
Abstract
Objective
This study aimed to assess the chondroprotective potential of atorvastatin in rat’s cartilage explant culture model of osteoarthritis, stimulated by interleukin-1β (IL-1β).
Materials and methods
The cartilage explants were treated with 20 ng/ml IL-1β alone or with 20 ng/ml IL-1β + various concentration of atorvastatin (1, 3, or 10 µM dissolved in DMSO) and incubated at 37 °C for 24 h. Also, control (0.25 % DMSO), stimulated (20 ng IL-1β) and treatment (atorvastatin 10 µM) cartilage explants were incubated without and with 1400W (10 µM). After 24 h of incubation, TNF-α, PGE2, MMP-13, TIMP-1, NO, and superoxide anion formation (O2 −) concomitant with glycosaminoglycans (GAGs) were estimated in the medium.
Results
Atorvastatin inhibited IL-1β-induced GAGs release, TNF-α, MMP-13, and O2 − with no effect on TIMP-1 and NO. In addition, the source of NO in normal and atorvastatin-treated cartilage was eNOS, while for IL-1β-stimulated cartilage it was iNOS. The cartilage degradation was associated with the combined effects of increased NO and O2 − rather than only NO.
Conclusion
The present study suggests that atorvastatin has the ability to protect cartilage degradation following IL-1β-stimulated cartilage in in vitro OA model and supports additional therapeutic application of atorvastatin in OA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) is a major cause of disability in aged people worldwide [1]. Progressive degeneration of the cartilage is one of the hallmarks of OA. Unfortunately, despite extensive research, the etiology of OA is poorly known and its treatment is still restricted to analgesics and non-steroidal anti-inflammatory drugs (NSAIDs) which are based on symptoms rather than underlying causes [2]. Therefore, a need to develop an alternative option which could modify or reverse the progression of cartilage degradation in affected joint is warranted.
Previously, OA was considered as a degenerative disease; however, due to the presence of inflammatory cytokines, immunoglobulin and other mediators in the joints, the role of inflammation in disease progression in cartilage degeneration has been widely accepted [3–5]. Tumor necrosis factor-α (TNF-α) and interleukin-1 beta (IL-1β)-mediated inflammatory cascade led to the production of matrix metalloproteinases (MMPs) and nitric oxide (NO). The role of MMPs through enzymatic cleavage together with cytokines in the initiation and progression of cartilage destruction had been demonstrated [6, 7]. The elevated NO levels cause hyperalgesia through prostaglandins (PGs)-mediated sensitization of nociceptors to other mediators [8, 9]. Furthermore, the extent of extracellular matrix (ECM) degradation is also highly associated with an imbalance between MMPs and tissue inhibitors of matrix metalloproteinases (TIMPs) [10]. Hence, a therapeutic approach regulating the inflammation and MMPs/TIMPs balance could be effective in the treatment of OA.
IL-1β, a proinflammatory cytokine—one of the most catabolic factors which plays a vital role in the pathogenesis of OA [11] through enhanced production of MMPs, inhibition of TIMPs [12, 13] and also by suppressed synthesis of ECM and increased apoptosis, thus inhibiting cartilage repair process [7]—has been extensively used to establish OA model in cartilage and chondrocytes [14, 15].
Statins (HMG-CoA reductase inhibitors) are widely used therapeutically in patients with hyperlipidemia in cardiovascular disease [16, 17]; however, lipid-independent beneficial effects of statins have also been recognized [17]. In addition, the beneficial effects of statins have also been demonstrated through its anti-inflammatory activity [18–20] and its ability to inhibit MMPs [21–23]. These properties of statins have been used to modify inflammatory disease states such as rheumatoid arthritis (RA) [24, 25]. Based on these properties of statins, we hypothesized that atorvastatin, a most widely prescribed statin, may have the potential to prevent degeneration of articular cartilage. Thus, in the present study, we investigated the potential of atorvastatin to protect cartilage against the imbalance of MMP-13/TIMP-1, inflammation and NO in an IL-1β-mediated OA model in cartilage explant culture.
Materials and methods
Animals
Adult male albino Wistar rats (180–250 g) were procured from the Laboratory Animal Resource Section of the institute. Experimental protocol and animal husbandry were conducted according to ethical principles and ethical guidelines of the CPCSEA. All animal experiments were duly approved by the Institute Animal Ethics Committee.
