
Abstract
Atmospheric aerosols, soon after their emission, may experience changes in its chemical composition, mass concentration, size, and its optical properties. These changes are dynamic in nature and occur over a short period of time. Since aerosols play a critical role in human health effects, cloud microphysics, hydrological cycle and climate perturbations, it is therefore of paramount importance to understand both qualitatively and quantitatively all the major changes, which an ambient particle could experience during its residence time in the atmosphere. High-resolution measurements (i.e. real-time measurements) are being carried out worldwide to capture any high-frequency changes in aerosol characteristics. In this study, we discuss the observations based on an open-access high-resolution data set retrieved from the Central Pollution Control Board (CPCB) for a location in central capital Delhi. Along with the particulate matter (PM) data, we also discuss some of the gaseous species owing to the reason that these gases influence the aerosol behaviour and its budget due to coating and secondary aerosol formation. The source strengths are highly variable (in both space and time) in Indo-Gangetic Plain (IGP) mainly due to industrial activities and seasonal influence of biofuels and biomass burning emission. This chapter presents a case study highlighting some of the important observations on temporal variability and processes from high-resolution atmospheric data set of aerosols and reactive gases. We also present here a review on the health effects of outdoor and indoor aerosol pollution.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
5.1 Introduction
Air pollution is the presence of any substance in the air at such concentrations, which are detrimental not only to the human beings, flora and fauna but also to the several components of the environment (Chakraborty et al. 2017; Choudhary et al. 2018). Air pollution is one of the major causes for degradation of environment (Yadav and Rajamani 2004). It occurs either from natural sources like volcanic eruptions, forest fires, sea spray, wind blown dust and pollen grains or can be as a result of various anthropogenic (human) activities like agricultural waste burning, vehicular emissions, power plants, and industrial emissions (Fig. 5.1). Air pollutants usually exist as tiny solid and liquid (e.g. dust, oil droplets and particulate matter), gases (e.g. NOx, SO2 and O3) and semi-volatile species [e.g. PAHs: polycyclic aromatic hydrocarbons] (Rajput et al. 2014b). It has been widely realized that air pollution has emerged not only as a local problem but also as a regional and a global problem (Izhar et al. 2018). Air pollution is widely being understood as one of the biggest environmental health risk factors of this century (Dockery et al. 1993; Rajput et al. 2014a; Schwartz 1995). Anthropogenic activities such as rapid industrialization, unrestricted population growth and increasing urbanization contribute increasingly to elevated emission rates of various air pollutants—among these, specifically higher levels of particulate matter (PM10 and PM2.5), sulphur dioxide (SO2), nitrogen oxides (NOX), carbon monoxide (CO) and ozone (O3)—leading to not only the degradation of the environment and climate change but also having a debilitating effect on human health (Dey et al. 2012; Pant et al. 2016). Simultaneously, over two-thirds of rural Indians caught in the ‘chulha trap’ use biomass fuels such as wood, twigs and dung cake to meet their cooking and heating needs, resulting in smoke-filled homes causing extremely high levels of exposure to the residents. Air pollution is especially severe in many developing parts of the world, which also happen to be very fast-growing urban regions contributing higher levels of pollution and are therefore subject to higher exposure. According to the World Health Organization’s (WHO) figures, 97% of the cities in the low- and middle-income countries (LMICs), which have more than 100,000 inhabitants, do not meet WHO air quality guidelines (WHO 2018a). In the year 2016, ambient air pollution is estimated to have caused 4.2 million premature deaths worldwide, of which 91% occurred in LMICs (WHO 2016).

The atmospheric aerosol (aka particulate matter) ranges from 0.001 to 100 μm in aerodynamic diameter. Having various sources of origin and different chemical composition, they are an intricate combination of small and big particles (Kumar et al. 2017). They can mainly be sub-divided into two parts: primary and secondary. Primary aerosols are those that are directly produced and emitted into the atmosphere from identifiable sources like vehicles, industries, desert areas, construction activities, fossil fuel combustions, and road dust. They consist of black carbon (BC), crustal elements and organic compounds of high molecular mass released from combustion sources, etc. (Sorathia et al. 2018). Secondary organic aerosols (SOA) are those that form when condensation of volatile organic compound (VOC) oxidation products takes place (Rajput et al. 2013; Seinfeld and Pankow 2003). Secondary/aged aerosols are either organic or inorganic that affects the physicochemical properties of the aerosols (Rajput et al. 2018a, b). Once produced, they grow to different sizes and can have different composition due to several physical and chemical modifications like coagulation, polymerization, photolysis, structural reorganization, and phase alteration and these processes are defined as atmospheric ageing (Fuzzi et al. 2006). SIAs (secondary inorganic aerosols) are formed from the chemical reactivity of gases like SO2, and NO2 and NO (collectively known as NOX) leading to the formation of particulate sulphate and nitrate (Rajput et al. 2016). A recent study (Rajput and Gupta 2020), through causal modelling, has shown that for every 10-unit change in O3 concentrations the SOA formation increases by ~3.2% during daytime under prevailing long-range transport of biomass burning emissions from upwind IGP. Overall, the main composition of an atmospheric aerosols includes crustal matter (mineral dust); sea salt which includes sulphate, magnesium, sodium and chloride; secondary particles like nitrate, sulphate and ammonium; trace metals like vanadium, chromium and lead; and carbonaceous material which includes both elemental and organic carbon and liquid water content (Senfield and Pandis 2006).
Also, depending upon the size of the particles, aerosols are classified into various categories. TSPs (total suspended particulate matters) are those whose aerodynamic diameter (d) is ≤100 μm (aerodynamic diameter of a particle is the diameter of a unit density sphere) (ρ = 1 g/cm3) having the same terminal velocity as the particle of interest (Senfield and Pandis 2006), PM10 (coarse mode) whose aerodynamic diameter (d) is ≤10 μm and PM2.5 (fine fraction) whose aerodynamic diameter is ≤2.5 μm. The fine fraction particles are further classified into nucleation mode (d ≤ 0.01 μm), Aitken mode (0.01 < d < 0.1 μm) and accumulation mode (0.1 < d < 1 μm) (Raes et al. 2000). Coarse mode particles are formed from various mechanical processes like wind-blown dust, sea salt spray, cement dust, milled flour and pollen, but the fine particles are mainly formed from the various combustion processes (causing formation of black carbon, smoke, etc.) and condensation processes or secondary conversion of gases into the particulates (Rajput et al. 2016).
