
Abstract
The practice of medicine has experienced a revolution in the use of catheter-based or endovascular techniques to manage age-related vascular disease over the past 15 years. In many scenarios the less invasive, endovascular method is associated with reduced morbidity and mortality than the traditional open surgical approach. Although somewhat delayed, the use of endovascular approaches in the management of certain trauma scenarios has also increased dramatically. With improvements in catheter-based and imaging technologies and a broader acceptance of the value of the endovascular approach, this trend is likely to continue to the benefit of patients. The use of endovascular techniques in trauma can be considered in three broad categories: (1) large-vessel repair (e.g. covered stent repair), (2) mid- to small-vessel hemostasis (e.g. coils, plugs, and hemostatic agents), and (3) large-vessel balloon occlusion for resuscitation (e.g. resuscitative endovascular balloon occlusion of the aorta). While not exclusive, these categories provide a framework from which to consider establishing a trauma-specific endovascular inventory and performance of these techniques in the setting of severe injury. The aim of this review is to use this framework to provide a current appraisal of endovascular techniques to manage various forms: vascular injury, bleeding, and shock; including injury patterns in which an endovascular approach is established and scenarios in which it is nascent and evolving.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In parallel with the use of endovascular procedures to manage age-related vascular disease, the use of catheter-based techniques to manage severe injury has increased steadily over the past ten years. An analysis of the National Trauma Data Bank reported that 8.1 % of acute arterial injuries in 2003 were treated with a catheter-based therapy, compared to only 2.1 % in 1994. In that same study nearly equal number of blunt (55 %) and penetrating (45 %) injuries were treated with endovascular therapy [1]. A more recent study, also using NTDB data, reported that 16 % of all vascular injuries were treated with an endovascular therapy, including 20 % of patients who were hypotensive at the time of the intervention [2]. In these and other reports, the use of endovascular therapies to manage certain patterns of severe injury is associated with lower rates of morbidity and mortality; a finding which also parallels the introduction of catheter-based methods to the management of age-related vascular disease. As familiarity with endovascular techniques increases and advancements in imaging and device technology occur, their place in the treatment algorithm of the injured patient is likely to increase [3].
A detailed description of the conduct of and requirements for various endovascular procedures is beyond the scope of this manuscript. However, for context it is worth reviewing that endovascular techniques involve over-the-wire access (percutaneous or direct exposure) to the arterial or venous system and placement of a working port, also referred to as a sheath. Once access is achieved, wires and catheters are directed within the vascular system with the aid of fluoroscopy to the anatomic site of interest or concern. Endovascular access to a given anatomic region may be achieved to perform a diagnostic contrast study (i.e. angiography), accomplish large-vessel occlusion, or render a therapy for vessel disruption and/or bleeding. Not uncommonly a combination of one or more of these is combined during the endovascular approach to injury.
The trauma-specific endovascular inventory is generally less complicated than that required to manage the full range of vascular disease [4, 5]. In addition to a standard array of access needles, wires, and sheaths, the endovascular inventory for trauma can be considered in the following categories: compliant balloon catheters, covered stent grafts, and coils and other thrombotic adjuncts. Devices from these categories are introduced over a wire at the access site through sheaths that vary in size and length depending upon the diameter and nature of the device. Because they are easiest to see, handle and manipulate in an urgent setting, 0.035″ diameter wires are favored for cases of acute injury management. Endovascular wires range in degree of stiffness, hydrophilic coating, and length (180, 260 or 300 cm) to facilitate the desired function. Most commonly, a wire is chosen to facilitate one of three broad maneuvers: (1) basic vascular access and catheter exchange, (2) specific branch vessel selection, and (3) advancement and positioning of a large sheath or endovascular device.
While endovascular procedures quickly become more involved from these basic steps and considerations, the underlying advantage rests in their less invasive and therefore less physiologically taxing approach. The aim of this review is to provide an appraisal of these techniques to manage various forms: vascular injury and hemorrhagic shock. The authors aim to demonstrate aspects of injury in which the endovascular approach is better suited and established as well as injury scenarios in which the use of an endovascular approach is nascent and evolving.
