
Abstract
Infections by influenza virus constitute a major and recurrent threat for human health. Together with vaccines, antiviral drugs play a key role in the prevention and treatment of influenza virus infection and disease. Today, the number of antiviral molecules approved for the treatment of influenza is relatively limited, and their use is threatened by the emergence of viral strains with resistance mutations. There is therefore a real need to expand the prophylactic and therapeutic arsenal. This chapter summarizes the state of the art in drug discovery and development for the treatment of influenza virus infections, with a focus on both virus-targeting and host cell-targeting strategies. Novel antiviral strategies targeting other viral proteins or targeting the host cell, some of which are based on drug repurposing, may be used in combination to strengthen our therapeutic arsenal against this major pathogen.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
8.1 Introduction
Infections by influenza virus constitute a major and recurrent threat for human health. Influenza viruses are the causative agents of seasonal flu epidemics, associated with up to 1 billion infections and 300,000–650,000 deaths worldwide and consequently with a large economic price including hospitalization costs and missing working days [1, 2]. In addition, influenza A viruses (IAV) have been the cause of several pandemics in recent human history, from the Spanish flu H1N1 in 1918 to the more recent H1N1 2009 pandemic [3].
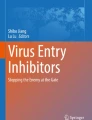
Together with vaccines, antiviral drugs play a vital part in the prevention and treatment of influenza virus infection and disease. During a normal influenza season, antiviral drugs are mainly used to treat critically ill patients, such as those hospitalized in intensive care. In a pandemic context, pending the availability of a vaccine, antiviral drugs are essential both to treat patients who have been infected and to prevent infection in those exposed, including healthcare workers. Today, the number of antiviral molecules approved for the treatment of influenza, based on the targeting of viral proteins, is relatively reduced and threatened by the emergence of strains with resistance mutations. There is therefore a real need to expand the prophylactic and reinforce the current therapeutic arsenal. This chapter summarizes the state of the art in drug discovery and development for the treatment of influenza virus infections, with a focus on both virus-targeting and host cell-targeting strategies (Fig. 8.1). Novel antiviral strategies targeting other viral proteins or targeting the host cell, some of which are based on drug repurposing, may be used in combination to strengthen our therapeutic arsenal against this major pathogen.

Influenza viral particle and viral cycle; current state of anti-influenza drug discovery and development. (a) Influenza A virus (IAV) particle. The IAV genome is composed of eight ribonucleoprotein complexes (vRNPs), composed of single-stranded negative-sense viral RNA (vRNA) encapsidated by viral nucleoprotein (NP) and a viral polymerase complex (PA, PB1, and PB2) positioned at the extremity of the vRNA segment. Three viral proteins, hemagglutinin (HA), neuraminidase (NA), and ion channel protein (M2), are embedded within the viral membrane. Matrix protein 1 (M1) holds the vRNPs inside the virion. (b) The viral particle binds to sialic acid receptors and enters the cell via receptor-mediated endocytosis. Acidification of the endocytic vesicles leads to virus uncoating mediated by the M2 ion channel. vRNPs are then released into the cytoplasm and transported into the nucleus. There, the viral RNA-dependent RNA polymerase complex snatches the host mRNA caps to initiate the negative vRNA transcription. Transcribed vRNAs then undergo an mRNA maturation phase, before export to the cytoplasm to be translated. vRNAs are also replicated in the nucleus to generate new vRNPs in association with neosynthesized viral proteins. Progeny vRNPs are transported toward the cytoplasmic membrane with viral components to be packaged into new infectious particles which are formed by cellular envelope budding. Classic virus-targeting strategies are highlighted in red and virus-host-targeted strategies in blue. Figure created by BioRender.com
8.2 From Existing Classic Antiviral Drugs to New Pre-Clinical Candidates
8.2.1 M2 Ion Channel Blockers (Amantadine/Rimantadine)
Influenza A M2 is a multifunctional viral homo-tetramer protein [4]. Its transmembrane (TM) domain forms a proton channel. This channel is required for the acidification of the viral endosome formed after fusion and endocytosis of the virus within the host cell. This process allows viral ribonucleoproteins (vRNPs) to dissociate from the matrix 1 (M1) protein. The proton conductance mechanism relies on the conserved H37XXXW41 sequence which is responsible for selectively gating H+ ions [5,6,7,8]. Channel blockers interfere with the proton conductance mechanism by binding to the transmembrane pore [9] (Fig. 8.2). When proton conductance through M2 is blocked by the adamantane drug, this dissociation is prevented, and the virus is no longer able to replicate. In recent years, adamantane drug-resistant mutants have become prevalent in circulating viruses. The most prevalent drug-resistant mutations are S31N, L26F, and V27A, all of which are located in the transmembrane region of M2 [11]. Figure 8.2a shows the strong interaction of amantadine with V27 in the upper part of the pore. Upon drug resistance V27A mutation, this interaction is lost. Recently developed spiro-amantadyl amine effectively binds to A27 of the pore (Fig. 8.2b) [10]. Recently, new amantadine derivatives effective against double mutants M2-S31N/L26I and M2-S31N/V27A viral strains have been developed by Musharrafieh et al. [12]. The antiviral efficacy of such compounds is summarized in Table 8.1. As a consequence of resistance mutations that appeared in M2 in H1N1/H3N2 circulating strains, both amantadine and rimantadine were removed from the WHO list of recommended anti-influenza agents for clinical use in 2009 [23].

Looking down the M2 channel in the presence of inhibitors: Structure of M2 WT and VA27 mutant in complex with amantadine and spiroamantadine. View down the pore channel in (a) WT-amantadine (V27 is colored in yellow, PDB ID 6BKK [9]) and (b) V27A-spiroamantadine complexes (A27 is colored in yellow, PDB ID 6NV1 [10])
8.2.2 Neuraminidase (NA) and Hemagglutinin (HA) Inhibitors
8.2.2.1 NA Inhibitors
NA inhibitors competitively inhibit terminal sialic acid residue removal from glycoproteins and carbohydrates found at the surface of host (mammalian) cells and influenza virus particles. Binding of virions to intact (uncleaved) sialic acid inhibits virion release. Among these NA inhibitors, peramivir, zanamivir, and oseltamivir carboxylate are the most frequently prescribed drugs and considered standard of care for influenza management (Table 8.1 and Fig. 8.3). Resistance to oseltamivir can be observed experimentally in a few cell passages and also found in the clinic. Typically, resistance originates from substitutions in the viral NA protein such as H274Y and I223R (predominant in H1N1 and H5N1 viruses) and E119V, R292K, or N294S (predominant in H3N2 viruses). Oseltamivir, peramivir and zanamivir are three NA inhibitors currently approved worldwide for the treatment of influenza A and B infections, oseltamivir being the most widely used. There is still a lot of debate about the effectiveness and real impact of inhibitors on the prevention and treatment of influenza. New oseltamivir derivatives, targeting either multiple sites or different NA cavities (as the “430” or the “150” cavity), have been recently developed. Some of these derivatives are very potent against multiple IAV and IBV strains, including oseltamivir-resistant ones (Table 8.1).

Structures of the approved NA inhibitors
8.2.2.2 Hemagglutinin Inhibitors
The surface glycoprotein HA is associated with viral entry into host cells. HA binding to cell-surface, sialic-acid-containing glycans further enables fusion between the viral and host membranes in endosomal compartments. HA is composed of head (HA1) and stem (HA2/HA1) domains. As the regions on HA involved in binding and fusion are highly conserved, they are attractive sites for the design of new antivirals (Table 8.2). The broad-spectrum antiviral drug arbidol shows efficacy against influenza viruses by targeting the hemagglutinin (HA) stem region [24]. This molecule is currently licensed in Russia and China for the treatment of influenza and other infections [35]. A challenging strategy aiming at mimicking antibodies binding sites was successfully developed by Wilson et al., targeting the conserved stem region and more recently at the interface of the trimeric head region [13, 27, 36] (Fig. 8.4a). The binding sites of the binding sites for CBS1117 and JNJ4796 were both found in the stem region close to the fusion peptide, highlighting the possibility of further structure-based designed compounds [29]. De novo design of high-affinity trimeric proteins called “HA mini-binders” that bind influenza A hemagglutinin trimer at a conserved region binding site (Fig. 8.4b) [33]. These molecules were developed as alternative to antibodies. These and other compounds are summarized in Table 8.2.

