
Abstract
Objectives
To review and describe available Knowledge Translation (KT) strategies that are designed for or applied in public health decision-making settings.
Introduction
KT is the exchange, synthesis, and ethically sound application of knowledge. This review proposes that KT strategies in public health settings should be understood as action plans that promote evidence use and facilitate evidence-informed decision-making.
Methods
This scoping review included studies that reported on KT strategies applied in public health settings, published between 2010 and 2017. Studies were searched using Medline, online KT database, and citation tracing. Data from 305 included studies were synthesized using a coding form and conceptually mapped to identify KT strategies used in public health settings.
Results
A total of 124 unique examples of KT methods or tools were identified and summarized into 38 recommended and promising KT strategies. Built on the lists of recommended strategies, this review synthesized a framework that matched all 38 KT strategies to 10 key components of the evidence-informed decision-making process.
Conclusions
The public health KT strategies summarized and organized by this review promote a better understanding and more effective use of KT strategies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Public health practice and policy should be based on the best available evidence (Jacobs et al. 2012). Yet, there is a knowledge-to-action (KTA) gap between “what is known” and “what is currently done” (Davis et al. 2003; Grol and Grimshaw 2003; Grol and Jones 2000). In recent years, investigators have adopted comprehensive and solution-driven approaches focusing on developing strategies to minimize the KTA gap in public health action. The term action is used because it is broader than the concept of practice. “action” encompasses both public health practice and policy, thus involves various types of knowledge use by different stakeholders (Field et al. 2014; Graham et al. 2006).
“Knowledge Translation” is the terminology developed to describe specific strategies and solutions to bridge the KTA gap (CIHR 2004). The Canadian Institutes for Health Research (CIHR) coined the term “Knowledge Translation (KT)” to capture the interactive steps between the creation of new knowledge and its application to bring about public polices with positive health impact for society. CIHR defined KT as: “the exchange, synthesis and ethically sound application of knowledge—within a complex system of interactions among researchers and users—to accelerate the capture of the benefits of research for Canadians” (CIHR 2004). KT models the bridging of KTA gap as an interactive process, potentially involving many different steps and various stakeholders (CIHR 2004). In recent years, the term “Knowledge Translation (KT)” has increased in importance and use in the fields of public health and medicine (CIHR 2004; Glasgow et al. 2003; Jacobson et al. 2003; Rogers et al. 2009).
In the context of evidence-informed public health, decision-makers recognize that it is essential to consider evidence in the context of the public health problems of concern (Bowen and Zwi 2005). In this context, the ultimate objective of KT should be to facilitate evidence-informed decision-making (EIDM) and to help integrate a spectrum of evidence into public health practice and policy (Armstrong et al. 2011). EIDM is thus defined as “distilling and disseminating the best available evidence from research, context and experience, and using that evidence to inform and improve public health practice and policy” (Ciliska et al. 2008a). According to the Canadian NCCMT, the public health EIDM process could be outlined in terms of seven decisions: (1) define the public health problem; (2) access to and search for evidence; (3) appraise the quality of evidence; (4) synthesize & select evidence; (5) adapt evidence to public health practices or to the local context; (6) implement the adapted evidence; and (7) evaluate the effectiveness of implementation efforts (Ciliska et al. 2008b).
This scoping review aims to provide a review of the literature on KT strategies used in the context of evidence-informed public health decision-making. This review describes and summarizes available KT strategies that are designed for and/or applied in public health decision-making settings. And this review attempts to outline how each of the identified KT strategy contributes to the decision-making of the public health EIDM process, in order to provide a guide for selection of KT strategies. To achieve these review aims, the scoping review methodology is ideal because it allows for flexibility in the definition of KT terms, accommodates a wide range of study designs and methods, and can help to develop a better understanding of the nature and scope of KT in public health settings (Munn et al. 2018). This review is not intended to be a comprehensive review of what KT strategies are tested or shown effective in public health settings. Instead, this review aims to examine previously reported public health KT strategies, carefully interpret their usefulness in the context of public health EIDM process, and disseminate this information to public health decision-makers (Bailey et al. 2015; Munn et al. 2018).
