
Abstract
Introduction
The aim of this study was to three-dimensionally analyze the net skeletal, dental, and temporomandibular joint (TMJ) treatment changes using Twin Block functional therapy in comparison to untreated subjects.
Materials and methods
The study (Twin Block) group comprised 22 female patients with skeletal Class II malocclusion due to mandibular retrusion. A total of 18 skeletal Class II untreated female subjects were included as controls. Skeletal, dental, and TMJ changes were evaluated using pre- and posttreatment/observational by cone beam computed tomography (CBCT) images. The treatment changes were compared with the growth changes observed in the control group using independent t‑tests.
Results
Compared to the changes induced by normal growth, the effective mandibular length, ramus, and corpus lengths increased by 3.19, 3.47, and 2.69 mm (P < 0.001 for all), respectively. The maxillary and mandibular incisors inclination and position were significantly reduced and increased, respectively (P < 0.001). The maxillary first molars were significantly moved distally and intruded by 1 and 0.36 mm, respectively, while the lower first molars moved mesially and intruded by 2.18 and 0.59 mm, respectively. There was a significant change in the condylar dimensions: increase in length, width, and height by 1.28, 0.88, 1.59 on the right and by 1.60, 0.53, and 1.10 mm on the left sides, respectively. There was significant forward positioning of the right and left condyle by 1.5 and 1.3 mm, respectively.
Conclusions
Treatment with the Twin Block functional appliance results in significant skeletal, dentoalveolar, and condylar changes in both dimensions and positions.
Zusammenfassung
Einleitung
Ziel der Studie war die Untersuchung skelettaler, dentaler und temporomandibulärer Veränderungen nach einer Twin-Block-Therapie im Vergleich mit einer unbehandelten Kontrollgruppe.
Material und Methoden
Die Interventionsgruppe (Twin Block) umfasste 22 Patientinnen mit skelettaler Klasse-II-Malokklusion und Unterkieferrücklage. 18 unbehandelte Klasse-II-Patientinnen dienten als Kontrollgruppe. Skelettale, dentale und temporomandibuläre Veränderungen wurden anhand von DVT-Aufnahmen evaluiert, die vor und nach Behandlung bzw. während der Behandlung angefertigt worden waren. Mittels t‑Tests für unabhängige Stichproben wurden die behandlungs- bzw. die wachstumsbedingten Veränderungen in der Interventions- und der Kontrollgruppe miteinander verglichen.
Ergebnisse
Im Vergleich mit den Veränderungen, die sich wachstumsbedingt ergeben haben, erhöhten sich die effektive Unterkieferlänge sowie die Längen von Ramus und Corpus mandibulae um 3,19, 3,47 bzw. 2,69 mm (p < 0,001 für alle). Inklination und Position der Oberkieferinzisivi verringerten sich signifikant (p < 0,001), Inklination und Position der Unterkieferinzisivi erhöhten sich dagegen signifikant (p < 0,001). Die ersten Molaren im Oberkiefer wurden signifikant um 1,0 bzw. 0,36 mm distalisiert und intrudiert, während die unteren ersten Molaren um 2,18 bzw. 0,59 mm mesialiert und intrudiert wurden. Es gab signifikante Veränderungen an den Kondylen: Länge, Breite und Höhe vergrößerten sich um 1,28, 0,88 bzw. 1,59 auf der rechten und um 1,60, 0,53 bzw. 1,10 mm auf der linken Seite. Auf beiden Seiten kam es zu einer signifikanten Vorverlagerung der Kondylen um 1,5 (rechts) bzw. 1,3 mm (links).
Schlussfolgerungen
Die Behandlung mit einem Twin-Block-Funktionsgerät führte zu signifikanten skelettalen, dentoalveolären und temporomandibulären Veränderungen.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Class II malocclusion is commonly seen in orthodontic practice [26]. It causes esthetic, functional, and psychological disturbances of varying intensity. The severity of this malocclusion depends on the amount of anteroposterior discrepancy and its interaction with the related soft tissue structures. Patients with Class II Division 1 malocclusion can exhibit maxillary protrusion, mandibular retrusion, or a combination thereof, together with abnormal dental relationship and facial esthetic disorders [13, 23].
Mandibular retrognathism is a main contributor to Class II malocclusion [19], which necessitates the use of advancement or functional appliances. These appliances are designed to enhance and/or redirect the growth in a favorable direction [25].
