
Abstract
Age estimation constitutes an important facet of human identification within forensic, bioarchaeological, repatriation, and humanitarian contexts. Within the human skeletal framework, the pubic symphysis comprises one of the more commonly utilized structures for age estimation. The present investigation was aimed at establishing the applicability of the McKern–Stewart pubic symphyseal age estimation method in males and females of an Indian population, an aspect previously unreported. Three hundred and eighty clinical CT scans of the pubic symphysis were collected and scored in accordance with the McKern–Stewart method. An overall accuracy of 68.90% was obtained on applying the method to males, demonstrating a limited applicability of the method in its primal form. Subsequently, Bayesian analysis was undertaken to enable accurate age estimation from individual components in both sexes. Bayesian parameters obtained with females suggest that McKern–Stewart’s components fail to accommodate for age-related changes within the female pubic bone. Improved accuracy percentages and reduced inaccuracy values were obtained with Bayesian analysis in males. With females, the error computations were high. Weighted summary age models were utilized for multivariate age estimation, and furnished inaccuracy values of 11.51 years (males) and 17.92 years (females). Error computations obtained with descriptive analysis, Bayesian analysis, and principal component analysis demonstrate the limited applicability of McKern–Stewart’s components in generating accurate age profiles for Indian males and females. The onset and progression of age-related changes within the male and female pubic bone may be of interest to biological anthropologists and anatomists involved in exploring the underlying basis for aging.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Age estimation is vital to the process of human identification within forensic, bioarchaeological, repatriation, and humanitarian contexts (Krogman 1986). Within forensic/medico-legal settings, age estimation is of paramount importance in cases involving and not limited to illegal immigrants, assigning criminal responsibility to individuals, disaster victim identification, and missing person identification. Age estimation in an archaeological sample aids in understanding and reconstructing the life of past populations. Age estimation, and by extension, human identification, additionally aids in the repatriation of refugees and victims of war. Within a humanitarian context, estimation of age is undertaken with the primary objective of preventing human rights violations in cases involving unaccompanied minors, human trafficking victims, child labour, pedopornography, and asylum seeking refugees. In cases where human skeletal remains present for examination, ossification and fusion of bones, as well as degenerative changes transpiring within the skeletal framework, are relied on for age estimation. Previously undertaken investigations have extensively explored the role of numerous bony markers for human age estimation (Ruengdit et al. 2018; Shedge et al. 2020, 2021; Widek et al. 2021; Brooks and Suchey 1990; Warrier et al. 2022a). Amongst these markers, the human pelvis, in addition to being a robust and resilient structure, houses multiple developmental and degenerative markers (Warrier et al. 2022b; Lottering et al. 2013; Rissech et al. 2006; Buckberry and Chamberlain 2002; Bartolini et al. 2018; Zhang et al. 2016). This confers to the pelvis the ability to estimate age across a broader age cohort, as opposed to other commonly utilized age markers which remain applicable for restricted age groups alone (Shedge et al. 2020; Widek et al. 2021; Kotecha 2016) .
Within the human pelvis, the pubic symphysis constitutes one of the more commonly utilized age markers (Miranker 2016; Moraitis et al. 2014). The pubic symphysis exhibits developmental changes in younger individuals, and degenerative changes in older adults, rendering it applicable for age estimation across a broader age class (McKern and Stewart 1957). Furthermore, its resistance to activity patterns involving constant flexion and extension confers the symphyseal face added significance over other regions within the pelvis. Multiple pubic symphyseal age estimation methods have been devised over the previous century (Brooks and Suchey 1990; McKern and Stewart 1957; Todd 1920; Berg 2008; Gilbert and McKern 1973; Hanihara and Suzuki 1978; Hartnett 2010; Chen et al. 2008), each targeted towards exploiting these advantages for human identification. Amongst these, McKern and Stewart’s component-based method (McKern and Stewart 1957) constitutes one of the more commonly employed methods for age estimation (Garvin and Passalacqua 2012). The method was initially developed using male pubic bones, and involves breaking down pubic symphyseal changes into three distinct components: dorsal plateau, ventral rampart, and symphyseal rim. Each component is scored on a scale of 0–5, and the obtained cumulative score (0–15) is then employed to ascertain the age of remains presenting for examination (McKern and Stewart 1957). In the years that followed the method’s conception, multiple researchers have undertaken evaluations of McKern–Stewart’s pubic symphyseal age estimation method using different population groups (Sinha and Gupta 1995; Sharma et al. 2008; Kumar et al. 2009; Kumar 2011; Singh et al. 2013; Prasad et al. 2015; Selvamurugan et al. 2019; Javvadi et al. 2016; Kumaran et al. 2019; Janardhan et al. 2016; Pal and Tamankar 1983; Madanraj and Suares 2021; Snow 1983; Klepinger et al. 1992; Gorchiya et al. 2020; Meindl et al. 1985). However, limited research investigations have attempted to ascertain the accuracy and precision of the method (Meindl et al. 1985; Lungmus 2009). Establishing the accuracy and error associated with different age estimation methods is of paramount significance for forensic, humanitarian, and bioarchaeological contexts. Furthermore, the applicability of McKern–Stewart’s components in aging female remains has rarely been explored (Sharma et al. 2008; Singh et al. 2013; Selvamurugan et al. 2019; Lungmus 2009), with all such investigations employing under-represented female study groups.
Recent decades have witnessed the predominance of digital visualization techniques for human age estimation. 3D visualization techniques such as computed tomography enable the scrutiny of age-related morphological changes transpiring within the human skeletal framework without having to invest in the resource intensive and time-consuming maceration process. In addition to this, CT evaluations help create large-scale image databases of contemporary human populations which can then be utilized to test and appropriately modify conventionally derived age estimation methods. This is of particular significance in present day scenarios, where the lack of modern human skeletal repositories outside the USA impedes such an analysis. Previously undertaken computed tomographic assessments with pubic symphyseal age estimation methods have indicated a satisfactory reproduction of age-related morphological features on CT images (Lottering et al. 2013; Gorchiya et al. 2020; Wink 2014; Hall et al. 2019; Hisham et al. 2019; Pattamapaspong et al. 2019; Villa et al. 2013; Merritt 2018; Truesdell 2011).
