
Abstract
Objectives
To assess the relationship between paid work, family characteristics and health status in Central American workers; and to examine whether patterns of association differ by gender and informal or formal employment.
Methods
Cross-sectional study of 8680 non-agricultural workers, based on the First Central American Survey of Working Conditions and Health (2011). Main explicative variables were paid working hours, marital status, caring for children, and caring for people with functional diversity or ill. Using Poisson regression models, adjusted prevalence ratios of poor self-perceived and mental health were calculated by sex and social security coverage (proxy of informal employment).
Results
A clear pattern of association was observed for women in informal employment who were previously married, had care responsibilities, long working hours, or part-time work for both self-perceived and mental health. No other patterns were found.
Conclusions
Our results show health inequalities related to unpaid care work and paid work that depend on the interaction between gender and informal employment. To reduce these inequalities suitable policies should consider both the labor (increasing social security coverage) and domestic spheres (co-responsibility of care).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Informal employment is one of the most important forms of labor market participation in low- and middle-income countries like those of Central America (ILO 2011), and is a key but seldom studied social determinant of health (Marmot et al. 2008). Labor markets in these countries are largely sustained by informal employment arrangements, where work is not regulated nor are workers protected by labor regulation and social security (ILO 2013). In Spanish-speaking Central American countries (Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua and Panama), more than 60 % of non-agricultural workers are in informal employment, with a higher proportion of women than men (ILO 2011). For example, according to ILO, 39 and 72 % of workers in non-agricultural informal employment in 2010 were women and 30 and 60 % were men in Costa Rica and El Salvador, respectively. Informal employment has been a way for many women to enter the labor market given there are fewer barriers to access and greater possibilities for combining employment and family demands (Benería 2001).
In Spanish-speaking Central American countries (hereafter Central America), the social organization of care is highly familist, mainly conducted in households and largely by women, with minimum co-responsibility from their male partners, the state or the market (Lexartza Artza 2012). Despite the dramatic transformation of family structures in the past decades, this social organization of care persists. Until the 1970s, nuclear families (father, mother, and several children) with a traditional model of gender division of labor (men as breadwinners and women as caregivers) were predominant. Currently, this model represents only about one-third of families in the region, with an increase in other types of families including nuclear dual-earner families with children, nuclear families without children, or households headed by women (Ariza and De Olivera 2004). These transformations in family structure are not considered in the design of public policy in the region, which seldom considers the domestic and family sphere, overloading women and generating or aggravating gender inequalities (Arriagada 2009). Consequently, when women combine employment and family responsibilities their total workload is much higher than for men. Moreover, the gender division of labor determines that while women devote more time to unpaid care work than to paid work, it is the opposite in men (Rodríguez Enríquez 2007).
Many studies find employed women (including those with family responsibilities) have better health than those who perform full-time unpaid care work. Despite this, the work conflict resulting from combining employment and unpaid care work can negatively impact their health status (Buvinic et al. 2002; Arcas et al. 2013). Studies in Spain, which also has a highly familist model, show a consistent relationship between family demands and several health outcomes primarily among working women (Artazcoz et al. 2001, 2004). In contrast, family demands in countries with traditional family models can damage men’s health in situations of family financial stress because of their role as breadwinners (Artazcoz et al. 2013).
Most studies of the relationship between health and the combination of employment, family, and domestic work were conducted in high-income countries. These have different gender, labor market, and family policies than low- and middle-income countries, where informal employment is a key feature of labor markets. A recent study from Central America—based on the same survey used in this research—showed that workers in informal employment had a poorer health status than workers in formal employment (López-Ruiz et al. 2015). It also found that lacking social security coverage (as a dimension of informality) was the strongest predictor of the association with poor health. Other studies in Latin America have also shown that workers in informal employment are more likely to report poor health status (Santana et al. 1997; Sales and Santana 2003; Ludermir and Lewis 2003, 2005; Giatti et al. 2008a, b). However, some studies were done exclusively in men (Giatti et al. 2008b) or women (Santana et al. 1997; Sales and Santana 2003), did not stratify by sex (Ludermir and Lewis 2003; Giatti et al. 2008a), or simply adjusted for family characteristics and/or unpaid care work (Santana et al. 1997; Ludermir and Lewis 2003, 2005; Giatti et al. 2008a). None of these studies examined the interaction between informal employment, marital status, and unpaid care work.
