
Abstract
Objectives
We examined the nationwide geographic variation of overweight and obesity in India, as well as a range of potential correlates of excess body fat.
Methods
We conducted cross-sectional analyses of the 2005–2006 Indian Demographic Health Survey (IDHS), based on 161,050 individuals (age range 18–54 years). Multivariate logistic regression models were used to determine odds ratios (OR) of overweight and obesity compared to normal weight with associated correlates.
Results
The overall prevalence was 12.4 % for overweight, 3.2 % for obesity, and 26.5 % for underweight. After multivariate adjustment, obesity was nearly thrice more likely in urban areas than in rural (OR 2.73, 95 % CI 2.53–2.94). Women were 2.71 times more likely to be obese than men (95 % CI 2.50–2.95). Better socioeconomic status was significantly associated with overweight and obesity. Overweight (OR 1.38, 95 % CI 1.31–1.47) and obesity (OR 1.46, 95 % CI 1.32–1.61) were most likely to occur in India’s Southern zone, when controlled for confounding factors.
Conclusions
High-risk estimates for overweight/obesity in urban settings, along with socioeconomic prowess in India and the resulting nutritional transition make a compelling case for public health policy on healthy lifestyles to avert the growing burden of non-communicable diseases associated with overweight/obesity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity and overweight are considered to be the fifth-leading risk factor for deaths worldwide, and at least 2.8 million adults die each year as a result of chronic conditions associated with excess body weight, in both more and less developed countries (Haslam and James 2005; WHO 2013b). The burden of non-communicable diseases (NCDs) such as diabetes, cardiovascular disease and hypertension associated with overweight/obesity (Whitlock et al. 2002; Sun et al. 2010; Jayawardena et al. 2012) is on the rise in India: the International Diabetes Federation projects the population affected by diabetes to rise to more than 101 million by 2030 (Gupta et al. 2012), while India’s hypertensive population is estimated to increase beyond 214 million by 2030 (Devi et al. 2012).
The Indian National Family Health Survey of 2006 (NFHS-3) demonstrated that the prevalence of overweight and obesity [body mass index (BMI) ≥25.00 kg/m2] was 9 % in men and 13 % among women (15–54 years); however, the results of the survey were limited to crude national prevalence estimates, with no examination of regional variation or the potential influence of urbanisation on prevalence estimates (IIPS 2007). Additionally, a review by Kalra and Unnikrishnan (2012) showed that there has been an overall increase in the prevalence of overweight/obesity among men and women (15–49 years) from 11 % as reported by NFHS-2 to 15 % as updated by NFHS-3.
The present study investigated the nationwide geographic variation of combined overweight and obesity for adults in India, and its association with urbanisation by examining prevalence estimates at the zone-level using the Indian Demographic Health Survey 2005–2006 (IDHS) data, while accounting for a number of potential risk factors and socio-demographic correlates. A supplementary analysis of underweight was also conducted in order to examine the association of urbanisation and socioeconomic status with the whole spectrum of BMI categories. The public health policy in India with regard to nutrition has originally been focused on addressing the prevalent under-nutrition (Khandelwal and Reddy 2013). The findings from studies investigating obesity in India and other low-resource settings will be valuable in informing a distribution of this policy focus with regard to the prevention of avertable chronic conditions associated with obesity (Khandelwal and Reddy 2013; Kandala et al. 2013, 2014; Kandala and Stranges 2014).
Methods
Study population
The 2005–2006 IDHS—also called the NFHS-3—covered 29 Indian states and was “designed to provide estimates of key indicators for India as a whole (and) … for all 29 states by urban–rural residence” (IIPS 2007). The survey included demographic, socioeconomic and health data for 124,385 women and 74,369 men between the ages of 15 and 49. For the present analysis, the following exclusion criteria were employed: (a) all pregnant women (5911 women); (b) all individuals of age less than 18 years at the time of the survey (22,413 individuals)—since our scope was limited to adult obesity; and (c) all individuals with missing BMI data (4732 women and 4648 men). The resulting sample had 161,050 individuals (61,208 men and 99,842 women), which was used for prevalence estimates and baseline demographic characteristics. For the multivariate regression analysis, missing data from each variable and “not de jure residents” from the standard of living variable were excluded since the standard of living index could not be determined without information on asset-ownership. Thus, the multivariate regression analysis for overweight analysis included 106,713 individuals, and the analysis for obesity included 92,742 individuals.
