
Abstract
Latin America and the Caribbean is the region with the largest population concentrated in megacities, 81% of the population live in urban areas, and by 2050 the proportion will hover at 89%. México, with its inequitable healthcare access and almost 100 million people living in 4,189 urban settlements faces a sustainable city agenda for climate action and good health and well-being. This chapter addresses morbidity and mortality pre-pandemic data related to heat-related diseases from the National Morbidity Yearbook and the National Mortality Census to identify and characterize trends by state, age, gender, and environmental conditions under the ICD-10 system. Evidence presented in a municipal case study indicates that ischemic heart disease counts for ≈33% of total deaths in the urban context, being an elderly female population above 55 years old the most vulnerable.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
The IPCC’s Special Report on the Impacts of 1.5 °C Global Warming [1] underlined the significant difficulty for cities in developing adaptation measures that allow for the maintenance of favorable circumstances for the population. The rise in sea level poses a risk of flooding in around 130 port towns worldwide with populations over one million, resulting in a slew of disputes related to population displacement and migration. However, there is evidence that climate change poses significant challenges to water, energy, food insecurity, and transportation infrastructure. Similarly, the increased frequency of heatwaves, hurricanes, forest fires, and changes in ecosystems endanger various tourist activities critical to the inhabitants’ economic activity. Although Reyes et al., [2] assert that new research approaches have increased awareness of the complexity that climate change implies for sustainable development, it will remain necessary to address fundamental issues such as increasing the certainty of environmental data monitoring [3], which aid in comprehending the problem. Additionally, it will be required to develop protocols that facilitate comparisons between investigations [4] to facilitate a more expansive decision-making process.
The Urban Heat Islands (UHI) refer to the increase in temperature experienced by cities concerning the surrounding non-urban areas. This is a typical occurrence regardless of the city’s size or climate type. The UHI's impact fields have been classified along seven axes: energy, health-morbidity, health-mortality, urban environmental quality, risk and vulnerability, human comfort, and demography [5]. It is critical to emphasize that two decades ago, UHI were demonstrated to have a considerable effect on building energy use [6]. Indeed, climate variability now plays a critical role in the development of methods for gaining greater control over the energy use of buildings [7]. Similarly, It is critical to optimize and establish criteria for a more effective inquiry design to collect more relevant data [8].
Urban overheating has several harmful implications on human health. Temperature increases drive greater air pollution levels and the duration of heatwaves, which can aggravate the health of people with chronic conditions [9]. Climate change increases respiratory and allergy illnesses because of the population's overexposure to ozone, smoke, pollen, mold, and diseases derived from water and food pollution [10]. In this regard, overheating can amplify the negative consequences of climate change on urban health. On the other hand, it has been calculated that temperature rises have a direct effect on mortality during the hot season, reaching an average estimate of 37%. However, the degree of effect varies significantly between countries and subregions [11]. As a result, additional research must define more precisely the boundaries of the impact of UHI on human health [12]. A greater understanding of inhabitants’ thermal comfort will enable more effective urban design [13], which should ideally reach neighborhood-scale [14], involving wind fluxes and vegetation morphology [15].
Elderly people, children, women, and those with chronic diseases, as well as those taking particular medications will be the most vulnerable to fluctuations in the environment’s temperature and humidity, as well as to infections spread by mosquito bites [1]. Water pollution is particularly hazardous to pregnant women, in fact, women are historically highly vulnerable to natural disasters. For their part, children under the age of five account for 88% of morbidity due to climate change, as they are more prone to become ill as a result of diverse environmental conditions. Indigenous peoples are also a vulnerable group, as they cannot access food, water, and shelter. It is critical to emphasize that those who work outdoors are directly exposed to poor air quality and various climatic occurrences [10]. Air pollution, in general, can have adverse effects on the respiratory system, heart, kidneys, eyes, skin, brain, bones, blood, and blood vessels. Air pollution has been shown to impair sleep, reproduction, and metabolism. Additionally, it can induce or worsen allergies, diabetes, and certain types of cancer [16, 17].
