
Abstract
Purpose
To explore the effect of admission physical examination findings, anamnesis, and computed tomography on dural penetration and prognosis in patients with cranial gunshot wound (CGW).
Methods
In this study, the medical data of 56 subjects who were admitted to the Emergency Department of Dicle University Hospital with CGWs between January 2011 and December 2013 were retrospectively reviewed. The effects of type of incident (suicidal vs non-suicidal), pupil diameter and light reflex, hemodynamic status, type (bullet or pellet), velocity, trajectory of foreign material, trauma scores, and imaging findings on dural penetration and mortality were explored.
Results
The mean age of the study population was 24.8 ± 13.50 years. Thirty (53.6 %) patients had penetrating injuries and 26 (46.4 %) had non-penetrating injuries; 9 (16.1 %) patients died and 47 (83.9 %) survived. Suicidal injury, pupil diameter and light reflex, bullet as foreign material, and high velocity and lateral trajectory of foreign material significantly affected dural penetration and mortality (p < 0.05). In addition, dural penetration, bilobar, multilobar, or bihemispheric involvement of brain parenchyma, presence of intracranial hemorrhage, subarachnoid hemorrhage, ventricular hemorrhage, fracture, shift, edema, and trauma scores significantly affected mortality (p < 0.05).
Conclusions
In CGWs, dural penetration and prognosis can be predicted by physical examination findings and patient characteristics on initial admission.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Once prevalent in regions of military conflict, cranial gunshot wounds (CGWs) are now increasingly common even in the absence of military clashes, especially affecting civilians living in developing countries [1, 2]. Penetrating brain injuries differ from blunt brain injuries primarily by the presence of dural perforation [3]. Despite technological advances, mortality and morbidity of CGWs remain substantially high [4, 5].
Our literature scan identified many studies on mortality, complications, and treatment approaches, as well as findings of admission physical examination, computed tomography (CT), and patient history in CGWs. However, there were no studies investigating in detail the impact on initial admission findings on dural penetration and prognosis in the emergency department [6–8].
The aim of the present study was to explore the impact of admission physical examination, anamnesis, and computed tomography on dural penetration and prognosis in patients with CGWs.
Patients and methods
This study retrospectively analyzed medical data of 56 successively enrolled patients with CGWs between January 2011 and December 2013. Patients were consecutively taken into the study. They were brought to the emergency department by paramedics via ambulance. All patients were examined in the emergency department; they were resuscitated in accordance with the ATLS (Advanced Trauma Life Support) program, and diagnostic and therapeutic procedures were performed in line with the available protocols. All patients underwent cranial tomography; they also received tetanus prophylaxis and antibiotic treatment, but no seizure prophylaxis. The neurosurgery department operated on patients with a large hematoma, although patients with a Glasgow Coma Score (GCS) of 3 and fixed pupils were not operated on, as were those without a large hematoma. Detailed trauma information was obtained from patients, patient relatives, or paramedics. Patients with missing medical information, patients injured by bomb, mine, or dynamite explosions, and patients who had died by the time of admission were excluded from the study. Bullet and pellet were selected among CGWs.
Type of injury incident (suicidal vs non-suicidal), pupil diameter and light reflex, hemodynamic status, type (bullet or pellet), velocity, and trajectory of foreign material, dural penetration, additional organ injury, and complications were analyzed. Trauma scores analyzed in the study were GCS, Revised Trauma Score (RTS), Injury Severity Score (ISS), Trauma Score-Injury Severity Score (TRISS). Bilobar, multilobar, and bihemispheric involvement of brain parenchyma, intracranial hemorrhage, epidural hematoma (EDH), subdural hematoma (SDH), subarachnoid hemorrhage (SAH), ventricular hemorrhage, pneumocephalus, fracture, shift, and edema constituted the CT findings examined. Factors affecting dural penetration and death were explored.
Statistical analyses were performed with SPSS 18.0 for Windows statistical package program. Numerical data were expressed as mean ± standard deviation (SD), and categorical data were presented as number and percentage (%). Normality of data distribution was tested, and normally distributed data were compared using independent t test between two independent groups, while the non-normally distributed data were compared with Mann–Whitney U test between two independent groups. Qualitative variables were compared using Chi Square test (χ 2). The hypotheses were tested two sided, with a p value of <0.05 being considered as statistically significant.
