
Abstract
Anger and hostility are described with special attention to their cognitive-motivational properties. Varying operational definitions related to anger self-report and behavioral observation are presented. The idea that anger can be maladaptive is now widely accepted as in DSM and alternative classifications of dysfunctional anger. The idea that maladaptive anger raises risks for hypertension and coronary heart disease is reviewed with reference to empirical findings on mediators such as atherosclerosis, cardiovascular reactivity, immune system changes, and unhealthy lifestyles. Given that anger is a relational emotion, it is not surprising that it befalls many interpersonal relations including close/intimate relationships. Dimensions of affiliation and control in relationships are presented as a framework for understanding how anger and hostility can develop and persist in these contexts. The further connection between such anger and cardiovascular function is illustrated. Fortunately, maladaptive anger is treatable, as explained with meta-analytic evidence on cognitive behavioral therapy (CBT). Also available are recent enhancements like CBAT that involve sequencing multiple cognitive, behavioral, and affective strategies appropriate to the process of anger from onset, through progression, to offset. Finally, traditional interpersonal therapies and newer therapeutic formulations such as acceptance and commitment therapy may address major themes in interpersonal conflict underlying the onset and maintenance of cardiovascular disease. Yet, many of these potential applications still await research and implementation in the field of psychocardiology.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- Anger
- Hostility
- Cardiovascular disease
- Reactivity
- Hypertension
- Interpersonal relationships
- Affiliation
- Dominance-submission
- Cognitive behavioral affective therapy
- CBAT
Introduction
Of the psychosocial factors implicated in cardiovascular disease (CVD) , anger and hostility have remained in the foreground for several decades (Chida and Steptoe 2009; Smith et al. 2004). In this chapter, evidence and theories are presented on the connection between CVD and anger/hostility. The focus will be on interpersonal contexts of anger and CVD, given the substantial accumulation of literature on this topic. As a preliminary, the concept of anger and related constructs are defined.
Phenomenology of Anger and Related Constructs
The many definitions of anger differ in points of emphasis. At a basic level, anger can be defined as, “an unpleasant emotion ranging in intensity from irritation or annoyance to fury or rage” (Smith 1994, p. 25). Some definitions emphasize that anger is a moral emotion in the sense that it implies a perceived discrepancy with a standard of conduct (e.g., Hutcherson and Gross 2011). Others see it as an approach emotion that occurs when progress toward desired goals is impeded (e.g., Carver and Harmon-Jones 2009), though indirect and even detached expression of anger should not go unrecognized especially in the present population of interest. Finally, a number of scholars point out that anger is a relational emotion that occurs in a socially constructed context (Laughlin and Warner 2005); this is highly consistent with the interpersonal perspective of anger in cardiovascular disease (Smith and Cundiff 2011).
There is little disagreement that anger is essentially unpleasant. Though it can certainly be functional in alerting one to a transgression or communicating displeasure to the offender, anger is hardly welcome to its experiencer or its recipient. The expression of anger can have beneficial consequences as when an opponent concedes or submits, but this does not mean that one likes to be angry for the sake of itself. The risks posed by anger include interpersonal conflict, impaired judgment, and a host of physical symptoms of which particularly pertinent for present purposes is the toll anger takes on cardiovascular health (Smith et al. 2004; Smith and Traupman 2011). As noted by Howells (2004), “the argument that angry emotions, when poorly regulated, understood and expressed, make a major contribution to human distress is a compelling one” (p. 195). The arousal of anger is often associated with universally recognized patterns of facial activation and expression and as described below a set of potentially unhealthy psychophysiological responses especially involving the cardiovascular system.
In keeping with the cognitive-motivational structure of emotions (Lazarus 2000), anger comprises a cognitive element of appraised wrongdoing and an action tendency to counter or redress that wrongdoing (Smedslund 1993; Wranik and Scherer 2010). Cognitive schemas closely associated with anger are often labeled hostility, referring to a “negative attitude toward others consisting of enmity, denigration, and ill will” (Smith 1994, p. 26). These cognitive styles include cynicism (i.e., a belief that other people are motivated largely by selfish concerns), mistrust (i.e., expectations that others are likely sources of mistreatment), and hostile attribution (i.e., the tendency to construe the actions of others as aggressive or hurtful in intent). Thus, cognitive-motivationally, hostility has been defined as “a devaluation of the worth and motives of others, an expectation that others are likely sources of wrongdoing, a relational view of being in opposition toward others, and a desire to inflict harm or see others harmed” (Smith 1994, p. 26).
Aggression, though often used as a proxy for measuring anger does not necessarily contain anger, as observed by Averill (1983) in his landmark paper. To be aggressive, according to the social psychological perspective, is to perform behavior that is intended to harm, hurt, or damage – physically or psychologically. These “attacking, destructive, or hurtful actions” (Smith 1994, p. 26.) range in degree or severity, from sarcasm or subtle criticism to direct and pointed insults, to intimidating postures and facial expressions (e.g., glaring, scowling), and to physically threatening behavior. A subtype of physical aggression is violence in which case the intended harm/hurt/damage does materialize.
In addition to its structure, anger, like all affective qualia, can be characterized in terms of form . Specifically, does it take the form of an emotion, mood, or temperament? (Fernandez 2008). As a discrete emotion, it has a marked onset and offset and this episode is labeled state anger. In the form of mood, it is relatively continuous and lower in intensity. As a recurrent occurrence, it is often regarded as temperament or trait anger. This is often used synonymously with the term hostility , which connotes a proneness to anger (Ramirez and Andreu 2006); as noted previously, hostility is often attributed to an attitudinal bias or underlying schema of strong disapproval toward others (Brodsky 2011). In short, anger takes three main forms depending on such parameters as frequency, duration, and intensity. To say that someone is in an angry state is quite different from saying that she/he is in an irritable/irascible mood, which in turn differs from characterizing someone as having a hostile temperament (Fernandez 2013).
