
Abstract
There is no doubt that food components can interact with mammal’s biological functions. Nutrients or nutritional metabolism in the body can influence the cytochrome P450, leading to biochemical changes. The capacity of converting toxicants of the body is also vulnerable to food deprivation. Furthermore, it should not be ignored that dietary fat may have influence on the synthesis and induction of the constitutive mixed-function oxidases. Several examples are given to explore the expanding field that involves the effects of the constituents in plant food on the metabolic process of organisms. Xenobiotics can be metabolized or biotransformed in all major organisms for their normal functioning, and biotransformation can dominate toxicokinetics. A multitude of dietary factors can affect the metabolism of xenobiotics, including nutritional status of the subject. Here, we give a brief introduction of metabolism and toxicity of toxicants influenced by macronutrients and micronutrients.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1.1 Introduction
A multitude of substances are metabolized by our body every day. The substances are divided into endogenous and exogenous ones. Endogenous substances include all kinds of bioactive materials, such as hormones and neurotransmitters. Exogenous substances are the xenobiotics that the human body is unavoidably composed to daily life, such as drugs, toxicants, food additives, environmental chemicals, and intestinal spoilage products. These materials may be interacted with nutrients, positively or negatively. Therefore, the interaction between nutrients and xenobiotics will be deeply interpreted in this chapter.
1.2 Nutrients in Detoxification and Metabolic System for Xenobiotics
Xenobiotics are any chemical compounds that are found in a living organism, but not generated in organisms. Several chemicals that occur naturally might be recognized as xenobiotics when present at excessive levels. The “xeno” in “xenobiotics” derives from the Greek word xenos and has the meaning of guest, stranger, or foreigner. It has been recognized that proper nutrition might build the body as a better fortress against invasion of xenobiotics. However, the effects of certain nutrients on metabolism of xenobiotics might be positive or negative. And understanding the basic metabolism system would help understand the potential mechanisms of the interaction.
1.3 The Basic Chemical Detoxification and Metabolism System
Metabolism refers to the processes of compounds’ decomposition in an organism, mainly through the role of enzymes, to produce energy and synthesize the components of biological molecules needed to maintain the life activities [1]. The process of xenobiotic metabolism is often expressed as the detoxification. The description, however, means that metabolic transformations is associated with decreased toxicity. Therefore, the expression is incorrect to some extent. In fact, metabolism might involve the production of new toxins or enhance the toxicity of parent compounds, and therefore, it is not always a detoxification process. This claim has been verified in some chemical carcinogens, organophosphates, and necrosis-inducing compounds. Since the same metabolic pathways can enhance or attenuate the toxicity of different xenobiotics, it is generally suggested that all these reactions involving structure transforming of the parent compound be referred to as biotransformation.
Nutrients and foreign compounds may share the same pathways in living organisms when considering metabolism and detoxification processes. The gastrointestinal tract (GI) is essentially the place where food, water, and related pollutants are all ingested [2]. However, our body may also be exposed to environmental and occupational toxicants via the respiratory tract and skin. Generally speaking, the skin, lungs, or gastrointestinal tract tend to absorb the compounds with strong lipophilicity [3]. Then, these lipophilic chemicals may accumulate in the body to toxic levels by continuous or even intermittent exposure unless effective elimination methods exist.
The possibility of biotransformation of xenobiotic compounds in vivo depends on the chemical properties [4]. It is difficult to enter the human body for highly polar compounds, such as relatively ionizable carboxylic acids; even though they enter, they are usually discharged rapidly. So these compounds are not available or can only be metabolized by enzymes in a very short time. On the contrary, volatile compounds such as dichloromethane or diethyl ether are excreted from the lungs so quickly that enzymatic metabolism can appear with little possibility.
Excretability is a vital feature for the toxicity of foreign compounds. The kidneys of vertebrates can induce electrolyte ionization better than nonelectrolytes. For example, the more completely organic acids are ionized at physiological pH, the more easily they are excreted by the kidney.
An extensive range of physique tissues and organs can metabolize the foreign compounds. As section of the body’s protection in opposition to the entry of xenobiotics, xenobiotic metabolism mainly occurs in the sites associated with the entry into the body. In this regard, the liver is especially important for xenobiotic compound metabolism, although the skin, lungs, and intestine wall are also the sites through which xenobiotic species enter the body [5,6,7]. The liver is rich in the enzymes or enzyme systems that catalyze the xenobiotic biotransformation. In addition, the liver is also the first organ for the substances to enter the systemic circulation from the gastroenterol tract. Therefore, these materials can be easily extracted from the blood and chemically modified by the liver before their storage or distribution.
The metabolism of xenobiotics generally takes place in the microsomal fraction (smooth endoplasmic reticulum) of hepatocytes [8]. Non-microsomal reactions can be visible in some biotransformations such as the redox reactions related to alcohols, aldehydes, and ketones. Some activities that promote the metabolism of xenogeneic organisms are limited for the overall biotransformation, although virtually every tissue of the human body exhibits such activities. However, the biotransformation of a chemical outside a hepatic tissue can have a vital toxicological significance for the specific tissue [4].
1.3.1 Biotransformation Reactions
The process of biotransformation is mediated by enzymes, resulting either in changes of parent molecules or in the formation of compounds associated with the combinations of normally occurring agents and the parent molecules. Several predominant enzyme systems are usually related to these reactions in the liver [9]. These enzymes can be roughly divided into phase I and phase II enzymes [10]. The phase I enzymes generally regulate the oxidation, reduction, or hydrolysis and mediate reactive, polar functional groups onto lipophilic toxicant molecules, resulting in the formation of more water-soluble products than the parent xenobiotic species. However, the water solubility and polarity of some substances do not change significantly after the phase I reactions, and substances or groups with stronger polarity need to be combined to further increase their polarity and promote excretion. These conjugation reactions belong to the phase II enzymatic reactions. The phase II reactions thus produce a conjugation product, which is combined between a functional group either on the parent compound or on the introducing group from a phase I reaction and easily excreted from the body (Fig. 1.1).

Two-phase scheme of the biotransformation
It is noteworthy that the biotransformation of many substances is complex. Not all xenobiotics go through both phase I and II reactions. Some products from phase I reaction can be directly excreted from the body. Also, a compound with a suitable conjugated functional group can also directly enter phase II reaction without undergoing phase I backward reaction.
1.3.2 Phase I Enzymes
The phase I enzymes mainly lie in the endoplasmic reticulum, which is a related channel network in the cytoplasm of most cells. The filamentous structure can be observed under the electron microscope, which can be divided into smooth-surface filaments and rough-surface filaments. The tubular endoplasmic reticulum can be broken following that the liver is homogenized into hepatocytes. Microvesicles, that is, microsomes, are formed through the seal of the membrane fragments. Microsomes, the main location of the phase I enzymes, are precipitated from smooth reticular endothelial cells. These enzymes are bound to the cell membrane because the endoplasmic reticulum is essentially a structure of conterminous layer consisting of lipids and proteins. The lipophilic chemicals mainly enter into the lipid layers, the sites of biotransformation; therefore, the enzymes within the lipoprotein matrix are very important. The centrifugation generates many kinds of soluble enzymes involved in phase II biotransformation responses in the supernatant or cytosol. Thus, a number of the critical enzymes involved in the biotransformation are regularly named as cytosolic or microsomal to mark their subcellular sites.
Monooxygenations refer to the combination of one atom of an oxygen molecule with the substrate, but the other atom is reduced to water by nicotinamide adenine dinucleotide phosphate (NADPH). Monooxygenation of xenobiotics, also known as mixed-function oxidations, is either catalyzed by two monooxygenase systems, including cytochrome P-450-dependent monooxygenase system (also known as multi-substrate monooxygenase system) and flavin-containing adenine dinucleotide (FAD) monooxygenase (also called mixed-function amine oxidase) [11, 12]. These enzyme systems are mainly located in the cellular endoplasmic reticulum and put a hydroxyl group to the xenobiotics.
Reduced NADPH may provide the electrons associated with the reduction of cytochrome P-450 or FAD. Then, a component of the microsomal enzymes that react with molecular oxygen is reduced to form an active oxygen intermediate, leading to the oxidation of the xenobiotic compound [13]. So monooxygenases are known as mixed-function oxygenase (MFO) or hydroxylase too.
The phase I enzymes encompass a series of hydrolases, esterases, and amidases besides the two monooxygenase systems. Regardless of the remaining chemical structure, the cleavage of the ester or amide bond produces two functional groups for further biotransformation: a carboxylic acid plus either an amine (from an amide) or an alcohol (from an ester). Furthermore, the phase I enzymes also include a series of oxidation-reduction enzymes whose functions are to turn over the oxidation state of a carbon, leading to easier excretion or biotransformation by the phase II enzymes.
