
Abstract
First, this chapter introduces the definition and classification of external causes of child traffic injury and reports the current situation and trends in mortality, years of life lost, years lived with disability, and disability-adjusted life years from road traffic injuries among children over the world, based on the Global Burden of Disease (GBD) 2019 estimates and other published literature. We describe differences in child traffic injury burden across age group, year, month, date, time, and transportation method. Then, we systematically summarize the major influencing factors of child road traffic injury from three aspects: human factors, vehicle factors, and environment factors. Finally, we introduce intervention theories and basic strategies (including Haddon’s ten basic strategies, 5Es intervention theory, active and passive intervention strategies) and summarize the published effective prevention interventions.
Data in this chapter from online resources of the Global Burden of Disease Study 2019 (GBD 2019) and reports by the World Health Organization (WHO). Using the data, we regraphed all figures. Therefore, this chapter does not involve informed consent and ethical review.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keyword
12.1 Introduction
Road traffic injury (RTI) has become an important global public health issue, with accelerating industrialization and urbanization. The Global Status Report on Road Safety 2018 by the World Health Organization shows that the number of road traffic deaths is approximately 1.35 million each year, yielding great impact on people’s health.
RTI is currently a leading cause of global child mortality. According to the World Report on Child Injury Prevention by the World Health Organization (WHO), RTI accounts for approximately 262 thousand child deaths every year, and more than 10 million children suffer a non-fatal injury. RTI is the leading cause of deaths for young people aged 15–19 years.
12.1.1 Definition
12.1.1.1 Children
We focus on road traffic crashes occurring on children younger than 18 years old according to the definition from the Convention on the Rights of the Child. Our analyses, however, were expanded to 19 years old because of data availability of GBD 2019 estimates.
12.1.1.2 Injury and Traffic Injury
According to the World Report on Child Injury Prevention, an injury event is defined as “the physical damage that results when a human body is suddenly subjected to energy in amounts that exceed the threshold of physiological tolerance—or else the result of a lack of one or more vital elements, such as oxygen.”
Road traffic crash is defined as “a collision or incident that may or may not lead to injury, occurring on a public road and involving at least one moving vehicle.”
Road traffic injury is defined as “fatal or non-fatal injuries incurred as a result of a road traffic crash.”
12.1.2 Classification
Currently, the International Classification of Diseases, 10th Revision (ICD-10), is widely used to classify type of injuries over the world. Based on the ICD-10, the Centers for Disease Control and Prevention (CDC) in the United States develops an injury matrix by combining external cause and intent of injury which specifies the classification of traffic injury (Table 12.1).
12.2 Epidemiological Characteristics
12.2.1 Mortality
Data from GBD 2019 by the Institute for Health Metrics and Evaluation (IHME) was used to evaluate the latest epidemiological characteristics of road traffic injury. From 1990 to 2019, global RTI mortality rates all decreased substantially for children under 5, aged 5–15 years, and 15–19 years. During the study time period, children from low-income countries generally had much higher RTI mortality rates than those from high-income countries for under-5 children and children aged 5–14 years. The exceptional trend for children aged 15–19 years mainly reflects differences in motorization and prevention efforts across the four country income categories. In 2019, the child RTI mortality rates for three age groups were 5.80 (95% UI: 4.65–7.51), 4.26 (95% UI: 3.69–4.95), and 11.30 (95% UI 10.03–12.55) deaths per 100,000 people, respectively (note: UI, uncertainty interval) (Figs. 12.1, 12.2 and 12.3).

Global road traffic injury mortality among under-5 children, 1990–2019. (Data source: GBD Compare, 2019)

Global road traffic injury mortality among children aged 5–14 years, 1990–2019. (Data source: GBD Compare, 2019)

Global road traffic injury mortality among children aged 15–19 years, 1990–2019. (Data source: GBD Compare, 2019)
Road traffic injuries emerged as a leading cause of deaths for three age groups in both 1990 and 2019. Specifically, the rank of road injuries fell from the 13th place in 1990 to the 14th place in 2019 (Fig. 12.4). In 2019, the rank of road injuries was the second place for children aged 5–14 years and the first place for children aged 15–19 years, respectively (Figs. 12.5 and 12.6).

Leading causes of global deaths for under-5 children, 2019 vs. 1990. (Data source: GBD Compare, 2019)

Leading causes of global deaths for children aged 5–14 years, 2019 vs. 1990. (Data source: GBD Compare, 2019)

Leading causes of global deaths for children aged 15–19 years, 2019 vs. 1990. (Data source: GBD Compare, 2019)
12.2.2 Years of Life Lost (YLLs)
Over the past three decades, YLLs per 100,000 population due to RTI all decreased in three age groups and four country income categories; but the rates were lowest among high-income countries. YLLs per 100,000 population were generally negatively correlated with country income, with higher country income corresponding to low rates. The trend for children aged 15–19 years in high-income countries was an exception; the YLLs per 100,000 population were higher than other country income categories before the early 2000s but then started to lower other categories; after 2013, it was lowest compared with the other three country income categories. In 2019, the YLLs per 100,000 population from RTI were 502.20 (95% UI: 402.39–650.27) among under-5 children, 337.82 (95% UI: 292.55–392.20) among children aged 5–14 years, and 806.69 (95% UI: 716.14–896.18) among children aged 15–19 years, respectively (Figs. 12.7, 12.8, and 12.9).