2 Motivation and Justification
In cities, high and extreme temperatures stimulate the concentration of pollutants. Different contaminants alter rainfall patterns and degrade water quality, wreaking havoc on the subsurface layers and aquatic ecosystems’ health. As a result, these pollutants amplify the effect of heat islands by retaining radiation in and around cities [18]. Prolonged exposure to pollutants influences the corrosion of metals, minerals, and vegetation; thus, it is critical to use Geographic Information Systems (GIS) to interpolate data that aids in decision-making to resolve the problem [19]. The shape of flora can help mitigate the effects of UHIs [20], yet the intensities of UHI are lower in cities with arid or semi-arid climates than in green places [21]. As a result, comprehending these dynamics is critical when considering the design or morphology of a city.
Thus, Latin America is the region with the largest population concentrated in megacities, 14.2% reside in six cities with 10 million inhabitants [22] challenged by global warming that exacerbates the risk of heat-related mortality. For decades, there has been a warning about the effects in Mexico and its relationship with the etiology of vector-borne, acute respiratory, and diarrheal diseases, or heat stroke due to extreme weather events on the health of the Mexican population [23]. Therefore, it is essential to understand patterns of mortality rates in urban areas as a matter of public policy interest [24]. This study reports morbidity and heat-related diseases in terms of the ICD-10 system for a pre-pandemic scenario in Mexico (2019), including sociodemographic, age, and environmental aspects in the national context, and through the selection of a local case study, the building cooling demands of two different locations can be observed.
3 Method
This study analyzed morbidity and mortality pre-pandemic data (2019) related to heat-related diseases to identify and characterize components by state, age, gender, and environmental conditions under the ICD-10 system. This study analyzes collected data from the Mexican health system under the criteria described below, in addition, a Case Study of Ensenada city from ongoing research is briefly explored to illustrate energy aspects regarding land surface temperature (LST) on contrasting cooling energy demand for two nodes with a different urban condition:
-
Taxonomy. Defined by the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), a widely used diagnostic tool for epidemiology, health management, and therapeutic purposes worldwide [25].
-
Data sources. On health and demographic aspects, Observations from the vital statistical data published in censuses and surveys of The National Institute of Statistics, Geography (INEGI, Census 2020) [26, 27], monthly cases per month of occurrence from the Morbidity Yearbook (period 1984–2019) of Mexico's Secretariat of Health [28]. On the environment, normalized climate data from the National Meteorology Service (SMN, period 1981–2010), interpolated data through the Meteonorm® software, which uses the climatic information values from the database of the Global Energy Balance File (GEBA) of the World Meteorological Organization (WMO) [29], and thermal maps from the Informatics Unit for Atmospheric and Environmental Sciences (UNIATMOS, period 1902–2015) [30].
-
Study Area. (a) National level. Mexico is a federation of 32 states and is bounded on the north by the USA, and on the southeast by Guatemala and Belize. It is the world's eleventh most populated country, with over 124 million citizens, 77% of whom live in metropolitan areas. The population is young, with roughly 27% of residents under the age of 15 and only 7% over 65. Inequality of income and poverty are ongoing health problems. Mexico has the highest rate of income inequality in the OECD [31]. (b) Municipal and city level (case study). The municipality of Ensenada is bounded at 28° and 32° N and −112.8° and −116.9 W, with its 52.51 thousand km2 of territory, represents 74.1% of the state of Baja California. For its part, Ensenada is a coastal city situated on Todos Santos Bay, a mid-rise building city that presents a mild semi-arid climate (Köppen BSk) [32].
-
LST Retrieval. An automated mapping algorithm created in ERDAS IMAGINE 2014 compatible with LANDSAT 8 was applied in Ensenada city. For data processing, it uses Bands 10, 4, and 5. The emissivity corrected land surface temperature Ts was calculated as follows using brightness temperature (BT), λ is the wavelength of emitted radiance, and ελ is the emissivity calculated [33]:
$$T_{S} = \frac{{{\text{BT}}}}{{\left\{ {1 + \left[ {\left( {\frac{{\lambda {\text{BT}}}}{\rho }} \right)\ln \varepsilon_{\lambda } } \right]} \right\}}}$$ -
Energy simulation. Estimation of energy loads on typical housing in Ensenada city was conducted using TRNSYS® 17, a simulation software used in the fields of building energy performance to simulate the behavior of transient systems [34].