Aerosols influence the quality of life by affecting health, visibility and the environment at a very profound level (Posfai and Buseck 2010). Various epidemiological studies show that the mortality and morbidity rate in human beings increases with increase in the concentration of aerosols, especially correlated with the fine fraction particles (Geller et al. 2002; Srivastava and Jain 2007; Dockery and Brunekreef 1996; Peters et al. 2000; Neas et al. 1999; Schwartz 1995; Korrick et al. 1998). Among those most affected are the women, children, senior citizens, and the subjects with respiratory illness.
Aerosols play an important role in the climatic system of the Earth and the biogeochemical cycle of oceans (Mahowald et al. 2005). Aerosols affect directly the Earth’s atmospheric radiative balance by scattering and absorbing incoming solar radiations, resulting in warming or cooling of the atmosphere. For instance, black carbon absorbs solar radiation and makes the global climate warm (Ramanathan and Carmichael 2008) and organic aerosols (net effect) scatter light, which led to reduction in incoming solar energy (Rudich 2003). Aerosols affect the climate indirectly by acting as CCN (cloud condensation nuclei) and IC (ice nuclei), i.e. act as nuclei for the condensation of water vapour and ice crystal (Novakov and Penner 1993; Spracklen et al. 2011). Indeed, if there were not any atmospheric aerosols, clouds would not be formed and would have resulted in no precipitation. Due to the increase in anthropogenic activities, burden on global mean aerosol concentration has changed considerably (Rajput et al. 2011). In order to enumerate these effects in a better way, a very good understanding of the formation, composition and transformation of aerosols is desired. Dry and wet scavenging processes are the two main removal pathways of aerosols from the atmosphere. Generally, the larger particles with d > 1 μm are removed by gravitational settling, but this process becomes less efficient as the particle size reduces. Particles with d < 1 μm can be removed efficiently by the wet deposition (Rajeev et al. 2016).
Worldwide research on exposure assessment of ultrafine and fine particles has suggested severe human health impacts due to inhalation (Nazarenko et al. 2014; Singh and Gupta 2016; Asbach et al. 2017; Dandona et al. 2017). A near-continuous assessment on morbidity and mortality from major diseases, injuries and risk factors is being carried out through Global Burden of Disease (GBD) research programme (GBD 2015). GBD estimates (Fig. 5.2) suggest that number of mortalities in India is rising year by year due to COPD, asthma, TBL cancer and whooping cough, among others.

Integrating the data set on mortality (Fig. 5.2), it has been inferred that death of about one million people (including both male and female subjects) in 2013 year (in India) was caused due to respiratory diseases. Furthermore, decadal monitoring of GBD data set suggests that premature mortality of males is more pronounced due to COPD and TBL cancer (among the respiratory diseases), whereas higher deaths of females were found due to asthma and whooping cough (Fig. 5.2). One of the plausible reasons suggested for observing higher mortality due to asthma and whooping cough in females relate to the fact that most of the Indian women are housewives and are therefore exposed for prolonged period to indoor air pollution and fresh emissions from biofuels as compared to the men (Parikh et al. 2001; Padhi et al. 2017).
5.2 Air Quality Guidelines
The air quality guidelines recommended by different organizations viz. World Health Organization (WHO), European Union (EU) and Indian region are listed in Table 5.1.
Air pollution kills an estimated seven million people worldwide every year. WHO data show that 9 out of 10 people breathe air containing high levels of pollutants. WHO is working with many countries to monitor air pollution and improve air quality. From smog hanging over cities to smoke inside the home, air pollution poses a major threat to health and climate. The combined effects of ambient (outdoor) and household air pollution cause about seven million premature deaths every year, largely as a result of increased mortality from stroke, heart disease, chronic obstructive pulmonary disease, lung cancer and acute respiratory infections. More than 80% of people living in urban areas are exposed to air quality levels that exceed WHO guideline limits, with low- and middle-income countries (LMICs) suffering from the highest exposures, in both indoors and outdoors.
5.3 Methodology
5.3.1 Air Pollution Monitoring in Delhi
Indian region, especially northern part, has experienced daunting challenges due to air pollution—according to several researchers, it kills every year more than one million in the country (Chatterjee 2019; Rajput et al. 2019). Many cities in India have exceeded over 5 times of the PM2.5 level recommended by the WHO guidelines. Fine particulates (PM2.5), comprising primarily of mineral dust, secondary aerosols and combustion products, are ~20 times smaller than a human hair, and they cause stroke, heart disease, chronic obstructive pulmonary disease, and lung cancer (WHO 2016, 2018b). In total, 90% of the world’s population breathe harmful air (https://news.un.org/en/story/2018/05/1008732). A global scenario on air pollution led mortality from various countries is shown in Fig. 5.3.

A global scenario on air pollution caused mortality data from various countries (https://www.statista.com/chart/13575/deaths-from-air-pollution-worldwide/)
India is making some progress in this area. The National Clean Air Programme aims to reduce air pollution levels by up to 30% by 2024. The country is also planning what it calls the world’s largest expansion of renewable energy by 2022.
A recent ‘world air quality report’, published by AirVisual (2018), has reported a list of 20 most polluted cities in South Asia, and 16 of these are cities in India (Fig. 5.4). Delhi is the capital of India, and it is one of the most polluted cities in the world.

Regional scenario of air pollution (annual average PM2.5 in year 2018) in Delhi and nearby cities in India and in neighbouring countries. Source: AirVisual (2018)
The heterogeneity in PM2.5 levels and other gaseous pollutants is dependent on the location (Zikova et al. 2017). Many previous studies have been carried out to investigate the air pollution over Delhi through offline measurements. Since 2017, CPCB initiated continuous ambient air quality monitoring measuring air quality on a near-real time to hourly time interval resolution. The best part of these measurements by CPCB is that the data set is open source. The regulatory bodies and public organizations have deployed a series of instruments based on the federal reference method (FRM) and federal equivalent method (FEM) for an accurate and reliable air quality measurements in Delhi (DPCC 2017). A total of 26 Continuous Ambient Air Quality Monitoring Stations (CAAQMS) have been set up to help improve air quality data sets and assess the spatiotemporal variabilities in the abundance of pollutants and their source contributions (http://www.dpccairdata.com).
This chapter also embodies observations and discussions on the variability, effects and the understanding of criteria air pollutants. This work on detailed characterization of the air masses in Delhi documents on the following: (1) temporal variability of air pollutants on an hourly, weekly and seasonally basis; (2) abundance of primary and secondary pollutants and their relative abundances; and (3) application of conditional probability function (CPF) and potential source contribution function (PSCF) to look into the new insights of air pollution over Delhi.
