
Abstract
Inherited retinal dystrophies (IRDs) are caused by mutations resulting in progressive functional loss of photoreceptors. The onset of these disorders could be by birth or affect an individual across various ages. Patients diagnosed with Leber congenital amaurosis, retinitis pigmentosa, Stargardt disease, macular dystrophies, choroideremia, etc. experience gradual vision impairment or blindness. Several genes responsible for these dystrophies are known based on extensive genetic studies which led to an understanding of their structure, function, and involvement in cellular pathways making them potential targets for therapeutics. Gene therapy using various delivery vectors such as recombinant adeno-associated virus (rAAV) as a treatment modality offers hope in such conditions that currently have no cure. This chapter provides an overview of different retinal diseases, key genes involved and their mutations resulting in pathological and clinical features, and gene therapy approaches applied. Safety and efficacy are the primary considerations for any gene therapy study. Developments in vector design, promoter modifications, split-gene strategies to express large expression cassettes, compatible vector serotypes or strains to use for efficient retinal cell transduction, alternate gene delivery systems, immune challenges such as the presence of neutralizing antibodies and other toxicity would be given special emphasis in this chapter. Some of the recent success stories of retinal gene therapy preclinical studies and clinical trials are discussed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
30.1 Introduction
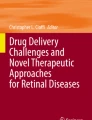
Over the last several years, the knowledge of genetics and genetic mutations driving various diseases including inherited retinal diseases has grown exponentially. This cumulative knowledge from human and animal model studies raised the hope of genetic therapies (Fig. 30.1). The eye is an easily accessible and fascinating organ for gene therapy. Gene delivery is safer as the eye is highly compartmentalized and has immune privilege to a certain extent. The presence of blood–retina and blood–aqueous barriers limit infection processes or immune activity and thus also hinders gene delivery parenterally to the typical ocular targets such as the retinal pigment epithelium (RPE) and neuronal retina. Thus, gene delivery to the internal layers of the eye depends on ingenuous surgical methods developed over the past few decades such as subretinal injection, supra-cameral injections, intravitreal injections, etc. Such methods deliver the genes directly to the target tissues while minimizing immune responses outside of the eye. Lack of active intraocular immune responses in the eye also protects vector transduced cells from being lost due to rejection. Most cellular layers in the eye do not replicate and hence a single appropriate dose of viral vector carrying the therapeutic gene is required for efficient transduction and prolonged gene expression. Though recombinant adeno-associated virus (rAAV) has a packaging capacity of around 4.7 kb, it is the vector of choice in clinical trials for ocular gene therapy. Intravitreal and subretinal injections of AAV serotype 1, 2, 5, 7, and 8 have been successfully used for high-level, long-term gene expression in retinal cells [1, 2]. Large genes (example: ABCA4 and USH2A) can be accommodated with improved vector design strategies such as overlapping, trans-splicing, and dual-hybrid vector systems while using rAAV [3]. Other gene delivery methods such as integration deficient lentivirus (IDLVs) to overcome risks of insertional mutagenesis and nanoparticle-based (such as liposomes, polymers, and peptide compacted DNA) have also been studied and successfully used in vivo on retinal cell types. Different nanoparticles have different biochemical properties that govern their internalization, endosomal escape, and transportation to the nucleus. Efficacy of gene transfer can be observed by simple noninvasive procedures like electroretinography and fundus examinations. Availability of both small and large animal models that mimic human disease conditions for several monogenic inherited retinal dystrophies (IRDs) makes it convenient to test strategies for therapeutic benefits in preclinical studies.