Large-vessel endovascular repair
Thoracic aortic injury
Repair of thoracic aortic injury has historically been accomplished using an open operative approach with direct replacement of the injured segment. Open repair is an established and durable procedure accomplished using either a clamp-and-sew technique or some form of distal aortic perfusion [6]. The use of stent grafts to manage thoracic aortic trauma stemmed from favorable observations (i.e. lower morbidity and mortality) from the use of endovascular techniques to treat thoracic aneurysm disease. As such, the initial stent-graft technology used to manage thoracic aortic trauma was tailored for older aortic pathology and not for younger, disease-free aortic injury. As a result, some of the early experiences using aneurysm devices off-label to treat aortic injuries included device-related complications [7]. Despite this “borrowing” of aneurysm technology to treat aortic injury, early clinical studies still showed lower rates of complications and better survival with this approach compared to open aortic repair [8–10]. Today, endovascular stent grafts have evolved significantly to better accommodate smaller, injured aortas including at grafts that are approved or seeking approval for trauma [11, 12].
Assessment and operative technique
If blunt thoracic aortic injury (BTAI) is suspected and the patient’s hemodynamic status allows, the initial assessment should include a contrast-enhanced CT scan of the chest, abdomen, and pelvis. If the diagnosis of BTAI is made and there are no contraindications, beta-blockade should be initiated to reduce stress on the injury while other therapeutic considerations are made. The decision regarding endovascular versus open repair is based largely on the position of the lesion relative to arch vessels. Traditionally, 2 cm of normal aorta proximal to the injury is considered necessary for effective deployment of a thoracic aortic stent graft, although newer endovascular devices have shown success in managing BTAI with shorter landing zones [11, 12]. Traumatic aortic injury is typically more focal or shorter in length than atherosclerotic aneurysm disease and thus requires less extensive aortic coverage for treatment. This fact along with the urgent or emergent need for most endovascular procedures for BTAI obviates the need for pre-operative drainage to reduce the risk of spinal cord ischemia in most cases.
It is not uncommon for thoracic endovascular aortic repair (TEVAR) to involve coverage of aortic branch vessels such as the left subclavian artery (LSCA). Typically this maneuver is performed to extend the landing zone of normal or uninjured aorta in which to deploy the proximal most aspect of the stent graft. While planned or even routine coverage of the left subclavian artery during TEVAR for BTAI has been reported without significant morbidity, other studies have shown this maneuver to be associated with slightly higher rates of spinal cord ischemia. To reduce this chance and maintain antegrade, pulsatile flow to the left subclavian artery and its branch vessels (i.e. left vertebral and mammary arteries), some institutions perform a preemptive left carotid to subclavian artery bypass prior to TEVAR for BTAI. In some situations such as patients with prior cardiac surgery and a left internal mammary to coronary artery, graft may also necessitate a carotid to subclavian bypass prior to placement of the stent graft and coverage of the left subclavian artery orifice. All patients being considered for TEVAR should undergo careful pre-operative assessment of the vertebral arteries to determine patency, size, and direction of flow to determine whether or not the origin of the left subclavian artery can be covered and whether or not a preemptive carotid to subclavian artery bypass would be advisable.
Outcomes
Thoracic endovascular aortic repair (TEVAR) is the currently the most studied endovascular intervention in trauma. The short-term data suggest that aortic stent-grafting is comparable to open repair, citing lower rates of paraplegia, blood loss, complications, and shorter hospital stays [8–14]. However, long-term data remain. With young patients receiving aortic stent grafts, the relationship of the aging stent graft to the aging aorta is unknown.
Complications
Adverse outcomes following TEVAR include stent collapse and “bird beaking” (the proximal portion of the stent graft does not oppose to the aortic wall) due to size mismatching and/or a small arch radius, and may ultimately lead to additional endovascular or open repair [13, 14]. AAST multi-institutional trials have documented the complication rates of TEVAR. Technology continues to advance rapidly, and many industry-sponsored multi-institutional trials are currently investigating aortic devices with improved deployment systems, improved conformability, and smaller delivery systems, particularly well suited for younger patients. Ongoing trials for branched and fenestrated grafts will allow devices suitable for coverage across arch vessels to be available if proven safe and effective.
