
Abstract
Prioritisation of diseases is an essential tool for policy-makers in charge of allocating resources for surveillance and control programmes or for research projects, to target diseases that need to be addressed ahead of others. Nevertheless, methods for prioritisation need to be transparent, standardised and repeatable to be effective and objective in setting priorities. To date, various models have been developed, experimenting different approaches, but it remains some room for improvement in the design of such tools. The definition of the criteria – indicators used to assess diseases regarding the objective of the prioritisation exercise – is one of the cornerstones of the efficiency of the methodology. In previous developed methods, this step was usually poorly addressed and up to now, no standardised method has been developed and described to select relevant and accurate criteria. Through the use of an electronic-based questionnaire to collect data about criteria from a large population of respondents, this study, based on the analysis of zoonoses and their impact in Southeast Asia, aimed at investigating an innovative approach to identify criteria that ensure a good differentiation between the diseases. The findings of this study highlighted that refining an initial list of criteria using multivariate analysis was a reliable approach to select clear, accurate and relevant criteria that allow a differentiation between diseases for a further prioritisation exercise. Furthermore, this study indicated that using an electronic-based questionnaire, carefully designed, might be an interesting alternative of expert opinion elicitation, for the collection of data. Finally, the results of this study opened to other new perspectives to develop and improve methods for the prioritisation of infectious diseases.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
In light of the fact that financial and human resources are limited, there is nowadays a general agreement at national, regional and international level that policy for prevention, surveillance and control of infectious diseases must be made cost effective by focusing on the most relevant risks for both animal and human populations (WHO 2006; OIE 2008; Cardoen et al. 2009). Nevertheless, decision making in controlling infectious diseases is a complex, conflicting process, characterised by a mixture of epidemiological, economical and social-ethical value judgements, and priority setting becomes a multidimensional problem in which technical information is often intertwined with those value judgements (Kurowicka et al. 2010; Ng and Sargeant 2013). In this context, in order to make the best use of limited human and financial resources, prioritisation is an efficient tool that can be used as an aid in making decisions for resource allocation in different areas, such as surveillance and control strategies and the formulation of key research questions. However, methods for prioritisation need to be transparent, standardised and repeatable to be effective in setting priorities. To date, various models have been developed, experimenting with different approaches, but there still remains some room for improvement in the design of such tools.
The definition of criteria is one of the cornerstones of the efficiency of a prioritisation exercise as they will support the assessment of the diseases and so their relative ranking. In previously developed methods, this step is usually poorly described. Criteria are selected either through bibliographic study (Kemmeren et al. 2006; Fosse et al. 2008; Krause 2008b; Eger et al. 2009; Havelaar et al. 2010) or through expert opinion (Capek et al. 2006; Perry et al. 2002; Defra 2006; WHO 2006; McKenzie et al. 2007; OIE 2008; Cardoen et al. 2009; Eger et al. 2009), but up to now, no standardised method has been developed and described to select relevant and accurate criteria.
After presenting and discussing the different methods and models for prioritisation of diseases, we propose to investigate an innovative approach to improve the choice of the criteria. Based on the analysis of zoonoses and their impact in Southeast Asia, this study used a web-based questionnaire to collect data on selection criteria from a large population of respondents and applied multivariate analysis to identify criteria that would ensure a clear and standardised differentiation between diseases and that could be used further on for a prioritisation exercise.
2 Methods for Prioritisation of Diseases
Methods for the prioritisation of infectious diseases had mainly two objectives, either identifying those diseases, which should be a priority focus of surveillance and control programmes, or selecting diseases, which should be addressed first in specific research programmes. Prioritisation exercises can focus on diseases currently present in the region of the study or on the most relevant hazards for the future, regarding environmental, economical and sociological changes (Discontools 2009). Three different approaches, qualitative, semi-quantitative and quantitative, can be used to support the different methods, but for whatever approach, all the models follow the same step-by-step outline.
2.1 A Step-by-Step Approach
The different steps that need to be rigorously followed to ensure an effective prioritisation exercise are the following:
-
Step 1. Setting a clear definition of the objective of the prioritisation exercise.
-
Step 2. Establishing the list of diseases that need to be ranked.
-
Step 3. Selecting the list of criteria against which the prioritisation is undergone (e.g. indicators that will be used to assess the importance of the disease regarding the objective of the prioritisation exercise).
-
Step 4. Allocating a score to each criterion: qualitative values, as low/medium/high for qualitative methods, quantitative scale (3–5 classes) for the semi-quantitative methods and true numerical values for quantitative methods.
-
Step 5. Applying a weighting system: allocate a weight to each criterion to take into account the relative importance of the criteria regarding each other and according to the objective of the prioritisation exercise.
-
Step 6. Aggregating the values of all criteria to obtain a total score per disease (methods range from very simple ones, such as summing weighted score, to more complex ones, such as aggregating probabilistic distributions of the scores).
-
Step 7. Ranking the disease from highest to lowest total score.
2.2 The Different Approaches for Prioritisation
Three approaches support the different methods for prioritisation.
2.2.1 Qualitative Approach
In this approach, criteria are assessed using qualitative value and data are then combined to obtain a total qualitative value per disease, regarding which the ranking is undergone.
Eger et al. (2009) use a qualitative approach for the prioritisation of diseases and target groups for integrated care measures at the national level of Austria. A catalogue of criteria is settled and assessed using literature review, grey literature and expert interviews. For each selected diseases, results are given in qualitative terms, such as average, clear, low, high, rising and existing. An expert workshop is then organised to value the criteria and the method, according to their experience and from the perspective of the national security. The final prioritisation process results in the summary of four weighted criteria for each of the selected disease. Diseases are then classified regarding three levels of priority.
Capek et al. (2006) use a qualitative method to prioritise non-food-borne zoonoses in order to allocate rationally resources for knowledge improvement, prevention and control, at the national scale of France. A preselected list of diseases is ranked regarding three criteria and using expert opinion. After discussion, a consensus is reached on the categorisation of diseases into three categories of different levels of priority.
2.2.2 Semi-quantitative Approach
The principle is quite similar to the one developed in quantitative approach but criteria are scored according to a scale: different classes are defined for each criterion and a numerical value is attributed to each class. Each criterion is classified into a class and so is allocated a numerical score. The sum of the scores leads to a total score per disease regarding which the diseases are ranked. The semi-quantitative approach has been largely used by organisations to settle a list of diseases on which surveillance and research programmes should focus on (Discontools 2009). Context and characteristics of the main semi-quantitative methods previously developed are presented in Table 14.1.