4 Results
Morbidity is recognized as a prelude to mortality, health systems define a picture of heat-related diseases under the ICD-10 system, the same illnesses and symptoms summarized by several researchers [35,36,37]. Table 1 and Fig. 1 report hospitalizations during the year of study (2019) concerning gender, month, and state. It is important to note that J18.2, J13, and J14, non-acute, care, or self-care cases were not included. As seen below, women are susceptible to respiratory diseases and heatstroke with a representativity of 56% and 54%, while men report vulnerability to ischemic and cerebrovascular diseases, 59% and 53%, respectively.

Heat-related hospitalizations in México based on UNIATMOS map (period: 1902-2015) (2019)
The map shows the 32 Federal Entities (FE) referred to through blue bubbles that indicate City of Reference (CoR), which concentrates the largest population of each FE, the total population of Mexico is 126,014,024 inhabitants, the most populated state is the Estado de México with 16,992,418 people and the least populated is Colima with 731,391 people. The national average of demographic concentration in CoR is 22.9% with a minimum of 1% in the state of Tlaxcala, up to Aguascalientes with ±60.6%, Mexico City, although it concentrates ±79% of its population, is distributed in its 16 delegations, of which it concentrates ±19% in Iztapalapa with 1,835,486 residents. The population with access to health services (white bubbles) in each CoR has a national average of 76%, the minimum CoR is Tuxtla Gutierrez in Chiapas at 59.1%, and the maximum is La Paz, Baja California Sur at 86.5%. The contrast in the diameter of the white and blue bubbles indicates the concentration of each state, regarding their access to health.
Even though the highest number of hospitalizations in México occurs in January due to the high prevalence of respiratory diseases, pneumonia, and influenza, the CoR’s predominant climate is Cwb (subtropical highland climate) [38], with the warmest month being May. The map depicts the may thermal distribution of the absolute extreme maximum temperatures reported by the UNIATMOS with historical datasets from 1902–2015, and temperatures ranging from 15.3 to 52.5 °C. The preceding is evident in the inverse trend that cases of respiratory diseases present concerning those of heat exposure, which increase in percentage terms during May, especially in the female population (14.8%), June (19.5%), July (18%), and August (18.2%). Similar behavior can be seen in cerebrovascular diseases, whose distribution is sustained and regular throughout the year, but with significant months where the male population stands out, such as July (10.6%), August (7.7%), and October (10.1%).
Referring back to the research aims, this national prelude on morbidity set an opposite reference to address mortality aspects in a more detailed resolution. The mortality rate connected with heat-related disorders was observed in the municipality of Ensenada, Baja California. 87,249 people live in urban regions and 43,474 individuals live in rural areas. The number of people who died in urban and rural areas in 2019 is shown in Table 2. According to the data, approximately 95.9% (1,145) of the deceased resided in urban regions and 4.1% (48 people) in rural areas. According to the data in this table, the major cause of circulatory death in both locations was ischemic heart disease, followed by cerebrovascular illness. However, influenza and pneumonia had a greater mortality rate attributable to respiratory causes in the urban context. Interestingly, the data in this table indicate that most of the population died from circulatory reasons.
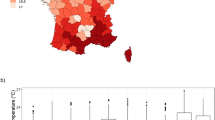
The four major causes of mortality are depicted in Fig. 2. The findings indicate that the highest death rate was observed in a population over the age of 55. According to this figure, women above the age of 70 have an elevated death rate. Additionally, the data indicates that 60% of deaths occurred among men and 40% occurred among women. Additionally, the findings indicated an increase in mortality among men (in blue) due to ischemic heart (I20-I25), with a notable increase between 35 and 39 years -productive age- and 60–64 years and a similar but, diluted pattern in cerebrovascular disease (I60-I69) records. Contrary to what was indicated by the number of hospitalizations nationwide, where it was appreciated that the female population was more susceptible through a clinical picture related to respiratory diseases. As for conditions of hyperthermia, women have upward trends and peak values in older ages, in all four cases of diseases, this can be seen from 7074 years with peak values in the last stage of life, 85 and more.

Mortality rate in Ensenada by gender, urban/rural context, and age based on UNIATMOS map & Pyrgou A & Santamouris M (2018)
4.1 A Brief Exploration of the Urban Overheating and Energy
Due to the escalation of Urban Overheating as a result of climate change, new issues have arisen in addressing the dangers and energy needs associated with meeting building thermal conditions. This section briefly explores the importance of paying attention to the vulnerability of inhabitants of temperate climates because of the thermal adaptability during the warm season (August). Remote sensing techniques were used to correlate LST Overheating criteria with energy consumption of a prototypical residential building and two dissimilar urban nodes in the CoR of Ensenada, Baja California, a port city with BSk climate condition, 330,652 residents, and 105,736 housing units [27] is situated on 31.86 N and −116.60 W [32].