5.3.2 Study Site
To assess the ambient air quality in urban area of Delhi, the Mandir Marg (MM) site was selected (Fig. 5.5).

Air quality data set in this work have been retrieved from CAAQM station (i.e. Mandir Marg: MM). Source: Real-Time Ambient Air Quality Data of Delhi (DPCC)
MM is situated in the central part of Delhi, and it is 200 m away from the ring road, and the site has an influence from local emissions such as light duty/heavy duty vehicle activities. At MM site, a real-time beta-attenuation monitor (BAM, Ecotech, AECOM Group, Australia) and gases monitor (Ecotech, AECOM Group, Australia) are installed by the CPCB for measuring criterion pollutants.
5.3.3 Data Source and Study Period
The hourly concentrations of particulate matter (PM2.5 and PM10) and other pollutants along with the meteorological parameters (wind speed, wind direction, temperature, and relative humidity) were obtained from the CPCB online portal for air quality data dissemination (https://app.cpcbccr.com/ccr/#/caaqm-dashboard-all/caaqm-landing). In this study, concentrations of these pollutants were analysed for the time period of 1 year from 01 January 2018 to 31 December 2018.
5.3.4 CBPF Analysis
In order to identify the local sources of pollutants, the conditional bivariate probability function (CBPF) analysis was performed. The CBPF was calculated using air pollutants by coupling of conditional probability function (CPF) with wind speed as a third variable, distributing, measured pollutant concentration to range of wind sector bins. CBPF is defined as follows:
where mΔθ, Δu ↓ c ≥ X is the number of samples while wind is blowing in the wind sector ‘Δθ’ with wind speed interval ‘Δu’ having concentration ‘c’ greater than a threshold value, ‘X’; and nΔθ, Δu is the total number of samples observed in that wind direction for a given speed interval. The threshold criterion was chosen at the 50th or 75th percentile of pollutant concentration. CBPF analysis was performed by openair R package (Carslaw and Ropkins 2012) in R-studio (version 3.1.1; R Core Team, 2014) statistical software. More details about the method are described in Uria-Tellaetxe and Carslaw (2014).
5.3.5 PSCF Analysis
Air mass backward trajectories (AMBTs) were retrieved for each day at intervals of 3 h for the duration of 120 h during the study period in year 2018 using National Oceanic and Atmospheric Administration (NOAA) Air Resources Laboratory (ARL) Hybrid Single Particle Lagrangian Integrated Trajectory (HYSPLIT) model (Rolph et al. 2017). The spatial resolution of the data is 1° × 1°, and the arrival heights of AMBTs were 500 m above the ground level. In this study, openair package in R has been utilized to download back trajectories. The functions and codes for downloading the monthly meteorological file from HYSPLIT PC model and merging every 3-h back trajectory end-point files (e.g. at MM site in this study) are discussed in openair R package manual. Furthermore, the potential source contribution function (PSCF) was also performed using the openair R package (Carslaw and Ropkins 2012).
5.3.6 Results and Discussion
Figure 5.6 shows the time-series plots (hourly variation) of PM10, PM2.5, CO, NO2, NO, and SO2 over the entire study period. The relevance of discussing here some of the gaseous species lies in the fact that they are connected with the emission source of PM and/or contribute to its burden through chemical reactivity (of these gases) and formation of secondary aerosols. The high concentrations of PM10 were observed in various episodes with frequent peaks in summer (March, April, May, and June 2018), and few peaks during the autumn season (November 2018). The PM10 mass concentrations exceeded over 75% of the National Ambient Air Quality Standards (NAAQS), attributable partially due to high load of mineral dust near the site. The highest mean (μ ± 1 σ) concentration of PM10 was observed as 292 ± 116 μg m−3 in winter, followed by 218 ± 126 μg m−3 in autumn (post-monsoon), 182 ± 101 μg m−3 in summer and 126 ± 86 μg m−3 in monsoon, respectively.

Time series of PM10, PM2.5, CO, NO2, NO, and SO2 monitored over an urban site (Mandir Marg) of Delhi during the year 2018
In contrast, the elevated levels of PM2.5 were observed during autumn (5 and 13 November 2018) and winter (22–24 and 29 December 2018) compared to summer and monsoon. The high concentrations of PM2.5 during autumn and winter are attributable to the emissions from regional agriculture residue burning and local burning for space heating. The PM2.5 concentrations exceeded over 55% as compared to NAAQS likely due to the anthropogenic sources (long-range transport of agricultural waste burning emissions, coal combustion, local biomass/waste burning, and vehicular emissions). The hourly mean PM2.5 concentrations were observed as 192 ± 92 μg m−3 during the winter season, followed by autumn (159 ± 147 μg m−3), summer (79 ± 55 μg m−3) and monsoon (49 ± 32 μg m−3), respectively (Fig. 5.6). The winter months are associated with low temperatures, low solar radiation, low mixing heights, and calm winds. All of these conditions are favourable for the accumulation of pollutants, and thus, leading to high concentrations of PM. The geographical setting of the region also plays a critical role in the dispersion/accumulation of air pollution.
High peaks of CO concentrations were found mainly during the winter (26–31 January 2018). The highest mean CO level was observed as 2.6 ± 4.8 μg m−3 during the winter season, followed by autumn (1.8 ± 1.4 μg m−3), summer (1.1 ± 0.8 μg m−3), and monsoon (0.5 ± 0.3 μg m−3) (Fig. 5.6). During winter and autumn seasons, local and regional source activities [burning of leaves and woods, and long-range transport of emissions from agricultural residue burning and the burning for heating purpose in winter] along with the lower boundary layer height could be the possible reasons for high concentrations of CO.
A near similar trend was observed for NO2 and NO concentration during the study period at MM site. However, the highest NO2 and NO concentrations were observed during night and early morning in winter and autumn season likely due to increasing heavy duty diesel vehicle emission, atmospheric chemistry and low mixing height. The highest mean NO and NO2 concentrations were 96 ± 146 μg m−3 and 74 ± 39 μg m−3 during winter season of 2018, followed by autumn (103 ± 136 μg m−3 for NO; 79 ± 43 μg m−3 for NO2), summer (47 ± 93 μg m for NO; 65 ± 43 μg m for NO2), and monsoon (21 ± 39 μg m−3 for NO; 38 ± 20 μg m−3 for NO2) seasons, respectively (Fig. 5.6). Interestingly, it is noted that NO level is lower in summer and monsoon as compared to NO2 level, which indicates the influence of photo-chemistry in regulating the abundance of NOX species.