1.3.3 Phase II Enzymes
In phase II processes, the biotransformation is regarded as biosynthetic reactions in nature, and then, energy is required to trigger. The activation of the cofactors or the production of high-energy intermediates is usually important for the biotransformation. In view of either direct or indirect activation of the cofactors with adenosine triphosphate (ATP), the energy status in the organ is necessary to determine the availability of cofactors [14].
1.3.4 Factors Affecting Xenobiotic Metabolism
Although the biotransformation reactions are complex, the following general conclusions may be proposed [15]:
-
1.
A functional group is usually introduced into a xenobiotic during the phase I reaction, enabling it to bind to endogenous compounds in the process of the phase II reaction.
-
2.
The phase II reactions generally produce more water-soluble and easily excreted conjugates than the parent compound or the phase I metabolites.
-
3.
During the metabolic process, especially in phase I metabolism, more toxic reactive intermediates than parent compounds can be generated. Therefore, xenobiotic metabolism may be a process of detoxification or intoxication.
-
4.
Since metabolic attack may initiate a large number of enzymes involved in phase I and II reactions and there are a number of sites located on organic molecules, the number of potential metabolites and intermediates available from a single substrate is frequently very large.
-
5.
Because there’re qualitative and quantitative differences among species, strains, individual organs, and cell types, a specific exogenous chemical may acquire quite different fates in different scenarios.
-
6.
Since toxicants may be used as inducers and/or inhibitors of the enzymes involved in xenobiotic metabolism and exogenous chemicals are substrates of exogenous metabolic enzymes, they may interact and lead to toxic sequelae, which may be different from the expectation of only using any exogenous chemical.
-
7.
Because the influence of exogenous metabolic enzymes by endogenous factors also affects the enzymes of xenobiotic metabolism, the toxic sequelae from specific toxicants are expected to vary depending on developmental stage, nutritional status, physiological status, gender, and stressors.
-
8.
It has been demonstrated that most of the xenobiotic-metabolizing enzymes appear in the form of several isozymes, which coexist within the same individual and often within the same subcellular organelle. An understanding of the biochemical and molecular genetic processes of these isozymes may help to illustrate the variation among species, individuals, sexes, organs, and developmental stages more clearly.
1.4 Nutritional Modulation of Metabolic Enzymes
The relationship between nutrition and exogenous metabolism has always been a subject of widespread concern in academic circles. Effects of nutrients and biological substances, not only on detoxification of xenobiotics but also on pathological process of chronic diseases, have been the hot spot of intensive research. Nutrients, often referred to as xenobiotics from normal food intake, regardless of their nutritional value, mostly have effects on metabolic process of xenobiotics. Due to the fact that most toxicants make enzymes inactivated, the effect of nutrition on drug metabolism is considered to be the effect of nutrition on toxicants. For example, grapefruit juice contains naringin that influences the inactivation of the calcium channel blocker nitrendipine to increase its plasma concentration. This section focuses on two basic mechanisms of nutrients’ reactions to xenobiotic metabolizing enzymes, namely, induction and inhibition.
The enzymatic mechanisms of detoxification are involved in two metabolic networks, phase I and phase II detoxification reactions. The cytochrome P450-containing monooxygenases are the major enzyme systems in phase I reactions. About 150 different genes regulate the enzyme, which can be divided into various families and subordinates. It is well accepted that the cytochrome P450 isoenzymes are named and classified. And other oxidative enzymes include microsomal flavin adenine dinucleotide (FAD)-containing monooxygenases, epoxide hydrolase, alcohol dehydrogenases, aldehyde dehydrogenase, esterases, and amidases. The critical enzyme systems involved in phase II biotransformation processes are glucuronosyltransferases, glutathione-S-transferases, sulfotransferases, methyl transferases, N-acetyl transferases, and so on. There are lots of enzymes and their systems in the liver that catalyze the biotransformation of xenobiotics. Several nutrients may enhance the activity of hepatic microsomal mixed-function oxidases, such as phenobarbital and 3-methylcholanthrene.
The mechanism by which nutrients interact with detoxification (and toxification) enzymes can occur at different levels. At present, there are a lot of discussions about the influences of diet, caloric restriction, and nutrients on metabolic enzyme cytochrome P450, but the nutritional regulation mechanism of cytochrome P450 patterns has not in all cases been extensively studied and elucidated. In the following part, the effects of nutrients on cytochrome P450 and other major metabolic enzymes will be described mainly from the following aspects: starvation diet, dietary fat, protein, sodium, magnesium, and plant constituents.
1.5 Effects of Nutrients/Nutrition on Metabolism and Toxicity of Toxicants
Nutrition is involved in the alterations in the body composition, physiological and biochemical functions, and nutritional status of the population. Metabolizing systems require essential macronutrients and micronutrients. A multitude of dietary factors can have obvious influences on the metabolism and toxicity of foreign compounds. Anyhow, the lack of nutrient may result in destroyed health. For example, the decrease in caloric intakes may enhance the toxicity of caffeine and dichlorodiphenyltrichloroethane (DDT) in rats [16]. Some enzymes involved in the detoxification can be affected by diet through different pathways.
Dietary deficiencies in any nutrients can influence protein synthesis, leading to the alteration of cellular membrane, damage of the cellular integrity, changes of the membrane permeability transition and the functions of various macromolecules. Consequently, the ability of the organism to metabolize foreign toxicants may be influenced. The concentrations of critical enzymes required for toxicant metabolism can be disturbed by the bioavailability of nutrients, which interferes with the metabolic reactions involved in toxicant activation, inactivation, and excretion, thus altering toxicity. Cytochrome P450 and flavin proteases are the main enzymes that take part in the reduction of xenobiotics in the body. There is higher oxidoreductase activity in intestinal microflora, which acts a pivotal part in the reduction of xenobiotics. It is known that specific deficiencies in diet may enhance the toxicity of various pesticides, heavy metals, and atmospheric contaminants such as ozone. The levels of important chemicals that participated in the detoxification may also be changed with dietary changes, in that many nutrients, such as protein, lipid, carbohydrate, vitamin C, folate, iodine, and selenium, can change the levels of cytochrome P450 enzymes. Therefore, the effects of nutrients and nutritional status on the metabolism and toxicity of xenobiotics are mainly described in this section, including starvation, dietary macronutrients, micronutrients, and plant constituents.
1.5.1 Starvation
Starvation is a special physiological state; changing the inherent dietary pattern will also increase the susceptibility to liver toxicity injury. Fasting increases catabolic effects and decreases the glycogen stores in the liver, which interferes with the preparation of microsomal enzyme fractions and improves gastric absorption, and thus compromises resistance against cytotoxic agents. However, a set of evidence shows that the mechanisms of metabolism, toxicity, and toxicokinetics of a drug may be influenced via fasting. Eight-hour fasting may result in hypoglycemia and change the activities of some enzymes that metabolize the toxicants. In addition, the activities of cytochrome P450 can also be triggered by fasting in the liver and kidneys of rats, leading to the depletion of glutathione and the production of reactive oxygen species (ROS), oxidative stress, and lipid peroxidation and the reduction in glucuronide conjugation and detoxification [17,18,19]. Fasting can also increase the amount of certain P450 isoenzymes. Cytochrome P450 increases by 60% and 116% after 24 and 48 h of fasting in rats, respectively. The vital point is that both its activity and the amount of protein itself are increased, possibly by better access of substrate to the enzyme. Immunoblotting and complementary DNA (cDNA) probing have shown an increase in the respective mRNA ensuing from multiplied gene expression. The biosynthesis of cytochrome P450 is affected by the state of starvation (i.e., glycogen depletion and acetonemia). Streptozotocin-induced diabetes mellitus had an effect very comparable to that of fasting on hepatic cytochrome levels, and the acetone/ethanol-inducible structure improved four- to fivefold in diabetic and in fasting rats. In contrast, different isoenzymes were reduced very notably in diabetic rats and multiplied in fasting rats. Cytochrome P450 PCN-e (cyanopregnenolone-inducible) decreases under the conditions in the opposite treatment, namely, hyperalimentation by parenteral infusion of glucose and crystalline amino acids. It is interesting that oral administration of the same nutrient solution does not induce these effects, assuming this reverse effect on blood protein synthesis may be due to the difference in blood composition in the portal vein, similar to the “first-pass effect.”
NADPH-producing enzymes have been investigated in an aquatic animal, the American eel, under the influence of fasting and a diet of worms or cow liver. There were no differences in several NADPH-producing enzymes between eels fed with the liver diet and fasting. However, the worm diet may enhance glucose-6-phosphate dehydrogenase (G6PDH) activity. In rats, feed restriction caused a significant increase in the activities of NADPH-generating enzymes in the liver; the enzymes of drug metabolism also were increased by feed restriction.