Methods
Review question
This scoping review used the “SPIDER” (sample, phenomenon of interest, design, evaluation, research type) tool to define review question (Table 1) (Methley et al. 2014). Using the PICO (Population, Intervention, Comparison, Outcome) tool as a starting point, the SPIDER tool has been created to develop effective search strategies of quantitative, qualitative, and mixed-methods research (Cooke et al. 2012).
Search strategy
Search strategies for this scoping review were developed based on previous research of KT-related terminology. Researchers have used many different terms to describe KT (Colquhoun et al. 2014). For instance, an inventory of KT-related terms identified over a hundred different terms to describe KT research, including “implementation science,” “quality improvement,” “dissemination,” etc. (McKibbon et al. 2013). McKibbon and colleagues found more than 90 terms used to describe use of research, and have identified terms that could KT articles from non-KT articles in all papers (McKibbon et al. 2010). LaRocca and colleagues also tested the usefulness of many KT-related terms in their 2012 systematic review of public health KT strategies (LaRocca et al. 2012).
Given the large number of potential search terms for KT, this scoping review carefully selected search terms that (1) were found to specifically discriminate KT articles from non-KT articles in all papers (McKibbon et al. 2010), and (2) were proven to be broad enough to comprehensively capture all KT-related concepts (LaRocca et al. 2012). Literature search was conducted in MEDLINE® using these highly discriminatory KT terms (detailed search strategy presented in Supplement S1). Search results were limited to English language only. The 2012 systematic review by LaRocca and colleagues comprehensively evaluated the effectiveness of public health KT strategies reported in randomized control studies published up to 2010 (LaRocca et al. 2012). In order to build upon this review, we expanded the scope for study designs and focused all literature searches between 2010 and 2017. The last search was executed on December 16, 2017.
The online KT database (KT + available at: http://plus.mcmaster.ca/kt/) was also searched using these search terms: community health, public health, and disease prevention. “Reference mining” or “citation tracing” were also conducted using the reference lists of included studies and reviews. Studies published before 2010 could be identified and included through “citation tracing” if they (1) meet eligibility criteria and (2) are not included in the 2012 systematic review by LaRocca and colleagues (LaRocca et al. 2012).
Study selection
This scoping review included any study that met the predefined “SPIDER” (sample, phenomenon of interest, design, evaluation, research type) criteria (Methley et al. 2014). For title and abstract screening, the review team intentionally set a broad review eligibility criteria. Specifically, we included any reports of the exchange, synthesis, and appropriate application of knowledge in any public health settings. Using this one-line eligibility criteria as a guide, all reviewers conducted a pilot screening of the same 200 articles. Based on the screening discrepancies of these 200 articles, the reviewers discussed the nuances of the eligibility criteria and translated the one-line eligibility criteria into a bullet list:
-
1.
Include studies that reported Knowledge Translation (KT) strategy. We defined KT strategy as activities or processes that are designed to support knowledge creation and synthesis, knowledge contextualization, knowledge application, monitoring and evaluation, and sustaining of knowledge use. We defined knowledge as evidence used in public health decision-making settings, mainly including three kinds: (1) Research evidence, specifically, “information derived from evaluation research that has assessed the effects and outcomes of potential [public health] interventions and programs” (Rychetnik et al. 2004); (2) Surveillance data (the state of health status of the targeted population) and evaluation results; (3) Community needs assessments and other local context data.
-
2.
Include studies that reported KT strategies that are applied in public health settings. We defined “public health setting” as non-healthcare focused settings where public health, “the science and art of preventing disease, prolonging life, and promoting health through organized efforts of society” (Nutbeam 1986; Smith et al. 2006), is practiced. Thus, we focused on settings where the main activities were focused on achieving disease prevention and not settings that included treatment services.
-
3.
Include a variety of study designs, e.g., randomized control trials, stepped wedge trial, before-after study, time series analysis, mixed-method study, qualitative study, narrative review, systematic review, mixed-method review, scoping review, theory studies, and formal report.
