
Abstract
Purpose
Major trauma remains a significant cause of morbidity and mortality in the developed and developing world. In 2013, nearly 5 million people worldwide died from their injuries, and almost 1 billion individuals sustained injuries that warranted some type of healthcare, accounting for around 10% of the global burden of disease in general. Behind the statistics, severe trauma takes a major toll on individuals, their families and healthcare systems. Management of the patient with severe trauma requires multiple interventions in a highly time-sensitive context and fragmentation of care, characterised by loss of information and time among disciplines, departments and individuals, both outside the hospital and within it, is frequent. Outcomes may be improved by better streamlining of pre- and intra-hospital care.
Methods
We describe the basis for development of a multi-stakeholder consortium by the European Critical Care Foundation working closely with a number of European Scientific Societies to address and overcome problems of fragmentation in the care of patients with severe trauma.
Result
The consortium will develop and introduce an information management system adapted to severe trauma, which will integrate continuous monitoring of vital parameters and point-of-care diagnostics. The key innovation of the project is to harness the power of information technologies and artificial intelligence to provide computer-enhanced clinical evaluation and decision-support to streamline the multiple points at which information and time are potentially lost.
Conclusions
The severe trauma management platform thus created could have multiple benefits beyond its immediate use in managing the care of injured patients.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Severe trauma, mainly resulting from traffic injuries and work accidents, can have a devastating impact on individuals, their families and society worldwide. Because the management of trauma is complex and time-sensitive, it requires sequential interventions to be performed by multiple pre- and intra-hospital teams. Numerous decision-makers are involved, causing fragmentation of care and delayed access to the right treatment, which is at least partially avoidable.
Fragmentation in healthcare has been defined as the process in which multiple decision makers make a set of decisions that would be made better through unified decision-making [1]. Individual decision makers may make sub-optimal decisions because of a lack of access to all the information. Fragmentation has been associated with poor outcomes and increased healthcare expenditure. There is ample evidence that integrating care through patient-centred approaches (termed streamlining in this manuscript) is associated with improved outcomes.
In this article, we summarise the epidemiology and impact of severe trauma, describe the factors that contribute to the fragmentation of care in this context, and examine the successful example of defragmentation of care in severe military trauma. Since most of the tools for streamlining care in civilian severe trauma do not exist, this White Paper formulates a strategic pathway for streamlining care in the civilian context, describes the tools needed, and outlines a phased project to develop the tools, and implement and evaluate improvements in the organisation of severe trauma care pathways.
Epidemiology of trauma
Major trauma continues to be an important cause of morbidity and mortality in the developed and developing world [2, 3]. In 2013, 973 million (uncertainty interval [UI] 942 to 993) individuals sustained injuries that warranted some type of healthcare, accounting for 10.1% (UI 9.5–10.8) of the global burden of disease in general; 4.8 million (UI 4.5 to 5.1) people died from injuries and years of life lost (YLLs) were responsible for 85.2% (UI 81.2–88.7) of injury disability-adjusted life years (DALYs) [3].
The principle contributors to injury DALYs are road and transport injuries (29.3%; UI 26.4–32.2), which are also among the most important leading causes of death for young individuals up to 24 years [4]. In 2013, nature-of-injury category “bone fractures of the lower extremities” (26.6%; UI 26.0–27.1) and the combination of multiple significant injuries (11.1%; UI 10.8–11.4) contributed most to the global years lived with disability (YLDs), the disability component of the DALY [3].
Causes, mechanisms and timing of deaths in trauma
Deaths from trauma and injuries display a predominantly bimodal distribution with a tendency towards elimination of the usual late peak in deaths and an overall shift towards earlier deaths [5, 6]. In recent years, death from exsanguination has become as frequent as lethal head injuries, but the incidence of fatal multi-organ failure is lower than previously reported [6]. Currently, injuries to the central nervous system, e.g. traumatic brain injury (TBI), and exsanguination are recognised as the most frequent time-sensitive pathologies and account for approximately 70% of all trauma-related deaths within the acute phase after impact [6, 7]. Rapid exsanguination has also been identified as the most common cause of preventable death after trauma, even during the pre-hospital phase of care [7,8,9], and this is frequently due to a delay in treatment (52.9% of cases in one study [10]). These epidemiological data underline the important burden that trauma continues to exercise on healthcare systems, society and individuals. Although prevention of trauma is a desirable goal, it is unlikely to be totally achievable. Hence, better management of trauma patients must be an immediate target and numerous recent reports strongly suggest that there is place for improvement, even in developed countries with well-structured healthcare systems [11,12,13].
