
Abstract
In this digital age, artificial intelligence and its applications have become ubiquitous in the world around us. The practice of modern medicine driven by scientific data and evidence is an obvious target for these applications. In this chapter, we explore the history of artificial intelligence, where we are now, how to interpret current evidence generated by algorithms and how to balance the hype and potential that comes with introduction of a new standard of care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1.1 Artificial Intelligence
To understand the concept of artificial intelligence (AI) and how it is being used in applications today, we first need to understand the concept of intelligence. The term intelligence is derived from the Latin noun ‘intellēctus’ or verb ‘intelligere’, which means to comprehend or perceive. This concept is however abstract and is better understood with examples of different types of intelligence and how humans display them.
-
1.
Visual-spatial: physical environment characteristics (architects when designing a building according to terrain and surroundings, navigating a boat in water).
-
2.
Kinaesthetic: body movements (technical skill and precision of a ballerina, surgeons or athletes).
-
3.
Creative: novel thought, typically expressed in art, music and writing (imagination-driven authors, painters and musicians).
-
4.
Interpersonal: interaction with others (interviewers, shopkeepers, businessmen).
-
5.
Intrapersonal: self-realisation (meditation, goal planning, self-preservation).
-
6.
Linguistic: manipulation of words for communication (day-to-day communication).
-
7.
Logical-mathematical: calculations, identifying patterns, analysing relationships (logic, puzzles, computing numbers).
From this classification, it is easy to understand what AI today is capable of and where we may be heading in the future. The simulation potential of logical-mathematical intelligence is the maximum and early development in AI almost exclusively focused on this domain. Robotics aims to mimic the kinaesthetic intelligence while sensor-driven (LiDAR scanners in self driven cars) applications leverage on visual-spatial intelligence. Chatbots are trying to mimic linguistic and interpersonal intelligence while the creative and intrapersonal intelligence are domains with limited to no simulation potential. Utility of algorithms has been explored to create music and draw art, but this is mainly driven by logical-mathematical intelligence.
When we understand what an algorithm can and cannot do, that is when we can maximise the utility of the algorithm. Thus, it is imperative to stay away from overoptimistic predictions and avoid false promises to increase the acceptability of algorithms and their potential widespread use. Some algorithms that have achieved this level of acceptance are the ‘search engine’ algorithms that offer personalised search results, spam filters in email clients, recommendations in applications like Netflix or Amazon and computational photography algorithms on mobile devices. Algorithms that have been developed for use in hospitals however are yet to see such levels of acceptance. This has been due to the inherent nature of patient–physician relationship, potential regulatory hurdles and multiple types of bias that confound these algorithms. However, with FDA approvals being given to 64 algorithms (SaMD: software as medical device) over the last 3 years, we can expect widespread availability of these options for clinicians in the future [1, 2]. Currently for ophthalmology only the IDx-DR has been approved as an autonomous AI diagnostic system for diabetic retinopathy [3,4,5].
1.2 The Past and What We Can Learn from It
The earliest examples of humans trying to build intelligent devices were the abacus like devices namely the nepohualtzintzin (Aztecs), suanpan (Chinese) or the soroban (Japan) [6]. These devices though based on simple concepts, reduced the time required for mathematical computations. This concept of reducing time and effort for repetitive computational tasks remains one of the driving concepts behind algorithm development.
The Antikythera mechanism was another ancient computing device that was probably used to track dates of important events, predict eclipses and even planetary motions [7]. Ramon Llull’s Ars Magna was another device that used simple paper-based rotating concentric circle to generate combinations of new words and ideas. It was a rudimentary step towards generating a logical system to produce knowledge [8]. Examples of such systems also exist in fictional literature like the book-writing engine in the city of Lagado in Gulliver’s Travels. Attempts to create a similar algorithm include the RACTER program which generated text for the first computer authored book titled ‘The Policeman’s Beard is Half Constructed’ in 1983 [9].
