
Abstract
Objectives
To investigate differences in expression of surface markers, cytokine profiles, and presence of CD4+CD8+ T cells in skin-derived T cell cultures from patients with extrinsic atopic dermatitis (AD), intrinsic AD, and psoriasis expanded in the presence of IL-2 and IL-4.
Material
Skin biopsies from patients with extrinsic AD (n = 6), intrinsic AD (n = 9) and psoriasis (n = 9).
Methods
Skin-derived T cell cultures were analyzed for expression of six surface markers, 11 intracellular cytokines, and three T cell subtype signature transcription factors by flow cytometry, and secreted cytokines by multiplex.
Results
A different IFN-γ profile emerged between the extrinsic AD and psoriatic T cell cultures; however, there was no difference in IL-17 profile. No differences with regard to cytokine expression were found between extrinsic AD and intrinsic AD cultures; however, cutaneous lymphocyte-associated antigen was expressed by a higher percentage of CD8+ than CD4+ T cells in the intrinsic AD cultures. Double-positive CD4+CD8+ T cells were only detected in two out of 15 AD cultures.
Conclusion
The data suggest that IL-2 and IL-4 affects the cytokine profile during culture. Earlier findings of substantial levels of double-positive CD4+CD8+ T cells in skin derived T cell cultures from AD skin was not reproduced in this study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Atopic dermatitis (AD) is an inflammatory skin disease with an underlying barrier defect in addition to a deregulated immune response, leading to the development of eczematous, pruritic lesions. Patients with AD can be divided into two groups: extrinsic AD, characterized by an increased total IgE level, and intrinsic AD with normal total IgE levels. AD is characterized by heavy infiltration of T cells in the skin [1] that together with keratinocytes can result in continuous cytokine secretion leading to chronic lesions. Acute AD lesions are dominated by Th2 cytokines as IL-4, IL-5, IL-13 and the Th22 cytokine IL-22, whereas more chronic lesions involve increased expression of the Th1-associated cytokines IFN-γ and IL-12 [2, 3]. Skin-derived T cell numbers from punch biopsies are unpredictable, and it is therefore a great advantage if these can be multiplied for extensive investigative and mechanistic studies. Bang et al. [4] and Hashizume et al. [5] expanded skin-derived T cells by placing skin biopsies from AD patient in media containing IL-2 and IL-4. In contrast to psoriatic skin-derived T cell cultures, Bang et al. [4] found increased levels of CD4+CD8+ T cells in AD skin-derived T cell cultures, which they related to immature T cells from the thymus in AD patients. CD4+CD8+ expression is a thymocyte marker, thus these CD4+CD8+ T cells could indicate a dysregulated thymus in AD patients which is also supported by the finding that the size of thymi in children with AD decline slower than do thymi from healthy children [6]. Since skin-derived T cell cultures cannot be established from normal skin by use of IL-2 and IL-4 [4], investigators have used psoriasis as controls for studies of atopic dermatitis. Psoriasis is an inflammatory skin disease considered to be partially divergent from AD with regard to the T cell subsets involved in their underlying immune response, with Th17 and Th1 cytokines dominating psoriatic lesions [7].
We aimed at studying the divergence in a broad range of cytokines and cell surface markers between extrinsic and intrinsic AD and psoriatic lesions in skin-derived T cell cultures. First, we asked whether a difference in cytokine profiles of extrinsic AD and intrinsic AD skin-derived T cell cultures could be found. Secondarily, we investigated the presence of CD4+CD8+ cells in the T cell cultures with the aim of exploring phenotypic differences between CD4+CD8+, CD4+ and CD8+ T cells in regards to expression of surface markers and cytokine production.