Cartilage explant culture
Articular cartilages (femoral head) were obtained surgically under sterile conditions from adult rats and submerged in complete medium (DMEM, supplemented with heat-inactivated 10 % fetal bovine serum (FBS); 100 unit/ml of penicillin; 10 µg/ml streptomycin). After rinsing several times with complete medium, the cartilage explants were then incubated for 24 h at 37 °C in a humidified 5 % CO2/95 % air incubator for stabilization. After 24 h, the medium was replaced with serum-free medium (DMEM, supplemented 100 unit/ml of penicillin; 10 µg/ml streptomycin without FBS). The cartilage were placed in 24-well plates and treated with various concentration of atorvastatin (Glenmark, India) followed by challenging with rat IL-1β. The cartilage explants were treated with 20 ng/ml IL-1β alone or with 20 ng/ml IL-1β + various concentrations of atorvastatin (1, 3, or 10 µM dissolved in 25 % DMSO to make a final concentration of 0.25 % DMSO) and incubated at 37 °C for 24 h. In parallel, explants were also cultured with DMSO (final concentration 0.25 %) without IL-1β and atorvastatin and were used as normal control (0.25 % DMSO control). To know the effect of NO and its sources, control (0.25 % DMSO), stimulated (20 ng IL-1β), and treatment (atorvastatin 10 µM) explants’ culture of cartilage were incubated without and with 1400W (10 µM). The supernatants were collected at 24 h and stored at −20 °C until use.
MTT assay for cartilage viability
The concentration of atorvastatin for our study was determined by cartilage viability test using MTT [26]. Articular cartilage of rats (femoral head) were placed in 24-well plate and incubated with various log doses of atorvastatin (1, 3, 10, 30, 100, and 300 µM dissolved in DMSO, with the final concentration of DMSO not more than 0.25 %) for 24 h at 37 °C in a humidified 5 % CO2/95 % air incubator. Cartilage explants were removed from medium, weighed, and incubated in 200 µl of a 0.1 % (w/v) solution of MTT in phosphate buffer saline at 37 °C for 4 h. After removal of MTT, the dye crystals were solubilized in extraction buffer (1000 µl of 96 % isopropanol and 4 % 1 M hydrochloric acid) for an additional 30 min at room temperature. The resulting solution was read on a spectrophotometer at an absorbance of 563 nm. The cartilage viability was expressed as absorbance at 563 nm/mg cartilage/ml of isopropyl alcohol. The results were expressed as viable cartilage (% of normal control) assuming 100 % of cartilage viability of normal control.
Enzyme-linked immunosorbent assay (ELISA)
The levels of TNF-α (Koma Biotech Inc. South Korea), PGE2 (Cayman chemical, USA), MMP-13, and TIMP-1 (Genetix Biotech Asia Pvt. Ltd.) in the harvested explant culture media after 24 h were quantified using ELISA kits according to the manufacturer’s instructions. Values were expressed as picograms per milligram of wet cartilage. A best-fit linear standard curve was developed for TNF-α (R 2 ≥ 0.999), PGE2 (R 2 ≥ 0.994), MMP-13 (R 2 ≥ 0.972), and TIMP-1 (R 2 ≥ 0.998).
Glycosaminoglycan (GAG) degradation assay
GAG levels in the explant culture medium were determined by the amount of polyanionic material reacting with 1, 9-dimethylmethylene blue (DMMB) [27], using shark chondroitin sulfate (Sigma-Aldrich, USA) as the standard. The samples were examined spectrophotometrically at 540 nm. The results were expressed as microgram GAG released into the medium per milligram of the cartilage tissue (wet weight).
Measurement of NO
Nitrite, a stable product of NO, was analyzed in culture medium, using the spectrophotometric method at 545 nm based on the Griess reaction [28]. The concentration of nitrite (µM/l) was measured from the standard curve and results were expressed as µM nitrite released into the medium per milligram wet weight of the cartilage tissue.
Measurement of superoxide anion (O2 −) formation
O2 − formation was indirectly estimated spectrophotometrically at 540 nm as reduced nitroblue tetrazolium which forms formazan as an index of superoxide anion generation [29]. The results were expressed as picomole/min/mg cartilage
Statistical analysis
The results were expressed as mean ± standard error of means (SEM) followed by one-way ANOVA along with Tukey’s multiple comparison tests using Graph Pad Prism Version-4.0 software. A p value <0.05 was considered to be statistically significant.
Results
Cartilage viability assay
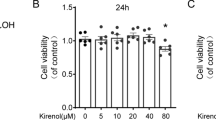
In the present study, cartilage viability was found to be 120, 117, 130, 90, 31, and 12 % respectively at 1, 3, 10, 30, 100, and 300 µM concentration of atorvastatin as compared to normal control cartilage (Fig. 1).

Effect of atorvastatin on cartilage viability in cartilage explant culturesn. Cartilage explants were treated with various concentrations of atorvastatin (1, 3, 10, 30, 100, and 300 µM) dissolved in DMSO (final concentration 0.25 %) for 24 h, followed by MTT assay. n = 5. Relative viability of atorvastatin-treated cartilage was expressed in percentage (%) of control group as 100 %. ATR atorvastatin
Atorvastatin inhibits the IL-1β-induced production of inflammatory cytokines
Inflammatory cytokines such as TNF-α and inflammatory product PGE2, estimated by ELISA, were increased significantly, compared to control group (0.25 % DMSO) in the cartilage explant culture media in response to IL-1β challenge (Fig. 2). Atorvastatin at 3 and 10 µM significantly decreased TNF-α and PGE2 levels.