1.5.2 Effects of Macronutrients on Metabolism and Toxicity of Toxicants
Macronutrients, including proteins, lipids, and carbohydrates, are needed in large amounts as energy sources. Excess of macronutrients may exaggerate the toxicity or the results of other macronutrient deficiencies or imbalance. For example, an increase in protein may lead to a decrease in one or both of lipids and carbohydrate.
1.5.2.1 Protein
Protein, an essential nutrient for the human body, is the major structural component to support the growth and tissue repair. Protein is also involved in the synthesis of important molecules like nucleic acid, enzymes, hormones, antibodies and in the maintenance of fluid and acid-base balance. Protein can provide fuel for the body’s energy need. Amino acids are the basis for forming a protein. Protein has wide variety and characteristics because 20 different amino acids can be infinitely combined and arranged in living organisms. Dietary protein consists of animal protein and plant protein, and animal protein plus soybean protein is usually considered as good-quality one. Sufficient protein can be easily acquired through a normal dietary intake. In fact, protein-energy malnutrition is one of the major nutritional problems worldwide. Possibly due to the differences in the consumptions of animal food and the economic levels, dietary intakes of protein differ extensively in a variety of components of the world [20]. As a major constituent of enzymes, protein is required in a variety of metabolic reactions. Lack of protein affects the enzymes involved in the metabolism of toxicants. For example, protein-deficient diets and specific changes in dietary protein type can decrease the concentrations of cytochrome P450 in liver microsomes, but not the changes in the amounts of protein [21].
The enzymes may influence the reactions that they catalyze because protein synthesis may be determined by the quality or quantity of amino acids. Protein deficiencies can result in the alterations in amino acid composition of the enzymes, the disturbance of substrate binding, or interaction with the enzyme, in turn the reduction of NADPH-cytochrome P450 (CYP450) reductase and some CYP450 isoenzymes [22]. Studies have shown that feeding rats with a low-protein diet of 6% casein will induce a very significant change in the amino acid composition of the purified form of hepatocyte cytochrome P450, with increased valine, isoleucine, and phenylalanine and decreased glutamine and tyrosine. These kinds of alteration may result in changes in, for example, substrate binding or catalytic activity.
Low-protein diet may also result in the interference with uridine diphosphate glucuronic acid (UDPGA)-glucuronyl transferases (UGT), glutathione-S-transferases (GST), and numerous antioxidant enzymes. UGTs are responsible for the conjugation of drugs with UDPGA. Dietary protein acts a pivotal part in the glutathione biosynthesis and the protection of cells against the injury by ROS. Some small molecules, such as glycine, glutamine, cysteine, and taurine, are also associated with the conjugation of xenobiotics. The capacity of detoxication is closely related to enzyme activities. For example, the increase in the activities of mixed-function oxidase led to an obvious decrease of sleeping time triggered by barbiturate in rats. The variation of dietary protein contents from 0% to 50% is correlated with the reduction of serum pentobarbital. With a low-protein diet in rats, it will be noted that the increase in GST-C and glucarate transferases is mainly in the intestines. Also, an increase in urinary recovery of oxazepam glucuronide was observed when changing from a high-protein/low-carbohydrate diet to a low-protein/high-carbohydrate diet.
Protein can influence the carcinogenesis. Male Wistar rats were paired with an isocaloric feed containing 5%, 15%, or 40% casein, and a single dose of aflatoxin B1 was used to induce tumorigenesis. Tumor initiation was achieved by 2-acetylaminofluorene. Significant differences in the total microsomal P450 could not be found, but steroid 16-α-hydroxylation was noted in a high rate. However, α-glutamyl transferase and glutathione-S-transferase in precancerous foci were increased in proportion to the dietary protein. The toxicity of several pesticides and other toxic agents can be enhanced by low-protein diets whereas protects against the hepatotoxicity of carbon tetrachloride and dimethylnitrosamine exposure in rats.
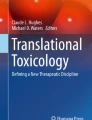
Low-protein diets may likely cause a decrease in microsomal enzyme systems and a suppression of protein availability for enzyme synthesis in protein-deficient animals [23]. This is probably the basis that low-protein diets exert protective roles in the toxicity of toxicants. On the other hand, some compounds may increase toxicity through conversion to a more toxic metabolite while exhibit decreased toxicity in malnourished animals. Heptachlor, a chlorinated hydrocarbon insecticide, is an example of such compounds. Heptachlor is converted to heptachlor epoxide, a more toxic metabolite, by mixed-function oxidases of liver microsomes. But this conversion is diminished in rats fed with low-protein diets. Protein deficiency may increase the LD50 for heptachlor by threefold in rats but has no significant effect on the LD50 for heptachlor epoxide, approximately equivalent in rats with pair-fed deficient, adequate, or high levels of protein (Fig. 1.2) [24]. Dietary protein intake also influences other pesticide toxicity: marked increase in the toxicity of carbamate carbaryl, parathion, and phthalidimide captan; the decrease in the toxicity of heptachlor; and no change of the toxicity of dimethoate. In summary, low-protein diets suppress CYP450 and finally may result in the elevation or depression of the toxicity of foreign substances, relying on the toxicity of the products.

Effects of diets with different amounts of protein on LD50 values for heptachlor and heptachlor epoxide in rats
High-protein diets may promote oxidative drug metabolism and hepatic mixed-function oxidase activities and reduce the toxicity of chemicals, though excess protein intake may be harmful to health. It was shown that high dietary protein fed to rats decreased the incidences of breast cancer induced by 7,12-dimethyl-benz(a)anthracene and the incidence of gastric cancer induced by N-methyl-N-nitro-N-nitrosoguanidine (MNNG) [25, 26]. Sulfur-containing amino acids can provide the protection against the toxicity of some metals. Besides, the toxic effect of cadmium can be antagonized by zinc because of its competition role with −SH. As a free radical scavenger, the special peptides in protein can remove free radicals, protect the cell membrane from suffering oxidative damage, prevent the erythrocyte hemolysis, and promote the reduction of methemoglobin.
1.5.2.2 Lipids
Lipid comprises a group of naturally occurring molecules soluble in organic solvents, including triglycerides (fats and oils), phospholipids, and sterols. Triglyceride is the chief form of lipid in foods and in the human body, accounting for 95%. A triglyceride molecule is made up of one unit of glycerol and three units of fatty acids. The fatty acids can be classified into saturated, monounsaturated, or polyunsaturated fatty acids according to the degree of saturation. Fatty acids in food may influence the composition of fats in the body. Lipids in the body mainly function as energy fuel and energy stores, cushion of vital organs as shock absorber through fat pad, insulation against extreme temperature, provision of structural materials for cell membranes, and participation in cell signaling. They are also sources of essential unsaturated fats and lipid-soluble vitamins. The primary issue on health problems for lipids is their function in chronic diseases, particularly in cardiovascular diseases and obesity.
Additionally, lipids are involved in the metabolism of toxins. The cytochrome P450 system is actually a coupled enzyme system composed of two enzymes: NADPH-cytochrome P450 reductase and a heme-containing enzyme, cytochrome P450. These enzymes are embedded in the phospholipid matrix of the endoplasmic reticulum. The lipid composition of the endoplasmic membranes not only extensively influences the activity and function of cytochromes P450 but, on the other hand, is susceptible to the number of the dietary fat. Phosphatidylcholine is important since the metabolism of toxins and the combination of substrates with mixed-function oxidases are enzymatically degraded by phospholipase C [27]. Phosphatidylcholine may play roles in maintaining membrane integrity. Steroids and fatty acids are located in CYP450-binding sites and then lead to the substitution of foreign substrates and the interference with their metabolism. The activities of certain toxicant-metabolizing enzymes are suppressed via feeding diet deficient in linoleic fatty acids and essential fatty acids. Dietary lipotropes include choline, methionine, glycine, folate, vitamin B6, vitamin B12, polyunsaturated fatty acids, and phosphate. They are required for the synthesis of phospholipids and membranes, which is essential for the constituents of the microsomal mixed-function oxidase system. The reduction in certain CYP450 isomers and the rise of tumorigenesis by chemical carcinogens may result from the deficiency of choline and methionine in the diet.
