
Abstract
Pentastomiasis is a zoonotic endoparasite with controversies looming over the taxonomy, nomenclature, diagnosis and treatment. Causative pentastomes are a group of obligate parasites maintained naturally among the reptiles and the rodents. Armillifer armillatus and Linguatula serrata are the commonest pentastomes infecting humans. The infection although is mostly asymptomatic and a self-limiting, acute infections and emergencies need timely intervention. Ecotourism with interests in snake farming, tribal delicacies, undercooked meat consumption and wild-life adventures are the current facilitators of the zoonosis. Neither a vaccine nor a validated medicine exists for the disease. Controlling the pentastomes is difficult due to an efficient parasitic lifestyle with an extensive natural distribution.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
FormalPara Learning Objectives-
1.
To review the clinical presentation of pentastomiasis and misdiagnosis with tuberculosis or malignancy.
-
2.
To understand the critical role played by microscopy in its diagnosis.
Introduction
Pentastomiasis is an often forgotten zoonotic infection caused by the pentastomes, a peculiar group of vermiform endoparasites. An annulated elongate body or tongue-like shape distinctly characterizes these unique ‘tongue worms ’. A single mouth flanked by two pairs of hooks initially generated the misimpression of five mouths naming as pentastome. Armillifer armillatus and Linguatula serrata are the causative agents in more than 90% of infection in humans. Largely, being asymptomatic and self-limited, opportunities to diagnose and treat the condition are restricted.
History
Pentastomes possibly parasitized the carnivorous dinosaurs in the Mesozoic times. Chabert, a French veterinary surgeon, first observed the parasite in 1787 in the nasal cavity of dogs, possibly Linguatula sp., but thought of a tapeworm. In 1845, Wyman first reported A. armillatus from western Africa and identified the adult pentastome in the nasopharynx of an African rock python within the next 3 years. However, Pruner (1847) in the meantime reported the first human pentastomiasis case from Cairo, Egypt. Stiles (1891) prioritized the name ‘Porocephalus’.
Taxonomy
Hesitancy to place the pentastomes under Annelida or Arthropoda is persisting. The advent of molecular techniques points their relative closeness to the crustacean arthropods, but most authorities prefer to retain them under a unique minor phylum Pentastomida. Inclusion in a more comprehensive phylum Lobopodia is under consideration.
The present taxonomical status for the common pentastomes infecting humans belongs to families Porocephalidae and Linguatulidae in the order Porocephalida; class Pentastomata; and phylum Pentastomida.
Linguatulidae family includes the genus Linguatula containing the medically important species Linguatula serrata. Porocephalidae family consists of numerous members with Armillifer genus being the commonest. Order, Cephalobaenida, contains primitive pentastomes affecting lizards and snakes. The species, among the pentastomes infecting humans, are Linguatula serrata, Armillifer armillatus, Armillifer moniliformis, Armillifer grandis, Armillifer agkistrodontis, Porocephalus crotali, Porocephalus taiwana and Sebakia sp. Reports of human infections by Leiperia cincinnalis, Railietiella hemidactyli and Railietiella gehyrae are also present.
Genomics and Proteomics
Mitochondrial genome sequencing of A. armillatus shows similarity to metazoan traits including 37 genes. Gene rearrangements suggest its inclusion within the phylum Arthropoda. However, studies suggest that the pentastomes might be closer to the nematodes than the arthropods. A. agkistrodontis has a complete mitochondrial transcript of length 16,521 bp containing 13 protein-coding genes (PCGs), 22 tRNA genes and 2 rRNA genes. The same number of PCGs, tRNA and rRNA prevails in A. grandis and L. serrata mitochondrial DNA with smaller genome lengths (16,073 bp and 15,328 bp, respectively). All pentastomes show an inherent A + T bias in their mitochondrial genomes. Genomic studies have been refining the much-debated taxonomical status of the pentastomes. It provides important genetic markers for the epidemiological studies too.
Proteomic studies are important for providing useful insights into the pathogenesis of pentastomiasis. However, studies are lacking in this aspect. Two proteins from A. armillatus, namely a serine endopeptidase and a G-protein-coupled receptor kinase, are under research. A 48 kDa metalloproteinase from the frontal glands is used for diagnostic purpose.
