
Abstract
Background
Between 2012 and 2016, Greece suffered yearly more than 800 deaths from road traffic incidents (RTIs), holding one of the worst performances in the European Union for RTI-related deaths per population. Our primary aim is to identify risk factors associated with mortality to set a targeted policy framework on road safety.
Methods
This is a retrospective analysis of data collected prospectively from Traffic Police. A correlation of 29 factors with adult drivers’ mortality was made, applying multivariate logistic regression models. At a second stage, a scoping literature review identified the best possible targeted prevention measures.
Results
A total of 93,019 drivers with a mean age of 42.2 ± 0.1 years were recorded, of which 2772 (3%) died. Age above 65 (aOR 3.1, p < 0.001), non-use of seatbelt (aOR 8.2, p < 0.001) or helmet (aOR 2.85, p < 0.001) and alcohol consumption (aOR 3.3 for cars, 4 for motorbikes, p < 0.001) were the driver-related parameters with the strongest correlation with a fatal outcome. Drivers’ behavior with specific high-risk maneuvers increased odds of death 2–4 times, depending on vehicle type. One-lane, rural road network was the environmental factor with the most significant impact. Based on the results of the analyses, our scoping review identified and suggested 23 specific measures for the Greek government and policymakers to examine.
Conclusion
Human-related factors were the parameters with the strongest impact on mortality after an RTI in Greece. These findings demonstrate an educational gap that must be primarily addressed with the introduction of missing road safety education in schools and an intensified and innovative population awareness campaign.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Trauma is a leading cause of death worldwide [1]. In Greece, road traffic incidents (RTIs) and falls almost equally account for as much as 75% of trauma [2]. RTIs, however, cause 60% of severe injuries (Injury Severity Score > 15), the majority of patients dead on arrival (DOA) [3] and have a large socioeconomic impact, affecting a much younger group of the population compared to falls. Reports suggest that more than half of RTI deaths occur within the first 1.5 h from the incident [4, 5]. Therefore, injury prevention is an integral part of road safety provision and campaigns in European countries have helped to reduce the burden from RTI-related trauma deaths.
Greece has made substantial steps in the road safety provision and managed to gradually improve from 18.1 deaths per 100,000 population in 1991 to a death rate of 7.6 per 100,000 inhabitants in 2016. However, this performance is still far from desirable, as Greece remains within the top five of the list of RTIs fatalities’ rate per population among the 28 EU countries (Fig. 1). This downward trend reached a plateau the last few years with an 8% decrease in the number of incidents but a small mortality increase of 0.5%. Currently, Greece does not have a trauma system with an associated registry and injury prevention program [6]. In the absence of these, RTI data to support the need for injury prevention can only be accessed by the Traffic Police (TP). To date, these data have never been analyzed in-depth and the characteristics of those involved in RTIs in Greece are currently unknown. Furthermore, the key factors associated with mortality after an RTI are unreported and it is not clear which parameters (human, road/environmental or vehicle-related) require urgent targeted prevention interventions (Fig. 2).

Source: Eurostat)
Road traffic fatalities per million inhabitants in the EU member states, 2016. (

Severity of outcome of participants in all officially recorded RTIs in Greece between 2012 and 2016 [7]
The primary aim of this study, therefore, is to utilize the census data to describe the demographics and epidemiological characteristics of the driving population involved in an RTI in the Greek region during the 5-year period (2012–2016). Secondly, to identify those risk factors that are associated with increased RTI mortality to plan targeted prevention with changes in laws, policies and traffic controls, as well as enhanced public education and awareness.
Materials and methods
Data sources
Raw data regarding the total of RTIs from 2012 to 2016 in the Hellenic region were granted with a special permission from the Hellenic Statistical Authority (ELSTAT) [7]. This is the most up-to-date 5-year period available, as 2017 data were not yet published at the study planning stage. All data are based on standardized forms collected prospectively and systematically on the scene from the TP and are subject to a 30-day follow-up of injured participants’ health status without a distinction between on-scene and delayed deaths within TP records.
Every driver involved in an RTI is included in this database, irrespective of the outcome. Exceptions were low energy incidents that may have caused no injuries and minor or no vehicle damage and for which TP was not present on-scene. Injuries are classified by the TP as mild or severe (which required hospitalization), with no clinical criteria recorded.
The dataset contained 58,955 incidents, including 100,043 vehicles. The 29 variables included were grouped into the human, vehicle, road and environmental/crash factors. The outcome was 30-day mortality. Weekend was defined as Friday from 18:00 to Sunday at 23:59 and seven national holidays throughout the year were included. We chose to use a zero-tolerance level of blood alcohol with concentrations varying widely in participants. Therefore, a BAC of 0.01 was considered as a positive test, while laws currently enforce a limit at 0.05.