Over the last 10 years, the Twin Block functional appliance developed by William J. Clark [8] has been the most popular functional appliance. Several clinical studies [5, 8, 16, 18, 20, 22, 24, 29, 30, 32, 33, 35] have been conducted to assess skeletal and dentoalveolar changes associated with Twin Block functional appliance therapy in Class II malocclusion. Concerning skeletal effects, some authors demonstrated a significant influence on mandibular growth [29, 33], while others [18, 24] claimed that it induced dentoalveolar changes with minimal skeletal effects.
A recently conducted systematic review [10] analyzed the effect produced by the Twin Block appliance concluded that it was not possible to analyze the effect of growth on the reported changes due to the limited data available. These studies were based on two-dimensional evaluation using lateral cephalometry with its intrinsic limitations that result in distorted images, enlarged in some areas and reduced in others, superimposition and inaccurate landmark localization [12]. On the other hand, recent systematic reviews [1, 14] investigated the effect of functional appliances on the temporomandibular joint (TMJ) found that there is a forward condylar positioning and remodeling but with minimally detailed results because the published three-dimensional study was either a pilot study [17] using class II elastics as a control group or a retrospective uncontrolled study [37].
The aim of this study was to three-dimensionally analyze the net skeletal, dental, and TMJ treatment changes using Twin Block functional therapy by cone beam computed tomography (CBCT) with a comparable control group of untreated subjects.
Materials and methods
This clinically controlled study conducted at the outpatient clinic of the Department of Orthodontics was approved by the Research Ethics Committee (1/13-8-2011), Faculty of Oral and Dental Medicine, Cairo University, Egypt. All patients’ parents were informed about the study procedures and informed written consents was obtained.
Sample size was calculated with an alpha value of 0.05 and a power of 90% based on the study conducted by Toth and McNamara [32]. They reported mean changes of Co-Gn (mandibular unit length) in the Twin Block group (5.7 ± 2.4 mm) and in the control group (2.7 ± 1.5 mm). Power analysis showed a minimum sample of 11 patients in each group.
The inclusion criteria were as follows: (1) females with a chronological aged between 10–13 years, (2) convex profile with retruded mandible, (3) ≥½ unit Class II molar and canine relationship, (4) overjet ≥5 mm, (5) skeletal age: stage 3 cervical vertebrae maturational indicators (CVMI) [5], (6) vertical growth pattern as verified clinically by steep mandibular plane, (7) no history of orthodontic treatment, (8) no history or clinically diagnosed TMJ disorders, and (9) free from any systemic disease or chronic medication use.
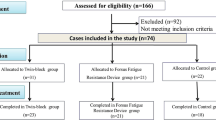
Based on the above criteria, 22 patients were included in the treatment group. CBCT images of 18 untreated clinically matching control patients were obtained from a control databank created by three research projects in the same institute [11]. All subjects in the control group were orthodontically treated after completion of the observational period.
All patients were scanned with CBCT to obtain detailed three-dimensional osseous evaluations of the TMJ and more accurate skeletal and dental measurements, while the control group data were obtained from the control databank of the institute. CBCT images were obtained using the commercially available Sirona GALILEOS CBCT machine (Sirona Dental Systems, Bensheim, Germany). Parameters of the CBCT scanner were set according to the recommendations of De Vos et al. [9] and provided a minimal set of CBCT device-related parameters to minimize the radiation dose to the minimum.
The treatment group subjects were treated with a standard Twin Block appliance according to Clark [8]. The patients were instructed to wear the appliance 24 h/day, especially during mealtimes and they were followed once every 4 weeks. The anteroposterior dental arch relationship was checked with and without the appliance during each appointment. When no difference existed and the mandible could not be retruded, the active treatment period was then finished, retention period started with the appliance for another 3 months. The functional phase lasted for 9.4 ± 1.33 months and the observational period for the control group was 8.12 ± 2.72 months.
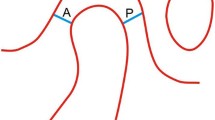
The skeletal, dentoalveolar, and temporomandibular (Fig. 1) three-dimensional landmarks (Table 1) were identified in CBCT images using Anatomage image processing software version 5.01. The skeletal, dentoalveolar, and temporomandibular (Fig. 2) three-dimensional measurements (Table 2) were obtained for all patients before the start of treatment (T0) and after the functional phase period (T1) in the treatment group and at the beginning (T0) and after 8 months (T1) of observation in the control group. Three-dimensional temporomandibular analysis was performed according to Alhammadi et al. [2,3,4], the intra- and interobserver reliability errors were analyzed by retracing CBCT projects 3 weeks after the first measurement.