Although informal employment and family characteristics are important independent determinants of workers’ health, we found no studies analyzing their interaction. Accordingly, the aims of this study were to assess the relationship between paid work and family characteristics (marital status and unpaid care work) and the health status of Central American workers; and to examine whether patterns of association differ by gender and informal or formal employment.
Methods
Data
Data were collected during the First Central American Survey of Working Conditions and Health of 2011, a cross-sectional study of a nationally representative sample of the occupied workforce (n = 12,024) aged ≥18 years. The study was performed in Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, and Panama (Benavides et al. 2014). Agricultural activities were excluded because of the complexity of distinguishing between subsistence agriculture and informal agricultural activities (ILO 2013). Also, employers with ≥5 employees were excluded because of an insufficient number of cases. Employers with <5 employees were included as a proxy of employers working in the informal sector (ILO 2013). The final study sample consisted of 8680 Central American workers engaged in non-agricultural activities (49 % of women).
Variables
Self-perceived health was dichotomized into good self-perceived health (combining very good, good, and fair responses) and poor self-perceived health status (poor and very poor). Mental health status was measured using a version of the General Health Questionnaire (12-item version) translated and adapted to Central American Spanish. Following the recommended threshold score for a few Latin American countries (Goldberg et al. 1997), mental health was dichotomized into good (score <4) and poor (score ≥4) mental health.
The main explicative variables were those related to paid and family characteristics. For paid work, we used weekly paid working hours grouped into three categories; <30 h (part-time), 30–48 h (full-time), or >48 h (long working hours). For family characteristics, we analyzed marital status (married or with a partner; single; or separated, divorced, or widowed); number of children aged ≤15 years requiring care (none, 1, 2, or ≥3), and whether care for people with functional diversity or ill (yes or no). This last variable was measured by asking how many people with any disability or who were ill were under the respondent’s care. We use the term “functional diversity” following a new paradigm that tries to overcome the negative connotations of the disability term and its implications (Patston 2007).
The covariates were employment status (employee, self-employed, or employer with <5 employees), type of contract (written, oral or no contract, or not applicable), country, age (18–30 years, 31–50 years, or >50 years), and occupation (management, scientific technicians or professionals; support technicians or professionals or clerical workers; service workers and vendors; or unskilled workers). Finally, the analysis was stratified by sex and by social security coverage (yes or no) as a proxy of formal/informal employment (ILO 2013).
Statistical analysis
Descriptive statistics including prevalence of both health outcomes across categories of the main study variables were performed. Poisson regression models with robust variance were used to obtain prevalence ratios (PR) and 95 % confidence intervals (CI) of poor self-perceived health and poor mental health. Analyses were stratified by sex and social security coverage to determine whether the observed associations differed between women and men, working in formal or informal employment. All analyses were adjusted for the covariates and included sampling weights for the Central American region (Benavides et al. 2014).
Results
There were more women (69 %) and men (66 %) working without social security coverage (informal employment) than with social security coverage (formal employment). Women in informal employment were older than women in formal employment. Among formal workers, almost 90 % were employees. Among informal workers, >25 % were employers with <5 employees, and 50 % of women and 42 % of men were self-employed. Among employees, about three-fourths of informal workers had either an oral or no contract. Women in informal employment were mostly vendors or service workers (69 %); men in the same situation were mostly in unskilled occupations (57 %). Among formal workers, men were mostly unskilled workers (42 %), whereas most women were in technical or professional occupations (34 %) (Table 1).
Around 40 % of women and men in informal employment worked long hours compared to 23 % of women and 34 % of men in formal employment. They also worked part-time more frequently than formal workers. Regarding marital status and unpaid care work, >50 % of the population was married or living with a partner and reported not performing unpaid care work (Table 1).