Statistical analysis
Excel spreadsheets were entered and merged in the STATA 15 statistical package and each variable examined for missing data and errors. Chi-squared and ANOVA tests were used for categorical and continuous variables respectively. Post hoc analyses with adjusted residuals were used to determine which categories of a variable were mostly responsible for its p value. The level of significance was set at 0.01 due to the very large number of observations which could lead to amplification of insignificant effects (Type I error).
Multivariate logistic regression analyses were performed to correlate the independent factors with death in adult drivers. Participants with missing data were excluded from the multivariate analysis. All variables were initially entered into each model for car and motorbike drivers (“Appendix”). We then excluded those factors showing little or no association in a stepwise manner. A significance level of 0.1 for inclusion and 0.05 for exclusion from the logistic regression model was used. After each exclusion or addition, models were compared to each other with likelihood-ratio tests and Akaike and Bayesian information criterion (AIC/BIC) to establish goodness of fit and minimization of information loss [8]. Separate analyses were run for car and 2-wheel vehicle drivers.
This was a retrospective study of prospectively collected data, approved by ELSTAT ethics committee. All data are anonymous with unique identification numbers that cannot be matched to individuals. Website and less important references can be found in the bibliography in the “Appendix”.
Results
During this 5-year period, there were 93,019 driver-related RTIs recorded. Mean age was 42.2 years old for all drivers and those who died were older by 4 years. In a subgroup analysis, people aged 65 years or greater had a threefold probability of a fatal outcome (aOR 3.1, 2.1–4.6, 99%CI) compared to the 18–35 age group. 4 out of 5 were males, nine out of ten had a Hellenic nationality. Cars accounted for more than half of RTIs (55%) and motorbikes for a third (35%). Compared to cars, bicycles and motorcycles > 116 cc had a fivefold and threefold probability for a fatal outcome respectively. Approximately one-quarter of all cars involved in an RTI each year were manufactured prior to 2000.
Overall mortality was low at 3.0%, almost half of the cohort had no injuries (48.4%), whilst 44.8% had mild injuries and severe injuries affected 3.8%. Regarding modifiable human factors, almost a tenth of the population were positive for alcohol (8%), only two-thirds of motorcyclists wore helmets and 87% of car drivers had fastened a seatbelt, but with high unknown rates (around 40%) (Tables 1, 2, 3).
The strongest risk factors for crude mortality were non-use of seatbelts (RR 13.2, OR 15.2) or helmets (RR 4.4, OR 4.8) and a positive test for alcohol consumption (RR 7.1, OR 7.5). These factors remained the most significant determinants in multivariate analysis, with non-seatbelt use carrying an eightfold increased risk (aOR 8.2, 5.6–12.2, 99%CI) (Table 4). Alcohol consumption presented a threefold to fourfold risk for different categories, worse for 2-wheel drivers. Subgroup analysis of Blood Alcohol Content (BAC) showed that levels between 0.01% and 0.1% raised the probability of death by almost half (p = 0.03), while BAC levels > 0.1% had a sevenfold increase in death, compared to being completely sober.
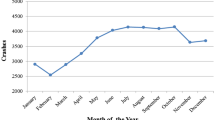
The summer period contained the most RTIs (36.5%) and driver deaths (38.7%), but the winter period and weekend raised adjusted risk for 2-wheel drivers (Appendix). Two-thirds of incidents took place between midday and midnight, however, the 00:00–06:00 period (9% of all incidents, 19% of fatal) increased risk, especially for 2-wheel drivers if lighting conditions were insufficient (aOR 1.80, p < 0.001). Regarding road type and characteristics, uninhabited areas were associated with more than half of fatal accidents (aOR 4.54, p < 0.001 for cars). This was more evident in one-lane, old national or county road network and non-highway parts of new national roads with no division wall.
Head-to-side collision was the most common type of crash occurring in one in two incidents, but higher probability of a fatal outcome was associated with collision with obstruction (aOR 3.54, p < 0.001) and lost control/off-road (aOR 2.85, p < 0.001). Responsible maneuvers analysis showed that one in four incidents was due to a STOP sign/red light violation, but most dangerous ones were entering opposite traffic flow (overtaking) and losing control of vehicle (Table 4). Excessive speeding was associated with a threefold risk of death for motorbike drivers (aOR 3.17, p < 0.001), but not for those in cars.
