
Abstract
Purpose
To evaluate functional outcomes after direct suturing of upper extremity nerve defects in high elbow or wrist flexion.
Methods
A retrospective review was conducted in patients treated for median, ulnar, or radial nerve defects between 2011 and 2019. Inclusion criteria were a defect > 1 cm and a minimal follow-up period of 1 year. Nerve defects were bridged by an end-to-end suture in 90° elbow flexion or 70° wrist flexion for 6 weeks.
Results
Nine patients with a mean age of 30.2 years were included. The patients presented with two ulnar nerve defects, four median nerve defects, and three radial nerve defects at various levels. The mean time to surgery was 13.5 weeks for recent injuries. The mean defect length was 2.9 cm, and the mean follow-up time was 22.4 months. Two patients had joint stiffness that was more likely related to the associated injuries than the 6-week immobilization. Successful outcomes were achieved in eight of the nine patients. Meaningful motor recovery was observed in seven patients, and all recovered meaningful sensation. Excellent nerve recovery was noted in pediatric patients and in those with distal nerve defects.
Conclusion
Temporary high joint flexion allows for direct coaptation of upper extremity nerve defects up to 4 cm located near the elbow or wrist. In this small and heterogenous cohort, functional outcomes seemed to be comparable to those obtained with short autografting.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Selection of the proper treatment for peripheral nerve defects continues to pose a challenging problem due to a wide variability in approach and outcome depending on the nerve considered and the level of injury. Direct tensionless end-to-end repair achieves the most predictable outcomes [1, 2]. However, excessive tension has been shown to significantly impair regeneration across a nerve repair by causing a reduction in microvascular flow and an increase in scarring [2,3,4]. When a tension-free direct suture is not possible, defects in mixed nerves are addressed by autografts (which remains the gold standard treatment) or nerve transfers [1, 2].
Another alternative has been specifically developed for sciatic nerve defects in which autografts give mixed results due to the large to the size of the nerve in both diameter and length [5, 6]. This technique involves a direct end-to-end nerve coaptation with the knee flexed at 90° for 6 weeks, as initially described by Bourrel [7, 8] and improved by Oberlin and Rantissi [9]. Using this approach, we have found that defects up to 8 cm could be bridged with meaningful motor and sensory recovery in both sciatic nerve territories without an impairment of knee function [5, 6, 10].
Considering these promising results, we have applied this technique to limited-sized nerve defects in the upper extremity when we found that autografting should be avoided [11]. A similar strategy has been used by Roganovic [12, 13] to manage median and ulnar nerve defects caused by missile injuries during the Balkans war. However, in these latter studies, direct suturing was performed in a timely manner after the treatment of associated fractures by humerus shortening or external elbow fixation, with ulnar flexion already present at the time of nerve repair [12, 13]. Various authors have described both anterior transposition and elbow positioning to overcome ulnar nerve defects, but such procedures have only been rarely used to treat median or radial nerve defects [12,13,14,15,16,17,18].
The current study aims to evaluate functional outcomes following the repair of upper extremity nerve defects by end-to-end suturing with elbow or wrist flexion. We hypothesized that this strategy is safe, provides the same favorable results obtained with sciatic nerve defect repairs, and can be proposed as an alternative to autografting in certain circumstances.
Methods
Population studied
A retrospective study was conducted in patients with median, ulnar, or radial nerve defects treated by direct suturing in high elbow or wrist flexion between 2011 and 2019. The inclusion criteria were a nerve defect larger than 1 cm with a minimal follow-up period of 1 year. Patients with a shorter follow-up and those presenting with defects up to 1 cm were excluded, since such small defects can be treated by direct coaptation without high joint flexion. Institutional review board approval was obtained for the study, and all patients (or parents) gave their oral consent for the scientific use of any data or images obtained during treatment.
Operative protocol and postoperative care
End-to-end nerve coaptation was performed using a protocol similar to that described previously for sciatic nerve defect management [5,6,7,8,9]. The procedure began with a mobilization of the distal nerve stump before elbow flexion, or with a mobilization of the proximal nerve stump before wrist flexion. In cases of ulnar nerve defects at the elbow level, a subcutaneous anterior transposition was performed prior to nerve suturing [12, 14,15,16,17]. The nerve ends were brought together by elbow flexion at 90° or wrist flexion at 70°, and circumferential 9–0 sutures were placed before adding fibrin glue. During the postoperative period, the joint was immobilized in this position using a dorsal splint. The splint was retained in place for 6 weeks without dressing changes. No wound care was performed to avoid any deleterious joint motion exposing to nerve suture rupture. Splint removal was then followed by a gradual recovery of elbow or wrist extension, with a 2-week period of self-rehabilitation before starting active physiotherapy, to permit a very progressive stretching of the suture site [5].
