
Abstract
Objectives
To determine whether there are differences in disability by immigrant generation and region of origin and recency of arrival in Canada, and the role of health literacy in this relationship.
Methods
A secondary analysis of the Canadian component of the 2003 International Adult Literacy and Skills Survey (IALSS) was undertaken.
Results
Compared to the third-plus generation, first-generation immigrants were less likely to report disability; these differences remained even after adjustment for sociodemographic and socioeconomic factors. No differences in disability were observed between the second- and third-plus generations. Among first-generation immigrants, those not from Europe or USA were less likely to report disability regardless of their duration in Canada. Health literacy was negatively associated with disability only in the analysis comparing generations of Canadians. However, its effect was largely accounted for by education, employment status and income.
Conclusions
First-generation immigrants were less likely to be disabled than the other generations. Education, employment and income provide important avenues through which individuals develop health literacy. Health literacy was not associated with disability among first-generation immigrants perhaps because health literacy is low in this group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Health literacy is the ability to access and use health information to make appropriate health decisions and maintain basic health (Canadian Council on Learning 2007; Rootman and Ronson 2005). It links levels of literacy with the ability to act upon health information and to take control of health, and is also an important pathway linking education to health and a contributor to health inequalities (Nutbeam 2000; Canadian Council on Learning 2007). For instance, Paasche-Orlow and Wolf (2007) show that health literacy impacts health outcomes at three distinct points along a continuum of health care, namely, access and use of health care, provider–patient interaction, and patient self-care. At each point, there are system, provider, and extrinsic factors that could modify or mediate the relationship between health literacy and health outcomes. Nonetheless, studies show that people with limited health literacy skills are likely to have difficulty in accessing health information and using medical services, and to report depression and poor self-rated health and to experience higher mortality (Sudore et al. 2006; Lincoln et al. 2006; Baker et al. 2007; Guerra and Shea 2007; Von Wagner et al. 2009; Omariba and Ng 2011). The causal mechanism between health literacy and health outcomes involves both patient level and healthcare system factors. These factors affect individuals’ self-care activities as well as access to and interaction with the healthcare system (Paasche-Orlow and Wolf 2007).
Only 40 % of Canadian adults posses the requisite level of health literacy (a score of ≥275 out of 500). However, fewer older people and immigrants have the required level of health literacy to maintain their health; 12 and 25 %, respectively (Canadian Council on Learning 2008). It can be expected that with the aging of the population and the shrinking youth cohort, a substantial number of Canadians would experience declining cognition which is directly related to the ability to process information. The low level of healthy literacy among immigrants is, however, a paradox because immigrants are on average more educated than the overall population. A potential explanation could be the growing immigrant population from countries with different cultures and languages from those of Canada (Canadian Council on Learning 2007; Chui et al. 2007). For instance, in 1971, only 11 % of immigrants to Canada were from Asia and 61 % from Europe. By 2006, the trends had been reversed; 58 % of the immigrants were from Asia compared to 16 % from Europe. Similarly, the results of the 2011 National Household Survey show that except for the USA, all of five immigrant sending countries were Asian, with Philippines being the leading immigrant source country (Statistics Canada 2013). Recent decades’ immigrants are, therefore, more likely to face adjustment and integration challenges in Canada because of limited language skills.
It is now established that immigrants initially arrive in their host society with better health compared to non-immigrants, but they lose this health advantage over time. Their health eventually mirrors that of non-immigrants (Ng et al. 2005; Newbold 2005; Hyman 2007). On the one hand, immigrants have better health at arrival mostly because they are selected for characteristics related to good health at the outset; it enables them to immigrate (Beiser 2005). On the other hand, the difficulties of settling, adjusting, and integrating in the host country, poor access to care, limited knowledge of services, low income, limited social supports and low proficiency in English or French are associated lead to the over-time decline in the health of immigrants (Vissandjée et al. 2001; Steele et al. 2002; Stewart et al. 2008; Zanchetta and Poureslami 2006; Pottie et al. 2008). From a health literacy perspective, poor knowledge of English or French means that individuals are not able to communicate, access, and use health information to maintain their health. This is an important issue to examine given the changing demographic profile of the major immigrants receiving countries like Canada.