Operational Definitions and Anger Assessment
The operationalization of anger , hostility, and related characteristics in research and practice has been handled using a range of psychological tests and structured interviews. The vast majority of these are self-report questionnaires. Beginning with offshoots of the MMPI (e.g., Cook-Medley Hostility Scale or Ho Scale; Cook and Medley 1954), attention was directed at hostility or trait anger . The early Buss-Durkee Hostility Inventory (BDHI; Buss and Durkee 1957) later revamped into the Buss-Perry Aggression Questionnaire (Buss and Perry 1992) introduced a valuable distinction between direct and indirect expression of anger. Other tests veered toward hypothetical scenarios of anger provocation (e.g., Novaco Anger Scale and Provocation Inventory (Novaco 1994, 2003)). Another wave of questionnaires highlighted distinctions between trait versus state anger and styles of anger expression (i.e., anger-in vs. anger-out). The most common of these is the State-Trait Anger Expression Inventory (STAXI; Spielberger 1988, 1991, 1999) which is referred to in several of the studies reported later. In fact, much of the literature on anger and CVD is based on MMPI derivatives such as the Ho Scale and from the more recent STAXI. Despite acceptable psychometrics, these instruments are not without shortcomings in how the vast and complex topography of anger is represented. A new generation of anger assessment instruments attempts to overcome some of these shortcomings by introducing a variety of additional parameters and expression styles of anger (see review by Fernandez et al. 2015).
Beyond the most commonly used self-report approaches, behavioral ratings of anger and hostility have been developed for use with structured interviews (Smith 1994), and informant ratings for these traits are also available (Smith et al. 2007). Although self-reports of anger, hostility, and aggressiveness predict the development and course of CVD and are consistently correlated with behavioral and informant ratings, the latter assessments are often more closely related to cardiovascular disease (Miller et al. 1996; Newman et al. 2011; Smith et al. 2007). This may reflect the fact that because anger and related traits are socially undesirable, individuals are often unwilling or unable to provide accurate self-reports, whereas their tendency to experience and display anger may be readily apparent to others. In clinical contexts, interview-based behavioral ratings and informant reports may be valuable additions to the typical self-report approaches.
Diagnosis of Dysfunctional Anger
In DSM-5 (American Psychiatric Association 2013), a mental disorder is “a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning” (p. 20). No longer is there a reference to significantly increased risk of “pain, disability, death, or important loss of freedom” as in DSM-IV (American Psychiatric Association 2000, p. xxxi). Thus, anger that portends such dire consequences as violence and incarceration would not ipso facto amount to a mental disorder. Yet, aggressive or violent anger raises the possibility of marked disturbance in actions, thoughts, or emotional control that render it dysfunctional. Despite that, anger, unlike depression and anxiety, does not appear as a separate diagnostic category in DSM. Rather it appears as isolated disorders or else it is embedded as a symptom within other disorders. Two of these in which anger is a defining feature are Intermittent Explosive Disorder (IED) and Disruptive Mood Dysregulation Disorder (DMDD) . The former is described as recurrently uncontrolled anger culminating in disproportionate physical or verbal aggression. The latter includes not only angry outbursts but also chronic irritability and hypomania. While it is beyond the scope of the present paper to discuss these disorders, it is worth keeping in mind that anger in CVD populations may be dysfunctional in ways that resemble IED or DMDD.
Anger, Hostility, and Cardiovascular Disease
The study of anger and related traits as influences on the development and course of coronary heart disease (CHD) and other forms of cardiovascular disease (CVD) such as essential hypertension and stroke has a long history in medicine (Smith et al. 2004). In more recent decades, this topic was an outgrowth of research on the Type A coronary-prone behavior pattern (Miller et al. 1996; Byrne 2000), in which research sought to identify the “toxic core” of the multifaceted Type A pattern. Quantitative reviews of prospective studies indicate that high levels of anger, hostility, and aggressiveness increase the risk of the initial development of CHD, as well as increase the risk of recurrent cardiac events and earlier mortality among patients with existing disease (Miller et al. 1996; Chida and Steptoe 2009).
Given the decades-long natural history of CHD (see chapter 1, this volume), these associations raise an important question as to which phases of the disease are potentially influenced by anger and hostility. The current evidence suggests a role in multiple disease stages. For example, among persons without any clinical signs of clinical CVD, anger and hostility are associated with early, asymptomatic indicators of atherosclerosis, including endothelial dysfunction and arterial stiffness (Gottdiener et al. 2003; Williams et al. 2006), atherosclerosis in the carotid arteries (Everson-Rose et al. 2006), and coronary artery calcification (Smith et al. 2007). Episodes of anger can also precipitate or “trigger” acute cardiac events, such as myocardial infarction (Mostofsky et al. 2013, 2014). Among patients with advanced coronary atherosclerosis, experimentally evoked anger (e.g., recall and discussion of anger-arousing events) can evoke myocardial ischemia (Strike and Steptoe 2005). Thus, anger and hostility most likely predict the development of CHD morbidity and mortality because they promote the initial development and progression of the underlying atherosclerosis but also because these traits can contribute to the precipitation of ischemia and acute coronary crises among persons with advanced disease.