2.3 Quantitative Approach
In this approach, each criterion is associated with a true numerical value and then all the values are aggregated to give a total value regarding which the diseases are ranked. Methods based on a purely quantitative approach are still few.
Kemmeren et al. (2006) developed a quantitative model to help Dutch decision makers to establish the priority of pathogenic microorganisms that can be transmitted by food, as a basis for effective and efficient policy-making on control, prevention and surveillance. The hierarchic classification of diseases is based on the quantitative assessment of the burden of the disease and the cost of illness using an outcome tree for each pathogen. The estimation the disease burden and the cost of illness is proceeded using an incidence approach, i.e. calculating the present expected sum of current and future costs accruing to all incident cases of disease in a specific time period, taking into account age-specific disease risk and related illness costs.
Fosse et al. (2008) propose a quantitative method to prioritise food-borne zoonoses due to consumption of pork and beef meat, to support decision making in veterinary public health area. The method is based on the construction of a hazard typology and the calculation of a risk score for each selected hazards (combination of the incidence of human cases due to pork consumption and of the severity of the cases).
Havelaar et al. (2010) work on a general method to prioritise pathogens in order to support the development of early warning and surveillance systems of emerging zoonoses in the Netherlands. The quantitative method is based on a multi-criteria method that allows the combination of objective information on the epidemiology and societal impact of zoonotic pathogens with subjective information on the relative weights of different criteria. The risk score is based on seven epidemiological and societal criteria that cover the complete pathway from introduction to societal impact of the diseases. Authors decided to restrict the number of criteria to avoid the challenge to develop complex validated databases.
Brookes et al. (2014) use a multi-criteria framework, combining disease information with pig producer values, in order to rank exotic diseases for the pig industry in Australia, as a decision aid to identify priority research topics. Thirty diseases, pathogens and syndromes were identified and evaluated by the research team, according to 9 criteria, using information from a literature review. Weights of importance for the criteria were elicited using a survey targeting the pig industry stakeholders. Finally, the diseases are ranked according to their final mean score after the aggregation of weights of importance for the criteria with criteria measurements for each disease.
Ng and Sargeant (2013) present a zoonoses prioritisation method, based on conjoint analysis, which is a well-established quantitative method in market research to explore consumer preferences. The research team selected 21 criteria, for which three or four levels were assigned, depending on the quantitative data available in the literature, which could be quantitatively measured with scientific data in the literature. Sixty-two diseases were included in the study. Participants of a survey were proposed different disease combinations containing varying levels of 5 of the 21 criteria and were asked to select one zoonosis to prioritise for control and prevention in the country. The analysis of the data allowed to identify the relative importance of the criteria for the prioritisation of zoonotic diseases and led to the development of a robust weighted point-scoring system to rank diseases in order of priority. This preference elicitation method overcomes the need to assign arbitrary scores and subjective weights as relative weighted scores for each characteristic are derived from the choice data.
2.4 Analysis of the Advantages and Disadvantages of Each Approach
The qualitative approach is a quick and simple tool, easy to communicate to decision makers. However, all the methods described previously are very subjective and show a lack of repeatability and transparency and so can lead to important bias in the ranking of the disease.
The semi-quantitative approach increases transparency and repeatability compared with the qualitative approach, but methods developed so far remain subjective and arbitrary (Krause 2008b; Kurowicka et al. 2010). There is no objective basis to combine highly divergent criteria on the same scale and then simply add up or multiply all scores (Kemmeren et al. 2006) and the linear relation between the different scales of a criterion or between criteria are often assumed but not supported by data (Havelaar et al. 2010). Some methods have attempted to improve the differentiation between the diseases by increasing the number of scales in the scoring system. However, the difficulty to generate clear definitions for each scale increases with the number of scale and there might not be sufficient detailed information available for many diseases and criteria to allow such a differentiated approach (Krause 2008b). Furthermore, not all the criteria have the same importance when undergoing a prioritisation exercise, and so a relative weight needs to be applied (Krause 2008a). For the approaches in which a weighting system is applied, there is a widespread lack of transparency and objectivity in the way the weightings are attributed to criteria. Finally, most of the methods require inputs from expert groups for the scoring of the criteria. There is a high risk that the answers of these experts are biassed by their individual professional focus, and there is thus an important part of subjectivity in the final result of disease ranking (Krause 2008b).
The quantitative approach is less arbitrary than the semi-quantitative approach as the criteria are scored using natural values or an associated numerical scale. Also, all criteria are weighted in proportion to their true values, instead of given arbitrary numbers, and so the final ranking result is expected to be more accurate and realistic (Kurowicka et al. 2010). A disadvantage is that the process is very resource intensive, requiring careful consideration of a large volume of data, and many data gaps may exist. Such data gaps result in uncertainties about the final results, but the quantitative approach also helps to prioritise between data needs and to identify key research questions. To avoid the complexity of gathering a large amount of data, quantitative methods use a restricted number of criteria. Even if the authors tried to reach a high level of integration in the choice of the criteria to cover the wider range of features, they may have missed some components of the diseases that could contribute to the objective of their study (Brookes et al. 2014; Ng and Sargeant 2013). Nevertheless, according to Cox et al. (2005), simple quantitative models will often be more accurate and useful than qualitative risk rating, while requiring no more information than would be needed to assess, justify and interpret qualitative rating.
The previous literature study illustrates the three main approaches which have been used to prioritise diseases, each with their limitations: the qualitative approach which is subjective and unable to support accurate models reliably, the semi-quantitative approach which leads to reproducible but still somewhat arbitrary models and the quantitative approach which is more transparent and objective but requires a large amount of data. A summary of principles, advantages and disadvantages of the three different approaches is presented in Table 14.2.