YLLs per 100,000 population due to RTI among under-5 children, 1990–2019. (Data source: GBD Compare, 2019)

YLLs per 100,000 population due to RTI among children aged 5–14 years, 1990–2019. (Data source: GBD Compare, 2019)

YLLs per 100,000 population due to RTI among children aged 15–19 years, 1990–2019. (Data source: GBD Compare, 2019)
12.2.3 Years Lived with Disability (YLDs)
During 1990–2019, YLDs per 100,000 population due to RTI demonstrated different trends in three age groups and four country income categories. The YLDs per 100,000 population were not strictly negatively correlated with country income, which probably reflected the effects of poor-quality non-fatal RTI data, varying prevention efforts and motorization levels. In 2019, the YLDs per 100,000 population due to RTI were 2.58 (95% UI: 1.64–3.88) among under-5 children, 19.57 (95% UI: 13.67–26.74) among children aged 5–14 years, and 60.59 (95% UI: 41.45–82.14) among children aged 15–19 years, respectively (Figs. 12.10, 12.11, and 12.12).

YLDs per 100,000 population due to RTI among under-5 children, 1990–2019. (Data source: GBD Compare, 2019)

YLDs per 100,000 population due to RTI among children aged 5–14 years, 1990–2019. (Data source: GBD Compare, 2019)

YLDs per 100,000 population due to RTI among children aged 15–19 years, 1990–2019. (Data source: GBD Compare, 2019)
12.2.4 Disability-Adjusted Life Years (DALYs)
During 1990–2019, DALYs per 100,000 population showed roughly consistent trends as shown for YLLs per 100,000 population in three age groups and four country income categories. In 2019, the DALYs per 100,000 population due to RTI was 504.78 (95% UI: 405.63–652.29) among under-5 children, 357.39 (95% UI: 312.38–410.73) among children aged 5–14 years, and 867.28 (95% UI: 775.85–960.48) among children aged 15–19 years, respectively. Low-income countries had the highest DALYs in all three age groups in 2019 (Figs. 12.13, 12.14, and 12.15).

DALYs per 100,000 population due to RTI among under-5 children, 1990–2019. (Data source: GBD Compare, 2019)

DALYs per 100,000 population due to RTI among children aged 5–14 years, 1990–2019. (Data source: GBD Compare, 2019)

DALYs per 100,000 population due to RTI among children aged 15–19 years, 1990–2019. (Data source: GBD Compare, 2019)
12.2.5 Economic Burden
Transport Research Laboratory [1], one of the most authoritative British institutions, reported that global road traffic injuries and deaths caused an economic loss of 518 billion dollars in 1997, which made up approximate 3% of GDP in most countries and had a great impact on global economic development. According to a study evaluating losses caused by road injuries in 21 countries, there is approximate 1% of GDP loss that could be attributed to road traffic injuries annually in developing countries, 1.5% loss in transition countries, and 2% in vehicle-popular countries. So far, no study evaluates economic burden caused by child road traffic crashes.
12.2.6 Age Group
Several studies [2,3,4] showed a higher risk of RTI in 5–9 age group as well as 15–19 age group, which was possibly associated with individual behaviors and transportation methods of children for two age groups. Road traffic injuries often happen as children riding in a car or crossing streets at the age group of 1–4 years; for the age group of 5–9 years, road traffic injuries frequently occur as children walking or crossing streets. 58.3% of students reported having suffered road injuries while riding, especially for those older than 16 years. Young children are usually accompanied by their parents on foot and in motor vehicles. As children grow up, they become more active and independent and have requirements for school, with correspondingly less parental supervision and more transportation options either by bicycle or motorcycle, which accordingly increases the risk of road injuries.
12.2.7 Region
Large child RTI morbidity and mortality variations exist across regions. At present, Africa has the highest child RTI mortality, followed by East Mediterranean. According to the WHO statistics [5], developing countries have higher rates of road traffic injuries, with 93% of fatalities occurring in low- and middle- income countries. Although Africa and East Mediterranean have the highest RTI mortality rates, two- thirds of global child road traffic deaths occur in Southeast Asia and West Pacific. Even in European Union countries where RTI mortality rates are comparatively low, 20% of total child deaths are caused by RTI.
12.2.8 Date and Time
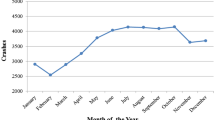
The occurring time of child RTI is closely related to pedestrian traffic density, children’s activities, and parental supervision. A study by Duan et al. [6] on the traffic safety status of child pedestrians in three Chinese cities reported that most child RTIs occur in summer holiday in Chinese cities. A study from Romania [7] reported a higher child RTI incidence in summer and linked higher rates with lack of supervision, range of activity area, and time during summer vacation.
Child RTIs mainly occur at around 8 a.m., 11–12 a.m., and 15–18 p.m., corresponding with school hours and peak traffic hours.
12.2.9 Transportation Method
The severity and type of child RTIs are related to the choice of transportation method. According to statistics of 70 countries by the WHO, approximately 33% of child fatalities were pedestrians, other 65% of whom were vehicle passengers, bicyclists, or motorcyclists.
Transportation method related to fatal child RTIs varies greatly with countries with different economic levels. In low- and middle-income countries, the most common transportation methods of fatal RTIs are walking, cycling, and motorcycling; pedestrians, bicyclists, and motorcyclists have to share the road, raising the risk of RTIs. Due to high motorization, low legal driving age, and high proportion of junior drivers, motor vehicle occupant mortality is much high in high-income countries, especially among junior drivers.
In 2019, pedestrians and motor vehicle passengers were the most common road users of global RTI mortality among under-5 children, accounting for 44.2% and 41.9% of fatal RTIs for boys and 48.3% and 41.6% of fatal RTIs for girls. Generally, under-5 RTI mortality for pedestrians and for motor vehicle occupants substantially decreased as the country income increased, fastest in high-income countries and slowest in low-income countries. In high-income countries, pedestrian, motor vehicle, motorcyclist, and cyclist deaths accounted for 43.5%, 50.0%, 2.8%, and 2.3% for boys and 35.0%, 59.0%, 2.7%, and 1.9% for girls; the numbers were 40.5%, 45.2%, 9.0%, and 4.3% for boys and 48.3%, 42.9%, 5.8%, and 1.8% for girls in low-income countries (Fig. 12.16).