These associations likely reflect multiple biobehavioral mechanisms. For example, anger and hostility are associated with unhealthy lifestyles, including tobacco use, alcohol abuse, physical inactivity, and poor diet (Bunde and Suls 2006). In some studies, these poor health behaviors mediate the association between anger /hostility and CHD outcomes (e.g., Boyle et al. 2008). However, in many other instances, anger and hostility predict CHD morbidity and mortality even when health behaviors are statistically controlled, suggesting a role for mechanisms beyond poor health habits.
The physiological effects of psychological stressors (e.g., Esler et al. 2008; Wright and Stewart 2012) also may play an important role. Frequent and pronounced increases in heart rate, blood pressure, and neuroendocrine events (e.g., catecholamines, cortisol) in response to stressful circumstances and the delayed recovery of these physiological responses can contribute to atherosclerosis and the triggering of acute CHD events (Chida and Steptoe 2009; Steptoe and Kivimaki 2013). Chronically angry and hostile persons, compared to more even-tempered and agreeable individuals, show heightened physiological responses to a variety of stressors but especially those involving interpersonal conflict or mistreatment (Smith et al. 2004). Anger and hostility also interfere with the otherwise beneficial effects of social support in dampening these physiological stress responses (Holt-Lunstad et al. 2008; Smith et al. 2004). That is, unlike more trusting and agreeable persons, chronically angry and hostile individuals do not display attenuated physiological responses to acute stressors when they receive social support. Trait anger and hostility are also associated with chronic systemic inflammation (Smith et al. in press; Suarez 2012), and this sustained immune system response is closely tied to the development and progression of atherosclerosis (Steptoe and Kivimaki 2013). Thus, increased frequency, degree, and duration of physiological stress responses may contribute to the association of anger and hostility with CVD in general and with CHD in particular.
Physiological stress responses typically recover during sleep, falling below daytime levels. Thus, adequate restorative sleep is associated with lower risk of CVD, whereas poor or inadequate sleep is associated with greater risk (e.g., King et al. 2008). Chronic anger and hostility are associated with poor sleep (Brissette and Cohen 2002), which may be an additional mechanism contributing to the association with CVD.
Anger in Interpersonal Relationships
High trait anger or hostility is associated with a wide variety of difficulties in interpersonal relationships, and these social processes may also contribute to their unhealthy effects (Smith et al. 2004; Smith and Cundiff 2011). For example, anger and hostility are associated with low levels of social support (Smith et al. 2004) and high levels of conflict and disruption in close relationships, such as marriage (Baron et al. 2007; Renshaw et al. 2010). Low social support and higher strain in intimate relationships are both associated with greater risk of CHD morbidity and mortality (Barth et al. 2010; Robles et al. 2014; Smith et al. 2011). Thus, anger and hostility may contribute to CHD in part because they are closely tied to other psychosocial risk factors, specifically those related to the quality of social relationships.
The interpersonal perspective in personality and clinical psychology (Horowitz and Strack 2011; Pincus and Ansell 2013) is useful in describing this association among multiple psychosocial risk factors for CHD and ultimately in providing an integrative account that could inform risk reduction efforts (Smith and Cundiff 2011; Smith et al. 2004). In this perspective, personality and emotional traits are seen as inseparably tied to recurring patterns of social interaction. Specifically, aspects of the social environment that are substantial and stable enough to affect the decades-long development and course of CHD (e.g., social support, isolation, conflict) are in large part manifestations of the individual’s personality. Such recurring interpersonal events not only reflect the individual’s personality and emotional adjustment but shape and maintain personality characteristics and emotional adjustment, as well, in an ongoing reciprocal process.
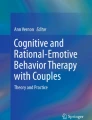
As seen in Fig. 1, interpersonal actions and stimuli can be described as varying blends of two basic dimensions of social behavior. Affiliation varies from warm, close, and supportive behavior to cold, hostile, and quarrelsome behavior. Control varies from dominant and directive actions to deferent, accommodating, or submissive responses. Anger and hostility are obviously associated with the tendency to express low levels of affiliation (i.e., low warmth and closeness, high isolation, and antagonism). Importantly, chronically angry and hostile persons not only display this pattern of low affiliation toward others, they also experience a similar pattern of behavior from others. Many different aspects of anger and hostility are consistently associated with this pattern of low affiliation, but they vary widely in terms of control. Some forms of anger and hostility, such as verbal aggressiveness and the tendency to express rather than suppress angry affect (i.e., anger-out), are characterized by a hostile-dominant interpersonal style. Other forms (e.g., resentment, cynicism, anger-in) are associated with a hostile-submissive interpersonal style (Smith et al. 2010). This will be taken up further in the section on anger suppression.

The interpersonal circumplex. Social behavior is described as various blends of the two basic dimensions of affiliation and control. Anger , hostility, and aggressiveness are all associated strongly with low affiliation, but different aspects of this domain range from hostile dominance to hostile submissiveness
In the interpersonal perspective, the behavior of one individual tends to invite or evoke a restricted class of responses from interaction partners. Specifically, expressions of warmth invite warmth in return, whereas expressions of hostility tend to invite or evoke quarrelsomeness, coldness, and other hostile actions in return. This general view, labeled the principle of complementarity in interpersonal theory (Pincus and Ansel 2013) may explain the fact that chronic anger and hostility are consistently associated with low levels of social support and high levels of interpersonal conflict. Warm expression of dominance tend to evoke friendly cooperation or deference in return, but hostile dominance evokes either resentful compliance from others or more pointed contexts for dominance and control. Thus, in social interactions, angry and hostile persons tend to reap what they sow, and over time these reactions from their social environment provide ample evidence for the angry and hostile person that their antagonistic stance toward others is well justified, in a recurring pattern of self-fulfilling prophecy. In this way, anger and hostility do not simply reflect characteristics of the individual but are fully embedded in a larger, ongoing interpersonal environment of low support and high conflict which itself confers risk for CVD.
