
Abstract
Hybrid magnetic resonance (MR)-positron emission tomography (MR-PET) is a novel technology with advantages over sequential MR and PET imaging, allowing maintain full individual diagnostic performance with negligible mutual interference between the two hardware settings. Obvious synergies between MR and PET in acquisition of anatomical, functional, and molecular information for neurological diseases into one single image pave the way for establishing clear clinical indications for hybrid MR-PET as well as addressing unmet neuroimaging needs in future clinics and research. Further developments in attenuation correction, quantification, workflow, and effective MR-PET data management might unfold the full potential of integrated multimodality imaging.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Magnetic resonance imaging (MRI) and positron emission tomography (PET) provide valuable metrics to assist in diagnosis and treatment of a wide range of neurological disorders. Obviously, each modality offers advantages and trade-offs in spatial and temporal resolution, signal-to-noise, contrast-to-noise, and ability for quantification of anatomical, physiological, cellular, and molecular events. The newly launched synchronous MR-PET scanners reflect the approaches to accommodate these complementary modalities into one apparatus. The advent of MR-PET, in conjunction with quantitative image synthesis and other important clinical and genetic data, is of paramount importance for the emerging personalized medicine and promises accurate diagnosis, rational targeted therapy, and treatment monitoring on an individual basis.
The article reviews the technical challenges, design, and workflow for the available clinical hybrid MR-PET systems, underpins distinct strengths afforded by synchronous systems, and highlights the key areas where simultaneously acquired MR-PET neuroimaging is anticipated to have a significant impact on clinical and research areas.
Clinical Hybrid MR-PET: Technical Challenges, Design, and Workflow
The key feature of hybrid MR-PET is that PET is not attached to an MRI but resides inside a 3T single gantry system. There are technical challenges when designing a MR-PET imaging system for making it clinically viable. The relatively bulky photomultipliers (PMTs) used to detect the scintillation light in traditional PET systems are not functional in the presence of magnetic field and radiofrequency noise whereas implementation of PET hardware in MR gantry deteriorates the field homogeneity. A decisive leap for the integration of PET into MR was the development of magnetic-field compatible solid-state light detectors, such as avalanche photodiodes (APDs) [1, 2].
Any hybrid MR-PET system is principally affected by suboptimal attenuation correction factors for the emission data as the signal intensity in standard MRI sequences is based on combinations of proton density and tissue relaxation, which are not directly related to electron density and to the linear attenuation coefficients of tissue as in PET-computed tomography (CT). Thus, using MRI metrics for attenuation correction is not straightforward and currently the most popular approach is the segmentation of MR data according to tissue class [3]. The method is robust and is clinically evaluated though its major drawback is the accurate segmentation between bone and air. As cortical bone and air do not provide signal in conventional MRI sequences, solid components of bone are currently not considered in MR attenuation correction. Ultrashort echo time (UTE) or zero echo time sequences are also able to display tissues with very short T2* (e.g., bone) are currently investigated. Thus, information about trabecular and cortical bone may be rendered and subsequently the linear attenuation coefficient (LAC) of bone will be assigned during image segmentation. An extension of segmentation-based methods is based on Dixon fat-water segmentation in which MR images are partitioned into five classes (not including bone) and a linear attenuation coefficient (LAC) is assigned to each of them. In current Dixon-based methods, bone is assigned the LAC of soft tissues during tissue segmentation. This leads to a systematic underestimation of the attenuating effects of cortical bone during MR attenuation correction. Nonetheless, the attenuation correction landscape is constantly evolving and atlas- or template-based methods as well as bone segmentation using ultra-short echo time imaging have been proposed [4].
In terms of workflow, software tools enabling patient-friendly static and dynamic data processing are also meaningful. Last but not least, scan protocol consideration is crucial for the effectiveness of simultaneous imaging in order to maximize the time benefit and tailor the exam to the patients’ needs. Henceforth, scanning recommendations and standardized combined MR-PET protocols for a wide range of neurological diseases would be tremendously helpful [5].
