
Abstract
Background
Quick sequential organ failure assessement (qSOFA) has been validated for patients with presumed sepsis and the general emergency department (ED) population. However, it has not been validated in specific subgroups of ED patients with a high mortality. We aimed to investigate the prognostic performance of qSOFA with respect to in-hospital mortality, intensive care unit (ICU) admission, and length of hospitalisation in patients with decompensated liver cirrhosis. Furthermore, we compared qSOFA to systemic inflammatory response syndrome (SIRS), model of end stage liver disease score (MELD), and Child–Pugh criteria and evaluated whether addition of sodium (Na+) levels to qSOFA increases its prognostic performance.
Methods
This observational study included patients admitted with the diagnosis of decompensated liver cirrhosis. All patients with a complete set of vital parameters were included in this study.
Results
A total of 186 patients were included. A positive qSOFA score was not associated with in-hospital mortality, ICU admission, or length of hospitalisation (all p > 0.15). MELD scores reliably predicted need for ICU admission and in-hospital mortality (both p < 0.01), but not the length of hospitalisation. qSOFA-Na+ only moderately increased the diagnostic performance of qSOFA with regard to need for ICU admission (AUCICU[qSOFA] = 0.504 vs. AUCICU[qSOFA-Na+] = 0.609, p = 0.03), but not for in-hospital mortality (AUCdeath[qSOFA] = 0.513 vs. AUCdeath[qSOFA-Na+] = 0.592, p = 0.054).
Conclusion
qSOFA does not predict in-hospital mortality, ICU admission or length of hospitalisation in patients with decompensated liver cirrhosis. Extension of qSOFA with a disease-specific component, the qSOFA-Na+, moderately increased the diagnostic ability of qSOFA.
Zusammenfassung
Hintergrund
Der „quick sequential organ failure assessement“(qSOFA)-Score wurde zur Prädiktion der Mortalität sowohl bei Patienten mit Verdacht auf Sepsis als auch bei Notfallpatienten im Allgemeinen validiert. Eine Validierung bei bestimmten Untergruppen von Notfallpatienten mit hoher Mortalität ist jedoch noch nicht erfolgt. Ziel dieser Arbeit war es, die prognostische Wertigkeit bei Patienten, die sich mit dekompensierter Leberzirrhose in der Notaufnahme vorstellen, in Bezug auf Krankenhaussterblichkeit, Verlegung auf die Intensivstation und Krankenhausverweildauer zu analysieren. Des Weiteren wurde qSOFA mit „systemic inflammatory response syndrome“(SIRS)-, „model of end stage liver disease score“(MELD)- und Child-Pugh-Kriterien verglichen. Es wurde überprüft, ob die Einbeziehung des Natriumspiegels (Na+) in qSOFA die prognostische Wertigkeit erhöht.
Methoden
Alle Patienten mit der Aufnahmediagnose einer dekompensierten Leberzirrhose, die sich über einen Zeitraum von 10 Jahren in der Notaufnahme des Universitätsklinikums Bern, Schweiz, vorstellten, wurden in die Beobachtungsstudie eingeschlossen. Die Dokumentation der Vitalparameter musste vollständig sein.
Ergebnisse
In die Studie wurden 186 Patienten eingeschlossen. Der MELD-Score war sowohl mit der Krankenhaussterblichkeit als auch mit der notfallmäßigen Verlegung auf die Intensivstation assoziiert (je p < 0,01), nicht jedoch mit der Krankenhausverweildauer. Ein positiver qSOFA-Score (≥2 Punkte) war dagegen nicht mit der Krankenhaussterblichkeit, Verlegung auf die Intensivstation oder Krankenhausverweildauer assoziiert (je p > 0,15). Eine Erweiterung des qSOFA-Scores um die Natriumkomponente (qSOFA-Na+) erhöhte die Vorhersagekraft bezüglich der notfallmäßigen Verlegung auf die Intensivstation moderat (AUC[qSOFA] = 0,504 vs. AUC[qSOFA-Na+] = 0,609, p = 0,03), die bezüglich der Krankenhaussterblichkeit dagegen nicht (AUC[qSOFA] = 0,513 vs. AUC[qSOFA-Na+] = 0,592, p = 0,054).