Under-5 road traffic injury deaths per 100,000 population by sex, road user, and country income in 2019. (Data source: GBD Compare, 2019)
Among children aged 5–14 years old, pedestrian and motor vehicle road injuries remained as the two main contributors of child RTIs mortality, which explained 46.3% and 36.1% for boys and 48.5% and 39.5% for girls of child road traffic deaths. In high-income countries, motor vehicle road injuries made up 46.0% of fatal RTI deaths for boys and 59.1% of fatal RTI deaths for girls. In addition, the proportion of cycling deaths rose in this age group, especially for boys (Fig. 12.17).

Road traffic injury deaths per 100,000 population among children aged 5–14 years by sex, road user, and country income in 2019. (Data source: GBD Compare, 2019)
Among children aged 15–19 years old, riding in motor vehicles (excluding motorcycles), motorcycling and walking were the leading transportation methods of RTI deaths, accounting for 40.2%, 29.8%, and 24.6% of RTI deaths for boys and 50.8%, 14.6%, and 29.6% for girls, respectively.
In high-income countries, RTI mortality for motor vehicle occupants, motorcyclists, and pedestrians accounted for 64.7%, 18.9%, and 12.6% of fatal RTI deaths for boys and 78.5%, 6.6%, and 11.8% for girls, respectively. While in low-income countries, the proportions were 51.1%, 12.2%, and 32.5% for boys and 53.1%, 6.4%, and 36.7% for girls, respectively (Fig. 12.18).