This dysfunctional interpersonal pattern is depicted in Fig. 2. Aspects of the angry and hostile individual’s internal experience (e.g., cynical beliefs about the motives of others, expectations of mistreatment, hostile attributions, and explanation for other’s actions) lead him/her to behave outwardly with low warmth and high hostility. These behavioral expressions limit the subjective impact of the angry actor’s behavior on their interaction partners, increasing the likelihood that angry, hostile, and aggressive behavior will be reciprocated, further maintaining and perhaps exacerbating the angry actor’s emotional, cognitive, and behavioral tendencies.

The transactional cycle . Individuals’ covert experiences (e.g., goals, affect, beliefs) guide their overt behavior, in ways that tend to constrict the range of possible covert and overt reactions by their interaction partners
This perspective suggests an expanded view of the role of physiological reactivity in the association of anger and hostility with CVD. As illustrated in Fig. 3, compared to the blood pressure response of the friendly person depicted in the lower panels, the hostile-dominant individual depicted in the upper panels responds with larger and more prolonged increases in blood pressure in response to the same laboratory stressor, such as a discussion of a previous anger-arousing event. Outside the laboratory, the hostile-dominant persons also responds to a common stressor (e.g., traffic congestion) with larger increases in blood pressure than shown by a friendly individual facing this same stressor. However, the overall much greater degree of blood pressure reactivity in the daily life of the hostile-dominant individual is due to not only greater reactivity to equivalent stressors but also to their exposure to more frequent, severe, and prolonged interpersonal stressors, relative to the friendly individual. That greater stress exposure, in turn, reflects the tendency of the hostile-dominant individual to create more frequent and severe interpersonal difficulties, through the impact of their actions and emotional expression on others. This pattern is also exacerbated by the hostile-dominant individual’s tendency to mentally rehearse past interpersonal difficulties and grievances (i.e., rumination), their tendency to undermine potential sources of social support, and their tendency to fail to benefit physiologically from social support when they get it.

Conceptual depiction of effects of individual differences in stress reactivity and exposure on overall levels of blood pressure observed during controlled laboratory conditions and during daily life for a hostile-dominant person (upper portion) and a friendly individual (lower portion). When experiencing the same stressor, the hostile-dominant individual displays greater blood pressure increase than the friendly person. In everyday life, the hostile-dominant person also encounters more frequent, severe, and prolonged stressors as a result of the impact on others of their own interpersonal behavior
Anger Suppression and CVD
The proverbial explosion or outburst is not the only way in which anger poses a threat to cardiovascular health. Rather, anger can be suppressed or else manifested in relatively attenuated and indirect ways (Fernandez 2008) consistent with the hostile-submissive personality style (Smith et al. 2010). Interpersonal relations within work and social contexts may place a premium on inhibition of angry behavior. However, this often comes at a cost of well-being, especially a cost to cardiovascular health (Mauss and Gross 2004).
Research points to a fairly reliable relationship between anger suppression and blood pressure. For example, Hosseini et al. (2011) compared hypertensive patients with a group of healthy normals matched on age, gender, and educational level. Anger-in but not anger-out (as measured by the STAXI) was significantly higher in the case group than the control group. Sharma (2003) found that in comparison to normotensive individuals, hypertensive patients reported more stress from life events, more suppression of anger, and more trait anger and trait anxiety. Conversely, hypertensives showed lower outward expression and control of angry feelings as measured on the STAXI.
Going beyond self-reports of trait anger, Quartana and Burns (2010) used a laboratory context to assess cardiovascular reactivity to experimentally induced anger. It was reported that when participants underwent an experimental manipulation to suppress anger, there was a delayed increase in systolic blood pressure.
Special attention has been directed at the cardiovascular effects of anger suppression in women, in the light of gender differences in expression but not experience of anger (Fernandez and Malley-Morrison 2013). Based on a Canadian sample of female managers, Greenglass (1996) suggested that cynical distrust and internalized anger might be precursors of hypertension . Thomas (1997) reported that when women suppressed anger in the home environment, it was accompanied by increases in systolic blood pressure and diastolic blood pressure. Using electron beam computed tomographic scans to determine coronary artery calcification, Low et al. (2011) observed that in postmenopausal women, anger-in was part of a psychosocial risk index predicting a significant increase in coronary artery calcification and a trend toward atherosclerosis over a 3-year period. In a review of the literature on psychosocial risks of CVD, Low et al. (2010) concluded that for women, there is ample evidence that anger suppression and the stress of family and interpersonal relationships are among the main psychosocial factors associated with increased CHD.
For a critical review of the research on the cardiovascular effects of emotion suppression, see Mauss and Gross (2004). As the authors point out, there is a complexity in emotion suppression that may require further elaboration of the findings in this area.
Treatment Options for Anger in CVD
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) is the dominant approach to treating anger. At a minimum, it is a two-pronged strategy of getting the angry person to reappraise and de-arouse, and this is particularly applicable in interpersonal conflict where misattributions and agitation abound. Meta-analysis of about 50 studies of CBT for anger produced a grand weighted mean effect size of +0.70, meaning that the average subject receiving CBT was better off than 76 % of no-treatment control subjects, on dependent measures of anger (Beck and Fernandez 1998). This was replicated in a subsequent meta-analysis by Di Giuseppe and Tafrate (2003). This approach has also been found to produce clinically meaningful reductions in anger, hostility, and aggressiveness for individuals diagnosed with Intermittent Explosive Disorder (McCloskey et al. 2008). Based on these findings, it is arguable that CBT can be applied to treat anger in patients with CVD.