3 An Innovative Approach to the Selection of Criteria for the Prioritisation of Diseases, Based on the Case Study of Zoonoses in Southeast Asia
3.1 Selection of the Zoonotic Diseases
In light of the expected large amount of zoonoses present in Southeast Asia, the scope of the study was restricted to: (1) zoonotic diseases for which animals still represent the main reservoir and source of the pathogens (e.g. exclusion of HIV, which became effectively and essentially transmissible from human to human after a single species jump), (2) zoonotic diseases for which species other than non-human primate species are commonly involved in disease transmission (e.g. exclusion of dengue and malaria), (3) food-borne diseases for which transmission to humans is due to primary contamination of raw animal products and (4) zoonotic diseases that can be transmitted from animals to humans, excluding those transmitted exclusively from humans to animals (e.g. H1N1). The geographical area of interest was continental Southeast Asia, consisting of Cambodia, two Southeastern Chinese provinces (Yunnan and Guangxi), Lao PDR, Myanmar, Thailand and Vietnam. The aim of this selection was not to end with an exhaustive list of zoonotic diseases occurring in this geographical area but to identify the most commonly described diseases, to serve as a basis for the study.
Regarding this case definition, searches of peer-reviewed literature were conducted using the PubMed database from January 1990 to September 2011. The scan involved searches for terms such as ‘zoonoses or zoonosis or zoonotic diseases Southeast Asia’, ‘emerging diseases Southeast Asia’, ‘bacteriosis Southeast Asia’, ‘virosis Southeast Asia’, ‘protozoosis Southeast Asia’, ‘mycosis zoonotic Southeast Asia’, ‘parasitosis Southeast Asia’, ‘unconventional agents Southeast Asia’, ‘food-borne Southeast Asia’ and ‘vector-borne Southeast Asia’.
3.2 Selection of the Criteria
The list of the criteria that were used as indicators to assess the different characteristics of the disease, as well as their different classes, was obtained through the study of a wide range of available prioritisation methods. In the context of prioritisation of zoonoses in Southeast Asia, a special focus was given to criteria that allow to assess diseases against a wide range of components at the human-animal-ecosystem interface (epidemiological features, animal and public health impact, socioeconomical impact) and take into account the cultural and economic issues of the region.
3.3 Web-Based Questionnaire
The questionnaire was a web-based survey, developed using the website SurveyMonkey©. Respondents entered it using an URL link. After providing details about their personal background and professional situation (position, organisation, disciplines, country of experience, specific expertise on zoonoses), respondents were asked to select a disease and, then, to choose the most appropriate class among the ones proposed for each criteria and to mention the level of confidence they had in their answer on a scale, ranging from 1 (low confidence in the answer) to 5 (very high confidence in their answer). The questionnaire was pretested on six experts to assess the explanation provided to recipients and the format of the questionnaire.
To define the population of recipients for the purpose of this study, a snowball sampling approach was used. The initial group of recipients was defined gathering different networks and sources, involving people working in the field of zoonoses in Southeast Asia. The questionnaire was sent to 204 people and they were asked to forward the questionnaire to people they might know with some expertise of zoonoses and working in Southeast Asia. The choice of this collection method was motivated by the need to collect as many answers as possible to support the study and by the fact that the identity of the respondents was not crucial (only their experience was taken into account for the interpretation of the results).
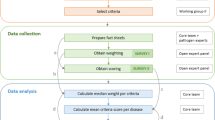
3.4 Data Analysis
Once the questionnaire was closed, all the surveys were downloaded from the website of SurveyMonkey© and the answers were displayed in an Excel© fact sheet. Only the complete questionnaires were taken into account for the study. A data matrix was obtained in which the respondents were identified with their IP address and criteria were considered as categorical variables (five modes per variable) and the levels of confidence as ordinal variables (ranging from 1 to 5).
Because of the large number of criteria (45), multivariate analysis (MA) was the most appropriate tool to describe the relationships between the diseases and to underline which criteria support their differentiation. MA encompasses several methods among which the multiple correspondence analysis (MCA) is specifically dedicated to investigating categorical variables. The main objective of MCA is to summarise the associations among a set of categorical variables in a small number of dimensions and to give a low-dimensional graphical representation of these associations. Basically, variables are summarised into factorial axis, which are characterised by their inertia, i.e. the variability of the data they represent. For each variable, a correlation ratio (CR) is computed, which measures the degree of representation of the variable by the factor, ranging from 0 (no representation of the variable by the factor) to 1 (complete representation of the variable by the factor) (Dohoo et al. 1997).
In order to investigate which criteria allow a differentiation between diseases without showing a wide variance in the respondents’ answers for a same disease, two different types of MCA were applied. First, a between-class MCA was conducted to identify variables (criteria) differentiating groups (diseases). The principle of the between-class MCA is to calculate factors in order to maximise the intergroup variance and minimise the intragroup variance, and thus the inter-CR measures the degree of participation of the variable in the intergroup variance of the data set, explained by the factors. Second, a within-class MCA was applied on the data set to identify variables that showed a high variability for a same disease. In contrast to the between-class MCA, factors are constructed in order to maximise the intragroup variance and minimise the intergroup variance. Thus, when a variable shows a high intra-CR, that means that its distribution is characterised by a high variance of the modes of the variables obtained for a same disease (within a same group). Finally, by performing the ratio between these global inter- and intra-CR, we obtained an indicator that measures the ability of the variables (criteria) to optimise the inter-variability (discrimination between the diseases) and to minimise the intra-variability of the data (discrepancies between the answers of the respondents for a same disease).
In a classical MCA, all the individuals and variables have the same weight in the calculation. To take into account the level of expertise and the level of confidence of the respondents in the computation of the data for the same group of diseases, a weighting system was applied to the modes taken by the variables (Birol et al. 2010).
Hierarchical cluster analysis (HCA) was used to differentiate between diseases with similar profiles (epidemiological complexity and impacts on health and socioeconomy). HCA used a set of dissimilarities for the diseases being clustered. Initially, each disease is assigned to its own cluster and then the algorithm proceeds iteratively, at each stage joining the two most similar clusters, continuing until there is just a single cluster. HCA was conducted on the factorial coordinates of the diseases provided by the previous between-class MCA, using the Ward’s minimum variance method of which the principle of aggregation is to minimise intracluster variance and to maximise intercluster variance (Costard et al. 2009). The distance matrix was computed based on the results of the first 14 factors (representing 90 % of the variance) from the previous MCA and using the Euclidean distance.
Multivariate analyses and classification were conducted with the statistical software R 2.11.1 (R Development Core Team 2014), using the package ade4 (Dray and Dufour 2007).