Composition of deaths by transportation methods for children aged 15–19, categorized by World Bank income levels. (Data source: GBD Compare, 2019)
12.3 Influencing Factors of RTI
The occurring mechanisms of injury change with external cause of injury. Based on the four-layer socio-ecological model proposed by Dahlberg et al [8], the US CDC divides the risk factors of injury individual, interpersonal, communal, and social levels.
The Haddon matrix, developed by William Haddon [9], has been widely regarded as the most recognized model to explore the occurrence and prevention of a given injury event. The Haddon matrix is a grid with four columns and three rows, which describes four types of influencing factors (host, vehicle, physical environment, social environment) in three phases (pre-event, event, post-event). Table 12.2 illustrates an application of the Haddon matrix to child RTI. The influencing factors of child RTI are briefly introduced according to the stratification of host (human), vehicle (vector), physical environment, and social environment.
12.3.1 Host
12.3.1.1 Driver
People, vehicle, and road environment are three types of factors that cause traffic crashes. Epidemiological studies [10] show that around 95% of traffic crashes are attributed to human factors in China and 90% of which are caused by drivers. Research evidences show that accident-prone drivers and non-accident drivers differ in many aspects such as body shapes, physiological functions, night visions, dynamic visions, depth perceptions, attentions, complex reaction judgments, operational skills, hazard judgments, safety attitude, personality, aggressive personality, psychological disorders, etc. Driving a motor vehicle is a complex mission, which takes drivers a long time to improve their skills from basic level to proficient level. A study conducted in four countries (Australia, Japan, Malaysia, and Singapore) from 1986 to 1987 found that motorcyclists with provisional licenses had the highest risk of RTI, followed by motorcyclists with driving experience less than 1 year. Another study reported that motorists with riding experience less than 1 year had the highest risk of RTI.
12.3.1.2 Victim
As children are small in stature and thus have limited and imperceptible view of road traffic environment, they are more vulnerable to RTI. Immature cognitive development also affects children’s ability to make judgments and decisions involving the safety of different transportation methods. Children have not yet developed a concept of traffic safety before 5–7 years old and cannot accurately identify road traffic hazards until they are 11 years old. Individuals are not mature in terms of competencies like drawing inferences, making decision, and controlling impulses before they are 20 years, making children tend to make incorrect judgments about traffic environment and have dangerous behaviors.
As children get older, especially when they enter puberty, their needs for independence and mobility increase. Driven by adolescent rebellion, impulsiveness, curiosity, and pursuit of excitement, children start to actively attempt some dangerous behaviors, which is more common among boys than girls; this is a major reason for the comparatively high road traffic injury risk among boys. Furthermore, children are susceptible to peer influence and attempting dangerous things encouraged by peers or performing dangerous behaviors to fill up self-vanity during puberty.
12.3.1.3 Seat Belt
Current research evidences show that the use of seat belt can reduce the risk of injury by 40–50%, serious injury by 43–65%, and fatalities by 40–60% for motor vehicle drivers and passengers. Because of differences in legislation and law enforcement, the use of seat belt in motor vehicles varies across countries. A research in Kenya [11] found that among drivers and passengers using seat belts, only 1% were injured in a crash. Another research in Argentina [12] reported that only 26% of drivers and front-seat passengers used seat belts in the city of Buenos Aires and 58% on national highways.
In the United States [13], the proportion of front passengers using seat belts rose from 58% in 1994 to 75% in 2002. A study [14] conducted in Guangzhou and Nanning of China found that the rate of seat belt use in the two cities was 72.2% and 71.9%, respectively.
12.3.1.4 Child Safety Seat
Child safety seats have an important role in preventing child RTI. It was reported [15] that proper installation and use of child safety seats can reduce the risk of death in crashes by about 70% for infants and 47–54% for children aged 1–4 years, respectively. Different types of safety seats should be considered for children with different ages. For infants aged 0–15 months and weighing less than 13 kg, rear-facing child safety seats provide better protection. The use of forward-facing child safety seats can reduce injuries by 34% and severe injuries by 60%, while rear-facing child safety seats can reduce injuries by 76% and severe injuries by 90%. Child safety seats are frequently utilized in developed countries, with 90% in Australia and 86% in the United States. However, incorrect installation and improper use of safety seats are common. Previous studies reported that incorrect use of safety seats ranged from 44% to 81%. A study conducted by the National Highway Traffic Safety Administration (NHTSA) [16] found that 72.6% of 3442 cases did not use safety seats correctly, and the most improper use of which were wearing adult seat belts and not fastening the belts on child safety seats. A study conducted among parents in Shanghai [17] showed that less than 30% of parents purchased safety seats for their children. The actual use of child safety seats was even lower due to children crying and the trouble of installation and disassembly.
12.3.1.5 Intoxicated Driving
Intoxicated driving raises the likelihood of both crashes and fatal or severe non-fatal injuries. A survey conducted in EU countries [18] showed that 1–3% of drivers reported having ever experienced an intoxicated driving. A study in low- and middle-income countries found that alcohol was detected in the blood of 33–69% of drivers killed in crashes and 8–29% of those injured. A study in New Delhi, India [19], reported that one-third of two-wheeled motorcyclists who were brought to hospital for treatment answered having drunk before driving. A similar risk exists in pedestrians consuming too much alcohol. A study in South Africa [20] revealed that over 61% of pedestrian dying in crashes had alcohol consumption. A recent British study [21] reported that 48% of pedestrians killed in car crashes had alcohol consumption.
12.3.1.6 Safety Helmet
Head trauma is a leading cause of death for two-wheeler motorcyclists and riders, explaining 75% of all-cause mortality in Europe and 55–88% in Malaysia. A study [22] by Kulanthayan et al. found that drivers not wearing safety helmets were three times more likely to suffer a head injury than those wearing safety helmets. Servadei [23] reported that safety helmets reduced fatal and severe head injuries by 20–45%. However, a US study found that nearly half of drivers and two-wheeled motorcycle riders using substandard safety helmets were at higher risk to suffer a head trauma than those not using safety helmets.
If children on bicycles wear safety helmets, the probability of experiencing a head injury in a crash would reduce by 63%, as well as loss of consciousness reduces by 86%. So far, legislative request that cyclists should wear safety helmets have been introduced in many countries like Australia, New Zealand, Sweden, and the United States.
12.3.1.7 Distracted Driving
Distracted driving behaviors involve all behaviors that interfere with driver’s attention while driving, and endanger safety of drivers, passengers, and others. Common distracted driving behaviors include answering the phone, making a phone call, sending and receiving a text message, eating, drinking, talking to passengers, making up, looking at maps, using navigation, watching videos, and using a radio, CD, or MP3 player, using wireless communication devices to make and receive phone calls and text messages. Recent studies show that drivers’ reaction time increases from 0.5 to 1.5 seconds while using mobile phone, making drivers difficult to keep in the right lane, maintain right speed, and make judgment for a safe distance. Drivers who use a mobile phone while driving are at four-time risk to suffer a crash than those not using mobile phone.
12.3.2 Vehicle
Vehicle design has a vital impact on RTI. Vehicle design defects lead to around 3–5% of traffic crashes. The design, testing, and maintenance of motor vehicles are closely correlated with the risk of RTIs. A British study reported that comprehensive improvements of vehicles, roads, legislation, and enforcement can reduce fatal or severe road traffic crashes by 33%, while the improvement of vehicle could reduce the number by 15.4%. Another study conducted in New Zealand drew a similar conclusion. It could reduce the hazards to pedestrians and cyclists if the front end of a vehicle is improved. The European Committee for the Promotion of Vehicle Safety [24] has designed performance tests for the front end of motor vehicles; the United States and the European Union has required to vehicles with forward crash prevention systems, and about 40 countries had agreed on the draft United Nations Regulation for cars with Advanced Emergency Braking Systems (AEBS) avoiding forward collision in 2019. Crashworthiness and immobilization devices need to be considered in the design of motor vehicles if we want to improve devices protecting passengers. In general, high-income countries adopt new test models of minibuses to ensure that the passenger compartment retains its shape and structure and the fixture devices function in a collision. Most high-income countries mandate that seat belts in cars and light trucks reach certain technical standards. In low- and middle-income countries, more than half of motor vehicles may not be equipped with reliable seat belts.
12.3.3 Natural Environment
About 2.9% of road traffic injuries can be attributed to road factors, and approximately 24.3% of road traffic injuries in China are associated with roads. Unsafe road environments increase the risk of child RTIs. Recently, the number of motor vehicles has increased rapidly in many countries and regions, but road construction and management lags in these countries. Lack of safe and efficient public transportation system not only causes road congestion but also raises the likelihood of RTIs. In addition, fast-traveling or slow-traveling motor vehicles and unreasonable road design are important risk factors of RTIs.
12.3.4 Socioeconomic Environment
12.3.4.1 Incidence of Traffic Crashes Among Children
Socioeconomic status is associated with the incidence of traffic crashes among children. The flourishing commercial economic activities increase people’s travels and therefore raise the chances of road traffic crashes.
The World Bank analyzed the data of 88 countries between 1963 and 1999 and found that the mortality of RTIs rose sharply with the increase of gross domestic product (GNP) per capita; when the GNP per capita reached 1180 US dollars, RTI mortality began to decline as the GNP per capita grew.
12.3.4.2 Emergency Care
Pre-hospital emergency care is closely related to the treatment outcome of RTI patients. A review of European countries concluded that about 50% of road traffic deaths occurred within minutes of the collision, some of them died on the spot of car crashes and some died on route to hospital; about 15% of deaths occurred within 4 hours of crashes and died in hospital; and 35% of deaths occurred 4 hours later than crashes. In low- and middle-income countries, the majority of RTI deaths occur on the road to the hospital. Lack or low-level pre-hospital emergency care significantly delays the best time of treatment.
12.3.4.3 Trauma Treatment
Trauma care has developed rapidly recently. Unfortunately, many people in low- and middle-income countries still cannot access public health or individual commercial insurance in hospitals due to a large shortage of qualified surgeons. A study in Ghana reported that, of people who experience severe injuries in car crashes, only 38% in rural areas and 60% in urban areas were admitted to hospitals for treatment. Traumatic brain injury is the leading cause of RTI deaths. Because of lack of hospital admissions and qualified physicians, children who are seriously injured in road traffic crashes cannot receive timely treatment and probably die or have lifetime disabilities.
12.4 Interventions
12.4.1 Theories of Injury Intervention
The general intervention theories are also applicable to child road traffic injury prevention. Here, we briefly describe Haddon’s ten strategies, the “5Es” intervention theory, and active and passive intervention strategies.
12.4.1.1 Haddon’s Ten Strategies
Haddon proposed ten prevention strategies based on the Haddon matrix, including:
-
① Prevent the creation of the hazard in the first place, such as stopping the manufacture of some toxic substances.
-
② Reduce the amount of energy contained in the hazard, such as car speed limits.
-
③ Prevent or reduce the release of the hazard, such as the bathroom floor should not be too slippery.
-
④ Modify the rate or spatial distribution of the hazard from its source, such as the use of seat belts.
-
⑤ Separate people in time or space from the hazard and its release, such as bicycle and pedestrian pathways.
-
⑥ Separate people from the hazard by interposing a material barrier, such as the use of insulation to separate the cable and pedestrians.
-
⑦ Modify the relevant basic qualities of the hazard, such as eliminating the angles of objects in the kindergarten.
-
⑧ Make the person more resistant to damage.
-
⑨ Counter the damage already done by the hazard, such as setting up alarm telephone along roadside.
-
⑩ Stabilize, repair, and rehabilitate the injured person.
The ten strategies apply to the design of injury prevention interventions of all injury causes at all age groups.
12.4.1.2 “5Es” Intervention Theory
Interventions can be divided into five categories by their characteristics (5Es are the abbreviation of the initials of five types of interventions), including:
-
① Education strategy: to enhance people’s awareness of the risk of injury through safety education and then reduce the dangerous behaviors
-
② Environmental modification strategy: to reduce the likelihood of injury to individuals by reducing environmental risk factors
-
③ Engineering strategy: to produce safer products through design and innovation
-
④ Enforcement strategy: to establish the laws and enforce the laws strictly to maintain certain behaviors and norms and also prohibit dangerous behaviors that increase the risk of injuries
-
⑤ Evaluation strategy: to evaluate the available interventions to prevent and control injuries and to determine the most effective interventions, programs, and policies
12.4.1.3 Active and Passive Intervention Strategies
Injury prevention strategies [25] can be divided into active interventions and passive interventions according to the behaviors that the host (individual) takes. Active interventions refer to intentional behavior changes through the choice of safety equipment or the adoption of safer behaviors to avoid injury, such as wearing a helmet correctly when riding a bicycle. Passive interventions refer to equipping the external environment with safety facilities to avoid injury or reduce the severity of injury when individuals are exposed to external intolerable energy such as installing airbags in a car, which will automatically open in the event of a crash.
12.4.2 Interventions
In 2010, the United Nations launched the Global Road Safety 2011–2020 Action Plan. The WHO released the Global Status Report on Road Safety 2009 in the same year and regularly updates the report every 2 years since then. This report systematically assesses the legislation and enforcement of proven RTI interventions of the participating countries. In 2013, the WHO proposed ten strategies to prevent road traffic injury for children, including controlling speed, reducing drink and driving, using helmets for bicyclists and motorcyclists, improving children’s ability to see and be seen, restraining children in vehicles, enhancing road infrastructure, adapting vehicle design, reducing risks for young drivers, providing appropriate care for injured children, and supervising children around roads.
Next, we present a brief summary of main interventions for child RTI based on the recent published literature.
12.4.2.1 Legislation
Legislation is a mandatory intervention. Legislation has the strongest public warning and enforcement power. Currently, the WHO recommends five legislative interventions to all WHO member states, including managing speeding, reducing drink-driving, increasing motorcycle helmet use, increasing seat belt use, and increasing child restraint use.
Between 2014 and 2017, 123 countries had laws meeting the best practice of at least one of five behavioral risk factors. However, only France, Hungary, Italy, Luxembourg, and Sweden had laws that meet the best practice of all five key risk factors (Fig. 12.19).