The present study was aimed at ascertaining the applicability of the McKern–Stewart method through a CT-based examination of the pubic symphysis in an Indian population. The objectives of the present study were threefold: (1) establishing the accuracy and precision of the McKern–Stewart method for Indian males based on descriptives reported within the original study for males (2) ascertaining the applicability of McKern–Stewart’s components in aging males, as well as females of an Indian population using Bayesian analysis, as it generates realistic age profiles while circumventing age mimicry (3) to perform multivariate age estimation using principal component analysis and weighted summary age models with the aim of garnering reliable age estimates, advantages of which have previously been demonstrated (Warrier et al. 2022c, d).
Materials and methods
Sample collection
The present prospective cross-sectional study was carried out in the Department of Forensic Medicine and Toxicology, and the Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, India. Prior to commencement of the study, ethical approval was obtained from the Institutional Ethics Committee (Letter no. AIIMS/IEC/2019-20/1007). For this study, individuals aged 10 years and above undergoing computed tomographic examinations of the pelvis/abdomen, as per directions of their treating physicians, at the Department of Diagnostic and Interventional Radiology were approached. Such individuals/their guardians were appraised about the study parameters in detail, and their consent for voluntary participation into the study was sought. CT scans of individuals who consented to participate in the study were incorporated following proof of age verification through valid documents. Individuals who could not provide valid proof of age, and/or those with known bone injuries/deformities/pathologies within the pelvic region, or those which became apparent during CT examination were excluded from the study. Additionally, CT scans presenting with technical/patient-movement induced artefacts interfering with the analysis of interest were also excluded.
CT scans of 480 consenting individuals were collected between the study period of January 2020 and December 2021. The total study set of 480 CT scans was divided into two sub-sets: an informative prior comprising of 100 individuals, and an equally represented male and female population of 380 individuals (190 males, 190 females). All 380 CT scans were coded to blind the investigator to information capable of inducing bias. The informative prior was utilized to ascertain hazard parameters for the population under scrutiny, a pre-requisite for Bayesian analysis.
Scanning parameters
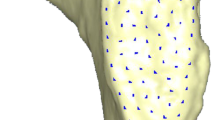
CT images of the pelvis of consenting individuals were obtained using Dual Source CT-SOMATOM Definition FlashTM (Siemens Medical Solutions, Erlangen, Germany). A slice thickness of 1 mm (standardized technical parameter utilized by the healthcare centre for diagnostic purposes) was employed within all scans. Obtained CT images were processed and assessed using 3D Slicer 4.11.20200930 (RRID: SCR_005619) (https://www.slicer.org/; Fedorov et al. 2012). For analysing the pubic symphysis, the bone window was selected, following which the generated image was cropped to narrow down on the region under scrutiny. Subsequently, a 3D volume rendered reconstruction of the cropped image was created. Using the scissor tool, additional interfering bony remnants were cut out to enable a clearer visualization of the pubic bone. The obtained pubic symphyseal reconstructions were examined from multiple planes to better appreciate transpiring morphological changes.
Age estimation using the McKern–Stewart method
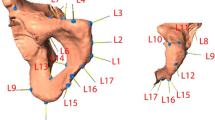
Age progressive morphological changes observed on 3D CT images of the male and female pubic symphysis were evaluated according to McKern–Stewart’s three component method (McKern and Stewart 1957). Each component was assigned a score from 0 to 5 based on the observed morphological changes. Subsequently, a cumulative score was computed using the individual scores of all three components and this was utilized for statistical analysis. Descriptions for individual components and the associated scoring system devised by McKern and Stewart are tabulated under Table 1. 3D CT representations of the component-based scoring method are shown in Figs. 1, 2, and 3.

3D CT representations of different gradations for the dorsal plateau

3D CT representations of different gradations for the ventral rampart

3D CT representations of different gradations for the symphyseal rim
Statistical analysis
Statistical analysis was performed using IBM Statistical Package for Social Sciences (SPSS) v26 and R Studio (RStudio Team (2022). RStudio: Integrated Development Environment for R. RStudio, PBC, Boston, MA URL http://www.rstudio.com/). R scripts and codes for specific statistical tests were obtained from previously undertaken studies (Konigsberg and Frankenberg 2013; Lyle W 2022 Konigsberg’s webpage: http://faculty.las.illinois.edu/lylek/; Getz 2020; Nikita et al. 2018; Nikita and Nikitas 2019). p < 0.05 was considered significant for all statistical evaluations.
Inter- and intra-observer error was assessed using Cohen’s weighted κ. Inter-observer error was computed based on the scoring of 40 pubic bones by two independent investigators. In order to compute the intra-observer error, the same 40 samples were re-evaluated by the lead investigator (VW) after a duration of 2 weeks from the time of initial examination. Obtained κ values were interpreted using the system described by McHugh (2012) as κ < 0.20: no agreement, κ = 0.21–0.39: minimal agreement, κ = 0.40–0.59: weak agreement, κ = 0.60–0.79: moderate agreement, κ = 0.80–0.90: strong agreement, and κ > 0.91: almost perfect agreement.
Bilateral differences in the scoring of individual components were evaluated using the Wilcoxon test, while sex differences associated with the same were analysed using the Mann–Whitney U test. The correlation between morphological changes transpiring within the pubic symphysis, and the documented age of participants was established using Spearman’s rho. Correlation coefficients were established for each individual component, as well as for the cumulative score, with age. Each of these statistical analyses were undertaken using the study set of 380 individuals.
In keeping with the first objective of this study, overall accuracy percentages, inaccuracy and bias values, and those associated with each individual component were established for males of this study set (N = 190). An individual was classified as accurately aged when their documented age fell within the age ranges reported by McKern and Stewart in their original study (McKern and Stewart 1957). Subsequently, accuracy percentages were estimated using the formula
Inaccuracy, an absolute estimate of the error associated with the method, was estimated following the prescribed formula
whereas bias, an estimate of the extent of under-aging/over-aging associated with the method, was garnered using the mathematical equation
Estimated mean point age values required for computations of inaccuracy and bias denote mean values reported by McKern–Stewart (1957).