Competitive Advantages of Simultaneous Hybrid MR-PET
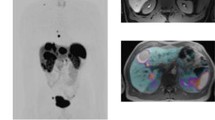
Though it is undoubtedly agreed upon the combination of MRI and PET data in the evaluation of various neurological diseases, the simultaneity of the hybrid imaging is still in debate given the possibility for retrospective, software-based rigid image registration, which is relatively reliable in brain imaging unlikely to motion-related artifacts hampered fused images in body imaging. Body imaging (e.g., pelvic and thoracic regions) may profit from simultaneous MR-PET but there is no evidence supporting its superiority over retrospectively fused PET and MRI in brain pathologies. However, the latter may be operator intensive, especially in cases of uncooperative patients with nonrigid motion artifacts, and the lag time between sequentially performed MR and PET may also be significant for rapidly spatiotemporally evolving pathologies or therapy assessment studies introducing bias in the image interpretation (Fig. 1). Furthermore, simultaneous acquisition facilitates correlation of the tracer kinetics, task-based and resting-state functional data, and the distribution of radiolabeled therapeutics in relation to underlying blood flow, vascular permeability, and proliferation [6].

Retrospective fusion of magnetic resonance (MR) with positron emission tomography (PET) (from PET-computed tomography (CT)) (a) and image fusion after simultaneously acquisition of MR and PET (b) in a patient who underwent fluorodeoxyglucose (FDG) PET-CT and subsequently hybrid MR-PET imaging. The slight co-registration errors near the skull (predominantly on the right side) in (a) are corrected after manual adjustment and iterative co-registration, whereas the MR and PET images from the simultaneous acquisition in (b) show a perfect spatial matching after fusion. (Image courtesy, S. Gatidis, MD, Tübingen)
Being still a maturing field, anatomical MR information (with accurate knowledge of tissue interfaces and boundaries) can be incorporated into the PET image reconstruction process in order to correct the expected different tracer uptake levels in each tissue type and reduce blurring artifacts [6, 7]. The latter is of paramount importance in evaluation of brain cortex pathologies. Gross or periodic head movement may also exacerbate the sometime burdensome retrospective MR-PET image registration. Synchronous MR-PET offers the advantage of MRI-based motion correction of PET data and reveals any obscure lesions while eliminates the erroneous localization of the disease and its quantification in static and dynamic images [8].
The inherent shortcomings of PET in pharmacokinetic modeling, namely moderate spatial and temporal resolution as well as partial volume effect, can partly be overcome by simultaneous MR-PET imaging. MRI provides the necessary anatomic landmarks for region-of-interest (ROI) positioning and captures in high accuracy the time-course of the tracer in the feeding vessel and in the tissue of interest. Partial volume effect may also be tackled by sophisticated methods like correction of the regional interaction between adjacent tissues [6]. The benefits of a hybrid system may be further enhanced by the development of dual-modality contrast agents. Iron oxide nanoparticles are usually tethered to positron emitters and the resulting contrast agents are reported to present improved circulation half-life, organ biodistribution, and selective uptake in target organs, thus allowing for exploration of synergisms between PET and MRI concerning monitor of cell dynamics and viability, receptor imaging, gene expression imaging, and enzyme activity imaging [9, 10]. An interesting application of an MR-PET agent would be the quantification of both concentration (PET-based) and relaxivity (MR-based) enabling to perform absolute quantitative dynamic MRI.
Patient comfort and convenience benefit exclusively from synchronous, “one-stop shop” MR-PET imaging. Patient anxiety and physical discomfort, total scan time, recalls for repeat scans, and risk for motion artifacts in each modality scan are drastically reduced in an integrated MR-PET scanner. In light of the discussion in the next section, if PET and MRI are anticipated to provide complementary information in certain diseases, simultaneous scanning eases extremely the workflow at the stage of the baseline diagnosis and more importantly in assessing treatment response in longitudinal studies. Especially in pediatric population, repeated MR and/or PET scans are notoriously anxiety and stress inducing and minimization of cumulative radiation exposure, arising from serial PET-CT scans, is desired [11]. The competitive advantages of MR-PET in workflow and patient compliance may potentially increase scanner throughput and reduce the related financial burden, which is a crucial economic argument since simultaneous MR-PET units are costly and study reimbursement schemes are still under consideration. Future cost-utility studies should address the diagnostic gain at any costs arising from performing one hybrid exam, though employment of less staff personnel and drastically less patient visits for neuroimaging should be encountered as possible advantages.
