
Abstract
Objectives
We examined perceived stress and food intake at University of Turku, Finland.
Methods
This study was conducted as an online survey (1189 students). We computed two composite food intake pattern scores (sweets, cakes and snacks; fruits and vegetables), a dietary guideline adherence index, and the subjective importance of healthy eating. We assessed the correlations between perceived stress, and two food intake pattern scores, dietary guideline adherence index and subjective importance of healthy eating. We tested the associations between stress and the same variables, controlling for potential confounders for the whole sample, by gender, and by Body Mass Index (BMI).
Results
Fruits and vegetables intake and dietary guideline adherence were both negatively associated with stress. These negative associations were more pronounced in overweight and less pronounced in underweight compared to healthy weight students. Sweets, cookies and snacks consumption were not associated with stress. Stress was associated with lower subjective importance of healthy eating, independent of gender and BMI.
Conclusions
Perceived stress might have relationships of different magnitudes in overweight vs. normal BMI or underweight persons. BMI could be an effect modifier of the stress–food habits association.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The University period is characterized by new settings, environments, relationships, challenges, pressures, and frequently new habits that could shape adulthood health-related practices and lifestyles. Hence, university students’ health/well-being is receiving attention (El Ansari 2014), with concerns about students’ stress levels and their nutrition.
People report anxieties about the stress in their life; however, for university students, the sources of stress are multiple and diverse. These include psychosocial changes in one’s social networks/support systems, new socializations, financial constraints, peer competition, scholarly workloads, achieving academic success, being away from family home, fear of failing, and conflict with roommate/s or faculty or staff member/s (Chan and Koh 2007; El Ansari and Stock 2010; Al-Naggar et al. 2013). In addition, various countries and cultures do not necessarily face the same stressors and could also respond differently, and we are in agreement with others that there are very few published studies of stressors among Finnish college students (Rautopuro and Vaisanen 2001). Such a range of stress predictors suggests that health-related habits, e.g. nutrition could also be related to stress.
The relationships between stress and food intake are not straightforward. Studies of animals show that stress can lead in some cases to increases, but mostly leads to decreases in food intake (Levine and Morley 1981; Morley et al. 1983). In humans, stress influences eating in a bidirectional manner; for some individuals, exposure to stress or reactions to it decreases food intake and are associated with loss of weight; while conversely, most people increase their food intake during stress (Epel et al. 2004; Stone and Brownell 1994).
In addition, assessments of the stress–food intake relationships need to consider many inter-related socio-demographic and lifestyle variables. In terms of socio-demographics, being female and overweight predicted eating more during stress (Adam and Epel 2007), and living with parents during the university period was associated with better eating habits (Schnettler et al. 2013). Likewise, BMI is also important, where among male civil servants, the effect of job strain on weight gain and weight loss was subject to baseline BMI. In the leanest quintile, at baseline, high job strain and low job control were associated with weight loss by follow-up, whereas for those in the highest BMI quintile, these stress indicators were associated with subsequent weight gain (Kivimäki et al. 2006).
Few studies on eating habits have been undertaken in Finland, especially among university students, and across a range of food groups. Some dietary research in Finland has been population based (Roos et al. 2008) or among adolescents (Pohjanheimo et al. 2010) and elementary school pupils (Laitinen et al. 1993); while others explored the intake of isolated food groups, e.g. daily vegetables (Roos et al. 2008) or bread (Prättälä et al. 2001). At the population level, on the one hand, daily consumption of fresh vegetables became overall more prevalent during 1979–2002 (Roos et al. 2008). Among Finnish undergraduates, some risk factors of non-communicable chronic conditions received more attention: there is smoking, drinking and PA research (Heikkinen et al. 2006; Kuuppelomäki and Utriainen 2003), but studies on students’ dietary intake/adherence to dietary guidelines seem much less.