Discussion
This is the first large-scale study to have examined risk factors associated with high mortality after an RTI in Greece. Our results indicate that particular factors were significant in all our analyses, irrespective of the type of vehicle and driver/passenger classification. Increased age, no seatbelt or helmet use, alcohol consumption and travelling in one-lane road network outside inhabited areas are all strongly associated with road deaths. Other environmental and crash-related factors were found to be key factors of poor outcome in specific categories of road users. These findings elucidate the public health issue in Greece and support the need for robust intervention. Following our original study, we continued with a scoping review of the English and Greek literature to support our findings with specific suggestions on policymaking to enhance targeted prevention in road safety. These proposals are integrated into this discussion section and presented in Table 5.
Human-related factors
Age was strongly associated with poor outcome after a RTI. It could be argued that advanced age suggests more driving experience, while the young age is associated with risky and unexperienced driving, causing incidents of worse outcome [9]. However, age also plays a huge role physiologically to the outcome of an injured person and elderly drivers may have decreased reflexes and diminished vision or hearing causing an RTI to occur [10]. Our findings confirmed other studies to show that the most elderly group of people (aged 65 years or more) is the most vulnerable [11,12,13].
Seatbelt non-use was most powerfully correlated with a fatal outcome in all categories. The protective effect of seatbelt use could be overestimated with low-energy incidents that cause only damage to property and would not have caused an injury whatsoever. Nevertheless, one could argue that in these incidents, an injury was prevented with seatbelt use [13]. Underreporting of property damage only (PDO) accidents could also overestimate the protective effect, while a differential misclassification could have been possible if some uninjured or mildly injured drivers were mistakenly registered as restrained, possibly for insurance coverage issues. Findings showed that seatbelt use worsened from 2012 to 2016, in young males, rural regions, winter months and nighttime hours (00:00–06:00). These findings warrant further investigation into how they could guide targeted intensification of police controls. Specific efforts are required to target younger people, for example during the compulsory military service and in schools, especially in regions with high death rates, whilst social media (YouTube, Instagram) may have a more direct effect on the 15–24 age group [14].
Almost a third of motorbike drivers did not wear a helmet at the time of incident, which is an increase from the 28% non-use reported a decade ago in 4th Hellenic Road Safety conference. Male gender, age (18–30, 65 + years old), alcohol consumption, small motorbikes and rural regions were all factors that lowered the probability of helmet use. Helmet use varies widely, and it may not be consistent even for the same individual [15]. Summer season, after hours (00:00–06:00) and weekends diminish the probability of helmet use, both for social reasons, limitation of the feeling of freedom, increased temperatures or higher alcohol consumption [16]. Alcohol not only lowers safety equipment use but impairs driving ability [17]. For people aged 15–29 in Europe, driving under the influence is one of the main causes of mortality [18]. Alcohol use was strongly associated with male gender, motorbikes < 115 cc, weekends, the 00:00–06:00 h, winter months and rural regions. Matching these findings with the current socioeconomic reality, DUI seems to be chosen over increased night rates of taxis due to non-existence of public transport during late hours [19]. At the same time, instead of increasing taxes on alcohol, government could propose alcohol companies to invest in the awareness and education campaign as a countermeasure.
Vehicle-related factors
In 2016, Greece earned a disheartening first place among all 28 EU countries in the death rate per population of motorbike drivers, 24 deaths per million inhabitants, more than three times the average in the Union. Our regression analysis revealed a fivefold and threefold risk of death for bicycle and any kind of motorcycle driver, respectively, when compared to cars. High fatality could be attributed in a number of factors, but predominately user’s exposed position and non-helmet use. Amongst two-wheeled vehicles, bicycle riders were the most vulnerable users. Designated bicycle lanes are scarce throughout the country; however, bike riders rarely wear protective equipment and tend to jump red lights or STOP signs. It is, therefore, apparent that new infrastructure would not be enough, but road safety education is also needed.
Whilst the age of the vehicle was not strongly associated with the outcome, it may explain the reduced seatbelt use in a quarter of the population. As fewer cars released before 2000 are in circulation, modern vehicle construction will hopefully diminish this factor. Similarly, large engine capacity was not correlated with adverse outcome. Locally, it is suggested that the recent economic crisis in Greece has caused a substantial proportion of vehicles to be badly maintained, and as a result, a mechanical problem or tyre failure could be the cause of a serious accident. No detailed information on the maintenance level of the vehicles could be accessed, however, at the time of the accident, around 6% of the vehicles had not been through MOT testing.
