent predictor of atherosclerotic cardiovascular endpoints. In contrast, the EURODIAB study showed that the initially significant link between hyperglycaemia and coronary heart disease was rendered insignificant once albuminuria and other candidate risk factors were included in the analysis [13]. Furthermore, while studies may adjust for multiple risk factors at baseline, competing effects of changes in risk factors over the study period, for example incident renal damage and long-term cholesterol levels, are often neglected. Such incompletely adjusted associations may overestimate the role of hyperglycaemia in human studies in light of the positive correlations seen between hyperglycaemia and other candidate causal agents, for example dyslipidaemia and the development of kidney disease [8, 9].
Our results suggest that hyperglycaemia due to insulin deficiency per se is not a promoter of atherosclerosis, and support alternative interpretations of the association between diabetes and atherosclerotic heart disease in humans. Although an investigation of type 2 diabetes is beyond the scope of this work, it is worth noting that glycaemic control in patients with type 2 diabetes has repeatedly failed to provide protection against atherosclerotic cardiovascular disease in randomised clinical trials [46, 47].
Strengths and limitations
The large-animal model used in this study includes the development of atherosclerotic lesions with many similarities to those seen in humans [27]. Porcine vessels contain a pre-existing intima, and lesions develop that show rich fibrous tissue, macrophage infiltration, necrosis and calcification. It was also possible to induce insulin deficiency and maintain severe hyperglycaemia during exogenous insulin therapy, thus replicating poor glycaemic control in diabetic humans. Importantly, this could be achieved without the diabetes-induced increases in cholesterol levels that are seen in other animal studies, presumably because of the clamped high level of PCSK9. An important limitation of the model, which it has in common with previous animal studies of diabetes and atherosclerosis, is that the lesions do not develop to the stage that causes thrombotic complications or stable stenosis in humans. Therefore, our study cannot disregard potential effects of diabetes on late-stage atherosclerosis, plaque vulnerability or arterial remodelling. Furthermore, potential effects of diabetes acting through changes in lipoprotein metabolism, including, in particular, changes in the distribution of lipoprotein sizes, may not be accurately addressed in porcine models because of the lack of cholesteryl ester transfer protein.
Conclusion
In conclusion, we have established a model of chemically induced diabetes in D374Y-PCSK9 + transgenic minipigs that is free of important factors that may obscure the link between impaired glucose control and atherosclerosis. We found that diabetes did not accelerate the extent of the atherosclerosis or promote complexity of the lesions. This supports the need to focus on diabetes-associated factors beyond hyperglycaemia to understand the causes of accelerated atherosclerotic cardiovascular disease in patients with type 1 diabetes.
Abbreviations
- DM:
-
Diabetes model group
- FPG:
-
Fasting plasma glucose
- HFHC:
-
High-fat high-cholesterol
- IQR:
-
Interquartile range
- LAD:
-
Left anterior descending
- PCSK9:
-
Proprotein convertase subtilisin/kexin type 9
- RCA:
-
Right coronary artery
- STZ:
-
Streptozotocin
References
Orchard TJ, Costacou T, Kretowski A, Nesto RW (2006) Type 1 diabetes and coronary artery disease. Diabetes Care 29:2528–2538
Lind M, Svensson AM, Kosiborod M et al (2014) Glycemic control and excess mortality in type 1 diabetes. N Engl J Med 371:1972–1982
Maahs DM, Jalal D, Chonchol M et al (2013) Impaired renal function further increases odds of 6-year coronary artery calcification progression in adults with type 1 diabetes: the CACTI study. Diabetes Care 36:2607–2614
Larsen JR, Tsunoda T, Tuzcu EM et al (2007) Intracoronary ultrasound examinations reveal significantly more advanced coronary atherosclerosis in people with type 1 diabetes than in age- and sex-matched non-diabetic controls. Diab Vasc Dis Res 4:62–65
Libby P, Nathan DM, Abraham K et al (2005) Report of the National Heart, Lung, and Blood Institute-National Institute of Diabetes and Digestive and Kidney Diseases Working Group on cardiovascular complications of type 1 diabetes mellitus. Circulation 111:3489–3493
Retnakaran R, Zinman B (2008) Type 1 diabetes, hyperglycaemia, and the heart. Lancet 371:1790–1799
Goldberg IJ (2004) Why does diabetes increase atherosclerosis? I don’t know! J Clin Invest 114:613–615
Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group (2003) Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA 290:2159–2167
O'Seaghdha CM, Hwang S-J, Upadhyay A et al (2010) Predictors of incident albuminuria in the Framingham Offspring cohort. Am J Kidney Dis 56:852–860