We examined the eating behavior and food intake of a sample of undergraduates at the University of Turku, Finland. We sought to answer the questions: “Is stress associated with decreased or increased food intake and healthy eating behaviours?”, and ‘Do these associations vary by gender and by BMI?’ The current study enriches the evidence base by exploring the (unadjusted and adjusted) associations between perceived stress of males and females as well as of underweight, normal weight and overweight undergraduates and their self-reported food intake, an index of subjective importance of healthy eating, dietary guidelines adherence, whilst controlling for many confounders: age, gender, living situation (accommodation during semester), economic situation, burdens (stressor), BMI, and moderate PA. Such knowledge is key for prevention and intervention initiatives for these young adults, assigning high significance to the study’s findings.
Methods
This cross-sectional study was a general student health and well-being survey implemented in several countries (El Ansari et al. 2014a, b, c, d). It included self-reported socio-demographic information (e.g., gender, age), food consumption habits of many food groups, and an item on the index of subjective importance of healthy eating.
Sample, ethics, and procedures
The research and ethics committee at the University of Turku, Finland approved the study, and data were collected via a secure online survey in English language (2013–2014). The University of Turku is situated in Southwest Finland, in the city of Turku, with units across Finland, from Lapland to the Archipelago Sea educating students in many different subjects. The University is an active academic community (25,000 students and staff members).
The sample comprised all first, second and third year undergraduates (inclusion criteria) at all faculties at the University (universal sampling, n = 4387). There were no exclusion criteria, and the total number of returned responses (sample) was 1189 (response rate of about 27 %). An invitation email was sent to the sample explaining the research aims and objectives and inviting students to participate by completing the online survey. Participation was voluntary and anonymous, and data were confidential and protected. Students were informed that by completing the survey, they agree to participate in the study and were provided with contact information in case they had questions. Two weeks after the start of the survey (first email invitation), a follow-up reminder email was sent again to the same sample of students. Additionally, posters about the study were positioned at locations in the students’ cafeteria/refectory at the University, and a reminder of the study was posted on the web homepage of the University. A pilot survey was conducted (May 2013) among 200 randomly assigned students using the English language questionnaire. Very few students reported any comprehensibility problems related to the English questionnaire, and the number of missing values related to items that reasonably could be expected to be answered by all participants were negligible (students who participated in the pilot were excluded from the final sample). The main survey was undertaken with the original questionnaire early in the first trimester (September 2013).
Respondents completed the online survey and submitted their electronic responses that were automatically saved and sent to the Student Management Office at the University of Turku which collated the online responses, and the data were imported into SAS software for analysis. For the current analysis, we excluded participants with missing data on the dietary items and on the questions of importance of eating healthy, BMI and perceived stress, reducing the number to 1076 students; 314 males (29.2 %) and 762 females (70.8 %). Participating students were enrolled at the seven faculties of the University: humanity (31.3 %), mathematics and natural science (21.2 %), medicine (12.8 %), law (6.5 %), social science (8.4 %), education (8.1 %), and economics (12.0 %).
Health and well-being questionnaire
Perceived Stress Scale (4 items): Cohen’s Perceived Stress Scale (PSS) in its 4-item short form assessed the extent to which participants considered life situations to be stressful (Cohen et al. 1983). The PSS-4 assesses the degree to which situations in one’s life over the past month are appraised as stressful (how unpredictable, uncontrollable, and overloaded respondents find their lives). All items began with: “In the past month, how often have you felt…?” (5-point scale: 0 = ‘never’, 4 = ‘very often’). We summed up the responses so that higher scores indicate more perceived stress. In this sample, Cronbach’s alpha for the 4 items was 0.76 signifying good internal consistency of the scale.