Three dimensional temporomandibular joint measurements: a sagittal, b coronal, c axial views. See Table 2 for explanation of numbers. VP vertical plane, MSP midsagittal plane, FHP Frankfort horizontal plane
Dreidimensionale Messungen am Kiefergelenk: a sagittale, b koronale, c axiale Sicht. Erläuterungen der Ziffern s. Tab. 2. VP vertikale Ebene, MSP Midsagittale, FHP Frankforter Horizontale
Statistical analysis
Statistical analysis was performed with SPSS* Statistics Version 21 (IBM Corp., Armonk, NY, USA). Paired samples t‑test was used to study the changes after treatment and observation period for all variables within the same group. Comparison of the change between the patients and control groups was carried out by independent samples t‑test. Interobserver and intraobserver reliability analysis was carried out by concordance correlation coefficient (CCC).
Results
The Twin Block and control groups comprised 18 participants each. In the treatment group, four patients dropped out at different times: two disappeared after the first month of treatment, one discontinued due to the psychological trauma upon using the appliance, one patient stopped using the appliance after five months of improved facial profile. There was a significant clinical improvement of the soft tissue profile, molars and canines’ relation, overjet, and overbite.
Intra- and interobserver reliability tests showed an excellent concordance correlation (0.903–0.970). Mean and standard deviation (SD) values of all skeletal, dental, and TMJ outcomes in starting form of the Twin Block/control group are presented in Tables 3 and 4, respectively. Mean and SD values of pre- and posttreatment and pre- and postobservational measurements of both groups are listed in Tables 5 and 6. The mean changes and differences between both groups for the same outcomes are presented in Tables 7 and 8.
Tables 3 and 4 showed that both groups are almost similar in the starting form with no significant differences between them except for four skeletal (AB diff (NV), PFH, Ag-Ag, and MP/SN) and three dental (LI-Nv, U6/FHP°, and LR6-LL6) measurements.
Compared to the changes induced by normal growth, Table 7 showed a net significant increase in both linear and angular anteroposterior facial profile measurements as indicated by ANB°, A‑B diff Nv (P ≤ 0.001), and increase in the vertical facial profile measurements as demonstrated by AFH (P ≤ 0.05) and PFH (P ≤ 0.001), and subsequently the jarabak ratio; S‑Go/N-Me (P ≤ 0.001).
The sole effect of the Twin Block on the maxillary base showed that there were no statistically significant changes in vertical position, effective maxillary length, maxillary base tipping, and maxillary base width. There was a significant increase in the palatal plane length (ANS-PNS) and minimal reduction in linear anteroposterior position of point A (P ≤ 0.01).
Comparison of the two groups showed that the net treatment effect on the mandibular base indicated that there was significant movement in anteroposterior position by 1.53°, 1.87 mm (P < 0.001 for all) as showed by SNB and both Nv-B and Nv-Pg, respectively. Similarly, the mandibular effective length, ramus length, and corpus length increased significantly by 3.19, 3.47, and 2.69 mm (P < 0.001 for all), respectively. The vertical mandibular position, mandibular width, and mandibular plane inclination were not affected.
Regarding the dentoalveolar effects, compared to the minimal changes induced by normal growth, the maxillary incisors inclination and position were significantly reduced (P < 0.001) by 7.98° and 2.57 mm, respectively. The mandibular incisor inclination and position was significantly increased by 3.32° and 1.82 mm, respectively. The net effect of the Twin Block showed that both overjet and overbite were significantly decreased by 4.89 and 2.11 mm, respectively. The maxillary first molars were significantly (P < 0.001) moved distally and intruded by 1 and 0.36 mm, respectively, while the lower first molars moved mesially and intruded by 2.18 and 0.59 mm, respectively.
Results of the net effect of the Twin Block on the osseous TMJ components and joint spaces presented in Table 8 that showed a significant change in the condylar dimensions (increase in length, width, and height by 1.28, 0.88, 1.59 on the right and by 1.60, 0.53, and 1.10 mm on the left sides, respectively). There was significant forward positioning of the right and left condyle by 1.5 and 1.3 mm, respectively. This dimensional and positional change of the condyles results in a net decrease of the anterior (0.77 and 0.84 mm in the right and left side, respectively) and medial joint spaces (0.65 mm and 0.67 in the right and left side, respectively) and a net increase of the posterior (0.80 and 1.11 mm in the right and left side, respectively) and superior joint spaces (0.79 and 0.90 mm in the right and left side, respectively).