An algorithm for automated mapping of the Land Surface Temperature using Landsat eight thermal infrared sensor Band 10 was performed, as seen in Fig. 3, is useful to observe the urban thermal environment of the ground surface across the city layout. In addition, an accurate and representative hourly time series for a weather typical year using a stochastic model through Meteonorm software was calculated. For this purpose, the location situation was set as “city” and statistical uncertainty is 8% on Global Radiation (W/m2), 7% on Beam Radiation (W/m2) and 1.1 °C on Dry Bulb Temperature (°C). Each location is related to a Basic Geostatistical Area (AGEB), which constitutes the basic unit of the INEGI´s National Geostatistical Framework (Table 3).

A brief exploration of urban overheating and energy. Imagen Landsat 8, retrieval date: Aug 20th, 2019, 6:16 pm
A numerical analysis was developed using a mathematical subroutine through Type 56 of TRNSYS® 17 software, a typical urban housing with a construction area of 38.5 m2 and a volume of 104 m3 was analyzed, which is built with concrete block walls of 0.12 m thick with a “U” value of 3.918 W/m2K, a joist and filler block roof system of 0.17 m thick and a “U” value of 1.98 W/m2K, 3 mm single glass window with U Value of 5.73/m2K reinforced concrete floor 0.10 m thick with “U” value of 4.68 W/m2K, wooden door 2.47 W/m2K.
Internal Building loads were defined for a typical family of four occupants with the following scheduled occupancy, one working parent, one dedicated to household duties, and two children with student activities. The occupant´s internal gains were defined as standing light work (185 W per occupant). Internal gain due to equipment considered with a radiative gain peak load of 5.52 kWh, convective peak loads of 1.61 kWh, artificial lightning gains of 5 W/m2, and finally a constant air change per hour rate (ACH) of 1.0, as infiltration/ventilation. The cooling system´s thermal and energy performance were pre-calculated to study the cooling demand of a real single package of 13 SEER, 1200 CFM, and a total net capacity of 35,000 BTU [39].
Figure 3 shows that July and August are the warmest months with the highest cooling energy demand, from September the temperatures present a decrease. However, when analyzing the relative humidity of the two nodes, it can be observed that node B presents a drier climate compared to the A values. Thus, to determine the energy consumption of the city of Ensenada’s warmest and coldest nodes, an energy simulation of these two nodes was conducted. It was discovered that the climate of node A consumes more energy during the summer, which is associated with the low humidity content of the environment, as illustrated in the figure. Contrary to node A, the B node has a greater number of operational days than July. This is because the average temperature in August is higher, which results in a more significant number of operational days.
The operating efficiency of the cooling system has a close relationship with the site´s climatic conditions since the cooling unit has refrigerant condensation problems. In the same figure, it can be seen that the cooling unit is affected when temperatures are greater than 30 C. While, in the case of relative humidity, it affects when you have lower relative humidity.
5 Discussion
Mexico is second only to the United States in terms of obesity prevalence; in terms of life expectancy, women live an average of 77.7 years, and men live to the age of 72. After diabetes mellitus, the only other heat-related chosen cause of death is ischemic heart disease (72.45 per 1000 total deaths). As in Pyrgou and Santamouris [37], the difficulty of predicting the adaptation potential of the population in the face of rising temperatures in the future is highlighted. Likewise, the results of this work also agree with the findings of Liu, et al. [36] about the importance of generating mitigation plans for vulnerability to hyperthermia conditions and managing emergency plans that favor timely actions. Ideally, local governments should implement strategies based on Geographic Information Systems (GIS), to solve the lack of information. However, in Mexico, there are few cases in which there is an uprising of this type throughout the cities.