An important issue in immigrant research is the short- and long-term consequences of immigration. In particular, to establish the success of immigrants in integrating into the host societies, researchers examine different socioeconomic and health outcomes by generation (Acevedo-Garcia et al. 2005). Studies show that the second-generation health is closer to that of the third-plus generation than the first generation. For instance, the classical study on immigrant health conducted by Marmot and Syme, found that first-generation Japanese immigrants in Hawaii had less cardiovascular disease than the second generation (Marmot and Syme 1976). The health profiles of the second generation were closer to those of non-immigrant Hawaiians (Third-plus generation). Similarly, a Swedish study found that second-generation immigrants were at a greater risk for suicide than their first-generation parents (Hjern and Allebeck 2002).
There is a dearth of population-based studies examining health by generational status and health literacy in Canada (Hyman 2007). Previous population-based studies examining the role of health literacy on health outcomes were not possible because of the lack of appropriate data. The International Adult Literacy and Skills Survey (IALSS), however, included information on health literacy and several health outcomes (Statistics Canada and Human Resources and Social Development Canada 2005). There is, therefore, no Canadian study that has examined the effect of health literacy on physical disability in Canada. It is the only dataset that provides researchers the information needed to examine the effect of health literacy on disability.
Methods
This study examines the relationship between immigration and generation and physical disability, and the influence of health literacy on this relationship. The analysis compared immigrants and non-immigrants (overall sample), immigrant groups defined by region of origin and recency of arrival in Canada; and the local-born defined by generation.
Study samples
Data were drawn from the Canadian component of the 2003 IALSS. The IALSS was undertaken by Statistics Canada and was aimed at determining how well adults used printed information to function in society. The target population of the survey was people aged ≥16 excluding institutional residents, people living in Canadian military bases, Indian reserves, and certain remote areas of the country.
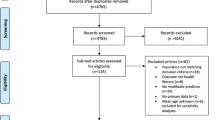
The survey was also designed to provide reliable estimates for special target populations including immigrants. Respondents on student, work and visitor’s visas, refugee claimants, and those missing information on immigration status (n = 220) were excluded. The analysis sample comprised 3,861 first, 2,823 second, and 16,134 third-plus generation immigrants aged ≥16. We applied survey weights to the data in our analyses to represent the target population.
Measures
Disability was ascertained from five questions on current disability and activity limitation related to vision, hearing problems, speech, learning, or any other disability or health problem lasting 6 months or more. Respondents who replied affirmatively to any of the listed conditions were considered as having a disability; all others were defined as disability free. Those with a disability were the predicted category. The issue of multiple disabilities is not considered in this analysis because of small numbers.
The generation variable had three categories: First, second, and third-plus immigrants. First-generation immigrants were people who were foreign born. Second generation are people for whom one or both of the parents are foreign born, while third-plus generation are those whom both parents were born in Canada. The first generation was further divided into two groups (because of sample size limitations): those from Europe or USA versus those from all the other countries. Further, they were categorized as either “recent” (arrived between 1994 and 2003) or “established” (arrived between 1900 and 1993). Eventually, the first generation comprised four categories: Established immigrants from Europe or USA, established immigrants from other countries, recent immigrants from Europe or USA, and recent immigrants from other countries.
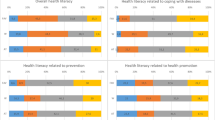
To derive the health literacy measure, information on respondents’ proficiency was collected from 350 items in four skill domains: prose and document literacy, numeracy, and problem solving. Of these, 191 were judged to measure health-related activities covering five dimensions of health (health promotion, health protection, disease prevention, healthcare, and system navigation). A Health Activities Literacy Scale with scores ranging from 0 to 500 was developed from these items. A score of ≥276 is required to maintain their health (Rudd et al. 2004). For our purposes, respondents scoring >275 were considered to have high health literacy and the rest low health literacy.