Cognitive Behavioral Affective Therapy (CBAT)
In addition to reappraisal and de-arousal, other cognitive and behavioral techniques can be included to enhance CBT. Furthermore, a whole class of affective techniques can be incorporated so that feelings are directly accessed and modified, as is appropriate especially when anger is suppressed. These techniques are consistent with some of the experiential and emotion-focused therapies (Greenberg and Goldman 2008; Paivio and Pascual-Leone 2010). The product is a new enhanced and integrative therapy termed cognitive behavioral affective therapy (CBAT; Fernandez 2010, 2013).
Fundamental to CBAT for anger is the premise that anger is a process. Specifically, anger unfolds over three main phases: onset, progression, and offset, respectively. Therefore, treatment is also triphasic, the first phase being prevention which is followed by intervention which is followed by postvention. The first phase entails preparation for possible anger-provoking events, the second involves intervention on outbursts or escalation of anger, and this is followed by a third phase, postvention, to remove residual traces of anger as may be found in anger suppressors.
Figure 4 (adapted from Fernandez and Kerns in press) illustrates this progressive filtering of anger. As shown, different techniques are not made available in a menu-driven manner but are sequenced to fit into specific phases. Within each phase too, techniques are presented in a contingent fashion so that the end result is a programmatic delivery of skills for the self-regulation of anger. A detailed exposition of CBAT self-regulation for anger can be found in Fernandez (2010) and Fernandez and Kerns (in press).

Anger filtered through phases of cognitive behavioral affective therapy
Preliminary research has found an effect size ranging from +0.80 to +0.99 on various dependent measures of anger targeted by CBAT (Fernandez and Scott 2009). While this is encouraging, new research is needed to determine the outcome efficacy of CBAT in CVD patients in whom anger is a comorbid problem.
Interpersonal Therapy and Other Perspectives
One reminder at this point is that like CBT for anger, CBAT is delivered very much in the format of a skills training program. Rather than engaging in psychotherapeutic dialogue, participants actually learn skills for implementation in everyday naturalistic settings when anger is likely to occur. In other words, anger is treated primarily as an intrapsychic problem. However, this chapter stresses that the anger of CVD patients often arises within a relational context that is often beset with perceived wrongdoings and conflict. The importance of addressing such interpersonal conflict is acknowledged in psychodynamic therapy. The tried and tested tools of marital and family therapy are particularly relevant in this context. Also productive may be strategies that have evolved within the conflict resolution literature. In more recent times, acceptance and commitment therapy (ACT) has rekindled interest in forgiveness, mindfulness, and other perspectives (e.g., Day et al. 2008) that have roots in many theological and philosophical traditions.
Usefulness in the Management of Coronary Disease
Some rehabilitation programs for CVD have had elements of counseling and therapy. A meta-analytic review found that stress management and related psychosocial interventions for CHD patients reduce recurrent cardiac events and mortality (Linden et al. 2007). Group-based therapy to reduce Type A behavior has been found to reduce recurrent coronary events among CHD patients (Friedman et al. 1986), and this approach also reduces anger and hostility (Mendes de Leon et al. 1991). Although relaxation training and reduced stress is a cornerstone of many of the CBT approaches to the treatment of anger described above, few studies have examined the effects of anger treatment in CHD patients. In one exception, a course of eight 90-min group CBT sessions reduced self-reports and behavioral ratings of anger and hostility and also reduced resting blood pressure (Gidron et al. 1999). The intervention also reduced rehospitalizations and related medical costs (Davidson et al. 2007). This specific approach utilized cognitive restructuring techniques to reduce hostile cognition, relaxation to address angry arousal, and related CBT approaches to modify aggressive behavior. This preliminary evidence suggests that cognitive, behavioral, and affective approaches to modifying anger and hostility in CHD patients may have clinical benefits, and this is encouraging news for further research in this field.
Conclusions
Anger and the closely related traits of hostility and aggressiveness are associated with an increased risk of CVD generally and CHD in particular. These associations have been demonstrated along the full course of the disease process, from the early indications of asymptomatic atherosclerosis to the later emergence and course of clinical manifestations of disease. This association may involve the mediating effects of poor health practices and physiological stress responses. Stress resulting from problematic interpersonal relationships may be a central mechanism in this regard, as chronically angry and hostile persons generally experience limitations in social support and heightened exposure to interpersonal conflict. In some situations, this is compounded by the overcontrol or suppression of angry behavior. There is robust empirical support for the value of CBT in the regulation of anger and preliminary support for the value of this approach to the management of CVD patients. The efficacy of such treatments may be strengthened by also taking into consideration the recurring interpersonal difficulties and themes of conflict that underlie anger and hostility.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.) Washington, D.C.: American Psychiatric Publishing.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, fifth edition (DSM-5). Washington, DC: American Psychiatric Publishing.
Averill, J. R. (1983). Studies on anger and aggression: Implications for theories of emotion. American Psychologist, 38, 1145–1160.
Baron, K., Smith, T. W., Butner, J., Nealey-Moore, J., Hawkins, M., & Uchino, B. (2007). Hostility, anger, and marital adjustment: Concurrent and prospective associations with psychosocial vulnerability. Journal of Behavioral Medicine, 30, 1–10.
Barth, J., Schneider, S., & von Kanel, R. (2010). Lack of social support in the etiology and the prognosis of coronary heart disease: A systematic review and meta-analysis. Psychosomatic Medicine, 72, 229–238.
Beck, R., & Fernandez, E. (1998). Cognitive-behavioral therapy in the treatment of anger: A meta-analysis. Cognitive Therapy and Research, 22, 63–74.