The way the classes of the criteria were encoded using a numerical scale that reflects the complexity and the burden of the disease allows to add the scores provided by the respondents to obtain a total score per disease or per category of variable, in order to quantify the impact of the disease in terms of five aspects:
-
Epidemiology: the epidemiological profiling aims at determining the expected level of complexity of a disease, such as the distribution and the pattern of transmission of the disease, the variability of the pathogen, etc.
-
Impact on public health: this step aims at determining the harm potential of the disease in terms of human health, taking into account two complementary notions, the strictly disease-related threat to human health and the possibility of controlling the disease in human; this will give the highest impact to diseases with a strong nuisance potential in humans and few possible means of control.
-
Impact on animal health: same input but at the animal level.
-
Impact on economy: the economic profiling of a disease aims at determining its nuisance potential for the economy and takes into account direct and indirect impact of the diseases at the animal and human scale.
-
Impact on society: the impact of the disease on society indicators allows to assess the perception of the disease by the public based on its impact on economy, environment, health, control means, etc.
To do so, the sum of the overall scores and the score for each category of criteria, divided by the number of criteria taken into account, was computed. In case several respondents answered for the same disease, the weighted median of their scores (based on the level of confidence and the level of expertise) was used.
3.5 Selected Diseases and Criteria
Searches in literature led to a list of 25 diseases (Table 14.3).
Diseases caused by fungi were not included as the mycoses were poorly described. In addition, no cases due to unconventional agents, such as prions, have been reported in the area. 45 criteria were selected, classified into five categories: epidemiological trends (8 criteria), impact on animal health (9 criteria), impact on public health (11 criteria), economical impact (7 criteria) and social impact (10 criteria). The list of criteria is presented in Table 14.4.
3.6 Descriptive Results of the Study Population
In total, 111 respondents entered the questionnaire in the website during the period of time of 45 days it was open. Fifty-nine people completed the questionnaire (53.2 %). Among the 111 respondents, the majority of respondents were veterinarians (56.8 %) and/or epidemiologists (31.5 %), working mainly for international and governmental organisations (respectively, 32.4 % and 35.1 %) and for research institutes (26.1 %). The field of expertise of the respondents was mainly animal health for 47.7 %, epidemiology for 47.7 %, veterinary public health for 31.5 % and public health for 24.3 %. Among respondents who completed the questionnaire, people mainly mentioned a specific expertise in zoonoses (71.2 %) and usually filled the questionnaire choosing the disease they had experience for (59.3 %). On the contrary, people without any experience on zoonoses were more numerous (61.5 %) among respondents who dropped the questionnaire before the end.
For the further analysis of the data, only complete questionnaires were considered.
On the 25 diseases, complete questionnaires were obtained only for 17 of them, and for some diseases, several complete questionnaires were filled, such as for HPAI (21), rabies (11), anthrax (3), leptospirosis (4), salmonellosis (3), scrub typhus (2), bovine tuberculosis (2), filariasis (2) and Streptococcus suis infection (2).
It was observed that 62.7 % of the respondents answered the questionnaire with a high level of confidence (classes 4 and 5), 35.6 % with a medium level of confidence (class 3) and 1.7 % with a low level of confidence (classes 1 and 2). The distribution of the level of confidence for all the variables was the following: low for 10.4 % of the answers, medium for 29.1 % and high for 58.1 %. 2.4 % of data about level of confidence are missing.
3.7 Evaluation of the Criteria
The 12 first criteria that represented the most the intergroup variance (i.e. the variability of the respondents answers between the different diseases) mainly belonged to the category about the impact on animal health (n = 4) and the economic impact (n = 4), followed by those belonging to the category about the impact on society (n = 3). Only one criterion was found in the category about the impact on public health and none in the one about the epidemiological features. The 12 first criteria that influenced the intragroup variance (i.e. the variability in the answers of respondents for the same disease) were distributed homogeneously between the different categories of criteria: epidemiological trends (n = 2), animal health (n = 2), human health (n = 3), economy (n = 3) and society (n = 2).
The values of the inter-/intra-CR for all the criteria allowed the identification of criteria that supports the differentiation between diseases. Upon a ratio greater than two, there were, respectively, three, four, three, four and five criteria related to epidemiology, animal health, human health, economy and society. The criteria related to epidemiology were speed of spread of the disease within animal population (3.35), zoonotic potential of the pathogen (2.48) and the variability of the pathogen (2.2). The criteria related to animal health were effectiveness of existing surveillance measures (2.7), success of control in other countries (2.35), impact at herd scale (2.34) and prevalence of the disease (2.06). The criteria related to human health were effectiveness of existing surveillance measures (3.98), impact at individual scale (3.69) and effectiveness of existing prevention measures (2.7). The criteria related to economy were impact on international trade (3.95), direct economic impact of animal disease (3.22), indirect economic impact of animal diseases (2.59) and poverty impact of the disease (2.04). The criteria related to society were level of priority for stakeholders (3.54), economic cost of the disease (2.91), potential impact on media (2.87), impact on animal welfare (2.82) and threat to species with a social value (2.39).
3.8 Profile of the Diseases
For eight diseases (44 %), the epidemiological profile was quoted the highest: bartonellosis, Japanese encephalitis, leptospirosis, rabies, salmonellosis, scrub typhus, swine influenza and trematodiasis.
For the other diseases, the economic impact was quoted the highest for six (33 %) of them (anthrax, HPAI, bovine tuberculosis, brucellosis, filariasis, leishmaniasis) and the public health impact for four (22 %) of them (giardiasis, Nipah, Streptococcus suis and taeniasis). For one disease (6 %), the social impact was quoted the highest (anthrax). For any of the diseases, the impact on animal health was assessed as the main burden of the disease.
Respondents allocated the highest overall score to trematodiases (3.53), followed by HPAI (3.38) and bartonellosis (3.24). Bartonellosis and trematodiases were scored with the greatest epidemiological impact (4.38). Furthermore, according to the respondents, trematodiases obtained the greatest impact on animal health (4.33) and human health (4.18) and HPAI on economy (4.43) as well as on society (3.9).
The scores of each disease regarding the different category of criteria and the criteria altogether are displayed in Table 14.5.
3.9 Classification of the Diseases
The hierarchical cluster analysis performed on the results of the between-class MCA provided the dendrograms of the clusters of diseases regarding their profile. Simultaneously, the total score computed for each disease was displayed within the classification.