Data analysis
The preoperative parameters collected were demographics, injury mechanism, injured nerve, defect level, and associated bone injury. Surgical parameters included time elapsed from trauma to surgery, nerve defect length, and eventual procedures combined for nerve repair. At the last follow-up, clinical outcomes were evaluated using the Medical Research Council’s Grading System for motor (M) and sensory (S) assessment and the Visual Analog Scale (VAS) for the patient’s perception of pain [19]. Electrodiagnostic examinations agreed with the physical examinations but were not analyzed since there were not carried out on all patients. Limitations in elbow or wrist range of motion were also assessed.
Motor recovery and global functional results in the distributions of the median, ulnar and radial nerves were assessed according to a standardized scoring system adapted from Kim et al. [20,21,22] (Tables 1 and 2). Motor recovery was defined as meaningful for a M score ≥ 3 in the nerve territory. Superficial pain sensation and some tactile sensation (S ≥ 2) had to be regained for meaningful sensory recovery [12, 13]. In cases of recent nerve injury, good and excellent recoveries were considered a successful outcome, and poor, fair, and moderate recoveries were considered an insufficient outcome. In cases of neuroma, a VAS score < 2 was considered successful. The outcomes were analyzed according to the injured nerve and the injury level.
Results
Nine patients (7 males and 2 females) with a mean age of 30.2 years (range 8–66 years) met the inclusion criteria during the study period (Table 3). The injury mechanisms included displaced fractures, open wounds, and iatrogenic trauma. The iatrogenic injuries occurred during carpal tunnel release (Case 6) or radial head arthroplasty revision (Case 9). The patients presented with two ulnar nerve defects, four median nerve defects, and three radial nerve defects at various levels, including one posterior interosseous nerve lesion. There were seven recent or subacute nerve injuries operated on after a mean time of 13.5 weeks (range 1–40 weeks), and two cases of neuroma-in-continuity of the median nerve lasting for several years (Fig. 1).

Case 6: Median nerve defect after excision of a neuroma-in-continuity (right). Direct suturing in 70° wrist flexion (left)
After nerve end trimming or neuroma resection, the mean nerve defect length was 2.9 cm (range 1.5–4 cm). Associated fractures mostly involved the humerus, including two supracondylar fractures in children (Fig. 2). The surgical procedures are detailed in Table 3. Anterior transposition was performed not only for the ulnar nerve but also for the radial nerve at the arm level. Combined procedures included bone internal fixation and tendon transfer.

Case 3: Median nerve defect related to a supracondylar humerus fracture in an 8-year-old boy (right—arrows show nerve ends before trimming). Direct suturing in 90° elbow flexion with a bowstringing effect (left)
The mean follow-up time was 22.4 months (range 12–48 months). Two patients presented with a limited articular range of motion following a gunshot injury to the elbow (Case 1) and a complex regional pain syndrome in the aftermath of an iatrogenic injury of the median nerve (Case 6). Successful outcomes were achieved in eight of nine patients (Table 4). There was only one insufficient result after repair of the ulnar nerve at the elbow level (Fig. 3). Meaningful motor recovery was observed in seven patients, but all recovered meaningful sensation. Excellent sensorimotor recovery was noted in pediatric patients and in those with distal nerve defects. Patients with long-lasting neuroma were free of pain but had a fair or moderate recovery. Good or moderate recovery was achieved in the other cases.

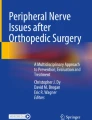
Case 1: Missile injury of the ulnar nerve at the elbow level (a). Nerve trimming led to a 4 cm defect (b). Direct suturing after anterior transposition of the nerve and positioning in 90° elbow flexion (c)
Discussion
To our knowledge, this is the first cases series reporting on direct suturing of median, ulnar, and radial nerves defects with elbow or wrist positioning. Using this simple technique, we achieved a successful outcome in almost all cases.