Methods
Patients
Seventeen patients with AD, diagnosed according to the criteria of Hanifin and Rajka [8] and 11 psoriasis patients [Psoriasis Area and Severity Index (PASI) 5.2 ± 2.3, age 42 ± 17; male/female 5/6] each donated three punch biopsies from lesional skin (two 3-mm and one 4-mm) and a blood sample. Use of systemic and topical immunosuppressants was not allowed 1 month and 2 weeks prior to sampling, respectively. Seven patients with AD were characterized as having extrinsic AD based on their total IgE >200 kU/l [total IgE 1642 ± 2246 (mean ± SD); Eczema Area and Severity Index (EASI) 10.4 ± 8.8, age 34 ± 13; male/female 2/5] and ten had intrinsic AD [total IgE 64 ± 54; EASI 3.1 ± 2, age 26 ± 7; male/female 3/7]. The EASI score for the extrinsic AD group was significantly higher than for the intrinsic AD group (p < 0.01, Mann–Whitney U test). Eight healthy controls (age 29 ± 8; male/female 6/2) each donated two punch biopsies and a blood sample. [All subjects gave written informed consent in accordance with the Declaration of Helsinki Principles for Human Tissue Research, and the study was approved by the local ethics committee (H-04-2011-068) and the Danish Data Protection Agency.]
T cell cultures
T cell cultures were established by placing a 4-mm punch biopsy in culture flask containing 5 ml RPMI-1640 supplemented with 10 % sterile filtered human AB serum, IL-2 (1000 U/ml), IL-4 (250 U/ml), penicillin (100 U/ml), streptavidin (100 µg/ml), and l-glutamine (1 mM) and kept at 37 °C. Fresh media with cytokines was added to the cultures three times a week or as needed, so that the cells were diluted to a concentration of 0.5 × 106 cells/ml.
Blood cell purification
Peripheral blood mononuclear cells (PBMCs) were purified from blood using lymphoprep (Axis-Shield Poc AS, Oslo, Norway) density centrifugation. Cells were centrifuged with lymphoprep for 15 min at 1000g at 17 °C. Subsequently, cells were washed four times, for 5 min at 600, 500, 400, and 300g respectively, using PBS+ [PBS without Ca2+ and Mg2+ (Invitrogen, Carlsbad, USA), supplemented with 0.5 % (v/v) ethylene diamine tetra acetate (Bie & Berntsen, Rødovre, DK) and 0.5 % (v/v) human serum albumin (ZLB Behring GmbH, Marburg, GE)]. PBMCs were analyzed for surface marker expression by flow cytometry subsequent to purification, whereas PBMCs for intracellular flow cytometry analysis were stored overnight before analysis at 37 °C in RPMI-1640 supplemented with 10 % sterile filtered human AB serum, penicillin (100 U/ml), streptavidin (100 µg/ml), and l-glutamine (1 mM) at a concentration of 1 × 106 cells/ml.
Flow cytometry
Skin-derived T cells were cultured without IL-4 for 24 h prior to analysis. Cells used for intracellular staining were re-stimulated with 25 ng/ml phorbol 12-myristate 13-acetate (Sigma-Aldrich) and 1 µg/ml ionomycin (Sigma-Aldrich) for 6 h and 10 µg/ml Brefeldin A (Sigma-Aldrich) was included for the last 4 h of incubation. All cells were stained with LIVE/DEAD fixable red dead cell stain kit (Invitrogen) according to the manufacturer’s protocol. For surface staining, cells were incubated with antibodies (abs) (Online Resource Table S1) or corresponding isotype controls for 15 min at room temperature. For intracellular staining, cells were fixed and permeabilized with IntraPrep from Beckman Coulter (Fullerton, CA, USA) according to the manufacturer’s protocol and stained with abs against intracellular targets together with abs specific for CD4 and CD8. For proliferation analysis, cells were stained with carboxyfluorescein diacetate succinimidyl ester (CFSE) approximately 72 h before surface marker staining. Cells were analyzed by a Beckman Coulter FC500 MPL flow cytometer (Beckman Coulter). Recommended compensation beads (Invitrogen) were used according to the manufacturer’s protocol for compensation of the FACS data prior to data analysis using FlowJo from Treestar (Ashland, OR, USA).
Supernatant analysis
For supernatant analysis, cells were cultured for 24 h without IL-4 and the supernatant was stored at −80 °C. Supernatants were analyzed for the following cytokines: IL-1β, IL-4, IL-5, IL-6, IL-9, IL-10, IL-12, IL-13, IL-21, IL-22, IL-25 (IL-17E), IL-17A, IL-17F, IL-31, IL-33, IFN-γ, and TNF-α by multiplex magnetic bead assay (BioRad, Berkeley, CA, USA), according to the manufacturer’s protocol on a Bio-Plex 200 System using Bio-Plex Manager 5.0 (BioRad).