For the dendrogram representing the diseases (Fig. 14.1), aggregated by the MCA, regarding all the variables, four clusters were clearly identified: one gathering leishmaniasis and Nipah; one gathering seven diseases (salmonellosis, anthrax, HPAI and rabies grouped together, leptospirosis and scrub typhus grouped altogether, filariasis, Japanese encephalitis); one gathering bovine tuberculosis, swine influenza, brucellosis and Streptococcus suis; and the last one gathering bartonellosis, giardiasis and trematodiasis.

Classification of the diseases regarding all the variables
4 Discussion
4.1 Data Collection
The findings of this study highlighted that data collection through a web survey may be an interesting alternative to expert opinion elicitation when collecting data about diseases.
Expert opinion is widely used in epidemiological surveys to collect data about diseases when data are scarce or too costly to collect through classical epidemiological studies (Gale et al. 2010; Mitchell et al. 2009; Birol et al. 2010; More et al. 2010). But it is challenging to select and involve experts with an enough good knowledge to give inputs about a broad range of zoonoses. In this study, the data collection method was designed to limit biases due to a lack of knowledge of experts for a broad range of zoonoses. Instead of asking a narrow list of participants to score various zoonotic diseases against a list of criteria, it was decided to ask numerous people involved with zoonotic diseases in Southeast Asia to fill out the questionnaire about a self-selected disease, expecting that they will pick the one they are the most familiar with. Even with the self-selection of the disease, varying levels of knowledge among respondents were also addressed by using a self-weighting assessment of respondents’ confidence in their own answers.
The snowball sampling approach used to maximise the number of recipients did not allow to select respondents by specific criteria of expertise and location, but the length of the questionnaire and the high level of knowledge required by the questions likely played a role in selecting respondents. Indeed, among respondents who filled entirely the questionnaire, most of them mentioned a specific experience for a zoonotic disease (71.0 %) and were specifically working in countries of Southeast Asia (88.1 %). As a result, most respondents (98.3 %) answered with an overall level of confidence of medium or high. Furthermore, even if most of the respondents were veterinarians or epidemiologists (likely because of their predominance in the starting mailing list), the level of confidence was acceptable in the field of public health, economy and society for which the percentage of respondents who were highly confident in their answers was respectively 59.1 %, 54.5 % and 50.9 %. Nevertheless, this sampling approach might have led to an over-representation of some professional categories (veterinarians) and a discrimination against countries where there is a weak Internet connection. Indeed, in case the connection failed, the questionnaire quits without saving the answers.
4.2 Assessment of the Criteria
The correlation ratio calculated for each criterion regarding the different factorial axes of the multiple correspondence analysis allowed to compare criteria on their ability to discriminate diseases.
The results obtained from the MCA performed on all the variables indicated that the economic impact was the category that triggered the most important variability between the diseases. Criteria that supported the variability intragroup were equally allocated to the different categories. Regarding the inter-/intra-ratio of the criteria within each category, both for animal and public health, indicators related to the efficiency of prevention and surveillance measures appeared to be the most pertinent to discriminate diseases. For the economic category, the results indicated that the economic impact of the animal diseases ensured a greater differentiation than the economic impact of the human diseases. Five criteria related to the societal impact among the 10 evaluated presented a value of the inter-/intra-ratio greater than two, underlining that the impact on society was an important component to differentiate diseases.
The ratio between the intra-CR and the inter-CR, obtained by performing MCA, and the level of confidence of the respondents, obtained through the questionnaire, are two measures that can be combined to help in selecting accurate and relevant criteria for prioritisation. For instance, in this study, in the category of epidemiology, a particular attention should be paid to the criteria ‘speed of spread of the disease in animal population’, ‘zoonotic potential of the agent’, as well as ‘variability of the pathogen’, which combined a high inter-/intra-correlation ratio (respectively, 3.35, 2.48 and 2.20) and a large proportion of respondents which answered with a high level of confidence (respectively, 77.6 %, 82.8 % and 63.2 %). On the contrary, criteria with the lowest inter-/intra-CR do not ensure a good discrimination between diseases because of the high variability of the answers of respondents for a same disease and a low variability of the answers between diseases. Nevertheless, looking at the level of confidence self-assessed by the respondents and associated to criteria with a high intra-CR may give some interesting insights about the source of this variability. A high intra-CR associated with a high level of confidence of the respondents may suggest that the source of the variability is mainly due to a difference of understanding between the respondents or an inappropriate definition of the classes which did not allow an efficient differentiation between the diseases, while a high intra-CR associated with a low level of confidence may be due to knowledge gaps about the disease on this specific point. So in the first case, it emphasises the need to refine the definition of the criteria and their classes, to improve their understanding and their ability to differentiate diseases, and in the second case, it identifies some gaps in the knowledge of the disease that could support further key research questions. For example, in this study, the criterion ‘presence of the disease in Southeast Asia’, which combined a high intra-ratio (0.23) and an important proportion of respondents with a high confidence in their answers (77.6 %), should have been understood differently by the different respondents or was not associated with classes that allowed a good differentiation between the diseases. On the other hand, the criterion ‘existence of risk groups’ showed a high intra-ratio (0.18) as well as a large proportion of respondents with a low level of confidence in their answers (20.7 %). This result suggested that the high variability in the respondent answers was mainly due to a lack of knowledge on this particular point.
These findings must be interpreted in light of a main bias in the methodology, due to a variability of size of the groups (diseases), ranging from 21 for HPAI to one for bartonellosis, brucellosis, giardiasis, Japanese encephalitis, leishmaniasis, Nipah, swine influenza, taeniasis and trematodiasis. Indeed, for diseases selected by several individuals, the weighted mean corresponding to the level of confidence and the specific expertise of the respondents was much more accurate than the single values obtained for disease with only one respondent. Furthermore, calculations performed by the MCA take into account the size of the different group of individuals and a weight, proportional to the size of the group, is applied in the calculations.
4.3 Profile and Classification of Diseases
Displaying the classification of disease simultaneously with the scores provided by the respondents provides a good overview of how the disease clustered regarding their profile and how important their impacts were in terms of epidemiology, health, economy and society.