Number of people covered by laws meeting the best practice, 2017 vs. 2014. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008.)
12.4.2.1.1 Speed Limits
A research by the WHO showed that high-speed driving accounted for about 1/3 of road traffic crashes in developed countries and up to 1/2 in developing countries. Driving at high speeds poses a significant threat to child road safety, especially on roads around schools, residential, and commercial areas. One study reported that a 5% reduction in average driving speed can reduce 30% of fatal crashes. Currently, the interventions for preventing high-speed driving include four categories: ① setting appropriate driving speeds according to use and quality of roads; ② setting maximum allowable speeds on roads with high occurring frequency of children (30 km/h is now recommended); ③ strengthening the control of road speed limits by installing automatic speed camera; and ④ separating pedestrians from speeding vehicles through establishing or improving urban sidewalks, street crossings, pedestrian underpasses, safety islands, and curb medians in road sections when needed.
-
(a)
Speed limits supplemented by installation of pedestrian countdown signals: New York City in the United States installed pedestrian countdown signals at 1500 intersections throughout the city, set a maximum speed of 32 km/h for living areas and 75 school speed limit zones, enforced speed limits on major traffic arteries, and used mass media to inform the public about road safety and engage the public in road safety activities. Such efforts were followed by an around 25–51% decline in road traffic crashes involving pedestrians in New York City.
-
(b)
Speed limits supplemented by pedestrian separation initiatives: London City in the United Kingdom has launched a “30 km/h” speed limit action in school zones and residential areas for a long time. The government has also built pedestrian segregation in the speed limit sections, such as street crossings, pedestrian underpasses, and safety islands. As a result of the comprehensive speed limit program, traffic safety has improved significantly among children aged 0–15 years old. Pedestrian fatality are reduced by 46% and bicyclist fatality reduced by 28% between 1987 and 2006.
-
(c)
The use of red light camera to enforce speed limits: An analysis that compared crash data from 253 intersections in Flanders, Belgium, between 2002 and 2007 before and after the introduction of red light cameras to assist with speed limits, showed a 14% decrease in major road crashes, despite a 44% increase in rear-end crashes. In January 2011, a study that assessed the effectiveness of installing red light camera at high-crash intersections in Miami-Dade County, Florida, showed that the use of cameras reduced red light running crashes by 14% and injuries by 12% over 2 years, despite the fact that rear-end crashes increased 40% in the first year and rose 50% in 2 years.
Setting speed limits is an effective measure to reduce road traffic injuries. Although many countries have established national speed limit laws, few meet the best practice criteria for speed limit laws. As shown in Fig. 12.20, 95 countries set up speed limits equal to or under 50 km/h in urban areas, but only 84 empower local authorities to modify speed limits in local laws. 51% of countries that satisfy the three best practice laws are from high-income countries, 36% from middle-income countries, and 13% from low-income countries.