Assessment of food consumption habits (12 items): students self-reported their nutritional habits in a food frequency questionnaire (FFQ) comprising 12 variables that measured their consumption of sweets, cakes/cookies, snacks and fast/canned food, fresh fruits, raw and cooked vegetables and salads, meat and fish, milk products, and cereals. The introductory question, “How often do you eat the following foods?” queried students about the frequency of their usual consumption of each food group individually (5-point scale: ‘several times a day’, ‘daily’, ‘several times a week’, ‘1–4 times a month’, and ‘never’). The question gathered information about respondents’ general food consumption. The instrument was based on pre-existing food frequency questionnaires, adapted for the study and used in previous publications (El Ansari et al. 2012, 2014a). No formal test of validity was performed, but the questionnaire was very similar to other food frequency questionnaires that had been validated (e.g., Osler and Heitmann 1996; Roddam et al. 2005). For descriptive purposes, the categories ‘several times a week’ and ‘daily’ were collapsed together. Two composite food intake pattern scores were developed (a priori derived). Scales for the less healthy options (sweets, cake/cookies, and snacks) and for the healthier options (fruits, raw and cooked vegetables) were summed (composite scores ranged between 3 and 15).
Dietary guideline adherence index was computed using the FFQ. For sweets, cake/cookies, snacks, fast food/canned food and lemonade/soft drinks, no specific guidelines exist; hence we employed ‘1–4 times a month’ and ‘never’ as recommended. To consider all sweets, cake/cookies and snacks together, we used the above composite food intake pattern score (Sweets, cookies and snacks score), and healthy eating was considered present if this score was ≤6, corresponding to 3 times intake of these items of ‘less often than 1–4 times a month’. Each of the fast food/canned food and lemonade/soft drinks were included as individual items in computing the objective guideline adherence index. For the remaining food groups, we used the WHO dietary guidelines recommendations for European region (WHO 2003). Consequently, for the number of daily fruit, raw and cooked vegetables servings, the cutoff was ‘daily’ or ‘several times a day’. For meat, the cutoff was ‘less than daily’; and for fish ‘several times per week’ was the cutoff. Milk and cereals were not included in computing of dietary guideline adherence index as the information about milk and cereals was generally too unspecific to categorize as healthy or unhealthy nutrition. The dietary guideline adherence index is a score with maximum 8 points (8 guidelines) calculated from the recommendations of 8 food groups: (1) sweets, cookies, snacks; (2) fast food/canned food; (3) lemonade/soft drinks; (4) fruits; (5) salad, raw vegetables; (6) cooked vegetables; (7) meat; and (8) fish.
Importance of eating healthy (1 item): “How important is for you to eat healthy?” on a 5-point scale (1 = ‘Not at all important’ to 5 = ‘very important’) (El Ansari et al. 2014a).
Under, normal and overweight (BMI): using self-reported weight (kg) and height (m), BMI was calculated (kg/m2) and categorized into underweight (BMI <18.5 kg/m2), normal weight (between 18.5 and 25 kg/m2) and overweight (>25 kg/m2) (WHO 2000). The overweight category also included obese students (BMI >30 kg/m2).
Due to their possible associations with eating behavior, potential confounders that were controlled for in the regression analysis included: (1) age; (2) gender; (3) economic situation (“How sufficient is your income?”, coded into sufficient vs. not sufficient); (4) living situation/arrangements during university terms (“Where do you live during university term time?”, coded into living with partner vs. not living with partner); (5) moderate PA (“On how many of the past 7 days did you participate in moderate exercise for at least 30 min?”). Participants answered with 0–7 days, we used a cutoff of ≥5 days/week as adherence to PA guidelines (Haskell et al. 2007); and, (6) BMI, categorized by WHO guidelines (WHO 2000).
Statistical analysis
Statistical analyses were conducted in SAS Version 9.4 (significance level P set <0.05). For descriptions, Chi-square (χ2) or Wilcoxon rank sum tested the gender differences across categorical or numerical variables, respectively. Spearman rank coefficient quantified the correlation between each of the nutrition-related variables and the stress score. The effects of the different nutrition-related exposures on perceived stress were analyzed by multiple linear regression models separately for gender and BMI categories. Data were adjusted for age, sex, living situation, economic situation, moderate PA, and BMI. Model assumptions were graphically tested and fulfilled for all models.