Mexico is also geographically extensive, has a continental area of 1,959,248 km2, with 21,000 primary care units operated by public institutions, and has a great variety of climates that hinder specific preventive medicine strategies, to mention, in the 32 CoR (Af, As, Aw, Bsh, BSk, Bwh, Bwk, Cfa, Cwb) with warm months that differ from April to August, there are localities with historical average maximum temperatures of 39.6 °C in Hermosillo, Sonora and extreme temperatures up to 52.0 °C in Mexicali, Baja California. However, the recurrence and magnitude of heatwaves are increasingly studied in temperate climates [40].
Additionally, the SARS-CoV-2 health crisis imposes a new constraint on the standardization of records, due to the federal government's hospital conversion edict. The most significant constraint on conducting mortality research is the unavailability of high-resolution geographic resources. The national basic geostatistical units (AGEBS) do not include mortality data, and the reasons for death are not linked to specific climatic zone scenarios. The development of protocols for reporting and monitoring claims related to the health of building occupants through Building Information Modeling (BIM) may represent a significant step forward; although in Mexico only the standard NMX-C-527–1-ONNCCE-2017 has been published [41], representing an alternative that is difficult to implement in the short or medium term.
6 Conclusion
Morbidity results in this study showed that the impact on women's health by presenting higher rates than men due to heat exposure (54%), respiratory failure (56%), and influenza (54%). However, the evidence indicates that the impact of pneumonia is similar between men and women. In contrast, men are significantly more affected by schematic heart diseases (59%) and cardiovascular accidents (53%). The latter is worrying for the public health system, given the high rate of obesity that leads to diseases such as diabetes mellitus and cerebrovascular disease.
In terms of Urban Overheating, there is a marked trend in hospitalization for reasons related to heat exposure. The three types of climates presented in 19 Urban areas of reference around México with the highest incidence are Subtropical highland climate (Cwb), Cold semi-arid climate (BSk), and Tropical Savana climate (Aw), they represent 60%.
The present analysis has substantial constraints as a result of the poor level of integration of information management and recording in the national health sector, which is composed of a mix of social insurance schemes, a voluntary public program for the uninsured, and private insurance systems. Among the existing limitations and conclusions, the following can be mentioned:
-
Urban overheating is a differential phenomenon that promotes risks in extreme heat events in urban areas of adverse sociodemographic characteristics of the city.
-
Acute respiratory infections in autumn/winter and circulatory diseases in spring/summer are dominant risk factors and significant concerns due to income inequality, gentrification, health inequities, and access to health system services.
-
Health access systems must develop preventive healthcare programs geared around demographic factors such as gender and age distribution during specific periods of urban overheating exacerbation on specific local climate zone.
-
Integrating health statistics into high-resolution geographic systems is critical for establishing preventive measures for chronic conditions in developing countries. [42].
-
The evidence refers to the need for alert protocols that connect heat-related pathologies to environmental and atmospheric conditions by seasons, such as temperature, humidity, and air quality.
-
A robust methodological strategy for smart cities should consider a tracking data philosophy [43] of relevant tools currently used such as Satellite Remote Sensing, stationary and mobile weather stations, online and print media, prospective scenarios, sectors by density, and landscape typology (residential, offices, industry, commerce, etc.) and implement protocols based on dynamic platforms, i.e., BIM, IoT, RFID, and/or GIS also by sectors depending on their sociodemographic aspects and national regulations [41].