The elevated peaks of SO2 were observed in winter through summer (March, April, and May), and then, declining levels are observed in monsoon and autumn seasons. The highest mean SO2 concentration was observed as 16.2 ± 10.3 μg m−3 during summer, followed by winter (11.0 ± 9.1 μg m−3), monsoon (10.9 ± 2.0 μg m−3), and autumn (5.4 ± 1.7 μg m−3) (Fig. 5.6).
5.3.7 PM2.5/PM10 Ratio
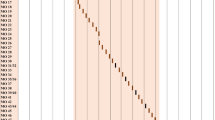
Figure 5.7 shows the calendar plot of hourly mean PM2.5/PM10 ratio at an urban site (MM) of Delhi. A high ratio of PM2.5/PM10 varying from 0.8 to 1.0 during the autumn and winter season has been observed in this study. The high ratios suggest the predominant impact of anthropogenic emissions and the intense atmospheric reactions leading to enhanced formation of secondary aerosol during the high PM2.5 pollution episodes. Furthermore, the PM2.5/PM10 ratios were found in the range of 0.2–0.4 during the summer months at the study site, which plausibly indicates that coarse particles were more prevalent in the summer season. This observation has linkage to enhanced mineral dust resuspension during the drier and hot summer season.

Calendar plot of PM2.5/PM10 ratio over an urban site (Mandir Marg) in Delhi during 2018
5.3.8 Influence of Meteorology
Besides atmospheric chemistry, the meteorological factors can also influence the level of air pollutants. Therefore, in order to understand the transport and the variabilities of criteria pollutants, conditional probability function (CPF) using wind speed and direction was analysed for the two high pollution witnessing seasons (winter and autumn). We plotted CPF by openair R package (Carslaw and Ropkins 2012) in R-studio (version 3.1.1; R Core Team, 2014) statistical software. More details about the functions are described in openair manual (Carslaw and Ropkins 2012).
The CBPF plots for diagnostic ratios (PM2.5/PM10, CO/NOX and SO2/NOX) are shown in Fig. 5.8 for two different seasons [top panel (winter) and bottom panel (autumn)]. Concisely speaking, one of the unique features from CBPF plots for all the assessed pollutants or its ratios herein is that their variability pattern is by and large governed by the winds from south-west to the south-east direction.

CBPF plots of PM2.5/PM10, CO/NOX and SO2/NOX in winter (top panel) and autumn (bottom panel) seasons over Mandir Marg in Delhi during year 2018. Threshold criteria were chosen at 75th percentile of species/pollutants
5.3.9 PSCF Analysis
Further, the PSCF approach helps to establish the comparative importance of regional and local sources by determining the contributions of potential source regions influencing the air pollution at the receptor site. The PSCF analysis also segregates the relevant back trajectories along with species concentrations at the receptor site. The PSCF plots for the PM2.5 are shown in Fig. 5.9 and the colour scale shown in each of these maps is a PSCF probability, indicating the possibility of source origin of a given species, which is measured at the receptor site. Threshold criteria were chosen at 75th percentile of pollutants for identifying the specific sources. For PM2.5, PSCF analysis identified regional source locations in north-western region encompassing areas from IGP region such as Delhi, Punjab, Haryana and northern Pakistan, especially in winter and autumn seasons. Some parts of Uttar Pradesh also contributed PM2.5 in autumn season (Fig. 5.9). It should be noted that the highest PM2.5 was associated with low winds. In a recent study (Rajput et al. 2021), it has been shown that ~73% of the total PM pollution originates within the city cluster in IGP region and rest of the PM pollution is governed through long-range transport of pollutants from upwind region.

PSCF plots of PM2.5 using 5-day air mass back trajectories at Mandir Marg in Delhi (at 500 m above ground level). Threshold criteria were chosen at 50th percentile of pollutants
The PSCF maps of PM2.5/PM10 ratio identify potential source locations mainly in north-west directions such as Punjab, Haryana, with some contributions from Uttar Pradesh. This indicates that fine particles were transported predominately from regional source regions during autumn and winter season (Fig. 5.10a). In winter and autumn, the PSCF plots of CO/NOX indicated that the probable locations influencing their concentrations are situated in the south-east and east directions (Ghaziabad and Dadri from Uttar Pradesh) (Fig. 5.10b).

PSCF plots of PM2.5/PM10 and CO/NOX ratio at Mandir Marg in Delhi. Threshold criteria were chosen at 50th percentile of pollutants
5.4 A Brief Review on Air Pollution and Public Health
5.4.1 Household Air Pollution (HAP) and Its Health Effects
According to the World Bank’s ‘The cost of air pollution: strengthening the economic case for action’, it is estimated that health and productivity loss in India due to air pollution, ambient and indoor combined, was about 5.7% of the GDP in 2013 (Balakrishnan et al. 2019). The same report also estimates that of this 5.7%, the 1.3% of GDP loss was due to indoor air pollution (IAP).
About IAP, the World Health Organization (WHO) asserts the rule of 1000, a rule which states that any pollutant released indoors is 1000 times more likely to reach into a person’s lung as compared to the scenario when it is released outdoors (WHO 2007). As a result, IAP has been found to be 10 times more potent as ambient air pollution (Ching-Boon 2016). According to the WHO, IAP has directly been linked to increased cases of pneumonia, stroke, ischaemic heart disease, chronic obstructive pulmonary disease (COPD), and lung cancer in women and children (WHO 2018b).
Moreover, studies indicate that IAP disproportionately affects under-developed and developing countries (Kankaria et al. 2014). 4.5% of global daily-adjusted life year (DALY) and 3.5 million deaths in 2010 were attributed to indoor air pollution. The World Bank Study also reported that the total welfare loss due to premature death as a result of air pollution increased by 94% between 1990 and 2013, in which the contribution of IAP increased by four times to the final tune of $1.5 trillion (adjusted to 2011 PPP, purchasing power parity).
5.4.2 Sources and Pollutants
-
(a)
Solid and biomass fuels—Incomplete combustion of biomass fuels generate pollutants like particulate matter (PM), carbon monoxide, polyaromatic hydrocarbons, polyorganic matter and formaldehyde. Combustion of coal, on the other hand, produces oxides of sulphur, arsenic and fluorine.
-
(b)
Bioaerosols—Airborne particles produced from microbial, viral, fungal and actinomycete, as well as microbes from organic materials, humidifiers, vaporizers, heating, ventilating and air conditioning systems (HVAC), lead to allergies, infections and poisoning.