8.2.3 Polymerase/Nucleoprotein/RNA inhibitors
8.2.3.1 Polymerase/Endonuclease Inhibitor (Favipiravir, Baloxavir Marboxil)
Influenza viruses transcribe and replicate their genome in the nucleus of infected cells by the means of a hetero-trimeric polymerase, PA, PB1, and PB2. The polymerase complex function requires the nucleoprotein NP, a protein associated with and protecting the segmented genomic RNA. Therefore, all four proteins are essential for replication. Whereas replication requires the generation of complementary positive polarity RNA intermediates (cRNA) that are then copied into progeny negative polarity segments (vRNPs), viral message is directly synthesized from vRNPs. Since the influenza virus polymerase is unable to form 5′ mRNA cap structures, its subunit PA is necessary for the generation of viral mRNAs via its endonuclease activity, transferring host mRNAs 5′-capped RNA primers in a cap-snatching mechanism. The endonuclease active site of PA-N terminal comprises a histidine and a cluster of three strictly conserved acidic residues (Glu80, Asp108, Glu119), which coordinate (together with Ile120) one or two manganese or magnesium ions [37] (Fig. 8.5a). PB2 binds capped primers, the enzymatic activity for phosphodiester bond formation being associated with the PB1 subunit.

Structure of some of the pre-clinical candidates targeting the polymerase. (a) Active-site PA N-terminal inhibitor compound 22 [38]; (b) PB2 inhibitor pimodivir [39] (the numbering is associated with this structure corresponding to the full-length PB2); (c) nucleozin-NP oligomeric complex PDB ID 5B7B; monomers A and B are in cyan and yellow, respectively; (d): naproxen F1-NP monomeric complex from docking studies [40]
Several classes of inhibitors are in the clinics (Fig. 8.6): baloxavir (PA), favipiravir (PB1), and pimodivir (PB2, Fig. 8.5b).

Structures of the approved polymerase inhibitors and some pre-clinical candidates
8.2.3.2 Pre-clinical Compounds Targeteinf the Polymerase PA, PB1 and PA subunits, Escape Mutations and Resistance
Pre-clinical candidates, some of them being listed in Tables 8.3 and 8.4, are in development, benefiting from the recent insight provided by the structures of PA-PB1, PB1-PB2, and whole polymerase complex with or without RNA by X-ray crystallography [71,72,73,74,75,76,77] and cryo-electron microscopy [78,79,80,81,82]. The error-prone nature of influenza viral replication can rapidly generate point mutants for the selection of resistance that have seriously compromised the efficacy of influenza therapeutics. Escape mutations were identified under the pressure selection of PA inhibitors: the hotspot mutation for escape from baloxavir marboxil is located at PA residue 38, including several substitutions (PA I38T/M/F) [41]. Similarly, escape mutations from L-742.001 [42] and RO-7 [44] treatments were also characterized although in laboratory resistance assays, escape mutants were not detected after multiple passages for L-742.001. While very tight affinities have been achieved by designing metal binding inhibitors to block the active site of the endonuclease activity in PA N-terminal (Table 8.2), the appearance of escape mutants often rapidly decreases their efficacy. Several recent reviews focus on the development of PA and polymerase inhibitors [83,84,85,86].
Different strategies have been undertaken to attempt overcoming induced resistance. Interfering with its proper assembly of the RdRP polymerase to inhibit function is pursued using protein-protein interaction (PPI) inhibitors. The advantage of such an approach is the relatively large interacting surface between the two proteins as compared to the binding site of an active-site ligand. Indeed, inducing simultaneous mutation of at least one residue on both proteins while maintaining their interaction is less likely to develop resistance and suggests that PPI inhibitors could be less prone to drug resistance than inhibitors of enzyme active sites. The recent identification of a single- domain antibody (nanobody) allowing to disrupt dimerization of FluA polymerase is among these lines [79]. PPI inhibitors have been developed based on the structural insight given by PA-PB1 crystal structures in 2012 [87]. The inhibition of the polymerase PA-PB1 subunit interface has become an active field of research with the goal of remaining active against resistant strains to amantadine and to oseltamivir (Table 8.3). Recently, compound 12 was identified by structure-based screening of compounds targeting the PA-PB1 structure. No resistant virus was selected in vitro under drug selection pressure of compound 12a [48]. Moreover, derivatives of cyclothiophene and R151785 were found active against multiple strains of influenza A and B [50,51,52].
Based on the ability of PA-PB1 to bind viral RNA, it is likely that novel types of inhibitors could be developed by structure-based design [88]. Additionally, inhibitors targeting PA C-terminal [47] and its interactions with vRNA or with PolII could be effective targets, based on the accumulating wealth of structural data [74, 75, 79, 82] and deeper insight in the multi-protein assembly required during replication/transcription.
8.2.3.3 Broad-Spectrum Inhibitors
Favipiravir inhibits RNA viruses of the arenavirus, bunyavirus, flavivirus, alphavirus, norovirus, picornavirus, paramyxovirus, and rhabdovirus families, in addition to influenza viruses; therefore, it is considered as a broad-spectrum drug [53]. This drug is incorporated into newly synthesized RNA by the viral polymerase in place of purines but not pyrimidines, resulting in increased frequencies of C-to-U and G-to-A transition mutations. Although the barrier for resistance is relatively high, this drug seems to present toxicity issues. N4-Hydroxycytidine (NHC) inhibits RSV and both highly pathogenic avian and seasonal influenza viruses as well as SARS-CoV-2 virus, thus being also a broad-spectrum antiviral candidate with oral efficacy [55].
8.2.3.4 Pre-Clinical Compounds Targeting the Polymerase PB2 Subunit
Crystal structure of the PB2 cap-binding domain has been exploited to develop different 7-methylguanine derivatives [59]. Pimodivir (VX-787) is an inhibitor targeting the polymerase PB2 subunit at the m7 GTP-binding site, forming extensive stacking interactions with several aromatic residues His (Figs. 8.5b and 8.6). It inhibits influenza virus replication and reduced viral load in animal infection models of H3N2 and H1N1 viruses, although potency was highest against H1N1 strains [39, 56]. Phase II clinical studies indicated that this drug is well-tolerated, reduced viral load, and resulted in slightly faster resolve of clinical signs. Further derivatives of pimodivir have been designed [57]. Targeting the PB1-PB2 interface by PPI inhibitors has been challenging: although PP7 exhibited antiviral activities against influenza virus subtypes A pandemic H1N1, H7N9, and H9N2, resistances have been unexpectedly detected in laboratory assays [60].
8.2.3.5 Pre-Clinical Compounds Targeting the Nucleoprotein or the Nucleoprotein-RNA Interactions
The nucleoprotein associated with viral RNA and the polymerase complex is essential for transcription and replication [77, 89, 90]. The assembly of NP-RNA oligomers into RNP has been determined by cryo-electron microscopy studies [77, 78, 89, 91]. In the X-ray structures of the NP [92], the protein adopts a trimeric structure. NP self-association to achieve trimer formation is mediated by a flexible tail loop that protrudes into a pocket of the adjacent subunit, via the formation of a critical interaction between R416 of one subunit and E339 of the adjacent subunit. The R416A mutant lacking this interaction adopts a monomeric structure [93]. The native protein can also be purified in a monomeric form at low salt and concentration conditions [93,94,95]. The ability to modify the oligomeric state of NP is the structural basis of most NP inhibitors presently developed. Nucleozin was the first NP inhibitor developed as a molecule impeding nuclear accumulation. Nucleozin enhanced higher-order structures [61, 63]. Figure 8.5c shows the interactions of one of the nucleozin ligands found in the X-ray structure (PDB ID 5B7B) stabilizing the interface between two NP subunits [62]. Escape mutants to nucleozin have been identified in laboratory assays. The opposite approach to impede nucleoprotein self-association has also been pursued by disrupting the important salt bridge R416-E339 mediating NP oligomerization [64]. Recently, new compounds with high affinity for NP were designed stabilizing monomeric NP [65]. Impeding NP binding to viral RNA has been achieved by naproxen drug repurposing, naproxen being a known inhibitor of cyclooxygenase (COX) [66]. As NP oligomerization is enhanced by the presence of RNA, naproxen binding to NP reduced NP oligomers and favored monomeric NP. Docking and single mutation studies identified Tyr148, the only aromatic residue within the RNA binding groove, and residues of the C-terminal part of NP R355, R361 and Phe489 being involved in the interaction of naproxen with NP. Laboratory assays showed no resistance after eight cell passages infected with influenza A. Naproxen exhibited antiviral effects in mice models of influenza A infection [40, 66] as well as influenza B virus [96]. Further structure-based design yielded new naproxen derivatives with improved antiviral effects and selectivity for NP without COX inhibition (Figs. 8.5d and 8.6) [40, 67] (Table 8.4). Some of these derivatives were found inhibiting NP-PA interactions [40, 97]. Naproxen derivatives also present antiviral properties against oseltamivir-resistant strains [40]. Additional compounds with some similarity of their hydroxyquinoline scaffold to the methoxynaphthalene scaffold of naproxen called NUD were designed and were also found to be resistant in escape mutation laboratory assays [68].