Results
A total of 145,282 patients were admitted to the emergency department of Dicle University Hospital during the study period between January 2011 and December 2013. Of these, 22,701 were trauma victims, of whom 837 suffered gunshot wounds. The total number of CGW cases was 56. The mean age of the study population was 24.8 ± 13.50 years (range 4–66 years) and 43 (76.8 %) patients were male, while 13 (23.2 %) patients were female. The average GCS was 11.96 ± 4.62. The clinical and demographic properties of the study population are presented in Table 1.
Thirty (53.6 %) patients had penetrating injuries and 26 (46.4 %) had non-penetrating injuries. Suicidal injury, pupil diameter and light reflex, bullet as the foreign material, and high velocity and lateral trajectory of foreign material significantly affected dural penetration (p < 0.05). GCS, RTS, ISS, and TRISS also significantly affected dural penetration (p < 0.05). The factors affecting dural penetration ae shown in Table 2.
Nine (16.1 %) patients died and 47 (83.9 %) survived in our study. Factors affecting mortality are shown in Table 1. Suicidal injury, anisocoric pupils, and unstable hemodynamics significantly affected mortality (p < 0.05). Bullet as the foreign material, high velocity, lateral trajectory of foreign material, and dural penetration also significantly affected mortality (p < 0.05). Similarly, bilobar, multilobar, or bihemispheric involvement had a significant effect on mortality (p < 0.05), as did intracranial hemorrhage, SAH, ventricular hemorrhage, fracture, shift, and edema (p < 0.05). A GCS equal to or lower than 8, as well as RTS, ISS, and TRISS scores significantly affected mortality (p < 0.05).
Discussion
Despite having a lower incidence among head traumas, CGWs continue to have a special place due to their worse prognosis and high mortality regardless of technological advances.
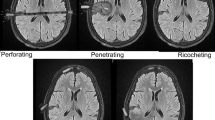
CGWs can be categorized into three types: perforating, penetrating, and superficial injuries [9]. In penetrating brain injuries, perforation of the dura mater is the main pathophysiological mechanism [3]. Compared to non-penetrating injuries, penetrating injuries are known to be associated with a worse prognosis and higher mortality [9]. Our study explored factors affecting mortality (Table 2) and found that dural penetration significantly affected mortality.
The mortality rate of CGWs range between 12 and 93 % [4, 5, 10]. Our study showed a mortality rate that was consistent with and at the lower boundary of the previously reported range. This may be due to nearly half of our study population being composed of non-penetrating cases.
Previous studies have reported a suicidal CGW rate of 13–88 % [11, 12]. Suicidal CGWs are known to be associated with a poor prognosis and high mortality [13–15]. A study linked poor prognosis of suicide to victim’s immobility during the shot and the shot’s close range [16]. Our results are in accordance with previous studies. To our opinion, additional reasons for poor prognosis of the suicidal cases in our study were a lateral bullet trajectory and bihemispheric involvement.
Former studies have reported that pupil diameter and light reflex are important prognostic factors. Especially dilated, non-active pupils and anisocoric pupils indicated a poor prognosis [17, 18]. In our study, the findings related to pupil diameter and light reflex were in accordance with previous reports; in addition, dilated and anisocoric pupils were related to dural penetration.
Hypotension is known to be a factor affecting mortality and prognosis in CGWs [19]. The hemodynamic instability rate ranges between 67 and 72 % in deceased patients [19]. Aldrich et al. [20], on the other hand, reported that hemodynamic instability had a high rate among deceased patients, although its correlation with mortality was not statistically significant. In our study, the correlation between hemodynamic instability and mortality was high and statistically significant.
CGWs are said to be of “low velocity” when the bullet velocity was lower than 1200 ft/s and of “high velocity” when it exceeded 1200 ft/s; high-velocity weapons cause more severe damage [21, 22]. Injury severity depends on a bullet’s kinetic energy, which is directly proportional to a bullet’s mass and square of its velocity. This can be formulated as:
where E is the kinetic energy, m the bullet’s mass, and v the bullet’s velocity [21, 22]. This formula can explain the significant impact of high bullet velocity on dural penetration and mortality in our study. In our opinion, a bullet’s higher velocity and greater mass compared to those of a pellet are the reasons for the higher rates of dural penetration and mortality associated with bullets.
Previous studies have shown the relationship of multilobar injuries with increased mortality and worse prognosis compared to unilobar injuries [23–26]. Bihemispheric lesions have also been demonstrated to correlate to increased mortality [13, 17, 18, 26]. Studies examining bullet trajectory have shown that a lateral trajectory is associated with a higher mortality and worse prognosis than an anterolateral trajectory [14, 27]. Our study results were in accordance with literature data. Since ventricular involvement and bihemispheric injury were inevitable in penetrating CGWs with a lateral trajectory, the latter was associated with increased mortality and worse prognosis.