The administration of a ketogenic diet containing corn oil for 4 days increased hepatic microsomal P450 2E1 compared with that of rats with lower fat/carbohydrate ratios. Unsaturated fats increase hemoprotein and enzyme activity by twofold compared to olive oil and lard. The induction of hemoprotein of dietary fat has been studied by comparing the effects of a fat free with a 20% corn oil diet. The corn oil admixture did not affect the synthetic level of P450 2B, but increased the constitutive level of P450 2E (ethanol inducible). The decrease in the biosynthesis efficiency of cytochrome P450 heme protein in a fat-free diet may be due to the following two phenomena: insensitivity to inducers and lack of fatty acids needed to synthesize a phospholipid matrix that correctly locates the active protein. Dietary corn oil can increase the activities of other isoenzymes, such as testosterone 6-hydroxylase. Similarly, the phenomenon that aryl hydrocarbon hydroxylase and 7-ethoxycoumarin O-deethylase activities was increased in the lung of food-restricted rats and decreased after high-fat diet, but not in liver. In addition, a 20% corn oil diet increases one form of glutathione-S-transferase, namely, GST-B, but not GST-A.
Unsaturated essential fatty acids are necessary to maintain membrane function. Therefore, the liver microsomal mixed-function oxidase was stimulated by high intake of polyunsaturated fatty acids. Menhaden oil can not only increase the liver cytochrome P450 but also increase the catalytic ability and affinity to some substrates. In particular, menhaden oil produces higher P4502E1 activity, which significantly increases the metabolic rate.
Both polyunsaturated fatty acids and dietary fat peroxides play an important role in oxidative demethylation as well as phenobarbital inducibility. Briefly, fats may have an effect on the exercise of P450 2B while enhancing the constitutive degree of the ethanol-inducible P450 2E, and it confirmed exclusive consequences on glutathione-S-transferases. Also, it appears transferases are influenced in a way similar to P450 in terms of activation by either food restriction or fat-containing diets.
Diet-induced adiposity may influence the availability of circulating toxicants via toxicant sequestration in adipose tissues. The levels of persistent organic pollutants (POPs) in plasma are negatively associated with fat composition in the body [28]. However, POPs exhibit high lipid solubility and bioaccumulation in fatty tissues. POPs may negatively influence the environment via long-distance transport and bioaccumulation. The first process makes these chemicals transfer far from their original source, and the second reconcentrates them to reach potentially dangerous levels for long periods of time. Therefore, these chemical compounds can persistently exist in the environment and also elevate their concentration and toxicity in the environment in view to the bioaccumulation when they are taken in by animals.
1.5.2.3 Carbohydrates
Carbohydrate is a massive and assorted type of organic substances found in nature, consisting of carbon, hydrogen, and oxygen in the ratio of 1:2:1. Carbohydrate is often divided into monosaccharides, disaccharides, and polysaccharides. Carbohydrates are widely located in plants and animals, where they play both structural and metabolic roles. They are essential for providing glucose for metabolic fuels and energy stores. Carbohydrates are also structural components of cell walls and nucleic acid (DNA and RNA) and integral linkers of many proteins and lipids as glycoproteins and glycolipids. There are relatively few reports on toxic effects related to carbohydrate intake in healthy people.
Few evidences are identified concerning the specific function of carbohydrates in biotransformation. Dietary carbohydrate may have generalized effects on intermediary metabolism, such as caloric effects and hormonal alteration effects. A large amount of sugar intake including glucose, sucrose, or fructose may prolong the sleeping time induced by phenobarbital in mice. The longer duration of sleep is negatively connected with the metabolism of the barbiturate. Compared with starch, high-sucrose diets potentiate the lethal reaction to benzylpenicillin because of lower conversion rates of its toxic products. Additionally, the levels of biphenyl 4-hydroxylase activity are lower in rats fed with high sucrose or glucose plus fructose, which has more to do with lower levels of cytochrome P450. Glucose is the precursor of glucuronic acid and closely correlated with phase II detoxification reactions [29]. It is shown that the activities of hepatic CYP450 are decreased and the activation and binding to DNA of carcinogen aflatoxin B1 are increased, given unrestricted feeding, which lead to the reduction of aflatoxin B1 detoxification in the body.
The incidence of spontaneous and chemical-triggered tumors was much lower in rodents and other animals when fed with calorie-restricted diet than fed ad libitum. For example, mammary tumors could not be induced by 7,12-dimethylbenz(alpha)anthracene in rats whose calories were intermittently restricted [30]. Furthermore, calorie restriction significantly elevated the activities of several drug-metabolizing enzymes (such as CYP2E1), compared with ad libitum feeding in animals [31]. Diet restriction may lead to the decrease in oxygen consumption, the increase in insulin binding, and the changes in energy metabolism through enzymatic alteration involved in glycolysis, gluconeogenesis, and lipid metabolism. Therefore, the activation of some phase II enzymes, such as UDP-glucuronyltransferases, glutathione-S-transferases, and N-acetyltransferase by calorie restriction, might suppress the incidence of chemical-induced tumors. It is speculated that calorie restriction could also reduce enzyme degradation associated with aging.
1.5.3 Effects of Micronutrients on Metabolism and Toxicity of Toxicants
Micronutrients, which are made up of vitamins and minerals, are essential to life, though the amount needed to meet the body’s needs is much less than macronutrients. Many vitamins and minerals have been detected to affect the metabolism of foreign chemicals through the microsome system. Moreover, most studies have shown that micronutrient deficiencies do not have a significant effect on microsomal enzymes as protein deficiencies. But the activities of poison-metabolizing enzymes will be influenced to some extent when micronutrients are severely deficient.
1.5.3.1 Vitamins
Vitamins are divided into water-soluble vitamins (B and C) and fat-soluble vitamins (A, D, E, and K) and play essential roles in health. Insufficient vitamin intakes can result in the classical deficiency diseases. So it is sometimes believed to consume vitamins in large concentrations, even 100 times the recommended dietary levels.
Large amounts of vitamin supplements or the misuse of specific foods can easily lead to toxic reactions.
1.5.3.1.1 Fat-Soluble Vitamins
Fat-soluble vitamins can accumulate in the body, if their intake exceeds the body’s requirements, leading to potential toxic effects. It is known that excessive intake of vitamin A and D can cause typical symptoms of toxicity.
Vitamin A may inhibit the bioactivation of carcinogens or bind foreign compounds to microsomal proteins; therefore, it has a function of antitumor. Retinol reduces the mutagenicity of heterocyclic amines by inhibiting their activity. Carotenoids, as provitamin A compounds, may inhibit the mutagenicity of aflatoxin B1 independent of vitamin A. Excessive intake of vitamin A compounds can cause permanent liver damage and stunting. Normally, when excessive intake is stopped, the symptoms of poisoning will be reversed. Common supplements do not easily cause acute toxicity in adults, but there are risks for children. Acute toxicity will appear symptoms within a few hours, such as nausea, vomiting, headache, dizziness, blurred vision, infant fontanelle protuberance, lethargy, and anorexia. Chronic toxicity may take weeks to months to develop clinical symptoms including headache, loss of appetite, hair loss, large liver, muscle pain and stiffness, dry and itchy skin, double vision, bleeding, vomiting, and coma.
Excessive intake of vitamin D will cause the body’s absorption of calcium and phosphorus to increase, resulting in hypercalcemia and hypercalciuria, thereby increasing the product of blood calcium and phosphorus in the body and abnormal calcification after reaching saturation. Due to the large amount of calcium excreted by the kidneys, kidney calcification is most obvious, followed by the heart, blood vessels, thyroid, and pancreas. The effects on the skeletal system are mainly thickening and widening of the calcification zone of the long bone metaphysis, thickening of some cortical bone, and bone sclerosis. The symptoms of acute toxicity are mainly hypercalcemia, nausea, vomiting, restlessness, low fever, diarrhea, acidosis, and severe cases include convulsions, coma, and even acute death. The symptoms of chronic toxicity include systemic fatigue, anorexia, polyuria, and constipation. Due to abnormal calcification, there may be different organ damages, such as renal calcification, renal tubular necrosis and proteinuria, hematuria, chronic renal insufficiency, or even kidney decline. Pulmonary calcification has localized epithelial cell necrosis, which can easily lead to repeated infections. Withdrawing the source of the vitamin can reverse the symptoms in general.
Vitamin D may have interactions with diverse inorganic ingredients such as essential minerals and toxic metals [32]. 25(OH)D3 is the dominant form of vitamin D in the blood and a precursor of 1,25-(OH)2D3 (the active form of vitamin D). Adequate amount of 25(OH)D3 can adjust the body’s absorption, metabolism, and excretion of mineral elements such as calcium, magnesium, iron, phosphorus, zinc, and copper. However, high levels of 25(OH)D3 increase the absorption of toxic elements such as aluminum, cadmium, cobalt, lead, and radioisotopes. Conversely, increased absorption of cadmium and lead may lead to decreased levels of active vitamin D in the kidney. In children, due to the increase in intestinal absorption in summer, the level of blood 25(OH)D3 will increase seasonally. In turn, the biological accumulation of these toxic metals can disrupt the body’s physiological function of vitamin D.