As the descriptives of mean age and age range required to compute aforementioned accuracy and error were reported by McKern–Stewart exclusively for males, these values were not utilized herein to establish accuracy, inaccuracy, and bias for female participants. However, the applicability of McKern–Stewart’s components in aging males and females was assessed using Bayesian parameters, with the aim of furnishing more realistic age profiles while circumventing age mimicry. Thus, highest posterior density (HPD) and highest posterior density region (HPDR) values were computed for males and females using probability density functions, i.e., Bayesian analysis, in keeping with the second objective of this study. HPD approximates the age-at-death/estimated age, and HPDR approximates the 95% confidence intervals of the HPD. In order to carry out such an analysis, the study set of 380 participants was divided arbitrarily into a larger training group comprising of 280 individuals (140 males, 140 females), and a smaller test group of 100 individuals (50 males, 50 females). Pubic symphyseal data obtained from the larger training group (N = 280) was utilized to compute HPD, and HPDR associated with individual components through probability density functions described within Bayes theorem, as follows:
where f(A) is the probability density function of age, or the prior probability.
P(MS/A) indicates the likelihood ratio, i.e., the probability of observing different age-related changes as a function of chronological age.
P(A/MS) denotes the posterior probability for age estimation.
ʃ P(MS/x) * f(x)dx is the constant of proportionality, with shift denoting the minimum age in the informative prior A = age; MS = Scores assigned to different components of the McKern–Stewart method
f(x) depicts the demographic profile of the informative prior. Demographic profile of the informative prior (see sample collection) was estimated herein using the Gompertz model (Nikita and Nikitas 2019).
Accuracy percentages, inaccuracy, and bias values were computed for each individual component using the HPD and HPDR values garnered with Bayesian analysis. In order to do so, the test group (N = 100) comprising of an equal number of male and female participants was utilized. Accuracy percentages were estimated by tallying the proportion of individuals whose documented ages fell within the computed HPDR values. Inaccuracy and bias values were established using the differences between HPD and the chronological age of individuals.
Lastly, in accordance with the third objective, weighted summary age models were derived with the aim of garnering more reliable estimates of age, as follows:
where WC1, WC2, and WC3 denote weighted coefficients for the dorsal plateau, ventral rampart, and symphyseal rim. These weighted coefficients were computed using principal component analysis, and denote the correlation of each component with the first principal component (Miranker 2016; Warrier et al. 2022b; Lovejoy et al. 1985; Bedford et al. 1993). MDP, MVR, and MSR represent the HPD values for the dorsal plateau, ventral rampart, and symphyseal rim, respectively.
Derived summary age models were further applied to the test group (N = 100), and inaccuracy and bias values associated with the same were established for either sex.
Results
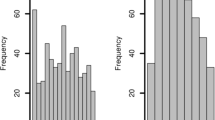
The total study sample of 380 participants comprised of an equal number of males and females, with a mean age ± SD of 45.92 ± 18.303 years and 48.69 ± 16.123 years, respectively. Age and sex distribution of this study sample is shown in Table 2. Box and whisker plots representing the age distribution pertaining to scores 0–5 of individual components are shown in Fig. 4 (males) and Fig. 5 (females). Within the study sample, no female participant displayed morphological features characteristic of score 0 for each of the three components.

Box and whisker plots representing the age distribution pertaining to different components (males)

Box and whisker plots representing the age distribution pertaining to different components (females)
Cohen’s weighted κ values for inter-observer error (dorsal plateau = 0.824, ventral rampart = 0.790, symphyseal rim = 0.740) and intra-observer error (dorsal plateau = 0.900, ventral rampart = 0.810, symphyseal rim = 0.780) illustrate a moderate to strong agreement in the scoring of different components using CT images, with the scoring of dorsal plateau changes exhibiting greater repeatability in comparison.
No statistically significant sex differences were observed with the scoring of all three components (dorsal plateau: p = 0.819, Z-score = −0.228; ventral rampart: p = 0.877, Z-score = −0.154; symphyseal rim: p = 0.060, Z-score = −1.880). No statistically significant bilateral differences (p > 0.05) were observed with the scoring of individual components (dorsal plateau: p = 0.405, Z-score = −0.832; ventral rampart: p = 0.236, Z-score = −1.185; symphyseal rim: p = 0.097, Z-score = −1.661). Owing to the lack of significant bilateral differences, further statistical analysis was undertaken with the left pubic bone.
An overall statistically significant correlation of 0.513 and 0.313 was obtained between morphological features pertaining to different cumulative scores, and documented age, in males and females, respectively. Amongst the three components, ventral rampart displayed the strongest correlation with age in both males (0.561) and females (0.333). In males, the dorsal plateau and symphyseal rim garnered correlation values of 0.495 and 0.463, respectively. In females, the corresponding correlations obtained were 0.283 and 0.302, respectively. Males displayed a relatively stronger correlation in comparison to females. An additional partial correlation analysis between all three components while controlling for age yielded statistically significant residual correlations between the components, in both sexes. With males, the correlation between individual components ranged from 0.754 to 0.851, whereas in females, this partial correlation ranged from 0.481 to 0.613.
Using the age ranges reported by McKern–Stewart, an overall accuracy percentage of 68.90% was obtained in males. The corresponding values for overall inaccuracy and bias, computed using mean ages given by McKern–Stewart for cumulative scores 0–15, were 15.12 years and −12.03 years. Highest and lowest accuracy percentages were obtained with the symphyseal rim and the dorsal plateau, respectively. Highest inaccuracy and bias values were obtained with the ventral rampart, whereas lowest error computations were furnished with the symphyseal rim (Table 3).
Hazard parameters, computed with the informative prior, for males include a3 (baseline mortality) = 0.003944482, b3 (senescent component) = 0.06188876, and shift (minimum age in the informative prior) = 10 years. With females, the corresponding hazard parameters were 0.001052896, 0.1, and 15 years, respectively. HPD and HPDR pertaining to each individual component are shown in Table 4. Higher HPD values were observed in females for all three components.