Schlussfolgerung
Der qSOFA-Score besitzt keine ausreichende Vorhersagekraft für die Krankenhaussterblichkeit, notfallmäßige Verlegung auf die Intensivstation oder Krankenhausverweildauer bei Patienten mit dekompensierter Leberzirrhose. Eine Erweiterung des qSOFA-Scores um eine erkrankungsspezifische Natriumkomponente erhöht die prognostische Wertigkeit moderat.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In February 2016 the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) were published and a new clinical score named quick Sequential Organ Failure Assessment (qSOFA) was presented [1]. The score contains a set of three variables (respiratory rate, mental status, systolic blood pressure) and was proposed as a bedside screening tool for patients with suspected sepsis [1]. Several studies have assessed the utility of qSOFA for prediction of outcome in the intensive care unit (ICU) and emergency department (ED) setting in patients with suspected sepsis [2,3,4,5,6,7,8,9,10,11,12,13]. qSOFA has also shown a good predictive value for adverse outcomes (ICU admission, length of hospitalisation, mortality) in the general ED and ICU population [14]. However, further validations in respective subgroups of ED patients with a high mortality have not yet been performed.
Liver cirrhosis was the eighth leading cause of death in the United States in 2010 [15] and has accounted for over a million deaths worldwide with a rising incidence over the last 30 years [16]. Admissions to hospitals due to liver cirrhosis are associated with an overall in-hospital mortality of about 8% [17] which increases to 35% in patients with decompensated liver cirrhosis [18]. Patients with decompensated liver cirrhosis show typical haemodynamic and pathophysiological changes [19] which have some similarity to sepsis [20], including alterations in mental status due to development of hepatic encephalopathy [19, 21]. It seems therefore probable that the use of qSOFA may help to distinguish patients with adverse outcomes from the ones with a favourable course in decompensated liver cirrhosis.
We therefore aimed to validate the prognostic performance of qSOFA in patients presenting with decompensated liver cirrhosis for the primary outcome of in-hospital mortality. Secondarily, we evaluated whether the use of qSOFA adequately predicts ICU admission and length of hospitalisation and compared its predictive value to other disease severity markers such as systemic inflammatory response syndrome (SIRS), model of end stage liver disease score (MELD) and Child–Pugh score. In addition, we tested whether a disease-specific alteration of qSOFA by extension with a point for hyponatraemia increases its prognostic performance.
Methods
Setting
The study site was the emergency department (ED) of Bern University Hospital (Inselspital), which is one of the largest hospitals in Switzerland with a catchment area of about 2 million people in the Canton Bern, Switzerland.
Data collection and eligibility criteria
All medical records of all adult patients admitted to our ED between January 1, 2002 and December 31, 2012 were screened with a keyword search of “decompensated liver cirrhosis” with different semantic combinations in the diagnosis or medical history field of our computerised patient database (Qualicare Office, Medical Database Software; Qualidoc AG, Bern, Switzerland). All patients older than 16 years with a primary diagnosis of decompensated liver cirrhosis were considered eligible for inclusion. Only the first presentation with decompensated liver cirrhosis was included in the analysis in case of multiple admissions. Exclusion criteria were as follows: lack of parameters for calculation of the qSOFA score, double entries in our database, patients with chronic decompensated liver cirrhosis, or any other primary reason for ED admission (e. g. trauma). Our study compromises a subset of patients of an already published cohort [22].
Data extraction
Sociodemographic (age, gender), clinical data (aetiology of liver cirrhosis, clinical signs of decompensation such as ascites, haemorrhage, encephalopathy, jaundice, hepatorenal syndrome, vital parameters [first value within an hour from admission], coexistence of hepatocellular carcinoma, concurrent diagnosis of spontaneous bacterial peritonitis), laboratory parameters as well as administrative data (intensive care unit [ICU] admissions, length of hospitalisation, and in-hospital mortality) were analysed. From the available data the Child–Pugh score, the Model of End Stage Liver Disease (MELD) score, the Systemic Inflammatory Response Syndrome (SIRS) criteria, CLIF-C AD score [23] and the qSOFA score were calculated. Additionally, the proportion of patients suffering from acute on chronic liver failure (ACLF) was determined.
Definitions
qSOFA
qSOFA was defined according to the Surviving Sepsis Campaign 2016 [1]. Patients were attributed 1 point for a Glasgow Coma Scale (GCS) of 14 or less, 1 point for a systolic blood pressure of 100 mm Hg or less and respiration rate of 22/min or more.
qSOFA-Na+
Hyponatraemia (defined as 130 mmol/l or lower) in patients with decompensated liver cirrhosis has been linked to increased disease severity and mortality [24,25,26]. The qSOFA was increased by one point for a serum sodium at ED admission of ≤130 mmol/l.