Effect of atorvastatin on the levels of TNF-α (a) and PGE2 (b) in IL-1β-induced cartilage explant culturesn. Cartilage explants were treated with IL-1β (20 ng/ml) or/and various concentration of atorvastatin (1, 3 and 10 µM) for 24 h, followed by ELISA. n = 6. The vertical lines at the top of the bars represent the SEM. The bars bearing no superscript in common differ significantly (p < 0.05). ATR atorvastatin
Effect of atorvastatin on MMP-13 and TIMP-1 in IL-1β-induced cartilage explant cultures
IL-1β enhanced MMP-13, but decreased TIMP-1 production in cultured cartilage explants (Fig. 3). Atorvastatin at 3 and 10 µM significantly inhibited the IL-1β-induced increased production of MMP-13; however, no effect was observed on TIMP-1 at any concentration of atorvastatin used in the present study.

Effect of atorvastatin on the activity of MMP-13 (a) and TIMP-1 (b) in IL-1β- induced cartilage explant culturesn. Cartilage explants were treated with IL-1β (20 ng/ml) or/and various concentration of atorvastatin (1, 3 and 10 µM) for 24 h, followed by ELISA. n = 6. The vertical lines at the top of the bars represent the SEM. The bars bearing no superscript in common differ significantly (p < 0.05). ATR atorvastatin
Effect of atorvastatin on GAGs, O2 −, and nitrite production in IL-1β-induced cartilage explant cultures
GAGs, O2 −, and nitrite production were significantly enhanced after IL-1β challenge to the cartilage. Atorvastatin at 3 and 10 µM significantly inhibited the IL-1β-induced increased production of GAGs and O2 −; however, no such effects were observed on nitrite at any concentration of atorvastatin in the present study (Fig. 4).

Effect of atorvastatin on the activity of GAGs release (a), O2 − formation (b), and nitrite production (c) in IL-1β- induced cartilage explant culturesn. Cartilage explants were treated with IL-1β (20 ng/ml) or/and various concentration of atorvastatin (1, 3 and 10 µM) for 24 h, followed by DMMB assay for GAGs, NBT reduction method for O2 −, and the Griess reaction assay for nitrite. n = 6. The vertical lines at the top of the bars represent the SEM. The bars bearing no superscript in common differ significantly (p < 0.05). ATR atorvastatin
Effect of 1400W on nitrite, O2 −, and GAGs production in normal, IL-1β-stimulated, and atorvastatin-treated cartilage in explant culture
Figure 5 depicts the effects of 1400W (10 µM) on nitrite, O2 −, and GAGs production in normal, IL-1β-stimulated and atorvastatin-treated cartilage in explant culture medium. 1400W did not cause any alteration in basal level nitrite, GAGs, and O2 − production in control groups (0.25 % DMSO). IL-1β stimulation caused significant increased production of nitrite, O2 −, and GAGs compared to control groups (0.25 % DMSO) which were significantly decreased by 10 µM 1400W. Atorvastatin (10 µM) significantly increased nitrite, but not O2 − and GAGs production as compared to control (0.25 % DMSO) and all these were not altered significantly by 1400W.

Effect of 1400W on nitrite production (a), O2 − formation (b), and GAGs release (c) in normal, IL-1β-stimulated, and atorvastatin-treated cartilage explant culturesn. Normal, stimulated (20 ng IL-1β), and atorvastatin (10 µM)-treated cartilage were incubated alone and with 1400W (10 µM) for 24 h, followed by Griess reaction assay for nitrite, NBT reduction method for O2 −, and DMMB assay for GAGs. n = 6. The vertical lines at the top of the bars represent the SEM. The bars bearing no superscript in common differ significantly (p < 0.05). ATR atorvastatin
Discussion
In the present study, we demonstrated the potential anti-inflammatory and chondroprotective effects of atorvastatin at multiple dose levels in IL-1β-induced cartilage degradation in an in vitro OA model.
Pain control, restoration of joint function, and the prevention of the cartilage degradation process are the prime goals of pharmacological treatment of OA. Unfortunately, at present, there is no available therapy to stop or reverse the cartilage degradation process. The current pharmacologic treatment of OA mainly aims to alleviate symptoms and therapy and thus remains unsatisfactory [30, 31]. NSAIDs have been used clinically for the past few years to treat arthritic disease; however, their potential adverse effects and the negative effects on cartilage make their use controversial [32, 33]. Therefore, development of alternative therapies with few side effects along with possible inhibition of cartilage degradation is needed.
Statins are widely used for preventing cardiovascular diseases. Although the lipid-lowering activity of statins is responsible in preventing cardiovascular diseases, the anti-inflammatory and immunomodulatory effects of statins independent of their lipid-lowering activity have been reported clinically and experimentally [34–37]. Furthermore, a beneficial effect of statins including atorvastatin in chronic inflammatory condition such as RA by inhibiting inflammatory markers has also been reported in patients [38, 39] and experimentally [24, 40].