The rationale for direct nerve suturing with high joint flexion in the upper extremity is more to avoid nerve graft harvesting than to improve nerve recovery. Unlike in sciatic nerve repair, there is no strong difference in efficacy between delayed nerve suturing and grafting in the upper extremity (except for long nerve grafts) [11,12,13, 20,21,22,23,24]. Only primary nerve suturing provides clearly better results [23, 24]. The current technique, however, is particularly useful in various situations: (1) to permit primary or early nerve repair of a posttraumatic defect without the need to wait for a delayed grafting; (2) to deal with limited donor nerve graft material; (3) to avoid painful complications at the donor site in patients with chronic pain; (4) as a primary procedure in children when graft harvesting can be avoided. All these situations were seen in the current clinical series. We believe that direct suturing of short nerve defect should be considered in patients presenting with multi-tissue injury, particularly in those requiring combined bone fixation. This technique could also be useful for management of nerve defect with limited resources or in the context of war as described by Roganovic [11,12,13].
The functional outcomes presented in this small and heterogenous cohort can hardly be compared to those reported in the literature [12, 13, 20,21,22,23,24,25,26]. However, like many authors, we found excellent recovery for young patients, short delay between injury and repair, and distal nerve defects [12, 13, 20,21,22,23,24,25,26]. In agreement with Kitta et al. [18], we noticed that direct suturing with 90° elbow flexion provides highly favorable results in pediatric patients presenting with nerve defects associated with supracondylar humerus fractures. We believe that this is an excellent alternative to nerve grafting in this situation considering that these defects are usually short [27, 28]. Due to the very limited number of cases, we could not compare functional results between nerves, but direct repair of distal defects resulted in successful outcomes in most cases. Conversely, fair recovery was noticed in cases with proximal ulnar nerve defect and long-lasting median nerve neuroma which are well-known factors of poor prognosis [20, 22,23,24,25]. Late repair in patients with median nerve neuroma (Cases 4 and 5) was mostly performed with the objective to treat the pain rather than to permit sensorimotor recovery which is very uncertain in these chronic lesions [25]. For this reason, an opponensplasty was combined to nerve repair in Case 4 who complained about limited thumb opposition. Outcomes for the radial nerve were good or excellent because of distal injuries, pediatric patients, or combined tendon transfer. Although Murovic [24] and Kim et al. [21] have respectively reported a 68% and 81% M3 recovery after suture or grafting of radial nerve injuries at various levels, we are used to combining nerve repair and tendon transfer for proximal radial nerve injuries in adults for several reasons [11, 26, 29]. First, tendon transfers permit early restoration of active wrist extension, eliminating the need for orthosis. A limited transfer (pronator teres to extensor carpi radialis brevis) may be sufficient [26]. Tendon transfers also avoid developing a flexion contracture during nerve recovery and likely enhance neural regeneration by stimulating neurotrophic factors in damaged nerves, thus increasing axon regeneration potential [11, 29].
In this study, the mean defect length was 2.9 cm and we found that a gap of ~ 4 cm could be considered the maximum limit of this technique. One can argue that we unnecessarily used high joint flexion for small-sized defects, since some authors have claimed that defects up to 2.5 cm are accessible to direct suture after nerve end mobilization [1, 12, 13]. However, this assertion is questionable because such sutures were in fact achieved after anterior transposition of the ulnar nerve or moderate flexion in the adjacent joint [12, 13]. The maximal defect length accessible to end-to-end suture depends on the nerve size. In an experimental study, we found that direct suturing of sciatic nerve defects was only possible for gaps less than 2 cm [10]. In the upper extremity, the threshold length is probably ≤ 1 cm due to the elastic properties of the nerve [2].
The conditions for application of the technique varied according to the injury level. The elbow and wrist were obviously the most compliant levels where the largest nerve defects were suturable. A bowstringing effect was noticed after the suturing of 4 cm defects, but the nerves always remained deep enough not to interfere with skin closure (Figs. 2 and 3). In the elbow, prior anterior transposition of the ulnar nerve permitted a reduction in the gap, as demonstrated by various authors [2, 12, 14,15,16,17]. Smetana et al. [17] found that transposition alone reduces the defect length by 2 cm. Like Trumble [14] and Abrams et al. [15], we demonstrated that anterior transposition combined with elbow flexion can overcome gaps up to 4 cm (Fig. 3). Conversely, elbow flexion was less effective at bridging nerve gaps in the distal arm or proximal forearm. A 4 cm radial nerve defect was also bridged thanks to an anterior transposition of the nerve ends in front of the humerus using a double approach [30]. However, we did not apply this technique for brachial level ulnar nerve defects because the ulnar nerve normally glides in a distal direction with elbow flexion.