Clinical Applications of Hybrid MR-PET Neuroimaging
There are key areas in neuroimaging that may pave the way for identification of meaningful applications of hybrid MR-PET with impact on clinical decision-making, patient management, and potentially patient outcome. The expected benefits should be divided into two distinctive categories: (i) the “low-hanging” benefits, including those that arise from the fusion of the different modalities images, and are palpable in the clinical routine requiring minor studies or validation and (ii) the “high-hanging” benefits that are due to the spatiotemporal co-registration of the functional and molecular data, but for which there is currently a paucity of evidence.
Neuro-oncology
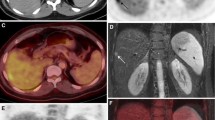
Immediate benefits from hybrid MR-PET comprise improved tumors delineation and staging accuracy opening a highway for “real-time” metabolic imaging in an ideally, economically, and logistically justifiable way [12, 13] (Fig. 2). In that case, the functional and molecular metrics could be an invaluable surrogate to the upcoming classification of brain tumors according to their molecular signature [14]. In the near future, hybrid MR-PET may also contribute substantially in therapy monitoring and in differentiating unspecific therapy-associated changes from tumor recurrence, based on the multiparametric information gained, though software packages allowing a customizable and flexible arrangement of multisequence/multicontrast MR-PET data to ensure true multimodal reading are mandatory. Finally, treatment planning may be immediately benefited by more accurate delineation of the target volume and improved workflow [15–17].

Fluid-attenuated inversion recovery (FLAIR)- (a) and contrast-enhanced T1-weighted (b) images in a patient with seizures and left-sided hemiparesis demonstrate a faintly enhancing tumor mass on the right periventricular white matter crossing the midline. Simultaneously acquired, fused magnetic resonance-positron emission tomography (MR-PET) imaging after injection of 11C-methionine (c) shows an avid uptake of the radionuclide. Metabolic surrogates of tumor activity, such as MR spectroscopy-measured choline, are also elevated in tumor tissue (d). The dynamic susceptibility contrast-enhanced imaging also reveals high blood volume values (e). According to MR-PET criteria, the lesion corresponds to a high-grade tumor and a WHO grade 3 oligoastrocytoma was histopathologically verified.
“High-hanging” benefits in the clinical arena include assessment of the kinetics of labeled drugs and cross calibration of potent tracers between the two modalities as biomarkers for therapy monitoring and survival prognosis, i.e., blood flow/perfusion, permeability/neo-angiogenesis, and metabolic turnover/hypoxia [18, 19]. Characteristic paradigms include MR spectroscopy-measured lactate with 18F-FMISO-PET, arterial spin labeling with H2 15O-PET, and permeability MR-measures with 18F-galacto-RGD. Prerequisites for such outcomes are optimization of PET tracer quantification, as in PET-CT, and awareness of any shortcomings of MR-based techniques, partly due to mutual hardware interface, that might introduce systematic bias. The list of conceivable research topics and clinical applications of MR-PET in neuro-oncology is extensive and the reader is directed to a comprehensive review in this topic [20].