Osteoarthritis like RA is another chronic inflammatory condition characterized by joint inflammation with concomitant destruction of cartilage. However, little is known about the effect of statins on cartilage. In fact, recently the chondroprotective effect of simvastatin [39, 41, 42] and pravastatin [43] has been evaluated on IL-1β-stimulated chondrocytes culture. The effect of atorvastatin had also been studied at higher concentrations (10 and 50 µmol/l) in chondrocytes [44]. To date, the chondroprotective efficacy of atorvastatin, a commonly used statin on cartilage explants, has not been investigated. Therefore, we aimed to evaluate the effect of atorvastatin at multiple doses on IL-1β-induced inflammatory cytokines, MMP-13/TIMP-1 alteration, and ROS such as O2 − and NO production and its correlation with cartilage degradation in an in vitro model of articular cartilage in this study. The choice of atorvastatin was based on the effectiveness of this drug in chronic inflammation models in rats and humans [34, 38]. The concentrations of DMSO and atorvastatin were selected for the study on the basis of % cartilage viability test by MTT assay (Fig. 1). Mitochondrial enzyme activity-based MTT assay is a good indicator of cell viability, regardless of cell cycle state. It is rapid, non-expensive, and reproducible which does not need any radioisotope and had been used previously to assess the viability of cartilage [26]. Indeed, the lack of uniform penetration of MTT in the cartilage explants may be a limiting factor of the assay; however, in the present study the cell viability of atorvastatin was compared with the control cartilage (% of control) to make the assay reliable. Although we did not evaluate the viability of the cartilage treated with IL-1 β, the concentration of IL-1β used in this study was selected on the basis of previous report [45]. The concentration we used had no adverse effect on cartilage viability as revealed by increased levels of O2 −, NO, and GAGs in explant culture medium, which are believed to be produced in live cartilage on stimulation with IL-1β.
The pathogenesis of OA involves the combined effects of mechanical stress and biochemical and genetic factors. In contrast to rheumatoid arthritis, OA is defined as a noninflammatory arthropathy. However, various evidences supports the involvement of inflammation in OA as evidenced by the presence of cytokines such as interleukin IL-1β and TNF-α in both the rheumatoid and osteoarthritic joints and synovial fluid [46], thus opening a new and potential target for its therapeutic intervention. Our finding of increased proinflammatory cytokines, TNF-α and its product PGE2, concomitant with enhanced degradation of cartilage as evidenced by increased GAGs by catabolic factor IL-1β, further supports the roles of inflammation in OA. In the present study, the inhibitory effects of atorvastatin on IL-β induced cartilage degradation through marked reduction of inflammatory cytokines may be important in devising new approaches for the prevention and treatment of OA as demonstrated earlier [44, 47]. The observed inhibitory effect of atorvastatin in this study in IL-1β-induced cartilage degradation may be due to its anti-inflammatory or antioxidative potential noted with other statins [24].
Although the etiology of OA is not completely understood, imbalanced MMPs and TIMPs have a vital role in the ECM turnover and breakdown under normal and disease conditions [48]. Excessive production of MMPs have a key role in OA progression through cartilage matrix destruction [49, 50]. Among the various MMPs, MMP-13 is of particular interest because of its elevated levels in osteoarthritic synovial fluid and more efficient to cleave proteoglycans (GAGs) and type II collagen, the major components of the cartilage matrix [48]. MMP-13 deficient mice are resistant to osteoarthritic cartilage erosion further supporting the role of MMP-13 in OA [51]. Excessive MMPs-mediated tissues breakdown is mainly controlled by irreversible binding of MMPs with endogenous TIMPs [52]. In chondrocytes and synovial cells, inhibition of MMPs is mainly mediated through a glycoprotein TIMP-1. Synthesis and secretion of MMPs by chondrocytes in response to stimulants including IL-1β and TNF-α [53, 54] indicate their therapeutic value in the treatment of OA. We, therefore, aimed to elucidate the effect of atorvastatin on IL-1β induced cartilage degradation by regulating MMP-13/TIMP-1 activity.
In the present study, we observed an increased MMP-13 and decreased TIMP-1 activity in IL-1β-induced cartilage explant. Atorvastatin is able to reverse the imbalance of MMP-13/TIMP-1; however, this was achieved by the reduction of MMP-13 rather than increased TIMP-1. The inhibition of MMP-13, concomitant with decreased GAGs, a marker of cartilage degradation by atorvastatin, suggests its ability to protect against IL-β-mediated cartilage degradation. In the present study, chrondroprotection by atorvastatin was achieved at two levels: one, by direct inhibition of MMP-13 and the other by inhibition of inflammatory cytokines which are known to stimulate the synthesis and secretion of MMPs by chondrocytes [53, 54]. A similar effect of pravastatin [43], simvastatin [41, 47], and atorvastatin [44] had been reported in chondrocyte culture.
