
Abstract
Objectives
Handlebar injuries are one of the most common causes of abdominal injuries in children. We aim to investigate the epidemiology of bicycle handlebar injuries and to emphasize the severity of the injuries.
Methods
A retrospective analysis of children admitted to our hospital with abdominal injury related to bicycle handlebars was performed.
Results
A total of 219 children (187 males and 32 females) younger than 17 years were hospitalized for abdominal handlebar injuries between 2005 and 2013. The age range of the patients was 4–17 (mean 10.93 ± 3.68) years. Most patients had an imprint of the handlebar edge on their abdomen. The most common abdominal organ injury was liver laceration. 33 patients had pancreas injury and 13 patients had hollow organ injury. Most patients were treated conservatively. Surgery was performed in 24 patients. Hospital stay was 4–60 (mean 9.63 ± 13.37) days.
Conclusions
Trend of bicycle handlebar trauma over this time period was related to the local floating population and economy. The most common abdominal organ injury was liver. Hollow organ injury required emergency exploratory laparotomy and the Roux-y anastomosis applied well in cases whose gastrointestinal tract damaged seriously. Pancreatic injury usually led to secondary pseudocyst. The percutaneous ultrasound-guided drainage of pancreatic pseudocyst was really an effective way. The trend in the amylase and lipase levels could reflect the pancreatic injury condition and predict prognosis. Early diagnosis and optimal care without delay may help to reduce the morbidity of injuries to the internal organs. Children with abdominal handlebar injuries should be treated with great care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bicycle riding is a popular pastime sports activity enjoyed by over three quarters of Chinese children of all ages. It becomes one of the most common causes of abdominal injuries in children. Injuries involving bicycle can be very serious among children [1–3]. With the widespread used of helmets, the incidence of serious head injuries has declined, while the serious abdominal injuries caused by handlebar should be deserved more concern [4]. Lam found that about 10 % of bicycle-related injuries were handlebar injuries [5]. Most of the bicycle injuries are skin abrasions and once comparing with abdominal injuries could be serious and even fatal. Sometimes, it will be overlooked. So the clinicians must observe them for signs of severe abdominal trauma incisively when they manage patients’ history of handlebar impact [6]. The aim of our study is to emphasize the seriousness of abdominal injury caused by bicycle handlebar in children. We retrospectively reviewed those cases’ management and outcomes for clinicians in their assessment of patients.
Patients and methods
Medical data were reviewed from the files of 219 patients (age 4–17 years) with bicycle handlebar injuries from January 2005 to December 2013 at the Department of Pediatric Surgery of Yuying Children’s Hospital of Wenzhou Medical University, China. All patients who were injured by bicycle handlebars impact admitted to our hospital had positive findings on physical examination, such as defense and/or rebound with abnormal blood tests. The collected data included demographies (such as age and gender) of the enrolled children, hospitalization details, length of hospital stay, complications of injury, laboratory values (mainly serum amylase, lipase and hepatic transaminases levels), ultrasonography (USG) and computed tomography (CT) findings, operative findings, management, and outcome.
Results
During the past 8 years, a total of 219 pediatric patients (187 males and 32 females) of handlebar injuries comprised the present study population. After performing a careful analysis, we found the peak incidence of blunt abdominal trauma caused by bicycle handlebars occured at the year of 2010. In many areas of China, the economic fluctuation will cause the population migration. Moreover, children bicycle injury cases were closely related to the local population change caused by local economy (Fig. 1). Most cases occurred in warm weather months (March–October) particularly the severe ones. The median age was 10.93 ± 3.68 years with a male predominance. Patients who had positive findings on physical examination underwent X-ray and USG. Most patients (n = 206; 94 % patients) underwent computed tomography (CT).

Numbers of floating population in Wenzhou district and patients with abdominal injury after bicycle-related trauma 2005–2013
The majority of abdominal injuries were solid organs, such as liver injuries (n = 184), pancreatic injuries (n = 33), splenic injuries (n = 23) and renal injuries (n = 16). Most of these injuries were isolated (n = 160; 73 % patients); the rest of the patients had associated injuries. The injury severity of patients was based on the Injury Scale of the American Association for the Surgery of Trauma (AAST), and therapeutic strategy was according to the injury grading. In our experience, the higher grade injuries (≥grade III) whose vital signs (mainly BP) were unstable needed emergency laparotomy.
The majority of lacerations of solid organs such as liver, pancreatic, splenic and renal injury could be relieved after conservative medical therapy. As shown in these data, for the unstable haemodynamics, eight patients with liver injury (1 grade III and 7 grade IV) and eight patients with pancreatic laceration (7 grade III and 1 grade IV) underwent laparotomy and the lacerations were oversewed.