Abdominal aortic injury
Abdominal aortic mechanism of injury relates to the biomechanical direct and indirect forces incurred while it is tethered among the spinal column, the peritoneum, and abdominal viscera [14–16]. Atherosclerotic changes of the aorta have been associated with a weakening of the intima in addition to loss of elasticity and compliance and thus thought to increase the risk of aortic injury. These forces can occur during motor vehicle collisions when the aorta is compressed by the seat belt thus termed “seat belt aorta”. Other mechanisms include long-distance falls from heights, direct compression of the aorta, and penetrating injuries.
Depending on the magnitude of the traumatic forces, BAAI presents as a spectrum of disease ranging from a minimal aortic injury (MAI) to free rupture of the aorta [15, 16]. There are increasing numbers of MAIs diagnosed as imaging technology improves. Along the spectrum of injury, traumatic intimal tears can occur and manifest as intimal flaps or dissection. These can be complicated by thrombosis, embolism, and acute arterial insufficiency. Injuries involving the adventitia lead to pseudoaneurysm formation or even rupture of the aortic wall. Rupture of the aortic wall can also be due to branch vessel avulsion. The majority of the injuries occur inferior to the renal arteries and the most common associated injuries are small bowel injuries (38 %) and thoracolumbar spine injuries (25 %) [15].
Assessment and operative technique
The initial presentation is dependent on the presence or absence of free rupture of the abdominal aorta, branch vessel avulsion, or concomitant inferior vena cava injury. These cases typically present with hemodynamic instability due to hemorrhagic shock. In a recent BAAI series, these patients were all hemodynamically unstable and 75 % had cardiac arrest in the emergency department with 38 % requiring an emergency department thoracotomy [15].
In the setting of a retroperitoneal hematoma, temporary tamponade may provide a period of hemodynamic stability, positively impacting survival. In cases of BAAI, abdominal wall ecchymosis due to seat belt injury (seat belt sign) is seen in one-third of the cases and should raise the index of suspicion for aortic injuries as well as hallow viscous injuries.
Management of aortic injury varies and risk of mortality rises with the severity of the pathologic lesion. In a recent review of the National Trauma Data Bank of 436 patients with BAAI from 180 centers from 2007 to 2009, 90 % was managed non-operatively [10]. Of those repaired, 69 % underwent endovascular repair, with the remainder undergoing open aortic repair and two extra-anatomic bypasses. In general, cases of BAAI with uncomplicated intimal flaps are managed non-operatively with anti-impulse (beta-blockers) and anti-platelet (aspirin) therapy and close follow-up. These lesions typically demonstrate a decrease in size and eventually complete resolution. Cases of aortic pseudoaneurysm require operative repair to prevent rupture, but this can be managed on a semi-elective basis during the initial hospitalization. Patients with perfusion deficits, expanding hematoma and concomitant intra-abdominal injuries requires emergent exploration and/or repair.
Reports of endovascular stent placement in cases of aortic injuries have recently increased in frequency similarly to that of blunt thoracic aortic injury. Most of the literature is limited to case reports. Small case series describe the use of endovascular devices in cases of both blunt and penetrating trauma [14]. Advantages include cases with associated gross contamination from hollow viscous injury that can jeopardize aortic grafts due to risk of infection, or management of injuries difficult to expose by conventional means. Endovascular interventions also can be used as a temporizing technique.
Outcomes
Injury to the abdominal aorta is highly lethal. Among those who survive the transport to the hospital, mortality rates range from 32 to 78 % with hemorrhagic shock being the most common cause of associated mortality. Outcomes in cases requiring a resuscitative thoracotomy remain poor. In BAAI, mortality varies by the type of aortic injury. Based on recent literature, aggregate mortality is 11 %. In cases treated by endovascular repair, the long-term durability of aortic endografts for abdominal aortic trauma has not been well described. Clearly long-term follow-up will be required in these cases. The ongoing AAST multi-institutional PROOVIT and AORTA trials will provide some answers in the near future.