Results
Perceived stress, food intake and dietary guidelines adherence of students in Finland
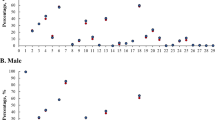
Table 1 shows the socio-demographic characteristics, moderate PA, and intake of 12 food groups for the whole sample and by gender. For both genders, the age ranged from 17 to 65 years (median = 21 years). Less than a third of students lived with their partners, and ≈40 % felt they have sufficient money. Thirteen percent of women and 30 % of men were overweight (BMI >25 kg/m2). Both genders rarely ate sweets, cakes and cookies, did not commonly eat fast food, and did not drink soft drinks on daily basis. Both genders ate fruits and vegetables regularly (daily/several times a day). Daily fish consumption was uncommon and differently distributed by gender. Because of the magnitude of significant differences between males and females, further analyses were gender stratified. Gender differences were particularly observed for fruit and vegetable consumption and meat and fish consumption.
Table 2 depicts students’ perceived stress levels, two food intake pattern scores, dietary guideline adherence index, and the index of subjective importance of healthy eating by gender and by BMI categories. Women reported significantly more stress than men, and also ate significantly more sweets, cookies, snacks, and significantly more fruits and vegetables than men. Additionally, women adhered more often to dietary guidelines and regarded healthy eating important more than men. Perceived stress and consumption of sweets, cookies and snacks did not differ between normal and overweight students. However, consumption of fruit, raw and cooked vegetables was less pronounced in overweight students, and dietary adherence was highest in underweight students and lowest in overweight students. The index of subjective importance of healthy eating was higher in underweight/normal weight students than in overweight.
Is food intake correlated with perceived stress? (unadjusted analysis)
Table 3 shows the correlation coefficients between stress and all nutritional variables stratified for sex and for BMI categories. Consumption of sweets and cookies was not associated with stress. Intakes of fresh fruits, raw and cooked vegetables, as well as fish, meat and milk products consumption were negatively associated with stress. Overall, the magnitudes and the significance of the correlations between stress and food intake showed no big gender differences. However, cooked vegetables and fast food were correlated with perceived stress only among males. In contrast, for BMI, the negative associations between stress and some food groups (fruits, raw and cooked vegetables, fish, meat and milk products) were less pronounced and not significant in underweight students, a little more pronounced in normal weight students, but most pronounced amongst overweight students.
The nutritional and dietary correlates of perceived stress (adjusted analysis)
Multiple linear regression adjusted for potential confounders is presented in Tables 4 and 5. The overall analysis as well as the sex-stratified analysis (Table 4) supported the findings of the crude analysis. Consumption of sweets, cookies and snacks was not associated with stress, but consumption of fruits, raw and cooked vegetables, increased dietary guideline adherence, as well as index of subjective importance of healthy eating were all negatively associated with stress. However, the r-square was low for all the multiple linear regression, where it varied between 3 and 7 %.
Table 5 shows the analysis stratified for BMI categories. There was a trend of an increasing association starting from underweight to overweight observed particularly for dietary guideline adherence index and the fruits and raw and cooked vegetables food intake pattern. For fruit, raw and cooked vegetables, the slope and therewith the rise of the association increased from being low and not significant in the underweight category, medium but significant in normal weight students, and high and even more significant among overweight students (see standardized Beta coefficients). Similar results were observed with the dietary guideline adherence index, but not with the index of subjective importance of healthy eating.