Dietary vitamin E is readily absorbed and transported to cell membranes and to intracellular sites. Vitamin E can scavenge free radicals, prevent oxidative damage to crucial biomolecules, and protect microsomal membranes against lipid peroxidation. A lack of tocopherols, the most abundant form of vitamin E, leads to decreased cytochrome P450 and drug metabolism [33]. Vitamin E can prevent chronic liver injury induced by carbon tetrachloride, increase the levels of CYP2C11 and CYP3A2 in the liver, and inhibit dimethyl benzanthracene mammary tumors. Vitamin E is a scavenger of free radicals. Lack of vitamin E increases free radicals in the body, leading to the body being more sensitive to various oxidative damage, such as ozone, nitrogen dioxide, and other air pollutants. High intakes of vitamin E and vitamin K seem to have relatively less toxicity. No mutagenic, carcinogenic, or teratogenic effects are reported. However, when the intake dose of vitamin E reaches ten times of dietary reference intakes, the immune system may be damaged, such as white cells. Excessive intake of vitamin E may affect platelet aggregation. It can influence blood coagulation system in people with low vitamin K. Although vitamin K is fat-soluble, it is readily excreted from the body and produces scarce toxicity.
1.5.3.1.2 Water-Soluble Vitamins
Water-soluble vitamins tend to produce lower toxic effects than fat-soluble vitamins, mainly due to the fact that they are easily dissolved in water and excreted outside the body. Accordingly, large or excessive consumption can be rapidly eliminated in the urine and sweat, and discernible harm to the individual can be avoided. Therefore, it should be ignored for some water-soluble vitamins that they may have an influence on the body in excessive doses.
Vitamin C, also known as ascorbic acid, is a potent reductant and plays critical roles in hydroxylation and redox reaction. One of its essential functions is to depress the microsomal oxygenation of many xenobiotics. Furthermore, vitamin C can be combined with glucuronides through UDPGA to promote the clearance of the phase I products [34]. Vitamin C deficiency has been shown to decrease the toxicant metabolisms in guinea pigs and also affects the contents of CYP1A and CYP2E in liver. Cytochrome P450 plays a vital role in activating carcinogens such as aflatoxin B1 and heterocyclic amines in foods. Vitamin C is an important antioxidant and free radical scavenger, which has the functions of antiaging, anticancer, reducing serum cholesterol, and preventing atherosclerosis. Vitamin C deficiency is also associated with decreased immunity, skeletal muscle atrophy, neurological disorders, poor wound healing, and impaired capillary integrity. On the other hand, there exist considerable controversies over the efficacy and toxicity of megadoses of vitamin C.
Vitamin B1, that is, thiamin, acts a pivotal part in the carbohydrate metabolism by means of forming thiamine pyrophosphate (TPP), its coenzyme derivative. Dietary deficiency of thiamin can increase aminopyrine and ethylmorphine metabolism. Thiamine deficiency is negatively correlated with increased cytochrome P450 activity, ROS induction, lipid peroxidation, and cytochrome P450 destruction [34]. The clinical manifestation of thiamine deficiency is anorexia, weight loss, cardiac involvement, and neurological involvement.
Vitamin B2, also known as riboflavin, is an important element of NADPH cytochrome P450 reductase and a cofactor for FAD and FMN. Vitamin B2 is involved in biological oxidation and energy metabolism in vivo and is related to carbohydrate, protein, nucleic acid, and fat metabolism. Its deficiency can significantly affect the metabolism of glucose and lipids in tissues and cells, leading to incomplete oxidation, reduced energy utilization, and ultrastructure of mitochondria. And this will also have an adverse effect on poison metabolism. The main clinical symptoms of vitamin B2 deficiency are the inflammations of the eye (blepharitis, photophobia, blurred vision, tears), mouth (stomatitis, glossitis, map tongue), skin (seborrheic dermatitis), and genital (scrotitis, vaginitis).
Niacin is the precursor of nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP), two coenzymes involved in almost all redox reactions. Besides, the two coenzymes formed by niacin are also the hydrogen transporters in the first biochemical reaction of the pentose phosphate pathway of glucose, which are related to the synthesis of nucleic acids. In the treatment of niacin deficiency, high doses of niacin (100–300 mg oral or 20 mg intravenous) can cause a variety of side effects including diarrhea, dizziness, fatigue, dry skin, itching, dry eyes, nausea, vomiting, high uric acid, arrhythmias, and hepatotoxic reactions. The treatment dose of niacin deficiency disease can be used to dilate blood vessels and reduce serum cholesterol, but it may be accompanied by some reversible adverse reactions such as pigmentation, dry skin, and ulcers. However, nicotinamide can not lower serum cholesterol, and high doses of this have no side effects.
Vitamin B6, also known as pyridoxol, when taken orally at 2 g/kg or 20 times the dietary reference intake for peripheral neuritis, can cause oral toxicity, resulting in convulsive disorders and inhibition of prolactin secretion. The remaining water-soluble B vitamins, such as pantothenic acid and thiamine, from dietary sources, show few side effects.
The important physiological function of folate is to participate in metabolism as a carrier of carbon monoxide and act a pivotal part in cell division and proliferation, and it is necessary for the growth of many organisms and microorganisms. Folate deficiency can lead to megakaryocytic anemia, hyperhomocysteinemia, preeclampsia, placental abruption, and fetal neural tube abnormalities and is associated with some cancers. Therefore, it is recommended that women of childbearing age increase their intake of folate. Folate is necessary to increase the conversion of toxicant-metabolizing enzymes during chronic drug administration in rats. High doses of folate can also have side effects, affecting zinc absorption, leading to zinc deficiency, delaying fetal growth, increasing low birth weight, inducing convulsions by interfering with the effects of anticonvulsants, masking vitamin B12 deficiency symptoms, and interfering with the diagnosis of the disease.
1.5.3.2 Minerals
1.5.3.2.1 Iron
The synthesis of heme, which is vital to the biosynthesis of cytochrome P450 and to regulate mixed-function oxidase activity, depends on iron. Iron deficiency causes anemia but rarely affects cytochrome P450. The levels of cytochrome c and myoglobin are reduced in anemic rats with iron-deficient diets [35]. Competitive low intake of iron promotes the absorption of lead, while high intake of iron may inhibit lead absorption and toxicity via the competition with intestinal mucosal carrier protein and other transport carriers. Iron protects against mercury toxicity, and mercury exposure may result in iron deficiency.
The iron content of the body is mainly controlled by the absorption mechanism, but there is no regulatory mechanism to discharge excess iron out of the body. Once the mechanism of iron absorption is damaged due to some reason, such as hereditary hemochromatosis, iron agent treatment, and repeated blood transfusion, the iron transferred into the plasma will increase, which will lead to excess iron in the body [36]. In hemochromatosis, iron is absorbed in excess, and parenchymal cells are loaded with too much iron, resulting in clinical complications of diabetes mellitus, endocrine abnormalities, cardiomyopathy, arthritis, liver cirrhosis, and even hepatic cancer. Furthermore, the main target organ of iron overload injury is the liver, which can cause liver fibrosis and hepatoma. Excessive iron can also lead to excessive production of reactive oxygen species and free radicals, which can cause mitochondrial DNA damage and induce mutations, which are related to colon cancer, rectal cancer, lung cancer, esophageal cancer, bladder cancer, etc. Iron also catalyzes the production of free radicals and promotes lipid peroxidation, which in excess increases the risk of cardiovascular disease and atherosclerosis.
1.5.3.2.2 Selenium
Selenium found in all cells and tissues is an essential trace element, but too much of it can be toxic. Seafood and animal offal are good sources of selenium. The selenium content of plant foods is related to the level of selenium in the surface soil layer. Drinking water contains inorganic forms of selenium, which are not as readily absorbed as the selenoamino acids present in vegetables. Selenium, an important ingredient of some antioxidant enzymes such as glutathione peroxidase and thioredoxin reductase, has the function of anti-oxidation, which can block the damage of reactive oxygen species and free radicals to the body so as to maintain the normal function of cells. Selenium protects cardiovascular and cardiac health. It also has immune-boosting and growth-promoting properties. Selenium and metal have a strong affinity and play a role in detoxification. Selenium is involved in the synthesis of deiodinase, which is necessary for the transformation of thyroxine (T-4) into triiodothyronine (T-3).