Perhaps one of the most significant inventions in primitive computing was the Difference Engine, proposed by Charles Babbage in 1822 [10]. In addition to this engine, Babbage also wanted to create the Analytical Engine which could be programmed using punch cards and had separate areas for number storage and computation. Ada Lovelace, the daughter of English poet, Lord Byron, gave the specifications for designing a program for this Engine. She is now considered by many as the first computer programmer [11].
Currently we know that data is stored in computers as a series of binary 1 s and 0 s called bits. Eight bits make up one byte. The fundamentals of this concept were published in a book, titled, ‘An Investigation into the Laws of Thought, on Which Are Founded the Mathematical Theories of Logic and Probabilities’, by George Boole in 1854 [12]. He wanted to reduce logic to simple algebra involving only 0 and 1, with three simple operations: and, or and not. Boolean algebra, which is named after him, is one of the foundations of this digital age.
Over the next few decades, there were incremental improvements in algorithms for applications like optical character recognition (OCR), handwriting recognition (HWR) and speech synthesis. The next breakthrough was the 1943 paper ‘A Logical Calculus of the Ideas Immanent in Nervous Activity’ by Warren McCulloch and Walter Pitts [13]. In this paper, they described the basic mathematical model of the biological neuron. This formed the basis for the development of artificial neural networks (ANN) and deep learning (DL).
ENIAC, short for Electronic Numerical Integrator and Computer, was unveiled in 1946 and represented the pinnacle of specialised electronic, reprogrammable, digital computers built to solve a range of computing problems [14]. This started the race for development of powerful computer hardware for specialised operations by different countries. However, by today’s standards even the Apollo Space Mission Guidance Computer (AGC) only had 64 KB memory and operated at 0.043 MHz, when compared to today’s smartphones running with GHz speed processors (A14 chips in iPhones and iPads run at 3.0GHz and thus clock 70,000 times faster) shows how far we have come in terms of computing power due to the development of semiconductor technology [15, 16].
The term, ‘artificial intelligence’ (AI) was coined by John McCarthy at the Dartmouth conference for experts in this field in 1956 [17]. The expectations from this conference were extremely high despite limited computing power and hardware at that time. Inability to meet the hype generated by this conference, thus led to the AI winters of 1974–1980 and 1987–1993 [18].
Meanwhile during this time interesting developments were taking place in the backdrop, like:
-
Rosenblatt concept of the perceptron [19] (1957).
-
Arthur Lee Samuel’s concept of machine learning [20] (1959).
-
ELIZA: The program that could respond to text input simulating a conversation [21] (1964).
-
Early deep learning using supervised multilayer perceptrons (1965).
-
MYCIN: Rule-based expert system to identify sepsis and to recommend antibiotics [22] (1970).
-
Fuzzy logic and its applications in automation [23] (1965–1974).
-
Lighthill Report (criticised the utter failure of artificial intelligence in achieving its ‘grandiose objectives’) that triggered the first AI winter [24] (1973).
-
Joseph Weizenbaum’s early idea of ethics in AI, suggestion that AI should not be used as substitutes for humans in jobs requiring compassion, interpersonal respect, love, empathy and care [25] (1976).
-
Expert system boom driven by LISP machines; however, LISP was soon overtaken by IBM/Apple with more powerful and cheaper consumer desktop computers, this led to collapse of the demand for expert systems [26] (1980–1987).
-
Alex Waibel’s Time Delay Neural Network (TDNN) which was the first convolutional network [27] (1987).
-
Moravec’s paradox: Tasks simple for humans like walking, talking, face/voice recognition are difficult for AI while humanly complex computational tasks involving mathematics and logic are simple [28] (1988).
-
Yan LeCun developed system to recognise handwritten ZIP codes [29] (1989).
-
Chinook (checkers playing algorithm) vs Marion Tinsley [30] (1994).
-
IBM Deep Blue (chess playing algorithm) vs Garry Kasparov [31] (1997).
-
Logistello (othello playing algorithm) vs Takeshi Murakami [32] (1997).