Aortic branch and extremity vessels
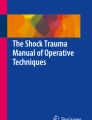
Treatment of aortic branch (e.g. subclavian, common carotid, mesenteric, and iliac) and extremity vessel injury can also be accomplished endovascular stent-graft techniques (Fig. 1). As previously described, the balloon may be a life-saving measure in the event of exsanguinating hemorrhage, particularly where body habitus may impede rapid dissection and proximal control. Injuries to the distal subclavian or axillary arteries can be managed with balloon tamponade, which may prevent an upper median sternotomy incision to achieve proximal control. A stent can then be placed across the lesion to prevent further blood loss, or the balloon may stay in place while an open exploration is performed. Injury to the subclavian or axillary vein, or brachial plexus, as well as the physiologic status of the patient and their body habitus, will determine whether an endovascular or a hybrid procedure is necessary.

Injury and occlusion of the axillary artery (a) successfully treated with a stent (b)
Endovascular treatment of extremity injuries is more common, although there exist only small case series in the literature. Limb-salvage and survival rates are reported up to 100 %, but no comparison between open and endovascular therapy treatment has been reported [17]. Injury to the carotid arteries is also amenable to endovascular therapy. With reported 30-day mortality and stroke rates of 5 %, this therapy may be comparable to open repair [18].
Mid- to small-vessel hemostasis
Trans-arterial catheter embolization is being used with increasing frequency in trauma patients. Interventionalists are employing a variety of techniques to accomplish minimally invasive hemorrhage control. The most commonly employed location is the pelvis, but techniques are being applied to the solid abdominal organs as well. Soft tissue, extremity and extracranial cerebral vessels are being treated as well. Despite the enthusiasm for these techniques many questions remain surrounding indications for interventions as well as the role of combined approaches and proper utilization of constantly improving technology.
There are several factors to consider when treating a hemorrhaging patient with embolization. Size of the vessel and duration of occlusion must be considered when choosing an embolization material. Generally coils and plugs are used in larger vessels and microcoils or gelatin sponge is used in small vessels [19]. Additionally, some materials are temporary and result in vessel recanalization in days to weeks [20]. Generally, supra-selective techniques employed with the patients are stable, to preserve organ function whenever possible, but in cases of multiple sites of large extravasation and in unstable patients more proximal embolization is necessary. Certain areas that have dual vascular supply or extensive collateral circulation are tolerant of large areas of embolization. This includes the liver, pelvis, upper gastrointestinal tract, and pancreas [19]. But this may also result in distal circulation leading to ongoing hemorrhage. In some situations, it is necessary to embolize both proximal and distal to the site of injury. End arterial organs such as the kidney do not tolerate proximal embolization and supra-selective embolization is necessary. Nonexpendable arteries of the extremities cannot be embolized and require either surgical reconstruction or stent-graft placement.
The most commonly embolized vascular bed and therefore the most studied is the pelvis. While debate remains some general recommendations do exist. Patients with signs of instability in the setting of pelvic factors require angiography after other sources of hemorrhage have been excluded. Those with ongoing blood loss should be considered for repeat angiography and embolization. Stable patients should be considered for embolization in the setting of active contrast extravasation on CT or angiography (Fig. 2). Hypotension at admission, severe abdominal trauma, and a blush diameter of >1.5 cm all predict need for intervention [21]. Complication rates are low and gluteal necrosis seems to be related to primary trauma and protracted hypotension rather than a direct result of ischemia.

Active extravasation of contrast on pelvic angiography (a) requiring coil embolization for hemostasis (b)
Non-operative of splenic trauma is generally accepted, but substantial failure rates in higher injury grades remain common, with one large study reporting rates of 19.6, 33.3, and 75 % for grades III, IV, and V, respectively [22, 23]. Embolization in these patients appears to improve the success of non-operative management. A study out of Wake Forest demonstrated that success can be improved from 25 to 5 % failure in stable patients in this category with the addition of embolization [24]. Evidence also suggests that both proximal and distal embolization techniques are acceptable in the spleen and have similar outcomes [25].