Outcome variable
We studied overweight and obesity as the two main outcomes in terms of BMI (kg/m2). The continuous BMI variable from the DHS dataset was converted into a categorical variable, with categories defined as per World Health Organisation (WHO) classifications: ≤18.49 kg/m2 as “underweight”; 18.50 to 24.99 kg/m2 as normal; 25.00 to 29.99 kg/m2 as “overweight”; and ≥30.00 kg/m2 as “obese” (WHO 2013a, b).
The outcome variable was re-coded into a binary variable with “normal weight”, and “overweight/obese” as the two possible outcomes for sex-stratified and zone-stratified analyses.
Exposure variables
The main exposure variable in the analysis was the “type of residence” in terms of the categories “urban” and “rural”—as defined by the Indian Census (Census Commissioner of India 2001). Other socio-demographic, lifestyle and geographic factors—sex, age, education level, standard of living, use of alcohol, tobacco smoking, religion and zonal council—that may influence the outcome were also included as confounders. Age was recorded by the DHS as a continuous variable, and was re-coded into a categorical variable of four 10-year categories, with a truncated first category for 18–24 year-olds. Education level was measured as “None”, “Primary”, “Secondary” and “Higher”, and a standard of living index was pre-calculated in the IDHS, categorised as “Low”, “Medium” and “High” (ICF International 2010). This index was created by the NFHS team as an economic measure using ownership of assets, arrived at with the help of a 27-item list of assets weighted according to the economic significance of ownership in India (IIPS 2007). Frequency of alcohol use was converted to a binary variable which reported consumption of alcohol in any frequency against no consumption. This was done in order to reduce the inherent recall and respondent bias in the variable.
The variable for religion was re-coded from eleven into six categories by combining the categories with the lowest numbers of adherents into an “Other” category. The 29 Indian states were re-coded into six zones as per administrative Zonal Council divisions set up with the States Re-organisation Act, 1956 in order to make populations sizes more comparable (Ministry of Home Affairs 2010). The category “Hindus” in the religion variable and the category “Northern” in the zone variable were used as references, since the former is the most populous (73.5 % of the sample), and the latter included the National Capital Region of Delhi, which is also the most populous urban area (Registrar General of India 2011).
Statistical analysis
The data were analysed using SPSS version 21 (IBM Corp. 2012). The prevalence of each BMI classification and the descriptive percentages of each socio-demographic factor were reported according to BMI category. The mean, standard deviation, and range were reported for BMI and age using existing continuous variables in the dataset. Odds ratios (ORs) and 95 % confidence intervals were used to determine a crude association between BMI and covariates.
The independent combined effect of all factors found to have significant (p < 0.05) relationships with BMI and type of residence in bivariate analysis—sex, age, education, standard of living, alcohol use, tobacco smoking, zone and religion—was assessed with a backwards multivariate logistic regression model.
The same model was then used by stratifying sex-wise, and obtaining the ORs and 95 % confidence intervals of overweight/obesity in both sexes for urban settings using rural settings as the reference categories. After stratifying zone-wise, the multivariate model was used to obtain ORs for urban vs. rural areas for each zone along with 95 % confidence intervals. The prevalence estimates of urban obesity and urban residence were obtained for each zone, re-coded into categorical variables and presented on a map of India for graphical comparison.
Results
Descriptive results
Baseline socio-demographic and lifestyle characteristics by BMI classification are presented in Table 1 (N = 161,050).
Overall, the mean age of the sample was 31.9 years ± 9.3 (age range 18–54). The mean BMI was 21.19 ± 3.94 kg/m2 (range 12.03–59.90 kg/m2). The prevalence of overweight was 12.4, 3.2 % for obesity, 26.4 % for underweight and 58.0 % for normal weight. The prevalence of overweight and obesity was 11.3 and 1.9 % among men, respectively, and 13.0 and 4.0 % among women.