The study included two basic demographic variables: (1) age organized into five groups: 16–25, 36–35, 36–45, 46–55, 56–65, and over 65, (2) gender, female (1) and male (0). We also included literacy- and education-related variables. The selection of these variables is based on the lifelong and lifewide perspective in literacy research (Desjardins 2003). (1) Language discordance (whether mother tongue is dissimilar to language of survey administration, English or French), Discordant (1), Concordant (2). (2) Literacy practices at home was a dichotomous variable derived from information on frequency (weekly or monthly) of using the library, or frequency (at least once weekly) of reading or using information from newspapers, magazines, books, and letters, notes, or emails. Those who engaged in literacy practices were categorized as (1) and otherwise (0). (3) Education had two categories: less than high school (0) and high school or higher (1).
Socioeconomic status (SES) indicators included the following: (1) Employment status classified into five categories: Employed (0), Looking for work (1), Retired (2), Student (3), and Other (4). (2) Census Metropolitan Area (CMA) of residence had four categories: Toronto (0), Montreal (1), Vancouver (2), other CMA (3), Non-CMA (4). (3) Income comprised two categories levels adjusted for household size: low income level included incomes of less than $30,000 for families of 2, less than $40,000 for families of 3 and 4, and less than $60,000 for families of 5 or more. Households with incomes above these cut offs were considered high income. A third category comprised those who did not state their income.
Analysis
Disability status is a binary measure and, therefore, logistic regression was used for the analysis. Because health literacy was derived using item response theory, it could not be analyzed using standard routines in statistical software (Statistics Canada and Human Resources and Social Development Canada 2005). Stattool, a SAS macro developed at Statistics Canada, was used for the analysis. The macro also allows for the use of jackknife weights to adjust for complex survey design. The t statistic was used to assess individual variables’ significance and log-likelihood ratio tests for overall model significance. Statistical significance was set at p < 0.05 level.
We fitted four separate models for the overall sample, and the sub-sample of immigrants. For the overall sample, Model 1 had age, sex, and the generation indicator. Model 2 added health literacy; Model 3 introduced language discordance, literacy practices at home and education, while Model 4 included all the control variables. This analytic strategy enabled us to examine the mediation effect of health literacy and the other independent variables on differences between generations and immigrants in disability.
Results
Table 1 presents the descriptive statistics of the sample. Overall, 27 % of Canadians 16 years and older reported having disability of some kind. Fewer first-generation Canadians (24 %) than second- and third-plus generation Canadians reported being disabled. First-generation Canadians had significantly lower mean health literacy compared to the second- and third-plus generation Canadians, 228 versus 266 and 263, respectively. There are also significant differences between generations in age, language discordance, literacy practices, employment status, CMA of residence, and income.
Compared to the third-plus generation, first-generation Canadians were less likely to report disability (OR = 0.65, Table 2, Model 1). This relationship increased in magnitude when health literacy was included (OR = 0.62, Model 2). People with high health literacy were less likely to report disability (OR = 0.74, Model 2). The results of Model 3 indicate that some of the effect of health literacy operated through language discordance, literacy practices at home, and education, but especially the latter. Nonetheless, controlling for the other socioeconomic factors rendered the effect of health literacy statistically insignificant.
The analysis for the first generation only by region of origin is presented in Table 3. Established and recent immigrants not from Europe or USA were less likely to report disability compared to established immigrants from Europe or USA. Differences between established immigrants not from Europe or USA and established immigrants from Europe or USA were rendered statistically insignificant once control was made for socioeconomic factors (Model 4). The most important of the socioeconomic factors are employment and CMA of residence. There were no differences between recent immigrants from other regions and their established counterparts. All the literacy- and education-related factors including health literacy were not significantly associated with disability.