Acute on chronic liver failure
The definitions for acute on chronic liver failure (ACLF) are very heterogeneous and still subject to much discussion [27]. We used a modified version of the CLIF-C ACLF score, a cumulative score for organ failure to define ACLF, to assess for ACLF. Patients with liver failure that did not fulfil one of the following three criteria were considered to have ACLF: (i) no organ failure, (ii) one organ failure (liver coagulation, circulatory, or respiratory) with creatinine <1.5 mg/dL and no hepatic encephalopathy (any grade), (iii) single cerebral failure and creatinine <1.5 mg/dL. In accordance with the CLIF-C ACLF, liver failure was defined as bilirubin levels above 12 mg/dL, and coagulation failure as an INR above 2.5 [28]. The definitions of brain failure, circulatory compromise and respiratory failure were modified as follows: brain failure was defined as the presence of hepatic encephalopathy (any grade), circulation failure as a systolic blood pressure below 90 mm Hg and respiratory failure as SpO2 levels of below 90%.
CLIF-C AD score
A linear combination of age, sodium levels and the logarithms of INR and white blood cells are used to calculate the score [23]. For the purpose of this study, we calculated the CLIF-C AD as a severity marker of the decompensation for all patients independently of the presence of ACLF.
Threshold values
qSOFA, qSOFA-Na+ and SIRS criteria were considered positive when the patient scored two or more points [1]. A MELD score of 25 or higher was considered to be high, where as a MELD score of 24 or lower was considered low [30]. A CLIF-C AD score of 44 or below was defined as low-risk acute decompensation [29].
Ethical considerations
The study was approved by the regional ethics committee of the Canton of Bern, Switzerland (KEK: 14-02-13). Individual informed consent was waived by the ethics committee.
Statistical analysis
Statistical analysis was performed using Stata® 13.1 (StataCorp, College Station, TX, USA). Interval variables are presented as medians with 25th–75th interquartile ranges (IQR). For categorical variables, the total number and respective proportions are given. Comparisons of interval variables between qSOFA-positive and qSOFA-negative groups were performed using the Mann–Whitney U test, and Kruskal–Wallis analysis of variance with post hoc testing using the Mann–Whitney U test. Comparisons of categorical variables between the qSOFA-positive and the qSOFA-negative group were performed by Fisher’s exact test. Predictive value of SIRS, MELD, Child–Pugh score and qSOFA-Na+ were analysed as described for qSOFA. To compare the diagnostic performance of qSOFA and qSOFA-Na+ with regard to in-hospital mortality and need for ICU admission, the equality of the area under the receiver operating curves (AUC) was tested using the roccomp command [31]. A p-value of <0.05 was considered as significant.
Results
Patients’ demographics
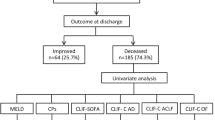
One hundred eighty-six (186) patients were eligible for study inclusion. The CONSORT flow chart is given in Fig. 1. The study population consists of 73.7% male patients with a median age of 57 years (IQR 52–66). Patient characteristics are given in Table 1. The most common aetiology of liver cirrhosis was chronic alcohol consumption (n = 92, 49.5%) followed by of chronic alcohol consumption and hepatitis B infection (n = 38, 20.4%) and hepatitis C infection (n = 20, 10.8%). The median MELD score was 15.1 (IQR 10.8–19.9) and Child–Pugh score C was the most common stage of liver cirrhosis (n = 102, 54.8%). A total of 65 patients (35.0%) were admitted to the ICU and 29 patients (15.6%) died in the hospital. The median duration of hospitalisation was 8 days (IQR 3–14). The percentage of ACLF was 23.3% (n = 37), the median CLIF-C AD score was 54 (IQR 47–61). Of patients with ACLF 54.1% (n = 20) were admitted to the ICU, the median length of hospitalisation was 11 days (IQR 2–20) and 35.1% (n = 13) of the patients died.

CONSORT flow chart. qSOFA quick Sequential Organ Failure Assessment
qSOFA assessment including qSOFA-Na+
The qSOFA score was positive in 22 patients (11.8%). Patients with a positive qSOFA score did not differ significantly with respect to age, aetiology of liver cirrhosis, Child–Pugh classification and MELD score from patients with a negative qSOFA score (p = 0.145, p = 0.770, p = 0.880, respectively p = 0.098, see Table 2).