Discussion
All subjects who participated in the study were females. This is to rule out the gender effect as the mandibular growth was clearly sex and age dependent [27].
The excellent concordance correlation between intra- and interobserver reliability measurements indicated high and precise landmark identification with CBCT that cannot be obtained by another conventional modality used for assessment of the complex temporomandibular region. Regarding the craniofacial changes, the present study showed that the Twin Block appliance produced an orthopedic effect in both anteroposterior and vertical directions. This presented by improvement in the facial profile by reduction in both anteroposterior linear and angular measurements. This was emphasized by the cephalometric studies of Lund and Sandler [18], Mills and McCulloch [20], Trenouth [34] and Sharma et al. [29], and the three-dimensional study of Yildirim et al. [37].
The facial profile was improved by reduction in the vertical pattern of growth mainly in the expense of increase in the posterior facial height three times than that of the anterior facial height. These findings were not in accordance with those stated by Mills and McCulloch [21]. They found that the mandibular plane angle and the anterior facial height were significantly increased in the Twin Block group more than the control group. They used the classical Twin Block appliance design without any modification specific for the vertical facial type patients.
There was a minimal restriction of maxillary forward growth that could be explained by the distal reciprocal force exerted on the maxilla (headgear effect) by the appliance. This finding was in accordance with the cephalometric studies [29, 31] and the three-dimensional study of Yildirim et al. [37]; others found no effect on the maxillary base [15, 28].
The significant net increase in the mandibular effective length (Co-Gn, 3.19 mm) must be emphasized. This increase was a net result of an increase in both ramal (3.47 mm) and body length (2.96 mm). The overall mandibular skeletal changes could be attributed to the increase in mandibular length by 3.19 mm and the change in mandibular position by 1.53°, 1.87 and 1.87 mm based on SNB, B‑Nv and Pg-Nv, respectively. The reported increase in the current study was greater than the increase produced by Twin Block appliance as reported in randomized clinical trials (RCTs) and controlled clinical trials (CCT) included in a recent systematic review [10]. The vertical mandibular position, mandibular width, and mandibular plane inclination were not affected.
Most of the effect on the maxilla was dentoalveolar due to the headgear effect of the incorporated labial arch in the upper block. These resulted in palatal tipping of the maxillary incisors by 7.98° and displacement by 2.57 mm. The opposite effect occurred for the mandibular incisors as they tipped and displaced labilally as those teeth are a part of the anchorage of the appliance with its inherent backward force. These incisors findings were in accordance with studies reported by Lund and Sandler [18], Mills and McCulloch [20, 21] and Jena et al. [15, 16]. Both skeletal and dentoalveolar effects were responsible for correction of both overjet and overbite.
The study group showed significant forward migration of the mandibular first molars accompanied with the backward migration of the maxillary first molars. This reciprocal migration of the molars could be attributed to the forward mandibular posturing effect of the appliance and its reciprocal backward on the maxilla, which is consistent with previously reported results [15, 16, 18, 20, 21, 29].
To date, almost no three-dimensional detailed dimensional and positional study has assessed the effect of the Twin Block appliance on the mandibular condyle which is considered as a growth site of the mandible and plays an important role in the final adult dimension of the mandible. In this study, a detailed three-dimensional analysis was used to evaluate this complex area. The net treatment effect of the Twin Block appliance showed forward displacement of the condyles relative to the vertical plane and this attributed to the forward posturing of the mandible by the appliance. This finding was in agreement with the finding reported by the cephalometric study of Baccetti et al. [5], the CBCT study of Liu et al. [6] and an MRI study by Chavan et al. [7].
Regarding the dimensional effect on the condyle, there was a more significant increase in the condylar length, width, and height on both sides by an average of 1.45 mm, 0.7 mm, and 1.35 mm, respectively. A recent uncontrolled study assessing the effect of the Twin Block appliance of the condylar volume showed a significant volume increase of 347 mm3 in the left and 273 mm3 in the right condyles. This increase gives an indication of three-dimensional increase of the condylar dimension [36].