Regarding the control factors, age and employment status were significantly associated with disability in both the overall sample analysis comparing between generations and in the analysis comparing between first-generation immigrants by country of origin and recency of arrival in Canada. People younger than age 65 were less likely, while those looking for work or were retired were more likely to report disability. On the other hand, gender, education and income were significantly associated with disability only in the overall study sample. Women and people having at least high school education, and those living in high income households were less likely to report disability. On the other hand, the CMA of residence was significant only for first-generation immigrants. People living in other CMAs besides Toronto, Montreal and Vancouver and those not living in CMAs, were more likely to report disability.
Discussion
The focus of this study was on the differences in self-rated physical disability between different generations of immigrants in Canada and the role of health literacy in this relationship. Relative to the third-plus generation, first-generation immigrants were less likely to report disability; these differences were not accounted for by the selected control factors. The study also showed that there were no differences in self-rated physical disability between the second- and third-plus generations. In the analysis focusing only on first-generation immigrants, people whose country of birth was not USA or European were less likely to report disability regardless of their duration of residence in Canada. Significant association between health literacy and disability was found only in the analysis comparing generations of Canadians. People with higher health literacy were less likely to report disability. However, its effect was largely accounted for by education, employment status and income.
The results of this analysis are consistent with previous research that shows that first-generation immigrants have a health advantage over third-plus generation (Newbold and Danforth 2003; Newbold 2005; Hyman 2007). Although their lower odds of reporting disability declined with the inclusion of different control factors, it remained significant. The results point to the role of unmeasured factors like cultural differences in diets and health behaviors (Rosenmöller et al. 2011; Girard and Sercia 2013). For example, relative to non-immigrants, Canadian immigrants have lower rates of alcohol consumption (McDonald 2006; Veldhuizen et al. 2007), which is an important risk factor for poor health including disability (LaCroix et al. 1993). The results of the analysis among the first generation only by source country suggest that the expected decline in health among immigrants as posited by the healthy immigrant hypothesis is also not consistent across all groups. In particular, immigrants not from Europe or USA enjoyed a health advantage regardless of their duration in Canada. The results also suggest differences in unmeasured factors between immigrant groups.
This analysis has confirmed the results of previous studies that low health literacy has negative effect on poor health outcomes including disability (Lincoln et al. 2006; Guerra and Shea 2007; Baker et al. 2007). In the Canadian context, health literacy is considered a social determinant of health. It is therefore not surprising that its effect on self-rated disability was mostly mediated by education, employment status and income. Education is a pre-requisite for developing health literacy, while employment provides the opportunity to both develop and enhance health literacy in the course of doing one’s job (Desjardins 2003; Statistics Canada and Organisation for Economic Co-operation and Development 2005). Employment could expose individuals to a social environment in which they participate and are exposed to additional sources of health-related information such as from colleagues or occupational health programs. This suggests that it is not just having a job that is important, but engaging in literacy practices in the course of doing one’s job. Income, on the other hand, is not only an important determinant of health; it can provide the means to access opportunities for developing and strengthening one’s health literacy (Baker et al. 2004, 2007). For example, income can enable individuals to purchase health literacy enhancing resources including magazines and books, and to engage in health literacy-related activities. The lack of relationship between health literacy and physical disability among immigrants could be attributable to the fact that health literacy is low in this group (Canadian Council on Learning 2008), and also a reflection of the healthy immigrant effect.