Neurodegeneration
Applications of MR-PET imaging in neurodegenerative disorders are likely to expand with dementia being the paradigm of harmonic synergism between MR and PET. These “low-hanging” benefits are expected to arise directly from the hybrid contrast. Specifically, amyloid PET imaging allows assessment of amyloid plaques and early risk stratification for Alzheimer disease during its insidious onset, whereas exquisite high-resolution anatomical MRI increases the specificity of the PET-based diagnosis and permits the differentiation from other dementias (Fig. 3) [21]. Noteworthy to be mentioned is that similar scenario exists for parkinsonism. Here, fluorine-18 fluorodeoxyglucose (18F-FDG)-PET allows discrimination between primary Parkinson disease and atypical parkinsonian syndromes, as major glucose consumption deficits only being found in the latter. Specifically, Parkinson’s disease presents with increased glucose metabolism and cerebral blood flow in the basal ganglia and cerebellum, and concurrently reduced metabolism and flow in other areas of the cerebral cortex [22]. This spatial covariance pattern has a disease progression-dependent consistency. Automated analysis of these spatial covariance patterns may result in a high specificity in identifying Parkinson’s disease (PD) and differentiating it from other akinetic-rigid disorders, such as multiple system atrophy (MSA) and progressive supranuclear palsy (PSP) [23]. Other PET tracers that target different components of dopaminergic transmission, including presynaptic dopamine function, dopamine-receptor binding, and dopamine release and turnover, are gaining acceptance [22]. High-resolution anatomical MRI, currently employed to detect specific atrophy patterns for different atypical parkinsonian syndromes, might be enriched by voxel-based morphometry and emerging methods to detect and quantify white matter fiber and structural connectivity decline (DTI), as well as iron accumulation (susceptibility-weighted imaging, T2* relaxometry), for example, in midbrain or striatal areas [24]. Tantalizingly, exploratory work on DTI is provisionally promising for differentiating PD from atypical parkinsonian syndromes by demonstrating reductions in fractional anisotropy (FA) and elevations in mean diffusivity (MD) in the cerebellum, pons, and cerebellar peduncles as means of distinguishing MSA from PD and also perhaps PSP. Infratentorial regional anisotropy and diffusivity changes were found in MSA, but these changes were absent in PD. Finally, the putamen also showed FA alterations and increased diffusivity in MSA compared with PD or controls [25].

Simultaneously acquired, fused magnetic resonance-positron emission tomography (MR-PET) imaging after injection of fluorine-18 fluorodeoxyglucose (18F-FDG) (a) and 11C- Pittsburgh compound B (PiB) (b) in a 68-year-old male patient having increasing declining memory performance during the last 3 years with development of stuttering speech and slow gait. Since 8 months, the patient developed visual and acoustical hallucinations, too. FDG-PET revealed decreased glucose metabolism in the parieto-temporal and occipital cortex including the visual cortex, whereas increased FDG-metabolism was observed in the basal ganglia. Non-pathological amyloid-β deposition thus excluding Alzheimer disease was shown on Pittsburgh compound B (PIB)-PET scan. After MR-PET imaging, the patient was diagnosed with Lewy body dementia
In future, not only the baseline diagnosis will be improved but also this will ultimately benefit any treatment approaches, accounting for the development of neuroprotective or neurorestorative medications. It is presumed that resting-state functional magnetic resonance imaging (fMRI) studies can be added to PET imaging, diffusion tensor imaging, and arterial spin labeling (also as surrogate to 18F-FDG tracer) to elucidate transmitter release, receptor affinity and metabolism in connected areas as substrates of networks connectivity in neurodegenerative diseases [26, 27]. Overall, it is clear that hybrid MR-PET can provide more convenience to these patients who are often elderly and may not tolerate repeated and long imaging sessions [28].
Epilepsy
PET (mostly using 18F-FDG) and MRI have been separately used and extensively searched for localization of epileptogenic foci and preoperative workup of intractable seizures. The synergy for improving diagnosis and patient outcome is uncontroversial and is established by retrospective image fusion for such clinical questions. Integrated MR-PET clearly offers the opportunity to surpass shortcomings of each technique such as lack of metabolic/functional information in MRI and obscured metabolic abnormality in radionuclide imaging due to low resolution [29]. Moreover, integrated MR-PET offers exact anatomical co-registration, compensation of any motion correction, segmentation of grey and white matter for metabolic activity atlases and patient convenience (Fig. 4). Apart from these ready for the clinical practice implementations of hybrid imaging, the possibility of temporospatially accurate correlation between PET data with MR-detected patterns of neural synchrony in grey and white matter (e.g., resting-state fMRI), diffusion tensor imaging, arterial spin labeling, and MR spectroscopy is intriguing and under current investigation [30]. A useful add-on would be the integration of surface electroencephalographic (EEG) real-time recording, resulting in trimodal imaging technique.

Simultaneously acquired, fused MR-PET imaging after injection of 18F-FDG (a) in this patient with focal epileptic seizures shows interictal hypometabolic cortical structures in the left central region. Arterial spin labeling imaging (b) shows hyperperfusion in the suspected focus and the surrounding region presumably due to early postictal discharges
Outlook
MR-PET is a required and valuable adjunct to modern healthcare and there is likely to be indications for mainstream placement in neurological patients. Regulatory requirements, training, and credentialing requirements for image interpretation, comparative effectiveness against sequential imaging, cost-utility, and study reimbursement are still open issues. Nonetheless, the hybrid MR-PET will hasten the verge of personalized medicine and subsequently the need for development of efficient methods for intelligent spatiotemporal analysis of the vast multi-parameter imaging data.