Boyle, S. H., Mortensen, L., Gronbaek, M., & Barefoot, J. C. (2008). Hostility, drinking patterns and mortality. Addiction, 103, 54–59.
Brissette, I., & Cohen, S. (2002). The contribution of individual differences in hostility to the association between daily interpersonal conflict, affect, and sleep. Personality and Social Psychology Bulletin, 28, 1265–1274.
Brodsky, S. L. (2011). Hostility and scorn. In S. L. Brodsky (Ed.), Therapy with coerced and reluctant clients (pp. 141–155). Washington, DC: American Psychological Association.
Bunde, J., & Suls, J. (2006). A quantitative analysis of the relationship between the Cook-Medley Hostility Scale and traditional coronary artery disease risk factors. Health Psychology, 25, 493–500.
Buss, A. H., & Durkee, A. (1957). An inventory for assessing different kinds of hostility. Journal of Consulting Psychology, 21, 343–349.
Buss, A. H., & Perry, M. (1992). The aggression questionnaire. Journal of Personality and Social Psychology, 63, 452–459.
Byrne, D. G. (2000). The frustration of success: Type A behavior, occupational stress and cardiovascular disease. In Stress and health: Research and clinical applications (pp. 411–436). Amsterdam: Harwood Academic Publishers.
Carver, C. S., & Harmon-Jones, E. (2009). Anger is an approach-related affect: Evidence and implications. Psychological Bulletin, 135, 183–204.
Chida, Y., & Steptoe, A. (2009). The association of anger and hostility with future coronary heart disease: A meta-analytic review of prospective evidence. Journal of the American College of Cardiology, 53, 774–778.
Cook, W. W., & Medley, D. M. (1954). Proposed hostility and pharisaic virtue scales for the MMPI. Journal of Applied Psychology, 38, 414–418.
Davidson, K. W., Gidron, Y., Mostofsky, E., & Trudeau, K. J. (2007). Hospitalization cost offset of a hostility intervention for coronary heart patients. Journal of Consulting and Clinical Psychology, 75, 657–662.
Day, A., Howells, K., Mohr, P., Schall, E., & Gerace, A. (2008). The development of CBT programmes for anger: The role of interventions to promote perspective-taking skills. Behavioural and Cognitive Psychotherapy, 36(3), 299–312.
DiGiuseppe, R., & Tafrate, R. C. (2003). Anger treatment for adults: A meta- analytic review. Clinical Psychology: Science and Practice, 10, 70–84.
Esler, M., Schwarz, R., & Alvarenga, M. (2008). Mental stress is a cause of cardiovascular diseases: From scepticism to certainty. Stress and Health: Journal of the International Society for the Investigation of Stress, 24, 175–180.
Everson-Rose, S. A., Lewis, T. T., Karavalos, K., Matthews, K. A., Sutton-Tyrrell , K & Powell, L. H. (2006). Cynical hostility and carotid atherosclerosis in African American and white women: the Study of Women's Health Across the Nation (SWAN) Heart Study. American Heart Journal, 152, 982, e7–13.
Fernandez, E. (2008). The angry personality: A representation on six dimensions of anger expression. In G. J. Boyle, D. Matthews, & D. Saklofske (Eds.), International handbook of personality theory and testing: Vol. 2: Personality measurement and assessment (pp. 402–419). London: Sage Publications.
Fernandez, E. (2010). Toward an integrative psychotherapy for maladaptive anger. In M. Potegal, G. Stemmler, & C. Spielberger (Eds.), The international handbook of anger: Constituent and concomitant biological, psychological, and social processes (pp. 499–514). New York: Springer.
Fernandez, E. (2013). Anger dysfunction and its treatment. In E. Fernandez (Ed.), Treatments for anger in specific populations: Theory, application, and outcome (pp. 1–14). New York: Oxford University Press.
Fernandez, E., & Kerns, R. D. (in press). New prospects for the alleviation of anger in the context of chronic pain. In Z. Bajwa, C. Warfield, & J. Wootton (Eds.), Principles and practice of pain medicine (3rd ed.). New York: McGraw-Hill.
Fernandez, E., & Malley-Morrison, K. (2013). Gender-inclusive and gender informed treatment of anger. In E. Fernandez (Ed.), Treatments for anger in specific populations: Theory, application, and outcome (pp. 213–235). New York: Oxford University Press.
Fernandez, E., & Scott, S. (2009). Anger treatment in chemically-dependent inpatients: Evaluation of phase effects and gender. Behavioural and Cognitive Psychotherapy, 37, 431–447.
Fernandez, E., Day, A., & Boyle, G. J. (2015). Measures of anger and hostility in adults. In G. J. Boyle, D. Saklofske, & G. Matthews (Eds.), Measures of personality and social psychological constructs (pp. 74–100). London: Academic Press.
Friedman, M., Thoreson, C. E., Gill, J. J., Ulmer, D., Powell, L. H., Price, V., et al. (1986). Alteration of Type A behavior and its effects on cardiac recurrences in post-myocardial infarction patients: Summary of results from the Recurrent Coronary Prevention Project. American Heart Journal, 112, 653–665.
Gidron, Y., Davidson, K., & Bata, I. (1999). The short-term effects of a hostility-reduction intervention on male coronary heart disease patients. Health Psychology, 18, 416–420.
Gottdiener, J. S., Kop, W. J., Hausner, E., McCeney, M. K., Herrington, D., & Krantz, D. S. (2003). Effects of mental stress on flow-mediated brachial artery dilation and influence of behavioral factors and hypercholesterolemia in subjects without cardiovascular disease. American Journal of Cardiology, 92, 687–691.