Thirteen patients had hollow organ injuries who were mainly injured in duodenum (Table 1). Eleven patients with intestinal perforation were diagnosed by X-ray with free air under diaphragm and all underwent exploratory laparotomy, including nine primary duodenal anastomoses and two Roux-en-Y anastomoses (Fig. 2a, b). There were two patients with hematoma over the duodenal wall identified by a CT scan who were managed by parenteral nutrition and decompression of the stomach. After the treatment, hematoma was resolved and the children did well.

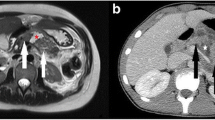
A 9-year-old boy had abdominal injuries caused by bicycle handlebars. a Arrows indicate tear of stomach and extraluminal retroperitoneal air adjacent to the duodenum and liver in CT scan. b Intra-operative photograph of complete transections of stomach. The tear is lifted by tweezers. The gastric mucosa can be seen through the tear
There were 8 patients with initial pancreatic injuries whose serum amylase and lipase levels were still high during the 6-month follow-up period, demonstrating pancreatic pseudocysts by CT scan (Fig. 3a, b). There were five patients whose health condition was improved after 14 days conservative medical therapy on a low-fat diet and discharged. Three children with the pancreatic pseudocyst that measured >6 cm underwent percutaneous ultrasound-guided drainage and treated with placement of transmural stents. After using octreotide, the pseudocyst had diminished in size by 50 %. All the patients were symptomatically better, after the transmural and transpapillary stents (if present) were removed by endoscopy. Their outcomes were good.

A male patient of 10 years old was hit by his bicycle handlebar. a The arrow indicates complete transections of pancreas in CT scan. b On a visit of 4 weeks after his discharge from our hospital, pancreatic pseudocyst was observed (arrow)
There were no deaths among the cases and the overall outcome in our series was good.
Discussion
Bicycling is a well-liked sporting activity in which many children participate; therefore, bicycle handlebar-related injuries continue to be a major health problem and frequently lead to hospitalization of children. Abdominal injuries resulting from bicycle handlebars remain a cause of mortality and morbidity in children. So we performed a retrospective review of our experience with particular emphasis on the abdominal injuries caused by it. We found that the total frequency of bicycle handlebar-related abdominal injuries continued to rise from year 2005 to 2010 and declined somewhat over the following years (Fig. 1). This trend was generally consistent with the changes of the region census and the economic situations during the study period. In many parts of China, the economic development almost inevitably results in massive migrations of population. There was a gradual increase in handlebar-related abdominal injuries found in the former 5 years of the study, which potentially may be the result of increasing quantity of transient population with improved economic progress. In the latter 3 years of the study, the reduction in cases was consistent with an outflow of population and a recessionary economic environment.
Throughout the study period, we found that the liver injuries were the most frequent bicycle handlebar-related abdominal injuries, so were pancreatic injuries in abdominal parenchymal viscera. USG and CT play a important role in the diagnosis of abdominal injuries. The level of liver transaminases could reflect accurately the state of liver healing. But for those of pancreatic injuries, the serum amylase and lipase levels were not useful or sensitive in determining the presence or severity of pancreatic damage [7]. One study supported that early endoscopic retrograde cholangiopancreatography (ERCP) is an essential part of the initial patient evaluation when pancreatic transection was highly suspected [8]. ERCP was a reliable method to accurately define continuity of the main pancreatic duct following pancreatic trauma; however, its application is limited for other pancreatic injuries. Although these tests had very poor correlation with either grade of injury or the need for operative intervention, they were closely related to complications of pancreatic injuries [9]. We found that on-going high level serum amylase might be a sign of injured pancreatic complications such as pseudocyst. In the present study, eight cases who had a progressive hyperamylasemia and lipase after nearly a month in hospital form pancreatic pseudocysts which are demonstrated by USG and CT.
The whole cases of hematomas and the majority of lacerations of solid organs such as liver, pancreatic, splenic and renal injury were relieved after conservative medical therapy. Because of unstable hemodynamics, 16 patients with liver and/or pancreatic laceration went through laparotomy and had laceration oversewed. Operative management appeared to be indispensable and effective, especially for the higher grade injuries, generally referred to grade III and above, which was in accordance with Cuenca’s report [9].