Milestones in retinal gene therapy. The progress in understanding diseases with discoveries in genetics and remarkable technological developments in the field of molecular biology and applications leading to gene therapy products are time lined in this figure
Retinal degeneration can be grouped under three broad classifications—(1) hereditary or inherited retinal dystrophies, (2) retinal degenerations, and (3) retinal dystrophies that are part of a syndrome. Some of the most common monogenic IRDs include several forms of retinitis pigmentosa (RP), Leber congenital amaurosis (LCA), Stargardt disease (STGD), choroideremia, achromatopsia, X-linked juvenile retinoschisis (XLRS), Usher syndrome, and other cone–rod and rod–cone dystrophies (CRDs and RCDs). Age-related macular degeneration (AMD), diabetic retinopathy (DR), vein occlusions, and retinopathy of prematurity (ROP) belong to a multifactorial class of degenerations. Similar retinal conditions could be part of syndromes such as Usher, Bardet–Biedlt, and others. Different genes encoding enzymes or structural components contributing to the visual cycle or retinal structure are responsible for various types of retinal disorders. The retina is a highly specialized structure consisting of light-sensitive cone and rod photoreceptor cells, which initiate neuronal signaling in response to light stimulation. The photoreceptor cells are supported by a monolayer of polarized retinal pigmented epithelium cells (RPE), which performs many key processes including the regeneration of visual pigment that is bleached following light exposure (the visual cycle). Key genes such as retinal pigment epithelium 65 (RPE65) retinoid isomerohydrolase, ATP binding cassette subfamily A member 4 (ABCA4), MER proto-oncogene tyrosine kinase (MERTK) , nuclear hormone receptor (NR2E3), etc. are responsible for the proper functioning of retinal cells facilitating essential processes such as phototransduction and homeostasis required for normal visual function. The RPE cells are located between the neural retina and the choroid and plays a critical role in the maintenance of visual function. RPE receives light, phagocytoses photoreceptor outer segments, participates in circadian rhythm, is involved in fatty acid metabolism, forms the outer blood–ocular barrier which maintains the subretinal space, performs repair and renewal of cells [4, 5]. RPE cells are polarized and maintain tight cell junctions. Disruption of RPE phagocytosis has been linked to disease phenotypes such as STGD disease and RP [6]. Therefore, the selection of patients for gene therapy requires prior knowledge of the mutated gene as well as the mode of inheritance. Sections in this chapter would include further details on all important considerations for a safer and highly efficacious gene transfer and recent developments in gene therapy, both preclinical and clinical trials for retinal dystrophies.
30.2 Recombinant Adeno-Associated Virus Vectors in Retinal Gene Therapy
Recombinant AAV used in gene therapy contains two inverted terminal repeats (ITRs) retaining the cis genome packaging signal. The rep (replication) and cap (capsid formation) genes required for virus production are supplied on a trans-helper plasmid. The DNA and promoter of interest placed in between the AAV ITRs is the transgene expression cassette [7, 8]. It can efficiently transduce nondiving cells and is nonpathogenic, which makes it safe for use in gene therapy. There are different strategies to expand the packaging capacity of AAV beyond the traditional 4.7 kb. One such approach is to make a truncated version of a large gene by excluding certain sequences without compromising protein function and retaining functionally relevant sequences [9]. Other strategies such as the cis-activation approach involve dividing the expression cassette into two parts (dual vectors)—one containing the promoter plus enhancer and the other containing the gene are packaged individually. These would get reconstituted upon co-transduction and concatemerization of the ITRs [10]. Additional dual vector approaches include trans-splicing, overlapping, and hybrid strategies. In the trans-splicing approach, the expression cassette is spilt into promoter plus 5′ half of coding sequence and splice donor signals in one vector and the other containing a splice acceptor signal with the 3′ half of the coding sequence. Reconstitution would occur when the 5′ and 3′ vectors form head-to-tail concatamers. Expression is achieved when the intervening double-ITR structure is removed from the mature mRNA using the host cell splicing machinery [11]. Overlapping dual vectors use recombinogenic sequences located in the middle of the gene where the two parts of the gene share an overlap sequence. Upon co-infection with the vectors carrying the two parts, the intact full-length gene is reconstituted by homologous recombination initiated at the overlap to generate the full-length expression cassette, such as alkaline phosphatase (AP) [3]. However, the trans-splicing vector efficiency is dependent on the splice site whereas the overlapping vector efficiency depends on the recombinogenic potential of the overlap sequence. The hybrid dual vector strategy is independent of the transgene properties as it is a novel combination of trans-splicing and overlapping systems [12]. The dual vector strategies may still not meet the need for gene therapy of larger genes (>8.5 kb) such as CDH23 known to cause Usher syndrome type ID. A triple AAV system to expand the cargo limits to 14 kb has been tested and shown to be 40% successful compared to single vector systems [13]. In general, the dose of virus, transgene properties, site of injection and serotype used are factors that contribute to an effective gene therapy without side effects of cellular toxicity [14]. A brief compilation of all the preclinical studies (Table 30.1) and AAV based clinical trials (Table 30.2) thus far are provided.