The way diseases were clustering was coherent with their epidemiological pattern and their burden on public and animal health. For instance, Nipah and leishmaniasis are two emerging/exotic diseases in the region grouped together. HPAI, salmonellosis, rabies and anthrax are main threats for both humans and animals and formed one cluster altogether. Finally, bovine tuberculosis, brucellosis and Streptococcus suis infection, gathered in a same group, are endemic in Southeast Asia and trigger some sporadic outbreaks in human and animal population.
But the results must be interpreted in light of biases in methodology at different levels. First, as explained previously, variable size of the groups was a main source of bias. When looking at the total score per disease, trematodiases obtained the highest score (score 3.53), followed by HPAI (score 3.38) and bartonellosis (score 3.24). This result is probably biassed by the fact that the sample size of the respondents is extremely different from one disease to another (1 for trematodiasis and bartonellosis and 21 for HPAI). It can be suspected than the high score obtained for trematodiasis and bartonellosis is influenced by the professional focus of the single respondent, contrary to HPAI for which the high number of respondents led to the dilution of the individual subjectivity and misinterpretation of the questions. For giardiasis, the level of confidence of the solitary respondent was very low (mode = 1) and this finding calls into question the reliability of the data collected from this participant. Then, the potential redundancy of some criteria might have also triggered some biases. Criteria related to animal health and economy are strongly interdependent as any disease with a great impact on animal health at the population scale (criterion belonging to animal health category) fatally triggers proportionate economic impact in terms of production losses and cost of control measures (criteria belonging to the economic category). Moreover, it is important to keep in mind that the economic impact is assessed regarding both the direct production losses due to the symptoms and the cost of the control measures. So, for a disease such as HPAI for which surveillance and control programmes have been carried out worldwide by international and national organisations, the cost of the prevention and control measures is very high and so a greater economic impact (score 4.43) is given to this disease compared with other economically important diseases such as brucellosis (score 3.29) or salmonellosis (3.57) for which no costly programme is applied. Finally the numerical scale applied to the different scales to allow to compute the scores is very arbitrary as there was no scientific evidence in applying a linear relation between the different classes.
4.4 Towards a New Approach to Prioritise Diseases
Prioritisation may be an efficient tool for policy-makers in charge of allocating resources for surveillance and control programmes or research projects, to target efficiently diseases that need to be addressed ahead of others. In developing countries, the importance to prioritise disease in an objective way is even more significant. In Southeast Asia, the occurrence of zoonoses and their spread is facilitated by the lack of public and animal health capacity on one hand and the exceptionally high population growth rate, the agricultural expansion and intensification, the human encroachment on game reserves, the globalisation of commerce and trade and more frequent contacts between humans, domestic animals and wildlife on the other hand (Cáceres and Otte 2009). Furthermore, the region is considered as a “hot spot” for future emergence and spread of zoonoses because of suitable environmental conditions (Jones et al. 2008): warm and humid climate, high biodiversity, high frequency of natural disasters (such as flooding), etc. So there is a strong need to address the prioritisation of zoonoses with objective tools, specifically adapted to the context of Southeast Asia.
The findings of the study opened new lines of work to improve prioritisation models or to develop new tools for prioritisation, based on the specific context of zoonoses in Southeast Asia. But this methodological framework could also be used in other contexts, depending on the objective of the prioritisation work.
Firstly, MCA can be a very useful tool to refine the list of criteria prior to performing the prioritisation exercise. The choice of the criteria against which the prioritisation is performed remains a weak point in most studies although it is determinant for the performance of the method (Krause 2008a). On one hand, their selection should be made with the objective of getting a well-balanced representation of the components of the disease to comply with the aim of the study – in the case study of zoonoses, public and animal health criteria, socioeconomic aspects in relation to public and animal health, environment impact and the perception by population. But on the other hand, to deal with the scarce availability of some data (Kemmeren et al. 2006; Fosse et al. 2008) and to ensure a clear differentiation between diseases (Cardoen et al. 2009), the list of criteria may be restricted as much as possible. The findings of this study indicate how MCA, combined with the analysis of the level of confidence of respondents in their answers, can help in identifying key criteria that ensure a good differentiation between diseases based on data collected through a web survey. According to the objective of the prioritisation exercise, an extended list of relevant criteria can be first set and followed by a preliminary analysis of the correlation ratio and the level of confidence, to determine those for which a reliable differentiation between diseases is obtained, those for which the definition needs to be improved and those which should be left. With a particular care to ensure that all the components of the diseases are taken into account to comply with the aim of the prioritisation, this approach allows to refine the list of criteria, in order to base the further scoring exercise on clear, relevant and accurate criteria. The clarity of the criteria and classes is a key point when using a web survey as participants answer on their own without any external help (such as a facilitator in a workshop) and there is no way to check for the correct understanding of the questions.
Secondly, the web-based questionnaire can be an interesting alternative to the scoring step by experts, commonly used in semi-quantitative models (Defra 2006). Despite the fact that there is no objective of prioritisation announced in first instance, the questionnaire was built following the example of those used for scoring diseases in semi-quantitative prioritisation methods. Once the objective of the prioritisation process is clearly defined, a numerical scale can be applied to the different classes in order to obtain a score for each criterion, which can be then aggregated to lead to an overall score per disease, which is then used as the base for the ranking. Contrary to the approach developed in previous methods, it is not a restricted panel of experts who are asked to rank a broad range of disease but a large population of stakeholders asked to give inputs about one disease that they have self-selected. So, this methodology circumvents the problem of the lack of knowledge and the subjectivity due to professional focus, encountered with expert opinion elicitation. In some methods, to manage the lack of ready knowledge of the experts for a wide range of diseases and to improve the objectivity and the accuracy of their responses, information data based on literature study are given to the experts to help them in scoring the criteria (WHO 2006; Cardoen et al. 2009). This approach presents different constraints and disadvantages. First, it is not always possible to gather from the literature all data about diseases, especially in developing countries, and it may be very resource intensive, which is why expert opinion elicitation is usually carried out to avoid these two constraints of data collection. Secondly, if this help aims to decrease the subjectivity of experts by making their scores evidence based, their own judgement are strongly biassed by the external information and the scoring is not based anymore on a purely expert opinion but on a mix of expert inputs and bibliographic data, in which the weight of each party cannot be assessed. Compared with expert opinion, the main advantages of such a questionnaire are that it is inexpensive and fast and makes a survey in a large population manageable. But possible disadvantages are related to the clarity of the questions, the validity of the responses and low response percentage (Ribbens et al. 2008). In this study, despite the pretesting step of the questionnaire, the high intragroup variability of the variables emphasised the fact that the criteria and the definition of the different classes associated were not clear enough to be understood the same way by all the respondents. Web-based questionnaires therefore appear to be a reliable alternative to expert opinion if the questionnaire is carefully designed in order to ensure that the discrepancies among respondent answers are due to a difference of opinion and not to a difference of understanding. The validity of data needs to be carefully analysed to be sure that all raters apply data collection method in a consistent manner. Different methods are currently available to evaluate the quality of collection method. Some are based on the inter-rater reliability assessment (probability), such as the kappa or the Fleiss’s test (Gwet 2008), as some others calculate the sensitivity and specificity of data regarding a gold-standard method (Garabed et al. 2009) or geographic information system (Richardson et al. 2009). Furthermore, as previously mentioned, to improve the accuracy of the approach proposed in this study, the analysis of data should be performed on the same number of individuals for each disease. The consultation of a high number of experts results in the dilution of the effect of individual subjectivity and misinterpretation and will allow to work with the distribution of score instead of single-point values. As a result, the final ranking of diseases will take into account the uncertainty and the variability of the system and will be more accurate (Cardoen et al. 2009; Havelaar et al. 2010).