Discussion
Stress was negatively associated with a variety of foods (fresh fruits, raw and cooked vegetables, fish, meat and milk products consumption) in this sample of undergraduate Finnish students. A body of the literature suggests instead a commonly positive association between stress and food intake (Michaud et al. 1990; Bakr et al. 2002), and between stress and greater motivation to eat (Sims et al. 2008; Groesz et al. 2012). However, evidence proposes that the stress–food consumption links are not clear-cut, might differ, and are possibly affected by the stress or stressor amount/type, and the eating habit/s. Others have noted bidirectional effects, as the individual difference model suggested that there are two ways in which stress may influence eating, resulting in either eating or not eating (Greeno and Wing 1994). Some studies found no associations—in the UK, exam stress had no effects on students’ eating behaviors/food intake (Pollard et al. 1995); while other studies reported a negative association—in Japan, 52.1 % of the sample of university students had a decreased appetitive response to stress (Yoshikawa et al. 2014). Our findings agree with others (Yoshikawa et al. 2014; Oliver and Wardle 1998). In addition, for fruits and vegetables intake, our findings support that increased stress is associated with decreased consumption of fruits and vegetables, where a study among 3706 undergraduates in England, Wales and Northern Ireland used the same research tool as in the current study and found that consuming ‘healthy’ foods (e.g. fresh fruits, salads, cooked vegetables) was significantly negatively associated with perceived stress for both sexes (El Ansari et al. 2014a). Such findings have implications for prevention and intervention efforts for university students where stress reduction programs should consider also healthy eating recommendations.
Interestingly, in our sample, sweets, cookies and snacks were not associated with stress-related eating behavior. This finding contrasts with the existing literature, as studies have shown that in stress-related overeating, particular palatable foods, like chocolate or fat-containing foods like snacks are overeaten in stressful situations (Adam and Epel 2007; Singh 2014). A possible explanation for our finding is that such food groups were only eaten very seldom in our Finnish sample. As Table 1 shows, very few students ate sweets, cookies and snacks on regular daily basis. Due to the small percentage of such eaters, it might be that such a potential association was not evident in the current study. Further research is warranted.
For overall dietary adherence, we found that increased stress was associated with decreased dietary guideline adherence. We agree with previous studies, as a survey among undergraduates (seven universities) in the UK (El Ansari et al. 2014a) found that students with high stress levels had two traits: they overate snacks, sweets and fast food; but also under-ate fruit and vegetables. Thus, adherence to dietary guidelines could be more challenging among persons with higher perceived stress.
Beside the negative association of stress with fruit and vegetable consumption and dietary adherence index, we found that the magnitude of this negative relationship was subject to the individual’s BMI, where it was more pronounced in overweight persons. We observed that among overweight students, stress was more strongly associated with unhealthy eating habits than it was for normal weight or underweight students. With regards to the associations between stress and food consumption stratified for normal and overweight persons, other studies found similar results. A follow-up of a Finnish birth cohort (3598 girls, 3347 boys) of the association between stress-related overeating and overweight, showed that stress driven eaters were significantly more obese and overweight (Jääskeläinen et al. 2014). In our current analysis, we found no stress-associated overeaters, rather we observed stress-associated under-eaters. However, our finding of a more profound association between stress and eating habits in overweight persons agrees with Jääskeläinen et al. (2014) who also observed a more pronounced association between stress and eating habits, although their association was positive (in contrast to our negative association). Furthermore, an experimental study suggested a possible relationship between adipose tissue and stress and food consumption via the acute stress-induced hypothalamic–pituitary–adrenal axis activity (Tryon et al. 2013). It is acknowledged that the link between food and mood remains to be fully understood, as it comprises highly complex, multiple and interacting risk factors and signaling pathways involved in the maintenance of energy balance and mood stability, with orexigenic and anorexigenic neuropeptides, metabolic factors, stress responsive hormones, and other factors (Rossetti et al. 2014).