30.2.1 Serotypes for Retinal Cell Transduction
Most IRDs originate from the retinal pigment epithelium cells (RPE) or rod and cone photoreceptors. To choose an AAV serotype that is specific and best for transduction of retinal cell types via any route of administration has been critical. Animal retina, which differ structurally as well (depending on species) to the human retina do not always recapitulate the same surface receptors as human retinal cell types for specific tropism. Ex vivo human retina and retinal pigment epithelium-choroid explants were used to check for transduction efficiency and tropism of AAV2/1, AAV2/2, AAV2/4, AAV2/5, AAV2/6, AAV2/8, and AAV2/9 carrying green fluorescent protein (GFP) driven by cytomegalovirus (CMV) promoter. AAV2/4 and AAV2/5 efficiently transduced photoreceptor cells, the latter being highly specific to the outer nuclear layer (ONL). AAV2/8 exhibited comparatively lower transduction of photoreceptors, whereas higher levels of transduction were observed in the inner retina. AAV2/8 also showed a preference to cone cells in particular. Good transduction of retina is achievable as seen in the pig model injected with AAV2/8 subretinally, suggesting some degree of difference in tropism across species [15]. Interestingly, retinoschisis and CHM gene therapy studies have used the AA8 serotype for gene delivery.
Greater understanding of AAV biology helped design strategies which could overcome proteasome degradation of vectors by incorporating point mutation of surface-exposed tyrosine to phenylalanine (Y-F) in the capsid of rAAV 2, 8, and 9 and achieve greater levels of transduction of retinal cells compared to their wild-type counterparts [16,17,18]. In a retinal degeneration study, three of the most efficacious AAV capsids AAV2/8(Y733F), AAV2/2(quad Y272, 444, 500, 730F) and AAV2/(7m8) were tested for transduction efficiency in an rd1 mouse model, monkey and human retinal explants. AAV2/2(7m8) resulted in a greater area of retinal transduction and the highest percentage of gene expression. Transduction of cell types and efficacy of AAV2/2(7m8) and AAV2/2(quad Y-F) via intravitreal or subretinal routes of delivery were similar and better compared to AAV2/8(Y733F). AAV2/2(7m8) was extremely efficient in transducing all retinal cell types compared to the other serotypes which selectively transduced few cell types [19]. rAAV2 (triple Y − F + T − V) efficiently transduced photoreceptors by intravitreal injections [20]. rAAV2/9 and 2/8 transduce RPE, photoreceptors (PR), Muller cells (MC), inner nuclear layer (INL), outer plexiform layer (OPL), and ganglion cells (GC) of mouse and dog retinal cells efficiently and result in high transgene expression [21, 22]. rAAV2/8 and rAAV2/7 are capable of infecting rods and cones at high levels of transduction efficiencies compared to AAV2/5 [23]. Subretinal delivery of rAAV2/5 and rAAV-2/4 carrying CMV. GFP were injected to dog, mouse, and macaque. rAAV2/5 transduced rods and cones better than RPE cells, whereas, with rAAV2/4, transduction was restricted to RPE cells and resulted in long-term gene expression [24]. There has been no report of successful transduction of retinal cells using rAAV2/3 serotype. RPE cells to some extent do get transduced by rAAV2/6 serotype [25]. rAAV/rh10 has been shown to efficiently transduce mice photoreceptor cells and rescue rhodopsin deficient phenotype [26]. rAAVShH10 (close variant of AAV6) has a greater tropism for Muller glial cells as tested in a rat model of RP [27, 28]. A summary of serotypes and their tropism is represented in Table 30.3.