-
4.
Include studies that reported KT strategies that are directed toward any public health decision-makers or any stakeholders in a population health setting, with their focus being primary or secondary prevention of a disease.
-
5.
Include studies that reported KT strategies designed for federal or state policymakers, public health practitioners, social workers, and health professionals.
-
6.
Include studies that reported KT strategies designed to translate research evidence, surveillance data, evaluation results, community needs assessments, or other local context data.
-
7.
Exclude studies that reported on KT of healthcare research, or studies of KT strategies designed to be applied in a disease treatment setting.
The first two bullet points of this detailed eligibility criteria outlined the most important eligibility criteria for our review question. During the study selection process, we used bullet points 1 and 2 to select studies first, and then used bullet points 3 through 7 to refine study selection. Using this detailed eligibility criteria as guide, We selected studies through three stages: first, title and abstract screening of all search results; second, full-text screening of all included abstracts; and lastly, citation tracking of studies included after full-text screening. The main reviewer (NZ) screened all of the titles and abstracts. Serving as the second screener, two research assistants applied the eligibility criteria to 30% of all titles and abstracts identified from the literature search. During double independent screening, we iteratively discussed study selection and resolved discrepancies as a group. Team discussions focused on important distinctions about several key concepts relevant to the eligibility criteria, including “public health settings,” “knowledge,” and “KT.” A detailed description of what was considered as KT, evidence, and public health setting is provided in Supplementary file S2. All title and abstract screening was completed in the open-source, online software Abstrackr (http://abstrackr.cebm.brown.edu/). For all abstracts that were deemed potentially relevant, full-text articles were retrieved. The main reviewer read and screened all full-text articles. And finally, after full-text screening was completed, we conducted “citation tracing” using the reference lists of included studies and reviews.
Data items and data extraction process
Given the complex and diverse range of literature identified from the search, this scoping review employed an exploratory approach to prioritize articles for more detailed data extraction. After the completion of full-text screening, the included studies were used for prioritized data extraction. A standardized data extraction form was first developed after reviewing 20 included studies. Then, two reviewers performed pilot data extraction of 30 studies using this form and discussed the results. To enhance the form’s relevance to KT strategies, we revised the data extraction form to include key elements from a KT intervention reporting framework. In 2012, an international working group defined an overarching reporting framework for KT interventions (Colquhoun et al. 2014). This reporting framework functioned as a guide to “think about” KT strategies. Our data extraction form included four elements from this KT reporting framework: “intervention strategies and techniques (active ingredients), how they function (causal mechanisms), how they are delivered (mode of delivery), and what they aim to change (intended targets)” (Colquhoun et al. 2014).
We used the final data extraction form to extract key characteristics from each included full-text study and study included from citation tracing. Based on the extracted data, we also categorized all studies into one of four groups: (1) conceptual: studies that outlined theory and framework of KT; (2) case studies: studies that reported the use of KT in a specific public health setting; (3) review: systematic review, narrative review, and scoping review of KT in sectors related to public health; (4) interventions: studies that tested the effectiveness of KT methods and strategies used in public health settings.
Synthesis of results
We drew lessons from critical interpretive synthesis (CIS), an approach described by Dixon-Woods et al. (Dixon-Woods et al. 2006), to synthesize the data extracted from all included studies. The CIS method is an iterative process that begins with identifying a “compass question,” which is eventually answered by the search results (Dixon-Woods et al. 2006). CIS focuses on developing “synthetic constructs” to interpret the review results and to transform the review findings into a new conceptual form (Dixon-Woods et al. 2006). This synthesis method has been proven useful in other KT review (Malla et al. 2018). Instead of conducting a formal CIS, we adopted the principles of CIS to our results synthesis, and aimed to answer this “compass question”: “How is knowledge/evidence used by public health practitioners and policy-makers to better support evidence-informed decision-making in public health settings?” For our purpose, each public health EIDM decision (define, search, appraise, synthesize & select, adapt, implement, and evaluate (Ciliska et al. 2008b)) served as the initial “synthetic constructs.” Using the completed data extraction form, we summarized the key information for each included study and the KT strategy this study reported, including these domains: KT strategy active ingredients, causal mechanisms, mode of delivery, and intended targets (Colquhoun et al. 2014). Studies reporting on similar KT strategies were then categorized into the same type. We then attempted to map the unique KT strategy types to an initially defined “synthetic construct.” During this process, we also decided whether new “synthetic construct,” or additional decisions important for the public health EIDM process, were needed. We first tested this process with 20 articles. Supplementary file S2 shows the specific types of KT strategies summarized from the included studies, and shows which included study was aligned with each type of KT strategy and how each type of strategy was mapped to a public health EIDM decision. We used the PRISMA-ScR Checklist as a guide for final results reporting (Tricco et al. 2018).