Besides income and education, the other control factors that were significantly associated with disability were age, gender, and CMA of residence. All these factors fall within the framework of the social determinants of health (Commission on Social Determinants of Health (CSDH) 2008). As would be expected, both income and education had a protective effect on disability in this study. SES characteristics like income and education, however, do not directly affect disability, but operate through other factors such as lifestyle choices (smoking, alcohol consumption, diet, or physical exercise) or psychological factors (perceived helplessness, social support and perceived discrimination) (Everson et al. 2002; Hagen et al. 2006; Luong et al. 2012; Newbold and Neligan 2012). For example, studies have shown that obesity and low physical exercise are associated disability (Baumgartner et al. 2004; Peters et al. 2005). There was a gradient in the relationship between age and disability with people younger than age 65 being less likely to report disability. This is consistent with aging-related decline in physical functioning. The result that women were less likely to report disability, however, contradicts previous research that showed men to be at a higher risk of reporting disability (Murtagh and Hubert 2004; Louie and Ward 2010; Hosseinpoor et al. 2012). Our results may reflect differences with the other studies in the definition of disability and the type of data used or that Canadian women are indeed less likely to report disability than men. Nonetheless, understanding why this is so deserves further study. Most immigrants to Canada settle in the three largest cities of Toronto, Montreal and Vancouver. This analysis showed that people living in the other CMAs and in non-CMAs were at higher risk of reporting disability. The reasons behind this are not readily apparent and deserve further analysis. However, it is possible that place of residence reflects the extent of access to health services that may enable those with low health literacy to overcome their disability.
Several limitations, however, are associated with this study. First, because the IALSS was not primarily a health survey, it did not collect information on relevant health outcomes and risk factors like smoking, physical activity, alcohol consumption, and body mass index. The estimated differences between the first and third-plus generations are likely to attenuate if these factors were included as adjusters. Second, the small sample size of first-generation immigrants does not permit a detailed analysis of immigrants beyond the broad categories we used here. A large sample size, however, would allow researchers to conduct country specific analysis to illuminate the design of culturally appropriate programs targeting immigrants. Third, although culture could be an important factor in self-reported disability, our data did not have any cultural variables that could test this effect. In addition, a larger sample would allow for an ethnic-based analysis that would serve the purpose of demonstrating the role of culture in health literacy and self-reported disability. Last, this study assumed a unidirectional association from health literacy to disability. However, it is well known that people with disabilities, including learning disabilities, have lower health literacy. It is possible then that there is a reverse association between disability and health literacy. Nonetheless, examining whether this is the case requires longitudinal data, which is currently not available in Canada.
Conclusion
This study was based on a relatively large sample of generations of immigrants and, therefore, permitted us to empirically examine differences in disability by immigrant generation and region of origin and recency of arrival in Canada, and the role of health literacy in this relationship.
The study used data from people living in the community and hence best approximates what would be expected on the relationship between health literacy and health outcomes. Further, by comparing across three generations of immigrants, the study provided a basis for assessing both the short-term and long-term impacts of immigration on health literacy and disability.
For the overall population, high school education or higher, employment status, and income appeared to mediate the relationship between health literacy and disability. This suggests that although efforts to improve health literacy could benefit everyone, people with less than high school education and those that are more likely to not be working will benefit more. Among first-generation immigrants, health literacy did not have a significant effect on disability pointing to the healthy immigrant effect. However, this is likely to change as their duration of residence in Canada increases and points to the need to focus efforts in improving both their language skills and designing culturally appropriate health information especially given the increasing diversity in the Canadian immigrant population. While age, gender, education, employment, income, and place of residence are all part of the social determinants of health, these factors work jointly with immigrant status and language in their relationship with disability. Nevertheless, the relative importance of immigrant status in the web of relationship within the social determinants of health in general, and of disability in particular would require further research.