Environmental and crash-related factors
There was a regional variation for the high death rates associated with RTIs in Greece. Attica (Athens metropolitan area) experiences nearly at five deaths per 100,000 population per year, whilst many rural regions including islands of south Aegean and Crete, Epirus, Central and Western Greece exceed ten deaths per 100,000 population per year [6]. Our findings confirmed some previous reports of increased alcohol consumption in these regions, poor seatbelt and helmet use, as well as specific characteristics of the road network [6, 20]. One-lane county, communal or old national roads with insufficient lighting conditions during night hours were associated with increased deaths. Older people may also be at increased risk if situated outside urban centers especially after retirement [21]. A study by Hasselberg et al. in 2005 suggested that education levels, lower-income and social status also raise the risk for traffic violations and more serious incidents in these regions [22].
From an environmental perspective, motorbike drivers may face an increased risk of an RTI during the winter season, not only due to a slippery surface but also decreased daytime illumination and increased alcohol consumption [13]. Poor weather and road surface conditions did not have a significant effect in this study, possibly due to speed adjustments and an increased state of alert under adverse conditions [23]. The 00:00–06:00 period had a higher probability for a fatal outcome for all-drivers, but this was a stronger association for 2-wheel drivers, together with the 07:00–08:00 rush hour. This confirms the findings of an increased rate of traffic violations in a previous study, as drivers may not be fully alert yet or hurry not to be late at work or school [24].
Overtaking, excessive speeding and losing control of vehicle were the most probable maneuvers or errors to cause a fatality, while collision with fixed obstruction and head-on were strongly associated with alcohol consumption. All the above dangerous maneuvers and errors explain why driving in a one-lane, high-speed road deserves a heightened level of alertness for anyone driving in the regional and rural road network.
Limitations of study
Whilst this retrospective study is based on data gathered by thousands of different observers, not every incident was recorded which may result in a potential overestimation of the effect of some risk factors. Furthermore, variability may exist in the completion of the standardized forms with more severe incidents drawing more attention and detailed recording [25]. This database does not contain clinical information, therefore, we were unable to examine clinical variables which may be associated with outcome. We had no information about distraction from mobile phones or sleepiness as a possible cause of RTI. No distinction is made between DOAs and later deaths, as no time to death confirmation was available. Moreover, the lack of additional data of risk exposure and performance indicators, the results of the analyses can only ensure correlation and not causation.
One of the major limitations of this study is the unknown percentage of seatbelt and helmet use. The Police did not record the information in more than 40% and 30% for car and motorbike drivers respectively, with comparable traffic studies recorded 20–30% rates of non-reporting [13, 23]. This may suggest that information is reported only if the observer is absolutely sure, certifying the validity of complete data. However, we were able to analyse the remaining proportion of seatbelt and helmets, with strong associations found with non-use. A high proportion of fatalities did not have results reported on alcohol consumption, possibly due to it not being tested by regional forensic services or the non-reporting back to the Police. Our findings have shown that where available, alcohol presence had a significantly deleterious effect, therefore, serious RTIs should be ideally investigated by a dedicated Forensic Crash Unit [23] as part of a wider, national injury prevention strategy.
Conclusion
These findings that derived from the official data of RTIs in Greece over the last 5 years indicate that human factors play a predominant role in the high mortality rates observed. In terms of preventive initiatives, the key may be to change people’s attitudes. Educational campaigns to raise awareness in schools, intensified in high-risk regions, could help to empower children to alter parental road safety behavior. At the same time, road traffic education will hopefully make future drivers, better drivers. Traffic Police controls should be denser during weekends and after hours and emphasize on high-risk regions until road network improvement is gradually accomplished. Future studies would ideally draw clinical information on the participants from a national trauma registry. Until then, targeted prevention strategy is readily available and should aim to further decrease the number of lives lost on the civilian battlefield of the road network.
Data availability statement
Application for provision of data from Hellenic Statistical Authority was made on Oct 18th and approved by the ethics committee on Nov 19th with protocol number ΓΠ—529/21.11.2018. Forms regarding the “Contract on access to confidential data for research purposes” have been signed, which declare that raw data cannot be published.
References
World Health Organization (2016). Global Health Observatory (GHO) Data. https://www.who.int/gho/mortality_burden_disease/causes_death/top_10/en/. Accessed 21 Jun 2019.
Prionas A, Toulias A, Tsoulfas G, Papadopoulos VN. Measuring the impact of trauma in Greece: a systematic review of greek trauma registries. Is quality improvement achievable? Hell J Surg. 2018;90(2):75–84.
Katsaragakis S, Theodoraki ME, Toutouzas K, Drimousis PG, Larentzakis A, Stergiopoulos S, et al. The implementation of a national trauma registry in Greece. Methodology and preliminary results. J Trauma. 2009;67(6):1421–5.