We acknowledge that a 6-week immobilization in high elbow or wrist flexion can be questionable regarding the risk of joint stiffness. High wrist flexion could also expose to complications such as complex regional pain syndrome or compartment syndrome. The rationale for this position and duration was to prevent tension at the suture site to minimize the development of fibrosis [2, 3]. We also decided to postpone physiotherapy after splint removal to permit a progressive and atraumatic recovery of extension, as we currently know that progressive limb elongation is possible without nerve damage [5, 9]. In this cohort, the limited articular range of motion noticed in two patients could not be attributed to the postoperative immobilization. Nevertheless, extended immobilization in 90° elbow flexion or 70° wrist flexion should be applied with caution based on associated bone and soft-tissue injuries.
This study has several limitations. First, its retrospective nature and the small size cohort make it necessary to draw conclusions carefully. In addition, this series is heterogenous regarding patient age, injury mechanism, and time to surgery. Lastly, combined tendon transfers partially biased nerve recovery assessment in two patients. However, a good sensory recovery and voluntary contractions of the reinnervated muscles attested to the success of nerve repair in these patients.
Conclusion
Temporary high joint flexion allows for direct coaptation of upper extremity nerve defects up to 4 cm located near the elbow or wrist. In this small and heterogenous cohort, functional outcomes seemed to be comparable to those obtained with conventional repair using short autografting. Careful patient selection, however, is essential to limit the risk of joint stiffness. This technique could advantageously avoid nerve grafting when combined procedures are required or in austere environments. We believe that it should be contemplated and evaluated on a larger scale.
References
Griffin JW, Hogan MV, Chhabra AB, Deal DN. Peripheral nerve repair and reconstruction. J Bone Joint Surg Am. 2013;95:2144–55.
Boyd KU, Fox IK. Nerve repair and grafting. In: Mackinnon SE, editor. Nerve surgery. New York: Thieme Medical Publishers; 2015. p. 75–100.
Millesi H. The interfascicular nerve grafting of the median and the ulnar nerves. J Bone Joint Surg Am. 1972;54:727–50.
Driscoll PJ, Glasby MA, Lawson GM. An in vivo study of peripheral nerves in continuity: biomechanical and physiological responses to elongation. J Orthop Res. 2002;20:370–5.
Mathieu L, Pfister G, Murison JC, Oberlin C, Belkheyar Z. Missile injury of the sciatic nerve: observational study supporting early exploration and direct suture with flexed knee. Mil Med. 2019;184:e937–44.
Mathieu L, Addas BMJ, Irimura SC, Oberlin C, Belkheyar Z. Management of sciatic nerve defects: lessons learned and proposal for a new strategy. Ann Plast Surg. 2020;84:559–64.
Bourrel P. Favorable results of sciatic nerve suturing performed 15 months after sectioning. Value of repeated exploratory surgery 2 months after the suturing. Mars Chir. 1965;175:203–8.
Bourrel P, De Bisschop G. Suture of the sciatic nerve performed 15 months after its section. Result 2 years later. Value of repeated exploration. Ann Chir. 1966;20:1145–9.
Oberlin C, Rantissi M. Gunshot injuries to the nerves. Chir Main. 2011;30:176–82.
Pfister G, Ghabi A, de Carbonnières A, Oberlin C, Belkheyar Z, Mathieu L. Direct suturing of sciatic nerve defects in high-degree knee flexion: an experimental study. World Neurosurg. 2020;133:e288–92.
Mathieu L, Goncalves M, Murison JC, Pfister G, Oberlin C, Belkheyar Z. Ballistic peripheral nerve injuries: basic concepts, controversies, and proposal for a management strategy. Eur J Trauma Emerg Surg. 2022. https://doi.org/10.1007/s00068-022-01929-8.