Immunohistochemistry
Biopsies were embedded in paraffin and stained by immunohistochemistry (IHC) with mouse anti-human CD4 (clone 4B12, Dako, Denmark; 1:40) or mouse anti-human CD8 (clone 144B, Dako, Denmark; 1:100). Negative controls excluding the primary antibody were conducted for all stainings. For further detail of the staining procedure see Online Resource Methods S1. Stained slides were scanned using a NanoZoomer 2.0 HT (Hamamatsu Photonics, Germany) and Visiopharm software (Visiopharm, Denmark) was used to assess the stained area (µm2) positive for CD4 and CD8, respectively, normalized to the length of the biopsy.
Statistical analysis
Statistics were calculated using GraphPad PRISM version 5. For all data except IHC data, Mann–Whitney U test was used for comparison of two groups, and Kruskal–Wallis with Dunn’s multiple comparison test was used when comparing several groups. The IHC data were log transformed and two groups were compared by two-tailed unpaired t tests, whereas several groups were compared using 1-way ANOVA with Tukey’s multiple comparison test.
Results
T cell cultures
Proliferating T cell cultures were established from 9 out of 13 biopsies from patients with psoriasis and from 15 out of 17 biopsies from patients with AD. From two patients with psoriasis cultures were established from two skin biopsies per patient, whereas for all patients with AD one culture was established per patient. Five biopsies from patients with psoriasis and two from patients with AD did not develop into proliferating cultures. T cell cultures reached 10 × 107 cells in 25 ± 4 (mean ± SD; n = 11) days, whereas the psoriatic cultures needed 30 ± 13 (mean ± SD; n = 6) days (Online Resource Fig. S1), similar to what has been found by others [9]. Eight biopsies (four from patients with AD and four from patients with psoriasis) were split in two and cultured in media with IL-4 and without IL-4. For the biopsies kept in media without IL-4 transient proliferation was only seen in one (max. 1.7 × 106 T cells) of the eight cultures, whereas continuously proliferating cultures were established from seven of the eight biopsies in media with IL-4, demonstrating the importance of IL-4 to induce sustained proliferation. All established cultures were analysed once a week after proliferation was apparent, which happened on day 20 and 25 for AD and psoriatic cultures, respectively. The presented data are from the first analysis of each culture. The first three AD and five psoriatic cultures were analysed by flow cytometry for the following markers: BDCA2, CD1a, CD14, and CD19, representing plasmacytoid dendritic cells, Langerhans cells, monocytes, and B cells. The percentage of positive cells for any of these markers was insignificant (mean ± SD, AD cultures 0.06 ± 0.07, psoriasis cultures 0.16 ± 0.15).
Cytokine analysis
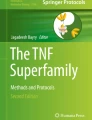
In the psoriatic cultures, a significantly higher percentage of the CD4+ T cells produced IFN-γ compared to the percentage of IFN-γ producing CD4+ T cells in the extrinsic AD cultures (p < 0.05). IFN-γ production was also found in a few of the intrinsic AD CD4+ T cells and the percentage of CD8+ T cells positive for IFN-γ showed a tendency similar to that of the CD4+ T cells (Fig. 1; Online Resource Table S2). Concordantly, IFN-γ was detected in the supernatant in two of nine psoriatic cultures, but not in any of the 15 AD cultures (Table 1). Also, a tendency towards higher percentages of t-bet+ and IFN-γ+t-bet+ CD4+ and CD8+ T cells was seen for the psoriatic cultures compared to the extrinsic AD cultures (p ≤ 0.15) (Online Resource Table S2). However, few cells were found to be positive for IL-17 and its transcription factor RORγt (Online Resource Table S2). No significant difference was detected for any of the other measured transcription factors or cytokines neither intracellularly or in the supernatant (Table 1, Online Resource Table S2). The cytokines IL-9, IL-12, IL-21, IL-25, IL-17A, IL-17F, and IL-33 could not be quantified in the supernatants of any culture. IL-22 was only quantifiable in media from a single extrinsic AD culture and IL-31 in two intrinsic AD cultures, and these cytokines were not detected in any of the psoriatic cultures. No differences were found comparing the cytokine profile of T cell cultures derived from extrinsic AD and intrinsic AD skin.