Trunkey DD. Trauma, accidental and intentional injuries account for more years of life lost in the US than cancer and heart disease. Among the prescribed remedies are improved preventive efforts, speedy surgery and further research. Sci Am. 1983;249(2):28–35.
Gunst M, Ghaemmaghami V, Gruszecki A, Urban J, Frankel H, Shafi S. Changing epidemiology of trauma deaths leads to a bimodal distribution. Proc (Bayl Univ Med Cent). 2010;23(4):349–54.
Anagnostou E, Larentzakis A, Vassiliu P. Trauma system in Greece: Quo Vadis? Injury. 2018;49(7):1243–50.
Hellenic Statistical Authority—Elliniki Statistiki Arxi (ELSTAT). Road traffic accidents and persons injured therefrom (2012–2016). Athens; (2012)
Sawa T. Information criteria for discriminating among alternative regression models. Econometrica. 1978;46(6):1273–91.
Bates LJ, Davey J, Watson B, King MJ, Armstrong K. Factors contributing to crashes among young drivers. Sultan Qaboos Univ Med J. 2014;14(3):e297–305.
Rubin GS, Ng ES, Bandeen-Roche K, Keyl PM, Freeman EE, West SK. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE study. Invest Ophthalmol Vis Sci. 2007;48(4):1483–91.
Massie DL, Campbell KL, Williams AF. Traffic accident involvement rates by driver age and gender. Accid Anal Prev. 1995;27(1):73–877.
Lyman S, Ferguson SA, Braver ER, Williams AF. Older driver involvements in police reported crashes and fatal crashes: trends and projections. Inj Prev. 2002;8(2):116–20.
Valent F, Schiava F, Savonitto C, Gallo T, Brusaferro S, Barbone F. Risk factors for fatal road traffic accidents in Udine Italy. Accid Anal Prev. 2002;34(1):71–84.
Kuppuswamy S, Narayan SPB. The impact of social networking websites on the education of youth. Int J Virtual Communities Soc Netw. 2010;2(1):67–79.
Papadakaki M, Tzamalouka G, Orsi C, Kritikos A, Morandi A, Gnardellis C, et al. Barriers and facilitators of helmet use in a Greek sample of motorcycle riders: which evidence? Transp Res Part F Traffic Psychol Behav. 2013;18(1):89–988.
Germeni E, Lionis C, Davou B, Petridou ET. Understanding reasons for non-compliance in motorcycle helmet use among adolescents in Greece. Inj Prev. 2009;15(1):19–23.
Mitchell MC. Alcohol-induced impairment of central nervous system function: behavioral skills involved in driving. J Stud Alcohol Suppl. 1985;10:109–16.
Alonso F, Pastor JC, Montoro L, Esteban C. Driving under the influence of alcohol: frequency, reasons, perceived risk and punishment. Subst Abuse Treat Prev Policy. 2015;10(1):11.
Jackson CK, Owens EG. One for the road: Public transportation, alcohol consumption, and intoxicated driving. J Public Econ. 2011;95(1):106–21.
Muelleman RL, Mueller K. Fatal motor vehicle crashes: variations of crash characteristics within rural regions of different population densities. J Trauma. 1996;41(2):315–20.
EUROSTAT. Statistical atlas regional yearbook 2018. Median age. https://ec.europa.eu/eurostat/statistical-atlas/gis/viewer/?year=&chapter=02=. Accessed 21 June 2019.
Hasselberg M, Vaez M, Laflamme L. Socioeconomic aspects of the circumstances and consequences of car crashes among young adults. Soc Sci Med. 2005;60(2):287–95.
Siskind V, Steinhardt D, Sheehan M, O'Connor T, Hanks H. Risk factors for fatal crashes in rural Australia. Accid Anal Prev. 2011;43(3):1082–8.
Kingham S, Sabel C, Bartie P. The impact of the ‘school run' on road traffic accidents: a spatio-temporal analysis. J Transp Geogr. 2011;19(4):705–11.
Maas MW, Harris S. Police recording of road accident in-patients: Investigation into the completeness, representativity and reliability of police records of hospitalized traffic victims. Accid Anal Prev. 1984;16(3):167–84.
Acknowledgements
We would like to thank Mr. Georgiou Savvas for his contribution at the statistical analyses and Prof. Petridou Eleni for her initial guidance through the planning stage.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflict of interest to declare.
Rights and permissions
About this article

Cite this article
Anagnostou, E., Cole, E. Targeted prevention of road traffic deaths in Greece: a multifactorial 5-year census-based study. Eur J Trauma Emerg Surg 47, 1137–1152 (2021). https://doi.org/10.1007/s00068-019-01290-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-019-01290-3