With respect to our primary and secondary study outcomes the qSOFA score did not discriminate between survivors and nonsurvivors (p = 0.755), ICU admissions (p = 0.152) and length of hospitalisation (p = 0.489). For a comparison between SIRS, Child–Pugh classification, MELD, ACLF, CLIF-C AD and qSOFA with respect to our study outcomes, see Table 3. The MELD score was the only established score to reliably predict ICU admissions (p = 0.007) and in-hospital mortality (p = 0.003) in our patient collective, but not the length of hospitalisation (p = 0.266).
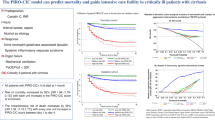
To test whether the addition of sodium to the qSOFA score would increase its predictive power the qSOFA-Na+ score was calculated. qSOFA-Na+ was significantly associated with in-hospital mortality (p = 0.038) and ICU admission (p = 0.001), but not with length of hospitalisation (p = 0.266; see Table 3). The sensitivity and negative predictive value for both (a) ICU admission and (b) in-hospital mortality was increased in qSOFA-Na+ compared to qSOFA without a notable decrease in specificity and positive predictive value (a) ICU admission: sensitivity: 0. 344 vs. 0.169, specificity: 0.875 vs. 0.909, positive predictive value: 0.595 vs. 0.500, negative predictive value: 0.714 vs. 0.671; (b) in-hospital: sensitivity: 0.357 vs. 0.138, specificity: 0.827 vs. 0.885, positive predictive value: 0.270 vs. 0.182, negative predictive value: 0.878 vs. 0.848. The addition of sodium to qSOFA increased its diagnostic performance with regard to ICU admissions (AUCICU qSOFA = 0.504 vs. AUCICU qSOFA-Na+ = 0.609, p = 0.006), but not with respect to in-hospital mortality (AUCdeath qSOFA: 0.513 vs. AUCdeath qSOFA-Na+: 0.592, p = 0.054, see Fig. 2). Adjusting the cut-off for qSOFA-Na+ to 1 point for a sodium level of 125 mmol/l and below, or 120 mmol/l and below did not increase its diagnostic ability (see Fig. 3).

Comparison of qSOFA-Na+ with qSOFA to predict a in-hospital mortality, b ICU admission. qSOFA quick sequential organ failure assessement, ICU intensive care unit

Comparison of qSOFA-Na+ (different cut-offs) with qSOFA to predict a in-hospital mortality, b ICU admission. qSOFA quick sequential organ failure assessement, ICU intensive care unit
Discussion
We present the first study investigating qSOFA in patients with decompensated liver cirrhosis. Despite the similarity in haemodynamic and pathophysiological features to sepsis, qSOFA does not predict mortality, ICU admissions or length of hospitalisation in patients with decompensated liver cirrhosis.
Several studies showed that the qSOFA score is a valuable predictor for in-hospital mortality and length of hospitalisation in patients presenting with suspected infection [2, 5, 6, 12, 14, 32] as well as for the general adult ED patient collective [14]. Whether qSOFA adequately predicts ICU admission in ED patients with suspected sepsis remains controversial [5, 6, 12, 14]. While some studies showed a clear association of qSOFA with ICU admissions [6, 14], others could not confirm these findings [5, 12]. In our study qSOFA was not associated with either in-hospital mortality, ICU admission, or length of hospitalisation. This may highlight that the predictive performance shown for the general adult ED population [14] may not be applicable to a specific subgroup of ED patients. Our hypothesis that the distinct physiological changes in patients with decompensated liver cirrhosis may share a certain similarity to sepsis and therefore qSOFA might have a similar predictive ability remains unconfirmed. Thus, it is possible that the change in mental state due to hepatic encephalopathy may not as gravely influence outcome as the mental alteration in patients with sepsis. This is underlined by the small percentage of patients with spontaneous bacterial peritonitis in our sample when compared to others [33, 34] and therefore the haemodynamic changes and mental alterations probably are mostly attributed to the decompensated liver disease and not due to infection in our study.
In addition, our study sample size is quite small and the predictive ability of qSOFA with regard to our study outcomes may not have become statistically significant. However, our sample had a similar length of hospitalisation and in-hospital mortality rates as others [17, 35, 36], and may therefore well be representative for patients with decompensated liver cirrhosis.
Amongst the already established outcome scores for patients with decompensated liver cirrhosis evaluated in our study, only the MELD score was associated with in-hospital mortality and ICU admission. This finding is not surprising as the MELD score is a highly disease-specific score that was developed to predict mortality in patients after transjugular portosystemic shunt [30] and has been validated for patients with decompensated liver cirrhosis in various studies [37,38,39]. In addition, it has been shown that qSOFA might not be superior when compared to “conventional” outcome scores such as APACHE II or Charlson Comorbidity index for prediction of mortality in patients with sepsis [6, 8, 40].