İntraventricular hemorrhage, SAH, shift, and edema on CT are predictive of poor prognosis and increased mortality in penetrating CGWs [17, 18, 20, 26]. The same CT findings were also correlated to poor prognosis and high mortality in our study.
Arabi [10] reported that among 435 subjects with CGW, 27 died and 19 survived among those with an admission GCS of 3–5; 26 died and 32 survived among those with an admission GCS score of 6–8; 10 died and 47 survived among those with an admission GCS score of 9–12; and 8 died and 266 survived among those with an admission GCS score of 13–15. In a study by Mansuco et al. [11] in 40 subjects with CGW, 16 died and 3 survived among subjects with a GCS ≤8, whereas all subjects with a GCS score greater than 8 survived. Studies in CGW have shown that admission GCS is the cornerstone for the determination of prognosis and mortality in CGWs, and mortality increases as GCS decreases [10, 14, 17, 20, 26]. Our results were in accordance with the literature data. The mortality rate was prominently higher when GCS was ≤8 and prominently lower when it was >8.
Bozdemir et al. [28], in a study investigating trauma scores in gunshot wounds, reported that ISS, RTS, and TRISS scores had a significant effect on mortality. Joseph et al. [29] also reported that ISS score significantly predicted mortality. Our study also demonstrated that ISS, RTS, and TRISS scores significantly affected dural penetration and mortality. To our knowledge, this may be due to a more severe body trauma occurring with penetrating injuries owing to the latter being high-energy traumas.
Conclusions
Among patients admitted to emergency department with CFAI, suicidal CFAI, dilated or anisocoric pupils, hemodynamic instability, bullet as the foreign material, and foreign material’s high velocity and lateral trajectory on initial admission were the factors affecting dural penetration and mortality. They may be easily used as prognostic markers independent of CT findings. As for CT findings, bilobar, multilobar, or bihemispheric involvement, SAH, ventricular hemorrhage, fracture, shift, and edema are correlated with increased mortality. In conclusion, findings of physical examination and patient characteristics on initial admission can predict dural penetration and prognosis, and the diagnosis and prognosis can be determined by CT findings.
References
Stone JL, Lichtor T, Fitzgerald LF. Gunshot wounds to the head in civilian practice. Neurosurgery. 1995;37:1104–12.
Ambrosi PB, Valença MM, Filho HA. Prognostic factors in civilian gunshot wounds to the head: a series of 110 surgical patients and brief literature review. Neurosurg Rev. 2012;35:429–36.
Santıago LA, Oh BC, Dash PK, Holcomb JB, Wade CE. A clinical comparison of penetrating and blunt traumatic brain injuries. Brain Inj. 2012;26(2):107–25.
Carey ME, Young HF, Rish BL, Mathis JL. Follow-up study of 103 American soldiers who sustained a brain wound in Vietnam. J Neurosurg. 1974;41:542–9.
Siccardi D, Cavaliere R, Pau A, Lubinu F, Turtas S, Viale GL. Penetrating craniocerebral missile injuries in civilians a retrospective analysis of 314 cases. Surg Neurol. 1991;35:455–60.
Tsuei YS, Sun MH, Lee HD, Chiang MZ, Leu CH, Cheng WY, Shen CC. Civilian gunshot wounds to the brain. J Chin Med Assoc. 2005;68:126–30.
Liebenberg WA, Demetriades AK, Hankins M, Hardwidge C, Hartzenberg BH. Penetratıng civilian craniocerebral gunshot wounds: a protocol of delayed surgery. Neurosurgery. 2005;57:293–9.
Martins RS, Siqueira MG, Santos MTS, Collange NZ, Moraes OJS. Prognostic factors and treatment of penetrating gunshot wounds to the head. Surg Neurol. 2003;60:98–104.
Pruitt BA, editor. Epidemiology: mode of injury, Guidelines for the management of patients with penetrating brain injury. J Trauma-Inj Infect Crit Care. 2001;51:S1–S57.
Aarabi B. Surgical outcome in 435 patients who sustained missile head wounds during the Iran–Iraq war. Neurosurgery. 1990;27:692–5.
Mancuso P, Chiaramonte I, Passanisi M, Guarnera F, Augello G, Tropea R. Craniocerebral gunshot wounds in civilians: report on 40 cases. J Neurosurg Sci. 1988;32:189–94.