Overall prevalence of poor health
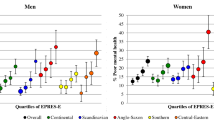
The prevalence of poor health outcomes was systematically higher among women than men and those in informal than in formal employment. Whereas 25 and 24 % of women in formal employment reported poor self-perceived health and poor mental health, respectively, these prevalences increased to 37 and 32 % for women in informal employment, respectively (Table 2). Similarly, men in formal employment had a lower prevalence of poor self-perceived health and poor mental health (19 and 21 %, respectively) than those in informal employment (31 and 29 %, respectively) (Table 3).
Paid working hours and health
Among women in informal employment, the highest prevalence of poor self-perceived and poor mental health was found for those working part-time (45 and 40 %, respectively) or working long hours (41 and 33 %, respectively). Women who worked part time in informal employment were significantly more likely to report poor self-perceived and mental health than those working full-time. The same pattern was found for long working hours in those engaged in informal employment, which was associated with poor self-perceived health (PR: 1.15, 95 % CI: 1.03–1.29) and poor mental health (PR: 1.35, 95 % CI: 1.18–1.55) (Table 2).
A similar pattern was found among men in informal employment, with the highest prevalence of poor self-perceived health in men working part time or long hours. However, poor mental health was more prevalent among those working full-time. Nevertheless, almost all associations with poor health were non-significant and showed an unclear pattern of association (Table 3).
Marital status and health
Over half of women in informal employment who were separated, divorced, or widowed (previously married) reported poor self-perceived health. Among this subgroup of women, there was a statistically significant association with poor self-perceived health (PR: 1.18, 95 % CI: 1.03–1.35) and poor mental health (PR: 1.41, 95 % CI: 1.19–1.68) compared to those who were currently married or cohabitating (Table 2).
On the contrary, among men in informal employment the prevalence of poor mental health was higher among married or cohabiting and single men (29 %), whereas a higher prevalence of poor self-perceived health was found among those previously married (35 %). However, there was no consistent pattern of association for men in informal or formal employment (Table 3).
Unpaid care work and health
Women in informal employment, who cared for ≥3 children, as well as those caring for people with functional diversity or ill, exhibited a higher prevalence of poor self-perceived health status (50 and 60 %, respectively). A statistically significant association was found for women in informal employment. Those who cared for ≥3 children were more likely to report poor self-perceived health (PR: 1.30, 95 % CI: 1.10–1.54), and those who cared for two children had poorer mental health (PR: 1.19, 95 % CI: 1.01-1.41) compared to those who did not care for any children. Also women in informal employment who cared for people with functional diversity or ill had significantly worse self-perceived and mental health (Table 2).
There was a gradient of poor mental health among men in informal employment who cared for children, with a significantly higher prevalence among those caring for ≥2 children. There were no associations with poor self-perceived health, irrespective of their employment situation (Table 3).
Discussion
This study contributes to the scarce knowledge about gender inequalities in health that are related to family characteristics and paid working hours among workers in formal and informal employment. To our knowledge, this is the first study addressing gender inequalities in health related to the combination of paid and unpaid care work among workers in non-agricultural informal employment. It provides plausible evidence of health inequalities related to unpaid care work and paid work in Central America. While men did not exhibit a consistent pattern of association, women in informal employment showed positive and strong associations between unpaid care work, marital status, paid working hours, and both poor self-perceived health and mental health.
The most important finding is that the associations are mostly limited to women in informal employment. This could be explained to a great extent by the possibly forced nature of informal employment among women with family responsibilities, coupled with the work overload for women combining paid and unpaid care work. Our results are consistent with other studies reporting that the combination of paid work and unpaid care work (in general and specifically for the care of children or people with functional diversity or ill) is associated with poor health primarily among women (Buvinic et al. 2002; Artazcoz et al. 2004, 2014; García-Calvente et al. 2004).