Our finding that stress was more strongly associated with unhealthy eating habits among overweight persons than it was for normal weight or underweight persons has implications: (1) for planning—when developing stress reduction programs and designing nutritional knowledge and healthy eating interventions, initiatives need to be tailored to sufficient/effective ‘strengths’ to account for the ‘stronger’ association between stress and unhealthy eating and decreased adherence in higher BMI individuals; and, (2) for implementation—prevention/intervention efforts for university students, stress reduction programs could possibly simultaneously influence healthy eating positively and could potentially increase adherence to dietary guidelines. These two potential possibilities could have stronger effects amongst higher BMI individuals. Future research should consider these aspects, and in addition, explore the complex associations and potential reasons for any observed differences in the food–mood relationships while considering overweight, obese and normal weight individuals.
This study has some limitations. We examined one university in Finland (there are currently 14 universities operating under the Finnish Ministry of Education and Culture). The response rate was not very high (27.1 %), hence cautious generalizations are required; however, this is a common problem in internet-based surveys and our response rate was similar to or even better than other surveys (Braverman et al. 2015; Fillman 2015). Self-reports are subject to sociability/social desirability. Females were more represented in our sample (a reality at higher education institutions across the globe), reflecting the female dominance in all but a few disciplines at universities in Finland (University World News 2009); hence we analyzed the relationships for the whole sample and by gender to avoid potential confounding gender effects. We did not objectively measure food consumption, and for some food groups, we did not assess serving sizes. As a cross-sectional survey, the direction of the association (temporal relationship) between food intake and perceived stress cannot be ascertained. As the study was part of a general health and well-being survey, to keep respondent burden to a minimum, we did not inquire about absence or presence of cooking facilities, respondents’ cooking abilities and other related variables. Students with higher stress levels might not have been at the university during the data collection and might not have had a further opportunity to participate in the study. Future research should consider such limitations. However, we used WHO dietary guidelines, appropriate for Finland. Recommendations for Nordic countries, as well as the recent Baltic sea diet exist (Kanerva et al. 2013; Uusitupa et al. 2013) but they differ from WHO recommendations only in terms of food items within food groups (e.g. fruit and vegetables found in Nordic countries are different than those recommended by the Mediterranean diet), but not in terms of portions and frequency. We are not aware of any previous studies in Finland of university students’ eating habits, diet quality and dietary guidelines adherence that undertook such tasks. Another limitation is a need to consider any potential longer term effects of other interventions in Finland, e.g. the North Karelia project (community-based heart health promotion to achieve community-wide reductions in risk factors and mortality associated with cardiovascular disease) (Puska et al. 1995) on the parents of these students and possible spinoffs for their children who would now be at university (positive parenting).
Conclusion
Perceived stress might have relationships of different magnitudes in overweight individuals as compared with individuals of normal BMI or underweight persons in relation to decreases in fruit, raw and cooked vegetables consumption and also in relation to decreases in dietary guideline adherence. Furthermore, perceived stress was not associated with increased intake of sweets, cookies and snacks, and the negative association of importance of healthy eating with perceived stress was independent of gender and weight. Further research should focus in more detail on BMI as an effect modifier of the association between stress and food habits.