Higher intracellular levels of IFN-γ in psoriatic CD4+ skin-derived T cells compared to extrinsic AD CD4+ skin-derived T cells. a Percentage of CD4+ skin derived T cells positive for IFN-γ. b Percentage of CD8+ skin derived T cells positive for IFN-γ. c Representative dot plot of skin-derived T cells from psoriatic skin. First plot gating of CD4+ and CD8+ T cells; second plot gating of IFN-γ+ and t-bet+ within the CD4+ population. d Representative dot plot of skin-derived T cells from AD skin. First plot gating of CD4+ and CD8+ T cells; second plot gating of IFN-γ+ and t-bet+ within the CD4+ population. Bars mean ± SEM. ADex extrinsic AD, ADin intrinsic AD, Pso psoriasis. *p < 0.05
Surface marker expression
All cells in all cultures expressed CD45RO, and thus were characterized as memory cells; in a single culture all cells were double positive for CD45RO and CD45RA (Online Resource Table S3). In the intrinsic AD cultures, the percentage of CD8+ T cells expressing the skin homing marker cutaneous lymphocyte-associated antigen (CLA) was significantly higher (p = 0.0127) than the percentage of CD4+ T cells expressing CLA (Fig. 2a; Online Resource Table S3), which was not seen for the extrinsic AD or psoriatic cultures. This finding was not reflected by a higher percentage of CD8+ T cells in the intrinsic AD skin-derived T cell cultures, and significantly higher percentages of CD3+CD4+ T cells in blood from patients with intrinsic AD expressed CLA compared to CD3+CD8+ T cells (Fig. 2b). An equivalent result was seen in blood T cells from healthy subjects, with a similar tendency for patients with extrinsic AD (p = 0.095) and psoriasis (p = 0.093). Quantification of the area of lesional skin staining positive for CD8 and CD4 respectively, by IHC, showed that the CD8+ and CD4+ areas were comparable both within and across all patient groups (Fig. 2c, d). In contrast, the CD4+ area was significantly higher than the CD8+ area in the healthy skin (Mann–Whitney U test). As expected the percentage of CD4+ T cells in the blood was significantly higher than the percentage of CD8+ T cells in all four groups (p < 0.05, Mann–Whitney U test). Comparing all groups (1-way ANOVA with Tukey’s multiple comparison test) the CD8+ area was significantly increased in all three lesional samples compared to healthy skin, which was not the case for the CD4+ area (p < 0.05, not shown on graph). This shows that the increase in percentages of CD8+CLA+ cells in the intrinsic AD skin-derived T cell cultures did not exhibit as increased infiltration of CD8+ cells in intrinsic AD lesional skin. No differences in expression of CD25, CRTH2, and CD56 were found between groups (Online Resource Table S3).

Increased cutaneous lymphocyte-associated antigen (CLA) expression on intrinsic AD skin-derived CD8+ T cells from skin-derived T cell cultures is not reflected in blood and do not cause increased staining of CD8 in lesional skin. a Percentages of CD4+ and CD8+ cells in skin-derived T cell cultures expressing CLA. b Percentages of CD3+CD4+ and CD3+CD8+ T cells in blood expressing CLA. Representative dot plots from staining of skin-derived T cells and blood: Online Resource Fig. S2. c Area of skin biopsies stained positive for CD4 and CD8, respectively, by immunohistochemistry, normalized to the length of the biopsy. d Representative staining with CD4 (left column) and CD8 (right column) of healthy skin, and lesional AD and psoriatic (Pso) skin. Scale bars 500 µm. Error bars mean ± SEM. ADex extrinsic AD, ADin intrinsic AD, Pso psoriasis. *p < 0.05 (a, b Mann–Whitney U test, c 1-way ANOVA with Tukey’s multiple comparison test)
Distribution and proliferation of CD4+, CD8+, and CD4+CD8+ subsets
The percentages of CD4+CD8+ cells were <2 % regardless of disease with the exception of one extrinsic AD and one intrinsic AD culture where the CD4+CD8+ T cells comprised 22.9 and 5.8 % of the respective cultures. The majority of the cultures developed into either pure CD4+ or CD8+ T cell cultures (Online Resource Fig. S3) as also found by Hashizume et al. [5]. Immunohistochemical staining of CD4+ and CD8+ cells was performed on skin biopsies sampled from the same lesional area as biopsies used to establish T cell cultures. Quantification of the stained area showed that the dominating T cell subset in a specific lesion was also predominant in the corresponding culture. When CD4+ and CD8+ cells were equally present in the lesions, the cultures varied between CD4 and CD8 dominance. These changes were confirmed by proliferation analysis of CFSE stained cell samples from each culture (Online Resource Fig. S4). For each culture, histograms of the CFSE profile for the CD4+, CD8+, and CD4+CD8+ subsets were compared and found to be predictive for changes in CD4 versus CD8 dominance.