Regarding evaluation of the mandibular joint spaces, a more significant increase in the superior and posterior joint spaces was observed, while there was a significant decrease in the anterior and medial joint spaces. This could be explained by the normal sequence of the anterior and inferior movement of the condyle by forward positioning of the mandible by the appliance.
Conclusions
-
Twin Block appliance therapy increase dimensions of mandibular condyle in the three planes of space and reposition toward a more forward position.
-
Increased posterior and superior and decreased anterior and medial joint spaces are another indication of anterior and inferior positioning of the condyle.
-
Significant improvement of the skeletal profile in anteroposterior and vertical direction; most of these changes were due to an increase in the effective mandibular, ramus, and corpus lengths and increase in posterior facial height, respectively.
-
Palatal displacement of maxillary incisors, labial displacement of mandibular incisors, forward migration of the mandibular first molars, and backward migration of the upper molars were responsible for correction of overjet and molar relation, respectively.
References
Al-Saleh M, Alsufyani N, Flores-Mir C, Nebbe B, Major P (2015) Changes in temporomandibular joint morphology in class II patients treated with fixed mandibular repositioning and evaluated through 3D imaging: a systematic review. Orthod Craniofac Res 18:185–201
Alhammadi M, Fayed M, Labib A (2017) Three-dimensional assessment of condylar position and joint spaces after maxillary first premolar extraction in skeletal class II malocclusion. Orthod Craniofac Res 20:71–78
Alhammadi MS, Fayed MS, Labib A (2016) Three-dimensional assessment of temporomandibular joints in skeletal class I, class II, and class III malocclusions: cone beam computed tomography analysis. J World Fed Orthod 5:80–86
Alhammadi MS, Shafey AS, Fayed MS, Mostafa YA (2014) Temporomandibular joint measurements in normal occlusion: a three-dimensional cone beam computed tomography analysis. J World Fed Orthod 3:155–162
Baccetti T, Franchi L, Toth LR, McNamara JA (2000) Treatment timing for twin-block therapy. Am J Orthod Dentofacial Orthop 118:159–170
Bowen L, Yanmin W, Fang S, Min L, Ying D, Li Z (2013) Cone-beam CT evaluation of the changes in the temporomandibular joint of patients with class II division 1 subdivision malocclusion before and after Twin-block treatment. Hua Xi Kou Qiang Yi Xue Za Zhi 31:610–614
Chavan SJ, Bhad WA, Doshi UH (2014) Comparison of temporomandibular joint changes in twin block and bionator appliance therapy: a magnetic resonance imaging study. Prog Orthod 15:57
Clark W (2014) Twin block functional therapy. JP Medical Ltd, London
De Vos W, Casselman J, Swennen G (2009) Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: a systematic review of the literature. Int J Oral Maxillofac Surg 38:609–625
Ehsani S, Nebbe B, Normando D, Lagravere MO, Flores-Mir C (2014) Short-term treatment effects produced by the twin-block appliance: a systematic review and meta-analysis. Eur J Orthod 37:170–176
Elkordy SA, Abouelezz AM, Salah Fayed MM, Attia KH, Rahman Ishaq RA, Mostafa YA (2015) Three-dimensional effects of the mini-implant—anchored forsus fatigue resistant device: a randomized controlled trial. Angle Orthod 86:292–305
Gribel BF, Gribel MN, Frazão DC, McNamara JA Jr, Manzi FR (2011) Accuracy and reliability of craniometric measurements on lateral cephalometry and 3D measurements on CBCT scans. Angle Orthod 81:26–35
Henry R (1957) A classification of class II, division I malocclusion. Angle Orthod 27:83–92
Ivorra-Carbonell L, Montiel-Company J‑M, Almerich-Silla J‑M, Paredes-Gallardo V, Bellot-Arcís C (2016) Impact of functional mandibular advancement appliances on the temporomandibular joint—a systematic review. Med Oral Patol Oral Cir Bucal 21:e565–e572
Jena AK, Duggal R, Parkash H (2005) Orthopedic and orthodontic effects of twin-block appliance. J Clin Pediatr Dent 29:225–230
Jena AK, Duggal R, Parkash H (2006) Skeletal and dentoalveolar effects of twin-block and bionator appliances in the treatment of class II malocclusion: a comparative study. Am J Orthod Dentofacial Orthop 130:594–602