Hepatic angio-embolization is indicated in situations when CT suggests high-grade injury or active extravasation. It is also a useful adjunct to laparotomy and perihepatic packing in those patients with inaccessible intrahepatic hemorrhage. Although liver-related mortality is low in these patients, morbidity is present in up to 30 % of patients including parenchymal necrosis, gallbladder necrosis, bile leaks, and abscesses. Super-selective embolization appears to reduce these complications but frequently clinical instability prevents this technique [26–28].
Resuscitative endovascular balloon occlusion of the aorta (REBOA)
The most common cause of death from aortic trauma remains hemorrhagic shock compounded by ongoing coagulopathy, thus early proximal control of the aorta is a life-saving maneuver. The intra-aortic occlusive balloon was first described for controlling major aortic hemorrhage in the Korean War [29]. Since that time, it has been used percutaneously in many clinical disciplines as an effective and minimally invasive means of achieving rapid proximal control. Reports of use for control of bleeding during pelvic surgery [30, 31], hepatobiliary surgery [32], orthopedic surgery [33], postpartum hemorrhage [34], and repair of ruptured AAA [35–38] suggest that the IAOB is a life-saving measure. Physiologic parameters such as serum lactate, pH, pCO2, and central, cerebral and coronary perfusion in animal models of hemorrhagic shock have been shown to improve with REBOA [37–40]. Descriptions of its use for trauma are few [41–43], but may be useful for control of non-compressible torso hemorrhage in the abdomen and pelvis. Of note, most of the proceduralists in these reports are interventional or vascular specialists with board certification in these areas, but the potential exists to train trauma surgeons in this technique. The use of REBOA to obtain proximal control at the level of the diaphragm prior to entering the abdomen may have a role in early control of hemorrhage from the injured aorta.
Assessment and operative technique
Placement of the REBOA can be done expeditiously and does not delay the laparotomy as demonstrated in proximal control of the aorta in cases of ruptured abdominal aortic aneurysms. Currently, indications for REBOA in our institution include persistent hypotension with hemorrhage below the diaphragm for placement of the balloon in zone 1, and severe pelvic hemorrhage for placement in zone 3 (Fig. 3). Contraindications for REBOA include suspected thoracic aortic injury, or other vascular injury above the diaphragm. The technique of REBOA begins with standard cannulation of the common femoral artery approximately 2 cm below the inguinal ligament. Ultrasound utilization is ideal, but landmarks, fluoroscopy, blind placement, or cut-down on the common femoral artery can be utilized. An Amplatz wire is advanced into the catheter to the level approximating the 2nd rib space (measured externally prior to insertion). In the absence of fluoroscopy, an X-ray demonstrating wire position must be obtained to confirm placement. Marking of the wire at its end point on a draped end table helps to keep wire position during the procedure. The arterial line catheter is removed and a 12Fr sheath is inserted to a level approximating the proximal iliac artery (measured externally to the umbilicus). The dilator is removed, and the CODA 32-mm balloon catheter is advanced over the wire to zone 1 (external landmark: xiphoid) or to zone 3 (external landmark: above umbilicus). A 30-cc syringe filled with 10cc of contrast and 20cc of normal saline is used to inflate the balloon quickly to a point not beyond high resistance. An X-ray may be obtained to confirm balloon placement. An immediate increase in SBP should be noticed if the REBOA technique is successful. Transportation to definitive treatment can occur with the REBOA in place (Fig. 4). Once aortic occlusion is no longer necessary, open repair of the common femoral artery is required. Careful attention should be paid to distal pulses, as any deficit may be due to prolonged cannulation and/or thromboembolism.