Discussion
In this study, the distribution of T cell subsets in skin-derived T cell cultures from patients with AD and psoriasis was investigated by a large number of cytokines and surface markers. A difference in IFN-γ profiles was found between skin-derived T cell cultures from patients with extrinsic AD and psoriasis, and a significantly higher percentage of CD8+ compared to CD4+ T cell expressed CLA in the intrinsic AD cultures. No difference in cytokine profiles was found for cultures established from extrinsic AD and intrinsic AD skin. Only in two out of 15 AD cultures, a substantial level of CD4+CD8+ T cells were found. The psoriasis-associated cytokine IL-17 was not detected in any of the cultures, suggesting that the high levels of IL-2 and IL-4 in the media may have suppressed the phenotype of the psoriatic Th/c 17 cells. Likewise the IL-2 and IL-4 in the media might have skewed the cytokine profile of other T cell subsets originally present in these biopsies, thereby clouding differences in cytokine profiles between T cell cultures derived from psoriasis, extrinsic AD and intrinsic AD skin. Nograles et al. [7] isolated fresh T cells from dermis of AD and psoriatic lesions and Hijnen et al. [10] derived T cells by skin explant cultures of patients with AD and psoriasis. In accordance with our results, these studies found increased levels of IL-4 and IL-13 in AD T cells and of IFN-γ in psoriatic T cells. However, in contrast to our results they also found increased levels of IL-17 in the psoriatic T cells. As IL-4 has been found to down regulate production of IL-17 and IFN-γ in vitro [11, 12], we expect that the IL-4 in the media has affected IL-17- and also to some degree IFN-γ-producing cells towards a Th2 phenotype. These data were confirmed by detection of GATA3, IL-5, and IL-13 in the psoriatic cultures. Although AD is characterized as a Th2 disease, other T cells subsets are also known to be involved. These might have been differentiated into Th2/Tc2 cells or been outcompeted by highly proliferative Th2/Tc2 cells. In this study, we were not able to establish proliferating T cell cultures when omitting IL-4 from the media. Bang et al. [4] tried to reduce the concentrations of IL-2 and IL-4 and to replace IL-4 with the T cell proliferative IL-7; however, both resulted in decreased proliferation. Hashizume et al. [5] compared the use of IL-2 and IL-4 with that of anti-CD3/CD28 antibody coated microbeads for establishment of skin-derived T cell cultures, and found the proliferation induced by anti-CD3/CD28 inferior to that induced by IL-2 and IL-4. Clark et al. [13] induced antigen-independent proliferation in skin-derived T cells from healthy skin by adding IL-2 and IL-15 to the media. However, Bang et al. [4] found that IL-2 and IL-4 in the media could neither induce migration and proliferation of skin T cells from healthy skin nor proliferation of lymphocytes from peripheral blood of patients with AD, indicating that IL-2 and IL-4 selectively promote expansion of in vivo activated and thus disease-associated T cells.