8.2.4 Drugs Targeting the Non-structural Protein-1 (NS1)
NS1 has a plethora of strategies to inhibit the host immune response due to its ability to establish multiple protein-protein and protein-RNA interactions. NS1 hampers different pathways both in the cytoplasm and in the nucleus of infected cells. NS1 antagonizes interferon-mediated antiviral host response by binding to double-stranded (ds) viral RNA, thus protecting it from cellular factors, by blocking retinoic acid-inducible gene-I (RIG-I) and NF-kB activation. One pathway by which NS1 increases virulence is through the activation of phosphoinositide 3-kinase (PI3K) by binding to its p85β subunit [98]. NS1 has two structural domains – RNA-binding domain (RBD) and the effector domain (ED) – connected by a short linker (LR) and a disordered C-terminal tail. New drugs binding to NS1 effector domain have been designed with low micromolar antiviral efficacy [69] (Table 8.4).
8.3 Host-Targeting and Drug Repurposing Approaches for the Treatment of Influenza
Considerable progress has been made in understanding the interactions between influenza viruses and the host cell in recent years. In this context, and in light of the emerging problem of resistance to available classical antivirals, many studies have focused on targeting host factors to limit virus replication, but also to modulate host immune response. The targeting of host factors and/or signaling pathways makes sense in the context of virally induced hypercytokinemia (also known as “cytokine storm”), which is directly correlated with tissue injury and an unfavorable prognosis of severe influenza [99]. Indeed, approaches to control or attenuate this disproportionate immune response are of particular interest and are the subject of numerous pre-clinical and clinical studies. As with all viruses, influenza viruses depend on cellular machinery for their replication and propagation. Many cellular factors essential for the replication of influenza viruses have been uncovered through genome-wide RNA interference approaches [100,101,102,103] but also more broadly through different integrated cell biology approaches using interactome and transcriptome data, for example [104, 105]. In order to list the different host-targeting strategies developed, a distinction can be made between molecules with a mode of action associated with a relatively well-defined stage of the viral cycle and molecules associated with the modulation of signaling pathways. It is these two main classes that will be described in the following sections.
8.3.1 Drugs Targeting Host Cell Component at Different Stages of Influenza Replication Cycle
The replication cycle of influenza viruses consists in distinct successive phases, 1) entry, 2) nuclear import of viral genome (viral ribonucleoprotein; vRNPs), 3) genome replication and protein synthesis, 4) nuclear-cytoplasmic export of vRNPs, and 5) plasma membrane transport and budding of neo-virions (Fig. 8.1). A number of molecules targeting host factors in these different steps, at different pre-clinical/clinical development stages, are known today.
Viral entry is a target of great interest, as it is likely to allow prophylactic approaches, by blocking the infection in its early stages. One of the most advanced strategies consists to target the viral receptor. DAS181 (Table 8.5) (Fludase, Ansun BioPharma) is a sialidase fusion protein that cleaves both the Neu5Ac α(2,3)- and Neu5Ac α(2,6)-Gal linkages of sialic acid on host cells. DAS181 is administered as an inhalable dry powder to deliver sialidase to the pulmonary epithelium for cleavage of sialic acids, which renders the cells inaccessible to infection by virus [131]. DAS181 was demonstrated to have broad-spectrum activity, given the conserved nature of influenza and parainfluenza viruses binding to respiratory epithelium. Pre-clinical in vitro and in vivo studies demonstrated that DAS181 has activity against a number of seasonal influenza strains including those containing the H274Y mutation (conferring resistance to oseltamivir), highly pathogenic avian influenza strains (H5N1), and pandemic 2009 influenza A (H1N1). This compound was assessed in different Phase I and Phase II clinical trials (NCT00527865, NCT01651494, NCT01037205) with results indicating a significant reduction of viral load in treated influenza patients [106] but with identification of respiratory adverse events and rapid clearance of the drug being consistent with the induction of antibodies against DAS-181 – this could be a limitation in the duration and dosages of such treatment [107]. Other approaches targeting viral entry have also been described (Table 8.5), e.g., targeting the endosome acidification step by inhibition of V-ATPase (e.g., bafilomycin A1, concanamycin) or inhibition of the internalization (e.g., Dynasore) or cleavage steps of hemagglutinin (e.g., camostat). Most of these strategies were primarily evaluated at the pre-clinical stage and have not been further evaluated as their efficacy was either limited or accompanied by cytotoxicity. One exception is the protease inhibitor aprotinin, which was approved as anti-influenza drug in Russia [112].
The step of nuclear import of vRNPs is a crucial one, for which there are today very few molecules with antiviral potential described in literature. Interestingly, it has been shown in vitro that ivermectin (Table 8.5), a well-known anti-parasite drug, was able to inhibit viral replication via inhibition of importins (IMPα/β) and therefore the nuclear import of vRNPs [116].
Targeting the replication stage of the virus is one of the earliest host-targeting strategies, with pioneer works on the antiviral efficacy of ribavirin in the 1970s [119]. However, this nucleoside analogue and its prodrug, less toxic, do not appear to be options being considered for the treatment of influenza virus infections of influenza viruses, despite interesting preliminary in vitro and in vivo results [120] (Table 8.5). Other, more recent strategies propose to target mRNA splicing. Influenza viruses are known to hijack cellular splicing machinery to their benefit, making them extremely dependent on it [132, 133]. Several studies show that the inhibition of Cdc2-like kinase 1 (CLK1), involved in the alternative splicing of M2 gene of influenza, appears to be an interesting antiviral option, with several molecules available (TG003, clypearin, corilagin, Table 8.5). Of all its molecules, clypearin has relatively low EC50s and very low toxicity, making it an attractive potential antiviral candidate [100, 117].
While strategies to prevent the nuclear import of vRNPs are relatively uncommon, paradoxically there are many more therapeutic approaches to block the nuclear-cytoplasmic transport of vRNPs. Indeed, in contrast to the inhibition of importins, the inhibition of exportin 1 (XPO1) by verdinexor (XPO1 antagonist KPT-335) allows to significantly reduce viral production in vitro and in vivo [121]. Another compound, DP2392-E10, inhibits nuclear export of both viral NP and nuclear export protein (NEP). More specifically, in vitro pull-down assays revealed that DP2392-E10 directly binds cellular CRM1, which mediates nuclear export of NP and NEP – highlighting CRM1 as a target of interest [122]. With the same objective, other strategies consist to target the Raf/MEK/ERK signaling pathway, known to be involved in the export of vRNPs [134]. Several MEK inhibitor molecules have been studied for their ability to inhibit the replication of influenza viruses, such as CI-1040 or U0126 [124, 125]. Interestingly, Schräder and colleagues have demonstrated that trametinib (GSK-1120212), a licensed MEK inhibitor used for the treatment of malignant melanoma, efficiently blocks influenza viral replication of different subtypes in vitro and in vivo [126] (Table 8.5).
Apical transport and budding, the last part of the last major step of the replication cycle, is also the object of several antiviral strategies, notably by blocking the transport of viral proteins to the plasma membrane (e.g., clonidine; [130]) or the cholesterol pathway, which would reduce virion egress (U18666A; [129]). One of the most advanced strategies is nitazoxanide, which was first approved for parasite infections’ treatment. Its antiviral properties against influenza virus were first reported by Rossignol et al. [128]. Interestingly, the proposed mode of action of nitazoxanide against influenza clearly differs from its anti-parasitic effects, acting at the post-translational level by selectively blocking the maturation of the viral glycoprotein HA. Consecutively, it impacted on intracellular trafficking and insertion into the host plasma membrane [135]. This drug is a potent antiviral against a large panel of circulating strains [136]. A Phase IIb/III trial showed the efficacy of nitazoxanide in treating patients with non-complicated influenza [137], with a further, currently assessed, Phase III clinical trial (NCT01610245).