References
Acevedo-Garcia D, Pan J, Jun HJ, Osypuk TL, Emmons KM (2005) The effect of immigrant generation on smoking. Soc Sci Med 61:1223–1242
Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, Ren J, Peel J (2004) Health literacy and use of outpatient physician services by Medicare Managed Care enrollees. J Gen Int Med 19:215–220
Baker DW, Wolf MS, Feinglass J, Thompson JA, Gazmararian JA, Huang J (2007) Health literacy and mortality among elderly persons. Arch Int Med 167:1503–1509
Baumgartner RN, Wayne SJ, Waters DL, Janssen I, Gallagher D, Morley JE (2004) Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res 12:1995–2003
Beiser M (2005) The health of immigrants and refugees in Canada. Can J Public Health 96:S30–S44
Canadian Council on Learning (2007) Health literacy in Canada: initial results from the international adult literacy and skills survey. Canadian Council on Learning, Ottawa
Canadian Council on Learning (2008) Health literacy in Canada: a healthy understanding. Canadian Council on Learning, Ottawa
Chui T, Maheux H, Tran K (2007) Immigration in Canada: a portrait of the foreign-born population, 2006 Census. Catalogue No. 97-557-XIE. Statistics Canada, Ottawa
CSDH (2008) Closing the gap in a generation: health equity through action on the social determinants of health. World Health Organization, Geneva
Desjardins R (2003) Determinants of literacy proficiency: a lifelong-lifewide learning perspective. Int J Edu Res 39:205–245
Everson SA, Maty SC, Lynch JW, Kaplan GA (2002) Epidemiologic evidence for the relation between socioeconomic status and depression, obesity, and diabetes. J Psychosom Res 53:89–895
Girard A, Sercia P (2013) Immigration and food insecurity: social and nutritional issues for recent immigrants in Montreal, Canada. Int J Migr Health Soc Care 9:32–45
Guerra CE, Shea JA (2007) Health literacy and perceived health status in Latinos and African Americans. Ethn Dis 17:305–312
Hagen KB, Tambs K, Bjerkedal T (2006) What mediates the inverse association between education and occupational disability from back pain?—a prospective cohort study from the Nord-Trøndelag health study in Norway. Soc Sci Med 63:1267–1275
Hjern A, Allebeck P (2002) Suicide in the first- and second-generation immigrants in Sweden: a comparative study. Soc Psychiatry Epidemiol 37:423–429
Hosseinpoor AR, Williams JS, Jann B, Kowal P, Officer A, Posarac A, Chatterji S (2012) Social determinants of sex differences in disability among older adults: a multi-country decomposition analysis using the World Health Survey. Int J Equity Health 11:52 (http://www.equityhealthj.com/content/11/1/52. Accessed 28 June 2014)
Hyman I (2007) Immigration and health: reviewing evidence of the healthy immigrant effect in Canada. CERIS Working Paper No. 55, Toronto
LaCroix AZ, Guralnik JM, Berkman LF, Wallace RB, Satterfield S (1993) Maintaining mobility in late life. II. Smoking, alcohol consumption, physical activity, and body mass index. Am J Epidemiol 137:858–869
Lincoln A, Paasche-Orlow MK, Cheng DM, Lloyd-Travaglini C, Caruso C, Saitz R, Samet JH (2006) Impact of health literacy on depressive symptoms and mental-health related: quality of life among adults with addiction. J Gen Int Med 21:818–822
Louie GH, Ward MM (2010) Sex disparities in self-reported physical functioning: true differences, reporting bias, or incomplete adjustment for confounding? J Am Geriatr Soc 58:1117–1122
Luong ML, Cleveland RJ, Nyrop KA, Callahan LF (2012) Social determinants and osteoarthritis outcomes. Aging Health 8:413–437
Marmot MG, Syme SL (1976) Acculturation and coronary heart disease in Japanese Americans. Am J of Epidemiol 104:225–247
McDonald JT (2006) The health behaviours of immigrants and native-born people in Canada. Atlantic Metropolis Centre Working Paper Series No. 01–06, Fredericton
Murtagh KM, Hubert HB (2004) Gender differences in physical disability among an elderly cohort. Am J of Public Health 94(8):1406–1411
Newbold KB (2005) Self-rated health within the Canadian immigrant population: risk and the healthy immigrant effect. Soc Sci Med 60:1359–1370