Some other lines of work should be also interesting to explore, in order to improve the accuracy and the relevancy of the data collection through a web survey. To enhance the representativeness of the respondents and to take into account the perception of the diseases by all the stakeholders involved with zoonoses, the questionnaire may be drawn up in different versions adapted to the different professions (veterinarians, medical doctors, economists, farmers, etc.). Furthermore to deal with the part of subjectivity which remains with respondents’ answers, the definition of the criteria may focus on the identification of ‘proxy criteria’. Those criteria do not present a great interest in themselves but they are not submitted to professional focus of respondents and they allow to assess other variables with which they are closely related to. Finally, the classification of disease based on the results of the MCA may provide clusters of diseases with similar profiles, which can be used as a start for the prioritisation exercise. Instead of ranking the diseases with regard to each other, they are first clustered together depending on their characteristics and then one in each cluster is selected as a priority. By focusing efficiently efforts on this disease to improve the surveillance and control systems, it can be expected that the future improvement obtained for this disease will spread to the other diseases of the same cluster (FAO 2008). This approach presupposes that the criteria are carefully selected to be sure that the clusters of diseases are accurate and relevant. An important advantage of this approach is that it avoids the risk of vertical programmes, which is always present when addressing the prioritisation task pathogen by pathogen (Krause 2008b). Indeed, when following a strict pathogen-focused approach, the original purpose of any health activity would be severely constrained and it would result in the competition of vertical programmes if decision makers do not keep in mind the operational commonalities among the high-priority diseases. To avoid this undesirable consequence of prioritisation, some research groups have therefore performed prioritisation exercises focused on general health issues rather than on individual pathogens (Eger et al. 2009), but the way diseases are grouped does not necessary lead to homogeneous clusters of diseases, which require the same individual methodological approach.
5 Conclusion
The findings of this study highlighted an innovative approach to improve objectivity and accuracy for some of the steps of prioritisation methodology. The use of a web-based questionnaire appeared to be an interesting alternative to expert opinion elicitation for the process of data collection and scoring, while the performance of multivariate analysis on a set of criteria prior to the prioritisation enhances the selection of clear, accurate and relevant criteria that allow a reliable differentiation between diseases. Nevertheless, the results of the study underlined several sources of bias in the methodology that need to be addressed to optimise the use of this new approach.
Dealing efficiently with zoonoses implies working on the human-animal-ecosystem interface. There is now an international consensus around the “One Health” approach (FAO 2008) that supports and legitimates the need of cooperation between animal, public and environmental health institutions to defeat emerging and re-emerging diseases that threaten both animal and human health. Since the emergence of the One Health concept, the management of several recent outbreaks (Q fever in the Netherlands in 2010, Hendra virus in Australia in 2009) underlined the importance of thinking about the animal-human-ecosystem interface to fight against old and emerging diseases (Leboeuf 2011).
This study underlined the need to address prioritisation within the One Health approach because criteria related to animal and human health, as well as those related to ecology and environment, contributed to a reliable and accurate differentiation of the diseases. Nevertheless, it also arose some difficulties in working within this framework, as it was challenging to gather reliable data about zoonoses from all the stakeholders involved with zoonotic diseases, both in the animal and health sectors. It is therefore important to continue the development of efficient tools for prioritisation in this context.