Reliability and validity
To guard against main reviewer’s subjectivity, two research assistants double-screen 30% of all titles and abstracts (Babbie 1998). Reliability issues are closely associated with subjectivity (Golafshani 2003). The inclusion and exclusion criteria of this scoping review were also improved as reviewers held regular meetings to discuss disagreements. Threats to validity were minimized as this review built its search strategies on the basis of existing reviews and studies of KT terms (LaRocca et al. 2012; McKibbon et al. 2010, 2013).
Results
Study selection
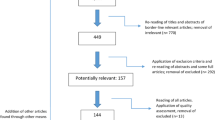
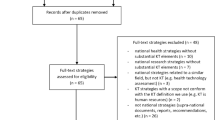
Comprehensive literature searches yielded a total of 11,075 references (see Fig. 1 for a summary of the review process). About one-third of all abstracts were double-screened with remaining abstracts single-screened. Total 876 potentially relevant full-text articles were included. Full texts of all 876 studies were then reviewed and finally 121 studies were included for data extraction. During data extraction process of these 121 studies, citation tracking identified another 184 relevant studies that met inclusion criteria. A final collection of 305 included studies was compiled and synthesized in this scoping review.

Flowchart outlining the study search and selection process in this scoping review of public health Knowledge Translation strategies
Study characteristics
A variety of KT studies were included: randomized control trials, clustered randomized trials, mixed-method studies, qualitative studies, reviews, and case studies (Table 2). Most KT strategies targeted individual decision-makers, while some papers reported on KT strategies designed for public health organizations, local health departments, and local governments. A few studies reported on KT strategies applied in a global health context (Table 2).
Results synthesis
For all the studies included after full-text screening, data were extracted to capture the essence of KT strategies reported. Using a structured data extraction form, we summarized characteristics of identified KT strategies from all included studies. A total of 124 unique examples of KT strategies or tools were identified in this scoping review. We then summarized these examples into 38 recommended and promising KT strategies. We mapped each identified KT strategy and example to the seven decisions of the evidence-informed public health decision-making process (Ciliska et al. 2008b): (1) Define the public health problem; (2) Access to and search for evidence; (3) Appraise the quality of evidence; (4) Synthesize & select evidence; (5) Adapt evidence to public health practices or to the local context; (6) Implement the adapted evidence; and (7) Evaluate the effectiveness of implementation efforts. During this mapping process, we decided that three new “synthetic constructs,” or three additional decisions important for the public health EIDM process, were needed: (1) Building individual and organizational capacity for evidence-informed public health decision-making; (2) Using evidence to promote evidence-informed decision-making in public health policy; and (3) Promoting two-way knowledge exchange between of public health knowledge producers and public health decision-makers. Together, these ten public health decisions illustrate the usefulness of KT strategies in public health settings (Table 3). We mapped the recommended KT strategies and unique KT examples to these ten decisions (Table 4, Supplement S3). Table 4 outlines our organization of available public health KT strategies and could be used to guide the selection of KT strategies in public health settings.