8.3.2 Drugs Targeting Host Cell Signaling Pathways and Host Response that Are Crucial for Influenza Replication Cycle
Our increased knowledge of signaling pathways that are crucial in the response to infection and/or those hijacked by the virus has allowed many research teams to explore complementary antiviral strategies that can be described here (Table 8.6). The targeting of the ref./MEK/ERK channel, mentioned above, could of course also have been listed here. At the crossroads of the regulatory pathways of the immune response and the stress response, the NF-kB pathway was one of the first to be studied (Table 8.6). In the context of cell biology approaches, it was initially shown that the anti-inflammatory drug acetylsalicylic acid (ASA) had interesting antiviral effect against influenza viruses in vitro and in vivo, via inhibition of the NF-kB activating IkkB kinase [138, 157, 158]. Several drugs targeting the NF-kB pathway have been evaluated since then, such as pyrrolidine dithiocarbamate or SC7574, with encouraging in vivo results [123, 139, 140]. BAY81–8781/LASAG (D,L-lysine acetylsalicylate-glycine) (Table 8.6), a modified version of ASA, demonstrates in vitro antiviral activity against several human and avian influenza viruses. In a mouse infection model, inhalation of LASAG reduced lung viral titers and protected mice from lethal infection [141]. More recently, a Phase II proof-of-concept trial compared LASAG versus placebo in patients with severe influenza. Aerosolized LASAG was demonstrated improving the time to symptom alleviation compared to placebo, although the reduction of viral load in LASAG-treated group was not statistically significant [142].
Based on clinical observations, 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors such as statins (Table 8.6), approved for indication of cholesterol metabolism regulators, have demonstrated pleiotropic anti-inflammatory and immunomodulatory properties, which could increase survival of patients with severe influenza [145, 146]. However, most in vivo studies reported so far failed to clearly demonstrate such a beneficial effect for influenza patients [159,160,161]. Nevertheless, an association between statin treatment with a reduction of mortality in patients hospitalized with laboratory-confirmed seasonal influenza was highlighted in observational studies [162, 163]. A randomized placebo-controlled Phase II clinical trial (NCT02056340) to evaluate the potential beneficial effect of atorvastatin in improving the status severely-ill influenza-infected patients is currently undergoing. The combination of naproxen with clarithromycin and oseltamivir twice daily reduced the both 30- and 90-day mortality and length of hospital stay of patients hospitalized for A(H3N2) influenza [164]. Other approaches, at the pre-clinical validation stages, propose to target the TNF-alpha (etanercept) or NOX2 (apocynin/ebselen) or lipoxygenase/COX pathway (celecoxib/mesalazine) pathways [147,148,149,150,151,152, 165]. A Phase III clinical trial is currently investigating the benefit of celecoxib for the treatment of severe influenza (NCT02108366). These molecules could be of interest to better control the inflammatory response, which is a very important aspect of the pathology.
Modulation of immune and inflammatory responses is a therapeutic avenue that has been much explored, but which may present risks given the ambivalent aspect of these pathways in relation to viral replication and the evolution of the pathology. Indeed, such treatment should stimulate induction of antiviral genes to control IAV spread, without driving immunopathology. In this context, IFN-lambda (Table 8.6) appears as a potent anti-influenza therapeutic, without the inflammatory side effects of IFN-alpha treatment [153]. Intranasal administration of IFN-λ2/3 was shown to significantly suppress infection of various influenza strains, including WS/33 (H1N1), PR (H1N1), and H5N1 in the mouse lung, and was accompanied by greater upregulation of ISGs [154]. More recently, using a transcriptome-based screening approach, we identified and validated diltiazem, a calcium channel blocker used as an anti-hypertensive drug, as a very promising host-targeted inhibitor of influenza infection. Interestingly, the study of the mode of action revealed that diltiazem was a strong induced or type III IFN [156]. An ongoing French multicenter randomized clinical trial is investigating the effect of diltiazem oseltamivir bi-therapy compared with standard oseltamivir monotherapy for the treatment of severe influenza infections in intensive care units (FLUNEXT trial NCT03212716).
8.4 Perspectives and Concluding Remarks
Among all the molecules listed in this chapter, some are already available on the market for other therapeutic indications and fall within the scope of drug repurposing. This is the case for naproxen, diltiazem, LASAG, or nitazoxanide, for example. Drug repurposing bypasses the long, risky, and expensive pre-clinical studies, an early clinical evaluation stage conventionally used for de novo drug development. It takes advantage of available resources, as extensive human clinical, pharmacokinetics, and safety data, as the starting point for the development [155] All these aspects make the repositioning of drugs a very interesting approach, in particular to enable a rapid response to the need for new antiviral strategies in the context of the emergence of a virus with pandemic potential.
Another very interesting perspective is the interest in combining different antiviral approaches with each other, including classical approaches targeting the virus with those targeting the host cell. The concept of combining therapies has already been used successfully, notably in the design of antiretroviral treatments [166]. Combination therapy can have several objectives, such as reducing the risk of the emergence of resistance by simultaneously targeting several viral proteins and/or key host factors, but also increasing the effectiveness of the treatments by obtaining additive or synergistic effects.
While there is relatively little convincing evidence to support the use of conventional virus-targeting antivirals in combination [167, 168], there are interestingly a growing number of examples of combinations of oseltamivir with host-targeted approaches. For example, we have shown that the combination of diltiazem and oseltamivir provides a much greater reduction in viral titers in a reconstructed human epithelium model compared to single treatments [156]. More recently, Schloer and colleagues have shown that a combination treatment of an antifungal molecule, itraconazole, with oseltamivir achieves much greater antiviral activity compared to monotherapy, making it possible to consider reducing the concentrations of drugs used and thus possibly reducing the problems of adverse effects and emergence of resistance mutations [169]. These results open up interesting prospects for the development of future therapeutic strategies, particularly for the treatment of severe forms of influenza. The potential arsenal for fighting influenza virus infections is potentially very extensive, in particular thanks to the combination of new molecules targeting the virus, resulting from docking and structure-based design strategies, with approaches targeting cellular factors and signaling pathways. In this context, the quality and relevance of the pre-clinical models, as well as the quality of the tools for evaluating combinations of molecules, are important critical elements.
Beyond influenza viruses, many of the antiviral molecules described in this chapter have the potential for broader-spectrum use. Indeed, some virus-targeted strategies can target viral determinants with very strong similarities between different viruses. This is particularly the case with naproxen for which we have previously demonstrated antiviral activity against both influenza viruses and SARS-CoV-2 [66, 170]. This property is explained by the fact that the nucleoproteins N of enveloped, positive-sense, single-stranded viruses coronavirus (CoV) share with negative-sense single-stranded viruses such as influenza A virus the ability to bind to and protect genomic viral RNA without sequence specificity and to form self-associated oligomers. Despite their differences, viruses induce and divert many common cellular pathways. As a result, host-targeted approaches can identify molecules with a broad spectrum of antiviral activity. An example is diltiazem, for which we have shown antiviral activity against influenza viruses [156], but which has been shown to be effective against other respiratory viruses, such as SARS-CoV-2 [171, 172], due to its mode of action involving the type III interferon response. Efforts to identify anti-influenza molecules therefore open up very interesting prospects for the broader development of antivirals. In many ways, antiviral research on influenza viruses is pioneering in this area and provides a starting point for the study of other emerging viruses.