a X-ray demonstrating severe pelvic fractures and REBOA in zone 3, b REBOA in zone 1, contrast with normal saline is ideal; however, normal saline alone can be used for inflation if contrast unavailable

REBOA in zone III ready for transport to definitive care (IR or hybrid OR)
Our earliest experience with REBOA in the clinical setting demonstrates this procedure to be a life-saving technique [44]. Currently the procedure uses FDA-approved devices not well suited for the trauma population. Lower profile devices are in development (ER-REBOA/Pryor) and will be available in the near future.
Conclusion
The use of endovascular techniques for the management of vascular disease has increased steadily for more than two decades. While the application of this minimally invasive technology in the setting of trauma has been relatively delayed, its utility is quickly being recognized and established. Certain patterns of injury such as blunt aortic and axillo-subclavian artery are already better approached with catheter-based methods and the technology shows promise in other areas of hemorrhage control and the management of shock. As vascular access, stent-graft, balloon and coil technologies are designed with more trauma-specific features the utility of this line of therapy in the emergency setting will increase. To convey the benefit in survival and recovery associated with endovascular technologies to their patients, trauma and emergency services will need to incorporate these approaches into practice; either through a readily available multi-disciplinary team or by having expertise within trained members of the individual emergency or trauma services.
References
Reuben BC, Whitten MG, Sarfati M, Kraiss LW. Increasing use of endovascular therapy in acute arterial injuries: analysis of the National Trauma Data Bank. J Vasc Surg. 2007;46:1222–6.
Avery LE, Stahfield KR, Corcos AC, Scifres AM, Ziembicki JA, Varcelotti J, Peitzman AB, Billiar TR, Sperry JL. Evolving role of endovascular techniques for traumatic vascular injury: a changing landscape. J Trauma Acute Care Surg. 2012;72(1):41–6.
Rasmussen TE, Woodson J, Rich NM, Mattox KL. Current opinion: vascular injury at a crossroads. J Trauma. 2011;70(5):1291–3.
Rasmussen TE, Clouse WD, Peck MA, Bowser AN, Eliason JL, Cox MW, Woodward EB, Jones WT, Jenkins DH. The development and implementation of endovascular capabilities in wartime. J Trauma. 2008;64:1169–76.
Holcomb JB, Fox EE, Scalea TM, Napolitano LM, Albarado R, Gill B, Dunkin BJ, Kirkpatrick AW, Cotton BA, Inaba K, DuBose JJ, Cohen AA, Azizzadeh A, Brenner M, Cohen MJ, Wade CE, Lumsden AB, Andrassy R, Rhee PM, Bass BL, Mattox KL, Britt LD, Eastman AB, Hoyt DB, Rasmussen TE. Current opinion on catheter-based hemorrhage control in trauma patients. J Trauma Acute Care Surg. 2014;76:888–93.
Mattox KL, Wall MJ. Historical review of blunt injury to the thoracic aorta. Chest Surg Clin N Am. 2000;10:167–82.
Fabian TC, Richardson JD, Groce MA, et al. Prospective study of blunt aortic injury: multicenter trial of the American Association for the Surgery of Trauma. J Trauma. 1997;42:374–80.
Demetriades D, Velmahos G, Scalea T, et al. Operative repair or endovascular stent/graft in blunt traumatic thoracic aortic injuries: results of an AAST multicenter study. J Trauma. 2008;64:561–70.
Demetriades D, Velmahos GC, Scalea TM, et al. Diagnosis and treatment of blunt thoracic aortic injuries: changing perspectives. J Trauma. 2008;64:1415–9.
Arthurs ZM, Starnes BW, Sohn VY, Singh N, Martin MJ, Andersen CA. Functional and survival outcomes in traumatic blunt thoracic aortic injuries: an analysis of the National Trauma Databank. J Vasc Surg. 2009;49:988–94.
Lee WA, Matsumura J, Mitchell RS, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery. J Vasc Surg. 2011;53:187–92.
Piffaretti G, Benedetto F, Menegolo M, et al. Outcomes of endovascular repair for blunt thoracic aortic injury. J Vasc Surg. 2013;58:1483–9.