Greenberg, L. S., & Goldman, R. N. (2008). Emotion-focused couples therapy: The dynamics of emotion, love, and power (pp. 351–364). Washington, DC: American Psychological Association.
Greenglass, E. R. (1996). Anger suppression, cynical distrust, and hostility: Implications for coronary heart disease. In Stress and emotion: Anxiety, anger, and curiosity (Vol. 16, pp. 205–225). Philadelphia: Taylor & Francis.
Horowitz, L. M., & Strack, S. (2011). Handbook of interpersonal psychology: Theory, research, assessment, and therapeutic interventions (2011). John Wiley & Sons Inc, Hoboken, NJ.
Holt-Lunstad, J., Smith, T. W., & Uchino, B. N. (2008). Can hostility interfere with the health benefits of giving and receiving social support? The impact of cynical hostility on cardiovascular reactivity during social support interactions among friends. Annals of Behavioral Medicine, 35, 319–330.
Hosseini, S. H., Mokhberi, V., Mohammadpour, R. A., Mehrabianfard, M., & Lashak, N. B. (2011). Anger expression and suppression among patients with essential hypertension. International Journal of Psychiatry in Clinical Practice, 15, 214–218.
Howells, K. (2004). Anger and its links to violent offending. Psychiatry, Psychology and Law, 11, 189–196.
Hutcherson, C. A., & Gross, J. J. (2011). The moral emotions: A social–functionalist account of anger, disgust, and contempt. Journal of Personality and Social Psychology, 100(4), 719–737.
King, C. R., Knutson, K. L., Rathouz, P. J., Sidney, S., Liu, K., & Lauderdale, D. S. (2008). Short sleep duration and incident coronary artery calcification. Journal of the American Medical Association, 300, 2859–2866.
Laughlin, M. J., & Warner, K. (2005). A relational approach to anger: A case study. Journal of Systemic Therapies, 24, 75–89.
Lazarus, R. S. (2000). Cognitive-motivational-relational theory of emotion. In Y. L. Hanin (Ed.), Emotions in sport (pp. 39–63). Champaign: Human Kinetics.
Linden, W., Phillips, M. J., & Leclerc, J. (2007). Psychological treatment of cardiac patients: A meta-analysis. European Heart Journal, 28(24), 2964–2966.
Low, C. A., Thurston, R. C., & Matthews, K. A. (2010). Psychosocial factors in the development of heart disease in women: Current research and future directions. Psychosomatic Medicine, 72, 842–854.
Low, C. A., Matthews, K. A., Kuller, L. H., & Edmundowicz, D. (2011). Psychosocial predictors of coronary artery calcification progression in postmenopausal women. Psychosomatic Medicine, 73, 789–794.
Mauss, I. B., & Gross, J. J. (2004). Emotion suppression and cardiovascular disease: Is hiding feelings bad for your heart? In Emotional expression and health: Advances in theory, assessment and clinical applications (pp. 61–81). New York: Brunner-Routledge.
McCloskey, M. S., Noblett, K. L., Deffenbacher, J. L., Gollan, J. K., & Coccaro, E. F. (2008). Cognitive-behavioral therapy for intermittent explosive disorder: A pilot randomized clinical trial. Journal of Consulting and Clinical Psychology, 76, 876–886.
Mendes De Leon, C. F., Powell, L. H., & Kaplan, B. H. (1991). Change in coronary-prone behaviors in the Recurrent Coronary Prevention Project. Psychosomatic Medicine, 53, 407–419.
Miller, T. Q., Smith, T. W., Turner, C. W., Guijarro, M. L., & Hallett, A. J. (1996). A meta-analytic review of research on hostility and physical health. Psychological Bulletin, 119, 322–348.
Mostofsky, E., Maclure, M., Tofler, G. H., Muller, J. E., & Mittleman, M. A. (2013). Relation of outbursts of anger and acute myocardial infarction. American Journal of Cardiology, 112, 343–348.
Mostofsky, E., Penner, E., & Mittleman, M. A. (2014). Outbursts of anger as a trigger of acute cardiovascular events: A systematic review and meta-analysis. European Heart Journal, 35, 1404–1410.
Newman, J. D., Davidson, K. W., Shaffer, J. A., Schwartz, J. E., Chaplin, W., Kirkland, S., & Shimbo, D. (2011). Observed hostility and the risk of incident ischemic heart disease: A prospective population study from the 1995 Canadian Nova Scotia Health Survey. Journal of the American College of Cardiology, 58, 1222–1228.
Novaco, R. W. (1994). Anger as a risk factor for violence among the mentally disordered. In J. Monahan & H. J. Steadman (Eds.), Violence and mental disorder (pp. 21–59). Chicago: University of Chicago Press.
Novaco, R. W. (2003). The novaco anger scale and provocation inventory: Manual. Los Angeles: Western Psychological Services.
Paivio, S. C., & Pascual-Leone, A. (2010). Emotion-focused therapy for complex trauma: An integrative approach. Washington, DC: American Psychological Association.
Pincus, A. L., & Ansell, E. B. (2013). Interpersonal theory of personality. In T. Millon & M. J. Lerner (Eds.), Handbook of psychology (vol. 5): Personality and social psychology (2nd ed., pp. 141–159). New York: Wiley.
Quartana, P. J., & Burns, J. W. (2010). Emotion suppression affects cardiovascular responses to initial and subsequent laboratory stressors. British Journal of Health Psychology, 15, 511–528.
Ramírez, J. M., & Andreu, J. M. (2006). Aggression, and some related psychological constructs (anger, hostility, and impulsivity): Some comments from a research project. Neuroscience and Biobehavioral Reviews, 30, 276–291.