Increased production of various reactive oxygen species (ROS) and reactive nitrogen species (RNS) such as NO, O2 −, and peroxynitrite as a consequence of proinflammatory cytokine IL-1β [3, 55] and its role in cartilage destruction [56, 57] had been documented in earlier studies. These ROS and RNS cause substantial destruction of the cartilage matrix through increased production of proteolytic enzymes such as aggrecanases and MMPs after stimulation of chondrocytes. In the present study, we found increased NO and O2 − formation concomitant with increased GAGs in IL-1β-induced cartilage explant, supporting the roles of ROS in cartilage degradation. Surprisingly, despite increased levels of NO, atorvastatin was able to protect cartilage degradation as evidenced by decreased GAGs release in the explant medium. Indeed, decreased O2 − production by atorvastatin used in this study may be responsible for its chondroprotective effects, which are known to induce cartilage degradation. Although we did not assess peroxynitrite, the chondroprotective effects of atorvastatin by inhibition of peroxynitrite could not be ruled out as O2 −, a precursor of peroxynitrite was significantly decreased by atorvastatin and this observation is supported by antioxidative potential [24] and direct scavenging effect of O2 − [58] by atorvastatin.
We demonstrated the sources of NO in normal, IL-1β-stimulated, and atorvastatin-treated cartilage by use of 1400W, a selective iNOS inhibitor. The nitrite level in the control cartilage was unaffected by 1400W, indicating that the source of basal NO levels in normal cartilage is eNOS. Also, the increased nitrite levels in cartilage (unstimulated/normal) treated only with atorvastatin compared to the normal one, which was unaffected by 1400W, suggesting that the source for increased NO is eNOS rather than iNOS and confirm previous similar reports on cultured osteoarthritic chondrocytes [44]. The statin including atorvastatin had been reported to increase eNOS expression [17]. As expected, increased nitrite levels in IL-1β-stimulated cartilage compared to normal were significantly reduced by 1400W, suggesting that the source of increased NO was iNOS rather than eNOS as in an earlier finding in cultured osteoarthritic chondrocytes [44]. The increased production of NO by increased iNOS expression had been observed in IL-1β-stimulated cartilage [59] and chondrocytes in patients with OA [60, 61]. Furthermore, we evaluated cartilage degradation in terms of GAGs release and its correlation with O2 − formation and NO production by iNOS inhibitor 1400W in normal, stimulated, and atorvastatin-treated cartilage. It is interesting to note that the basal levels of nitrite, O2 −, and GAGs in normal cartilage were unaffected by 1400W; however, the increase in the levels of nitrite and O2 − along with GAGs in IL-1β-stimulated cartilage compared to normal was decreased by 1400W. Atorvastatin significantly increased nitrite, but not O2 − and GAGs production as compared to control. Neither the increased nitrite nor the normal levels of O2 − and GAGs were altered significantly by 1400W. This observation suggests that not increased NO, but increased NO along with O2 − is responsible for cartilage degradation, as observed in IL-1β-stimulated cartilage. Further, peroxynitrite generated by the combination of NO and superoxide contributes to a number of destructive events in cartilage including apoptosis [62, 63]. Our results are in agreement with a previous study where it was demonstrated that both NO and ROS are required for cartilage destruction, suggesting that NO alone may have beneficial effects on chondrocytes [61].
The effects of atorvastatin on most parameters were seen at concentrations in the range of 1–10 μM, with the maximum effect at 10 µM. These concentrations were not cytotoxic to the cartilage, as assessed by cartilage viability using MTT assay. Moreover, the effects observed at concentrations of atorvastatin used in our study are consistent with previous studies on in vitro model of OA for various statins [41, 43, 44, 47, 53, 54].
In conclusion, the present study suggests that atorvastatin has the ability to protect cartilage degradation following IL-1β-stimulated cartilage in an in vitro OA model. The chondroprotective effect of atorvastatin was mainly mediated through its anti-inflammatory action by decreasing cytokines, its inhibitory effects on MMP-13, and its ROS scavenging potential. In addition, the study further suggests that not only increased NO, but increased NO along with O2 − is responsible for cartilage degradation and supports the additional therapeutic application of atorvastatin in OA besides its major cholesterol-lowering effect.
Abbreviations
- MMP:
-
Matrix metalloproteinases
- TIMP:
-
Tissue inhibitors of matrix metalloproteinases
- TNF-α:
-
Tumor necrosis factor-α
- IL-1β:
-
Interleukin-1 beta
- PGE2 :
-
Prostaglandin E2
- NO:
-
Nitric oxide
- GAGs:
-
Glycosaminoglycans
- DMSO:
-
Dimethyl sulfoxide
- DMMB:
-
1, 9-dimethylmethylene blue
- MTT:
-
Methylthiazolyldiphenyl-tetrazolium bromide
- ROS:
-
Reactive oxygen species
References
Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646–56.
Baker CL, Ferguson CM. Future treatment of osteoarthritis. Orthopedics. 2005;28:227–34.