Countries with speed laws meeting the best practice in 2017. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008)
12.4.2.1.2 Restricting Drink-Driving
Laws and regulations for drink-driving mainly emphasize to raise the legal drinking age and set a maximum limit of blood alcohol concentration for drivers.
-
(a)
Increasing the legal drinking age: The United States has an extremely strict limit for teenage drinking (current legal drinking age: 21 years old). Many states in the United States have set age limits for the purchasers who buy alcoholic beverages in supermarkets and other stores. Although China has not specified the rule, its law on the Protection of Minors of the People’s Republic of China (article 11) requests that adult guardians should forbid people younger than 18 years old to drink alcohol beverages.
-
(b)
Setting a limit of blood alcohol concentration (BAC) for drivers: Implementation of a BAC limit for motor vehicle drivers can reduce a number of road traffic fatalities related to drunk driving. The usual threshold of BAC is 20 mg/100 ml for drivers. Studies indicated that young drivers with a BAC of 50 mg/100 ml are twice as likely to have a road traffic crash than experienced drivers. The best practice is to set a lower BAC (20 mg/100 ml or lower) for young and novice drivers, which can dramatically reduce the number of alcohol-related traffic accidents.
A BAC of 50 mg/100 ml is acceptable. 174 countries have laws on drink-driving. Among these, 136 countries set up BAC limits; but only 45 countries both set specific limits for the general population (0.05 g/dl) and for young and novice drivers (0.02 g/dl). As shown in Fig. 12.21, 56% of countries that satisfy the three best practice laws are from high-income countries, 42% from middle-income countries, and 2% from low-income countries.

Countries with drink-driving laws meeting the best practice in 2017. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008)
In addition, there are other interventions for drink-driving, but the effectiveness of these interventions is controversial, warranting further research to generate more solid evidence.
-
(a)
Setting alcohol testing checkpoints: A study in the United States reported that frequent checkpoints with high publicity and visibility reduced road traffic injury crashes by about 18–24%. Alcohol testing checkpoints can easily detect drunk drivers and have a strong warning effect.
-
(b)
Development and promotion the fitment of alcohol-locks: The American academic community has discussed the installation of alcohol concentration detection and lockout devices on motor vehicles since the 1960s. It contains an alcohol meter. Once the driver’s blood alcohol level is detected to be high, the device will automatically lock the engine of motor vehicle. In 2009, Toyota Motor Corporation in Japan, together with its affiliated truck manufacturer Hino Motors, announced that they were designing an anti-drunk driving car with an alcohol interlock system in the car. The system includes a miniature alcohol meter and a digital camera, which are used to detect the alcohol level and take a picture of the driver’s face to determine the identity. When the test result is positive (namely, the driver’s blood alcohol concentration exceeds the law limit), the system will give a warning or lock the engine of car. Alcohol interlock systems have improved a lot recently. Several engineering studies in 2013 indicated that the conception of anti-drunk driving lockout system can be realized through integrating multiple technologies such as alcohol sensors, microcontrollers, and voice transmission.
-
(c)
Mass media campaigns: Mass media is believed to be helpful for establishing correct social norms against drunk driving. But implementation details must be considered.
-
(d)
School safety education: School-based alcohol education programs were found to reduce drunk driving. Further studies showed that the success of school-based intervention programs is related to the length of time the intervention program implemented, the content of the program, and the extent of interaction with students.
12.4.2.1.3 Wearing Safety Helmets
Head and neck injuries are the leading cause of death and disability for motorcycle crashes. Substantial evidence suggests that the use of helmets effectively reduce motorcyclist injuries and fatalities. In motorcycle crashes, the rate of head injury for motorcyclists not wearing helmets is 2.19 times higher than those wearing helmets.
In late 2007, Vietnam had passed a law requesting all motorcyclists and passengers (including children) to wear a helmet. Following the law, the rate of wearing safety helmets quickly exceeded 90%, resulting in a dramatic decrease in head injury and fatality rates among motorcyclists and passengers. However, the law does not authorize traffic polices to penalize children aged 14 and under who did not wear safety helmets and their parents. Consequently, the rate of wearing helmets remained less than 40% among children.
In April 2010, the government amended the law to require children above the age of 6 to wear safety helmets when riding, which was a responsibility for their parents. After the regulation was implemented, the rate of wearing helmets in Vietnamese children rose to 56% by 2013.
Currently, the enforcement of helmet-wearing laws is generally weak. 167 countries have mandatory helmet laws for motorcyclists, but only 49 countries meet the overall best practice criteria. As shown in Fig. 12.22, 41% of countries that satisfy the overall best practice laws are from high-income countries, 53% from middle-income countries, and 6% from low-income countries.