-
(c)
Volatile organic compounds—Pollutants such as aldehydes, volatile and semi-volatile organic compounds from resins, waxes, polishing materials, cosmetics and binders.
-
(d)
Heavy metals like zinc, cadmium, chromium, mercury, lead and copper. Radon, pesticides, tobacco smoke and carbon monoxide.
-
(e)
Biological pollutants like dust mites, moulds, pollen and infectious agents produced in stagnant water, mattresses, carpets and humidifiers too pollute indoor air.
-
(f)
Infiltration of outdoor polluted air.
Additionally, indoor air quality (IAQ, Tables 5.2 and 5.3) gets further affected by
-
1.
Building characteristics such as the air tightness and ventilation
-
2.
Building occupancy and living space
-
3.
Equipment used within the buildings (e.g. photocopiers, printers and heaters)
-
4.
The customs, habits and tradition of the residents
-
5.
The economic status of occupants
In India, combustion of fuels is the largest contributor to indoor air pollution (IAP). Balakrishnan et al. (2019) find that IAP continues to wreak havoc in India due to excessive residential use of solid fuels (wood, dung, agricultural residue, coal and charcoal) for cooking and heating purposes (Fig. 5.11). Furthermore, more than half of India’s population was exposed to IAP in 2017 (Balakrishnan et al. 2019).

PM2.5 mass concentrations and use of solid fuels in the states of India, 2017: (a) Population-weighted mean ambient air PM2.5 and (b) proportion of population using solid fuels. (Adapted from Balakrishnan et al. 2019)
5.4.3 Health Status
Of the 1.24 million deaths in India in 2017 due to air pollution (12.5% of all deaths in India that year), 0.48 million deaths were attributed to IAP (Balakrishnan et al. 2019). 8.1% of total DALYs in India (38.7 million in 480.7 million) for the same year were due to air pollution; 3.3% were due to IAP. Lancet report informs that 1 out of every 8 deaths in India in 2017 were due to air pollution (Balakrishnan et al. 2019). This indicates that air pollution puts a disproportionate health burden on India. This same fact also means that India has the most to gain by undertaking reforms. The same Lancet report informs that reduction in air pollution and bringing air quality level to minimum accepted level would add 1.7 years to the average life expectancy of Indian population.
According to the State of Global Air Report, 2019 (Health Effects Institute 2019), Indian region was observed to have the second highest concentration of indoor PM2.5 averaging at 91 μg m−3 in South Asia (after Nepal’s 100 μg m−3) in 2017. Even in 2017, 56% of the population was still using solid fuels. A study done in rural areas of India found that PM exposure in a household that uses biomass for cooking averaged at 231 ± 109 mg m−3, compared to households that used cleaner fuel where the daily average exposure stood at 82 ± 39 mg m−3 (Kankaria et al. 2014). The findings from the above-mentioned study are presented below:
A study conducted in Mumbai found that PM2.5 average concentration from tobacco smoke was 363 μg m−3 at venues where smoking was allowed, compared to 97 μg m−3 where it was not (Raute et al. 2011).
Besides households, other settings where IAP is a cause of concern are schools, offices, and hospitals. A Greenpeace India report found that pollution levels in Delhi schools were five times higher than the safe limit recommended by WHO (Press Trust of India 2015). Other studies done in Delhi (Singh et al. 2017), Chennai (Nagendra and Harika 2010), Himachal Pradesh (Shree et al. 2019) and international experiences (WHO 2018b) all corroborate this finding and confirm that IAP level remains far worse inside the classroom than outside with exaggerated PM levels being the most threatening pollutant.
The Lancet (Stokel-Walker 2018) reports that 800,000 people globally die every year due to air quality issues at their workplace, and many more suffer due to the ‘sick building syndrome’ (EPA 1991), which includes headaches, cough, fever and chest pain caused due to contamination of air inside buildings. Lack of nationwide data in the Indian context makes it hard to comment on the corresponding figures for India, but a presentation given at Griha Summit summarizes the following with respect to buildings in NCR (Meattle 2016). Other studies in Rajasthan (Singhvi et al. 2019) support the finding of poor indoor quality in buildings.
The WHO reports that at any time 1.4 million people around the world are influenced with hospital-acquired infections (HAIs) and as many as 80,000 people around the world every year die due to HAI (Sidhu 2018). The IAQ and HAI incidence is dependent on factors like dimensional space, design features, cleaning and maintenance activities (Gola et al. 2019) and presence of bacteria, fungi, moulds and germs (Sidhu 2018). Emissions of pollutants (PM2.5, PM10, O3 and NO) from nearby sources like road traffic and parking (Gola et al. 2019) also contribute to poor air quality in hospitals. A study done in hospitals in Chennai found high level of contamination of bioaerosols and pathogens in indoor air (Sudharsanam et al. 2008).
5.4.4 Health Effects
IAP disproportionately affects children, women and elderly (over the age of 60) because they spend most of their time at home and thus are exposed to pollutants for a longer period (Table 5.4). Sustained exposure of pregnant women has been reported to affect both the mother and the unborn. According to WHO factsheet, 3.8 million people globally die prematurely every year due to IAP. Among these, 27% are due to pneumonia, 18% due to stroke, 27% due to ischaemic heart disease, 20% due to COPD and 8% due to lung cancer (WHO 2018b).
Studies have found that the use of solid fuels causes acute respiratory tract infection and COPD, poor perinatal outcomes like low birthweight and stillbirth, cancer of nasopharynx, larynx, lung and leukaemia (Kankaria et al. 2014). PM and nitrogen dioxide have been found to cause respiratory infections. PM causes chronic bronchitis and COPD, while nitrogen dioxide affects lung function and causes wheezing. Sulphur dioxide too causes wheezing and exacerbates asthma, COPD and CVD (Cardiovascular disease). Carbon monoxide (CO) has been found to lead to low birthweight and perinatal death, while polycyclic aromatic hydrocarbon (PAH) has been found to lead to cancers of lungs, mouth, nasopharynx and larynx. These PAHs are released by the combustion sources, which also produce metal ions, both of which cause cataract.