Surprisingly, however positive SIRS criteria were not associated with in-hospital mortality or ICU admission in our study. Positive SIRS score was clearly linked to outcome in patients with decompensated liver cirrhosis by others [41,42,43] and was equally predictive when compared to the MELD score [43]. On the other hand, a recently published study by Piano and co-workers demonstrated that qSOFA and sepsis-3 criteria were significantly better prognostic factors with respect to mortality than SIRS in patients with decompensated liver cirrhosis and bacterial infections [44]. However, in this trial only patients with a proven or highly suspected bacteria/fungal infection were included and not the general patient presenting with decompensated liver cirrhosis as in our study. Thus, qSOFA seems to be an insufficient screening tool in the overall patient collective with decompensated liver cirrhosis, but may have some strength in patients with decompensated liver cirrhosis and proven infection.
The failure of positive SIRS criteria to adequately predict outcomes in this study is surprising for another reason. Several studies have shown that SIRS criteria are more sensitive, thus less specific than qSOFA [6, 7, 11, 45]; therefore we would have expected SIRS criteria to be a better predictor for outcome in our study than qSOFA. However, both scores attribute one point to a deranged respiratory function (increased rate of breathing). Patients suffering from decompensated liver cirrhosis do not usually exhibit similarly profound changes in respiratory rate as seen in sepsis; therefore it is possible that assessment of respiratory rate is not as valuable for detection of disease severity in patients with decompensated liver disease when compared to patients with sepsis. This might explain why neither qSOFA nor SIRS adequately discriminate between survivors and non-survivors in patients with decompensated liver cirrhosis.
A significant percentage of patients with decompensated liver cirrhosis suffer from hyponatraemia due to volume excess [24,25,26]. Hyponatraemia was linked to increased mortality in patients with decompensated liver cirrhosis in several studies [24,25,26] and a version of the MELD score incorporating sodium as an additional variable showed good predictive ability for outcome in patients with decompensated liver cirrhosis [46,47,48]. Sodium was shown to be an independent predictor for mortality in multivariate analysis in patients with liver disease [46, 47]. It was therefore tempting to create an extended qSOFA by adding a sodium component to the qSOFA score. Taking the presence of hyponatraemia into account to calculate an extended qSOFA score increased its predictive performance with regard to ICU admission and in-hospital mortality. qSOFA-Na+ showed good specificity with a high negative predictive value for in-hospital mortality. However, sensitivity and overall accuracy remained poor. Thus, the extension of qSOFA by a sodium component may add only moderate diagnostic value in outcome prediction in patients with decompensated liver cirrhosis. However, validation is certainly warranted, especially as case numbers in our study were too small to evaluated lower sodium cut-offs. The extension of qSOFA with a disease-specific variable has been investigated by others [3, 7, 8, 49]. The addition of lactate levels to qSOFA did result in an increase in predictive power of qSOFA in patients with suspected infection [3, 7, 8]. However, this increase was only moderate as in our study.
Several others have evaluated an SOFA variation in patients with decompensated liver cirrhosis [50, 51]. A liver specific adaptation of SOFA score (CLIF-SOFA) showed the best AUC for in-hospital mortality when compared to MELD and SOFA in patients with acute on chronic liver disease [51]. A recently published study evaluated a new disease-specific variation of quick CLIF-SOFA including creatinine, bilirubin, INR and vasopressin levels as well a blood pressure criterion (mean arterial pressure below 70 mm Hg) [50]. This test showed good predictive power with respect to in-hospital mortality [50]. However, the calculation of CLIF-SOFA requires extensive laboratory work-up and is therefore not fit for bedside triage.
In conclusion, a disease-specific modification of qSOFA may result in the addition of diagnostic value. However, its usefulness should be further evaluated with careful evaluation of the respective components.
Limitations
Our study is limited by several factors that appear mainly driven by study design. First, our study includes a relatively small sample of patients and therefore the predictive value of qSOFA in patients with decompensated liver cirrhosis could have been missed. A significant percentage of available patients had to be excluded due to the lack of sufficient parameters to calculate qSOFA or incomplete records. Second, this is a retrospective database study; therefore interpretation of data is subject to bias. Third, the proportion of patients suffering from spontaneous bacterial peritonitis is lower in our study when compared to others [33, 34]. It is therefore possible that qSOFA might have predictive value in a population with a higher incidence of spontaneous bacterial peritonitis. Fourth, we only used sodium to extend qSOFA. Other parameters such as lactate levels or base excess as well as adaptions in the cut-off values of the qSOFA score might have more additional value to qSOFA than sodium levels. This should be subject to further investigation. Our study is further limited by our definition of acute on chronic liver failure, due to the retrospective study design with anonymisation of the primary data after data extraction, we were not able to assess for variables such as the grade of hepatic encephalopathy or the need for vasoactive agents to assess qSOFA in specific subgroups of liver failure.