Countries with helmet laws meeting the best practice in 2017. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008)
12.4.2.1.4 Using Seat Belts
Substantial studies have proved that wearing seat belts is effective in protecting motor vehicle drivers and passengers of all age groups. It is estimated that the use of seat belt can reduce road traffic deaths and serious injuries by 60% in the United States, avoiding 18,000 deaths and an economic loss of more than 17 billion dollars. Rutledge et al. reported that the fatality rate of motor vehicle drivers and passengers was 7% for those not wearing seat belts and 3% for those wearing seat belts, and the head injury rate was 50.0% and 32.9% for the two occasions, respectively.
Of 161 countries with national seat belt laws in 2017, 105 countries have laws that met the overall best practice of mandating use of seat belts to all occupants, 41% of countries that are from high-income countries, 52% from middle-income countries, and 7% from low-income countries (Fig. 12.23).

Countries with seat belt laws meeting best practice in 2017. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008)
12.4.2.1.5 Using of Child Restraints
Child car seats are effective in preventing non-fatal injuries and fatalities among child passengers. If correctly installed and used, child car seats can effectively protect children in vehicles and reduce the chance of hospitalization among under-5 children by 69%, the risk of road traffic deaths by 70%, and deaths of under-5 children by 54%. Compared with the use of seat belts alone, together using seat belts and child car seats can lead to a 59% reduction in the road traffic injury for children aged 4–7 years.
84 countries have national child restraint laws in 2017. Among these 33 countries, 9% of the world’s population have laws that meet the overall best practice criteria, 85% of countries that are from high-income countries and 15% from middle-income countries (Fig. 12.24).