Pelletier JP, Martel-Pelletier J, Abramson SB. Osteoarthritis, an inflammatory disease: potential implication for the selection of new therapeutic targets. Arthritis Rheum. 2001;44:1237–47.
Hegemann N, Wondimu A, Kohn B, Brunnberg L, Schmidt MF. Cytokine profile in canine immune-mediated polyarthritis and osteoarthritis. Vet Comp Orthop Traumatol. 2005;18:67–72.
Sakkas LI, Platsoucas CD. The role of T cells in the pathogenesis of osteoarthritis. Arthritis Rheum. 2007;56:409–24.
Klatt AR, Klinger G, Neumüller O, Eidenmüller B, Wagner I, Achenbach T, Aigner T, Bartnik E. TAK1 downregulation reduces IL-1beta induced expression of MMP13, MMP1 and TNF-alpha. Biomed Pharmacother. 2006;60:55–61.
Pujol JP, Chadjichristos C, Legendre F, Bauge C, Beauchef G, Andriamanalijaona R, Galera P, Boumediene K. Interleukin-1 and transforming growth factor-beta 1 as crucial factors in osteoarthritic cartilage metabolism. Connect Tissue Res. 2008;49:293–7.
Higgins AJ, Lees P, Sedgwick AD. Development of equine models of inflammation. Vet Rec. 1987;120:517–22.
May SA, Lees P. Nonsteroidal anti-inflammatory drugs. In: McIlwraith CW, Trotter GW, editors. Joint disease in the horse. Philadelphia: Saunders WB; 1996. p. 223–37.
Burger D, Rezzonico R, Li JM, Modoux C, Pierce RA, Welgus HG, Dayer JM. Imbalance between interstitial collagenase and tissue inhibitor of metalloproteinases 1 in synoviocytes and fibroblasts upon direct contact with stimulated T lymphocytes: involvement of membrane-associated cytokines. Arthritis Rheum. 1998;41:1748–59.
Van der Kraan PM, van den Berg WB. Anabolic and destructive mediators in osteoarthritis. Curr Opin Clin Nutr Metab Care. 2000;3:205–11.
Mengshol JA, Vincenti MP, Coon CI, Barchowsky A, Brinckerhoff CE. Interleukin-1 induction of collagenase 3 (matrix metalloproteinase 13) gene expressions in chondrocytes require p38, c-Jun N-terminal kinase, and nuclear factor kappaB: differential regulation of collagenase 1 and collagenase 3. Arthritis Rheum. 2000;43:801–11.
Fernandes JC, Martel-Pelletier J, Pelletier JP. The role of cytokines in osteoarthritis pathophysiology. Biorheology. 2002;39:237–46.
Bau B, Gebhard PM, Haag J, Knorr T, Bartnik E, Aigner T. Relative messenger RNA expression profiling of collagenase and aggrecanases in human articular chondrocytes in vivo and in vitro. Arthritis Rheum. 2002;46:2648–57.
Roman-Blas JA, Contreras-Blasco MA, Largo R, Alvarez-Soria MA, Castañeda S, Herrero-Beaumont G. Differential effects of the antioxidant n-acetylcysteine on the production of catabolic mediators in IL-1beta-stimulated human osteoarthritic synoviocytes and chondrocytes. Eur J Pharmacol. 2009;623:125–31.
Smith DA, Galin I. Statin therapy for native and periinterventional coronary heart disease. Curr Mol Med. 2006;6:589–602.
Laufs U, La Fata V, Plutzky J, Liao JK. Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97:1129–35.
Collins P, Ford I, Croal B, Ball D, Greaves M, Macaulay E, Brittenden J. Haemostasis, inflammation and renal function following exercise in patients with intermittent claudicating on statin and aspirin therapy. Thromb J. 2006;4–9.
Stoll G, Bendszus M. Inflammation and atherosclerosis: novel insights into plaque formation and destabilization. Stroke. 2006;37:1923–32.
Coward WR, Marei A, Yang A, Vasa-Nicotera MM, Chow SC. Statin-induced proinflammatory response in mitogen-activated peripheral blood mononuclear cells through the activation of caspase-1 and IL-18 secretion in monocytes. J Immunol. 2006;176:5284–92.
Wilson WR, Evans J, Bell PR, Thompson MM. HMG-CoA reductase inhibitors (statins) decrease MMP-3 and MMP-9 concentrations in abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2005;30:259–62.
Thunyakitpisal PD, Chaisuparat R. Simvastatin, an HMG-CoA reductase inhibitor, reduced the expression of matrix metalloproteinase-9 (Gelatinase B) in osteoblastic cells and HT1080 fibrosarcoma cells. J Pharmacol Sci. 2004;94:403–9.
Luan Z, Chase AJ, Newby AC. Statins inhibit secretion of metalloproteinases-1, -2, -3, and -9 from vascular smooth muscle cells and macrophages. Arterioscler Thromb Vasc Biol. 2003;23:769–75.