Accuracy, inaccuracy, and bias obtained with Bayesian analysis in males and females is shown in Table 5. Highest accuracy percentages of 92.00% were obtained with the ventral rampart, in males, whereas the dorsal plateau and symphyseal rim garnered highest accuracy percentages of 82.00% in females. Lowest error computations were observed with the symphyseal rim in males, and the ventral rampart in females. Males, in comparison to females, furnished higher accuracy percentages, and lower inaccuracy and bias values for all three components. Using Bayesian analysis, a tendency of under-aging was observed with the dorsal plateau and symphyseal rim in males. With females, over-aging was obtained throughout (Table 5).
Bartlett’s test (p < 0.001) and Kaiser–Meyer–Olkin test (KMO measure = 0.716) indicated a satisfactory correlation between the three components, permitting a principal component analysis of data (Kaiser 1970; Dziuban and Shirkey 1974). Summary age models yielded inaccuracy and bias values of 11.51 years and −0.40 years, respectively, in males. The corresponding error computations obtained with females were 17.92 years and 13.04 years, respectively (Table 6).
Discussion
The pubic symphysis constitutes a robust and relatively immobile region within the human pelvis. This limited mobility, coupled with its gradual display of developmental and degenerative changes, renders the pubic symphysis an ideal marker for human age estimation (Lungmus 2009). With the aim of exploiting these advantages for human identification, Todd, in 1920, derived the first pubic symphyseal age estimation method by grouping transpiring morphological changes into ten distinct phases (Todd 1920). In order to overcome limitations encountered within Todd’s method, McKern–Stewart, in 1957, subsequently devised their three-component age estimation method using skeletal remains of young American males (McKern and Stewart 1957). Their approach, a modification of Todd’s ten-phase method, grouped observed morphological changes into what they considered to be three independently developing components. They believed that such a component-based approach would not only confer objectivity to the evaluation process but also encompass the individual variability overlooked within Todd’s method (McKern and Stewart 1957; Lungmus 2009). A systematic review and meta-analysis of data procured from several studies employing the McKern–Stewart method indicated that the method demonstrates uniformity for aging the human pubic symphysis of different population affinities (Warrier et al. 2022a). However, this review could not empirically comment on the overall accuracy and precision associated with the method, as observational studies incorporated within the review had not reported the same.
The present study endeavoured to ascertain the applicability of the McKern–Stewart method, through computations of accuracy and precision by employing an equally represented male and female study group. While no statistically significant sex differences were observed with the scoring of individual components, a negligible to low positive correlation (Mukaka 2012; Hinkle et al. 2003) with age was obtained in females. Males, on the other hand, furnished a moderate positive correlation (Mukaka 2012; Hinkle et al. 2003) with age. Our findings pertaining to sexual symmetry are in contrast to those reported by Sharma et al. (2008). However, female participants within this singular investigation were significantly under-represented in comparison to males. Our study attempted to overcome this methodological limitation by incorporating an equal number of male and female participants. Similar investigations employing homogenously represented population groups are currently wanting in order to validate our findings pertaining to sexual symmetry. Within the present investigation, no statistically significant bilateral differences were observed during the scoring of individual components. Our findings pertaining to bilateral symmetry corroborate those of previous studies (Sharma et al. 2008; Kumar et al. 2009; Gorchiya et al. 2020). Hence, either pubic symphysis can be utilized for age estimation with equal vigour, and by extension, human identification.
Regarding the primary objective of this study, i.e., establishing the accuracy and precision of the McKern–Stewart method in Indian males, overall low accuracy percentages of 68.90% were obtained. Lungmus (2009) reported higher accuracy percentages of 77.80% with males of the Bass collection, in comparison to the present study. Amongst the three components, symphyseal rim yielded highest accuracy percentages and dorsal plateau the lowest. Overall inaccuracy and bias values obtained with males herein are comparable to those reported by Lungmus (2009). Highest and lowest inaccuracy and bias values were obtained with the ventral rampart and the symphyseal rim, respectively, in males. Our findings pertaining to the differential accuracy percentages, inaccuracy, and bias values obtained across the three components could not be corroborated due to a lack of similar data. An overall tendency of under-aging was observed on applying the McKern–Stewart method to Indian males. This could be attributed to the age structure of the original study population which comprised largely of younger males. Low accuracy percentages and high error rates garnered within the present investigation indicates that the McKern–Stewart method, in its primal form, lacks both accuracy and precision, a vital requisite within forensic, bioarchaeological, repatriation, and humanitarian contexts. Moreover, applying mean ages and age ranges reported by McKern–Stewart within their original study to different population groups can result in age mimicry (Vossoughi et al. 2022), thus garnering imprecise estimates of age and dampening the applicability of the method.
In order to overcome these issues of age mimicry and furnish more accurate estimates of age, a Bayesian analysis of McKern–Stewart’s components was undertaken, in keeping with the second objective of this study. Since the applicability of the McKern–Stewart method in its primal form was not evaluated for females, as the original study reports descriptives for male remains alone, applicability of these three components in aging males and females of an Indian population was subsequently evaluated through Bayesian inference. Such a Bayesian analysis using McKern–Stewart’s components is presently lacking.
Obtained Bayesian HPD values suggest that pubic symphyseal changes described by McKern and Stewart transpire at a much later age in females, with scores 2–5 for all three components garnering mean ages ≥40 years. Contrary to this, with males, a gradual progression from development to degeneration was observed with increasing age. These findings indicate that age-related changes transpiring within female pubic bones cannot be efficiently elucidated using McKern–Stewart’s components. Higher inaccuracy and bias values obtained with females corroborate the limited applicability of McKern–Stewart’s components in aging this sex. Hence, an in-depth understanding of the anatomical construct of different age markers, as well as the various intrinsic and extrinsic factors influencing the aging process, is warranted prior to devising and applying age estimation methods for human identification.
High accuracy percentages were obtained on applying HPDR values garnered with Bayesian analysis to males and females of the test group. Higher accuracy associated with a Bayesian approach, as opposed to the simple descriptive analysis of data/non-Bayesian approach, can be ascribed to the age brackets garnered with the former. Broader, closed age brackets were computed using Bayesian analysis, as opposed to the optimistically narrow age intervals described by McKern–Stewart for scores 0–4, and the open-ended age cohorts described by them for score 5, of each component. The increment in accuracy percentages obtained with individual components can be attributed to these realistic yet broad age brackets garnered with Bayesian analysis. These broad confidence intervals, in turn, illustrate the wide variability associated with changes transpiring within each component. Since McKern and Stewart scrutinized and described pubic symphyseal changes presenting within young pubic bones alone, they were unable to accommodate for features specific to older individuals. Thus, all individuals presenting with a score 5, i.e., a flat and granulated dorsal demi-face, and/or, a completed rampart, and/or, a broken rim with rarefaction of the symphyseal face, were coalesced into a single broad age category, inclusive of both young and old individuals. Incorporating a scored evaluation of additional features described by Hartnett (2010) might help further differentiate between younger and older individuals, garnering narrower age brackets.