References
Roberts D, Pidcock R, Chen Y, Connors S, Tignor M (2019) 2018: global warming of 1.5 °C. An IPCC special report on the impacts of global warming of 1.5 °C above pre-industrial levels and related global greenhouse gas emission pathways, in the context of strengthening the global response to the threat of climate c. Nairobi
Reyers B, Folke C, Moore ML, Biggs R, Galaz V (2018) Social-ecological systems insights for navigating the dynamics of the anthropocene. Annu Rev Environ Resour 43:267–289
Xi DDZ, Taylor SW, Woolford DG, Dean CB (2019) Statistical models of key components of wildfire risk. Annu Rev Stat Appl 6:197–222
Otto FEL (2017) Attribution of weather and climate events. Annu Rev Environ Resour 42:627–646
Gonzalez-Trevizo ME, Martinez-Torres KE, Armendariz-Lopez JF, Santamouris M, Bojorquez-Morales G, Luna Leon A (2021) Research trends on environmental, energy and vulnerability impacts of Urban Heat Islands: an overview. Energy Build 246(111051):1–27
Santamouris M et al (2001) On the impact of urban climate on the energy consuption of building. Sol Energy 70(3):201–216
Li H, Wang Z, Hong T (2021) A synthetic building operation dataset. Sci Data 8(1):1–14
Kim SW, Brown RD (2021) Urban heat island (UHI) variations within a city boundary: A systematic literature review. Renew Sustain Energy Rev 148(August 2020):111256
United States Environmental Protection Agency (2021) “Heat Island.” Heat Island Impacts
Levy BS, Patz JA (2017) The impact of climate change on public health, human rights, and social justice, vol 1–5. Elsevier Inc
Vicedo-Cabrera AM et al (2021) The burden of heat-related mortality attributable to recent human-induced climate change. Nat Clim Chang 11(6):492–500
Leal Filho W et al (2021) Addressing the urban heat islands effect: a cross-country assessment of the role of green infrastructure. Sustain 13(2):1–20
Pigliautile I, Pisello AL, Bou-Zeid E (2020) Humans in the city: Representing outdoor thermal comfort in urban canopy models. Renew Sustain Energy Rev 133(August):110103
Martinez S, Machard A, Pellegrino A, Touili K, Servant L, Bozonnet E (2021) A practical approach to the evaluation of local urban overheating—a coastal city case-study. Energy Build. 253:111522
Di Bernardino A et al (2021) Urban microclimate modelling for comfort and energy studies. In Palme M, Salvati A (eds) Urban microclimate modelling for comfort and energy studies, 1st ed., Cham
Schraufnagel DE et al (2019) Air pollution and noncommunicable diseases: a review by the forum of international respiratory societies’ environmental committee, part 1: the damaging effects of air pollution. Chest 155(2):409–416
Schraufnagel DE et al (2019) Air pollution and noncommunicable diseases: a review by the forum of international respiratory societies’ environmental committee, part 2: air pollution and organ systems. Chest 155(2):417–426
Mirzaei PA (2015) Recent challenges in modeling of urban heat island. Sustain Cities Soc 19:200–206
Vidal F, Vicente R, Mendes Silva J (2019) Review of environmental and air pollution impacts on built heritage: 10 questions on corrosion and soiling effects for urban intervention. J Cult Herit 37:273–295
Dugord PA, Lauf S, Schuster C, Kleinschmit B (2014) Land use patterns, temperature distribution, and potential heat stress risk—the case study berlin, Germany. Comput Environ Urban Syst 48:86–98
Shahraiyni HT, Sodoudi S, El-Zafarany A, El Seoud TA, Ashraf H, Krone K (2016) A comprehensive statistical study on daytime surface urban heat island during summer in urban areas, case study: Cairo and its new towns. Remote Sens 8(8):1–20
ECLAC—United Nations (2021) Regional urban statistics: Urban and cities platform. Urban and cities platform of Latin America and the Caribbean [Online]. Available: https://plataformaurbana.cepal.org/en/regional-urban-statistics. [Accessed 01 Dec 2021]
Instituto Nacional de Ecología and Instituto Nacional de Salud Publica (2006) Estudio Diagnostico sobre los efectos del cambio climático en la salud humana de la poblacion de México. Mexico
Baca-López K, Fresno C, Espinal-Enríquez J, Flores-Merino MV, Camacho-López MA, Hernández-Lemus E (2021) Metropolitan age-specific mortality trends at borough and neighborhood level: the case of Mexico City. PLoS One 16(1 January):1–26
World health organization (2016) International statistical classification of diseases and related health problems, 1st edn. WHO Press, Switzerland