The summary of KT strategies and examples in Table 4 and Supplement S3 revealed some important overall themes. First of all, many of the identified KT strategies are designed to facilitate the use of knowledge during a specific step of the evidence-informed public health decision-making process. In this context, KT strategies are often used to improve research-driven knowledge utilization, especially the use of evidence-based public health programs and interventions. In this context of supporting general knowledge use, relevant and credible research must first be synthesized. Credible synthesis methods include systematic review and meta-analysis, narrative reviews, government agency evidence reports, and knowledge brokerage organization’s recommendation reports. Decision-makers also need to select the knowledge that will address the problem of their interest. Decision-makers also need to adapt the knowledge to their local context. End-users need to have the appropriate skills to identify, critically evaluate, and apply research-driven knowledge for decision-making. Monitoring and measuring the impact of knowledge use is also important to support the use of knowledge in decision-making. And finally, organizational support and culture are key to sustain knowledge use. Supportive organizational culture and sufficient capacity are needed for researchers and end-users to engage in KT activities.
Secondly, some identified KT strategies are relevant for all steps of the evidence-informed decision-making process. They either help build overall capacity for evidence-informed decision-making, or facilitate the making of public health policies, or support the two-way exchange of knowledge between knowledge users and producers. These KT strategies either target to change individual behaviors of public health decision-makers, or to target change at the level of organizational systems and public policies. In this context, many KT strategies are used to support evidence-informed policymaking in both local and national levels. And in the context of evidence-informed policymaking, knowledge use is a more complex and negotiated process. Policymaking involves the consideration of competing influences, including values and beliefs of policymakers and many external influences. If amplified by the appropriate KT strategies, research-driven knowledge in public health could play a broad and transformative role in every step of the health-related policymaking process. For instance, in local government settings, KT strategies can increase evidence use and consequently help generate new ideas for policy and give voice to under-represented groups.
Discussion
This scoping review identified 124 unique examples of KT methods or tools and summarized 38 recommended and promising KT strategies applied in public health settings, through analyzing 305 included studies. KT in public health aims to ensure that the best available knowledge is used to inform public health practice and policy. This review summarized key point from each identified KT strategy and then mapped each KT strategy to decisions important for the public health EIDM process. Such organization provides a guide to KT strategy selection and help to support more effective use of KT strategies, thus better ensure that decision-makers at all levels of the public health system are aware of and use research-driven knowledge to inform public health decision-making.
This study’s organization of KT examples and strategies could provide decision-makers with a better understanding of how KT strategies vary according to the targeted user audience (e.g., policymaker, program manager), strategy application settings (e.g., developed countries vs. developing countries), and the type of knowledge being translated (e.g., epidemiological, behavioral). Public health practice and policymaking is rarely a linear or completely rational process. We cannot assume that one KT strategy will work in all circumstances and be best for all decision-makers. The organized table of KT strategies can provide a road map for public health decision-makers to navigate their selection of KT strategy and to plan specific KT activities. For instance, suppose a local public health department plans to conduct community-based obesity intervention in a township with high obesity prevalence. They could use appropriate KT strategies to select evidence-based program, and then use strategies such as Intervention Mapping (IM) or holding stakeholder consensus workshops to increase the selected program’s fit with their local context.
Findings of this review are not relevant to KT in the healthcare or other disease treatment settings. Rather, this review fills a gap in providing comprehensive reviews examining potential applications of KT strategies in public health. To date, the existing systematic reviews of KT strategies have primarily focused on KT strategies in public health decision-making settings reported by quantitative studies. The Cochrane Collaborations published a protocol in 2011 for a large-scale systematic review of KT strategies in public health, intended to capture a larger variety of study designs (Armstrong et al. 2011). One systematic review conducted a comprehensive search of KT in public health settings (LaRocca et al. 2012); however, the synthesis focused solely on randomized control trials of KT strategies, thus resulting in a small number of included studies. Instead of just focusing on quantitative studies, this scoping review covers a wide range of study designs, and can help to develop a better understanding of the nature and scope of KT in public health settings (Munn et al. 2018).