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
References
Judenhofer MS, Wehrl HF, Newport DF, Catana C, Siegel SB, Becker M, Thielscher A, Kneilling M, Lichy MP, Eichner M, Klingel K, Reischl G, Widmaier S, Röcken M, Nutt RE, Machulla HJ, Uludag K, Cherry SR, Claussen CD, Pichler BJ. Simultaneous PET-MRI: a new approach for functional and morphological imaging. Nat Med. 2008;14(4):459–65.
Zaidi H, Del Guerra A. An outlook on future design of hybrid PET/MRI systems. Med Phys. 2011;38(10):5667-89.
Keereman V, Mollet P, Berker Y, Schulz V, Vandenberghe S. Challenges and current methods for attenuation correction in PET/MR. Magma. 2013;26(1):81–98.
Hofmann M, Bezrukov I, Mantlik F, Aschoff P, Steinke F, Beyer T, Pichler BJ, Schölkopf B.MRI-based attenuation correction for whole-body PET/MRI: quantitative evaluation of segmentation- and atlas-based methods. J Nucl Med. 2011;52(9):1392-9.
Vargas MI, Becker M, Garibotto V, Heinzer S, Loubeyre P, Gariani J, Lovblad K, Vallée JP, Ratib O. Approaches for the optimization of MR protocols in clinical hybrid PET/MRI studies. Magma. 2013;26(1):57–69.
Yankeelov TE, Peterson TE, Abramson RG, Izquierdo-Garcia D, Arlinghaus LR, Li X, Atuegwu NC, Catana C, Manning HC, Fayad ZA, Gore JC. Simultaneous PET-MRI in oncology: a solution looking for a problem? Magn Reson Imaging. 2012;30(9):1342–56.
Shidahara M, Tsoumpas C, Hammers A, Boussion N, Visvikis D, Suhara T, Kanno I, Turkheimer FE. Functional and structural synergy for resolution recovery and partial volume correction in brain PET. NeuroImage. 2009;44(2):340–8.
Tsoumpas C, Mackewn JE, Halsted P, King AP, Buerger C, Totman JJ, Schaeffter T, Marsden PK. Simultaneous PET-MR acquisition and MR-derived motion fields for correction of non-rigid motion in PET. Ann Nucl Med. 2010;24(10):745–50.
Hoehn M, Himmelreich U, Kruttwig K, Wiedermann D. Molecular and cellular MR imaging: potentials and challenges for neurological applications. J Magn Reson Imaging. 2008;27(5):941–54.
Lee HY, Li Z, Chen K, Hsu AR, Xu C, Xie J, Sun S, Chen X. PET/MRI dual-modality tumor imaging using arginine-glycine-aspartic (RGD)-conjugated radiolabeled iron oxide nanoparticles. J Nucl Med. 2008;49(8):1371–9.
Schäfer JF, Gatidis S, Schmidt H, Gückel B, Bezrukov I, Pfannenberg CA, Reimold M, Ebinger M, Fuchs J, Claussen CD, Schwenzer NF. Simultaneous whole-body PET/MR imaging in comparison to PET/CT in pediatric oncology: initial results. Radiology. 2014;273(1):220–31.
Bisdas S, Ritz R, Bender B, Braun C, Pfannenberg C, Reimold M, Naegele T, Ernemann U. Metabolic mapping of gliomas using hybrid MR-PET imaging: feasibility of the method and spatial distribution of metabolic changes. Invest Radiol. 2013;48(5):295–301.
Gempt J, Soehngen E, Förster S, Ryang YM, Schlegel J, Zimmer C, Meyer B, Ringel F, Grams AE, Förschler A. Multimodal imaging in cerebral gliomas and its neuropathological correlation. Eur J Radiol. 2014;83(5):829–34.
Weller M, Pfister SM, Wick W, Hegi ME, Reifenberger G, Stupp R. Molecular neuro-oncology in clinical practice: a new horizon. Lancet Oncol. 2013;14(9):e370–9.