Nathan DM, Cleary PA, Backlund J-YC et al (2005) Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 353:2643–2653
Cleary PA, Orchard TJ, Genuth S et al (2006) The effect of intensive glycemic treatment on coronary artery calcification in type 1 diabetic participants of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study. Diabetes 55:3556–3565
Olson JC, Erbey JR, Forrest KY-Z et al (2002) Glycemia (or, in women, estimated glucose disposal rate) predict lower extremity arterial disease events in type 1 diabetes. Metabolism 51:248–254
Soedamah-Muthu SS, Chaturvedi N, Toeller M et al (2004) Risk factors for coronary heart disease in type 1 diabetic patients in Europe: the EURODIAB Prospective Complications Study. Diabetes Care 27:530–537
Otero P, Bonet B, Herrera E, Rabano A (2005) Development of atherosclerosis in the diabetic BALB/c mice. Prevention with vitamin E administration. Atherosclerosis 182:259–265
Park L, Raman KG, Lee KJ et al (1998) Suppression of accelerated diabetic atherosclerosis by the soluble receptor for advanced glycation endproducts. Nat Med 4:1025–1031
Calkin AC, Forbes JM, Smith CM et al (2005) Rosiglitazone attenuates atherosclerosis in a model of insulin insufficiency independent of its metabolic effects. Arterioscler Thromb Vasc Biol 25:1903–1909
Zuccollo A, Shi C, Mastroianni R et al (2005) The thromboxane A2 receptor antagonist S18886 prevents enhanced atherogenesis caused by diabetes mellitus. Circulation 112:3001–3008
Nestel PP, Fujii AA, Allen TT (2006) The cis-9, trans-11 isomer of conjugated linoleic acid (CLA) lowers plasma triglyceride and raises HDL cholesterol concentrations but does not suppress aortic atherosclerosis in diabetic apoE-deficient mice. Atherosclerosis 189:6
Keren P, George J, Shaish A et al (2000) Effect of hyperglycemia and hyperlipidemia on atherosclerosis in LDL receptor-deficient mice: establishment of a combined model and association with heat shock protein 65 immunity. Diabetes 49:1064–1069
Renard CB, Kramer F, Johansson F et al (2004) Diabetes and diabetes-associated lipid abnormalities have distinct effects on initiation and progression of atherosclerotic lesions. J Clin Invest 114:659–668
Kako Y, Massé M, Huang LS et al (2002) Lipoprotein lipase deficiency and CETP in streptozotocin-treated apoB-expressing mice. J Lipid Res 43:872–877
Wang Y-X, Fitch R, Li W et al (2002) Reduction of cardiac functional reserve and elevation of aortic stiffness in hyperlipidemic Yucatan minipigs with systemic and coronary atherosclerosis. Vasc Pharmacol 39:69–76
Dixon JL, Stoops JD, Parker JL et al (1999) Dyslipidemia and vascular dysfunction in diabetic pigs fed an atherogenic diet. Arterioscler Thromb Vasc Biol 19:2981–2992
Gerrity RG, Natarajan R, Nadler JL, Kimsey T (2001) Diabetes-induced accelerated atherosclerosis in swine. Diabetes 50:1654–1665
Hamamdzic D, Fenning RS, Patel D et al (2010) Akt pathway is hypoactivated by synergistic actions of diabetes mellitus and hypercholesterolemia resulting in advanced coronary artery disease. Am J Physiol Heart Circ Physiol 299:H699–H706
van den Heuvel M, Sorop O, Koopmans S-J et al (2012) Coronary microvascular dysfunction in a porcine model of early atherosclerosis and diabetes. Am J Physiol Heart Circ Physiol 302:H85–H94
Al-Mashhadi RH, Sørensen CB, Kragh PM et al (2013) Familial hypercholesterolemia and atherosclerosis in cloned minipigs created by DNA transposition of a human PCSK9 gain-of-function mutant. Sci Transl Med 5:166ra1
Virmani R, Kolodgie FD, Burke AP et al (2000) Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 20:1262–1275
Kim HD, McManus TJ (1971) Studies on the energy metabolism of pig red cells. I. The limiting role of membrane permeability in glycolysis. Biochim Biophys Acta 230:1–11
Kunjathoor VV, Wilson DL, LeBoeuf RC (1996) Increased atherosclerosis in streptozotocin-induced diabetic mice. J Clin Invest 97:1767–1773
Goldberg IJ, Isaacs A, Sehayek E et al (2004) Effects of streptozotocin-induced diabetes in apolipoprotein AI deficient mice. Atherosclerosis 172:47–53
Reaven P, Merat S, Casanada F et al (1997) Effect of streptozotocin-induced hyperglycemia on lipid profiles, formation of advanced glycation endproducts in lesions, and extent of atherosclerosis in LDL receptor-deficient mice. Arterioscler Thromb Vasc Biol 17:2250–2256
Kako Y, Huang LS, Yang J et al (1999) Streptozotocin-induced diabetes in human apolipoprotein B transgenic mice. Effects on lipoproteins and atherosclerosis. J Lipid Res 40:2185–2194
Bentzon JF, Falk E (2010) Atherosclerotic lesions in mouse and man: is it the same disease? Curr Opin Lipidol 21:434–440
Chai S, Chai Q, Danielsen CC et al (2005) Overexpression of hyaluronan in the tunica media promotes the development of atherosclerosis. Circ Res 96:583–591