Duodenal trauma in the pediatric population is relatively uncommon and usually caused by blunt abdominal trauma, and associated intra-abdominal injuries are common with duodenal injuries [10, 11]. The emergency exploratory laparotomy was performed on 11 patients with subdiaphragmatic free air. The entire abdomen was inspected and duodenal perforation was discovered in nine cases who were rectified with primary duodenal anastomosis, whereas more complex procedures were used for severe injury. Serious gastrointestinal tract damage which was not suitable to perform primary anastomosis could take the Roux-en-Y anastomosis. Complete transections of the duodenum as well as stomach were detected in two children and they had subtotal gastrectomy, Roux-en-Y anastomosis, primary duodenal anastomosis, Stamm gastrostomy and feeding jejunostomy performed, also washing and drainage. In hemodynamically stable children with solitary traumatic duodenal perforation, several published studies have appeared in recent years, describing the use of laparoscopy in the management of primary repair of the duodenal perforation [12–14]. Although the laparoscopic approach was time-consuming and not applicable at the hemodynamically unstable ones, it held promise for providing advantages seen with minimally invasive approaches in other procedures, such as postoperative recovery and cosmetic considerations. Demonstrative CT images of duodenal obstruction of two patients, who showed digestive dysfunction, nausea, emesis and not eating, had no sign of pneumoperitoneum. They were diagnosed with duodenal hematoma and made uneventful recovery with conservative form of treatment.
Most of the complications found during the follow-up, resulting from pancreatic injuries, were pseudocysts. Some pseudocysts could resolve spontaneously while others could not but require treatment. We suggest that the therapeutic method of percutaneous ultrasound-guided drainage in combination with the octreotide is effective for isolated pseudocyst whose diameter exceeds 6 cm. There is a report claiming that the use of single-step EUS-guided drainage of pancreatic fluid collections is effective and safe for children [15]. There was no mortality in our series.
This study underlines the serious nature of handlebar injuries in children. No matter how trivial the accident appears, the handlebar injuries must be considered potentially serious. Especially, the abdominal wall should be treated with great care.
References
Davidson CM, Torunian M, Walsh P, Thompson W, McFaull S, Pickett W. Bicycle helmet use and bicycling-related injury among young Canadians: an equity analysis. Int J Equity Health. 2013;12:48.
Tracy ET, Englum BR, Barbas AR, Foley C, Rice HE, Shapiro ML. Pediatric injury patterns by year of age. J Pediatr Surg. 2013;48(6):1384–8.
Dennis J, Ramsay T, Turgeon AF, Zarychanski R. Helmet legislation and admissions to hospital for cycling related head injuries in Canadian provinces and territories: interrupted time series analysis. BMJ. 2013;346:f2674.
Acton CHC, Thomas S, Nixon JW. Children and bicycles: what is really happening? Studies of fatal and non-fatal bicycle injury. Inj Prev. 1995;1(2):86–91.
Lam JP, Eunson GJ, Munro FD, Orr JD. Delayed presentation of handlebar injuries in children. BMJ. 2001;322(7297):1288–9.
Alkan M, Iskit S, Soyupak S, et al. Severe abdominal trauma involving bicycle handlebars in children. Pediatr Emerg Care. 2012;28(4):357–60.
Adamson WT, Hebra A, Thomas PB, et al. Serum amylase and lipase alone are not cost effective screening methods for pediatric pancreatic trauma. J Pediatr Surg. 2003;38(3):354–7.
Klin B, Abu-Kishk I, Jeroukhimov I, et al. Blunt pancreatic trauma in children. Surg Today. 2011;41(7):946–54.
Cuenca AG, Islam S. Pediatric pancreatic trauma: trending toward nonoperative management? Am Surg. 2012;78(11):1204–10.
Clendenon JN, Meyers RL, Nance ML, et al. Management of duodenal injuries in children. J Pediatr Surg. 2004;39(6):964–8.
Ladd AP, West KW, Rouse TM, et al. Surgical management of duodenal injuries in children. Surgery. 2002;132(4):748–52.
Marwan A, Harmon CM, Georgeson KE, et al. Use of laparoscopy in the management of pediatric abdominal trauma. J Trauma. 2010;69(4):761–4.
Huang CL, Lee JY, Chang YT. Early laparoscopic repair for blunt duodenal perforation in an adolescent. J Pediatr Surg. 2012;47(5):E11–4.
Tytgat SHAJ, Zwaveling S, Kramer WLM, et al. Laparoscopic treatment of gastric and duodenal perforation in children after blunt abdominal trauma. Injury. 2012;43(9):1442–4.
Ramesh J, Bang JY, Trevino J. Endoscopic Ultrasound–guided Drainage of Pancreatic Fluid Collections in Children. J Pediatr Gastroenterol Nutr. 2013;56(1):30–5.
Acknowledgments
We would like to thank our colleagues from the Department of Pediatric Surgery, for their assistance with data collection.
Conflict of interest
Li–Na Dai, Cong-De Chen, Xiao-Kun Lin, Yong-Biao Wang, Li-Guang Xia, Ping Liu, Xiao-Ming Chen and Zhong-Rong Li declare that they have no conflict of interest
Compliance with ethical requirements
This article does not contain any studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dai, LN., Chen, CD., Lin, XK. et al. Abdominal injuries involving bicycle handlebars in 219 children: results of 8-year follow-up. Eur J Trauma Emerg Surg 41, 551–555 (2015). https://doi.org/10.1007/s00068-014-0477-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-014-0477-5