Khoynezhad A, Azizzadeh A, Donayre CE, Matsumoto A, Velazquez O, White R. RESCUE investigators. Results of a multicenter, prospective trial of thoracic endovascular aortic repair for blunt thoracic aortic injury (RESCUE trial). J Vasc Surg. 2013;57(4):899–905.
Azizzadeh A, Ray HM, Dubose JJ, Charlton-Ouw KM, Miller CC, Coogan SM, Safi HJ, Estrera AL. Outcomes of endovascular repair for patients with blunt traumatic aortic injury. J Trauma Acute Care Surg. 2014;76(2):510–6.
Shalhub S, Starnes BW, Tran NT, Hatsukami TS, Lundgren RS, Davis CW, Quade S, Gunn M. Blunt abdominal aortic injury. J Vasc Surg. 2012;55(5):1277–85.
Starnes BW, Lundgren RS, Gunn M, Quade S, Hatsukami TS, Tran NT, Mokadam N, Aldea G. A new classification scheme for treating blunt aortic injury. J Vasc Surg. 2012;55(1):47–54.
DuBose JJ, Rajani R, Gilani R, Arthurs ZA, Morrison JJ, Clouse WD, Rasmussen TE. Endovascular management of axillo-subclavian arterial injury: a review of published experience. Injury. 2012;43:1785–92.
du Toit DF, Coolen D, Lambrechts A, de Odendaal VJ, Warren BL. The endovascular management of penetrating carotid artery injuries: long-term follow-up. Eur J Vasc Endovasc Surg. 2009;38(3):267–72.
Lopera JE. Embolization in trauma: principles and techniques. Semin Intervent Radiol. 2010;27(1):14–28.
Abada HT, Golzarian J. Gelatin sponge particles: handling characteristics for endovascular use. Tech Vasc Interv Radiol. 2007;10:257–60.
Michailidou M, Velmahos GC, van der Wilden GM, Alam HB, de Moya M, Chang Y. “Blush” on trauma computed tomography: not as bad as we think! J Trauma Acute Care Surg. 2012;73(3):580–4.
Peitzman AB, Harbrecht BG, Rivera L, et al. Failure of observation of blunt splenic injury in adults: variability in practice and adverse consequences. J Am Coll Surg. 2005;201:179–87.
Miller PR, Chang MC, Hoth JJ, Mowery NT, Hildreth AN, Martin RS, Holmes JH, Meredith HW, Requarth JA. Prospective trial of angiography and embolization for all grade III to V blunt splenic injuries: nonoperative management success rate is significantly improved. Am Coll Surg. 2014;218(4):644–8.
Schnüriger B, Inaba K, Konstantinidis A, Lustenberger T, Chan LS, Demetriades D. Outcomes of proximal versus distal splenic artery embolization after trauma: a systemic review and meta-analysis. J Trauma. 2011;70(1):252–6.
Letoublon C, Morra I, Chen Y, Monnin V, Voirin D, Arvieux C. Hepatic arterial embolization in the management of blunt hepatic trauma: indications and complications. J Trauma. 2011;70(5):1032–6.
Mohr AM, Lavery RF, Barone A, et al. Angiographic embolization for liver injuries: low mortality, high morbidity. J Trauma. 2003;55:1077–81.
Dabbs DN, Stein DM, Scalea TM. Major hepatic necrosis: a common complication after angioembolization for treatment of high-grade liver injuries. J Trauma. 2009;66:621–7.
Huges C. Use of intra-aortic balloon catheter tamponade for controlling intra-abdominal hemorrhage in man. Surgery. 1954;36(1):65–8.
Yang L, Chong-Qi T, Hai-Bo S, Lan Z, Tian-Fu Y, Hong D, et al. Appling the abdominal aortic-balloon occluding combine with blood pressure sensor of dorsal artery of foot to control bleeding during the pelvic and sacrum tumors surgery. J Surg Oncol. 2008;97(7):626–8.
Veith FJ, Gupta S, Daly V. Technique for occluding the supraceliac aorta through the abdomen. Surg Gynecol Obstet. 1980;51:426–8.