Abbreviations
- CoV:
-
Coronavirus
- COX:
-
Cyclooxygenase
- HA:
-
Hemagglutinin
- IAV:
-
Influenza A virus
- IFN:
-
Interferon
- M2:
-
Matrix 2
- NA:
-
Neuraminidase
- NOX:
-
NADPH oxidase
- NP:
-
Nucleoprotein
- p09:
-
H1N1 2009-pandemic strain
- PA:
-
Polymerase acidic subunit
- PB1:
-
Polymerase basic subunit 1
- PB2:
-
Polymerase basic subunit 2
- PPI:
-
Protein-protein interaction
- RdRP:
-
RNA-dependent ribonucleoprotein complex
- RIG-I:
-
Retinoic acid-inducible gene-I
- TNF-α:
-
Tumor necrosis factor-α
- vRNP:
-
Viral ribonucleoproteins
References
Iuliano AD, Roguski KM, Chang HH et al (2018) Estimates of global seasonal influenza-associated respiratory mortality: a modelling study. Lancet 391:1285–1300
World Health Organization (2018) Influenza (seasonal). http//www/cho.int/fact-sheets/details/influenza-(seasonal). Accessed 18 Jul 2020
Krammer F, Smith GJD, Fouchier RM et al (2018) Influenza. Nat Rev Dis Primers 4:3
Jalily PH, Duncan MC, Fedida D et al (2020) Put a cork in it: plugging the M2 viral ion channel to sink influenza. Antiviral Res 178:104780
Hu F, Luo W, Hong M (2010) Mechanisms of proton conduction and gating in influenza M2 proton channels from solid-state NMR. Science 330:505–508
Mould JA, Li HC, Dudlak CS et al (2000) Mechanism for proton conduction of the M(2) ion channel of influenza A virus. J Biol Chem 275:8592–8599
Sharma M, Yi M, Dong H et al (2010) Insight into the mechanism of the influenza A proton channel from a structure in a lipid bilayer. Science 330:509–512
Tang Y, Zaitseva F, Lamb RA et al (2002) The gate of the influenza virus M2 proton channel is formed by a single tryptophan residue. J Biol Chem 277:39880–39886
Thomaston JL, Polizzi NF, Konstantinidi A et al (2018) Inhibitors of the M2 proton channel engage and disrupt transmembrane networks of hydrogen-bonded waters. J Am Chem Soc 140:15219–15226
Thomaston JL, Konstantinidi A, Liu L et al (2020) X-ray crystal structures of the influenza M2 Proton Channel drug-resistant V27A mutant bound to a Spiro-Adamantyl amine inhibitor reveal the mechanism of Adamantane resistance. Biochemistry 59:627–634
Thomaston JL, Wu Y, Polizzi N et al (2019) X-ray crystal structure of the influenza a M2 Proton Channel S31N mutant in two conformational states: an open and shut case. J Am Chem Soc 141:11481–11488
Musharrafieh R, Ma C, Wang J (2020) Discovery of M2 channel blockers targeting the drug-resistant double mutants M2-S31N/L26I and M2-S31N/V27A from the influenza A viruses. Eur J Pharm Sci 141:105124
Yao Y, Kadam RU, Lee CD et al (2020) An influenza A hemagglutinin small-molecule fusion inhibitor identified by a new high-throughput fluorescence polarization screen. Proc Natl Acad Sci U S A 117:18431–18438
Cady SD, Schmidt-Rohr K, Wang J et al (2010) Structure of the amantadine binding site of influenza M2 proton channels in lipid bilayers. Nature 463:689–692
Schnell JR, Chou JJ (2008) Structure and mechanism of the M2 proton channel of influenza a virus. Nature 451:591–595
Russell RJ, Haire LF, Stevens DJ et al (2006) The structure of H5N1 avian influenza neuraminidase suggests new opportunities for drug design. Nature 443:45–49
Collins PJ, Haire LF, Lin YP et al (2008) Crystal structures of oseltamivir-resistant influenza virus neuraminidase mutants. Nature 453:1258–1261
Li P, Du R, Wang Y et al (2020) Identification of Chebulinic acid and Chebulagic acid as novel influenza viral neuraminidase inhibitors. Front Microbiol 11:182
Ai W, Zhang J, Zalloum WA et al (2020) Discovery of novel "dual-site" binding oseltamivir derivatives as potent influenza virus neuraminidase inhibitors. Eur J Med Chem 112147:191
Jia R, Zhang J, Ai W et al (2019) Design, synthesis and biological evaluation of “multi-site”-binding influenza virus neuraminidase inhibitors. Eur J Med Chem 178:64–80
Zhang J, Poongavanam V, Kang D et al (2018b) Optimization of N-substituted Oseltamivir derivatives as potent inhibitors of Group-1 and -2 influenza a neuraminidases, including a drug-resistant variant. J Med Chem 61:6379–6397
Ju H, Xiu S, Ding X et al (2020) Discovery of novel 1,2,3-triazole oseltamivir derivatives as potent influenza neuraminidase inhibitors targeting the 430-cavity. Eur J Med Chem 187:111940
Dong G, Peng C, Luo J et al (2015) Adamantane-resistant influenza a viruses in the world (1902-2013): frequency and distribution of M2 gene mutations. PLoS One 10:e0119115
Kadam RU, Wilson IA (2017) Structural basis of influenza virus fusion inhibition by the antiviral drug Arbidol. Proc Natl Acad Sci U S A 114:206–214
Wang Y, Ding Y, Yang C et al (2017) Inhibition of the infectivity and inflammatory response of influenza virus by Arbidol hydrochloride in vitro and in vivo (mice and ferret). Biomed Pharmacother 91:393–401
Wright ZVF, Wu NC, Kadam RU et al (2017) Structure-based optimization and synthesis of antiviral drug Arbidol analogues with significantly improved affinity to influenza hemagglutinin. Bioorg Med Chem Lett 27:3744–3748
Van Dongen MJP, Kadam RU, Juraszek J et al (2019) A small-molecule fusion inhibitor of influenza virus is orally active in mice. Science 363:eaar6221
Kim JI, Lee S, Lee GY et al (2019) Novel small molecule targeting the hemagglutinin stalk of influenza viruses. J Virol 93:e00878-19
Antanasijevic A, Durst MA, Cheng H et al (2020) Structure of avian influenza hemagglutinin in complex with a small molecule entry inhibitor. Life Sci Alliance 3(8):e202000724
Gaisina IN, Peet NP, Cheng H et al (2020) Optimization of 4-aminopiperidines as inhibitors of influenza a viral entry that are synergistic with Oseltamivir. J Med Chem 63:3120–3130
Hussein AFA, Cheng H, Tundup S et al (2020) Identification of entry inhibitors with 4-aminopiperidine scaffold targeting group 1 influenza a virus. Antiviral Res 177:104782
Basu A, Komazin-Meredith G, Mccarthy C et al (2017) Molecular mechanism underlying the action of influenza a virus fusion inhibitor MBX2546. ACS Infect Dis 3:330–335
Strauch EM, Bernard SM, La D et al (2017) Computational design of trimeric influenza-neutralizing proteins targeting the hemagglutinin receptor binding site. Nat Biotechnol 35:667–671
Wu G, Yu G, Yu Y et al (2020) Chemoreactive-inspired discovery of influenza a virus dual inhibitor to block Hemagglutinin-mediated adsorption and membrane fusion. J Med Chem 63:6924–6940
Blaising J, Polyak SJ, Pecheur EI (2014) Arbidol as a broad-spectrum antiviral: an update. Antiviral Res 107:84–94
Bangaru S, Lang S, Schotsaert M et al (2019) A site of vulnerability on the influenza virus Hemagglutinin head domain trimer interface. Cell 177:1136–1152.e1118
Dias A, Bouvier D, Crepin T et al (2009) The cap-snatching endonuclease of influenza virus polymerase resides in the PA subunit. Nature 458:914–918
Credille CV, Morrison CN, Stokes RW et al (2019) SAR exploration of tight-binding inhibitors of influenza virus PA endonuclease. J Med Chem 62:9438–9449
Clark MP, Ledeboer MW, Davies I et al (2014) Discovery of a novel, first-in-class, orally bioavailable azaindole inhibitor (VX-787) of influenza PB2. J Med Chem 57:6668–6678
Dilly S, Fotso Fotso A, Lejal N et al (2018) From naproxen repurposing to naproxen analogues and their antiviral activity against influenza a virus. J Med Chem 61:7202–7217
Omoto S, Speranzini V, Hashimoto T et al (2018) Characterization of influenza virus variants induced by treatment with the endonuclease inhibitor baloxavir marboxil. Sci Rep 8:9633
Song MS, Kumar G, Shadrick WR et al (2016) Identification and characterization of influenza variants resistant to a viral endonuclease inhibitor. Proc Natl Acad Sci U S A 113:3669–3674
Jones JC, Kumar G, Barman S et al (2018) Identification of the I38T PA substitution as a resistance marker for next-generation influenza virus endonuclease inhibitors. mBio 9:e00430-18. Erratum in: mBio. 2018 Nov 13;9(6)
Kowalinski E, Zubieta C, Wolkerstorfer A et al (2012) Structural analysis of specific metal chelating inhibitor binding to the endonuclease domain of influenza pH1N1 (2009) polymerase. PLoS Pathog 8:e1002831
Yuan S, Chu H, Singh K et al (2016) A novel small-molecule inhibitor of influenza A virus acts by suppressing PA endonuclease activity of the viral polymerase. Sci Rep 6:22880
Carcelli M, Rogolino D, Gatti A et al (2016) N-acylhydrazone inhibitors of influenza virus PA endonuclease with versatile metal binding modes. Sci Rep 6:31500
Lo CY, Li OT, Tang WP et al (2018) Identification of influenza polymerase inhibitors targeting C-terminal domain of PA through surface plasmon resonance screening. Sci Rep 8:2280
Zhang J, Hu Y, Foley C et al (2018a) Exploring Ugi-Azide four-component reaction products for broad-Spectrum influenza antivirals with a high genetic barrier to drug resistance. Sci Rep 8:4653
D’agostino I, Giacchello I, Nannetti G et al (2018) Synthesis and biological evaluation of a library of hybrid derivatives as inhibitors of influenza virus PA-PB1 interaction. Eur J Med Chem 157:743–758
Desantis J, Nannetti G, Massari S et al (2017) Exploring the cycloheptathiophene-3-carboxamide scaffold to disrupt the interactions of the influenza polymerase subunits and obtain potent anti-influenza activity. Eur J Med Chem 138:128–139
Nannetti G, Massari S, Mercorelli B et al (2019) Potent and broad-spectrum cycloheptathiophene-3-carboxamide compounds that target the PA-PB1 interaction of influenza virus RNA polymerase and possess a high barrier to drug resistance. Antiviral Res 165:55–64
Zhang J, Hu Y, Wu N et al (2020) Discovery of influenza polymerase PA-PB1 interaction inhibitors using an in vitro Split-luciferase complementation-based assay. ACS Chem Biol 15:74–82
Yoon JJ, Toots M, Lee S et al (2018) Orally efficacious broad-Spectrum Ribonucleoside analog inhibitor of influenza and respiratory syncytial viruses. Antimicrob Agents Chemother 62:e00766-18.