Renshaw, K. D., Blais, R. K., & Smith, T. W. (2010). Components of negative affectivity and marital satisfaction: The importance of actor and partner anger. Journal of Research in Personality, 44, 328–334.
Robles, T. F., Slatcher, R. B., Trombello, J. M., & McGinn, M. M. (2014). Marital quality and health: A meta-analytic review. Psychological Bulletin, 140, 140–187. doi:10.1037/a0031859.
Sharma, S. (2003). Life events stress, emotional vital signs and hypertension. Psychological Studies, 48, 53–65.
Smedslund, J. (1993). How shall the concept of anger be defined? Theory and Psychology, 3, 5–33.
Smith, T. W. (1994). Concepts and methods in the study of anger, hostility, and health. In A. W. Siegman & T. W. Smith (Eds.), Anger, hostility, and the heart (pp. 23–42). Hillsdale: Lawrence Erlbaum.
Smith, T. W., & Cundiff, J. M. (2011). An interpersonal perspective on risk for coronary heart disease (pp. 471–489). Hoboken: Wiley.
Smith, T. W., & Gallo, L. C. (1999). Hostility and cardiovascular reactivity during marital interaction. Psychosomatic Medicine, 61, 436–445.
Smith, T. W., & Traupman, E. K. (2011). Anger, hostility, and aggressiveness in coronary heart disease: Clinical applications of an interpersonal perspective. In R. Allan & J. Fisher (Eds.), Heart and mind: The practice of cardiac psychology (pp. 197–217). Washington, DC: American Psychological Association. doi: http://dx.doi.org/10.1037/13086-008.
Smith, T. W., Glazer, K., Ruiz, J. M., & Gallo, L. C. (2004). Hostility, anger, aggressiveness, and coronary heart disease: An interpersonal perspective on personality, emotion, and health. Journal of Personality, 72, 1217–1270.
Smith, T. W., Uchino, B. N., Berg, C. A., Florsheim, P., Pearce, G., Hawkins, M., … Yoon, H. C. (2007). Hostile personality traits and coronary artery calcification in middle-Aged and older married couples: Different effects for self-reports versus spouse-ratings. Psychosomatic Medicine, 69, 441–448.
Smith, T. W., Traupman, E., Uchino, B. N., & Berg, C. (2010). Interpersonal circumplex descriptions of psychosocial risk factors for physical illness: Application to hostility, neuroticism, and marital adjustment. Journal of Personality, 78, 1011–1036.
Smith, T. W., Uchino, B. N., Florsheim, P., Berg, C. A., Butner, J., Hawkins, M., … Yoon, H.-C. (2011). Affiliation and control during marital disagreement, history of divorce, and asymptomatic coronary artery calcification in older couples. Psychosomatic Medicine, 73, 350–357.
Smith, T. W., Baron, C. E., & Grove, J. L. (2014). Personality, emotional adjustment, and cardiovascular risk: Marriage as a mechanism. Journal of Personality, 82, 502–514.
Smith, T. W., Uchino, B. N., Bosch, J. A., & Kent, R. G. (in press). Trait hostility is associated with systemic inflammation in married couples: An actor-partner analysis. Biological Psychology.
Spielberger, C. D. (1988). Manual for the state–trait anger expression inventory. Odessa: Psychological Assessment Resources.
Spielberger, C. D. (1991). State-trait anger expression inventory: Revised research edition: Professional manual. Odessa: Psychological Assessment Resources.
Spielberger, C. D. (1999). STAXI-2: State–trait anger expression inventory professional manual. Odessa: Psychological Assessment Resources.
Steptoe, A., & Kivimaki, M. (2013). Stress and cardiovascular disease: An update on current knowledge. Annual Review of Public Health, 34, 337–354.
Strike, P., & Steptoe, A. (2005). Behavioral and emotional triggers of acute coronary syndromes: A systematic review and critique. Psychosomatic Medicine, 67, 179–186.
Suarez, E. C. (2012). The association between measures of inflammation and psychological factors associated with an increased risk of atherosclerotic cardiovascular disease: Hostility, anger, and depressed mood and symptoms. In S. C. Segerstrom (Ed.), The Oxford handbook of psychoneuroimmunology (pp. 170–194). New York: Oxford University Press.
Thomas, S. P. (1997). Women’s anger: Relationship of suppression to blood pressure. Nursing Research, 46, 324–330.
Williams, J. E., Din-Dzietham, R., & Szklo, M. (2006). Trait anger and arterial stiffness: Results from the atherosclerosis risk in communities study. Preventive Cardiology, 9, 14–20.
Wranik, T., & Scherer, K. R. (2010). Why do I get angry? A componential appraisal approach. In M. Potegal, G. Stemmler, & C. Speilberger (Eds.), International handbook of anger (pp. 243–266). New York: Springer.
Wright, R. A., & Stewart, C. C. (2012). Multifaceted effects of fatigue on effort and associated cardiovascular responses. In How motivation affects cardiovascular response: Mechanisms and applications (pp. 199–218). Washington, DC: American Psychological Association.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Singapore
About this entry
Cite this entry
Fernandez, E., Smith, T.W. (2016). Anger, Hostility, and Cardiovascular Disease in the Context of Interpersonal Relationships. In: Alvarenga, M., Byrne, D. (eds) Handbook of Psychocardiology. Springer, Singapore. https://doi.org/10.1007/978-981-287-206-7_31
Download citation
DOI: https://doi.org/10.1007/978-981-287-206-7_31
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-287-205-0
Online ISBN: 978-981-287-206-7
eBook Packages: Behavioral Science and PsychologyReference Module Humanities and Social SciencesReference Module Business, Economics and Social Sciences