Suddaby L, Weir B, Forsyth C. The management of.22 caliber gunshot wounds of the brain: a review of 49 cases. Can J Neurol Sci. 1987;14:268–72.
Jacobs DG, Brandt CP, Piotrowski JJ, McHenry CR. Transcranial gunshot wounds: cost and consequences. Am Surg. 1995;61:647–53.
Grahm TW, Williams FC Jr, Harrington T, Spetzler RF. Civilian gunshot wounds to the head: a prospective study. Neurosurgery. 1990;27:696–700.
Nagib MG, Rockswold GL, Sherman RS, Lagaard MW. Civilian gunshot wounds to the brain: prognosis and management. Neurosurgery. 1986;18:533–7.
Hofbauer M, Kdolsky R, Figl M, Grünauer J, Aldrian S, Ostermann RC, Vècsei V. Predictive factors ınfluencing the outcome after gunshot ınjuries to the head—A Retrospective Cohort Study. J Trauma. 2010;69:770–5.
Kaufman HH, Levy ML, Stone JL, Germanson T, Shaffrey CI, Jane JA. Patients with Glasgow Coma Scale scores 3, 4, 5 after gunshot wounds to the brain. Neurosurg Clin N Am. 1995;6:701–14.
Shaffrey ME, Polin RS, Phillips CD, Germanson T, Shaffrey CI, Jane JA. Classification of civilian craniocerebral gunshot wounds: a multivariate analysis predictive of mortality. J Neurotrauma. 1992;9:279–85.
Pruitt BA, editor. Systemic measures: hypotension, Guidelines for the management of patients with penetrating brain injury. J Trauma-Inj Infect Crit Care. 2001;51:S60–S61.
Aldrich EF, Eisenberg HM, Saydjari C, et al. Predictors of mortality in severely head-injured patients with civilian gunshot wounds: a report from the NIH Traumatic Coma Data Bank. Surg Neurol. 1992;38:418–23.
Kirkpatrick JB, Di Maio V. Civilian gunshot wounds of the brain. J Neurosurg. 1978;49:185–98.
Kaufman HH, Loyola WP, Makela ME, Frankowski RF, Wagner KA, Bernstein DP. Civilian gunshot wounds: the limits of salvageability. Acta Neurochir (Wein). 1983;67:115–25.
Kennedy F, Gonzalez P, Dang C, Fleming A, Sterling-Scott R. The Glasgow Coma Scale and prognosis in gunshot wounds to the brain. J Trauma. 1993;35:75–7.
Levi L, Borovich B, Guilburd JN, et al. Wartime neurosurgical experience in Lebanon, 1982–1985, I: penetrating craniocerebral injuries. Br J Med Sci. 1990;26:548–54.
Shoung HM, Sichez JP, Pertuiset B. The early prognosis of craniocerebral gunshot wounds in civilian practice as an aid to the choice of treatment: a series of 56 cases studied by the computerized tomography. Acta Neurochir (Wien). 1985;74:27–30.
Bhat AR, Wani MA, Kirmani AR, Raina TH, Javed S, Altaf R, Alam S, Arif S. Disaster management of civilian gunshot head wounds in north Indian state. Indian J Neurotrauma. 2009;6:27–42.
Izci Y, Kayali H, Daneyemez M, Koksel T. Comparison of clinical outcomes between anteroposterior and lateral penetrating craniocerebral gunshot wounds. Emerg Med J. 2005;22:409–10.
Bozdemir MN, Cander B, Dur A, Kocak S, Dundar DZ, Uyar M, Girisgin S, Gul M. The prognostic value of trauma scoring systems for gunshot injuries. Pak J Med Sci. 2011;27:1121–5.
Joseph B, Aziz H, Pandit V, Kulvatunyou N, O’Keeffe T, Wynne J, et al. Improving survival rates after civilian gunshot wounds to the brain. J Am Coll Surg. 2014;218:58–65.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
There is no ethical approval because it was a retrospective study.
Conflict of interest
Mustafa İçer, Yılmaz Zengin, Recep Dursun, Hasan Mansur Durgun, Cemil Göya, İsmail Yıldız and Cahfer Güloğlu declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
İçer, M., Zengin, Y., Dursun, R. et al. Factors affecting dural penetration and prognosis in patients admitted to emergency department with cranial gunshot wound. Eur J Trauma Emerg Surg 43, 611–615 (2017). https://doi.org/10.1007/s00068-015-0564-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-015-0564-2