More than 52 % of the individuals lived in rural settings. More than 26 % of those with a higher education were either overweight or obese. Among those with a high living standard, 24 % were overweight/obese. A large majority in all categories did not smoke tobacco or drink alcohol. Nearly 21.0 % of the sample from the Southern zone was overweight/obese, while only 10.3 % of the sample from the North-eastern zone was overweight/obese. The vast majority of the sample (73.5 %) was Hindu, followed by 12.4 % Muslims and 9.0 % Christians.
Regression analysis results
Results of the unadjusted and multivariate analyses are presented in Table 2. After adjusting for all factors, the likelihood of overweight in urban areas was almost twice that of rural areas (OR 1.78, 95 % CI 1.71–1.85), while it was nearly three times for obesity (OR 2.73, 95 % CI 2.53–2.94).
Females were 1.50 times more likely to be overweight and nearly three times more likely to be obese than males (OR 2.71, 95 % CI 2.50–2.95); the oldest age group was nearly 12 times more likely to be obese than the youngest age group (OR 11.73, 95 % CI 10.26–13.41); the highest education level was nearly twice as likely to be overweight or obese than no education; and odds of obesity in a high standard of living were 4.40 times that of low living standards (95 % CI 3.63–5.35). Tobacco smoking had a reduced association with overweight and obesity (OR 0.77 and OR 0.70, respectively), and alcohol use had a slightly increased significant association with overweight (OR 0.79, 95 % CI 0.76–0.82), but an insignificant and reduced association with obesity (OR 0.95, 95 % CI 0.84–1.08).
After adjustment, Christians were the least likely to be overweight when compared to Hindus (OR 0.87, 95 % CI 0.81–0.93), while Buddhists were the least likely to be obese (OR 0.66, 95 % CI 0.49–0.89). Sikhs were the most likely to be obese when compared to Hindus (OR 3.28, 95 % CI 2.81–3.82).
Individuals in the North-eastern zone were the least likely to be overweight (OR 0.71, 95 % CI 0.66–0.77) or obese (OR 0.35, 95 % CI 0.30–0.41). Overweight and obesity were both most likely in the Southern zone (OR for overweight = 1.38, 95 % CI 1.31–1.47; OR for obesity = 1.46, 95 % CI = 1.32–1.61).
Sex-wise stratification
The results of the sex-wise stratification are presented in Table 3. When adjusted for confounding factors, urban women were 2.01 times more likely than rural women to be overweight/obese (95 % CI 1.93–2.11), while urban men were 1.79 times more likely than rural men to be overweight/obese (95 % CI 1.69–1.91).
Zone-wise analysis
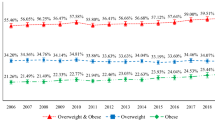
Results of zone-wise analysis are presented in Table 4 and Fig. 1. The highest combined prevalence of urban overweight/obesity was in the Southern zone (28.4 %), but the highest prevalence of urban obesity was in the Northern zone (7.1 %). The odds of overweight/obesity in an urban area as compared to rural areas were highest for the Eastern zone (OR 2.44, 95 % CI 2.19–2.72), despite the fact that urbanisation and overweight/obesity prevalence were relatively low in this zone. The North-eastern zone had a low prevalence of urban overweight/obesity (15.4 %), as well as low urbanisation (Fig. 1). In the Northern zone, the prevalence of urban overweight/obesity was high (>25 %), but the level of urbanisation appeared to be low (40–45 % urban dwellers). In general, urban areas were consistently associated with a higher risk of overweight/obesity across all zones.

Zone-wise overweight/obesity prevalence in urban areas, and urbanisation for each zone in India (India Demographic Health Survey, India 2005–2006; Dalet 2007)
Discussion
To our knowledge, this is the largest epidemiological investigation of geographic variations across the whole spectrum of BMI categories for both sexes in a nationwide representative sample of the Indian population, with the focus on differences between urban and rural settings. The main hypothesis—a positive association between urban-dwelling and overweight/obesity—was strongly supported by the results of this study. When adjusted for confounders, an individual residing in an urban area was almost twice as likely to be overweight/obese as compared to an individual living in a rural area.