Efficient management of severe trauma: a time-sensitive approach
Clinical observations have indicated that patients who receive rapid and definitive care soon after trauma have better outcomes than other patients [14, 15]. This has led to the introduction of comprehensive and integrated trauma management systems to deal with trauma victims promptly, following standardised protocols, thereby reducing the overall burden of the consequences of trauma [16]. In recent years, a number of developments and measures have been implemented in various countries to improve early trauma care, such as injury prevention and educational programs (Advanced/Pre-Hospital Trauma Life Support or A/PHTLS, Definitive Surgical Trauma Care [DSTC] and Definitive Anaesthetic Trauma Care [DATC], team resource management, etc), rapid transport and designated trauma centres with specialised personnel, logistics and infrastructure to rapidly deliver appropriate diagnosis, care and rehabilitation [17,18,19]. Approaches, such as evacuation communication strategies (9-liner MEDEVAC request), derived from the military setting, are also currently being transferred into the civilian arena against the background of increasing threats through terror actions and attacks [20, 21].
Despite these efforts, differences in pre-hospital trauma care across European countries are still substantial and morbidity and mortality remain considerable. This heterogeneity reinforces the need for improved and comprehensive management of severe trauma victims from the site of injury to complete stabilisation and rehabilitation [22]. According to the German Trauma Registry database (TR-DGU®) [23], pre-hospital rescue times have consistently been around 72 min for the last two-and-half decades. There is substantial geographical variation, with longer times in rural areas [23]; however, extended pre-hospital rescue times have also been reported even for heavily populated European metropolitan areas [24]. When in-hospital time for diagnostic procedures is added—for example, the time to access either whole body or selected computed tomography (CT)—the injured patient rarely receives interventional/surgical care before 2–3 h after the initial impact and this at best. Some of this delay is related to the fragmentation of pre- and intra-hospital care, including time-consuming and anachronistic methods and errors in communication [8, 25, 26].
The available epidemiological data related to outcomes are a strong argument to conclude that there is still a major need to improve processes of care in patients with severe trauma.
Fragmentation of care
Definitions
The ideal model of healthcare is “patient-centred”, defined as “the experience (to the extent the informed, individual patient desires it) of transparency, individualisation, recognition, respect, dignity, and choice in all matters, without exception, related to one’s person, circumstances, and relationships in healthcare” [1]. However, patient-centred care is far from being the rule in complex healthcare systems, which are often more accurately characterised as fragmented [27].
Several levels of fragmentation in healthcare have been described [1]: (1) lack of coordination of different professionals when treating a patient during a single hospital admission/stay; (2) lack of coordination of health professionals when simultaneously taking care of a patient with several diseases; (3) lack of coordination over time for the same patient with several diseases; (4) lack of coordination with healthcare allocated to one patient group while another group required it in priority. Groups here are loosely defined and could include populations at the level of a region or country.
In the complex setting of trauma, all levels of fragmentation are relevant to patient management. As underlined by Einer Elhauge [1], not all non-integration of healthcare should be considered as deleterious fragmentation. Fragmentation starts being deleterious when by not being patient-centred it results in poorer than expected outcomes [1]. It is accepted that there is an optimum level of integration and that lower or higher levels of integration may be associated with worse outcomes [1].
Causes and consequences
Several causes of fragmentation have been identified [1], and are mainly the result of loss of information or poor communication among the medical specialties involved. Although fragmentation arising from multiple interacting medical specialties is universal, some national healthcare systems perform better than others, suggesting that fragmentation is also related to economic, legal and political issues that govern medical practices and influence the uptake of integrated care strategies [1]. This implication was also highlighted in the recent report of the Belgian Health Knowledge Centre [28], which reviewed the provision of trauma care services in the context of a larger reform of the hospital landscape.
The consequences of fragmentation of care have been identified [29] and globally include worse outcomes and rising costs. Stated otherwise, fragmentation is associated with inefficiency, ineffectiveness, inequality, commoditisation, commercialisation, de-professionalisation, depersonalisation, and despair/discord [29]. Addressing fragmentation of healthcare to improve the process of care and outcomes for patients with severe trauma and for healthcare systems is, therefore, a credible goal.