Leung BP, Sattar N, Crilly A, Prach M, McCarey DW, Payne H, Madhok R, Campbell C, Gracie JA, Liew FY, McInnes IB. A novel anti inflammatory role for simvastatin in inflammatory arthritis. J Immunol. 2003;170:1524–30.
McKay A, Leung BP, McInnes IB, Thomson NC, Liew FY. A novel anti-inflammatory role of simvastatin in a murine model of allergic asthma. J Immunol. 2004;172:2903–8.
Csonge L, Bravo D, Newman-Gage H, Rigley T, Conrad EU, Bakay A, Strong DM, Pellet S. Banking of osteochondral allografts. Part I. Viability assays adapted for osteochondrol and cartilage studies. Cell Tissue Bank. 2002;3:151–9.
Farndale RW, Buttle DJ, Barrett AJ. Improved quantitation and discrimination of sulfated glycosaminoglycans by use of dimethylmethylene blue. Biochim Biophys Acta. 1986;883:173–7.
Sastry KVH, Moudgal RP, Mohan J, Tyagi JS, Rao GS. Spectrophotometric determination of serum nitrite and nitrate by copper–cadmium alloy. Anal Biochem. 2002;306:79–82.
Wang HD, Pagano PJ, Du Y, Cayatte AJ, Quinn MT, Brecher P, Cohen RA. Superoxide anion from the adventitia of the rat thoracic aorta inactivates nitric oxide. Circ Res. 1998;82:810–8.
Laufers S. Osteoarthritis therapy—are there still unmet needs? Rheumatology. 2004;43:i9–15.
Farkouh ME, Greenberg JD, Jeger RV, Ramanathan K, Verheugt FW, Chesebro JH, Kirshner H, Hochman JS, Lay CL, Ruland S, Mellein B, Matchaba PT, Fuster V, Abramson SB. Cardiovascular outcomes in high risk patients with osteoarthritis treated with ibuprofen, naproxen or lumiracoxib. Ann Rheum Dis. 2007;66:764–70.
Akhund L, Quinet RJ, Ishaq S. Celecoxib-related renal papillary necrosis. Arch Intern Med. 2003;163:114–5.
Stephen Y, Chang MD, Colin W, Howden MD. Is no NSAID a good NSAID? approaches to NSAID associated upper gastrointestinal disease. Curr Gastroenterol Rep. 2004;6:447–53.
Youssef S, Stuve O, Patarroyo JC, Rulz PJ, Radosevich JL, Hur EM, Bravo M, Mitchell DJ, Sobel RA, Steinman L, Zamvill SS. The HMG-CoA reductase inhibitors, atorvastatin, promote a Th2 bias and reverse paralysis in central nervous system autoimmune disease. Nature. 2002;420:78–84.
Garcia PJ. Pleiotropic effects of statins: moving beyond cholesterol control. Curr Atheroscler Rep. 2005;7:34–9.
Greenwood J, Steinman L, Zamvil SS. Statin therapy and autoimmune disease: from protein prenylation to immunomodulation. Nat Rev Immunol. 2006;6:358–70.
Van der Most PJ, Dolga AM, Nijholt IM, Luiten PG, Eisel UL. Statins: mechanisms of neuroprotection. Prog Neurobiol. 2009;88:64–75.
McCarey DW, McInnes IB, Madhok R, Hampson R, Sherbakova O, Ford I, Capell HA, Sattar N. Trial of atorvastatin in rheumatoid arthritis (TARA): double-blind, randomised placebo-controlled trial. Lancet. 2004;363:2015–21.
Dombrecht EJ, Van Offel JF, Bridts CH, Ebo DG, Seynhaeve V, Schuerwegh AJ, Stevens WJ, De Clerck LS. Influence of simvastatin on the production of proinfl amatory cytokines and nitric oxide by activated human chondrocytes. Clin Exp Rheumatol. 2007;25:534–9.
Barsantea MM, Roffea E, Yokorob CM, Tafuric WL, Souzab DG, Pinhoa V, Castrob MDSA, Teixeiraa MM. Anti-inflammatory and analgesic effects of atorvastatin in a rat model of adjuvant-induced arthritis. Eur J Pharmacol. 2005;516:282–9.
Lazzerini PE, Capecchi PL, Nerucci F, Fioravanti A, Chellini F, Piccini M, Bisogno S, Marcolongo R, Laghi PF. Simvastatin reduces MMP-3 level in interleukin 1b stimulated human chondrocyte culture. Ann Rheum Dis. 2004;63:867–9.
Yudoh K, Karasawa R. Statin prevents chondrocytes aging and degeneration of articular cartilage in osteoarthritis (OA). Aging. 2010;2:990–8.
Baker JF, Walsh PM, Byrne DP, Mulhall KJ. Pravastatin suppresses matrix metalloproteinase expression and activity in human articular chondrocytes stimulated by interleukin-1b. J Orthop Traumatol. 2012;13:119–23.