These findings are corroborated by previous studies, which demonstrated significantly higher odds for obesity in urban areas, while also illustrating the urban–rural differences in their findings as different for either sex (Pednekar et al. 2008; Yadav and Krishnan 2008). For example, a study in North India demonstrated that urban areas had the highest prevalence of overweight and obese individuals, followed by urban slums and then rural areas, even though the study was limited by not considering potential confounding factors such as socioeconomic status and education (Yadav and Krishnan 2008).
Previous studies have been confined to either cross-sectional surveys of a single site, or compared locations which occurred within a single region. Gouda and Prusty (2014) utilised the same dataset from the Indian DHS survey, but limited their study to overweight and obesity among urban women in India. Other than prevalence results in the official report of the Third National Family Health Survey (IIPS 2007), we were unable to find studies which explored geographic variation of overweight/obesity across India as a whole. This analysis is unique since it is able to examine the variation and draw comparisons between Indian zones.
In our study, when looking at prevalence of overweight/obesity in urban areas alone, the results showed that the Southern zone had the highest prevalence (28.4 %), followed by the Northern zone (27.4 %) and then the Western zone (22.2 %). The high prevalence of overweight/obesity despite low levels of urbanisation in the Northern and Eastern zones could be due to a high occurrence of overweight/obese cases in urban areas, a reduction in physically demanding labour in rural areas due to mechanisation of agriculture, or even proliferation of sugary drinks. On a very crude level, this finding is salient because it potentially suggests that within a relatively small urban population, the likelihood of overweight/obesity is still high. This is illustrated by the very high odds of urban overweight/obesity and relatively high prevalence of overweight and obesity in urban areas found in the Eastern zone, while the rural prevalence of overweight and obesity is the lowest in this zone.
Regarding socioeconomic factors, results demonstrated that better education and better living standards were associated with higher odds of overweight/obesity after adjusting for confounders, including urban vs. rural setting. This is likely a consequence of the ongoing nutritional and epidemiological transition occurring in these settings. In fact, developing countries have not yet reached the same phase of nutritional transition as an economically affluent country, and while high-calorie diets comprising fast-food are the more economically affordable option in the latter, such diets are still reserved for the more affluent individuals in a country like India, where economic growth has only just begun to allow affluent individuals to afford fast-food (Pednekar et al. 2008). This relationship between socioeconomic affluence and overweight/obesity was also reported during a similar nutritional phase for Brazil, and corroborated for India (Chhabra and Chhabra 2007; Sichieri et al. 1994). A more specific example in the context of this epidemiological and nutritional transition is the rising socioeconomic status of Tangkhul Naga tribal women in North-eastern India, resulting in a transition to high-calorie foods and a sedentary lifestyle, and contributing to overweight/obesity among the tribal women (Mungreiphy and Kapoor 2010).
The association of urban overweight/obesity with education, while consistent with existing literature (Dinsa et al. 2012; Khandelwal and Reddy 2013; Gouda and Prusty 2014), could be due to sedentary occupations which usually result from better levels of education, as opposed to physically intensive occupations that follow from lower education levels.
The study of overweight and obesity among urban women in India demonstrated that media exposure was significantly associated with overweight and obesity (Gouda and Prusty 2014). Exposure to media could be correlated to affordability of television sets due to economic status. This could lead to inactivity, compounded by exposure to marketing of high-calorie diets and sugary drinks, eventually contributing to the nutritional transition evidenced in low-income countries.
The results of this study demonstrate that the odds of being overweight/obese increase with increasing age, corroborating the existing literature (Dinsa et al. 2012; Khandelwal and Reddy 2013; Gouda and Prusty 2014). This could be due to decreasing physical activity with age—especially among women—compounded with an increasing general access to high-calorie diets in India (Misra and Khurana 2008), as well as the high-calorie diets that are culturally recommended for Indian pregnant women (Choudhry 1997), the effects of which might linger beyond their gravid status.