Fragmentation in severe trauma
Both pre- and early in-hospital trauma management prior to intensive care unit (ICU) admission is complex because of its nature, involving several specialties as well as multiple decision-makers with individual priorities and distinct communication patterns, who need to make a set or series of healthcare and management decisions. Frequently, there is insufficient communication and exchange of information among professionals treating the trauma victim in ambulance vehicles and emergency and intervention rooms, operating theatres (surgery, anaesthesia) and ICUs, as well as imaging, interventional radiology, blood bank and laboratory departments. This information deficiency carries a high potential to delay decision-making and treatment. In this complex, time-sensitive context, individual decision-makers may make less than appropriate decisions due to lack or loss of relevant data and information.
Severe trauma patient management in Europe
Pre-hospital trauma care is highly variable across the European Union with some systems paramedic-based and others physician-based including physicians from different specialities [30]. Pre-hospital rescue times and actions are also highly variable. The trauma rescue chain is usually activated via an emergency call to a local dispatch centre that activates (Helicopter) Emergency Medical Service [(H)EMS] according to specific triggers. After the arrival of (H)EMS at the scene, initial assessment and treatment follow standardised algorithms (Pre-Hospital Trauma Life Support [PHTLS]) and feedback to the dispatch centre is usually provided either by the physician or (H)EMS via phone or mobile radio. Based upon the information received from the scene, the dispatch centre then searches for an appropriate receiving hospital depending on available data regarding capacities and capabilities for immediate access to adequate care. Various problems arise:
-
Information may not be accurate and up-to-date at the moment of the search and non-real time information may be distributed.
-
Bidirectional oral communication in a loud and hectic environment carries a high risk of information loss and miscommunication.
-
Information may be communicated and shared by non-specialists because there is hardly any direct physician-to-physician contact.
-
Inappropriate dispatch may be a problem in larger communities with numerous hospitals potentially receiving patients, or if the initial assessment is flawed due to limited experience of the physician or (H)EMS at the scene.
-
There is hardly any en route contact with the receiving hospital, in particular under unstable and critical conditions. The receiving hospital thus usually receives only rudimentary, very basic information, sometimes only indirectly through third parties such as the dispatch centre, prior to patient arrival. It therefore, needs to respond quickly and flexibly upon admission of the patient to the trauma bay (or a different trauma care model). In some centres, this flexibility may be limited by local logistics and infrastructure.
While ambulance design and equipment have evolved rapidly during the last decades, the organisation of (H)EMS and transport systems still varies, resulting in frequent media reports of patients being transported to hospitals not optimally equipped (or prepared) to receive them, substantial waits in emergency departments and/or missed diagnoses. Relatively few hospitals can offer optimal, rapid care of patients with multiple injuries, severe TBI and/or massive bleeding. However, despite limited evidence, there is consensus that organising and integrating a “trauma system” is associated with a 15% reduction in trauma mortality with cases of “preventable deaths” reduced by half [12].
The consensus of the medical experts contributing to this White Paper is that the major sources of fragmentation that must be addressed are: (1) between the pre- and early in-hospital emergency care teams; (2) among the emergency teams and the dispatch centre that coordinates the rescue mission; and (3) between the different individual decision-makers from different specialities involved in the early in-hospital patient management, all acting in a highly dynamic and rapidly changing environment. Streamlining severe trauma care pathways by interfacing pre-hospital emergency care with the receiving in-hospital medical and surgical teams has high potential to improve processes of care, and therefore, outcomes.
Examples of successful streamlining: lessons to be learned
From military trauma care
A report published in 2016 by the National Academies of Sciences, Engineering, and Medicine (NASEM) [15] summarised the achievements of military and civilian trauma care in a model of a “learning health system” as developed by the Best Care at Lower Cost report of the Institute of Medicine in the United States [31]. The United States have adopted an overall aim for both civilian and military trauma, designated as “zero preventable deaths after injury” [15].