LeCornu M, Cevidanes LH, Zhu H, Wu C‑D, Larson B, Nguyen T (2013) Three-dimensional treatment outcomes in class II patients treated with the Herbst appliance: a pilot study. Am J Orthod Dentofacial Orthop 144:818–830
Lund DI, Sandler PJ (1998) The effects of twin blocks: a prospective controlled study. Am J Orthod Dentofacial Orthop 113:104–110
Jr McNamara JA (1981) Components of class II malocclusion in children 8–10 years of age. Angle Orthod 51:177–202
Mills CM, McCulloch KJ (1998) Treatment effects of the twin block appliance: a cephalometric study. Am J Orthod Dentofacial Orthop 114:15–24
Mills CM, McCulloch KJ (2000) Posttreatment changes after successful correction of class II malocclusions with the twin block appliance. Am J Orthod Dentofacial Orthop 118:24–33
Morris DO, Illing HM, Lee RT (1998) A prospective evaluation of bass, Bionator and twin block appliances. Eur J Orthod 20:663–684
Moyers RE, Riolo ML, Guire KE, Wainright RL, Bookstein FL (1980) Differential diagnosis of class II malocclusions: part 1. Facial types associated with class II malocclusions. Am J Orthod 78:477–494
O’Brien K, Wright J, Conboy F, Sanjie Y, Mandall N, Chadwick S, Connolly I, Cook P, Birnie D, Hammond M (2003) Effectiveness of early orthodontic treatment with the twin-block appliance: a multicenter, randomized, controlled trial. Part 1: dental and skeletal effects. Am J Orthod Dentofacial Orthop 124:234–243
Pinheiro F (2015) Twin block functional therapy: applications in dentofacial orthopedics. Am J Orthod Dentofacial Orthop 147:636
Proffit WR, Fields H Jr, Moray L (1997) Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg 13:97–106
Ruf S, Baltromejus S, Pancherz H (2001) Effective condylar growth and chin position changes in activator treatment: a cephalometric roentgenographic study. Angle Orthod 71:4–11
Saikoski LZ, Cançado RH, Valarelli FP, KMSd F (2014) Dentoskeletal effects of class II malocclusion treatment with the twin block appliance in a Brazilian sample: a prospective study. Dental Press J Orthod 19:36–45
Sharma A, Sachdev V, Singla A, Kirtaniya B (2012) Skeletal and dentoalveolar changes concurrent to use of twin block appliance in class II division I cases with a deficient mandible: a cephalometric study. J Indian Soc Pedod Prev Dent 30:218–226
Sidlauskas A (2005) The effects of the twin-block appliance treatment on the skeletal and dentolaveolar changes in class II division 1 malocclusion. Medicina (Kaunas) 41:392–400
Singh G, Hodge M (2002) Bimaxillary morphometry of patients with class II division 1 malocclusion treated with twin block appliances. Angle Orthod 72:402–409
Toth LR, McNamara JA (1999) Treatment effects produced by the twin-block appliance and the FR-2 appliance of Fränkel compared with an untreated class II sample. Am J Orthod Dentofacial Orthop 116:597–609
Trenouth M (2000) Cephalometric evaluation of the twin-block appliance in the treatment of class II division 1 malocclusion with matched normative growth data. Am J Orthod Dentofacial Orthop 117:54–59
Trenouth M (2002) Proportional changes in cephalometric distances during twin block appliance therapy. Eur J Orthod 24:485–491
Varlık SK, Gültan A, Tümer N (2008) Comparison of the effects of twin block and activator treatment on the soft tissue profile. Eur J Orthod 30:128–134
Vedavathi H, Chirag A (2016) Comparative assessment of condylar changes in patients treated with twin block appliance: a cone-beam computed tomography study. J Dent Med Sci (IOSR-JDMS) 15:1–7
Yildirim E, Karacay S, Erkan M (2014) Condylar response to functional therapy with twin-block as shown by cone-beam computed tomography. Angle Orthod 84:1018–1025
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H.Y. Elfeky, M.S. Fayed, M.S. Alhammadi, S.A.Z. Soliman and D.M. El Boghdadi declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Elfeky, H.Y., Fayed, M.S., Alhammadi, M.S. et al. Three-dimensional skeletal, dentoalveolar and temporomandibular joint changes produced by Twin Block functional appliance. J Orofac Orthop 79, 245–258 (2018). https://doi.org/10.1007/s00056-018-0137-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-018-0137-1
Keywords
- Class II malocclusion
- Functional orthopedic appliance
- Twin Block
- Temporomandibular joint
- Cone beam computed tomography