Roganovic Z. Missile-caused ulnar nerve injuries: outcomes of 128 repairs. Neurosurgery. 2004;55:1120–9.
Roganovic Z. Missile-caused median nerve injuries: results of 81 repairs. Surg Neurol. 2005;63:410–8.
Trumble TE. Overcoming defects in peripheral nerves. In: Gelberman RH, editor. Operative nerve repair and reconstruction. 1st ed. Philadelphia: JB Lippincott; 1991. p. 507–23.
Abrams RA, Fenichel AS, Callahan JJ, Brown RA, Botte MJ, Lieber RL. The role of ulnar nerve transposition in ulnar nerve repair: a cadaver study. J Hand Surg. 1998;23A:244–9.
Choudhry IK, Bracey DN, Hutchinson ID, Li Z. Comparison of transposition techniques to reduce gap associated with high ulnar nerve lesions. J Hand Surg Am. 2014;39:2460–3.
Smetana BS, Jernigan EW, Rummings WA Jr, Weinhold PS, Draeger RW, Patterson MM. Submuscular versus subcutaneous ulnar nerve transposition: a cadaveric model evaluating their role in primary ulnar nerve repair at the elbow. J Hand Surg Am. 2017;42(571):e1-7.
Kitta MI, Ariandi M, Nugroho YA, Nur A, Arden F. Neurological recovery across a 2-cm gap of radial nerve using end to end suture following supracondylar humerus fracture: case report. Int J Surg Case Rep. 2021. https://doi.org/10.1016/j.ijscr.2021.105896.
Medical research council of the United Kingdom. Aids to the examination of peripheral nervous system. Memorandum No. 45, London, Her Majesty’s Stationery Office, 1976.
Kim DH, Kam AC, Chandika P. Surgical management and outcomes in patients with median nerve lesions. J Neurosurg. 2001;95:584–94.
Kim DH, Kam AC, Chandika P, Tiel RL, Kline DG. Surgical management and outcome in patients with radial nerve lesions. J Neurosurg. 2001;95:573–83.
Kim DH, Han K, Tiel RL, Murovic JA, Kline DG. Surgical outcomes of 654 ulnar nerve lesions. J Neurosurg. 2003;98:993–1004.
Birch R, Raji ARM. Repair of median and ulnar nerves. J Bone Joint Surg Br. 1991;73:154–7.
Murovic JA. Upper-extremity peripheral nerve injuries: a Louisiana State University Health Sciences Center literature review with comparison of the operative outcomes of 1837 Louisiana State University Health Sciences Center median, radial, and ulnar nerve lesions. Neurosurgery. 2009;65:A11–7.
Ruijs AC, Jaquet JB, Kalmijn S, Giele H, Hovius SER. Median and ulnar nerve injuries: a meta-analysis of predictors of motor and sensory recovery after modern microsurgical nerve repair. Plast Reconstr Surg. 2005;116:495–6.
Pan CH, Chuang DCC, Rodríguez-Lorenzo A. Outcomes of nerve reconstruction for radial nerve injuries based on the level of injury in 244 operative cases. J Hand Surg Eur. 2010;35:385–91.
Ramachandran M, Birch R, Eastwood DM. Clinical outcome of nerve injuries associated with supracondylar fractures of the humerus in children. The experience of a specialist referral centre. J Bone Joint Surg [Br]. 2006;88B:90–4.
Kwok IHY, Silk ZM, Quick TJ, Sinisi M, MacQuillan A, Fox M. Nerve injuries associated with supracondylar fractures of the humerus in children. Our experience in a specialist peripheral nerve injury unit. Bone Joint J. 2016;98-B:851–6.
Hagemann C, Harhaus L. Combined distal nerve and tendon transfer in drop wrist for treatment of high injuries of the radial nerve. Oper Orthop Traumatol. 2021;33:399–404.
Acciari N, Davalli C, Poppi M, Scoto S, Staffa G. Interruption of the radial nerve at proximal level: reconstruction following anterior transposition. Chir Organi Mov. 1998;83:435–40.
Funding
No source of funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Mathieu, L., Diner, C., Chataigneau, A. et al. Treatment of upper extremity nerve defects by direct suturing in high elbow or wrist flexion. Eur J Trauma Emerg Surg 48, 4661–4667 (2022). https://doi.org/10.1007/s00068-022-01986-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-01986-z