Instituto Nacional de Estadística y Geografía (INEGI) (2021) Mortalidad. Registros administrativos—estadísticas vitales [Online]. Available: https://www.inegi.org.mx/programas/mortalidad/#Tabulados. [Accessed: 15 Nov 2021]
Instituto Nacional de Estadística y Geografía (INEGI) (2021) SCINCE 2020. Sistema para la Consulta de Información Censal. [Online]. Available: https://gaia.inegi.org.mx/scince2020/. [Accessed: 01 Nov 2021]
Gobierno de México (2021) Casos de enfermedad por mes de ocurrencia (2019). Anuario de morbilidad 1984–2019. [Online]. Available: https://epidemiologia.salud.gob.mx/anuario/html/casos_mes.html. [Accessed: 15 Nov 2021]
Genossenschaft Meteotest (2020) Handbook part I: Software. Bern
Fernández Eguiarte A et al. Mapa de temperatura máxima extrema absoluta (1902-2015), Umbrales de exposición. Atlas climático de México, Unidad de Informática para las Ciencias Atmosféricas y Ambientales (UNIATMOS), Instituto de Ciencias de la Atmósfera y Cambio Climático, UNAM. [Online]. Available: http://uniatmos.atmosfera.unam.mx/ACDM/servmapas. [Accessed: 01 Dec 2021]
Gonzalez-Block MA, Reyes Morales H, Cahuana-Hurtado L, Balandran A, Mendez E (2020) Mexico health system review. Health Syst Transit 22(2)
XXII Ayuntamiento de Ensenada (2017) Anuario estadistico municipal de Ensenada, Ensenada
Avdan U, Jovanovska G (2016) Algorithm for automated mapping of land surface temperature using LANDSAT 8 satellite data. J Sensors 2016
Thermal Energy System Specialists (2021) What is TRNSYS?. [Online]. Available: http://www.trnsys.com/. [Accessed: 06 Nov 2021]
Aghamohammadi N, Fong CS, Idrus MHM, Ramakreshnan L, Sulaiman NM (2021) Environmental heat-related health symptoms among community in a tropical city. Sci Total Environ 782:146611
Liu X, Yue W, Yang X, Hu K, Zhang W, Huang M (2020) Mapping urban heat vulnerability of extreme heat in Hangzhou via comparing two approaches. Complexity 2020
Pyrgou A, Santamouris M (2018) Increasing probability of heat-related mortality in a mediterranean city Due to urban warming. Int J Environ Res Public Health 15(8):1–14
Beck HE, Zimmermann NE, McVicar TR, Vergopolan N, Berg A, Wood EF (2018) Present and future köppen-geiger climate classification maps at 1-km resolution. Sci Data 5:1–12
TRANE (2008) TRANE product data. Single packaged convertible gas/electric 13 SEER. [Online]. Available: http://www.climatesolutionsinc.com/wp-content/uploads/Trane-2YCC3-Brochure.pdf. [Accessed: 18 Nov 1BC]
Molina MO, Sánchez E, Gutiérrez C (2020) Future heat waves over the mediterranean from an Euro-CORDEX regional climate model ensemble. Sci Rep 10(1):1–10
Gobierno de México, Declaratoria de vigencia de la Norma Mexicana NMX-C-527–1-ONNCCE-2017. México: Diario Oficial de la Federación, 2017, p. 1.
United States Global Change Research Program (2021) National integrated heat health information system (NIHHIS) | U.S. climate resilience toolkit [Online]. Available: https://toolkit.climate.gov/tool/national-integrated-heat-health-information-system-nihhis. [Accessed: 28 Nov 2021]
California Department of Public Health and the Centers for Disease Control’s (CDC) (2021) Tracking California information action for healthier communities. Views, maps and data [Online]. Available: https://trackingcalifornia.org/main/maps-and-data. [Accessed: 01 Nov 2021]
Acknowledgements
The time dedicated to this research was possible due to the UABC internal financing research projects, and its Library system data base, Programa para el Desarrollo Profesional Docente (PRODEP) and research activities supported by Consejo Nacional de Ciencia y Tecnología (CONACyT) through its Sistema Nacional de Investigadores (SNI). In addition, the authors would like to gratefully acknowledge B. Eng. Randy Martinez for his valuable orientation and our undergraduate students Alina Vasquez, Linette Carrillo, Lidia Ornelas, Melissa Salgado, and Erick Sanchez for their enthusiasm and assistance with data collection details.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
González-Trevizo, M.E., Martínez-Torres, K.E., Luna-León, A., Armendáriz-López, J.F., Sandoval-Félix, J. (2022). Impact of Urban Overheating and Heat-Related Mortality in Mexico. In: Aghamohammadi, N., Santamouris, M. (eds) Urban Overheating: Heat Mitigation and the Impact on Health. Advances in Sustainability Science and Technology. Springer, Singapore. https://doi.org/10.1007/978-981-19-4707-0_17
Download citation
DOI: https://doi.org/10.1007/978-981-19-4707-0_17
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-4706-3
Online ISBN: 978-981-19-4707-0
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)