Incomplete combustion of biomass also produces formaldehyde, which has been known to cause acute irritation and bronchitis, reduce vital capacity and act as a carcinogen that can cause leukaemia and lung cancer. India-specific studies show that use of biomass combustion for cooking leads to active tuberculosis (odds ratio: OR = 3.66, 95% CI: 2.82–4.50). In fact, 51% of all cases of active tuberculosis in the age group of 20 years and above could be attributed to smoke from cooking. Users of biomass fuels were also found to be at 50% excess risk of stillbirths and 1.5 times more likely to have low birthweight babies. On average, these babies weigh 73 g lighter (mean birthweight 2883.8 g versus 2810.7 g, p < 0.001). There is also an increased risk to asthma (Sehgal et al. 2014a, b). Besides this, the cognitive abilities and productivity levels of those exposed to higher level of indoor pollutions are severely hampered. Holding constant other risk factors, apart from LPG, all other cooking fuels were found to cause acute lower respiratory tract infection (adjusted OR = 4.73). In fact, the use of biomass fuels was found to significantly contribute to a prolonged nasal mucociliary clearance time (765.8 ± 378.16 s) when compared to the use of cleaner fuels (545.4 ± 215.55 s). Similarly, biomass use was also found to lead to higher cases of COPD (OR: 1.24), especially among those who spend more than 2 h a day for cooking. Additionally, the carcinogens (PAHs, HCHO, etc.) released by biomass fuels reportedly led to cases of lung cancer in women (Kankaria et al. 2014). Among women, the study conducted by Sehgal et al. (2014a, b) found that IAP contributes to 2.4 million of the 5.6 million cases of chronic bronchitis, 0.3 million of the 0.76 million cases of TB and five million of the 51.4 million cases of cataract. Her paper also corroborates aforementioned IAP health effects of COPD (OR from 1 to 3.04), lung cancer (OR from 1.5 to 3.8) and acute lower respiratory tract infections (OR from 1.5 to 3.7).
Studies that have been used to present above the health effects of IAP have been tabulated in table 5.4:
5.4.5 Vulnerable Population
IAP is more likely to affect rural and poor/low socio-economic status (SES) households compared to urban and richer households and women and younger children are the more vulnerable population compared to men (Kankaria et al. 2014). Since combustion of cooking fuels contributes to IAP the most, women get disproportionately affected due to household air pollution. According to the Global Burden of Disease programme, globally India records the highest number of deaths attributed to illnesses caused due to IAP from solid fuel burning. According to the World Health Organization’s report ‘Air Pollution and Child Health’ in 2016, indoor air pollution led to the death of 66,890 children below the age of 5 years, out of which 36,073 were girls and 30,817 were boys. In totality, 101,788 children in India under 5 years of age died due to ambient and indoor air pollution combined, which roughly translates to around 12 deaths per hour in 2016. Besides women and children, it is the elderly (age ≥ 60 years) who are extremely vulnerable to IAP and studies show that the elderly in households that use biomass fuels more often suffer from asthma (as compared to households that use cleaner fuels, OR = 1.59; 95% CI: 1.30–1.94). The same study also confirmed that women are more vulnerable to asthma caused by IAP as compared to men.
5.5 Conclusions
We have presented here the current status of air pollution focusing over a typical urban site of Delhi and a brief overview of health effectsof air pollution. We report on detailed characterization of the air masses in Delhi and investigate the following aspects: (i) temporal variability of particulate matter (PM2.5 and PM10) on an hourly, weekly, monthly and seasonally basis; (ii) the primary and secondary pollutants and their relative abundances; and (iii) conditional probability function (CPF) and potential source contribution function (PSCF) are also discussed for the data set over Delhi. In Delhi, clear seasonal trends were observed for PM2.5, PM10, CO, SO2 and NOX. High abundance episodes of PM2.5, PM10, CO and NOX were observed in winter and autumn due to emissions from local and regional sources and from the long-range transport. High PM2.5/PM10 ratio in autumn and winter is attributable to predominant impact from anthropogenic emission sources. CPF and PSCF analysis showed that besides local sources the long-range transport affected the local and regional ambient air quality in Delhi. Overall, the PSCF analysis has revealed that by and large the high concentration of air pollutants, mainly during the winter and autumn seasons, was associated with air masses arriving from north-west direction in Delhi. This study highlights the utility of other CAAQM stations in India for the exploration of air quality research, public health and awareness and policy framework.
References
AirVisual (2018) 2018 world air quality report: region & city PM2.5 ranking
Asbach C et al (2017) On the effect of wearing personal nanoparticle monitors on the comparability of personal exposure measurements. Environ Sci Nano 4:233–243
Balakrishnan K et al (2019) The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: the Global Burden of Disease Study 2017. Lancet Plane Health 3(1):e26–e39
Bassani DG, Jha P, Dhingra N, Kumar R (2010) Child mortality from solid-fuel use in india: a nationally-representative case-control study. BMC Public Health 10(1). https://doi.org/10.1186/1471-2458-10-491
Behera D, Balamugesh T (2005) Indoor air pollution as a risk factor for lung cancer in women. J Assoc Physicians India 53
Bhat YR, Manjunath N, Sanjay D, Dhanya Y (2012) Association of indoor air pollution with acute lower respiratory tract infections in children under 5 years of age. Paediat Int Child Health 32(3):132–135. https://doi.org/10.1179/2046905512y.0000000027
Burnett R et al (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122(4):397–403. https://doi.org/10.1289/ehp.1307049
Capistrano S, Reyk DV, Chen H, Oliver B (2017) Evidence of biomass smoke exposure as a causative factor for the development of COPD. Toxics 5(4):36. https://doi.org/10.3390/toxics5040036
Carslaw D, Ropkins K (2012) The openair manual—an R package for air quality data analysis. Environ Model Softw 27:52–61
Chakraborty A, Rajeev P, Rajput P, Gupta T (2017) Water soluble organic aerosols in indo gangetic plain (igp): insights from aerosol mass spectrometry. Sci Total Environ 599:1573–1582