The complete pathway of a severely injured patient starts at the site of injury and finishes with rehabilitation and return to the community [15]. The initial time-critical periods when managing patients with severe trauma are most sensitive to unstructured transitions, resulting in lower quality of care. The NASEM report underlined the importance of an effective information management system (IMS) [15], which could solve the problems related to fast operational tempo, limited and unstructured data collection, both on-site and during transportation (designated here as pre-hospital). The bidirectional (pre-hospital to in-hospital-to pre-hospital) IMS was considered by NASEM as a key element to accelerate pre-hospital care. It was shown during the war in Afghanistan that more rapid pre-hospital care (from 90 to 44 min) performed by medical personnel was associated with a 66% decrease in mortality from blast and penetrating injuries [15].
From acute myocardial infarction management
Another example of successful defragmentation, this time in Europe, concerns the management of patients with acute myocardial infarction (AMI). Since the prognostic benefits of primary percutaneous coronary intervention (PCI) in treating acute coronary syndromes were demonstrated in the early 2000s, concerted efforts have been made to understand variations in the use of this therapy and implement measures to improve access to it. The vital importance of integration between pre- and in-hospital systems in the care of patients with AMI became a specific recommendation in the most recent European Society of Cardiology Myocardial Revascularisation Guidelines [32, 33], based on evidence showing how service organisation impacted on mortality and morbidity. The ideal model for implementation of the guidelines is based on the identification of a geographical area where a single EMS system operates in a network of hospitals providing 24/7 coverage for the provision of optimal reperfusion therapy. The adoption of a multi-disciplinary, integrated approach, increasing communication and exchange of information between general practitioners, EMS, and healthcare professionals in primary PCI networks led to improved access to treatment and contributed to a decrease in total AMI mortality in several European countries. Initiated by the European Critical Care Foundation, collaboration between primary-PCI centres in Italy (Trieste) and Slovenia is currently under discussion to enable patients to benefit from the optimal organisation of primary PCI networks including cross-border settings [34,35,36,37,38].
From stroke management
Similar streamlining of care has also been reported for patients with stroke. For example, use of a specialised ambulance (stroke emergency mobile unit) was associated with a significantly increased number of patients who underwent thrombolysis within one hour resulting in better short-term outcomes [39]. Other authors reported that multidisciplinary streamlining (continuous feedback, standardised immediate emergency department attendance, interventional team activation for all potential interventions, pre-notification by the EMS, minimising additional diagnostic testing and direct transport to the CT scanner and then to the angiography suite) resulted in a significantly shorter duration to recanalisation [40]. Many other reports strongly suggest that multidisciplinary streamlining of care in stroke patients results in faster reperfusion and better outcomes [41, 42].
Goals of the European Critical Care Foundation project
From the lessons learned in several medical contexts, such as AMI and stroke, and from the recent achievements in military trauma [15], development of defragmentation tools must be adapted to each clinical context; in this case, severe civilian trauma across diverse European countries.
There are numerous opportunities to optimise the flow of patients with severe trauma from the site of the accident to early acute in-hospital trauma care. The challenges at a European level are obvious, but also provide an incentive to overcome them. The major elements of the proposed strategy are outlined in Fig. 1, and can be achieved through the development of a severe trauma management platform that streamlines pre- and in-hospital care pathways.

Decision making process in severe trauma: a patient-centred approach. A process for creative/efficient interactions among the complementary components. ED emergency department, ICU intensive care unit, EM emergency medicine
The design of the platform and related tools must be conceived at the outset, so that they can be adapted to populations with specific needs, such as paediatric patients, pregnant patients and the very elderly. It is clear from the NASEM report that populations with special needs are more at risk of fragmentation of care in case of severe trauma, because of a lack of knowledge of their specificities [15]. It is likely that computer-enhanced clinical evaluation and integrated monitoring systems would be of great value for medical and paramedical personnel who are not always specialised in managing those particular patient populations.
The platform would include the following elements:
-
i.
An IMS adapted to severe trauma with integrated continuous monitoring of vital parameters to test the functional reserve of the patient. Experts and end-users will define the items of information that should be included in the IMS. The group will include representatives from the emergency services and accident experts to allow on-line accident analysis that may help predict lesions. The final proposal for the content of the IMS will be submitted to scientific societies for review and approval.
The system will be designed as a prototype that could also be adapted to other time-sensitive diseases. It will be developed to:
-
1.
Allow use at the regional/national/European level within a model of a ‘learning IMS’.
-
2.
Promote leadership, make continuous learning and improvement a priority and provide the resources and environment necessary to achieve the systems aims.
-
3.
Permit up-scaling for disaster medicine.
-
1.