-
Oh and Jung demonstrated power of graphical processing units (GPUs) for network training [33] (2004).
-
ImageNet database [34] (2009).
-
IBM DeepQA-based Watson winning the quiz show Jeopardy [35] (2011).
-
Google DeepMind AlphaGo (based on ANN and Monte Carlo tree search algorithm defecting Lee Sedol) and AlphaGo Zero (trained by self-play without using previous data) which subsequently defected AlphaGo [36] (2017).
-
Stanford death predictor [39] (2019).
Perhaps the most important developments that renewed interest in the field of AI and allowed widespread access over the last decade are the availability of large amounts of data and increased computational power at cheaper costs using modalities like graphical processing units (GPUs). ImageNet has especially been used to train popular models like the AlexNet [40], VGG16 [41], Inception modules [42] and the currently used ResNet [43].
Other datasets are also available for applications like music, facial recognition, text and speech processing [44]. As AI is a rapidly evolving field, today new innovations also happen with the same pace. However, understanding the history of AI is vital in predicting how it may affect the future. In further sections, we discuss why AI has become so popular today and how it may help in optimising patient care by evolving into an effective decision support system.
1.3 Why Should a Clinician Bother About AI?
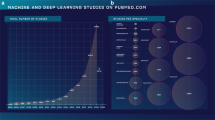
A quick PubMed search shows how the number of articles published in the field of AI has grown to 112,594 results with 35,140 (31.2%) being published since 2018 [45]. Another insight comes from the Gartner Hype Index that monitors and predicts how a technology will evolve over time [46]. Machine learning (ML) was at the peak of inflated expectation indicating impact of publicity and expectations in 2016, DL at the same peak in 2018. These peaks also translate to the increase in applications that were developed using these technologies in this time. PubMed search shows a total of 49, 721 results till 2020 for ML, with 3885 results in 2016, 5217 in 2017 and 8169 in 2018. The last 2 years have seen 24,230 results which is 48.73% of total results [47]. Similarly, for DL, PubMed search shows 18,082 results till 2020 with 3020 results in 2018, 5401 in 2019 and 7383 in 2020 [48]. The last 2 years represent 70.7% of the total results. These numbers show how these technologies are being increasingly tried and tested for use in medicine.
Due to the lack of special training for understanding or evaluating these applications or their underlying concepts, a lot of effort has been recently initiated to make the clinicians more aware and sensitised about the use of AI in providing patient care [49,50,51]. In the next section, we describe a checklist approach to reading an AI paper with emphasis on evidence assessment and evaluation of future potential for translation to clinical use. We believe that this approach can help in better understanding of the scientific merit of the publication and its potential impact on care delivery practice patterns.
1.4 How to Read an Artificial Intelligence Paper?
Jaeschke et al. provided a framework to evaluate diagnostic tests in clinical medicine [52]. We have expanded the same framework to include relevant information about AI-based algorithms. We will initially describe the framework and then provide example of using the framework [53, 54]. The framework is as follows:
-
Step 1: Evaluate if the study results are valid.
Primary Guide
-
Was there an independent, blind comparison with a reference standard?
-
Did the patient sample include an appropriate spectrum of patients to whom the diagnostic test will be applied in clinical practice?
For AI-based algorithms these can be adapted as:
-
Are the datasets appropriate and described in sufficient detail?
-
Was the gold standard for algorithm training appropriate and reliable?
-
Secondary Guide
-
Did the results of the test being evaluated influence the decision to perform the reference standard?
-
Were the methods for performing the test described in sufficient detail to permit replication?
For AI-based algorithms these can be adapted as:
-
Is the methodology of algorithm development described in sufficient detail to allow replication?
-
Are the algorithm/datasets used available for external validation?
-
-
-
Step 2: Evaluate the presented results.
-
Are likelihood ratios for the test results presented or data necessary for their calculation provided?
For AI-based algorithms these can be adapted as:
-
Are adequate and appropriate performance metrics reported? [50].
-
-
-
Step 3: Evaluate the utility of results in providing care for your patients.