The Parasite Morphology
Adult Worm
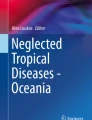
Pentastomes have elongated cylindrical or flat tongue-like bodies divided into a short cephalothorax and a long abdomen (Fig. 1). Males are shorter than the females. Length varies from few mm to 15 cm. The cephalothorax contains a mouth with two pairs of chitin hooks. The non-segmented abdomen has encircling pseudoannulations in A. armillatus (18–22), A. moniliformis (around 30), A. agkistrodontis (7–9) and A. grandis (more than 25). A straight tube of primitive digestive system is flanked by paired frontal glands. An extensive reproductive system and the absence of respiratory and circulatory systems are the characteristic features of the worm. The genital pore in the female is located anteriorly in family Cephalobaenida and at the posterior end in family Porocephalida.

Schematic diagram of adult Armillifer armillatus adult
Eggs
Eggs are ovoid (105 μm × 125 μm), double-shelled containing a mite-like embryo when deposited.
Larvae
The first-stage larva (L1) has rudimentary appendages that are lost subsequently upon moulting (Fig. 2). The third-stage larva (L3) or the nymph has hooks and morphology akin to the adult in a miniature form. Apart from L. serrata, which has spines, all pentastome larvae have smooth cuticle. The 5- to 10-μm thick cuticle contains numerous sclerotized openings. Sebaceous glands and muscle fibres, both circular and longitudinal, lie under the cuticle. Armillifer sp. (L3) larvae are 9–23 mm long, cylindrical with spiral rings. L. serrata (L3) larvae are 4–6 mm long, flat, annulated with a row of spines on each annulus.

Schematic diagram of a pentastome larva
Cultivation of Parasites
In vitro culture has not been successful for pentastomes. Experimentally, P. crotali eggs withstood desiccation for 2 weeks and survived 6 months in water. Development requires an appropriate living host.
Laboratory Animals
Hamsters serve as experimental paratenic hosts. Recently, a multi-host model has been developed for A. agkistrodontis. This type of model helps in understanding the pathogenesis and the transmission. The model uses snakes as the definitive hosts and rodents as intermediate hosts.
Life Cycle of Pentastomes
Hosts
Definitive Hosts
Snakes are the definitive hosts for Armillifer sp. and Porocephalus sp. , while dogs and wolves are the hosts for Linguatula sp.
Intermediate Hosts
Various rodents and monkeys act as the intermediate hosts for Armillifer sp. and Porocephalus sp. Ruminants like sheep and goat serve as intermediate hosts for Linguatula spp.
Humans act as an aberrant intermediate host, rarely aberrant/accidental definitive host for L. serrata.
Infective Stage
Third-stage larvae are the infective stage for the definitive hosts, while embryonated eggs are infective for the intermediate hosts.
Transmission of Infection
Definitive host acquires infection by ingestion of the third-stage larvae in infected rodent tissue (or herbivore tissue, for Linguatula sp.). Intermediate hosts, including humans, acquire infection by ingestion of eggs from food and water contaminated with snake droppings (Fig. 3).

Life cycle of a pentastome
The reptiles carry the adults in their respiratory passage. Mating takes place 3–4 months after infection. The fertilized female deposits embryonated eggs in the snake’s oral cavity after 4–8 months, which are discharged outside or passed in the faeces. An intermediate host such as rodent ingests egg through water or vegetations. Inside the rodents, the first-stage larva (L1) hatches out in the intestine and penetrates the gut wall to enter the peritoneum or spread haematogenously. It loses appendages and encysts in the internal organs to transform into the infective third-stage larva (L3) after moultings. A definitive host eats the rodent tissue to release the larvae in the stomach. The L3 larvae then actively migrate to the lungs, mature and reinitiate the life cycle. In aberrant intermediate hosts such as humans, the larvae distribute in various organs and peritoneum but die within 2 years, disrupting the cycle.
In L. serrata, carnivore mammals carry the adult pentastomes in their nasal passages. After the embryonated eggs are deposited on grass and vegetations, the herbivores (sheep, goat) take up with similar events following. In place of carnivores, if a human being takes up the infected herbivore tissue the infective larvae migrate to the throat to provoke halzoun or marrara syndrome . Rarely, L. serrata larvae develop into adults in humans.