Conclusions
qSOFA does not predict in-hospital mortality, ICU admission or length of hospitalisation in patients with decompensated liver cirrhosis in our study. Unsurprisingly, the MELD score was the best already established scoring system to adequately predict in-hospital mortality in our patient collective. Interestingly, SIRS score was not associated with outcome in this study. The reasons therefor stay elusive. The extension of qSOFA with a disease-specific component, the qSOFA-Na+, significantly increased the predictive ability of qSOFA. The addition of specific disease makers to qSOFA therefore seems tempting; however further validation is certainly needed.
References
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M et al (2016) The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315(8):801–810
Finkelsztein EJ, Jones DS, Ma KC, Pabon MA, Delgado T, Nakahira K et al (2017) Comparison of qSOFA and SIRS for predicting adverse outcomes of patients with suspicion of sepsis outside the intensive care unit. Crit Care 21(1):73
Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A et al (2016) Assessment of clinical criteria for sepsis: For the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315(8):762–774
Churpek MM, Zadravecz FJ, Winslow C, Howell MD, Edelson DP (2015) Incidence and prognostic value of the systemic inflammatory response syndrome and organ dysfunctions in ward patients. Am J Respir Crit Care Med 192(8):958–964
Quinten VM, van Meurs M, Wolffensperger AE, Ter Maaten JC, Ligtenberg JJM (2017) Sepsis patients in the emergency department: Stratification using the Clinical Impression Score, Predisposition, Infection, Response and Organ dysfunction score or quick Sequential Organ Failure Assessment score? Eur J Emerg Med. https://doi.org/10.1097/MEJ.0000000000000460
Kim M, Ahn S, Kim WY, Sohn CH, Seo DW, Lee YS et al (2017) Predictive performance of the quick Sequential Organ Failure Assessment score as a screening tool for sepsis, mortality, and intensive care unit admission in patients with febrile neutropenia. Support Care Cancer 25(5):1557–1562
Henning DJ, Puskarich MA, Self WH, Howell MD, Donnino MW, Yealy DM et al (2017) An emergency department validation of the SEP-3 sepsis and septic shock definitions and comparison with 1992 consensus definitions. Ann Emerg Med 70(4):544–552.e5. https://doi.org/10.1016/j.annemergmed.2017.01.008
Ho KM, Lan NS (2017) Combining quick sequential organ failure assessment with plasma lactate concentration is comparable to standard sequential organ failure assessment score in predicting mortality of patients with and without suspected infection. J Crit Care 38:1–5
Donnelly JP, Safford MM, Shapiro NI, Baddley JW, Wang HE (2017) Application of the third international consensus definitions for sepsis (Sepsis-3) classification: A retrospective population-based cohort study. Lancet Infect Dis 17(6):661–670. https://doi.org/10.1016/S1473-3099(17)30117-2
Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens YE, Avondo A et al (2017) Prognostic accuracy of Sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA 317(3):301–308
Williams JM, Greenslade JH, McKenzie JV, Chu K, Brown AF, Lipman J (2017) Systemic inflammatory response syndrome, quick sequential organ function assessment, and organ dysfunction: Insights from a prospective database of ED patients with infection. Chest 151(3):586–596
Wang JY, Chen YX, Guo SB, Mei X, Yang P (2016) Predictive performance of quick sepsis-related organ failure assessment for mortality and ICU admission in patients with infection at the ED. Am J Emerg Med 34(9):1788–1793
Chen YX, Wang JY, Guo SB (2016) Use of CRB-65 and quick sepsis-related organ failure assessment to predict site of care and mortality in pneumonia patients in the emergency department: A retrospective study. Crit Care (Lond) 20(1):167
Singer AJ, Ng J, Thode HC Jr., Spiegel R, Weingart S (2017) Quick SOFA scores predict mortality in adult emergency department patients with and without suspected infection. Ann Emerg Med 69(4):475–479