References
Adam TC, Epel ES (2007) Stress eating and the reward system. Physiol Behav 91:449–458
Al-Naggar RA, Bobryshev YV, Mohd Noor NA (2013) Lifestyle practice among Malaysian university students. Asian Pac J Cancer Prev 14(3):1895–1903
Bakr EM, Ismail NA, Mahaba HM (2002) Impact of life style on the nutritional status of medical students at Ain Shams University. J Egypt Public Health Assoc 77(1–2):29–49
Braverman MT, Hoogesteger LA, Johnson JA (2015) Predictors of support among students, faculty and staff for a smoke-free university campus. Prev Med 71:114–120
Chan GC, Koh D (2007) Understanding the psychosocial and physical work environment in a Singapore medical school. Singapore Med J 48(2):166–171
Cohen S, Kamarck T, Mermelstein R (1983) A global measure of perceived stress. J Health Soc Behav 24(4):385–396
El Ansari W (2014) Health and well-being of students at higher education institutions–time for urgent action? Cent Eur J Public Health 22(2):67
El Ansari W, Stock C (2010) Is the health and wellbeing of university students associated with their academic performance? Cross sectional findings from the United Kingdom. Int J Environ Res Public Health 7(2):509–527
El Ansari W, Stock C, Mikolajczyk RT (2012) Relationships between food consumption and living arrangements among university students in four European countries—a cross-sectional study. Nutr J 11:28. doi:10.1186/1475-2891-11-28
El Ansari W, Adetunji H, Oskrochi R (2014a) Food and mental health: relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent Eur J Public Health 22(2):90–97
El Ansari W, Dibba E, Stock C (2014b) Body image concerns: levels, correlates and gender differences among students in the United Kingdom. Cent Eur J Public Health 22(2):106–117
El Ansari W, Khalil K, Crone D, Stock C (2014c) Physical activity and gender differences: correlates of compliance with recommended levels of five forms of physical activity among students at nine universities in Libya. Cent Eur J Public Health 22(2):98–105
El Ansari W, Oskrochi R, Haghgoo G (2014d) Are students’ symptoms and health complaints associated with perceived stress at university? Perspectives from the United Kingdom and Egypt. Int J Environ Res Public Health 11(10):9981–10002
Epel E, Jimenez S, Brownell K, Stroud L, Stoney C, Niaura R (2004) Are stress eaters at risk for the metabolic syndrome? Ann N YAcad Sci 1032:208–210
Fillman VM (2015) Career interest, self-efficacy, and perception in undecided and nursing undergraduate students: a quantitative study. Nurse Educ Today 35(1):251–255
Greeno C, Wing RR (1994) Stress-induced eating. Psychol Bull 115:444–464
Groesz LM, McCoy S, Carl J, Saslow L, Stewart J, Adler N et al (2012) What is eating you? Stress and the drive to eat. Appetite 58:717–721
Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A, American College of Sports Medicine, American Heart Association (2007) Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 116(9):1081–1093
Heikkinen R, Kivastik J, Kingisepp PH, Hirvonen L, Näyhä S (2006) Smoking differences between university faculties in Tartu, Estonia, and Oulu, Finland, after the disruption of communism. Soz Praventivmed 51(6):381–391
Jääskeläinen A, Nevanperä N, Remes J, Rahkonen F, Järvelin MR, Laitinen J (2014) Stress related eating, obesity and associated behavioural traits in adolescents a prospective population based cohort study. BMC Public Health 14:321
Kanerva N, Kaartinen NE, Schwab U, Lahti-Koski M, Mannisto S (2013) Adherence to the Balti Sea diet consumed in the Nordic countries is associated with lower abdominal obesity. Br J Nutr 109:520–528
Kivimäki M, Head J, Ferrie JE, Shipley MJ, Brunner E, Vahtera J, Marmot MG (2006) Work stress, weight gain and weight loss: evidence for bidirectional effects of job strain on body mass index in the Whitehall II study. Int J Obes (Lond). 30(6):982–987
Kuuppelomäki M, Utriainen P (2003) A 3 year follow-up study of health care students’ sense of coherence and related smoking, drinking and physical exercise factors. Int J Nurs Stud 40(4):383–388
Laitinen P, Nissinen A, Myllykangas M (1993) Fat consumption of first-grade students in elementary school. Quality and quantity of fats used at home and at school. Hoitotiede 5(2):50–55
Levine AS, Morley JE (1981) Stress-induced eating in rats. Am J Physiol 241:R72–R76