Pathogenesis and Pathology
In the definitive hosts, adult pentastomes do not provoke significant tissue reactions. In the intermediate hosts, varied tissue reactions occur but of mild degree, probably due to the immunomodulatory action of the excretory/secretory proteins coating the cuticle. Humans ingest the pentastome eggs through food and water contaminated with snake droppings, handling and consumption of contaminated snake products such as meat and bile. The eggs hatch to release the first-stage larvae, which penetrate the gut wall with stylet, aided by the frontal gland enzymes and enter abdomen to encyst in the peritoneum and other viscera. Typically, a thin-walled cyst encases a single larva. With moulting, the larva grows larger in size, nearly 1000-fold and the cuticle merges with the cyst wall preserving the sclerotized openings and spines of L. serrata. This increased volume creates pressure effects on the adjacent viscera. In a couple of years, the larvae die with granuloma formation in a few cases, particularly in humans acting as an aberrant definitive host. A hyalinized calcified nodule is the final stage of an encysted pentastome.
The exact cause of death of the parasite in the infected host is unknown. Depending upon the stage, three patterns emerge during biopsy/autopsy: (a) necrotic pentastomida granuloma occurs commonly. This reveals a disintegrated parasite into amorphous and calcified debris preserving a C-shape and the perioral hooks. (b) The presence of a viable larva occurs in recent infection; and c) least commonly, the occurrences of a cuticle granuloma. It consists of the cuticular remnants shed during a migrating larva appearing as refractile structures stained by periodic acid–Schiff.
In visceral linguatuliasis, pearly protuberant nodules of size smaller than 1 cm are seen over the peritoneum, pleura and under the capsules of liver and spleen. These ‘Linguatula bodies ’ are probably a larva migrans effect due to the migration of the larvae. Different mechanisms act in halzoun/marrara syndrome where the humans act as aberrant definitive hosts for L. serrata. The migrating larvae create mechanical and hypersensitive events resulting in violent cough, asphyxia and congestive oedema of the gum, tonsils and the Eustachian tubes.
Immunology
The pentastomes behave like a true parasite by escaping from or downregulating the host immune responses. The encystment of the larva and frontal gland secretions coating the cuticle possibly hinder exposure of the antigenic epitopes to the host immune system. The literature in immunological experiment in human infection is scarce. However, autopsy studies indicate granulomatous tissue response with foreign body giant cells can occur after the parasite disintegrates. A possibility of delayed hypersensitivity exists. The death of larvae in humans could be due to an immune response; nevertheless, a scientific explanation is lacking.
Infection in Humans
Visceral pentastomiasis and nasopharyngeal pentastomiasis are two forms of pentastomiasis in humans.
Visceral pentastomiasis, acquired by ingestion of pentastome eggs, is usually asymptomatic. In symptomatic infections, the condition has protean manifestations. Peritonitis, pneumonitis, lung collapse, meningitis, nephritis and pericarditis have been documented. The condition involving the eye causes iritis, subluxation of the lens, secondary glaucoma, conjunctivitis and lacrimal canaliculitis. Rarely, the condition may present with acute or chronic non-specific abdominal symptoms.
The nasopharyngeal pentastomiasis is caused by ingestion of the nymph of L. serrata. The larvae travel to the nasopharynx to induce paroxysmal cough, discomfort in nose and throat, sneezing, dysphagia and vomiting. Asphyxia, Eustachian tube congestion and aural pruritus may also occur.
Cases of creeping subcutaneous human infection with R. hemidactyli have been reported in the Southeast Asian tribes who eat live lizards as a folk remedy for respiratory disease. A pruritic serpiginous burrow over a patient’s abdomen, caused by Sebakia sp., has been reported.
Infection in Animals
Visceral linguatulosis caused by Linguatula sp. occurs in sheep, cattle and rodents. Usually, animal infection is asymptomatic. Diarrhoea, reluctance to eat or stand and gradual emaciation, occurs in symptomatic infections. Adult Linguatula worms appear in the tongue, nasal passage, frontal sinus and tympanic cavities of dogs. True autoinfection also occurs in snakes.
Epidemiology and Public Health
The majority of human infections are caused primarily by A. armillatus and distributed mainly in the West and Central Africa (Table 1). A. armillatus infection in African immigrants in America and Europe has been documented. A. moniliformis is the commonest isolate from human cases in Malaysia. A. grandis caused a large series of human ocular infections from the Sankuru district of the Democratic Republic of Congo. P. crotali cases have been reported mainly from the Americas though they occur worldwide. Pentastomiasis due to Sebakia sp. has been reported from Costa Rica.