Choice of informal employment and family responsibilities
In the conventional model of labor markets, informal employment is due to labor market segmentation such that those working informally do so against their will. However, emerging evidence suggests that a share of informal employment is voluntarily chosen and may offer specific benefits and opportunities to certain individuals or groups (Günther and Launov 2012). Although pay and job security are important values of employment, they are not the only ones. This study estimated that around 45 % of informal employment within the entire informal sector is involuntary. Nevertheless, these studies did not include a gender perspective.
While the choice of informality is likely to be voluntary for many men, it could be involuntary for many women since they may be pressured to work in informal employment because of their care responsibilities. For example, in countries such as those in Central America where public and private co-responsibility for care is lacking (Lexartza Artza 2012), women with care responsibilities use informality to insert themselves into the labor market. Informality provides them with a paid job with flexibility, autonomy, and often, a work location close to home (Cassirer and Addati 2007), enabling them to combine paid and unpaid care work (Benería 2001). In the slums of Guatemala City, 40 % of mothers working in informal employment and caring for their children reported they preferred informal employment because of the lack of available childcare, since they would be unable to take their children with them to their workplace if they were formally employed (Cassirer and Addati 2007). In Costa Rica, women reported that family responsibilities were their main reason for working in domestic or other informal employment because of the flexibility it provided in working hours (Cassirer and Addati 2007).
Interestingly, in our study, while around two-thirds of women in informal employment with care responsibilities reported that their work schedule was flexible and of their choice, this decreased to 20 % in women with formal employment. Additionally, >50 % of these women declared that their home was their main workplace (results not shown).
Yet, this presumed choice requires reflection. As noted, women with care responsibilities are likely under pressure to choose work in informal employment because of their caregiver role, which is socially imposed and individually assumed. Thus, they select this role over better quality jobs or the mere possibility of seeking other jobs with better conditions. In contrast, men may be more likely to choose informal employment because of the better employment and working conditions (Jütting et al. 2008).
Family constraints may force women into informal employment, which is usually characterized by poor employment and working conditions, precariousness, and poverty, which could lead to extreme social exclusion (Sauma 2003; Carr and Chen 2004). In turn, informal employment is also associated with poor health status (Santana et al. 1997; Sales and Santana 2003; Ludermir and Lewis 2003, 2005; Giatti et al. 2008a, b). Coupled with its possibly forced nature and the double burden of work (Artazcoz et al. 2014), this combination might explain the poorer health among women in informal employment with care responsibilities versus men, but also of women in informal employment without those responsibilities.
Informal employment and poverty
Poverty can also play an important role in explaining the poor health outcomes observed among women in informal employment with care responsibilities. Around two-thirds of these women earned <301$PPP/month compared to one-third of women in formal employment with care responsibilities (results not shown). The low income among those women could put them in a situation of economic vulnerability, which is associated with poor health status (Menéndez et al. 2007).
Additionally, income insecurity is higher in the informal than the formal sector, because social and labor protections are lacking (Lund and Srinivas 2000). Workers in informal employment have no access to social benefits such as sickness absence, forcing them to work for as long as they are able when sick. Conversely, women in formal employment have all these social benefits and in addition may afford to hire domestic work, thus reducing their total workload (Batthyány et al. 2015). Consequently, their health would be less affected. It is important to note that most domestic employment is performed by women in informal employment, with high levels of precariousness, and lack of social protections (ILO 2010).
Informal employment and working hours
Some studies report that long working hours are related to poor health outcomes, primarily when people are forced into them because of economic vulnerability and accept poor working conditions (Artazcoz et al. 2009, 2013). In our study, >50 % of women in informal employment with long working hours had people who depended on them economically, and around 43 % worked >20 h/week in domestic work (12 % > 40 h/week) (results not shown). These women had low salaries (almost 70 % earned <301$PPP/month) so they may actually be forced into long paid working hours to increase their household income.