Accuracy and precision values computed within the present investigation demonstrate the superior performance of Bayesian analysis, over the conventionally employed descriptive statistics for age estimation. Furthermore, the significant under-aging observed initially on applying the McKern–Stewart method to males was also redressed through Bayesian analysis. However, an effective application of Bayesian inference warrants the careful selection of an informative prior, with best results garnered when the informative prior and the target population exhibit similar demographic characteristics. In forensic, bioarchaeological, and repatriation contexts, the target sample constitutes the unknown, and thus pertinent information regarding the demographic profile of the target is, more often than not, lacking. Previous investigations have demonstrated that even when the informative prior and target sample originate from different population groups, the overall accuracy obtained with Bayesian analysis remains higher than those obtained with a descriptive reporting of data (Godde and Hens 2012). Alternatively, a uniform prior may also be employed for age estimation (Godde and Hens 2012).
Previously undertaken investigations with the McKern–Stewart method utilized cumulative score-based approaches for age estimation (Sinha and Gupta 1995; Sharma et al. 2008; Kumar et al. 2009; Kumar 2011; Singh et al. 2013; Prasad et al. 2015; Selvamurugan et al. 2019; Javvadi et al. 2016; Kumaran et al. 2019; Janardhan et al. 2016; Pal and Tamankar 1983). However, such an approach presents with the issue of assigning equal weight to all contributing components. Similar investigations with the acetabulum have empirically demonstrated that individual features contribute differentially towards the final estimate of age (Warrier et al. 2022b, c). The differing accuracy percentages, inaccuracy, and bias values obtained herein using both descriptive analysis and Bayesian statistics substantiate the same. The statistically sound approach for multivariate age estimation using all three components involves incorporating the partial correlation between all three components (Boldsen et al. 2002). Failure to do so reinforces the assumption of conditional independence, resulting in age ranges that are too narrow, and hence, imprecise (Sgheiza 2022). Partial correlations obtained herein between the three components invalidate this assumption of conditional independence. Nevertheless, the computational syntax required in order to carry out such a multivariate analysis (Boldsen et al. 2002; Hirk et al. 2020; Genz et al. 2021) was found to be quite complicated. As an alternative, a simplified multivariate approach has been suggested within this study-weighted summary age models.
Within these models, the generated intercorrelation matrix is subjected to principal component analysis, and the correlation of individual components with the first principal component is taken as the weight of each component (Lovejoy et al. 1985). The resulting weights were subsequently utilized to generate weighted summary age models, in keeping with the tertiary and final objective of this study. Summary age models derived using McKern and Stewart’s components garnered lower error rates in comparison to Bayesian error computations for the dorsal plateau and the ventral rampart, in males. The symphyseal rim, however, furnished even lower inaccuracy and bias values in comparison to summary age models, illustrating its efficiency as an independent age marker in males. With females, summary age models garnered lower error rates in comparison to the symphyseal rim, alone. An overall tendency to over-age females and under-age males was demonstrated through summary age models.
Although the present study indicated no statistically significant sex differences with McKern–Stewart’s components, weaker correlations, lower accuracy percentages and higher inaccuracy, and bias values were obtained with females. Furthermore, the three components described by McKern and Stewart fail to appropriately accommodate for age-related changes transpiring within the female pubic bone. While Bayesian analysis and summary age models did garner increased accuracy and precision with males of the study group, overall error computations associated with the method remain still quite high. Moreover, Bayesian age brackets, while realistically account for individual variability, are too broad to be of practical utility for human identification. Thus, McKern–Stewart’s age estimation method exhibits limited applicability for males and females of an Indian population. Alternative pubic symphyseal age estimation methods such as those devised by Suchey–Brooks (1990), Gilbert–McKern (1973), Berg (2008), and Hartnett (2010) should be investigated for an Indian population.
Computed tomographic investigations are slowly taking precedence over gross macroscopic examination due to the numerous advantages that they offer. CT scans remain resistant to superimposition induced artefacts and magnification errors, problems commonly encountered with alternate visualization techniques of conventional radiography (Ekizoglu et al. 2016; Lottering et al. 2017; Carew et al. 2019). Previously undertaken CT-based investigation with the McKern–Stewart method indicates a satisfactory reproduction of morphological changes on CT scans (Gorchiya et al. 2020). CT-images obtained within the present study corroborate these findings. Low inter- and intra-observer errors associated with the scoring of individual components, too, validate the potential of CT for age estimation. Computed tomographic examinations can further be extrapolated to incorporate various sub-surface features for age estimation (Villa et al. 2013). Trabecular bone criteria, scrutinized within previous investigations, have illustrated satisfactory results as an age marker (Acśadi and Nemeskéri 1970). Incorporating these additional features might help further enhance the significance of CT for human age estimation. Despite these multifarious advantages, the use of computed tomography for age estimation is not recommended in living individuals. Alternatively, clinically obtained CT data can be relied on as a corroborative evidence for age estimation in repatriation and humanitarian contexts. Furthermore, post-mortem CT evaluations can be undertaken in the deceased to enable a non-invasive evaluation of age-related changes within forensic and bioarchaeological contexts.
The present study incorporated CT scans of individuals undergoing routine examinations following the advice of their treating physicians, and thus, a large, homogenous representation of participants within the informative prior and study group could not be ensured. A quasi-novel observation within this study was that age-related pubic symphyseal changes can be appreciated in males and females as young as 10 years old.