-
ii.
Artificial intelligence capabilities that enable computer-enhanced clinical evaluation and decision support in pre and in-hospital settings. The computer-enhanced evaluation system will take into account time-dependent changes in clinical conditions and enable a decrease in the inter-rater and intra-rater variability as already reported for neurological variability [43]. In the time-sensitive context of care for patients with severe trauma, clinical decisions are dependent on the expertise of the team leader and prone to errors. A clinical decision support system designed specifically for severe trauma has a high probability of improving the quality of the clinical decision and thus improving outcomes, as already demonstrated by several scientific reports [44, 45].
An educational tool that includes the defragmentation of care in both initial and continuous medical training for severe trauma will be needed. This forum already exists via the European Trauma Course Organisation (a joint initiative of four different scientific organisations) and will require adaptation to different European countries with emphasis on streamlining.
Overview of the severe trauma management platform
The development of the following elements within the severe trauma management platform would largely address the problems identified in the management of patients from the initial site of injury to stabilisation in the hospital.
-
i.
The IMS, adapted to severe trauma and designed for sharing a defined set of structured information, is the conceptual basis of the platform (Fig. 2). It should include information about: (1) the mechanism of accident and injury with reference to the (estimated) magnitude of physical impact; (2) the patient pattern of injury and dynamic physiology; and (3) hospital capabilities and capacities to support EMS treatment and transport decisions. Given the complexity of modern hospitals, such a bidirectional IMS should have simultaneous in-hospital display facilities across departments (anaesthesia, operating theatre, ICU, imaging and interventional radiology, laboratories, transfusion, etc.). This would allow the multiple potential decision-makers on site medical/paramedical EMS teams, transportation teams, dispatch teams, in-hospital teams to share the same structured information. The user-interface must be designed to provide graphical and numerical information for fast evaluation of the severity category of the patient including dynamic changes, and decision support for therapeutic interventions and management. In Europe, such an IMS should also be able to provide continuity in cross-border contexts where neighbouring countries speak different languages, for example, through access to real-time machine translation [46]. An example here are cross-border EMS teams involving air rescue systems (“Europe” air rescue helicopters).
Fig. 2 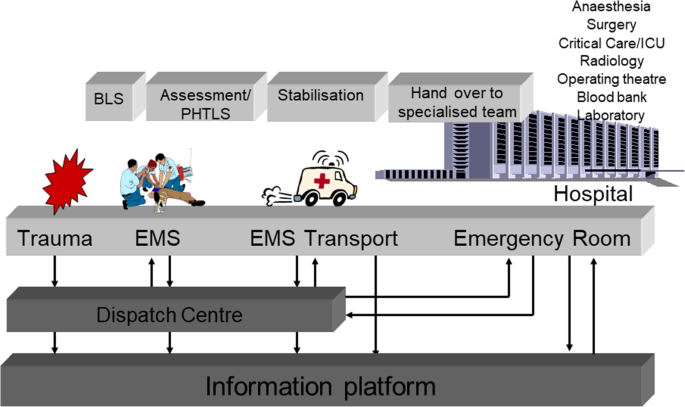
Process of defragmentation of prehospital care for outcome improvement in time-sensitive trauma pathologies. EMS emergency medical services, BLS basic life-support, PHTLS prehospital trauma life support
-
ii.
Modern technologies such as spoken dialogue systems allow real-time interaction between machines and humans [46]. Such voice-to-computer technologies could be used to structure and improve the initial pre-hospital evaluation and care, including through enabling database searches and automated reporting of procedures. This could help improve the quality of care arising from variations in the expertise of the work force managing severe trauma patients. The authors estimate that the best model would be one that uses human and computer expertise in parallel [47]. Further improvements could be envisaged to improve the intelligibility of ambulance-to-wayside communication depending on the particular problems identified in each local context.
-
iii.
Continuous monitoring of vital parameters to test the functional reserve of the patient should be integrated into the IMS. Such integrated monitoring systems already exist. However, the challenge is to interface existing monitoring techniques from different manufacturers into a single application.
-
iv.
Capturing data in clinical settings remains a cumbersome task for which caregivers seldom find the time, especially in emergency situations. The inevitable result is missing entries and/or low-quality data. However, much valuable qualitative information is present in the form of textual documents, such as medical reports and notes. Converting these so-called unstructured sources into structured data could provide additional input to the decision support system.