This study also points out a need for future research to provide more assessment on KT strategy effectiveness. For example, in a recent scoping review, Strifler et al. (2018) identified 159 KT theories, models, or frameworks (Strifler et al. 2018). However, 60% of the identified theories, models, or frameworks were only tested in one study, providing very limited evidence base for these KT strategies’ effectiveness (Strifler et al. 2018). If more effectiveness information is made available, the strategy examples identified by this scoping review could potentially be ranked according to an order of effectiveness, making the organization tables more useful for public health decision-makers.
Unlike a systematic review, this scoping review could not provide quality assessment of included studies. In addition, given the large variety of terminology used to describe KT in the published literature, there is potential for misclassification of KT strategies. This review limited search to English language articles only. And due to the large number of returned hits, this study was not able to expand its primary search effort beyond Medline, nor was able to have more than one researcher work on all abstract screening, full-text screening, and data extraction. However, the scoping review methodology allowed this study to cover a broadly defined search question and include all study types in study selection. During the study selection and data extraction process, this study was able to help clarify many key concepts important for KT in public health settings. The concept definitions, search terms, and study eligibility criteria used in this study could all serve as precursor to a future systematic review. Another strength of this scoping review is how it charted all data relevant to KT strategy in public health settings according to key decisions of the public health evidence-informed decision-making process, providing a useful tool for public health decision-makers. By utilizing the scoping review methodology, this study found that KT strategies in public health should be viewed as action plans designed to promote use of evidence in public health decision-making settings. This review provided a guide for the selection of KT strategy in public health settings to promote a better understanding of and more effective use of KT strategies, and to ensure that the best available knowledge is used to inform public health policy and practice.
List of abbreviations
Knowledge-to-action (KTA)
The gap between “what is known” and “what is currently done” in practice settings (Davis et al. 2003; Grol and Grimshaw 2003; Grol and Jones 2000). The term action denotes a generic concept encompassing various types of knowledge use by different stakeholders.
Knowledge Translation (KT)
As defined by the Canadian Institutes for Health Research (CIHR), Knowledge Translation is “the exchange, synthesis and ethically sound application of knowledge-within a complex system of interactions among researchers and users-to accelerate the capture of the benefits of research for Canadians” (CIHR 2004).
Evidence-informed decision-making (EIDM)
“The process of distilling and disseminating the best available evidence from research, context and experience, and using that evidence to inform and improve public health practice and policy” (Armstrong et al. 2011; Bowen and Zwi 2005).
KT framework
A framework of Knowledge Translation outlines the basic structure underlying this concept and could be used to help its end-users to better understand Knowledge Translation.
NCCMT
National Collaborating Centre for Methods and Tools (Canada).
References
Armstrong R, Waters E, Dobbins M, Lavis JN, Petticrew M, Christensen R (2011) Knowledge translation strategies for facilitating evidence‐informed public health decision making among managers and policy‐makers. Cochrane Database of Systematic Reviews
Babbie ER (1998) The practice of social research, vol 112. Wadsworth Publishing Company, Belmont
Bailey J, Mann S, Wayal S, Hunter R, Free C, Abraham C, Murray E (2015) Scoping review methodology. In: Sexual health promotion for young people delivered via digital media: a scoping review. NIHR Journals Library
Bowen S, Zwi AB (2005) Pathways to “evidence-informed” policy and practice: a framework for action. PLoS Med 2:e166
Cihr C (2004) Knowledge translation strategy 2004–2009: innovation in action. Canadian Institutes of Health Research, Ottawa
Ciliska D, Thomas H, Buffett C (2008a) A compendium of critical appraisal tools for public health practice links
Ciliska D, Thomas H, Buffett C (2008b) An introduction to evidence-informed public health and a compendium of critical appraisal tools for public health practice. National Collaborating Centre for Methods and Tools, Ontario