Body image ideals in India are changing along with the economic and nutritional transition: while the results of a study from 1993 suggested that South Asian women in Britain were less likely to be dissatisfied with their body weight or describe themselves as “too fat” when compared with Caucasian women (Wardle et al. 1993), more recent studies suggest that Indian youth are more likely to idealise a slimmer body image, at times to an unhealthy extent (Goswami et al. 2012; Priya et al. 2010; Stigler et al. 2011; Swaminathan et al. 2013). This could only partially explain the low OR of overweight/obesity in the younger age group, since socioeconomic status and media exposure have been demonstrated as important combined factors of overweight and obesity for urban populations (Gouda and Prusty 2014). At present, any inference of a direct relationship between the high prevalence of socioeconomically affluent individuals and overweight/obesity in urban areas should be treated as being speculative with the available data, since urban areas in India also have large slum populations with economically deprived residents and it has been demonstrated that an urban-slum population had a significantly higher mean BMI than rural populations (Yadav and Krishnan 2008). Our study was limited by the lack of distinction between urban slum and settled or more affluent urban areas, and further study with a larger sample size is required to compare both types of urban settlements with rural settlements in order to build on the findings of Yadav and Krishnan (2008).
Women were found to consistently bear a greater burden than men. Furthermore, when stratified according to sex, the OR of overweight/obesity among urban women was twice that of rural women. This finding is consistent with all previous studies, which had similar results with varying degrees due to specific contexts (Gouda and Prusty 2014; Mungreiphy and Kapoor 2010; Pednekar et al. 2008; Yadav and Krishnan 2008). Gouda and Prusty (2014) demonstrated that non-poor urban women were 2–3 times more likely to be overweight/obese as compared to women from lower economic strata. Our results suggest that there is a need for investigating the geographic and socioeconomic variation between urban and rural settings for both sexes separately. The overwhelming evidence in the literature establishes that women are at a higher risk for overweight/obesity than men, and women are worse-affected than men during nutritional transitions: in rural areas, women are victims of under-nutrition and being underweight when compared to men, while women in urban areas are more likely to be obese than men (Montiero et al. 2004; Yadav and Krishnan 2008).
Overall, the findings are strong and consistent, but temporality regarding urbanisation and the increase in prevalence of overweight/obesity cannot be established (Hill 1965). It has previously been shown that extended exposure to urban risks and lifestyle does not necessarily result in overweight/obesity (Ebrahim et al. 2010). At this juncture, therefore, causality cannot be ascertained.
As a secondary data-analysis, the study was constrained by intrinsic limitations of the DHS dataset. While the dataset had variables on potentially influential pre-existing conditions such as tuberculosis infection, diabetes, anaemia and asthma, the available data were not complete for most of the individuals. Data on important correlates of body weight, such as physical activity, dietary habits, sleep patterns, chronic and psychiatric comorbidities, were also not available. As a result, only women reported as “currently pregnant” were excluded from analysis. The analysis also excluded all individuals who were under 18 years at the time of the survey, since the scope of our study was limited to adult obesity. However, we believe that childhood obesity is an urgent concern for countries undergoing nutritional transition, and needs to be studied at length.
The cut-offs used for BMI classifications were as defined by WHO (WHO 2013a). However, the WHO has recently recommended different cut-offs for the Asia–Pacific region, based on the notion that body-fat composition for Asian individuals is underestimated for the same BMI values as other ethnicities; under the new classifications, Asian individuals with BMI >23 kg/m2 should be considered overweight. While Pednekar et al. (2008) did not find any substantial changes to their results with the use of these values, these new classifications were not employed since there is no agreement on what BMI scale should be employed for each ethnicity. The Asian scale developed by the WHO is based on Chinese studies (WHO 2000), and the results of Dudeja et al. (2001) show that the scale is not the same for Indian ethnicities. Waist circumference measures for central adiposity is better suited to the South Asian context, since this measure has been shown to be associated with high risks of diabetes and hypertension, and the South Asian population is particularly at risk for insulin resistance (Khandelwal and Reddy 2013).