Sheahan TP, Sims AC, Zhou S et al (2020) An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Sci Transl Med 12:eabb5883
Toots M, Yoon JJ, Hart M et al (2020) Quantitative efficacy paradigms of the influenza clinical drug candidate EIDD-2801 in the ferret model. Transl Res 218:16–28
Byrn RA, Jones SM, Bennett HB et al (2015) Preclinical activity of VX-787, a first-in-class, orally bioavailable inhibitor of the influenza virus polymerase PB2 subunit. Antimicrob Agents Chemother 59:1569–1582
Mcgowan DC, Balemans W, Embrechts W et al (2019) Design, synthesis, and biological evaluation of novel Indoles targeting the influenza PB2 cap binding region. J Med Chem 62:9680–9690
Liu T, Liu M, Chen F et al (2018) A small-molecule compound has anti-influenza a virus activity by acting as a ''PB2 inhibitor. Mol Pharm 15:4110–4120
Pautus S, Sehr P, Lewis J et al (2013) New 7-methylguanine derivatives targeting the influenza polymerase PB2 cap-binding domain. J Med Chem 56:8915–8930
Yuan S, Chu H, Ye J et al (2017) Identification of a novel small-molecule compound targeting the influenza A virus polymerase PB1-PB2 interface. Antiviral Res 137:58–66
Kao RY, Yang D, Lau LS et al (2010) Identification of influenza A nucleoprotein as an antiviral target. Nat Biotechnol 28:600–605
Pang B, Cheung NN, Zhang W et al (2016) Structural characterization of H1N1 nucleoprotein-Nucleozin binding sites. Sci Rep 6:29684
Gerritz SW, Cianci C, Kim S et al (2011) Inhibition of influenza virus replication via small molecules that induce the formation of higher-order nucleoprotein oligomers. Proc Natl Acad Sci U S A 108:15366–15371
Shen YF, Chen YH, Chu SY et al (2011) E339...R416 salt bridge of nucleoprotein as a feasible target for influenza virus inhibitors. Proc Natl Acad Sci U S A 108:16515–16520
Woodring JL, Lu SH, Krasnova L et al (2020) Disrupting the conserved salt bridge in the Trimerization of influenza a nucleoprotein. J Med Chem 63:205–215
Lejal N, Tarus B, Bouguyon E et al (2013) Structure-based discovery of the novel antiviral properties of naproxen against the nucleoprotein of influenza A virus. Antimicrob Agents Chemother 57:2231–2242
Tarus B, Bertrand H, Zedda G et al (2015) Structure-based design of novel naproxen derivatives targeting monomeric nucleoprotein of influenza A virus. J Biomol Struct Dyn 33:1899–1912
Makau JN, Watanabe K, Ishikawa T et al (2017) Identification of small molecule inhibitors for influenza a virus using in silico and in vitro approaches. PLoS One 12:e0173582
Kleinpeter AB, Jureka AS, Falahat SM et al (2018) Structural analyses reveal the mechanism of inhibition of influenza virus NS1 by two antiviral compounds. J Biol Chem 293:14659–14668
Patnaik S, Basu D, Southall N et al (2019) Identification, design and synthesis of novel pyrazolopyridine influenza virus nonstructural protein 1 antagonists. Bioorg Med Chem Lett 29:1113–1119
Crepin T, Dias A, Palencia A et al (2010) Mutational and metal binding analysis of the endonuclease domain of the influenza virus polymerase PA subunit. J Virol 84:9096–9104
Guilligay D, Tarendeau F, Resa-Infante P et al (2008) The structural basis for cap binding by influenza virus polymerase subunit PB2. Nat Struct Mol Biol 15:500–506
Obayashi E, Yoshida H, Kawai F et al (2008) The structural basis for an essential subunit interaction in influenza virus RNA polymerase. Nature 454:1127–1131
Pflug A, Guilligay D, Reich S et al (2014) Structure of influenza a polymerase bound to the viral RNA promoter. Nature 516:355–360
Reich S, Guilligay D, Pflug A et al (2014) Structural insight into cap-snatching and RNA synthesis by influenza polymerase. Nature 516:361–366
Sugiyama K, Obayashi E, Kawaguchi A et al (2009) Structural insight into the essential PB1-PB2 subunit contact of the influenza virus RNA polymerase. EMBO J 28:1803–1811
Wandzik JM, Kouba T, Karuppasamy M et al (2020b) A structure-based model for the complete transcription cycle of influenza polymerase. Cell 181:877–893.e821
Coloma R, Valpuesta JM, Arranz R et al (2009) The structure of a biologically active influenza virus ribonucleoprotein complex. PLoS Pathog 5:e1000491
Fan H, Walker AP, Carrique L et al (2019) Structures of influenza a virus RNA polymerase offer insight into viral genome replication. Nature 573:287–290
Fodor E, Te Velthuis AJW (2019) Structure and function of the influenza virus transcription and replication machinery. Cold Spring Harb Perspect Med 10:a038398
Robb NC, Te Velthuis AJW, Fodor E et al (2019) Real-time analysis of single influenza virus replication complexes reveals large promoter-dependent differences in initiation dynamics. Nucleic Acids Res 47:6466–6477
Walker AP, Fodor E (2019) Interplay between influenza virus and the host RNA polymerase II transcriptional machinery. Trends Microbiol 27:398–407
Ju H, Zhang J, Huang B et al (2017) Inhibitors of influenza virus polymerase acidic (PA) endonuclease: contemporary developments and perspectives. J Med Chem 60:3533–3551
Ju H, Zhan P, Liu X (2019) Designing influenza polymerase acidic endonuclease inhibitors via ‘privileged scaffold’ re-evolution/refining strategy. Future Med Chem. https://doi.org/10.4155/fmc-2018-0489.