Seeger A, Braun C, Skardelly M, Paulsen F, Schittenhelm J, Ernemann U, Bisdas S. Comparison of three different MR perfusion techniques and MR spectroscopy for multiparametric assessment in distinguishing recurrent high-grade gliomas from stable disease. Acad Radiol. 2013;20(12):1557–65.
la Fougere C, Suchorska B, Bartenstein P, Kreth FW, Tonn JC. Molecular imaging of gliomas with PET: opportunities and limitations. Neuro-oncology. 2011;13(8):806–19.
Thorwarth D, Henke G, Müller AC, Reimold M, Beyer T, Boss A, Kolb A, Pichler B, Pfannenberg C. Simultaneous 68Ga-DOTATOC-PET/MRI for IMRT treatment planning for meningioma: first experience. Int J Radiat Oncol Biol Phys. 2011;81(1):277–83.
Furtner J, Bender B, Braun C, Schittenhelm J, Skardelly M, Ernemann U, Bisdas S. Prognostic value of blood flow measurements using arterial spin labeling in gliomas. PloS One. 2014;9(6):e99616.
Jansen NL, Suchorska B, Wenter V, Eigenbrod S, Schmid-Tannwald C, Zwergal A, Niyazi M, Drexler M, Bartenstein P, Schnell O, Tonn JC, Thon N, Kreth FW, la Fougère C. Dynamic 18F-FET PET in newly diagnosed astrocytic low-grade glioma identifies high-risk patients. J Nucl Med. 2014;55(2):198–203.
Bisdas S, Nägele T, Schlemmer HP, Boss A, Claussen CD, Pichler B, Ernemann U. Switching on the lights for real-time multimodality tumor neuroimaging: the integrated positron-emission tomography/MR imaging system. AJNR Am J Neuroradiol. 2010;31(4):610–4.
Nasrallah IM, Wolk DA. Multimodality imaging of Alzheimer disease and other neurodegenerative dementias. J Nucl Med. 2014;55(12):2003–11.
Stoessl AJ, Martin WW, McKeown MJ, Sossi V. Advances in imaging in Parkinson’s disease. Lancet Neurol. 2011;10(11):987–1001.
Tang CC, Poston KL, Eckert T, Feigin A, Frucht S, Gudesblatt M, Dhawan V, Lesser M, Vonsattel JP, Fahn S, Eidelberg D. Differential diagnosis of parkinsonism: a metabolic imaging study using pattern analysis. Lancet Neurol. 2010;9(2):149–58.
Barthel H, Schroeter ML, Hoffmann KT, Sabri O. PET/MR in dementia and other neurodegenerative diseases.Semin Nucl Med. 2015;45(3):224–33.
Cochrane CJ, Ebmeier KP. Diffusion tensor imaging in parkinsonian syndromes: a systematic review and meta-analysis. Neurology. 2013;80(9):857–64.
Felicio AC, Shih MC, Godeiro-Junior C, Andrade LA, Bressan RA, Ferraz HB. Molecular imaging studies in Parkinson disease: reducing diagnostic uncertainty. Neurologist. 2009;15(1):6–16.
Griffa A, Baumann PS, Thiran JP, Hagmann P. Structural connectomics in brain diseases. NeuroImage. 2013;80:515–26.
Jadvar H, Colletti PM. Competitive advantage of PET/MRI. Eur J Radiol. 2014;83(1):84–94.
Ding YS, Chen BB, Glielmi C, Friedman K, Devinsky O. A pilot study in epilepsy patients using simultaneous PET/MR. Am J Nucl Med Mol Imaging. 2014;4(5):459–70.
Storti SF, Boscolo Galazzo I, Del Felice A, Pizzini FB, Arcaro C, Formaggio E, Mai R, Manganotti P. Combining ESI, ASL and PET for quantitative assessment of drug-resistant focal epilepsy. Neuroimage. 2014;102(Pt 1):49–59.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bisdas, S., lá Fougere, C. & Ernemann, U. Hybrid MR-PET in Neuroimaging. Clin Neuroradiol 25 (Suppl 2), 275–281 (2015). https://doi.org/10.1007/s00062-015-0427-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00062-015-0427-6