Dixon JL, Shen S, Vuchetich JP et al (2002) Increased atherosclerosis in diabetic dyslipidemic swine: protection by atorvastatin involves decreased VLDL triglycerides but minimal effects on the lipoprotein profile. J Lipid Res 43:1618–1629
Wade DP, Knight BL, Soutar AK (1988) Hormonal regulation of low-density lipoprotein (LDL) receptor activity in human hepatoma Hep G2 cells. Insulin increases LDL receptor activity and diminishes its suppression by exogenous LDL. Eur J Biochem 174:213–218
Ai D, Chen C, Han S et al (2012) Regulation of hepatic LDL receptors by mTORC1 and PCSK9 in mice. J Clin Invest 122:1262–1270
Goldberg IJ, Hu Y, Noh H-L et al (2008) Decreased lipoprotein clearance is responsible for increased cholesterol in LDL receptor knockout mice with streptozotocin-induced diabetes. Diabetes 57:1674–1682
Havel PJ, Hahn TM, Sindelar DK et al (2000) Effects of streptozotocin-induced diabetes and insulin treatment on the hypothalamic melanocortin system and muscle uncoupling protein 3 expression in rats. Diabetes 49:244–252
Kwong LK, Feingold KR, Peric-Golia L et al (1991) Intestinal and hepatic cholesterogenesis in hypercholesterolemic dyslipidemia of experimental diabetes in dogs. Diabetes 40:1630–1639
Young NL, Lopez DR, McNamara DJ (1988) Contributions of absorbed dietary cholesterol and cholesterol synthesized in small intestine to hypercholesterolemia in diabetic rats. Diabetes 37:1151–1156
Nordestgaard BG, Stender S, Kjeldsen K (1988) Reduced atherogenesis in cholesterol-fed diabetic rabbits. Giant lipoproteins do not enter the arterial wall. Arteriosclerosis 8:421–428
Shankar A, Klein R, Klein BEK, Moss SE (2007) Association between glycosylated hemoglobin level and cardiovascular and all-cause mortality in type 1 diabetes. Am J Epidemiol 166:393–402
The Diabetes Control and Complications Trial DCCT Research Group (1995) Effect of intensive diabetes management on macrovascular events and risk factors in the Diabetes Control and Complications Trial. Am J Cardiol 75:894–903
Hemmingsen B, Lund SS, Gluud C et al. (2013) Targeting intensive glycaemic control versus targeting conventional glycaemic control for type 2 diabetes mellitus. Cochrane Database Syst Rev (11) Art. no.:CD008143
Lincoff AM, Tardif J-C, Schwartz GG et al (2014) Effect of aleglitazar on cardiovascular outcomes after acute coronary syndrome in patients with type 2 diabetes mellitus: the AleCardio randomized clinical trial. JAMA 311:1515–1525
Olson JC, Edmundowicz D, Becker DJ et al (2000) Coronary calcium in adults with type 1 diabetes: a stronger correlate of clinical coronary artery disease in men than in women. Diabetes 49:1571–1578
Conway B, Costacou T, Orchard T (2009) Is glycaemia or insulin dose the stronger risk factor for coronary artery disease in type 1 diabetes? Diab Vasc Dis Res 6:223–230
Acknowledgements
We thank A. M. Toft, K. P. Jensen (AU-Foulum, Aarhus University, Denmark) and the rest of the personnel at AU-Foulum’s stable facilities for the blood sampling, insulin injection and practical handling of the pigs; K. D. Winther (AU-Foulum, Aarhus University, Denmark) for veterinary consultations; and Z. P. Nasr, D. W. Qualmann and L. M. Røge (Department of Clinical Medicine, Aarhus University, Denmark) and C. Berthelsen (AU-Foulum, Aarhus University, Denmark) for providing excellent technical assistance.
Funding
Funding was received from the Danish Council for Independent Research|Medical Sciences, Lundbeck Foundation, Danish Heart Foundation, Aase og Ejnar Danielsen Foundation, Snedkermester Sophus Jacobsen og hustru Astrid Jacobsens Foundation and Murermester Lauritz Peter Christensen og hustru Kirsten Sigrid Christensens Foundation.
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
EF and JFB conceived the study. RHA, EF and JFB planned and performed the induction of diabetes. RHA organised the blood sampling, insulin treatment and other practical aspects. RHA, CC and TL acquired the plasma data and undertook the subsequent chemical analysis and interpretation. RHA, MMB, MBM and JFB killed the animals and undertook the tissue data extraction and subsequent pathological analysis and interpretation. RHA performed the final data analysis. JFB supervised the experiments. RHA, EF and JFB wrote the manuscript. All authors critically revised the manuscript and approved the final version. RHA is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author information
Authors and Affiliations
Corresponding authors
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Methods
(PDF 76 kb)
ESM Table 1
(PDF 67 kb)
ESM Fig. 1
(PDF 128 kb)
ESM Fig. 2
(PDF 109 kb)
ESM Fig. 3
(PDF 93 kb)
Rights and permissions
About this article

Cite this article
Al-Mashhadi, R.H., Bjørklund, M.M., Mortensen, M.B. et al. Diabetes with poor glycaemic control does not promote atherosclerosis in genetically modified hypercholesterolaemic minipigs. Diabetologia 58, 1926–1936 (2015). https://doi.org/10.1007/s00125-015-3637-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-015-3637-1