Miura F, Takada T, Ochiai T, Asano T, Kenmochi T, Amano H, Yoshida M. Aortic occlusion balloon catheter technique is useful for uncontrollable massive intraabdominal bleeding after hepato-pancreato-biliary surgery. J Gastrointest Surg. 2006;10(4):519–22.
Siebler J, Dipasquale T, Sagi HC. Use of temporary partial intra-iliac balloon occlusion for decreasing blood loss during open reduction and internal fixation of acetabular and pelvis fractures. J Orthop Trauma. 2012;26:e54–7.
Harma M, Harma M, Kunt AS, Andac MH, Demir N. Balloon occlusion of the descending aorta in the treatment of severe post-partum hemorrhage. Aust NZ J Obstet Gynaecol. 2004;44:170–1.
Matsuda H, Tanaka Y, Hino Y, Matsukawa R, Ozaki N, Okada K, et al. Transbrachial arterial insertion of aortic occlusion balloon catheter in patients with shock from ruptured abdominal aortic aneurysm. J Vasc Surg. 2003;38(6):1293–6.
Assar AN, Zarins CK. Endovascular proximal control of ruptured abdominal aortic aneurysms: the internal aortic clamp. J Cardiovasc Surg. 2009;50:381–5.
Malina M, Veith FIKSBS. Balloon occlusion of the aorta during endovascular repair of ruptured abdominal aortic aneurysm. J Endovasc Ther. 2005;12(5):556–9.
Spence PA, Lust RM, Chitwood WR Jr, Iida H, Sun YS, Austin EH 3rd. Transfemoral balloon aortic occlusion during open cardiopulmonary resuscitation improves myocardial and cerebral blood flow. J Surg Res. 1990;49:217–21.
Sesma J, Labandeira J, Sara MJ, Espila JL, Arteche A, Saez MJ. Effect of intra-aortic occlusion balloon in external thoracic compressions during CPR in pigs. Am J Emerg Med. 2002;20:453–62.
White JM, Cannon JW, Stannard A, Markov NP, Spencer JR, Rasmussen TE. Endovascular balloon occlusion of the aorta is superior to resuscitative thoracotomy with aortic clamping in a porcine model of hemorrhagic shock. Surgery. 2011;150:400–9.
Avaro JP, Mardelle V, Roch A, Gil C, de Biasi C, Oliver M, Fusai T, Thomas P. Forty minute endovascular aortic occlusion increases survival in an experimental model of uncontrolled hemorrhagic shock caused by abdominal trauma. J Trauma. 2011;71:720–6.
Gupta BK, Khaneja SC, Flores L, Eastlick L, Longmore W. GWS. The role of intra-aortic balloon occlusion in penetrating abdominal trauma. J Trauma. 1989;29(6):861–5.
Martinelli T, Thony F, Declety P, Sengel C, Broux C, Tonetti J, Payen JF, Ferretti G. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shock from pelvic fractures. J Trauma. 2010;68:942–8.
Stannard A, Eliason JE, Rasmussen TE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma. 2011;71:1869–72.
Brenner M, Hoehn M, Pasley J, Dubose J, Stein D, Scalea T. A clinical series of REBOA(Resuscitative Endovascular Balloon Occlusion of the Aorta) for trauma: a military-civilian collaboration in hemorrhage control. J Trauma Acute Care Surg. 2014;77(2):286–91.
Conflict of interest
M. Brenner, M. Hoehn, and T. E. Rasmussen declare that they have no conflict of interest.
Compliance with ethical requirements
This work is in compliance with ethical requirements. M. Brenner, M. Hoehn, and T. E. Rasmussen declare that this is a review article that includes no studies on humans or animals.
Author information
Authors and Affiliations
Corresponding author
Additional information
The views expressed in this manuscript are those of the authors and do not reflect the official position or policy of the United States Air Force or the Department of Defense.
Rights and permissions
About this article

Cite this article
Brenner, M., Hoehn, M. & Rasmussen, T.E. Endovascular therapy in trauma. Eur J Trauma Emerg Surg 40, 671–678 (2014). https://doi.org/10.1007/s00068-014-0474-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-014-0474-8