Coupled with this, the total workload may further limit women’s time for themselves, including leisure time and resting hours to recover from paid and unpaid work. A study in Bolivia showed that women in a situation of poverty (mostly indigenous) had no leisure time, but when they did, they used it to do more paid work to increase their household income (Benería 2008). Another issue to consider is that precarious jobs and economic insecurity translate into precarious lives and poor living conditions (Benería 2001). The time spend doing unpaid domestic work is directly associated with household and living conditions (poor household conditions mean a greater burden of domestic work) (Rodríguez Enríquez 2007). Therefore, women in informal employment are most likely combining long paid and unpaid working hours, potentially leading to a worse health status.
On the other hand, part-time employment is associated with working women who have family responsibilities. In low- and middle-income countries, not only do women have a higher proportion of part-time work than men, informal employment is more frequent among female part-time workers (Fagan et al. 2014). Much of part-time work is involuntary. Those who seek part-time work due to economic and family responsibilities often end up in informal employment because there are practically no opportunities in the formal economy. In fact, a study carried out in Honduras found that part-time work was seen as a “luxury consumption” for many women, principally those in poverty, because they could not afford to work only a few hours (López Bóo et al. 2010).
In our study, >50 % of women performing informal part-time work had people who depended on them economically (results not shown). Therefore, women in informal employment may work part-time involuntarily because of their family constraints, which restricts their choices and forces them into informal employment, and causes them to accept or remain in less desirable jobs with poorer job quality (Cassirer and Addati 2007; López Bóo et al. 2010). Furthermore, the relationship between part-time work, working and employment conditions, and health status depends, among other factors, on gender and on the voluntary or forced nature of this kind of work. This, in turn, depends on the employment offered by companies, labor regulations, and the existence of public care services among other variables (Bartoll et al. 2014).
Informal employment and marital status
Another finding that may be explained by economic vulnerability is the poor health of separated, divorced, or widowed women in informal employment, over half of whom had people who depended economically on them (results not shown). In fact, the proportion of single-parent households headed by women in poverty situations is >60 % in some Central American countries (Ariza and De Olivera 2004). Economic vulnerability coupled with the lack of public care services and the work overload of lacking a partner could tie these women to informal employment, leaving them without any form of social security and worse health (Artazcoz et al. 2014). Another related mechanism that could be operating is financial stress, which is usually associated to men in the breadwinner role. Nevertheless, these women must assume both the caregiver and breadwinner roles, and this could negatively affect their health (Artazcoz et al. 2009).
Limitations
This study has several limitations that should be considered. The questionnaire items on care are quite ambiguous so the interpretation of the questions and its answer by women and men may differ because of gender roles. For example, “¿cuántos menores de 15 años atiende o cuida usted?”. In Spanish, the verbs “atender” and “cuidar” could have different connotations. For most women, who may be assuming a caregiver role, this question might be a better approximation to their unpaid care work. In contrast, men may understand it as if they live or are responsible for children, but not as if they really assume their care. Moreover, the family relationship with the person who is cared for was not known, although we can assume that most were family members. Finally, because of the cross-sectional nature of the study, the results could be affected by reverse causality whereby people with poorer health status are more likely to work in informal employment. However, our results are consistent with the previous literature.
Conclusions
Our study results provide plausible evidence of health inequalities related to unpaid care work and informal paid work among women in countries with high levels of informal employment, and a highly familist organization of care. The wide social vulnerability that affects women with care responsibilities may force them into informal employment. Several mechanisms may link this to poor health such as poverty, precarious working and living conditions, long and part-time working hours, and financial insecurity, requiring further research. This not only affects their health, but also generates health inequalities between women and men and between women performing informal and formal employment. Paid work and unpaid care work are two completely interconnected spheres that should not be examined separately. Labor market organization is closely related to the social organization of care, making it impossible to influence one without affecting the other. To change the unfair organization of both spheres, improve the health of all workers, women and men in informal and formal employment, and reduce inequalities, both labor and care policies—that are usually planned and managed by different policies and authorities—should be considered. Two such policy entry points are increasing social security coverage in the labor sphere, and co-responsibility of care in the domestic sphere.