Colquhoun H, Leeman J, Michie S et al (2014) Towards a common terminology: a simplified framework of interventions to promote and integrate evidence into health practices, systems, and policies. Implement Sci 9:781
Cooke A, Smith D, Booth A (2012) Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res 22:1435–1443
Davis D, Davis ME, Jadad A et al (2003) The case for knowledge translation: shortening the journey from evidence to effect. BMJ 327:33–35
Dixon-Woods M, Cavers D, Agarwal S et al (2006) Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med Res Methodol 6:1–13
Field B, Booth A, Ilott I, Gerrish K (2014) Using the knowledge to action framework in practice: a citation analysis and systematic review. Implement Sci 9:172
Glasgow RE, Lichtenstein E, Marcus AC (2003) Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am J Public Health 93:1261–1267
Golafshani N (2003) Understanding reliability and validity in qualitative research. Qual Rep 8:597–606
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, Robinson N (2006) Lost in knowledge translation: time for a map? J Contin Educ Health Prof 26:13–24
Grol R, Grimshaw J (2003) From best evidence to best practice: effective implementation of change in patients’ care. Lancet 362:1225–1230
Grol R, Jones R (2000) Twenty years of implementation research. Fam Pract 17:S32–S35
Jacobs JA, Jones E, Gabella BA, Spring B, Brownson RC (2012) Peer reviewed: tools for implementing an evidence-based approach in public health practice. Preventing chronic disease 9
Jacobson N, Butterill D, Goering P (2003) Development of a framework for knowledge translation: understanding user context. J Health Serv Res Policy 8:94–99
LaRocca R, Yost J, Dobbins M, Ciliska D, Butt M (2012) The effectiveness of knowledge translation strategies used in public health: a systematic review. BMC Public Health 12:751. https://doi.org/10.1186/1471-2458-12-751
Malla C, Aylward P, Ward P (2018) Knowledge translation for public health in low-and middle-income countries: a critical interpretive synthesis. Glob Health Res Policy 3:1–12
McKibbon KA, Lokker C, Wilczynski NL et al (2010) A cross-sectional study of the number and frequency of terms used to refer to knowledge translation in a body of health literature in 2006: a Tower of Babel? Implement Sci 5:16
McKibbon KA, Lokker C, Keepanasseril A, Colquhoun H, Haynes RB, Wilczynski NL (2013) WhatisKT wiki: a case study of a platform for knowledge translation terms and definitions—descriptive analysis Implementation. Science 8:13
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S (2014) PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res 14:579
Munn Z, Peters MD, Stern C, Tufanaru C, McArthur A, Aromataris E (2018) Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 18:143
Nutbeam D (1986) Health promotion glossary. Health Promot Int 1(1):113–127
Rogers JD, Martin FH, Force NKTT (2009) Knowledge translation in disability and rehabilitation research: lessons from the application of knowledge value mapping to the case of accessible currency. J Disabil Policy Stud 20:110–126
Rychetnik L, Hawe P, Waters E, et al (2004) A glossary for evidence based public health. J Epidemiol Community Health 58:538–545
Smith BJ, Tang KC, Nutbeam D (2006) WHO health promotion glossary: new terms. Health Promot Int 21:340–345
Strifler L, Cardoso R, McGowan J et al (2018) Scoping review identifies significant number of knowledge translation theories, models, and frameworks with limited use. J Clin Epidemiol 100:92–102
Tricco AC, Lillie E, Zarin W et al (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med 169:467–473
Acknowledgements
The authors thank Zhuxuan Fu and Jian Shi for serving as second screener for some of the articles.
Author information
Authors and Affiliations
Contributions
N.Z., S.K.W., A.L., and M.C. contributed to study concept and design. N.Z. finalized the search strategy and completed data acquisition and cleaning. N.Z. and M.C. interpreted the data. N.Z. drafted the manuscript. S.K.W., A.L., and M.C. provided valuable input and revised the manuscript. M.C. provided funding for research assistants’ time. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
None.
Financial support
This work was completed as part of N.Z.’s DrPH dissertation, which received stipend support from the Department of Public Health and Community Medicine, at Tufts University School of Medicine.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the section “Knowledge synthesis, translation and exchange.”
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Zhao, N., Koch-Weser, S., Lischko, A. et al. Knowledge translation strategies designed for public health decision-making settings: a scoping review. Int J Public Health 65, 1571–1580 (2020). https://doi.org/10.1007/s00038-020-01506-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-020-01506-z