According to the epidemiological investigation of the population, it was found that the incidence rate of tumors in selenium-deficient areas increased significantly, suggesting that selenium may have a protective effect on a variety of human tumors. The anticancer mechanisms may include the protection of DNA from oxidative degradation, the promotion of carcinogen metabolism, the enhancement of immune function, the regulation of cell cycle, and the changes in apoptosis [37, 38]. Two large-scale trials (prevention of Cancer by Intervention with Seleniumm pilot study (PRECISE) in Europe and The Selenium and Vitamin E Cancer Prevention Trial (SELECT) in the United States) on the anticancer effect of selenium, which were recruited by over 30,000 participants, respectively, can play an important role in the future.
Selenium deficiency can cause Keshan disease characterized by myocardial injury, which may be related to enhanced lipid peroxidation caused by selenium deficiency, resulting in myocardial fibrosis and necrosis, myocardial arteriole, and capillary injury. Selenium deficiency also leads to growth retardation, neurological visual impairment, and reduced immune function. In addition, selenium deficiency is believed to be an important cause of Kashin-Beck disease. However, long-term excessive dietary selenium can result in growth inhibition, liver damage, and chronic selenium poisoning, with symptoms including hair and nail loss, skin damage and neurological abnormalities, numbness and convulsions in the extremities, and death in severe cases. Elevated levels of dietary selenium may also increase superoxide radicals. Consumption of high intake of selenium should be avoided because the safe range of dietary intake for selenium is narrow.
1.5.3.2.3 Zinc
Zinc deficiency can increase oxidative damage, decrease the activity of various zinc-containing enzymes, weaken the immune function of the body, and affect the growth and development of the fetus. There is an evidence that zinc toxicity that impairs immune response and turns down the levels of high-density lipoprotein (HDL) cholesterol is caused by long-term high doses intakes (about 6–20 times the recommended nutrient intake (RNI)). Zinc toxicity also induced copper deficiency. Symptoms of acute zinc toxicity include vomiting, epigastric pain, fatigue, and lethargy. Zinc supplementation decreases the accumulation of lead in tissues. Zinc protects against methylmercury damage. On the other hand, lead inhibits zinc for intestinal absorption and replaces zinc on hem enzyme; cadmium also inhibits zinc for absorption and replaces zinc on metallothionein.
1.5.3.2.4 Other Minerals
Long-term excessive intake of sodium chloride may have influences on the amount of cytochrome P450 and glutathione peroxidase activity. After a 360 days’ feeding of an 8% sodium chloride diet, a phenomenon that a decrease of cytochrome P450 content and an increase of glutathione peroxidase activity may lead to influence the capacity of activating benzo[a]pyrene to Ames-positive mutagens was found, suggesting that the detoxification ability of the body was affected under the condition of long-term excessive intake of sodium.
Magnesium poisoning is not easy to occur under normal circumstances, but in patients with renal insufficiency or treatment with magnesium, magnesium poisoning is often caused by excess magnesium in the body. Excessive intake of magnesium can lead to diarrhea, nausea, gastrointestinal spasm, and other gastrointestinal reactions; serious patients may appear to have drowsiness, muscle weakness, weak knee tendon reflex, muscle paralysis, and other clinical symptoms. It was found that the production of glucuronic acid in isolated hepatocytes was reduced by about 50% after 10 days of feeding the rats with magnesium-deficient feed.
Excessive copper intakes over the binding capacity of the liver may cause toxicity. Early signs of copper toxicity include weakness, listlessness, and anorexia, followed by hepatic necrosis, vascular collapse, coma, and even death. Manganese poisoning mainly damages the central nervous system and causes reproductive secretion dysfunction.
1.5.4 Phytochemicals
With the discovery of phytochemicals in cruciferous vegetables, more and more evidences show that these secondary metabolites can improve certain biological functions, and their content in food is low.
The major sulfur-containing constituent in the garlic, diallyl sulfide (DAS), is proved to have the function of inhibiting the process of cytochrome P450-catalyzed oxidations. Under the catalysis of cytochrome enzyme, DAS is oxidized to DASO and finally to DASO2, competitively inhibiting cytochrome P450 2E1. On the other hand, garlic oil has the hypolipidemic function, which is attributed to the activation of lipase and the deprivation of NADPH. In addition, as an inhibitor and inactivator of P450 2E1, the sulfur-containing compound disulfiram can inhibit aminopyrine demethylation in vivo and in vitro.
Naringin is the active form of a flavonoid from citrus fruits. Naringenin, the aglycone of naringin, is readily formed in human bodies after consuming grapefruit juice. This compound can inhibit the oxidative metabolism of drugs by inhibiting cytochrome P450 3A4. The function of the active ingredients in the grapefruit juice has been reported to promote drug metabolism. Felodipine, the dihydropyridine calcium channel antagonist, increased over fivefold greater in the plasma under the action of grapefruit juice compared to the water. One study reported that the cytochrome P450 3A4-mediated 7-hydroxylation of coumarin in the human bodies is not inhibited by naringin when given in water instead of grapefruit juice, as measured by the urinary excretion of 7-hydroxcoumarin, while various amounts of naringin added to grapefruit juice show a dose-dependent inhibition. Thus, it can be deduced that a possible synergism between grapefruit juice (or one of its components) and naringin and the inhibitory potency of grapefruit juice can be amplified by naringin.
Prenylated flavonoids extracted from hops are found to be very effective in inhibiting human P450 enzymes in vitro. Hops contain a large number of flavonoids, of which xanthohumol has the strongest inhibitory effect on the 7-ethoxyresorcinol deethylase activity expressed by human P450CYP1B1 cDNA expressed at low molar concentrations. This suppression is inherently competitive. However, whether the intake of hop-related inhibitors is sufficient to be effective in the human body remains to be verified. Since isoxanthohumol and 8-pentenylnaringenin can also inhibit the in vitro metabolic activation of carcinogen AFB1, the abovementioned phytochemicals may prevent the carcinogenic effects of AFB1.
1.6 Other Interactions of Nutrients/Nutrition and Toxicants
Nutrition and toxicants are connected in three main ways (Fig. 1.3). First, food is the medium of exposure to poison and enhance the individual exposure chances. Second, when a toxicant enters into the human body, it might also have an interaction with an individual’s nutrition status and have an effect on the quantity of toxicant retainment and bioavailability. Toxicants may affect nutrient absorption and stores as well. Third, nutrients and their metabolism may also interact with the toxicant via affecting a specific health outcome in the body. Other factors should be considered at the same time, since they influence both nutritional status and toxicant exposure, such as age and gender.

A model of interaction between nutrients and toxicants
1.6.1 Nutritional Deficiencies May Influence the Exposure and Toxicity of Toxicants
Lead, as a heavy metal used in chemical industry, can be found everywhere in our lives. However, if consumed in excess, it can lead to lead poisoning, especially in children and pregnant women, who are at high risk of lead exposure. Moreover, lead exposure causes irreversible damage to the growth and development, psychological and behavioral development, intellectual development, and potential development of fetus and infant [39]. The interactions between lead and micronutrients occur in intestinal absorption, brain neurochemistry, and cognitive function. The divalent metal transporter 1 is a common intestinal transporter for iron and lead. So iron deficiency may increase the absorption of lead.
A number of evidences prove that higher doses intake of calcium may inhibit lead absorption in blood. Placental transfer of lead is lower in pregnant women who consume diets rich in iron and diets with higher hemoglobin levels. Nutritional interventions may contribute to the prevention against lead exposure in the condition of extensive exposure or the source beyond the control. Iron and calcium supplementation shows some positive effects.
Cadmium exposure is associated with renal tubular toxicity and bone metabolism disorder. Health effects associated with cadmium are more common in women than men. Cadmium is not an essential element in the body, but is absorbed from the environment after birth, mainly through foods such as shellfish, leafy vegetables, rice, grains, and beans, which may contain relatively high levels of cadmium, water, and air. Tobacco smoke is an important source of environmental cadmium. The absorption mechanism of cadmium is basically the same as that of iron, calcium, and zinc. Dietary protein, vitamin D, calcium, zinc, and other elements can affect the absorption of cadmium. Vitamin D can promote the absorption of cadmium, and cadmium can, in turn, interfere with the absorption of dietary iron. Low protein, low calcium, and low level of iron contribute to the absorption of cadmium. Low iron stores and intake may result in higher cadmium burdens in the body [40]. Both cadmium and iron are ingested into the colon by means of the divalent metal transporter 1, and after that, cadmium (and lead) is likely rearranged into the circulation system through calcium transporters and ferroportin. It is possible that the absorption of cadmium may increase at very early stages of iron deficiency.