Conclusion
The McKern–Stewart method for pubic symphyseal age estimation simplifies the evaluation of age-related changes through its component-based approach. No statistically significant bilateral differences were observed with the scoring of the pubic bone, indicating that either pubic symphysis can be utilized for human age estimation with equal vigour. While no statistically significant sex differences were observed with McKern–Stewart’s components, a weaker correlation, lower accuracy percentages, and higher error rates were observed in females. Thus, an in-depth understanding of the anatomical construct of different age markers, as well as various intrinsic and extrinsic factors influencing the aging process in both sexes, is warranted prior to utilizing different age estimation methods. Inaccuracy and bias values computed with descriptive analysis, Bayesian inference, and principal component analysis demonstrate the limited applicability of the McKern–Stewart method for human age estimation within forensic, bioarchaeological, repatriation, and humanitarian contexts. Alternate methods should be explored to enable accurate and precise human identification.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
3D Slicer image computing platform | 3D Slicer [Internet]. [cited 2022 Feb 7]. Available from: https://www.slicer.org/
Acsadi G, Nemeskeri J (1970) History of human life span and mortality. Akadémiai Kiadó, Budapest
Bartolini V, Pinchi V, Gualco B, Vanin S, Chiaracane G, D’Elia G et al (2018) The iliac crest in forensic age estimation: evaluation of three methods in pelvis X-rays. Int J Legal Med 132(1):279–288. https://doi.org/10.1007/s00414-017-1629-z
Bedford ME, Russell KF, Lovejoy CO, Meindl RS, Simpson SW, Stuart-Macadam PL (1993) Test of the multifactorial aging method using skeletons with known ages-at-death from the Grant Collection. Am J Phys Anthropol 91(3):287–297. https://doi.org/10.1002/ajpa.1330910304
Berg GE (2008) Pubic bone age estimation in adult women. J Forensic Sci 53(3):569–577. https://doi.org/10.1111/j.1556-4029.2008.00712.x
Boldsen JL, Milner GR, Konigsberg LW, Wood JW (2002) Transition analysis: a new method for estimating age from skeletons. In: Hoppa RD, Vaupel JW, Hoppa RD, Vaupel JW (eds) Paleodemography. Cambridge University Press, pp 73–106
Brooks S, Suchey JM (1990) Skeletal age determination based on the os pubis: A comparison of the Acsádi-Nemeskéri and Suchey-Brooks methods. Hum Evol 5(3):227–238
Buckberry JL, Chamberlain AT (2002) Age estimation from the auricular surface of the ilium: a revised method. Am J Phys Anthropol 119(3):231–239. https://doi.org/10.1002/ajpa.10130
Carew R, Viner M, Conlogue G, Grant N, Beckett S (2019) Accuracy of computed radiography in osteometry: A comparison of digital imaging techniques and the effect of magnification. J Forensic Radiol Imaging 19:100348. https://doi.org/10.1016/j.jofri.2019.100348
Chen X-P, Zhang Z, Tao L (2008) Determination of male age at death in Chinese Han population: using quantitative variables statistical analysis from pubic bones. Forensic Sci Int 175(1):36–43. https://doi.org/10.1016/j.forsciint.2007.04.231
Dziuban CD, Shirkey EC (1974) When is a correlation matrix appropriate for factor analysis? Some decision rules. Psychol Bull 81:358–361
Ekizoglu O, Inci E, Erdil I, Hocaoglu E, Bilgili MG, Kazimoglu C et al (2016) Computed tomography evaluation of the iliac crest apophysis: age estimation in living individuals. Int J Legal Med 130(4):1101–1107. https://doi.org/10.1007/s00414-016-1345-0
Fedorov A, Beichel R, Kalpathy-Cramer J, Finet J, Fillion-Robin JC, Pujol S et al (2012) 3D slicer as an image computing platform for the quantitative imaging network. Magn Reson Imaging 30(9):1323–1341. https://doi.org/10.1016/j.mri.2012.05.001
Garvin HM, Passalacqua NV (2012) Current practices by forensic anthropologists in adult skeletal age estimation. J Forensic Sci 57(2):427–433. https://doi.org/10.1111/j.1556-4029.2011.01979.x
Genz A, Bretz F, Miwa T, Mi X, Leisch F, Scheipl F, et al (2021) mvtnorm: Multivariate normal and t distributions [Internet]. 2021 [cited 2023 Jan 26]. Available from: https://CRAN.R-project.org/package=mvtnorm
Getz SM (2020) The use of transition analysis in skeletal age estimation. WIREs Forensic Science 2(6):e1378. https://doi.org/10.1002/wfs2.1378
Gilbert BM, McKern TW (1973) A method for aging the female Os pubis. Am J Phys Anthropol 38(1):31–38. https://doi.org/10.1002/ajpa.1330380109
Godde K, Hens SM (2012) Age-at-death estimation in an Italian historical sample: a test of the Suchey-Brooks and transition analysis methods. Am J Phys Anthropol 149(2):259–265. https://doi.org/10.1002/ajpa.22126
Gorchiya A, Kochar SR, Pathak D, Shedge R (2020) The application of McKern-Stewart’s method for age estimation using Computed Tomography imaging of the pubic symphysis of living individuals. Forensic Imaging 23:200415. https://doi.org/10.1016/j.fri.2020.200415
Hall F, Forbes S, Rowbotham S, Blau S (2019) Using PMCT of individuals of known age to test the Suchey-Brooks method of aging in Victoria, Australia. J Forensic Sci 64(6):1782–1787. https://doi.org/10.1111/1556-4029.14086
Hanihara K, Suzuki T (1978) Estimation of age from the pubic symphysis by means of multiple regression analysis. Am J Phys Anthropol 48(2):233–239. https://doi.org/10.1002/ajpa.1330480218
Hartnett KM (2010) Analysis of age-at-death estimation using data from a new, modern autopsy sample--part I: pubic bone. J Forensic Sci 55(5):1145–1151. https://doi.org/10.1111/j.1556-4029.2010.01399.x
Hinkle DE, Wiersma W, Jurs SG (2003) Applied statistics for the behavioural sciences. Houghton Mifflin, Boston
Hirk R, Hornik K, Vana L (2020) mvord: An R package for fitting multivariate ordinal regression models. J Stat Softw. 93(4). https://doi.org/10.18637/jss.v093.i04