In India’s case, this policy on nutrition and healthy lifestyles would have to be tailored to address under-nutrition as well, since the country—like other developing countries—is affected on both sides of the spectrum. Therefore, future studies are warranted to assess the relationship between urbanisation and malnutrition in more detail, since the underweight aspect was not within the scope of this study.
From a public health perspective, the conditions of overweight and obesity are preventable and could potentially attenuate the health and social burden associated with excess body fat. Awareness for overweight and obesity could be developed using mass media, educational campaigns and workplace campaigns, since our findings suggest that the well-educated and the most affluent are at the greatest risk.
References
Census Commissioner of India (2001) Census of India: Census Data 2001/Metadata. http://censusindia.gov.in/Metadata/Metada.htm#2b. Accessed 17 July 2013
Chhabra P, Chhabra SK (2007) Distribution and determinants of body mass index of non-smoking adults in Delhi, India. J Health Popul Nutr 25:294–301
Choudhry UK (1997) Traditional practices of women from India: pregnancy, childbirth, and newborn care. J Obstet Gynecol Neonatal Nurs 26:533–539
Dalet D (2007) India: outline, states (white). d-maps.com. http://d-maps.com/carte.php?num_car=24853&lang=en. Accessed 20 Aug 2013
Devi P et al. (2012) Prevalence, risk factors and awareness of hypertension in India: a systematic review. J Hum Hypertens 27:281–287
Dinsa G, Goryakin Y, Fumagalli E, Suhrcke M (2012) Obesity and socioeconomic status in developing countries: a systematic review. Obes Rev 13:1067–1079
Dudeja V, Misra A, Pandey RM, Devina G, Kumar G, Vikram NK (2001) BMI does not accurately predict overweight in Asian Indians in Northern India. Brit J Nutr 86:105–112
Ebrahim S et al. (2010) The effect of rural-to-urban migration on obesity and diabetes in India: a cross-sectional study. PLoS Med 7:e1000268
Goswami S, Sachdeva S, Sachdeva R (2012) Body image satisfaction among female college students. Ind Psychiatry J 21:168–172
Gouda J, Prusty R (2014) Overweight and obesity among women by economic stratum in urban India. J Health Popul Nutr 32:79–88
Gupta R, Guptha S, Sharma K, Gupta A, Deedwania P (2012) Regional variations in cardiovascular risk factors in India: India heart watch. World J Cardiol 4:112–120
Haslam D, James W (2005) Obesity. Lancet 366:1197–1209
Hill AB (1965) The environment and disease: association or causation? Proc R Soc Med 58:295–300
IBM Corp. (2012) IBM SPSS Statistics for Windows, Version 21.0. IBM Corp., Armonk, NY
ICF International (2010) NFHS-3 supplemental documentation: Data Set Version 52. Measure DHS, Calverton, MD
IIPS (2007) National Family Health Survey (NFHS-3), 2005–2006. IIPS, Mumbai
Indian Ministry of Home Affairs (2010) Zonal Council. http://www.mha.nic.in/uniquepage.asp?ID_PK=470. Accessed 10 Sep 2013
Jayawardena R, Ranasinghe P, Byrne NM, Soares MJ, Katulanda P, Hills AP (2012) Prevalence and trends of the diabetes epidemic in South Asia: a systematic review and meta-analysis. BMC Public Health 12:380
Kalra S, Unnikrishnan AG (2012) Obesity in India: the weight of the nation. J Med Nutr Nutraceut 1:37–41
Kandala N-B, Stranges S (2014) Geographic variation of overweight and obesity among women in Nigeria: a case for nutritional transition in Sub-Saharan Africa. PLoS One 9:e101103
Kandala N-B, Tigbe W, Manda S, Stranges S (2013) Geographic variation of hypertension in Sub-Saharan Africa: a case study of South-Africa. Am J Hypertens 26:382–391
Kandala N-B, Manda S, Tigbe W, Mwambi H, Stranges S (2014) Geographic distribution of cardiovascular comorbidities in South Africa: a national cross-sectional analysis. J Appl Stat 41:1203–1216