-
v.
A clinical evaluation and decision-support system must be designed with appropriate artificial intelligence support, to relay the best available up-to-date information to the physician or primary-care provider. It would use all data gathered in the IMS, intelligently filtered or presented at appropriate times, to enhance trauma care processes. The decision support would broadly be developed through applications for:
-
a)
Alert & Reminder to help in continuous monitoring of vital parameters, alerting the physician when certain data in trauma care processes is missing, or exceeds particular thresholds or indicates a particular risk for the patient.
-
b)
Therapy critiquing & planning to identify possible treatment plans as well as looking for inconsistencies, errors, omissions, or potential contraindications. The system would evaluate the proposed treatment against the patient data and known standards of care. Furthermore, the platform would use a knowledge base of treatment protocols and guidelines to actually assist in the creation of a treatment pathway.
-
a)
-
vi.
In many cases, imaging is needed to diagnose the full extent of traumatic injuries, with CT imaging being the modality of choice for severe trauma cases. Often, because of limited prior information, this involves whole-body imaging, making the human analysis of the image data time-consuming and prone to error. Automated medical image analysis, whereby algorithms automatically detect anomalies from CT imaging and alert the physician to the presence of potential injuries, could improve the efficiency and sensitivity of the radiological workflow.
-
vii.
Big data storage and retrieval technologies suited to analysing variable clinical data and of very high speed will be needed to support the real-time analytics performed by the trauma care management platform.
-
viii.
Shared treatment pathways could be synchronised between pre- and in-hospital care and could also already be initiated at the scene or en route and then continued without any delay in the receiving hospital.

Project Interact: tool development, deployment and evaluation
To promote the streamlining of care in patients with severe trauma and fulfil the above-mentioned tasks, the European Critical Care Foundation will bring together a consortium of:
-
1.
European Scientific Societies and other experts.
-
2.
Academic partners with expertise to develop the tools and pilot hospitals, cities and regions interested in collaborating in initial validation studies.
-
3.
Representatives of the biomedical and information technology (IT) industries to collaborate through public/private funding opportunities at EU, national, regional, and city levels.
After definition of the strategy, the consortium will formulate technical aspects of the project, define process-of-care targets to evaluate the efficacy of the defragmentation tools, carry out an in-depth analysis of legal and ethical issues relating to the project, including possible issues related to new data protection and privacy laws, and a health economic analysis. Results arising from the project will be disseminated through numerous scientific and policy networks. In a future step, the project will initiate multicentre trials across Europe.
Conclusions and future directions
There is ample evidence for the need to improve processes of care for severe trauma casualties at the European level and further afield. The particular challenges of managing patients with severe trauma −time constraints, information and communication needs− lend themselves ideally to the application of innovative information management, artificial intelligence and telemedicine solutions. Applied to other critical illnesses, situations and geographies, the strategy outlined in this White Paper could ultimately redefine the organisation of pre- and in-hospital acute care pathways, bringing benefits to patients and their families and to healthcare systems.
References
Elhauge E. The fragmentation of US health care. Causes and solutions. Oxford: Oxford University Press; 2010.
Rhee P, Joseph B, Pandit V, Aziz H, Vercruysse G, Kulvatunyou N, et al. Increasing trauma deaths in the United States. Ann Surg. 2014;260:13–21.
Haagsma JA, Graetz N, Bolliger I, Naghavi M, Higashi H, Mullany EC, et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Inj Prev. 2016;22:3–18.
Mokdad AH, Forouzanfar MH, Daoud F, Mokdad AA, El BC, Moradi-Lakeh M, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2016;387:2383–401.
Gunst M, Ghaemmaghami V, Gruszecki A, Urban J, Frankel H, Shafi S. Changing epidemiology of trauma deaths leads to a bimodal distribution. Proc Bayl Univ Med Cent. 2010;23:349–54.
Evans JA, van Wessem KJ, McDougall D, Lee KA, Lyons T, Balogh ZJ. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34:158–63.
Davis JS, Satahoo SS, Butler FK, Dermer H, Naranjo D, Julien K, et al. An analysis of prehospital deaths: who can we save? J Trauma Acute Care Surg. 2014;77:213–8.
Ha M, Kim BC, Choi S, Cho WH, Choi HJ. Preventable and potentially preventable traumatic death rates in neurosurgery department: a single center experience. Korean J Neurotrauma. 2016;12:67–71.