Chatterjee P (2019) Indian air pollution: loaded dice. Lancet Planet Health 3(12):e500–e501
Ching-Boon K (2016) Why indoor air pollution may be worse than it is outdoors. South China Morning Post, June 10, 2016. https://www.scmp.com/lifestyle/health/article/1820604/why-indoor-air-pollution-may-be-worse-it-outdoors
Choudhary V et al (2018) Light absorption characteristics of brown carbon during foggy and non-foggy episodes over the indo-gangetic plain. Atmos Pollut Res 9(3):494–501. https://doi.org/10.1016/j.apr.2017.11.012
CPCB, 2018. Ambient air quality data of delhi stations
Dandona L et al (2017) Nations within a nation: variations in epidemiological transition across the states of india, 1990-2016 in the global burden of disease study. Lancet 390:2437–2460
Dey S et al (2012) Variability of outdoor fine particulate (PM2.5) concentration in the indian subcontinent: a remote sensing approach. Remote Sens Environ 127:153–161
Dockery DW, Brunekreef B (1996) Longitudinal studies of air pollution effects on lung function. Am J Respir Crit Care Med 154:250–256
Dockery DW et al (1993) An association between air pollution and mortality in six u.S. Cities. N Engl J Med 329:1753–1759
DPCC (2017) Environmental concerns. https://doi.org/10.1016/B978-1-893997-92-9.50028-1
EPA (1991) Indoor Air Facts No. 4: Sick Building Syndrome. Air and Radiation (6609J). EPA, February 1991. https://www.epa.gov/sites/production/files/2014-08/documents/sick_building_factsheet.pdf
Fuzzi S et al (2006) Critical assessment of the current state of scientific knowledge, terminology, and research needs concerning the role of organic aerosols in the atmosphere, climate, and global change. Atmos Chem Phys 6:2017–2038
GBD (2015) Institute for health metrics and evaluation (IHME), GBD compare. IHME, University of Washington, Seattle, WA. Accessed 30 Sept 2016
Geller MD et al (2002) Indoor/outdoor relationship and chemical composition of fine and coarse particles in the southern California deserts. Atmos Environ 36:1099–1110
Gola M, Gaetano S, Stefano C (2019) Indoor air quality in inpatient environments: a systematic review on factors that influence chemical pollution in inpatient wards. J Healthcare Eng. Hindawi. https://www.hindawi.com/journals/jhe/2019/8358306/abs/#B18
Health Effects Institute (2019) State of Global Air 2019. Special Report. Health Effects Institute, Boston, MA. ISSN 2578-6873
Izhar S, Rajput P, Gupta T (2018) Variation of particle number and mass concentration and associated mass deposition during diwali festival. Urban Clim 24:1027–1036
Johnson P et al (2011) Prevalence of chronic obstructive pulmonary disease in rural women of Tamilnadu: implications for refining disease burden assessments attributable to household biomass combustion. Glob Health Action 4(1):7226. https://doi.org/10.3402/gha.v4i0.7226
Kankaria A, Baridalyne N, Gupta SK (2014) Indoor air pollution in india: implications on health and its control. Indian J Community Med 39(4):203–207. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4215499/
Korrick SA et al (1998) Effects of ozone and other pollutants on the pulmonary function of adult hikers. Environ Health Perspect 106:93–99
Kumar V, Goel A, Rajput P (2017) Compositional and surface characterization of HULIS by UV-VIS, FTIR, NMR and XPS: wintertime study in northern india. Atmos Environ 164:468–475
Mahowald NM et al (2005) Atmospheric global dust cycle and iron inputs to the ocean. Global Biogeochem Cycles 2005:19. https://doi.org/10.1029/2004GB002402
Meattle K (2016) Smart buildings & good indoor air quality. TERI-Griha Summit. https://www.grihaindia.org/grihasummit/tgs2016/presentations/18feb/IndoorEnvQuality/Kamal_Meattle.pdf
Nagendra SMS, Harika PS (2010) Indoor air quality assessment in a school building in Chennai City, India. Air Pollution XVIII 2010. https://doi.org/10.2495/air100241
Nazarenko Y, Lioy PJ, Mainelis G (2014) Quantitative assessment of inhalation exposure and deposited dose of aerosol from nanotechnology-based consumer sprays. Environ Sci Nano 1:161–171
Neas LM, Schwartz J, Dockery D (1999) A case-crossover analysis of air pollution and mortality in Philadelphia. Environ Health Perspect 107:629–631
Neogi S et al (2015) Association between household air pollution sand neonatal mortality: an analysis of annual health survey results, India. WHO South-East Asia J Public Health 4(1):30–37. https://doi.org/10.4103/2224-3151.206618
Novakov T, Penner JE (1993) Large contribution of organic aerosols to cloud-condensation-nuclei concentrations. Nature 365:823–826
Padhi BK et al (2017) Predictors and respiratory depositions of airborne endotoxin in homes using biomass fuels and lpg gas for cooking. J Expo Sci Environ Epidemiol 27:112–117
Pant P, Guttikunda SK, Peltier RE (2016) Exposure to particulate matter in India: a synthesis of findings and future directions. Environ Res 147:480–496
Parikh J, Balakrishnan K, Laxmi V, Biswas H (2001) Exposure from cooking with biofuels: pollution monitoring and analysis for rural Tamil Nadu, india. Energy 26:949–962
Peters A et al (2000) Air pollution and incidence of cardiac arrhythmia. Epidemiology 11:11–17
Posfai M, Buseck PR (2010) Nature and climate effects of individual tropospheric aerosol particles. Annu Rev Earth Planet Sci 38:17–43
Press Trust of India (2015) Indoor air quality in Delhi Schools Very Bad, Says Green Body. NDTV.com, December 4, 2015. https://www.ndtv.com/delhi-news/indoor-air-quality-in-delhi-schools-very-bad-says-green-body-1250879
Raes F et al (2000) Formation and cycling of aerosols in the global troposphere. Atmos Environ 34:4215–4240
Rajeev P et al (2016) Chemical characteristics of aerosol and rain water during an El Niño and PDO influenced Indian summer monsoon. Atmos Environ 145:192–200
Rajput P, Gupta T (2020) Instrumental variable analysis in atmospheric and aerosol chemistry. Front Environ Sci 8:267. https://doi.org/10.3389/fenvs.2020.566136
Rajput P et al (2011) Atmospheric polycyclic aromatic hydrocarbons (PAHs) from post-harvest biomass burning emissions in the Indo-Gangetic Plain: isomer ratios and temporal trends. Atmos Environ 45:6732–6740
Rajput P, Sarin MM, Kundu SS (2013) Atmospheric particulate matter (PM2.5), EC, OC, WSOC and PAHs from NE-Himalaya: abundances and chemical characteristics. Atmos Pollut Res 4:214–221
Rajput P, Sarin MM, Sharma D, Singh D (2014a) Atmospheric polycyclic aromatic hydrocarbons and isomer ratios as tracers of biomass burning emissions in northern india. Environ Sci Pollut Res 21:5724–5729