References
Arcas MM, Novoa AM, Artazcoz L (2013) Gender inequalities in the association between demands of family and domestic life and health in Spanish workers. Eur J Public Health 23:883–888. doi:10.1093/eurpub/cks095
Ariza M, De Olivera O (2004) Familias, pobreza y necesidades de políticas públicas en México y Centroamérica. In: Arriagada I, Aranda V (eds) Cambio de las familias en el marco de las transformaciones globales: necesidad de políticas públicas eficaces. ECLAC, Santiago de Chile, pp 153–195
Arriagada I (2009) La diversidad y desigualdad de las familias latinoamericanas. Rev Latinoam en Estud Fam 1:9–21
Artazcoz L, Borrell C, Benach J (2001) Gender inequalities in health among workers: the relation with family demands. J Epidemiol Community Health 55:639–647
Artazcoz L, Artieda L, Borrell C, Borrell C, Cortès I, Benach J, García V (2004) Combining job and family demands and being healthy: what are the differences between men and women? Eur J Public Health 14:43–48. doi:10.1093/eurpub/14.1.43
Artazcoz L, Cortès I, Escribà-Agüir V, Cascant L, Villegas R (2009) Understanding the relationship of long working hours with health status and health-related behaviours. J Epidemiol Community Health 63:521–527. doi:10.1136/jech.2008.082123
Artazcoz L, Cortès I, Escribà-Agüir V, Bartoll X, Basart H, Borrell C (2013) Long working hours and health status among employees in Europe: between-country differences. Scand J Work Environ Health 39:369–378. doi:10.5271/sjweh.3333
Artazcoz L, Cortès I, Puig-Barrachina V, Benavides FG, Escribà-Agüir V, Borrell C (2014) Combining employment and family in Europe: the role of family policies in health. Eur J Public Health 24:649–655. doi:10.1093/eurpub/ckt170
Bartoll X, Cortès I, Artazcoz L (2014) Full- and part-time work: gender and welfare-type differences in European working conditions, job satisfaction, health status, and psychosocial issues. Scand J Work Environ Health 40:370–379. doi:10.5271/sjweh.3429
Batthyány K, Genta N, Perrotta V (2015) El aporte de las familias y las mujeres al cuidado no remunerado de la salud en el Uruguay. ECLAC, Santiago de Chile
Benavides FG, Wesseling C, Delclos GL, Felknor S, Pinilla J, Rodrigo F (2014) Working conditions and health in Central America: a survey of 12,024 workers in six countries. Occup Environ Med 71:459–465. doi:10.1136/oemed-2013-101908
Benería L (2001) Shifting the risk: new employment patterns, informalization, and women’s work. Int J Polit Cult Soc 15:27–53
Benería L (2008) The crisis of care, international migration, and public policy. Fem Econ 14:1–21. doi:10.1080/13545700802081984
Buvinic M, Giuffrida A, Glassman A (2002) Gender inequality in health and work: the case of Latin America and the Caribbean. Inter-American Development Bank, Washington DC
Carr M, Chen M (2004) Globalization, social exclusion and gender. Int Labour Rev 143:129–160. doi:10.1111/j.1564-913X.2004.tb00548.x
Cassirer N, Addati L (2007) Expanding women’s employment opportunities: informal economy workers and the need for childcare. ILO, Geneva
Fagan C, Norman H, Smith M, González Menéndez MC (2014) In search of good quality part-time employment. ILO, Geneva
García-Calvente M, Mateo-Rodríguez I, Maroto-Navarro G (2004) El impacto de cuidar en la salud y la calidad de vida de las mujeres. Gac Sanit 18:83–92
Giatti L, Barreto SM, Comini César C (2008a) Household context and self-rated health: the effect of unemployment and informal work. J Epidemiol Community Health 62:1079–1085. doi:10.1136/jech.2007.069740
Giatti L, Barreto SM, Comini César C (2008b) Informal work, unemployment and health in Brazilian metropolitan areas, 1998 and 2003. Cad Saude Publica 24:2396–2406. doi:10.1590/S0102-311X2008001000020
Goldberg D, Gater R, Sartorius N et al (1997) The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol Med 27:191–197. doi:10.1017/S0033291796004242