Countries with child restraint laws meeting the best practice in 2017. (Data source: Global status report on road safety 2018. Geneva: World Health Organization, 2008)
Research evidence showed that the use of child restraints was significantly associated with parental perception on its importance. In many developed countries, parents pay much more attention to the safety of children, with child safety seat use rate as high as 90%. Since July 1, 2012, the government of China implements a national standard for child safety seats (GB27887-2011); but the rate of using child car seats is still very low.
A study in Beijing [26] evaluated the effect of comprehensive interventions (including measures such as group discussions, showing child car safety promotional films, instruction and live demonstration of child booster seats, and free distribution of child car seats). The results found that 84.5% of children by car had never used a booster seat before the intervention, and 98% of children almost every day used the seat after 6 weeks, and 97% of parents indicated that they intended to continue using child car seats for the next 6 months. The results of this study indicate that appropriate measures can increase the proportion of correctly using child car seats in China.
12.4.2.2 Increasing the Visibility of Children Pedestrians
A study by Wells et al. [27] showed that wearing retro-reflective and fluorescent clothes and white or light-colored helmets and using headlights are simple and practical ways to effectively reduce road traffic crashes and deaths and non-fatal injuries in motor vehicle crashes.
12.4.2.3 Choosing Suitable Car Seats for Children
Research evidence shows that the locations with the least risk of head injury to children in motor vehicles are braking position and crash test dummy position, while those with the greatest risk are innermost and outermost positions; the locations with the lowest risk of chest injury to children are medial position and crash test dummy position, while those with the highest risk are lateral position and braking position. Therefore, it is best for children to take the rear seats. Forbidding children sitting in the forward passenger seat can reduce the likelihood and severity of injuries to children during motor vehicle collisions.
12.4.2.4 School Safety Education
Road traffic safety education mainly focuses on primary and secondary schools in China. In 1986, the Notice on Reforming the Road Traffic Management System issued by the State Council of China clearly listed traffic safety publicity and education as a priority of all traffic management work of public security agencies. In 1996, the former State Education Commission, together with six ministries and commission issued a notice to establish the Safety Education Day for Primary and Secondary Schools. However, the effectiveness of school-based safety education model in reducing child RTIs remains unexamined by rigorous studies.
12.4.2.5 Graduated Driver Licensing
Graduated Driver Licensing (GDL) program involves three-level training according to the driver’s age and driving experience:
-
(a)
To obtain a learner’s driver’s license (G7, basic level), requesting that the applicants shall be above 14 years old, pass a written test and a vision test, have a valid identity document, and get parental consent if they are younger than 18 years old. If the applicants want to drive, they must be supervised by an adult driver with full license and cannot drive at midnight and early morning.
-
(b)
To obtain an intermediate license (G5, trainee level), requesting that the applicants shall be above 16 years old and have held a G7 license at least 1 year. The applicants can drive alone but are ineligible to serve as an accompanying driver of a learner with a G7 license.
-
(c)
To get a full or unrestricted license (G5, can instruct G7 holders to drive). The applicants must have held a junior G5 for 2 years and have no infraction record in the last year and pass an advanced road test.
In 2011, Russell et al. summarized 34 studies that evaluated the effects of 21 GDL cases and concluded that the implementation of GDL program resulted in a reduction of 8% to 27% in crash rate and of 2% to 46% in injury rate in the first year after 16-year-old teen drivers received their licenses, suggesting that GDL can significantly reduce road traffic crashes caused by lack of skills and experience of drivers.
12.4.2.6 Using Airbags with Caution
It has been proved that airbags pose a threat to child passengers in motor vehicles. Between January 1990 and January 2005, 157 children under the age of 13 were killed by the popped airbag in the non-fatal collision of low-speed vehicles in the United States. A study by the National Highway Traffic Safety Administration, with 3790 teenagers aged from 1 month to 18 years who seated in the right front seat while driving, found that children under 15 years old faced a great risk of injury when the airbag popped up. The strong impact of airbag popping up probably causes a serious injury or even lethal outcome to the children.
12.4.2.7 Improving Train for Young Drivers
Young drivers have been found to be a major cause of teenage car crashes. The results of many studies showed that underage drivers who get driving license prematurely upon the driver training are apt to cause road traffic crashes when driving.
12.4.2.8 Avoiding Distracted Driving
A review of 19 articles published between 2000 and 2013 examined the relationship between the use of a mobile phone while driving and the incidence of motor vehicle traffic crashes; the results suggested that drivers should take measures to avoid distractions (including using their mobile phones to access social media sites such as Facebook and Twitter), especially for young and inexperienced drivers. Texting and receiving messages during driving increase the risk of fatal road traffic crashes.
12.5 Conclusion
Currently, injury academic community in China and abroad has developed many effective interventions for child road traffic injury prevention. For most countries, the major challenge is how to strictly implement these interventions and monitor the progress of road traffic injury prevention interventions with reliable and valid data. Of course, necessary modifications or tailoring are needed when low- and middle-income countries like China translate the interventions proven in high-income countries. Each individual government should open child road traffic injury data to the researchers and encourage them to use the data to improve road traffic injury prevention. High-quality researches should be supported to assess the current status of child road traffic injury, identify new problems, and develop targeted interventions. Low- and middle-income countries may consider combining proven interventions with their national health initiatives to popularize these interventions.
References
Jacobs G, Thomas AA, Astrop A. Estimating global road fatalities. 1st ed. Crowthorne: Transport Research Laboratory; 2000.
Chen RH, Zhang PB, Deng JY. An epidemiological survey of car accident injury deaths in children aged 0-14 years in Jiangsu Province. Chin J Pediatr. 1999;37(11):661–3.
Wang XX, He GS, Hao AH, et al. Epidemiological analysis of road traffic injuries among primary and secondary school students in Gansu Province. Disease Surveillance. 2004;19(9):353–5.
Chi GB, Wang SB. Analysis of long-term trends in road traffic injuries and the factors influencing them in the towel country. Chin J Epidemiol. 2007;28(2):148–53.
World Health Organization. Global burden of disease: 2004 update. Geneva: World Health Organization; 2008.
Duan LL, Sun YM, Deng X, et al. A retrospective study of road traffic safety among pedestrians in three cities in China. China Health Education. 2007;23(5):330–58.
Duma OO. Profile of service provided by an accident and emergency care department in connection with road traffic injuries involving children, 2003–2005. Cent Eur J Public Health. 2007;15(4):154–7.
Dahlberg LL, Krug EG. Violence-a global public health problem. Geneva: world health. Organization. 2002;1:56.
Haddon W Jr. A logical framework for categorizing highway safety phenomena and activity. J Trauma. 1972;12(3):193–207.
Jin HQ. Review and outlook of epidemiological studies on car accidents in China. Chin J Epidemiol. 2004;25(3):190–2.
Evans T, Whitehead M, Bhuiya A, et al. Challenging inequities: from ethics to action. 1st ed. Oxford: Oxford University Press; 2001.
Silveira AJ. Seat belt use in Argentina: a 10-year struggle. Traffic Inj Prev. 2003;4:173–5.
Glassbrenner D. Safety belt and helmet use in 2002: overall results. Washington DC: Department of Transport; 2002.
Li GL, Li LP, Mark S, Rebecca I, et al. A survey on the wearing status of seat belts in cars in Guangzhou and Nanning. Chin J Epidemiol. 2006;27(8):698–701.
Zaza S, Sleet DA, Thompson RS, et al. Reviews of evidence regarding interventions to increase use of child safety seats. Am J Prev Med. 2001;21(4S):31–7.
Lawrence ED, Kathy HL, Alan WB. Misuse of child restraints: results of a workshop to review field data results. Washington DC: NHTSA; 2005.
Wu XY, Yang L, Dong LP, et al. Analysis of the current situation of in-vehicle injuries among child occupants in China. J Jiamusi Univ. 2013;31(5):676–9.
European Transport Safety Council. Reducing injuries from alcohol impairment. Brussels: European Transport Safety Council; 1995.
Mishra BK, Banerji AK, Mohan D. Two-wheeler injuries in Delhi, India: a study of crash victims hospitalized in a neuro-surgery ward. Accid Anal Prev. 1984;16:407–16.
Peden M, Knottenbelt JD, van der Spuy J, et al. Injured pedestrians in Cape Town: the role of alcohol. S Afr Med J. 1996;16:1103–005.
Keigan M, Tunbridge R. The incidence of alcohol in fatally injured adult pedestrians. TRL REPORT TRL 579, 2003.
Kulanthayan S, Umar RS, Hariza HA, et al. Compliance of proper safety helmet usage in motorcyclists. Med J Malays. 2000;55:40–4.
Servadei F, Begliomini C, Gardini E, et al. Effect of Italy’s motorcycle helmet law on traumatic brain injuries. Inj Prev. 2003;9:257–60.
European Road Safety Action Programme. Halving the number of road accident victims in the European Union by 2010: a shared responsibility. Brussels: Commission of the European Communities; 2003.
Liu XX, Si DM, Shi DH. Factors of childhood injury and its intervention control. Chin J Prev Med. 2000;34(4):250–2.
Cao RX, Zhang R. A study on parents’ perceptions of car seats and interventions in Beijing. China School Health. 2015;05:548–9.
Wells S, Mullin B, Norton R, et al. Motorcycle rider conspicuity and crash related injury: case-control study. BMJ. 2004 Apr 10;328(7444):857.
Acknowledgments
Author acknowledges Lei Yang and YouYou Wu from “Department of Epidemiology and Health Statistics, Xiangya School of Public Health, Central South University, Changsha, China” for their draft translating the chapter to English.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 People's Medical Publishing House, PR of China
About this chapter

Cite this chapter
Hu, G. (2022). Progress in Epidemiology of Child Road Traffic Injury. In: Ye, DQ. (eds) Progress in China Epidemiology. Springer, Singapore. https://doi.org/10.1007/978-981-19-2199-5_12
Download citation
DOI: https://doi.org/10.1007/978-981-19-2199-5_12
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-2198-8
Online ISBN: 978-981-19-2199-5
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)