-
Will the reproducibility of the test result and its interpretation be satisfactory in my setting?
-
Are the results applicable to my patient?
-
Will the results change my management?
-
Will the patients be better off because of the test?
For AI-based algorithms these can be adapted as:
-
Are the findings of the algorithm explainable? Does the algorithm exhibit generalisability (can it be easily adapted for a different machine input or population)? Was the original algorithm performance too optimistic?
-
Has the algorithm been validated in my local population?
-
Is there any independent comparison of the algorithm with existing standard of care? Is there a cost-effectiveness analysis for rationale of algorithm use?
-
Will there be a significant impact on patient well-being after algorithm deployment? Is there an attempt to measure this impact?
-
-
Table 1.1 shows how this framework can be used to evaluate an artificial intelligence paper.
1.5 Conclusion
We have exciting times ahead of us, due to the immense potential of AI as a clinical decision support tool. However potential ethical and legal issues of liability management, reduction in clinical skills due to excessive algorithm use, inappropriate data representation especially for minorities, lack of personal privacy, ‘biomarkup’ due to excessive testing and inadequate understanding of algorithm results (AI black box) can hamper the deployment and acceptance of these AI algorithms [55,56,57,58,59]. Humans are intelligent, flexible and tenacious but are also liable to make mistakes. The embarrassing inability of Apple HealthKit to track menstrual cycles while tracking innocuous parameters for health monitoring like weight, height, inhaler use, alcohol content, blood sugar, sodium intake is just one example of this oversight [60]. Inherently the algorithms are unbiased but the bias from data used for training and the developers inherent bias can ultimately create complex ethical problems. An attitude of critical evaluation by all stakeholders before adoption of any new technology will thus help to separate the real from the hype. IBM Watson is an excellent example of how AI struggles with real-world medicine, messy hospital records and the expectations of industry, hospitals, physicians and patients [61]. We must keep in mind that our primary goal is always providing our patients the ‘best’ standard of care available. The affordability, availability and widespread social impact of the ‘model of care’ should also be considered while making this critical decision.
References
Benjamens S, Dhunnoo P, Meskó B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: an online database. NPJ Digit Med. 2020;3(1):118.
Software as a Medical Device (SAMD): clinical evaluation—guidance 2018 [updated 2018/08/31/]. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/software-medical-device-samd-clinical-evaluation.
Abramoff MD, Lou Y, Erginay A, et al. Improved automated detection of diabetic retinopathy on a publicly available dataset through integration of deep learning. Invest Ophthalmol Vis Sci. 2016;57(13):5200–6.
Abràmoff MD, Lavin PT, Birch M, Shah N, Folk JC. Pivotal trial of an autonomous AI-based diagnostic system for detection of diabetic retinopathy in primary care offices. NPJ Digit Med. 2018;1(1):39.
Grzybowski A, Brona P. A pilot autonomous AI-based DR screening in Poland. Acta Ophthalmol. 2019;97(S263)
Projects CtW. Abacus—Wikipedia 2020 [updated 2020/11/02/]. Available from: https://en.wikipedia.org/w/index.php?title=Abacus&oldid=986730574.
Projects CtW. Antikythera mechanism—Wikipedia 2020 [updated 2020/11/03/]. Available from: https://en.wikipedia.org/w/index.php?title=Antikythera_mechanism&oldid=986880521.
Jensen T, editor. Ramon Llull’s Ars magna. Cham: Springer; 2018.
Racter—visual melt 2020 [updated 2020/11/05/]. Available from: https://visualmelt.com/Racter.
Park E. What a difference the difference engine made: from Charles Babbage’s calculator emerged today’s computer. Smithsonian Magazine; 1996.
Ada Lovelace: founder of scientific computing 1998 [updated 1998/03/24/]. Available from: https://www.sdsc.edu/ScienceWomen/lovelace.html.
Boole G. An investigation of the laws of thought: on which are founded the mathematical theories of logic and probabilities. Walton and Maberly; 1854.