Rajput P, Sarin MM, Sharma D, Singh D (2014b) Characteristics and emission budget of carbonaceous species from post-harvest agricultural-waste burning in source region of the Indo-Gangetic Plain. Tellus-B. https://doi.org/10.3402/tellusb.v66.21026
Rajput P et al (2016) Chemical characterisation and source apportionment of PM1 during massive loading at an urban location in Indo-Gangetic Plain: impact of local sources and long-range transport. Tellus B 68:30659. https://doi.org/10.3402/tellusb.v68.30659
Rajput P, Singh DK, Singh AK, Gupta T (2018a) Chemical composition and source-apportionment of sub-micron particles during wintertime over northern india: new insights on influence of fog-processing. Environ Pollut 233:81–91
Rajput P et al (2018b) Indices used for assessment of air quality, Air pollution: sources, impacts and controls. https://doi.org/10.1079/9781786393890.0096
Rajput P et al (2019) Deposition modeling of ambient aerosols in human respiratory system: health implication of fine particles penetration into pulmonary region. Atmos Pollut Res 10:334–343
Rajput P et al (2021) Source contribution of firecrackers burst vs. long-range transport of biomass burning emissions over an urban background. Front Sustain Cities 2:68. https://doi.org/10.3389/frsc.2020.622050
Ramanathan V, Carmichael G (2008) Global and regional climate changes due to black carbon. Nat Geosci 1:221–227
Raute LJ, Gupta PC, Pednekar MS (2011) Smoking ban and indoor air quality in restaurants in Mumbai, India. Indian J Occup Environ Med 15(2):68–72
Rolph G, Stein A, Stunder B (2017) Real-time environmental applications and display sYstem: READY. Environ Model Softw 95:210–228. https://doi.org/10.1016/j.envsoft.2017.06.025
Rudich Y (2003) Laboratory perspectives on the chemical transformations of organic matter in atmospheric particles. Chem Rev 103:5097–5124
Saha A (2005) Ocular morbidity and fuel use: an experience from India. Occup Environ Med 62(1):66–69. https://doi.org/10.1136/oem.2004.015636
Schwartz J (1995) Short term fluctuations in air pollution and hospital admissions of the elderly for respiratory disease. Thorax 50:531–538
Sehgal M, Rizwan SA, Krishnan A (2014a) Disease burden due to biomass cooking-fuel-related household air pollution among women in India. Co-Action Publishing, Global health action. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221659/
Sehgal M, Suliankatchi AR, Anand K (2014b) Disease burden due to biomass cooking-fuel-related household air pollution among women in India. Global health action. Co-Action Publishing. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4221659/
Seinfeld JH, Pankow JF (2003) Organic atmospheric particulate material. Annu Rev Phys Chem 54:121–140
Senfield JH, Pandis SN (2006) Atmospheric chemistry and physics, 2nd edn. Wiley
Shree V, Marwaha BM, Awasthi P (2019) Indoor air quality investigation at primary classrooms in Hamirpur, Himachal Pradesh, India. Journal of Water, Energy and Environment, Hydro Nepal. https://www.nepjol.info/index.php/HN/article/view/23583
Sidhu S (2018) Maintaining indoor air quality in hospitals. Biospectrum. https://www.biospectrumindia.com/features/70/12163/maintaining-indoor-air-quality-in-hospitals.html
Singh DK, Gupta T (2016) Effect through inhalation on human health of PM1 bound polycyclic aromatic hydrocarbons collected from foggy days in northern part of india. J Hazard Mater 306:257–268
Singh P, Arora R, Goyal R (2017) Indoor air quality assessment in selected schools of Delhi-NCR, India. Int J Appl Home Sci 4(5 & 6):389–394
Singhvi R, Rathore NS, Rathore H (2019) Indoor air quality in residential buildings in Rajasthan (India). http://www.irbnet.de/daten/iconda/CIB10196.pdf
Sorathia F et al (2018) Dicarboxylic acids and levoglucosan in aerosols from Indo-Gangetic Plain: inferences from day night variability during wintertime. Sci Total Environ 624:451–460
Spracklen DV, Carslaw KS, Poschl U, Rap A, Forster PM (2011) Global cloud condensation nuclei influenced by carbonaceous combustion aerosol. Atmos Chem Phys 11:9067–9087
Sreeramareddy C, Rahul T, Shidhaye R, Sathiakumar N (2011) Association between biomass fuel use and maternal report of child size at birth—an analysis of 2005-06 India Demographic Health Survey Data. BMC Public Health 11(1). https://doi.org/10.1186/1471-2458-11-403
Srivastava A, Jain VK (2007) A study to characterize the suspended particulate matter in an indoor environment in Delhi, India. Build Environ 42:2046–2052
Stokel-Walker C (2018) The hidden air pollution inside your workplace—BBC Worklife. BBC News. BBC, October 16, 2018. https://www.bbc.com/worklife/article/20181016-the-hidden-air-pollution-inside-your-workplace
Sudharsanam S, Padma S, Merline S, Ralf S (2008) Study of the indoor air quality in hospitals in South Chennai, India—microbial profile. Indoor Built Environ 17(5):435–441. https://doi.org/10.1177/1420326x08095568
Tielsch JM et al (2009) Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in South India. Int J Epidemiol 38(5):1351–1363. https://doi.org/10.1093/ije/dyp286
Uria-Tellaetxe I, Carslaw DC (2014) Conditional bivariate probability function for source identification. Environ Model Softw 59:1–9. https://doi.org/10.1016/j.envsoft.2014.05.002
WHO (2007) Indoor air pollution: national burden of disease estimates. World Health Organization, Geneva, p 2007
WHO (2016) Ambient air pollution—a major threat to health and climate. https://www.who.int/airpollution/ambient/en/
WHO (2018a) WHO global ambient air quality database (update 2018). https://www.who.int/airpollution/data/cities/en/
WHO (2018b) Household air pollution and health. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health
Yadav S, Rajamani V (2004) Geochemistry of aerosols of northwestern part of India adjoining the Thar Desert. Geochim Cosmochim Acta 68(9):1975–1988
Zikova N, Masiol M, Chalupa D, Rich D, Ferro A, Hopke P, Zikova N, Masiol M, Chalupa DC, Rich DQ, Ferro AR, Hopke PK (2017) Estimating hourly concentrations of PM2.5 across a metropolitan area using low-cost particle monitors. Sensors 17:1922. https://doi.org/10.3390/s17081922
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Rajput, P., Prakash, J., Sharma, D. (2022). High-Resolution Ambient Record of Aerosols over Delhi and Associated Typical Health Effects. In: Sonwani, S., Shukla, A. (eds) Airborne Particulate Matter. Springer, Singapore. https://doi.org/10.1007/978-981-16-5387-2_5
Download citation
DOI: https://doi.org/10.1007/978-981-16-5387-2_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-5386-5
Online ISBN: 978-981-16-5387-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)