Ray JJ, Meizoso JP, Satahoo SS, Davis JS, Van Haren RM, Dermer H, et al. Potentially preventable prehospital deaths from motor vehicle collisions. Traffic Inj Prev. 2016;17:676–80.
Teixeira PG, Inaba K, Hadjizacharia P, Brown C, Salim A, Rhee P, et al. Preventable or potentially preventable mortality at a mature trauma center. J Trauma. 2007;63:1338–46.
Brazinova A, Majdan M, Leitgeb J, Trimmel H, Mauritz W. Factors that may improve outcomes of early traumatic brain injury care: prospective multicenter study in Austria. Scand J Trauma Resusc Emerg Med. 2015;23:53.
Celso B, Tepas J, Langland-Orban B, Pracht E, Papa L, Lottenberg L, et al. A systematic review and meta-analysis comparing outcome of severely injured patients treated in trauma centers following the establishment of trauma systems. J Trauma. 2006;60:371–8.
Holst JA, Perman SM, Capp R, Haukoos JS, Ginde AA. Undertriage of trauma-related deaths in US emergency departments. West J Emerg Med. 2016;17:315–23.
Cowley RA. The resuscitation and stabilization of major trauma patients in a trauma center environment. Clin Med. 1976;83:16–22.
National Academies of Sciences Engineering and Medicine. A National Trauma Care System. Integrating military and civilian trauma systems to achieve zero preventable deaths after injury. Washington: National Academies Press; 2016.
West JG, Trunkey DD, Lim RC. Systems of trauma care. A study of two counties. Arch Surg. 1979;114:455–60.
Mohammad A, Branicki F, Abu-Zidan FM. Educational and clinical impact of advanced trauma life support (ATLS) courses: a systematic review. World J Surg. 2014;38:322–9.
Jayaraman S, Sethi D, Chinnock P, Wong R. Advanced trauma life support training for hospital staff. Cochrane Database Syst Rev 2014;CD004173.
Johansson J, Blomberg H, Svennblad B, Wernroth L, Melhus H, Byberg L, et al. Prehospital trauma life support (PHTLS) training of ambulance caregivers and impact on survival of trauma victims. Resuscitation. 2012;83:1259–64.
Woolley T, Round JA, Ingram M. Global lessons: developing military trauma care and lessons for civilian practice. Br J Anaesth. 2017;119:i135–42.
Sonesson L, Boffard K, Lundberg L, Rydmark M, Karlgren K. The potential of blended learning in education and training for advanced civilian and military trauma care. Injury. 2018;49:93–6.
Alarhayem AQ, Myers JG, Dent D, Liao L, Muir M, Mueller D, et al. Time is the enemy: mortality in trauma patients with hemorrhage from torso injury occurs long before the “golden hour”. Am J Surg. 2016;212:1101–5.
TraumaRegister DGU®. Annual Report 2016. Available at: http://www.dgu-online.de/fileadmin/published_content/5.Qualitaet_und_Sicherheit/PDF/2016_Annual_Report_TraumaRegister_DGU_2015.pdf Accessed 30 August, 2018.
Desmettre T, Yeguiayan JM, Coadou H, Jacquot C, Raux M, Vivien B, et al. Impact of emergency medical helicopter transport directly to a university hospital trauma center on mortality of severe blunt trauma patients until discharge. Crit Care. 2012;16:R170.
Hartl R, Gerber LM, Iacono L, Ni Q, Lyons K, Ghajar J. Direct transport within an organized state trauma system reduces mortality in patients with severe traumatic brain injury. J Trauma. 2006;60:1250–6.
Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J, Fernandez-Mondejar E, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fourth edition. Crit Care. 2016;20:100.
Institute of Medicine (US) Committee on Quality Health Care in America. Crossing the quality chasm: a new health system for the 21st century. Washington: National Academy Press; 2001.
Farfan-Portet MD, Dubois C, Mistiaen P, Cordon A, Stordeur S, Van Den Heede K. Towards an inclusive system for major trauma. Brussels: Belgian Health Care Knowledge Centre (KCE); 2017.
Stange KC. The problem of fragmentation and the need for integrative solutions. Ann Fam Med. 2009;7:100–3.