However, a precise estimate of prevalence is unattainable owing to the asymptomatic and self-limiting nature of the disease. Wide discordances among the prevalence rates obtained by serological, radiological and post-mortem surveys have been noted. Radiological prevalence rates in Nigeria and Congo are much lower than the seroprevalence statistics at Ivory Coast (less than 1.5% versus 4.2%). On the other hand, autopsy series pop up with much higher prevalence ranging between 22.5% (in Congo) and 33% (in Nigeria). A high prevalence rate of 45.5% was observed in West Malaysia from consecutive 30 autopsies on aborigines. Autopsy prevalence statistics from Cameroon also range between 7.8 and 12.6%. These differences reflect possibly the failure of imaging methods to detect non-calcified nymphs and low sensitivity of the serological tools compared to the large scope of detection by the autopsy.
Canine infection with Linguatula sp. has numerous public health implications. Prevalence among the canine population from Nigeria is more than 35%. A study of the slaughtered dogs from the dog markets in Nigeria demonstrated a high prevalence of 48.26% with the puppies being affected the most (55.45%). The people in impoverished rural and semi-urban areas commonly consume dog viscera propagating the disease.
Snakes, especially their meat and the bile, have been in use for animalistic rituals and medicinal purpose. Tropical snake farming, python totemism and a shift from the bushmeat to the reptile meat create an economy-driven transmission opportunity. China reports very few cases of pentastomiasis mostly caused by Porocephalus taiwana and Armillifer agkistrodontis . A. moniliformis has also been detected in Cynomolgus monkeys, cockroaches and wild rats. The house geckos and lizards have been shown to harbour Railietiella sp. The estimated prevalence rate varies from 1.8% to 20.7% in Malaysian wild animals.
Diagnosis
Various diagnostic methods are available for diagnosis of pentastomiasis (Table 2).
Microscopy
Histopathology is frequently helpful. Characteristic sclerotized cuticular openings are often demonstrated in the tissue sections stained by haematoxylin and eosin. Movat’s pentachrome stain of the tissue section appears to be better. The presence of the cuticular spines distinguishes L. serrata larvae from Armillifer sp. The presence of the striated muscle fibres differentiates these from those of cysticercus, spargana and nematodes but not from the fly larva. The latter is distinct by the presence of the tracheal tracts and no cuticular sclerotized opening.
Microscopy of an intact larva, if available, is highly useful for species identification of the pentastome. A lower number (7–9) of annulations suggests A. agkistrodontis, whereas relatively large numbers of (18–22) annulations suggest A. armillatus. Positions of the genital pore and annulations are helpful features in diagnosing adult worms.
Serodiagnosis
Various antibody-based tests such as gel diffusion, immunoelectrophoresis, immunofluorescence, ELISA and Western blot are used in serodiagnosis of pentastomiasis both in humans and in animals. Most of these tests use a crude antigen from canine omentum containing pentastome larvae. An ELISA method using a 48 kDa frontal gland metalloproteinase has shown increased efficacy. The 97 kDa and 37 kDa bands on Western blot with L. serrata help in diagnosis.
In animals, a sandwich ELISA for detecting antibodies against excretory/secretory antigens of L. serrata showed excellent sensitivity compared to microscopy in animals.
Antigen-based methods are yet to be evaluated.
Molecular Diagnosis
Polymerase chain reaction (PCR) and DNA sequencing have been highly useful for molecular diagnosis. The tests differentiate A. agkistrodontis, A. armillatus and few other species confidently. BLAST analysis following the sequencing of a 424 bp amplicon is the usual procedure. However, high cost and limited access prohibit their routine use. Necrosis and formalin fixation of tissue hamper nucleic acid detection by PCR.
Other Methods
Crescentic or coiled opacities on lung radiology (Fig. 4), liver imaging (Fig. 5) or discovery during laparotomy or autopsy are frequently used methods in the diagnosis of the condition.

Chest radiograph showing multiple tiny C-shaped opacities in the lungs in a visceral pentastomiasis case (image reproduced from BJR Case Rep 2019; 5: 20180058; CC by 4.0)

Multifocal calcification in the liver and spleen in a visceral pentastomiasis case (image reproduced from BJR Case Rep 2019; 5: 20180058; CC by 4.0)
Treatment
The asymptomatic nature and eventual death of the parasite limit the opportunity and requirement of treatment in human visceral pentastomiasis.