McCulloch WS, Pitts W. A logical calculus of the ideas immanent in nervous activity. 1943. Bull Math Biol. 1990;52(1–2):99–115. discussion 73–97
Levy S. The brief history of the ENIAC computer. Smithsonian Magazine; 2013.
Computers on board the Apollo spacecraft 2014 [updated 2014/07/04/]. Available from: https://history.nasa.gov/computers/Ch2-5.html.
Your smartphone is millions of times more powerful that all of NASA’s combined computing in 1969 2020 [updated 2020/02/11/]. Available from: https://www.zmescience.com/science/news-science/smartphone-power-compared-to-apollo-432.
Rajaraman V. JohnMcCarthy—father of artificial intelligence. Resonance. 2014;19(3):198–207.
History of AI winters. Actuaries Digital 2020 [updated 2020/11/06/]. Available from: https://www.actuaries.digital/2018/09/05/history-of-ai-winters/#_ednref2.
Rosenblatt F. The perceptron: a probabilistic model for information storage and organization in the brain. Psychol Rev. 1958;65(6):386–408.
Arthur Samuel 2007 [updated 2007/12/08/]. Available from: http://infolab.stanford.edu/pub/voy/museum/samuel.html.
Eliza, a chatbot therapist 2018 [updated 2018/07/18/]. Available from: https://web.njit.edu/~ronkowit/eliza.html.
van Melle W. MYCIN: a knowledge-based consultation program for infectious disease diagnosis. Int J Man-Mach Stud. 1978;10(3):313–22.
Cintula P, Fermüller CG, Noguera C. Fuzzy logic 2016 [updated 2016/11/15/]. Available from: https://plato.stanford.edu/entries/logic-fuzzy.
Lighthill report 2017 [updated 2017/12/20/]. Available from: http://www.chilton-computing.org.uk/inf/literature/reports/lighthill_report/contents.htm.
Weizenbaum J. Computer power and human reason: W.H. Freeman & Company; 1976.
Pollack A. Setbacks for artificial intelligence. NY Times; 1988.
Waibel A, Hanazawa T, Hinton G, Shikano K, Lang KJ. Phoneme recognition using time-delay neural networks. Readings in speech recognition. Morgan Kaufmann Publishers Inc.; 1990. p. 393–404.
Moravec H. Mind children. Cambridge, MA: Harvard University Press; 1990.
LeCun Y, Boser B, Denker JS, et al. Backpropagation applied to handwritten zip code recognition. Neural Comput. 1989;1(4):541–51.
Play Chinook—World man- machine checkers champion 2012 [updated 2012/03/08/]. Available from: https://webdocs.cs.ualberta.ca/~chinook/play.
IBM100—Deep blue. IBM corporation; 2012 [updated 2012/03/07/]. Available from: https://www.ibm.com/ibm/history/ibm100/us/en/icons/deepblue.
LOGISTELLO’ homepage 2011 [updated 2011/02/03/]. Available from: https://skatgame.net/mburo/log.html.
Oh K-S, Jung K. GPU implementation of neural networks. Pattern Recogn. 2004;37(6):1311–4.
Deng J, Dong W, Socher R, et al. ImageNet: a large-scale hierarchical image database. IEEE.
The DeepQA research team—IBM 2020 [updated 2020/11/06/]. Available from: https://researcher.watson.ibm.com/researcher/view_group_subpage.php?id=2160.
AlphaGo Zero: starting from scratch 2020 [updated 2020/11/06/]. Available from: https://deepmind.com/blog/article/alphago-zero-starting-scratch.
Brown T, Mane D, Roy A, Abadi M, Gilmer J. Adversarial patch. Google Research; 2017.
Su J, Vargas DV, Kouichi S. One pixel attack for fooling deep neural networks. arXiv. 2017.
Avati A, Jung K, Harman S, et al. Improving palliative care with deep learning. arXiv. 2017.
Krizhevsky A, Sutskever I, Hinton GE. ImageNet classification with deep convolutional neural networks. Commun ACM. 2017;60(6):84–90.