CLA is a skin-homing marker expressed primarily by memory T cells [14]. Comparable to other studies [15, 16], we found higher percentages of CD4+ than CD8+ T cells expressing CLA in blood from healthy controls and patients with AD, but in contrast to these studies we did not see increased expression of CLA on blood CD4+ T cells from patients with AD compared to healthy subjects. However, the latter might be due to our patients having mild AD (EASI <10 for all except one patient), as only the level of circulating CD4+CLA+ T cells from patients with severe AD has been found to be significantly higher from normal blood [16]. For the healthy controls, the increased expression of CLA on blood CD4+ T cells was reflected in the skin as increased CD4 staining compared to CD8 staining, whereas no difference in CD4 and CD8 staining was seen for the lesional skin samples. This is in contrast to a study [17], finding ratios >1.5 for CD4:CD8 in blood and skin from patients with both extrinsic and intrinsic AD. Significantly lower CLA+CD4:CD8 ratio in AD skin-derived T cell cultures compared to AD PBMCs have previously been found [15], which is in line with our finding for the intrinsic AD cultures where a higher percentage of CD8+ than CD4+ T cells expressed CLA; conversely, not reflected as an increased percentage of CD8+ cells in our intrinsic AD skin-derived cultures compared to the extrinsic AD and psoriatic cultures. In this study, double staining of CLA with CD4 and CD8, respectively, was not performed. However, if the increased percentage of CLA+ CD8+ T cells in the intrinsic AD cultures is a reflection of the lesional skin, the difference might be explained by the increased severity score of the extrinsic AD group. As the discussion above together with other studies [10, 18] indicate that the majority of CD8+CLA+ in diseased skin may be epidermal resident T cells whereas the CD4+CLA+ are circulating between the skin and blood, patients with an increased AD severity score may have an increased percentages of CD4+CLA+ infiltrating their skin, resulting in a decreased CLA+CD4:CD8 ratio.
In AD skin-derived T cell cultures, Bang et al. [4] found the average percentage of CD4+CD8+ T cells to be 26 %. In this study, CD4+CD8+ T cells were only found in two out of 15 established AD cultures, and no difference in detection was found when comparing the antibodies used by Bang et al. [4] to ours. CD4+CD8+ T cells have been found in various diseases as cancers, inflammatory diseases, and viral infections [19–22]. Flamand et al. [21] found that stimulation of purified CD8+ T cells with superantigens produced by Staphylococcus aureus induced CD4 expression on 26–59 % of CD8+ T cells, and colonization with superantigen-producing S. aureus has been found to correlate with increasing severity score (SCORAD) in AD patients [23]. The cultures from Bang et al. [4] were donated from patients with moderate to severe AD, whereas our patients had a low mean EASI score. Thus, the patients from Bang et al. [4] were more likely to have been colonized with superantigen-producing S. aureus. If the CD4+CD8+ T cells are induced by superantigens, these merely represent an inflammatory signature rather than a cell type especially associated with development of AD.
In summary, establishment of skin-derived T cell cultures using IL-2 and IL-4 is effective when large amount of cells are needed. Although their cytokine profile does not completely resemble that of the lesional skin, these skin-derived T cells may prove useful for studies of more stable T cell characteristics as T cell receptor specificity. Furthermore, earlier findings of substantial levels of double-positive CD4+CD8+ T cells in skin derived T cell cultures from AD skin was not reproduced in this study.
References
Ellingsen AR, Sorensen FB, Larsen JO, Deleuran MS, Thestrup-Pedersen K. Stereological quantification of lymphocytes in skin biopsies from atopic dermatitis patients. Acta Derm Venereol. 2001;81:258–62.
Gittler JK, Shemer A, Suarez-Farinas M, et al. Progressive activation of T(H)2/T(H)22 cytokines and selective epidermal proteins characterizes acute and chronic atopic dermatitis. J Allergy Clin Immunol. 2012;130:1344–54.
Hamid Q, Naseer T, Minshall EM, Song YL, Boguniewicz M, Leung DY. In vivo expression of IL-12 and IL-13 in atopic dermatitis. J Allergy Clin Immunol. 1996;98:225–31.
Bang K, Lund M, Wu K, Mogensen SC, Thestrup-Pedersen K. CD4+ CD8+ (thymocyte-like) T lymphocytes present in blood and skin from patients with atopic dermatitis suggest immune dysregulation. Br J Dermatol. 2001;144:1140–7.
Hashizume H, Hansen A, Poulsen LK, Thomsen AR, Takigawa M, Thestrup-Pedersen K. In vitro propagation and dynamics of T cells from skin biopsies by methods using interleukins-2 and -4 or anti-CD3/CD28 antibody-coated microbeads. Acta Derm Venereol. 2010;90:468–73.
Olesen AB, Andersen G, Jeppesen DL, Benn CS, Juul S, Thestrup-Pedersen K. Thymus is enlarged in children with current atopic dermatitis. A cross-sectional study. Acta Derm Venereol. 2005;85:240–3.
Nograles KE, Zaba LC, Shemer A, et al. IL-22-producing “T22” T cells account for upregulated IL-22 in atopic dermatitis despite reduced IL-17-producing TH17 T cells. J Allergy Clin Immunol. 2009;123(1244–52):e2.
Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol. 1980;Suppl 92:44–7.
Bang K, Lund M, Mogensen SC, Thestrup-Pedersen K. In vitro culture of skin-homing T lymphocytes from inflammatory skin diseases. Exp Dermatol. 2005;14:391–7.
Hijnen D, Knol EF, Gent YY, et al. CD8(+) T cells in the lesional skin of atopic dermatitis and psoriasis patients are an important source of IFN-gamma, IL-13, IL-17, and IL-22. J Invest Dermatol. 2013;133:973–9.
Newcomb DC, Boswell MG, Zhou W, et al. Human TH17 cells express a functional IL-13 receptor and IL-13 attenuates IL-17A production. J Allergy Clin Immunol. 2011;127(1006–13):e1–4.
Yamaguchi E, de Vries J, Yssel H. Differentiation of human single-positive fetal thymocytes in vitro into IL-4- and/or IFN-gamma-producing CD4+ and CD8+ T cells. Int Immunol. 1999;11:593–603.
Clark RA, Chong BF, Mirchandani N, et al. A novel method for the isolation of skin resident T cells from normal and diseased human skin. J Invest Dermatol. 2006;126:1059–70.
Picker LJ, Michie SA, Rott LS, Butcher EC. A unique phenotype of skin-associated lymphocytes in humans. Preferential expression of the HECA-452 epitope by benign and malignant T cells at cutaneous sites. Am J Pathol. 1990;136:1053–68.
Akdis M, Simon HU, Weigl L, Kreyden O, Blaser K, Akdis CA. Skin homing (cutaneous lymphocyte-associated antigen-positive) CD8+ T cells respond to superantigen and contribute to eosinophilia and IgE production in atopic dermatitis. J Immunol. 1999;163:466–75.
Dworzak MN, Froschl G, Printz D, et al. Skin-associated lymphocytes in the peripheral blood of patients with atopic dermatitis: signs of subset expansion and stimulation. J Allergy Clin Immunol. 1999;103:901–6.
Akdis CA, Akdis M, Simon D, et al. T cells and T cell-derived cytokines as pathogenic factors in the nonallergic form of atopic dermatitis. J Invest Dermatol. 1999;113:628–34.
Cheuk S, Wiken M, Blomqvist L, et al. Epidermal th22 and tc17 cells form a localized disease memory in clinically healed psoriasis. J Immunol. 2014;192:3111–20.
Desfrancois J, Derre L, Corvaisier M, et al. Increased frequency of nonconventional double positive CD4CD8 alphabeta T cells in human breast pleural effusions. Int J Cancer. 2009;125:374–80.
Desfrancois J, Moreau-Aubry A, Vignard V, et al. Double positive CD4CD8 alphabeta T cells: a new tumor-reactive population in human melanomas. PLoS One. 2010;5:e8437.
Flamand L, Crowley RW, Lusso P, Colombini-Hatch S, Margolis DM, Gallo RC. Activation of CD8+ T lymphocytes through the T cell receptor turns on CD4 gene expression: implications for HIV pathogenesis. Proc Natl Acad Sci USA. 1998;95:3111–6.
Parel Y, Aurrand-Lions M, Scheja A, Dayer JM, Roosnek E, Chizzolini C. Presence of CD4+CD8+ double-positive T cells with very high interleukin-4 production potential in lesional skin of patients with systemic sclerosis. Arthritis Rheum. 2007;56:3459–67.
Nada HA, Gomaa NI, Elakhras A, Wasfy R, Baker RA. Skin colonization by superantigen-producing Staphylococcus aureus in Egyptian patients with atopic dermatitis and its relation to disease severity and serum interleukin-4 level. Int J Infect Dis. 2012;16:e29–33.
Acknowledgments
Britta C. Martel is supported by LEO Pharma A/S. The authors wish to thank the patients and healthy controls for their participation in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
In relation to this manuscript, all authors declare that they have no conflicts of interest.
Additional information
Responsible Editor: Bernhard Gibbs.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Martel, B.C., Dyring-Andersen, B., Skov, L. et al. Different cytokine profiles of skin-derived T cell cultures from patients with atopic dermatitis and psoriasis. Inflamm. Res. 65, 265–272 (2016). https://doi.org/10.1007/s00011-015-0912-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-015-0912-z