Michaud C, Kahn JP, Musse N, Burlet C, Nicolas JP, MeJean L (1990) Relationships between a critical life event and eating behavior in high school students. Stress Med 6:57–64
Morley JE, Levine AS, Rowland NE (1983) Minireview. Stress induced eating. Life Sci 32:2169–2182
Oliver G, Wardle J (1999) Perceived effects of stress on food choice. Physiol Behav 66(3):511–515
Osler M, Heitmann BL (1996) The validity of a short food frequency questionnaire and its ability to measure changes in food intake: a longitudinal study. Int J Epidemiol 25:1023–1029
Pohjanheimo T, Luomala H, Tahvonen R (2010) Finnish adolescents’ attitudes towards wholegrain bread and healthiness. J Sci Food Agric 90(9):1538–1544
Pollard TM, Steptoe A, Canaan L, Davies GJ, Wardle J (1995) Effects of academic examination stress on eating behavior and blood lipid levels. Int J Behav Med 2:299–320
Prättälä R, Helasoja V, Mykkänen H (2001) The consumption of rye bread and white bread as dimensions of health lifestyles in Finland. Public Health Nutr 4(3):813–819
Puska P, Tuomilehto J, Nissinen A et al (eds) (1995) The North Karelia Project. 20 year results and experiences. Finland University Press, Helsinki
Rautopuro J, Vaisanen P (2001) Non-traditional students at university: a follow-up study of young and adult students’ orientations, satisfaction and learning outcomes. In: Paper presented at the European conference on educational research, Lille, 5–8 September 2001
Roddam AW, Spencer E, Banks E, Beral V, Reeves G, Appleby P, Barnes I, Whiteman DC, Key TJ (2005) Reproducibility of a short semi- quantitative food group questionnaire and its performance in estimating nutrient intake compared with a 7-day diet diary in the Million Women Study. Public Health Nutr 8:201–213
Roos E, Talala K, Laaksonen M, Helakorpi S, Rahkonen O, Uutela A, Prättälä R (2008) Trends of socioeconomic differences in daily vegetable consumption, 1979–2002. Eur J Clin Nutr 62(7):823–833
Rossetti C, Halfon O, Boutrel B (2014) Controversies about a common etiology for eating and mood disorders. Front Psychol 5:1205
Schnettler B, Denegri M, Miranda H, Sepúlveda J, Orellana L, Paiva G, Grunert KG (2013) Eating habits and subjective well-being among university students in southern Chile. Nutr Hosp 28(6):2221–2228
Sims R, Gordon S, Garcia W, Clark E, Monye D, Callender C et al (2008) Perceived stress and eating behaviors in a community-based sample of African Americans. Eat Behav 9:137–142
Singh M (2014) Mood, food and obesity. Front Psychol 5:925
Stone A, Brownell K (1994) The stress-eating paradox: multiple daily measurements in adult males and females. Psychol Health 9:425–436
Tryon MS, DeCant R, Laugero KD (2013) Having your cake and eating it too: a habit of comfort food maz link chronical stress exposure and acute stress-induced cortisol hyporesponsiveness. Physiol Behav 114–115:32–37
University World News (2009). FINLAND: women dominate the campus. http://www.universityworldnews.com/article.php?story=20091211083716523
Uusitupa M, Hermansen K, Savolainen MJ, Schwab U, Kolehmainen M, Brader L, Mortensen LS, Cloetens L et al (2013) J Intern Med 274:52–66
WHO (2000) Obesity: preventing and managing the global epidemic. World health organization, Geneva
WHO (2003) Food based dietary guidelines in the WHO European Region, World health organization regional office Copenhagen
Yoshikawa T, Tanaka M, Ishii A (2014) Association of fatigue emotional-eating behaviour and the response to mental stress in food intake in a young adult population. Behav Med 40:149–153
Acknowledgments
The authors acknowledge the University, the Faculties and students who participated in this study. There was no external financial support/ funding for this study. The authors also acknowledge and thank the Student Management Office at the University of Turku for their assistance with the online survey and for their inputs in data collection. The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
El Ansari, W., Suominen, S. & Berg-Beckhoff, G. Mood and food at the University of Turku in Finland: nutritional correlates of perceived stress are most pronounced among overweight students. Int J Public Health 60, 707–716 (2015). https://doi.org/10.1007/s00038-015-0717-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-015-0717-4