Murray CJ, Atkinson C, Bhalla K, Birbeck G, Burstein R, Chou D et al (2013) The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 310(6):591–608
Mokdad AA, Lopez AD, Shahraz S, Lozano R, Mokdad AH, Stanaway J et al (2014) Liver cirrhosis mortality in 187 countries between 1980 and 2010: A systematic analysis. Bmc Med 12:145
Mathur AK, Chakrabarti AK, Mellinger JL, Volk ML, Day R, Singer AL et al (2017) Hospital resource intensity and cirrhosis mortality in United States. World J Gastroenterol 23(10):1857–1865
Alsultan MA, Alrshed RS, Aljumah AA, Baharoon SA, Arabi YM, Aldawood AS (2011) In-hospital mortality among a cohort of cirrhotic patients admitted to a tertiary hospital. Saudi J Gastroenterol 17(6):387–390
Koch A, Trautwein C, Tacke F (2017) Acute liver failure. Med Klin Intensivmed Notfmed 112(4):371–381
Al-Hamoudi WK (2010) Cardiovascular changes in cirrhosis: Pathogenesis and clinical implications. Saudi J Gastroenterol 16(3):145–153
Ferenci P, Lockwood A, Mullen K, Tarter R, Weissenborn K, Blei AT (2002) Hepatic encephalopathy – definition, nomenclature, diagnosis, and quantification: Final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 35(3):716–721
Pfortmueller CA, Wiemann C, Funk GC, Leichtle AB, Fiedler GM, Exadaktylos AK et al (2014) Hypoglycemia is associated with increased mortality in patients with acute decompensated liver cirrhosis. J Crit Care 29(2):316.e7–316.e12
CLIF-C (2017) AD (Acute Decompensation) score and expected mortality rates 2017. https://www.clifresearch.com/ToolsCalculators.aspx
Morales BP, Planas R, Bartoli R, Morillas RM, Sala M, Cabre E et al (2017) Early hospital readmission in decompensated cirrhosis: Incidence, impact on mortality, and predictive factors. Dig Liver Dis 49(8):903–909. https://doi.org/10.1016/j.dld.2017.03.005
Barakat AA, Metwaly AA, Nasr FM, El-Ghannam M, El-Talkawy MD, Taleb HA (2015) Impact of hyponatremia on frequency of complications in patients with decompensated liver cirrhosis. Electron Physician 7(6):1349–1358
Moller S, Krag A, Bendtsen F (2014) Kidney injury in cirrhosis: Pathophysiological and therapeutic aspects of hepatorenal syndromes. Liver Int 34(8):1153–1163
Arroyo V, Jalan R (2016) Acute-on-chronic liver failure: Definition, diagnosis, and clinical characteristics. Semin Liver Dis 36(2):109–116
Jalan R, Saliba F, Pavesi M, Amoros A, Moreau R, Gines P et al (2014) Development and validation of a prognostic score to predict mortality in patients with acute-on-chronic liver failure. J Hepatol 61(5):1038–1047
Jalan R, Pavesi M, Saliba F, Amoros A, Fernandez J, Holland-Fischer P et al (2015) The CLIF Consortium Acute Decompensation score (CLIF-C ADs) for prognosis of hospitalised cirrhotic patients without acute-on-chronic liver failure. J Hepatol 62(4):831–840
Li N, Huang C, Yu KK, Lu Q, Shi GF, Zheng JM (2017) Validation of prognostic scores to predict short-term mortality in patients with HBV-related acute-on-chronic liver failure: The CLIF-C OF is superior to MELD, CLIF SOFA, and CLIF-C ACLF. Medicine (Baltimore) 96(17):e6802
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 44(3):837–845
Forward E, Konecny P, Burston J, Adhikari S, Doolan H, Jensen T (2017) Predictive validity of the qSOFA criteria for sepsis in non-ICU inpatients. Intensive Care Med 43(6):945–946. https://doi.org/10.1007/s00134-017-4776-2
Oladimeji AA, Temi AP, Adekunle AE, Taiwo RH, Ayokunle DS (2013) Prevalence of spontaneous bacterial peritonitis in liver cirrhosis with ascites. Pan Afr Med J 15:128
Rimola A, Garcia-Tsao G, Navasa M, Piddock LJ, Planas R, Bernard B et al (2000) Diagnosis, treatment and prophylaxis of spontaneous bacterial peritonitis: A consensus document. International Ascites Club. J Hepatol 32(1):142–153
Antunes AG, Teixeira C, Vaz AM, Martins C, Queiros P, Alves A et al (2017) Comparison of the prognostic value of Chronic Liver Failure Consortium scores and traditional models for predicting mortality in patients with cirrhosis. Gastroenterol Hepatol 40(4):276–285
Zubieta-Rodriguez R, Gomez-Correa J, Rodriguez-Amaya R, Ariza-Mejia KA, Toloza-Cuta NA (2017) In-hospital mortality in cirrhotic patients at a tertiary care center. Rev Gastroenterol Mex 82(3):203–209. https://doi.org/10.1016/j.rgmx.2016.10.002
Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P et al (2003) Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 124(1):91–96
Lyles T, Elliott A, Rockey DC (2014) A risk scoring system to predict in-hospital mortality in patients with cirrhosis presenting with upper gastrointestinal bleeding. J Clin Gastroenterol 48(8):712–720
Balekian AA, Gould MK (2012) Predicting in–hospital mortality among critically ill patients with end-stage liver disease. J Crit Care 27(6):740 e1–740 e7
Innocenti F, Tozzi C, Donnini C, De Villa E, Conti A, Zanobetti M et al (2017) SOFA score in septic patients: incremental prognostic value over age, comorbidities, and parameters of sepsis severity. Intern Emerg Med 13(3):405–412. https://doi.org/10.1007/s11739-017-1629-5
Das K, Das K, Datta S, Pal S, Hembram JR, Dhali GK et al (2010) Course of disease and survival after onset of decompensation in hepatitis B virus-related cirrhosis. Liver Int 30(7):1033–1042
Cazzaniga M, Dionigi E, Gobbo G, Fioretti A, Monti V, Salerno F (2009) The systemic inflammatory response syndrome in cirrhotic patients: Relationship with their in-hospital outcome. J Hepatol 51(3):475–482
Thabut D, Massard J, Gangloff A, Carbonell N, Francoz C, Nguyen-Khac E et al (2007) Model for end-stage liver disease score and systemic inflammatory response are major prognostic factors in patients with cirrhosis and acute functional renal failure. Hepatology 46(6):1872–1882
Piano S, Bartoletti M, Tonon M, Baldassarre M, Chies G, Romano A et al (2017) Assessment of Sepsis-3 criteria and quick SOFA in patients with cirrhosis and bacterial infections. Gut. pii: gutjnl-2017-314324. https://doi.org/10.1136/gutjnl-2017-314324
Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, Bellomo R et al (2017) Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 317(3):290–300
Chen RC, Wang XD, Dong JZ, Lin Z, Wu JM, Cai YJ et al (2017) A MELD-based nomogram for predicting 3‑month mortality of patients with acute-on-chronic hepatitis B liver failure. Clin Chim Acta 468:195–200
Shi KQ, Cai YJ, Lin Z, Dong JZ, Wu JM, Wang XD et al (2017) Development and validation of a prognostic nomogram for acute-on-chronic hepatitis B liver failure. J Gastroenterol Hepatol 32(2):497–505
Cai YJ, Dong JJ, Dong JZ, Chen Y, Lin Z, Song M et al (2017) A nomogram for predicting prognostic value of inflammatory response biomarkers in decompensated cirrhotic patients without acute-on-chronic liver failure. Aliment Pharmacol Ther 45(11):1413–1426
ffrench-O’Carroll R, Frohlich S, Murphy N, Conlon N (2015) Predictors of outcome in decompensated liver disease: Validation of the SOFA-L score. Ir Med J 108(4):114–116
Zhou XD, Zhang JY, Liu WY, Wu SJ, Shi KQ, Braddock M et al (2017) Quick chronic liver failure-sequential organ failure assessment: An easy-to-use scoring model for predicting mortality risk in critically ill cirrhosis patients. Eur J Gastroenterol Hepatol 29(6):698–705
Sy E, Ronco JJ, Searle R, Karvellas CJ (2016) Prognostication of critically ill patients with acute-on-chronic liver failure using the chronic liver failure-sequential organ failure assessment: A Canadian retrospective study. J Crit Care 36:234–239
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Müller, J. C. Schefold, A. B. Leichtle, D. Srivastava, G. Lindner, A. K. Exadaktylos and C. A. Pfortmueller declare that they have no competing interests.
The study was approved by the regional ethics committee of the Canton of Bern, Switzerland (KEK: 14-02-13). Individual informed consent was waived by the ethics committee.
Additional information
Redaktion
M. Buerke, Siegen
Rights and permissions
About this article

Cite this article
Müller, M., Schefold, J.C., Leichtle, A.B. et al. qSOFA score not predictive of in-hospital mortality in emergency patients with decompensated liver cirrhosis. Med Klin Intensivmed Notfmed 114, 724–732 (2019). https://doi.org/10.1007/s00063-018-0477-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00063-018-0477-z