References
Birol E, Asare-Marfo D, Yakhshilikov Y (2010) Efficacy and adoption of strategies for avian flu control in developing countries (no 1023). International Food Policy Research Institute (IFPRI)
Brookes VJ, Hernández-Jover M, Cowled B, Holyoake PK, Ward MP (2014) Building a picture: prioritisation of exotic diseases for the pig industry in Australia using multi-criteria decision analysis. Prev Vet Med 113:103–117
Cáceres SB, Otte MJ (2009) Blame apportioning and the emergence of zoonoses over the last 25 years. Transbound Emerg Dis 56:375–379
Capek I, Vaillant V, Mailles A, De Valk H (2006) Définition de priorités et actions réalisées dans le domaine des zoonoses non alimentaires, 2000–2005. Buletin Epidémiologique Hebdomadaire 27–28:196
Cardoen S, Van Huffel X, Berkvens D, Quoilin S, Ducoffre G, Saegerman C, Speybroeck N, Imberechts H, Herman L, Ducatelle R, Dierick K (2009) Evidence-based semiquantitative methodology for prioritization of foodborne zoonoses. Foodborne Pathog Dis 6:1083–1096
Costard S, Porphyre V, Messad S, Rakotondrahanta S, Vidon H, Roger F, Pfeiffer DU (2009) Multivariate analysis of management and biosecurity practices in smallholder pig farms in Madagascar. Prev Vet Med 92:199–209
Cox LA, Babayev DB, Huber W (2005) Some limitations of qualitative risk rating systems. Risk Anal 25(3):651–662
DEFRA (2006) Approaches to the prioritisation of resources: a brief review of selected public sector organisations in the UK and abroad. http://archive.defra.gov.uk/foodfarm/farmanimal/diseases/vetsurveillance/documents/prioritisation-resources.pdf. Retrieved 3 Oct 2014
Discontools (2009) Approaches to the prioritization of diseases: a worldwide review of existing methodologies for health priority settings. www.discontools.eu/documents/1207_Draft%20Review%20of%20existing%20methodologies%20for%20priority%20settings.pdf. Retrieved 3 Oct 2014
Doherty JA (2000) Establishing priorities for national communicable disease surveillance. Can J Infect Dis 11:21
Dohoo IR, Ducrot C, Fourichon C, Donald A, Hurnik D (1997) An overview of techniques for dealing with large numbers of independent variables in epidemiologic studies. Prev Vet Med 29:221–239
Dray S, Dufour AB (2007) The ade4 package: implementing the duality diagram for ecologists. J Stat Softw 22:1–20
Eger K, Gleichweit S, Rieder A, Stein KV (2009) Prioritising integrated care initiatives on a national level. Experiences from Austria. Int J Integr Care 9:e91
FAO-OIE-WHO-UNSIC-UNICEF-WB (2008) Contributing to one world, one Health. A strategic framework for reducing risks of infectious diseases at the animal-human-ecosystems interface. ftp://ftp.fao.org/docrep/fao/011/aj137e/aj137e00.pdf. Retrieved 3 Oct 2014
Fosse J, Seegers H, Magras C (2008) Foodborne zoonoses due to meat: a quantitative approach for a comparative risk assessment applied to pig slaughtering in Europe. Vet Res 39:1–16
Gale P, Brouwer A, Ramnial V, Kelly L, Kosmider R, Fooks AR, Snary EL (2010) Assessing the impact of climate change on vector-borne viruses in the EU through the elicitation of expert opinion. Epidemiol Infect 138:214–225
Garabed RB, Perez AM, Johnson WO, Thurmond MC (2009) Use of expert opinion for animal disease decisions: an example of foot-and-mouth disease status designation. Prev Vet Med 92:20–30
Gwet KL (2008) Computing inter-rater reliability and its variance in the presence of high agreement. Br J Math Stat Psychol 61:29–48
Havelaar AH, van Rosse F, Bucura C, Toetenel MA, Haagsma JA, Kurowicka D, Heesterbeek JHAP, Speybroeck N, Langelaar MFM, van der Giessen JWB, Cooke RM, Braks MA (2010) Prioritizing emerging zoonoses in the Netherlands. PLoS One 5:e13965
Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL, Daszak P (2008) Global trends in emerging infectious diseases. Nature 451:990–993
Kemmeren JM, Mangen M-JJ, van Duynhoven YTHP, Havelaar AH (2006) Priority setting of foodborne pathogens—disease burden and costs of selected enteric pathogens. National Institute for Public Health and the Environment, Bilthoven. http://rivm.openrepository.com/rivm/bitstream/10029/7316/1/330080001.pdf. Retrieved 3 Oct 2014
Krause G (2008a) How can infectious diseases be prioritized in public health? EMBO Rep 9: S22–S27
Krause G (2008b) Prioritisation of infectious diseases in public health – call for comments. Eurosurveillance 13(40):1–6
Kurowicka D, Bucura C, Cooke R, Havelaar A (2010) Probabilistic inversion in priority setting of emerging zoonoses. Risk Anal 30:715–723
Leboeuf A (2011) Making sense of one health: cooperating at the human-animal-ecosystem health interface. Health and Environment Reports 7. http://onehealthinitiative.com/publications/IFRI_ifrihereport7alineleboeuf.pdf. Retrieved 3 Oct 2014
McKenzie J, Simpson H, Langstaff I (2007) Development of methodology to prioritise wildlife pathogens for surveillance. Prev Vet Med 81:194–210
Mitchell RJ, Williamson AM, O’Connor R (2009) The development of an evaluation framework for injury surveillance systems. BMC Public Health 9:260
More SJ, McKenzie K, O’Flaherty J, Doherty ML, Cromie AR, Magan MJ (2010) Setting priorities for non-regulatory animal health in Ireland: results from an expert Policy Delphi study and a farmer priority identification survey. Prev Vet Med 95:198–207
Ng V, Sargeant JM (2013) A quantitative approach to the prioritization of zoonotic diseases in North America: a health professionals’ perspective. PLoS One 8:e72172
Perry BD, Randolph TF, McDermott JJ, Sones KR, Thornton PK (2002) Investing in animal health research to alleviate poverty. International Livestock Research Institute (ILRI), Nairobi. http://mahider.ilri.org/handle/10568/2308. Accessed March 2012
R Development Core Team (2014) R tutorial. http://cran.r-project.org/doc/manuals/r-release/R-intro.pdf. Retrieved 3 Oct 2014
Ribbens S, Dewulf J, Koenen F, Mintiens K, De Sadeleer L, de Kruif A, Maes D (2008) A survey on biosecurity and management practices in Belgian pig herds. Prev Vet Med 83:228–241
Richardson E, Good M, McGrath G, More SJ (2009) The use of Geographic Information System (GIS) and non-GIS methods to assess the external validity of samples postcollection. J Vet Diagn Invest 21:633–640
World Health Organization (2006) Setting priorities in communicable disease surveillance. http://whqlibdoc.who.int/hq/2006/WHO_CDS_EPR_LYO_2006_3_eng.pdf. Retrieved 3 Oct 2014
World Organization for Animal Health (2008) Terms of reference and call for tender for a new OIE study: listing and categorisation of priority animal diseases, including those transmissible to humans. http://www.test.oie.int/fileadmin/Home/eng/Support_to_OIE_Members/docs/ppt/study_partnership_oie.pdf. Retrieved 3 Oct 2014
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Bordier, M., Léger, L., Kasemsuwan, S., Wongnarkpet, S., Roger, F. (2015). Methods for Prioritisation of Diseases: Case Study of Zoonoses in Southeast Asia. In: Morand, S., Dujardin, JP., Lefait-Robin, R., Apiwathnasorn, C. (eds) Socio-Ecological Dimensions of Infectious Diseases in Southeast Asia. Springer, Singapore. https://doi.org/10.1007/978-981-287-527-3_14
Download citation
DOI: https://doi.org/10.1007/978-981-287-527-3_14
Publisher Name: Springer, Singapore
Print ISBN: 978-981-287-526-6
Online ISBN: 978-981-287-527-3
eBook Packages: MedicineMedicine (R0)