Monod A, Swale C, Tarus B et al (2015) Learning from structure-based drug design and new antivirals targeting the ribonucleoprotein complex for the treatment of influenza. Expert Opin Drug Discov 10:345–371
Zhou Z, Liu T, Zhang J et al (2018) Influenza a virus polymerase: an attractive target for next-generation anti-influenza therapeutics. Drug Discov Today 23:503–518
Massari S, Goracci L, Desantis J et al (2016) Polymerase acidic protein-basic protein 1 (PA-PB1) protein-protein interaction as a target for next-generation anti-influenza therapeutics. J Med Chem 59:7699–7718
Swale C, Monod A, Tengo L et al (2016) Structural characterization of recombinant IAV polymerase reveals a stable complex between viral PA-PB1 heterodimer and host RanBP5. Sci Rep 6:24727
Coloma R, Arranz R, De La Rosa-Trevin JM et al (2020) Structural insights into influenza A virus ribonucleoproteins reveal a processive helical track as transcription mechanism. Nat Microbiol 5:727–734
Wandzik JM, Kouba T, Cusack S (2020a) Structure and function of influenza polymerase. Cold Spring Harb Perspect Med, a038372
Arranz R, Coloma R, Chichon FJ et al (2012) The structure of native influenza virion ribonucleoproteins. Science 338:1634–1637
Ye Q, Krug RM, Tao YJ (2006) The mechanism by which influenza a virus nucleoprotein forms oligomers and binds RNA. Nature 444:1078–1082
Chenavas S, Estrozi LF, Slama-Schwok A et al (2013b) Monomeric nucleoprotein of influenza A virus. PLoS Pathog 9:e1003275
Chenavas S, Crepin T, Delmas B et al (2013a) Influenza virus nucleoprotein: structure, RNA binding, oligomerization and antiviral drug target. Future Microbiol 8:1537–1545
Tarus B, Bakowiez O, Chenavas S et al (2012) Oligomerization paths of the nucleoprotein of influenza A virus. Biochimie 94:776–785
Zheng W, Fan W, Zhang S et al (2019) Naproxen exhibits broad anti-influenza virus activity in mice by impeding viral nucleoprotein nuclear export. Cell Rep 27:1875–1885.e1875
Vidic J, Noiray M, Bagchi A et al (2016) Identification of a novel complex between the nucleoprotein and PA(1-27) of influenza a virus polymerase. Biochemistry 55:4259–4262
Cho JH, Zhao B, Shi J et al (2020) Molecular recognition of a host protein by NS1 of pandemic and seasonal influenza A viruses. Proc Natl Acad Sci U S A 117:6550–6558
Liu Q, Zhou YH, Yang ZQ (2016) The cytokine storm of severe influenza and development of immunomodulatory therapy. Cell Mol Immunol 13:3–10
Karlas A, Machuy N, Shin Y et al (2010) Genome-wide RNAi screen identifies human host factors crucial for influenza virus replication. Nature 463:818–822
König R, Stertz S, Zhou Y et al (2010) Human host factors required for influenza virus replication. Nature 463:813–817
Meliopoulos VA, Andersen LE, Birrer KF et al (2012) Host gene targets for novel influenza therapies elucidated by high-throughput RNA interference screens. FASEB J 26:1372–1386
Stertz S, Shaw ML (2011) Uncovering the global host cell requirements for influenza virus replication via RNAi screening. Microbes Infect 13:516–525
Powell JD, Waters KM (2017) Influenza-Omics and the host response: recent advances and future prospects. Pathogens 6:25
Watanabe T, Kawaoka Y (2015) Influenza virus-host interactomes as a basis for antiviral drug development. Curr Opin Virol 14:71–78
Moss RB, Hansen C, Sanders RL et al (2012) A phase II study of DAS181, a novel host directed antiviral for the treatment of influenza infection. J Infect Dis 206:1844–1851
Zenilman JM, Fuchs EJ, Hendrix CW et al (2015) Phase 1 clinical trials of DAS181, an inhaled sialidase, in healthy adults. Antiviral Res 123:114–119
Yeganeh B, Ghavami S, Kroeker AL et al (2015) Suppression of influenza A virus replication in human lung epithelial cells by noncytotoxic concentrations bafilomycin A1. Am J Physiol Lung Cell Mol Physiol 308:L270–L286
Muller KH, Kainov DE, El Bakkouri K et al (2011) The proton translocation domain of cellular vacuolar ATPase provides a target for the treatment of influenza A virus infections. Br J Pharmacol 164:344–357
Chen HW, Cheng JX, Liu MT et al (2013) Inhibitory and combinatorial effect of diphyllin, a v-ATPase blocker, on influenza viruses. Antiviral Res 99:371–382
Bimbo LM, Denisova OV, Makila E et al (2013) Inhibition of influenza A virus infection in vitro by saliphenylhalamide-loaded porous silicon nanoparticles. ACS Nano 7:6884–6893
Zhirnov OP, Klenk HD, Wright PF (2011) Aprotinin and similar protease inhibitors as drugs against influenza. Antiviral Res 92:27–36
Yamaya M, Shimotai Y, Hatachi Y et al (2015) The serine protease inhibitor camostat inhibits influenza virus replication and cytokine production in primary cultures of human tracheal epithelial cells. Pulm Pharmacol Ther 33:66–74
De Vries E, Tscherne DM, Wienholts MJ et al (2011) Dissection of the influenza A virus endocytic routes reveals macropinocytosis as an alternative entry pathway. PLoS Pathog 7:e1001329
Harada S, Yokomizo K, Monde K et al (2007) A broad antiviral neutral glycolipid, fattiviracin FV-8, is a membrane fluidity modulator. Cell Microbiol 9:196–203
Götz V, Magar L, Dornfeld D et al (2016) Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import. Sci Rep 6:23138
Zu M, Li C, Fang J-S et al (2015) Drug discovery of host CLK1 inhibitors for influenza treatment. Molecules 20:19735–19747
Slaine PD, Kleer M, Smith NK et al (2017) Stress granule-inducing eukaryotic translation initiation factor 4A inhibitors block influenza a virus replication. Viruses 9:388
Durr FE, Lindh HF, Forbes M (1975) Efficacy of 1-beta-D-ribofuranosyl-1,2,4-triazole-3-carboxamide against influenza virus infections in mice. Antimicrob Agents Chemother 7:582–586
Sidwell RW, Bailey KW, Wong MH et al (2005) In vitro and in vivo influenza virus-inhibitory effects of viramidine. Antiviral Res 68:10–17
Perwitasari O, Johnson S, Yan X et al (2014) Verdinexor, a novel selective inhibitor of nuclear export, reduces influenza a virus replication in vitro and in vivo. J Virol 88:10228–10243
Chutiwitoonchai N, Mano T, Kakisaka M et al (2017) Inhibition of CRM1-mediated nuclear export of influenza A nucleoprotein and nuclear export protein as a novel target for antiviral drug development. Virology 507:32–39
Haasbach E, Reiling SJ, Ehrhardt C et al (2013) The NF-kappaB inhibitor SC75741 protects mice against highly pathogenic avian influenza A virus. Antiviral Res 99:336–344
Pleschka S, Wolff T, Ehrhardt C et al (2001) Influenza virus propagation is impaired by inhibition of the Raf/MEK/ERK signalling cascade. Nat Cell Biol 3:301–305
Courtin N, Fotso AF, Fautrad P et al (2017) Antiviral activity of formyl peptide receptor 2 antagonists against influenza viruses. Antiviral Res 143:252–261
Schräder T, Dudek SE, Schreiber A et al (2018) The clinically approved MEK inhibitor Trametinib efficiently blocks influenza A virus propagation and cytokine expression. Antiviral Res 157:80–92
Hu Y, Zhang J, Musharrafieh RG et al (2017) Discovery of dapivirine, a nonnucleoside HIV-1 reverse transcriptase inhibitor, as a broad-spectrum antiviral against both influenza A and B viruses. Antiviral Res 145:103–113
Rossignol JF, La Frazia S, Chiappa L et al (2009) Thiazolides, a new class of anti-influenza molecules targeting viral hemagglutinin at the post-translational level. J Biol Chem 284:29798–29808
Musiol A, Gran S, Ehrhardt C et al (2013) Annexin A6-balanced late endosomal cholesterol controls influenza A replication and propagation. mBio 4:e00608–13
Matsui K, Ozawa M, Kiso M et al (2018) Stimulation of alpha2-adrenergic receptors impairs influenza virus infection. Sci Rep 8:4631
Malakhov MP, Aschenbrenner LM, Smee DF et al (2006) Sialidase fusion protein as a novel broad-spectrum inhibitor of influenza virus infection. Antimicrob Agents Chemother 50:1470–1479
Dubois J, Terrier O, Rosa-Calatrava M (2014) Influenza viruses and mRNA splicing: doing more with less. mBio 5:e00070–14
Dubois J, Traversier A, Julien T et al (2019) The nonstructural NS1 protein of influenza viruses modulates TP53 splicing through host factor CPSF4. J Virol 93:e02168-18