Günther I, Launov A (2012) Informal employment in developing countries. Opportunity or last resort? J Dev Econ 97:88–98. doi:10.1016/j.jdeveco.2011.01.001
ILO (2010) Decent work for domestic workers. In: International labour conference, 99th Session. ILO, Geneva
ILO (2011) 2011 labour overview. Latin America and the Caribbean. ILO, Lima
ILO (2013) Measuring informality: a statistical manual on the informal sector and informal employment. ILO, Geneva
Jütting J, Parlevliet J, Xenogiani T (2008) Informal employment re-loaded. IDS Bull 39:28–36. doi:10.1111/j.1759-5436.2008.tb00442.x
Lexartza Artza L (2012) La organización social de los cuidados en Centroamérica y la República Dominicana. Barreras para el acceso de las mujeres al mercado laboral. ILO, San José
López Bóo F, Madrigal L, Pagés C (2010) Part-time work, gender and job satisfaction: evidence from a developing country. J Dev Stud 46:1543–1571. doi:10.1080/00220388.2010.492864
López-Ruiz M, Artazcoz L, Martinez JM, Rojas M, Benavides FG (2015) Informal employment and health status in Central America. BMC Public Health 15:698. doi:10.1186/s12889-015-2030-9
Ludermir AB, Lewis G (2003) Informal work and common mental disorders. Soc Psychiatry Psychiatr Epidemiol 38:485–489. doi:10.1007/s00127-003-0658-8
Ludermir AB, Lewis G (2005) Is there a gender difference on the association between informal work and common mental disorders? Soc Psychiatry Psychiatr Epidemiol 40:622–624. doi:10.1007/s00127-005-0938-6
Lund F, Srinivas S (2000) Learning from experience: a gendered approach to social protection for workers in the informal economy. ILO, Geneva
Marmot M, Friel S, Bell R, Houweling TAJ, Taylor S (2008) Closing the gap in a generation: health equity through action on the social determinants of health. Lancet 372:1661–1669. doi:10.1016/S0140-6736(08)61690-6
Menéndez M, Benach J, Muntaner C, Amable M, O’Campo P (2007) Is precarious employment more damaging to women’s health than men’s? Soc Sci Med 64:776–781. doi:10.1016/j.socscimed.2006.10.035
Patston P (2007) Constructive functional diversity: a new paradigm beyond disability and impairment. Disabil Rehabil 29:1625–1633. doi:10.1080/09638280701618778
Rodríguez Enríquez C (2007) Economía del cuidado, equidad de género y nuevo orden económico internacional. In: Giron A, Correa E (eds) Del Sur hacia el Norte: Economía política del orden económico internacional emergente. CLACSO, Buenos Aires, pp 229–240
Sales EC, Santana VS (2003) Depressive and anxiety symptoms among housemaids. Am J Ind Med 44:685–691
Santana VS, Loomis D, Newman B, Harlow SD (1997) Informal jobs: another occupational hazard for women’s mental health? Int J Epidemiol 26:1236–1242. doi:10.1093/ije/26.6.1236
Sauma P (2003) La Situación del empleo en el istmo centroamericano: informalidad, precariedad laboral, crecimiento económico y pobreza. In: Sojo A (ed) Pobreza y vulnerabilidad social: mercado de trabajo e inversión social en el Istmo Centroamericano a inicios del milenio. ECLAC, México, pp 28–74
Acknowledgments
We acknowledge Edurne Jiménez and George L. Delclòs for their review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the Parc de Salut MAR Ethical Committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the survey.
Additional information
This article is part of the special issue "Development and Public Health".
Rights and permissions
About this article

Cite this article
Lopez-Ruiz, M., Benavides, F.G., Vives, A. et al. Informal employment, unpaid care work, and health status in Spanish-speaking Central American countries: a gender-based approach. Int J Public Health 62, 209–218 (2017). https://doi.org/10.1007/s00038-016-0871-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-016-0871-3