Newbold KB, Danforth J (2003) Health status and Canada’s immigrant population. Soc Sci Med 57:1881–1895
Newbold KB, Neligan D (2012) Disaggregating Canadian immigrant smoking behaviour by country of birth. Soc Sci Med 75:997–1005
Ng E, Wilkins R, Gendron F, Berthelot J-M (2005) The changing health of immigrants, Can Social Trends (spring) 15–19 (http://www.statcan.gc.ca/pub/11-008-x/2005002/article/8454-eng.pdf. Accessed 10 June 2014)
Nutbeam D (2000) Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int 15:259–267
Omariba DWR, Ng E (2011) Immigration, generation and self-rated health in Canada: on the role of health literacy. Can J Public Health 102(4):281–285
Paasche-Orlow MK, Wolf MS (2007) The causal pathways linking health literacy to health outcomes. Am J Health Behav 31:S19–S26
Peters TJ, Sanders C, Dieppe P, Donovan J (2005) Factors associated with change in pain and disability over time: a community-based prospective observational study of hip and knee osteoarthritis. Br J Gen Pract 55:205–211
Pottie K, Ng E, Spitzer D, Mohammed A, Glazier R (2008) Language proficiency, gender and self-reported health: an analysis of the first two waves of the Longitudinal Survey of Immigrants to Canada. Can J Public Health 99:505–510
Rootman I, Ronson B (2005) Literacy and health research in Canada: where have we been and where should we go? Can J Public Health 96:S62–S77
Rosenmöller DL, Gasevic D, Seidel J, Lear SA (2011) Determinants of changes in dietary patterns among Chinese immigrants: a cross-sectional analysis. Int J Beh Nutr Phy Act 8:42. http://www.ijbnpa.org/content/8/1/42. Accessed 24 June 2014)
Rudd R, Kirsch I, Yamamoto K (2004) Literacy and health in America. Policy Information Center, Education Testing Service, Princeton
Statistics Canada (2013) Immigration and ethnocultural diversity in Canada. Ottawa, Statistics Canada (http://www12.statcan.gc.ca/nhs-enm/2011/as-sa/99-010-x/99-010-x2011001-eng.pdf. Accessed 24 June 2014)
Statistics Canada and Human Resources and Social Development Canada (2005) Building our competencies: Canadian results of the international adult literacy and skills survey. Catalogue No.89-617-XIE. Statistics Canada, Ottawa
Statistics Canada and Organisation for Economic Co-operation and Development (2005) Learning a living: first report of the adult literacy and Statistics Canada lifeskills survey. Statistics Canada and Organisation for Economic Co-operation and Development, Paris and Ottawa
Steele L, Lemieux C, Clark J, Glazier R (2002) The impact of policy changes on the health of recent immigrants and refugees in the inner city. Can J Public Health 93:118–122
Stewart M, Anderson J, Beiser M, Mwakarimba E, Neufeld A, Simich L, Spitzer D (2008) Multicultural meanings of social support among immigrants and refugees. Int Mig 46:123–159
Sudore RL, Mehta KM, Simonsick EM, Harris TB, Newman AB, Satterfield S, Rosano C, Rooks RN, Rubin SM, Ayonayon HN, Yaffe K (2006) Limited literacy in older people and disparities in health and healthcare access. J Am Geriatr Soc 54:770–776
Veldhuizen S, Urbanoski K, Cairney J (2007) Geographical variation in the prevalence of problematic substance use in Canada. Can J Psychiatry 52:426–433
Vissandjée B, Weinfeld M, Dupere S, Abdool S (2001) Sex, gender, ethnicity, and access to health care services: research and policy challenges for immigrant women in Canada. J Int Migr Integr 2:55–75
Von Wagner C, Semmler C, Good A, Wardle J (2009) Health literacy and self-efficacy for participating in colorectal cancer screening: the role of information processing. Pat Edu Counseling 75:352–357
Zanchetta MS, Poureslami IM (2006) Health literacy within the reality of immigrants, culture and language. Can J Public Health 97:S26–S30
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Omariba, D.W.R., Ng, E. Health literacy and disability: differences between generations of Canadian immigrants. Int J Public Health 60, 389–397 (2015). https://doi.org/10.1007/s00038-014-0640-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-014-0640-0