Schreiber A, Boff L, Anhlan D et al (2020) Dissecting the mechanism of signaling-triggered nuclear export of newly synthesized influenza virus ribonucleoprotein complexes. Proc Natl Acad Sci U S A 117:16557–16566
Rossignol J-F (2014) Nitazoxanide: a first-in-class broad-spectrum antiviral agent. Antiviral Res 110:94–103
Tilmanis D, Van Baalen C, Oh DY et al (2017) The susceptibility of circulating human influenza viruses to tizoxanide, the active metabolite of nitazoxanide. Antiviral Res 147:142–148
Haffizulla J, Hartman A, Hoppers M et al (2014) Effect of nitazoxanide in adults and adolescents with acute uncomplicated influenza: a double-blind, randomised, placebo-controlled, phase 2b/3 trial. Lancet Infect Dis 14:609–618
Mazur I, Wurzer WJ, Ehrhardt C et al (2007) Acetylsalicylic acid (ASA) blocks influenza virus propagation via its NF-kappaB-inhibiting activity. Cell Microbiol 9:1683–1694
Wiesener N, Zimmer C, Jarasch-Althof N et al (2011) Therapy of experimental influenza virus infection with pyrrolidine dithiocarbamate. Med Microbiol Immunol 200:115–126
Ehrhardt C, Rückle A, Hrincius ER et al (2013) The NF-κB inhibitor SC75741 efficiently blocks influenza virus propagation and confers a high barrier for development of viral resistance. Cell Microbiol 15:1198–1211
Droebner K, Haasbach E, Dudek SE et al (2017) Pharmacodynamics, pharmacokinetics, and antiviral activity of BAY 81-8781, a novel NF-kappaB inhibiting anti-influenza drug. Front Microbiol 8:2130
Scheuch G, Canisius S, Nocker K et al (2018) Targeting intracellular signaling as an antiviral strategy: aerosolized LASAG for the treatment of influenza in hospitalized patients. Emerg Microbes Infect 7:21
Nacken W, Ehrhardt C, Ludwig S (2012) Small molecule inhibitors of the c-Jun N-terminal kinase (JNK) possess antiviral activity against highly pathogenic avian and human pandemic influenza A viruses. Biol Chem 393:525–534
Choi MS, Heo J, Yi CM et al (2016) A novel p38 mitogen activated protein kinase (MAPK) specific inhibitor suppresses respiratory syncytial virus and influenza A virus replication by inhibiting virus-induced p38 MAPK activation. Biochem Biophys Res Commun 477:311–316
Fedson DS (2013) Treating influenza with statins and other immunomodulatory agents. Antiviral Res 99:417–435
Mehrbod P, Omar AR, Hair-Bejo M et al (2014) Mechanisms of action and efficacy of statins against influenza. Biomed Res Int 2014:872370
Shi X, Zhou W, Huang H et al (2013) Inhibition of the inflammatory cytokine tumor necrosis factor-alpha with etanercept provides protection against lethal H1N1 influenza infection in mice. Crit Care 17:R301
Ye S, Lowther S, Stambas J (2015) Inhibition of reactive oxygen species production ameliorates inflammation induced by influenza a viruses via upregulation of SOCS1 and SOCS3. J Virol 89:2672–2683
Oostwoud LC, Gunasinghe P, Seow HJ et al (2016) Apocynin and ebselen reduce influenza A virus-induced lung inflammation in cigarette smoke-exposed mice. Sci Rep 6:20983
Davidson S (2018) Treating influenza infection, from now and into the future. Front Immunol 9:1946
Carey MA, Bradbury JA, Rebolloso YD et al (2010) Pharmacologic inhibition of COX-1 and COX-2 in influenza A viral infection in mice. PLoS One 5:e11610
Zheng B-J, Chan K-W, Lin Y-P et al (2008) Delayed antiviral plus immunomodulator treatment still reduces mortality in mice infected by high inoculum of influenza a/H5N1 virus. Proc Natl Acad Sci U S A 105:8091–8096
Davidson S, Mccabe TM, Crotta S et al (2016) IFNλ is a potent anti-influenza therapeutic without the inflammatory side effects of IFNα treatment. EMBO Mol Med 8:1099–1112
Kim S, Kim M-J, Kim C-H et al (2017) The superiority of IFN-λ as a therapeutic candidate to control acute influenza viral lung infection. Am J Respir Cell Mol Biol 56:202–212
Pizzorno A, Padey B, Terrier O et al (2019a) Drug repurposing approaches for the treatment of influenza viral infection: reviving old drugs to fight against a long-lived enemy. Front Immunol 10:531
Pizzorno A, Terrier O, Nicolas De Lamballerie C et al (2019b) Repurposing of drugs as novel influenza inhibitors from clinical gene expression infection signatures. Front Immunol 10:60
Wurzer WJ, Ehrhardt C, Pleschka S et al (2004) NF-kappaB-dependent induction of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) and Fas/FasL is crucial for efficient influenza virus propagation. J Biol Chem 279:30931–30937
Yin MJ, Yamamoto Y, Gaynor RB (1998) The anti-inflammatory agents aspirin and salicylate inhibit the activity of I(kappa)B kinase-beta. Nature 396:77–80
Belser JA, Szretter KJ, Katz JM et al (2013) Simvastatin and oseltamivir combination therapy does not improve the effectiveness of oseltamivir alone following highly pathogenic avian H5N1 influenza virus infection in mice. Virology 439:42–46
Kumaki Y, Morrey JD, Barnard DL (2012) Effect of statin treatments on highly pathogenic avian influenza H5N1, seasonal and H1N1pdm09 virus infections in BALB/c mice. Future Virol 7:801–818
Salomon R, Hoffmann E, Webster RG (2007) Inhibition of the cytokine response does not protect against lethal H5N1 influenza infection. Proc Natl Acad Sci U S A 104:12479–12481
Enserink M (2005) Infectious disease. Old drugs losing effectiveness against flu; could statins fill gap? Science 309:1976–1977
Vandermeer ML, Thomas AR, Kamimoto L et al (2012) Association between use of statins and mortality among patients hospitalized with laboratory-confirmed influenza virus infections: a multistate study. J Infect Dis 205:13–19
Hung IFN, To KKW, Chan JFW et al (2017) Efficacy of clarithromycin-naproxen-Oseltamivir combination in the treatment of patients hospitalized for influenza a(H3N2) infection: an open-label randomized, controlled, phase IIb/III trial. Chest 151:1069–1080
Lejal N, Truchet S, Bechor E et al (2018) Turning off NADPH oxidase-2 by impeding p67(phox) activation in infected mouse macrophages reduced viral entry and inflammation. Biochim Biophys Acta 1862:1263–1275
Chaudhuri S, Symons JA, Deval J (2018) Innovation and trends in the development and approval of antiviral medicines: 1987-2017 and beyond. Antiviral Res 155:76–88
Escuret V, Cornu C, Boutitie F et al (2012) Oseltamivir-zanamivir bitherapy compared to oseltamivir monotherapy in the treatment of pandemic 2009 influenza a(H1N1) virus infections. Antiviral Res 96:130–137
Pizzorno A, Abed Y, Rhéaume C et al (2014) Oseltamivir-zanamivir combination therapy is not superior to zanamivir monotherapy in mice infected with influenza A(H3N2) and A(H1N1)pdm09 viruses. Antiviral Res 105:54–58
Schloer S, Goretzko J, Pleschka S et al (2020) Combinatory treatment with Oseltamivir and Itraconazole targeting both virus and host factors in influenza a virus infection. Viruses 12:703
Terrier O, Dilly S, Pizzorno A et al (2020) Broad-spectrum antiviral activity of naproxen: from influenza A to SARS-CoV-2 coronavirus. bioRxiv. https://doi.org/10.1101/2020.04.30.069922
Pizzorno A, Padey B, Dubois J et al (2020a) In vitro evaluation of antiviral activity of single and combined repurposable drugs against SARS-CoV-2. Antiviral Res:104878
Pizzorno A, Padey B, Julien T et al (2020b) Characterization and treatment of SARS-CoV-2 in nasal and bronchial human airway epithelia. Cell Rep Med 1:100059
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Terrier, O., Slama-Schwok, A. (2021). Anti-Influenza Drug Discovery and Development: Targeting the Virus and Its Host by All Possible Means. In: Liu, X., Zhan, P., Menéndez-Arias, L., Poongavanam, V. (eds) Antiviral Drug Discovery and Development. Advances in Experimental Medicine and Biology, vol 1322. Springer, Singapore. https://doi.org/10.1007/978-981-16-0267-2_8
Download citation
DOI: https://doi.org/10.1007/978-981-16-0267-2_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-16-0266-5
Online ISBN: 978-981-16-0267-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)