Acute abdominal cases in human visceral pentastomiasis are treated by exploratory laparotomy and peritoneal lavage to diagnose and remove the larvae. In a few cases, as many as 100 A. armillatus nymphs were removed by laparotomy. Halzoun/marrara syndrome requires surgical removal of free or encysted parasites in eye, throat or nasal passage.
No validated medical treatment is available for visceral pentastomiasis. Medical therapy aims to kill and remove dead worm excreted out in the stool. Monotherapy and combination therapy with praziquantel, albendazole and mebendazole have been in practice along with Chinese traditional medicines. Diethylcarbamazine has been suggested for the treatment of infections by Linguatula sp. Associated allergic manifestations respond to therapy by antihistaminic and/or corticosteroids. Ivermectin has shown some curative effects in pentastome infections in animals such as snakes and captive lizards.
Prevention and Control
Since snake dropping and contaminated food and water are important sources of infection, food and water hygiene is necessary to prevent the infection. Cautious and hygienic handling of contaminated snake products such as their muscle and bile and avoiding their consumption are essential preventive measures. Avoidance of eating uncooked meat (dog, rodent and sheep) and avoidance of contact with infected reptiles needs are important personal preventive measures. Screening of canine population helps in controlling Linguatula sp. infection in these animals.
Further Readings
Flood R, Karteszi H. Incidental thoracic, hepatic and peritoneal calcifications: a case of pentastomiasis. BJR Case Rep. 2019;5:20180058.
Meyers, W. et al. Topics on the pathology of protozoan and invasive arthropod diseases. (2011).
Muller R. Worms and human diseases. In: Commonwealth Agricultural Bureaux. 2nd ed. Walling Ford: CABI; 2002. p. 240–2.
Ogbu K, Tion M, Ochai S, Olaolu O, Ajegena I. Prevalence of tongue worm (Linguatula serrata) in dogs slaughtered in Jos-south local government area of plateau state. Nigeria South Asian J Parasitol. 2018;1(3):1–7.
Tappe D, Büttner D. Diagnosis of human visceral pentastomiasis. PLoS Negl Trop Dis. 2009;3(2):e320.
Tappe D, Meyer M, Oesterlein A, Jaye A, Frosch M, Schoen C. Transmission of Armillifer armillatus ova at Snake farm, the Gambia. West Afr Emerg Infect Dis. 2011;17(2):251–4.
Tappe D, Sulyok M, Rózsa L, Muntau B, Haeupler A, Bodó I, Hardi R. Molecular diagnosis of abdominal Armillifer grandis pentastomiasis in the Democratic Republic of Congo. J Clin Microbiol. 2015;53:2362–4.
Vanhecke C, Le-Gall P, Le Breton M, Malvy D. Human pentastomiasis in sub-Saharan Africa. Med Mal Infect. 2016;46:269–75.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Case Study
Case Study
A 50-year-old man comes to you with acute abdominal pain and vomiting. He was having constipation for the last 7 days. He is a professional snake hunter and avidly takes folk medicines. Clinical examination shows marked epigastric tenderness. You ordered a straight X-ray abdomen, which surprisingly showed numerous tiny C-shaped opacities in the abdomen with a collection of gas under the diaphragm. You decided for an emergency laparotomy.
-
1.
What could be those opacities?
-
2.
Are the opacities causing the problem in this patient?
-
3.
What could be the possible findings during this laparotomy?
-
4.
How would you proceed further?
Research Questions
-
1.
What is the mechanism of the pentastome larval death in humans?
-
2.
What are the immunological aspects of pentastomiasis particularly the immune evasion strategies and the indiscernible host response?
-
3.
What should be the therapeutic approach need elucidation in relation to one health concept?
Rights and permissions
Copyright information
© 2022 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Maiti, S. (2022). Pentastomiasis. In: Parija, S.C., Chaudhury, A. (eds) Textbook of Parasitic Zoonoses. Microbial Zoonoses. Springer, Singapore. https://doi.org/10.1007/978-981-16-7204-0_58
Download citation
DOI: https://doi.org/10.1007/978-981-16-7204-0_58
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-7203-3
Online ISBN: 978-981-16-7204-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)