Simonyan K, Zisserman A. Very deep convolutional networks for large-scale image recognition. arXiv. 2014.
Szegedy C, Liu W, Jia Y, et al. Going deeper with convolutions. arXiv. 2014.
He K, Zhang X, Ren S, Sun J. Deep residual learning for image recognition. arXiv. 2015.
Datasets. Deep learning 2020 [updated 2020/11/06/]. Available from: http://deeplearning.net/datasets.
Artificial intelligence—Search results—PubMed 2020 [updated 2020/11/06/]. Available from: https://pubmed.ncbi.nlm.nih.gov/?term=artificial+intelligence&filter=years.1951-2020&timeline=expanded.
Hype cycle research methodology 2020 [updated 2020/11/06/]. Available from: https://www.gartner.com/en/research/methodologies/gartner-hype-cycle.
Machine learning—Search results—PubMed 2020 [updated 2020/11/06/]. Available from: https://pubmed.ncbi.nlm.nih.gov/?term=machine+learning&filter=years.1957-2020&timeline=expanded.
Deep learning—Search Results—PubMed 2020 [updated 2020/11/06/]. Available from: https://pubmed.ncbi.nlm.nih.gov/?term=deep+learning&filter=years.1954-2020&timeline=expanded.
Carin L, Pencina MJ. On deep learning for medical image analysis. JAMA. 2018;320(11):1192–3.
Yu M, Tham Y-C, Rim TH, et al. Reporting on deep learning algorithms in health care. Lancet Digit Health. 2019;1(7):e328–e9.
Liu Y, Chen P-HC, Krause J, Peng L. How to read articles that use machine learning: users’ guides to the medical literature. JAMA. 2019;322(18):1806–16.
Jaeschke R, Guyatt GH, Sackett DL, et al. Users’ guides to the medical literature: III. How to use an article about a diagnostic test B. what are the results and will they help me in caring for my patients? JAMA. 1994;271(9):703–7.
De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med. 2018;24(9):1342–50.
Moraes G, Fu DJ, Wilson M, et al. Quantitative analysis of OCT for neovascular age-related macular degeneration using deep learning. Ophthalmology. https://doi.org/10.1016/j.ophtha.2020.09.025.
Cabitza F, Rasoini R, Gensini GF. Unintended consequences of machine learning in medicine. JAMA. 2017;318(6):517–8.
Verghese A, Shah NH, Harrington RA. What this computer needs is a physician: humanism and artificial intelligence. JAMA. 2018;319(1):19–20.
Wang F, Casalino LP, Khullar D. Deep learning in medicine—promise, progress, and challenges. JAMA Intern Med. 2019;179(3):293–4.
Price WN II, Gerke S, Cohen IG. Potential liability for physicians using artificial intelligence. JAMA. 2019;322(18):1765–6.
Mandl KD, Manrai AK. Potential excessive testing at scale: biomarkers, genomics, and machine learning. JAMA. 2019;321(8):739–40.
Eveleth R. The Atlantic 2018 [updated 2018/04/05/]. Available from: https://www.theatlantic.com/technology/archive/2014/12/how-self-tracking-apps-exclude-women/383673.
How IBM Watson overpromised and underdelivered on AI health care—IEEE Spectrum 2020 [updated 2020/11/06/]. Available from: https://spectrum.ieee.org/biomedical/diagnostics/how-ibm-watson-overpromised-and-underdelivered-on-ai-health-care.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Thakur, S., Cheng, CY. (2021). A Clinician’s Introduction to Artificial Intelligence. In: Ichhpujani, P., Thakur, S. (eds) Artificial Intelligence and Ophthalmology. Current Practices in Ophthalmology. Springer, Singapore. https://doi.org/10.1007/978-981-16-0634-2_1
Download citation
DOI: https://doi.org/10.1007/978-981-16-0634-2_1
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-0633-5
Online ISBN: 978-981-16-0634-2
eBook Packages: MedicineMedicine (R0)