Hisham S, Abdullah N, Mohamad Noor MH, Franklin D (2019) Quantification of Pubic Symphysis Metamorphosis Based on the Analysis of Clinical MDCT Scans in a Contemporary Malaysian Population. J Forensic Sci 64(6):1803–1811. https://doi.org/10.1111/1556-4029.14125
Janardhan K, Subhedar A, Khan MT (2016) Determination of age by pubic symphysis metamorphosis in hyderabad population. Medico-Legal Update 16(2):232. https://doi.org/10.5958/0974-1283.2016.00097.9
Javvadi S, Agarwal S, Mestri S, Raj H, Kumar A, Kumar A (2016) A cross sectional study of age related pubic symphyseal changes in 3rd and 4th decades of life. Medico-Legal Update 16:114. https://doi.org/10.5958/0974-1283.2016.00025.6
Kaiser HF (1970) A second generation little jiffy. Psychometrika 35:401–415
Klepinger LL, Katz D, Micozzi MS, Carroll L (1992) Evaluation of cast methods for estimating age from the os pubis. J Forensic Sci 37(3):763–770
Konigsberg LW, Frankenberg SR (2013) Bayes in biological anthropology. Am J Phys Anthropol 152(S57):153–184. https://doi.org/10.1002/ajpa.22397
Kotecha SD (2016) Dental age estimation in children: a review. FRCIJ 3(1):264–267. https://doi.org/10.15406/frcij.2016.03.00085
Krogman WM, Iscan MY (1986) The human skeleton in forensic medicine. Charles C Thomas, Springfield
Kumar RGH (2011) Estimation of age by morphological changes in symphyseal surface of pubis in males - a cross sectional study. Rajiv Gandhi University of Health Sciences, Bangalore
Kumar A, Tyagi A, Banerjee K (2009) Estimation of age by pubic symphysis metamorphosis in East Delhi population. J Indian Acad Forensic Med 31(1):22–24
Kumaran M, Singh D, Bansal YS, Mandal SP, Murali G (2019) Applicability of Three Component System of Age Estimation in Haryana Population. Medico Legal Update 19(1):36–41. https://doi.org/10.37506/mlu.v19i1.879
Lottering N, MacGregor DM, Meredith M, Alston CL, Gregory LS (2013) Evaluation of the Suchey-Brooks method of age estimation in an Australian subpopulation using computed tomography of the pubic symphyseal surface. Am J Phys Anthropol 150(3):386–399. https://doi.org/10.1002/ajpa.22213
Lottering N, Alston-Knox CL, MacGregor DM, Izatt MT, Grant CA, Adam CJ et al (2017) Apophyseal ossification of the iliac crest in forensic age estimation: computed tomography standards for modern Australian subadults. J Forensic Sci 62(2):292–307. https://doi.org/10.1111/1556-4029.13285
Lovejoy CO, Meindl RS, Mensforth RP, Barton TJ (1985) Multifactorial determination of skeletal age at death: a method and blind tests of its accuracy. Am J Phys Anthropol 68(1):1–14. https://doi.org/10.1002/ajpa.1330680102
Lungmus EK (2009) An examination of error in the application of pubic aging techniques. The University of Montana, Montana
Lyle W (2022) Konigsberg’s webpage [Internet]. [cited 2022 Apr 26]. Available from: http://faculty.las.illinois.edu/lylek/
Madanraj SS (2021) Age estimation from morphological changes in pubic symphysis. IJFCM 8(3):161–165
McHugh ML (2012) Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 22(3):276–282
McKern TW, Stewart TD (1957) Skeletal age changes in young American males, analyzed from the standpoint of age identification. Headquarters Quartermaster Research and Development Command, Natick
Meindl RS, Lovejoy CO, Mensforth RP, Walker RA (1985) A revised method of age determination using the os pubis, with a review and tests of accuracy of other current methods of pubic symphyseal aging. Am J Phys Anthropol 68(1):29–45. https://doi.org/10.1002/ajpa.1330680104
Merritt CE (2018) Part II-adult skeletal age estimation using CT scans of cadavers: Revision of the pubic symphysis methods. J Forensic Radiol Imaging 14:50–57. https://doi.org/10.1016/j.jofri.2018.08.004
Miranker M (2016) A comparison of different age estimation methods of the adult pelvis. J Forensic Sci 61(5):1173–1179. https://doi.org/10.1111/1556-4029.13130
Moraitis K, Zorba E, Eliopoulos C, Fox SC (2014) A test of the revised auricular surface aging method on a modern European population. J Forensic Sci 59(1):188–194. https://doi.org/10.1111/1556-4029.12303
Mukaka M (2012) A guide to appropriate use of Correlation coefficient in medical research. Malawi Med J 24(3):69–71
Nikita E, Nikitas P (2019) Skeletal age-at-death estimation: Bayesian versus regression methods. Forensic Sci Int 297:56–64. https://doi.org/10.1016/j.forsciint.2019.01.033
Nikita E, Xanthopoulou P, Kranioti E (2018) An evaluation of Bayesian age estimation using the auricular surface in modern Greek material. Forensic Sci Int 291:1–11. https://doi.org/10.1016/j.forsciint.2018.07.029
Pal GP, Tamankar BP (1983) Preliminary study of age changes in Gujarati (Indian) pubic bones. Indian J Med Res 78:694–701
Pattamapaspong N, Kanthawang T, Singsuwan P, Sansiri W, Prasitwattanaseree S, Mahakkanukrauh P (2019) Efficacy of three-dimensional cinematic rendering computed tomography images in visualizing features related to age estimation in pelvic bones. Forensic Sci Int 294:48–56. https://doi.org/10.1016/j.forsciint.2018.10.003
Prasad MI, Babu M, Reddy GV et al (2015) Reliability of McKern and Stewart method for estimating age in males: an autopsy study in a teaching hospital in Tirupati. J Evid Based Med Healthc (2):3940–3944. https://doi.org/10.18410/jebmh/2015/558
Rissech C, Estabrook G, Cunha E, Malgosa A (2006) Using the acetabulum to estimate age at death of adult males. J Forensic Sci 51:213–229. https://doi.org/10.1111/j.1556-4029.2006.00060.x
RStudio Team (2022) RStudio: Integrated Development Environment for R. RStudio, PBC, Boston http://www.rstudio.com/
Ruengdit S, Prasitwattanaseree S, Mekjaidee K, Sinthubua A, Mahakkanukrauh P (2018) Age estimation approaches using cranial suture closure: A validation study on a Thai population. J Forensic Leg Med 53:79–86. https://doi.org/10.1016/j.jflm.2017.11.009