1.6.2 Nutrients Affect the Disposition of Toxicants
Besides the influence of absorption, nutrients can also affect the toxicity of xenobiotics by sequestration into body depots, such as the deposition of chlorinated hydrocarbons in adipose tissue or lead in the bone. Then, these compounds have relatively less chances for adverse effects on metabolism than the case that they would be deposited in the liver or kidney. For example, chlorinated hydrocarbons are mainly stored in adipose tissue of mammals. Under the condition of starvation for short periods, fat is mobilized from the depots for energy provision, and simultaneously, the excretion of dieldrin obviously elevates in blood of rats [41]. Moreover, the duration of exposure to dieldrin needed to produce overt poisoning is connected with the size of adipose tissue in dogs, while force-feedings of dogs may delay or prevent dieldrin poisoning, possibly by sequestering the dieldrin in adipose tissue. On the other hand, when given low-calcium diets, bone formation is lower, or the bone is resorbed to provide calcium, and lead deposition is dramatically increased in the kidney and blood (Fig. 1.4).

Effects of dietary calcium deficiency on lead disposition
1.6.3 Nutrient Deficiencies and Toxicants Affect Similar Outcomes
Arsenic toxicity is caused by excessive consumption of arsenic from food and water contaminated with arsenic, as well as long-term exposure to arsenic at work. Arsenic is linked to lung, bladder, and skin cancers and is related to an increased risk of diabetes mellitus and hypertension, particularly in populations with high exposures. An interaction may occur between arsenic and nutrient status and metabolism (folate) on health outcomes [42].
Malnourished individuals may be more susceptible to adverse health effects of toxic substances. Because of the physiological changes in women of reproductive age and the growth and development of characteristics of young children, they are more likely to suffer from malnutrition and toxicant exposure. Chemical exposures may cause neurodevelopmental disorders.
Fetal growth requires a lot of nutrition, so women of reproductive age are more likely to be undernourished during pregnancy. In addition, the environmental exposure of women of reproductive age is particularly dangerous because of their connection to fetuses and infants through placental exchange and breast milk. Finally, exposure to toxicant may accelerate the development and course of chronic diseases in adulthood, particularly neurodegenerative diseases. Exposures to toxicants during early life may program later disease and adverse outcomes through epigenetic processes [43].
The fraction of environmental exposure–related disease may be small, but the importance of nutrition in affecting health cannot be neglected. The interaction between chemical exposures and poor nutrition may result in chronic diseases with high costs to health.
Nutrients and toxicants may also regulate the function of the same enzymes and organ systems. For example, the activity of the enzyme 8-aminolevulinic acid dehydratase (ALAD) requires zinc but is inhibited by lead. Zinc can antagonize ALAD inhibition generated by lead in vivo and in vitro [44]. Lead can inhibit the synthesis of protein, and a portion of this inhibition can be overcome by higher concentrations of Fe in vitro.
Similarly, nutrients and toxicants often influence the same organ systems or parameters of toxicity, although affecting different enzymes or different steps in biochemical synthesis. For example, in the hematopoietic system, an anemia occurs with deficiencies of cobalt, copper, iron, and fluorine as well as with toxicities of cadmium, lead, manganese, molybdenum, selenium, and zinc. The development of poisoning-triggered anemia can be dependent on the levels of the nutrients [45]. The anemia of manganese toxicity is associated with low iron levels in the serum, liver, kidney, and spleen and may be improved by increasing dietary iron. Anemia due to cadmium toxicity is associated with low levels of iron in plasma and the liver. The increase in dietary intake of ascorbic acid may improve the anemia through increasing liver iron contents.
1.6.4 Nutrient Deficiencies May Produce More Complicated Alterations of Toxicity
Nutritional deficiency and toxic substances can also arouse more complicated alterations of toxicity, such as nonspecific behavioral changes including growth inhibition or animal anorexia. In certain situations, the decrease in the dietary levels of the toxic compound may improve the behavioral defect. For example, iron deficiency and lead poisoning in children can lead to clinical behavioral defects, such as hyperkinesia. Iron deficiency, which is common in children, is often accompanied by high exposure to lead, so lead-related behavioral changes may be due in part to iron deficiency [46].
The interactions between nutrients and toxicants are complex. Simply feeding high levels of nutrients does not certainly protect against toxic compounds. Dietary intake of a nutrient from deficient to adequate levels may provide protective effects against toxicity. However, much higher levels of the nutrient may lead to increased risk of toxicity itself, but also, the protection from the toxicants may be reversed or not needed. In some cases, ingesting high levels of nutrients may simply speed up their transformation into more active forms of metabolism.
1.6.5 Some Nutrients in Food Can Block Nitroso Reaction
N-nitroso compounds exhibit strong carcinogenic properties with specific targeting for the liver. Vitamins C and E, phenolic acids, and flavonoids have strong effect to block the nitroso reaction. Some foods, such as tea, kiwi, and sea buckthorn fruit juice can prevent against the toxicity of nitrosamines. Garlic may inhibit the activities of nitrate-reducing bacteria in the stomach, therefore significantly decreasing nitrite contents in the stomach. As precursors of n-nitroso compounds, nitrates, nitrites, and amines exist widely in the living environment. Due to the presence of pH value, catalysts, inhibitors, and other factors, the absorption rate of the precursor will be affected, thus affecting the reaction rate and yield of the synthesis of n-nitroso compounds. Until now, it has been impossible to estimate the number of nitrosamines formed in the stomach from ingested precursors. As a result, their overall effectiveness cannot be assessed.
1.6.6 Some Nutrients in Food Can Influence the Metabolism of Toxicant
In addition, the levels of various key enzymes necessary for metabolism, transformation, degradation, and excretion of toxins in the body can be disturbed by the availability of nutrients, and these interactions may alter toxicity. For example, cytochrome P450, a member of a heme-thiolate protein superfamily, is involved in the metabolism of endogenous and exogenous substances, including drugs and environmental compounds. It has been shown to act a pivotal part in the metabolism of POPs and N-nitrosamines, and it and flavoproteins are the major enzymes involved in the reduction of exogenous substances in vivo. There is higher oxidoreductase activity in intestinal microflora, which acts a pivotal part in the reduction of xenobiotics [47, 48]. In all, many dietary nutrients including dietary protein, fat, sugar, vitamin C, vitamin E, folate, betaine, iodine, and selenium may alter Cyp450 enzyme levels via various pathways.
References
Kirchmair J, Howlett A, Peironcely JE, Murrell DS, Williamson MJ, et al. How do metabolites differ from their parent molecules and how are they excreted? J Chem Inf Model. 2013;53:354–67.
Goodman BE. Insights into digestion and absorption of major nutrients in humans. Adv Physiol Educ. 2010;34:44–53.
Björck I, Granfeldt Y, Liljeberg H, Tovar J, Asp NG. Food properties affecting the digestion and absorption of carbohydrates. Am J Clin Nutr. 1994;59:699S–705S.
Dick HM, Opperhuizen A. Biotransformation rates of xenobiotic compounds in relation to enzymes activities: a critical review. Toxicol Environ Chem. 1989;23:181–90.
Atashgahi S, Shetty SA, Smidt H, Willem M. Flux, impact, and fate of halogenated xenobiotic compounds in the gut. Front Physiol. 2018;10:1–9.
Gibaldi M, Boyes RN, Feldman S. Influence of first-pass effect on availability of drugs on oral administration. J Pharm Sci. 1971;60:1338–40.
Varma VS, Obach R, Rotter C, Howard R, George C, et al. Physicochemical space for optimum oral bioavailability: contribution of human intestinal absorption and first-pass elimination. J Med Chem. 2010;53:1098–108.
Kuramoto N, Baba K, Gion K, Sugiyama C, Taniura H, Yoneda Y. Xenobiotic response element binding enriched in both nuclear and microsomal fractions of rat cerebellum. J Neurochem. 2003;85:264–73.
Almazroo OA, Miah MK, Venkataramanan R. Drug metabolism in the liver. Clin Liver Dis. 2017;21:1–20.
Iyanagi T. Molecular mechanism of phase I and phase II drug-metabolizing enzymes: implications for detoxification. Int Rev Cytol. 2007;260:35–112.
Ioannides C. Up-regulation of cytochrome P450 and phase II enzymes by xenobiotics in precision-cut tissue slices. Xenobiotica. 2013;43(1):15–28.
Stavropoulou E, Pircalabioru GG, Bezirtzoglou E. The role of cytochromes P450 in infection. Front Immunol. 2018;9:89.
Kolrep F, Rein K, Lampen A, Hessel-Pras S. Metabolism of okadaic acid by NADPH-dependent enzymes present in human or rat liver S9 fractions results in different toxic effects. Toxicol In Vitro. 2017;42:161–70.
Jancova P, Anzenbacher P, Anzenbacherova E. Phase II drug metabolizing enzymes. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2010;154:103–16.
Kedderis GL. Biotransformation of toxicants. Comprehensive. Toxicology. 2010;1:137–51.