Timm A, Maegele M, Lefering R, Wendt K, Wyen H. Pre-hospital rescue times and actions in severe trauma. A comparison between two trauma systems: Germany and the Netherlands. Injury. 2014;45(Suppl 3):43–52.
Institute of Medicine. Best care and lower cost: the path to continuously learning health care in America. Washington: National Academies Press; 2013.
Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, Falk V, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35:2541–619.
Steg PG, James SK, Atar D, Badano LP, Blomstrom-Lundqvist C, Borger MA, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569–619.
Smith FG, Brogan RA, Alabas O, Laut KG, Quinn T, Bugiardini R, et al. Comparative care and outcomes for acute coronary syndromes in Central and Eastern European Transitional countries: a review of the literature. Eur Heart J Acute Cardiovasc Care. 2015;4:537–54.
Kristensen SD, Laut KG, Fajadet J, Kaifoszova Z, Kala P, Di MC, et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014;35:1957–70.
Laut KG, Gale CP, Lash TL, Kristensen SD. Determinants and patterns of utilization of primary percutaneous coronary intervention across 12 European countries: 2003–2008. Int J Cardiol. 2013;168:2745–53.
Laut KG, Gale CP, Pedersen AB, Fox KA, Lash TL, Kristensen SD. Persistent geographical disparities in the use of primary percutaneous coronary intervention in 120 European regions: exploring the variation. EuroIntervention. 2013;9:469–76.
Kristensen SD, Fajadet J, Di MC, Kaifoszova Z, Laut KG, Deleanu D, et al. Implementation of primary angioplasty in Europe: stent for life initiative progress report. EuroIntervention. 2012;8:35–42.
Ebinger M, Kunz A, Wendt M, Rozanski M, Winter B, Waldschmidt C, et al. Effects of golden hour thrombolysis: a prehospital acute neurological treatment and optimization of medical care in stroke (PHANTOM-S) substudy. JAMA Neurol. 2015;72:25–30.
Aghaebrahim A, Streib C, Rangaraju S, Kenmuir CL, Giurgiutiu DV, Horev A, et al. Streamlining door to recanalization processes in endovascular stroke therapy. J Neurointerv Surg. 2017;9:340–5.
Candelaresi P, Lattuada P, Uggetti C, Dacco R, Fontana G, Frediani F. A high-urgency stroke code reduces in-hospital delays in acute ischemic stroke: a single-centre experience. Neurol Sci. 2017;38:1671–6.
Wang H, Thevathasan A, Dowling R, Bush S, Mitchell P, Yan B. Streamlining workflow for endovascular mechanical thrombectomy: lessons learned from a comprehensive stroke center. J Stroke Cerebrovasc Dis. 2017;26:1655–62.
Cohen YC, Hassin-Baer S, Olmer L, Barishev R, Goldhammer Y, Freedman L, et al. MS-CANE: a computer-aided instrument for neurological evaluation of patients with multiple sclerosis: enhanced reliability of expanded disability status scale (EDSS) assessment. Mult Scler. 2000;6:355–61.
Ranta A, Yang CF, Funnell M, Cariga P, Murphy-Rahal C, Cogger N. Utility of a primary care based transient ischaemic attack electronic decision support tool: a prospective sequential comparison. BMC Fam Pract. 2014;15:86.
Silveira PC, Dunne R, Sainani NI, Lacson R, Silverman SG, Tempany CM, et al. Impact of an information technology-enabled initiative on the quality of prostate multiparametric MRI reports. Acad Radiol. 2015;22:827–33.
Hirschberg J, Manning CD. Advances in natural language processing. Science. 2015;349:261–6.
Semigran HL, Levine DM, Nundy S, Mehrotra A. Comparison of physician and computer diagnostic accuracy. JAMA Intern Med. 2016;176:1860–1.
Author information
Authors and Affiliations
Contributions
The text was written following discussions among members of the European Critical Care Foundation. DL, JLV and MM wrote the first draft. All other authors revised it for critical content. All authors read and approved the final draft.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts to declare related to this manuscript.
Rights and permissions
About this article

Cite this article
Longrois, D., Maegele, M., Bersini, H. et al. Streamlining pre- and intra-hospital care for patients with severe trauma: a white paper from the European Critical Care Foundation. Eur J Trauma Emerg Surg 45, 39–48 (2019). https://doi.org/10.1007/s00068-018-1053-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-018-1053-1