Selvamurugan A, Gokula Pandia Sankar M, Tamilmani K, Manivasagam M (2019) Component analysis of pubic symphysis morphology: is it still a gold standard tool of age assesment? Indian J Forensic Med Toxicol 13(3):53–56
Sgheiza V (2022) Conditional independence assumption and appropriate number of stages in dental developmental age estimation. Forensic Sci Int 330:111135. https://doi.org/10.1016/j.forsciint.2021.111135
Sharma G, Gargi J, Kalsey G, Singh D, Rai H, Sandhu R (2008) Determination of age from pubic symphysis: an autopsy study. Med Sci Law 48(2):163–169. https://doi.org/10.1258/rsmmsl.48.2.163
Shedge R, Kanchan T, Garg PK, Dixit SG, Warrier V, Khera P et al (2020) Computed tomographic analysis of medial clavicular epiphyseal fusion for age estimation in Indian population. Leg Med (Tokyo) 46:101735. https://doi.org/10.1016/j.legalmed.2020.101735
Shedge R, Kanchan T, Garg PK, Gupta Dixit S, Warrier V, Krishan K (2021) Age estimation from sternebral fusion in an Indian population - A computed tomographic evaluation. Leg Med (Tokyo) 53:101951. https://doi.org/10.1016/j.legalmed.2021.101951
Singh B, Aggrawal A, Mittal A (2013) A comparative study of symphyseal surface of pubic bone at autopsy for age estimation using Mckern - Stewart criteria. Medico-Legal Update 13:102. https://doi.org/10.5958/j.0974-1283.13.2.025
Sinha A, Gupta V (1995) A study on estimation of age from pubic symphysis. Forensic Sci Int 75(1):73–78. https://doi.org/10.1016/0379-0738(95)01772-b
Snow CC (1983) Equations for estimating age at death from the pubic symphysis: a modification of the McKern-Stewart method. J Forensic Sci 28(4):864–870
Todd TW (1920) Age changes in the pubic bone: I. The male White pubis. Am J Phys Anthropol 3:285–334. https://doi.org/10.1002/ajpa.1330030301
Truesdell J (2011) Living proof: applying the Suchey-Brooks method for ageing the os pubis to a living London population through computed tomography. University College London, London. https://doi.org/10.13140/RG.2.2.33946.75207
Villa C, Buckberry J, Cattaneo C, Lynnerup N (2013) Technical note: Reliability of Suchey-Brooks and Buckberry-Chamberlain methods on 3D visualizations from CT and laser scans. Am J Phys Anthropol 151(1):158–163. https://doi.org/10.1002/ajpa.22254
Vossoughi M, Movahhedian N, Ghafoori A (2022) The impact of age mimicry bias on the accuracy of methods for age estimation based on Kvaal’s pulp/tooth ratios: a bootstrap study. Int J Legal Med 136(1):269–278. https://doi.org/10.1007/s00414-021-02651-7
Warrier V, Shedge R, Garg PK, Dixit SG, Krishan K, Kanchan T (2022a) Applicability of the Calce method for age estimation in an Indian population: A clinical CT-based study. Leg Med 59:102113. https://doi.org/10.1016/j.legalmed.2022.102113
Warrier V, Shedge R, Garg PK, Dixit SG, Krishan K, Kanchan T (2022b) Computed tomographic evaluation of the acetabulum for age estimation in an Indian population using principal component analysis and regression models. Int J Legal Med. https://doi.org/10.1007/s00414-022-02856-4
Warrier V, Kanchan T, Garg PK, Dixit SG, Krishan K, Shedge R (2022c) CT-based evaluation of the acetabulum for age estimation in an Indian population. Int J Legal Med 136(3):785–795. https://doi.org/10.1007/s00414-021-02757-y
Warrier V, Shedge R, Krishan K, Kanchan T (2022d) McKern-Stewart method as a technique for analysing age related pubic symphyseal changes: A systematic review and metaanalysis. Med Sci Law 258024221092196. https://doi.org/10.1177/00258024221092196
Widek T, Genet P, Ehammer T, Schwark T, Urschler M, Scheurer E (2021) Bone age estimation with the Greulich-Pyle atlas using 3T MR images of hand and wrist. Forensic Sci Int 319:110654. https://doi.org/10.1016/j.forsciint.2020.110654
Wink AE (2014) Pubic symphyseal age estimation from three-dimensional reconstructions of pelvic CT scans of live individuals. J Forensic Sci 59(3):696–702. https://doi.org/10.1111/1556-4029.12369
Zhang K, Dong XA, Fan F, Deng ZH (2016) Age estimation based on pelvic ossification using regression models from conventional radiography. Int J Legal Med 130(4):1143–1148. https://doi.org/10.1007/s00414-016-1383-7
Acknowledgements
This research article is a part of an ongoing doctoral research being conducted by one of the authors (VW) in the Department of Forensic Medicine and Toxicology, All India Institute of Medical Sciences, Jodhpur, India. The principal author is grateful to the University Grants Commission, New Delhi for awarding the research fellowship (UGC-JRF) for pursuing PhD. The authors are also thankful to the individuals who participated in this study, and to the authorities of the institution for allowing us to conduct this research.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by VW, RS, and TK. The first draft of the manuscript was written by VW and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Approval was obtained from the Institutional Ethics Committee (Letter no. AIIMS/IEC/2019-20/1007) prior to commencement of the study. Compliance with ethical standards was ensured at each step of the present study.
Informed consent
All participants were informed about parameters of the study and CT images of consenting individuals were collected.
Conflict of interest
The authors declare no competing interests.
Additional information
Communicated by: Matthias Waltert
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Warrier, V., Shedge, R., Garg, P.K. et al. An evaluation of the three-component pubic symphyseal human age estimation method: a CT-based exploration in an Indian population. Sci Nat 110, 21 (2023). https://doi.org/10.1007/s00114-023-01851-y
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00114-023-01851-y