Khandelwal S, Reddy K (2013) Eliciting a policy response for the rising epidemic of overweight-obesity in India. Obes Rev 14:114–125
Misra A, Khurana L (2008) Obesity and the metabolic syndrome in developing countries. J Clin Endocrinol Metab 93:s9–s30
Montiero CA, Conde WL, Popkin BM (2004) The burden of disease from undernutrition and overnutrition in countries undergoing rapid nutrition transition: a view from Brazil. Am J Public Health 94:433–434
Mungreiphy NK, Kapoor S (2010) Socioeconomic changes as covariates of overweight and obesity among Tangkhul Naga tribal women of Manipur, North-East India. J Biosoc Sci 42:289–305
Pednekar MS, Hakama M, Herbert JR, Gupta PC (2008) Association of body mass index with all-cause and cause-specific mortality: findings from a prospective cohort study in Mumbai. Int J Epidemiol 37:524–535
Priya D, Prasanna KS, Sucharitha S, Nafisa V (2010) Body image perception and attempts to change weight among female medical students at Mangalore. Ind J Comm Med 35:316–320
Registrar General and Census Commissioner of India (2011) Census India: million-plus cities in India. http://censusindia.gov.in/2011-prov-results/paper2/data_files/india2/Million_Plus_UAs_Cities_2011.pdf. Accessed 15 Sep 2014
Sichieri R, Coitinho DC, Leão MM, Recine E, Everhart JE (1994) High temporal, geographic, and income variation in body mass index among adults in Brazil. Amer J Public Health 84:793–798
Stigler M, Arora M, Dhavan P, Shrivastav R, Reddy KS, Perry C (2011) Weight-related concerns and weight-control behaviors among overweight adolescents in Delhi, India: A cross-sectional study. Int J Behav Nutr Phys Act 8:9
Sun Z, Zheng L, Detrano R, Zhang X, Xu C, Li J, Hu D, Sun Y (2010) Incidence and Predictors of Hypertension Among Rural Chinese Adults: Results From Liaoning Province. Ann Fam Med 8:19–24
Swaminathan S, Selvam S, Pauline M, Vaz M (2013) Associations between body weight perception and weight control behaviour in South Indian children: a cross-sectional study. BMJ Open 3:e002239
Wardle J, Bindra R, Fairclough B, Westcombe A (1993) Culture and body image: body perception and weight concern in young Asian and Caucasian British women. J Community Appl Soc Psychology 3:173–181
Whitlock G, Lewington S, Mhurchu CM (2002) Coronary heart disease and body mass index: a systematic review of the evidence from larger prospective cohort studies. Semin Vasc Med 2:369–381
WHO (2000) The Asia-Pacific perspective: redefining obesity and its treatment. http://www.wpro.who.int/nutrition/documents/docs/Redefiningobesity.pdf. Accessed 28 Aug 2013
WHO (2013) BMI classification. http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed 17 July 2013
WHO (2013) Obesity and overweight. http://www.who.int/mediacentre/factsheets/fs311/en/index.html. Accessed 4 April 2013
Yadav K, Krishnan A (2008) Changing patterns of diet, physical activity and obesity among urban, rural and slum populations in north India. Obes Rev 9:400–408
Acknowledgments
The authors thank ICF International for providing free access to 2005–2006 Demographic and Health Survey [Third National Family Health Survey (NFHS-3)] from India. Ngianga-Bakwin Kandala is also supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care West Midlands at University Hospitals Birmingham NHS Foundation Trust. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Siddiqui, S.T., Kandala, NB. & Stranges, S. Urbanisation and geographic variation of overweight and obesity in India: a cross-sectional analysis of the Indian Demographic Health Survey 2005–2006. Int J Public Health 60, 717–726 (2015). https://doi.org/10.1007/s00038-015-0720-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-015-0720-9