Planning Committee for a Workshop on Potential Health Hazards Associated with Consumption of Caffeine in Food and Dietary Supplements, Food and Nutrition Board, Board on Health Sciences Policy, Institute of Medicine. Caffeine in food and dietary supplements: examining safety: workshop summary. Washington, DC: National Academies Press; 2014.
Sadek K, Saleh E. Fasting ameliorates metabolism, immunity, and oxidative stress in carbon tetrachloride-intoxicated rats. Hum Exp Toxicol. 2014;33(12):1277–83.
Rasmussen MK, Bertholdt L, Gudiksen A, Pilegaard H, Knudsen JG. Impact of fasting followed by short-term exposure to interleukin-6 on cytochrome P450 mRNA in mice. Toxicol Lett. 2018;282:93–9.
de Vries EM, Lammers LA, Achterbergh R, Klümpen HJ, Mathot RA, Boelen A, Romijn JA. Fasting-induced changes in hepatic P450 mediated drug metabolism are largely independent of the constitutive androstane receptor CAR. PLoS One. 2016;11(7):e0159552.
Geissler C, Powers H. Human nutrition. 13th ed. Oxford: Oxford University Press; 2017.
Walter-Sack I, Klotz U. Influence of diet and nutritional status on drug metabolism. Clin Pharmacokinet. 1996;31(1):47–64.
Ronis MJ, Rowlands JC, Hakkak R, Badger TM. Inducibility of hepatic CYP1A enzymes by 3-methylcholanthrene and isosafrole differs in male rats fed diets containing casein, soy protein isolate or whey from conception to adulthood. J Nutr. 2001;131(4):1180–8.
Amelizad Z, Narbonne JF, Daubeze M, Bonnamour D, Oesch F. Monooxygenase activity of systems reconstituted with fractions from rats fed standard and low protein diets. Biochem Pharmacol. 1986;35(18):3169–71.
Weatherholtz WM, Campbell TC, Webb RE. Effect of dietary protein levels on the toxicity and metabolism of heptachlor. J Nutr. 1969;98(1):90–4.
Clinton SK, Imrey PB, Alster JM, Simon J, Truex CR, Visek WJ. The combined effects of dietary protein and fat on 7,12-dimethylbenz(a)anthracene-induced breast cancer in rats. J Nutr. 1984;114(7):1213–23.
Tatsuta M, Iishi H, Baba M, Uehara H, Nakaizumi A, Iseki K. Reduction in NaCl-enhanced gastric carcinogenesis in rats fed a high-protein diet. Cancer Lett. 1997;116(2):247–52.
Yamada A, Shimizu N, Hikima T, Takata M, Kobayashi T, Takahashi H. Effect of cholesterol on the interaction of cytochrome P450 substrate drug chlorzoxazone with the phosphatidylcholine bilayer. Biochemistry. 2016;55(28):3888–98.
La Merrill M, Emond C, Kim MJ, Antignac JP, Le Bizec B, Clément K, Birnbaum LS, Barouki R. Toxicological function of adipose tissue: focus on persistent organic pollutants. Environ Health Perspect. 2013;121(2):162–9.
Teel RW, Strother A. Glucose alters rat liver S9-mediated mutagenesis, metabolism and DNA-binding of aflatoxin B1. Cancer Lett. 1990;54(3):163–9.
Mehta RS, Harris SR, Gunnett CA, Bunce OR, Hartle DK. The effects of patterned calorie-restricted diets on mammary tumor incidence and plasma endothelin levels in DMBA-treated rats. Carcinogenesis. 1993;14(8):1693–6.
Manjgaladze M, Chen S, Frame LT, Seng JE, Duffy PH, Feuers RJ, Hart RW, Leakey JE. Effects of caloric restriction on rodent drug and carcinogen metabolizing enzymes: implications for mutagenesis and cancer. Mutat Res. 1993;295(4–6):201–122.
Schwalfenberg GK, Genuis SJ. Vitamin D, essential minerals, and toxic elements: exploring interactions between nutrients and toxicants in clinical medicine. Sci World J. 2015;2015:318595.
Podszun M, Frank J. Vitamin E-drug interactions: molecular basis and clinical relevance. Nutr Res Rev. 2014;27(2):215–31.
Yoo JS, Park HS, Ning SM, Lee MJ, Yang CS. Effects of thiamine deficiency on hepatic cytochromes P450 and drug-metabolizing enzyme activities. Biochem Pharmacol. 1990;39(3):519–25.
McKay RH, Higuchi DA, Winder WW, Fell RD, Brown EB. Tissue effects of iron deficiency in the rat. Biochim Biophys Acta. 1983;757(3):352–8.
Stål P, Johansson I, Ingelman-Sundberg M, Hagen K, Hultcrantz R. Hepatotoxicity induced by iron overload and alcohol. Studies on the role of chelatable iron, cytochrome P450 2E1 and lipid peroxidation. J Hepatol. 1996;25(4):538–46.
Shrimali RK, Irons RD, Carlson BA, Sano Y, Gladyshev VN, Park JM, Hatfield DL. Selenoproteins mediate T cell immunity through an antioxidant mechanism. J Biol Chem. 2008;283(29):20181–5.
Luo H, Yang Y, Duan J, Wu P, Jiang Q, Xu C. PTEN-regulated AKT/FoxO3a/Bim signaling contributes to reactive oxygen species-mediated apoptosis in selenite-treated colorectal cancer cells. Cell Death Dis. 2013;4:e481.
Anticona C, San SM. Anemia and malnutrition in indigenous children and adolescents of the Peruvian Amazon in a context of lead exposure: a cross-sectional study. Glob Health Action. 2014;7:22888.
Olsson IM, Bensryd I, Lundh T, Ottosson H, Skerfving S, Oskarsson A. Cadmium in blood and urine—impact of sex, age, dietary intake, iron status, and former smoking—association of renal effects. Environ Health Perspect. 2002;110(12):1185–90.
Zabik ME, Schemmel R. Dieldrin storage of obese, normal, and semistarved rats. Arch Environ Health. 1973;27(1):25–30.
Spratlen MJ, Gamble MV, Grau-Perez M, Kuo CC, Best LG, Yracheta J, Francesconi K, Goessler W, Mossavar-Rahmani Y, Hall M, Umans JG, Fretts A, Navas-Acien A. Arsenic metabolism and one-carbon metabolism at low-moderate arsenic exposure: evidence from the strong heart study. Food Chem Toxicol. 2017;105:387–97.
Goodrich JM, Dolinoy DC, Sánchez BN, Zhang Z, Meeker JD, Mercado-Garcia A, Solano-González M, Hu H, Téllez-Rojo MM, Peterson KE. Adolescent epigenetic profiles and environmental exposures from early life through peri-adolescence. Environ Epigenet. 2016;2(3):dvw018.
Tian L, Zheng G, Sommar JN, Liang Y, Lundh T, Broberg K, Lei L, Guo W, Li Y, Tan M, Skerfving S, Jin T, Bergdahl IA. Lead concentration in plasma as a biomarker of exposure and risk, and modification of toxicity by δ-aminolevulinic acid dehydratase gene polymorphism. Toxicol Lett. 2013;221(2):102–9.
Horiguchi H, Oguma E, Kayama F. Cadmium induces anemia through interdependent progress of hemolysis, body iron accumulation, and insufficient erythropoietin production in rats. Toxicol Sci. 2011;122(1):198–210.
Kordas K, Stoltzfus RJ, López P, Rico JA, Rosado JL. Iron and zinc supplementation does not improve parent or teacher ratings of behavior in first grade Mexican children exposed to lead. J Pediatr. 2005;147(5):632–9.
Yamamoto FY, Diamante GD, Santana MS, Santos DR, Bombardeli R, Martins CC, Oliveira Ribeiro CA, Schlenk D. Alterations of cytochrome P450 and the occurrence of persistent organic pollutants in tilapia caged in the reservoirs of the Iguaçu River. Environ Pollut. 2018;240:670–82.
Sasaki S, Sata F, Katoh S, Saijo Y, Nakajima S, Washino N, Konishi K, Ban S, Ishizuka M, Kishi R. Adverse birth outcomes associated with maternal smoking and polymorphisms in the N-nitrosamine-metabolizing enzyme genes NQO1 and CYP2E1. Am J Epidemiol. 2008;167(6):719–26.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Zhao, Y., Zhang, L., Shen, J., Ma, L., Wang, L. (2022). Effects of Nutrients/Nutrition on Toxicants/Toxicity. In: Zhang, L. (eds) Nutritional Toxicology. Springer, Singapore. https://doi.org/10.1007/978-981-19-0872-9_1
Download citation
DOI: https://doi.org/10.1007/978-981-19-0872-9_1
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-19-0870-5
Online ISBN: 978-981-19-0872-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)