Simopoulou T, Malizos KN, Poultsides L, Tsezou A. Protective effect of atorvastatin in cultured osteoarthritic chondrocytes. J Orthop Res. 2010;28:110–5.
Palmer AW, Wilson CG, Baum EJ, Levenston ME. Composition-function relationships during IL-1-induced cartilage degradation and recovery. Osteoarthr Cartil. 2009;8:1029–39.
Westacott CI, Whicher JT, Barnes IC, Thompson D, Swan AJ, Dieppe PA. Synovial fluid concentration of five different cytokines in rheumatic diseases. Ann Rheum Dis. 1990;49:676–81.
Barter MJ, Hui W, Lakey RL, Catterall JB, Cawston T, Young DA. Lipophilic statins prevent matrix metalloproteinase-mediated cartilage collagen breakdown by inhibiting protein geranylgeranylation. Ann Rheum Dis. 2010;69:2189–98.
Burrage PS, Mix KS, Brinckerhoff CE. Matrix metalloproteinases: role in arthritis. Front Biosci. 2006;11:529–43.
Bluteau G, Gouttenoire J, Conrozier T, Mathieu P, Vignon E, Richard M, Herbage D, Mallein-Gerin F. Differential gene expression analysis in a rabbit model of osteoarthritis induced by anterior cruciate ligament (ACL) section. Biorheology. 2002;39:247–58.
Mengshol JA, Mix KS, Brinckerhoff CE. Matrix metalloproteinases as therapeutic targets in arthritic diseases: bull’s-eye or missing the mark? Arthritis Rheum. 2002;46:13–20.
Little CB, Barai A, Burkhardt D, Smith SM, Fosang AJ, Werb Z, Shah M, Thompson EW. Matrix metalloproteinase 13–deficient mice are resistant to osteoarthritic cartilage erosion but not chondrocyte hypertrophy or osteophyte development. Arthritis Rhemat. 2009;60:3723–33.
Cawston TE. Metalloproteinase inhibitors and the prevention of connective tissue breakdown. Pharmacol Ther. 1996;70:163–82.
Iannone F, Lapadula G. The pathophysiology of osteoarthritis. Aging Clin Exp Res. 2003;15:364–72.
Mandelbaum B, Waddell D. Etiology and pathophysiology of osteoarthritis. Orthopedics. 2005;28:207–14.
Loeser RF. Molecular mechanisms of cartilage destruction: mechanics, inflammatory mediators, and aging collide. Arthritis Rheum. 2006;54:1357–60.
John DR, Orrenius S. Role of mitochondria in toxic cell death. Toxicology. 2002;491–496.
Davies CM, Guilak F, Weinberg JB, Fermor B. Reactive nitrogen and oxygen species in interleukin-1-mediated DNA damage associated with osteoarthritis. Osteoarthr Cartil. 2008;16:624–30.
Bakogiannis C, Antoniades C, Tousoulis D, Demosthenous M, Antonopoulos AS, Psarros T, Ekonomopoulos G, Sfyras N, Channon KM. Atorvastatin directly reduces vascular superoxide generation in human vein grafts ex vivo, by improving eNOS coupling and reducing NADPH-oxidase activity. JACC. 2010;55:A51.E480–A51.E480.
Wahl SM, McCartney-Francis N, Chan J, Dionne R, Ta L, Orenstein JM. Nitric oxide in experimental joint inflammation. Benefit or detriment? Cell Tissue Organ. 2003;174:26–33. doi:10.1159/000070572.
Amin AR, Di Cesare PE, Vyas P, Attur M, Tzeng E, Billiar TR, Stuchin SA, Abramson SB. The expression and regulation of nitric oxide synthase in human osteoarthritis-affected chondrocytes: evidence for up-regulated neuronal nitric oxide synthase. J Exp Med. 1995;182:2097–102.
Melchiorri C, Meliconi R, Frizziero L, Silvestri T, Pulsatelli L, Mazzetti I, Borzi RM, Uguccioni M, Facchini A. Enhanced and coordinated in vivo expression of inflammatory cytokines and nitric oxide synthase by chondrocytes from patients with osteoarthritis. Arthritis Rheum. 1998;41:2165–74.
Del Carlo M, Loeser RF. Nitric oxide-mediated chondrocytes cell death requires the generation of additional reactive oxygen species. Arthritis Rheum. 2002;46:394–403.
Pacher P, Beckman JS, Liaudet L. Nitric oxide and peroxynitrite in health and disease. Physiol Rev. 2007;87:315–424.
Conflict of interest
All authors declare that they have no conflicts of interest concerning this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: John Di Battista.
Rights and permissions
About this article

Cite this article
Pathak, N.N., Lingaraju, M.C., Balaganur, V. et al. Anti-inflammatory and chondroprotective effects of atorvastatin in a cartilage explant model of osteoarthritis. Inflamm. Res. 64, 161–169 (2015). https://doi.org/10.1007/s00011-014-0794-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-014-0794-5