30.2.2 Broadly Active Versus Specific Promoters
To ensure cell type-specific gene expression, use of a cell-specific or gene-specific promoter is essential to circumvent unwanted transgene expression at off-target areas. An efficient promoter driving high and clinically relevant levels of therapeutic gene expression is necessary so that a single appropriate dose of the vector would be sufficient for treatment. This would overcome consequences of immune response or cellular toxicity resulting from multiple or high virus dosage. Gene therapy studies over the past decades have used broadly active promoters such as CMV [29], human ubiquitin C promoter (UbiC) [30], and chicken beta-actin promoter (CAG) [31]. Some retina-specific promoters used are the RPE-specific promoter—Best1 (bestrophin-1) [32] and RPE65 promoter [33], photoreceptor-specific promoters such as human red opsin (RedO) [34, 35], human rhodopsin (Rho) [23, 35], human rhodopsin kinase (RK) [36], mouse cone arrestin (CAR) [37], etc. Choosing a promoter needs careful assessment as some promoters could pose a certain level of toxicity to the retina such as shortening of the cone outer segment, reduction of the outer nuclear layer, and dysmorphic pigment epithelium [38]. Toxicity due to AAV has been observed in some studies involving animals and humans. Sheep with achromatopsia were treated with AAV2-CNGA3 at a high dose of 1012, showed retinal atrophy and lymphocytic infiltration [39]. Another study, involving NHP eye treated with subretinal AAV8-CNGA3 showed responses of both innate and adaptive immunity [40]. An LCA2 gene therapy clinical trial reported strong evidence of an inflammatory response in five out of eight individuals treated with the higher dose of AAV2-RPE65 [41]. The Alberta choroideremia gene therapy clinical trial, reported an adverse effect resulting in functional loss of the subject’s retina [42]. Broad expression promoters typically may have higher expression levels compared to tissue-specific ones. An example is a study which compared transgene expression by five different promoters—cytomegalovirus immediate-early gene promoter (CMV), human desmin (Des), human alpha-myosin heavy chain (α-MHC), rat myosin light chain 2 (MLC-2), and human cardiac troponin C (cTnC) to drive LacZ mediated by AAV9 intravascular delivery in mice. CMV outperformed other tissue-specific promoters resulting in the highest level of transgene expression [43].
30.2.3 Injection Methods
Intravenous injection of AAV would not deliver the therapeutic gene to the target site due to the presence of the blood–retina barrier. Therefore, AAV must be delivered directly to a specific site in the eye where the RPE and photoreceptors are transduced easily (Fig. 30.2). The space between the RPE and photoreceptors, the subretinal space, is the most effective and preferred site for gene therapy. High titer virus preparations are typically required for ocular administration so that the injection volume of the vector may be minimized. In this procedure, a parafoveal bleb is created by subretinal injection of normal saline followed by injection of the vectors through the same self-sealing retinotomy. Preoperative interventions include optical coherence tomography (OCT), pars plana vitrectomy, inner limiting membrane (ILM) staining. Postoperative follow-ups can be done using OCT and fundus scans [44]. During the subretinal injection procedure, there is a risk of reflux of vector into the vitreous which may lead to vitritis due to immune reactions to the capsid.

Injection sites for AAV administration. The intravitreal and subretinal spaces are two common sites of injection to deliver therapeutic AAV particles. In the subretinal route, a bleb is created separating the RPE layer and photoreceptors. The intravitreal route is a less invasive procedure where the viral particles are delivered in the vitreous humor
On the other hand, intravitreal injection is less invasive but may be disadvantageous due to the dilution of the virus within the vitreous or presence of neutralizing antibodies (nAbs) leading to poor transduction of retinal layers [45]. ILM is a wall separating the vitreous and neural retina. A recent injection method called the “subILM,” a surgical route to the space between the ILM and neural retina could better serve the purpose of overcoming issues of intravitreal injections [46]. On the basis of AAV being thermostable and negatively charged, yet another recent development was to enhance AAV uptake by applying an in vivo low electric current across the eye to further enhance retinal transduction after intravitreal administration. The electric current was reported to be safe and does not cause damage to the retina structure or function as tested in a wild-type mouse retina using AAV8 [47].
30.2.4 Immune Responses, Bio-distribution, and Cellular Toxicity
Recombinant AAVs are known to be nonpathogenic and less toxic. Humans or other animals are naturally exposed to AAV and this poses a challenge to the safety and efficacy of therapy using wild-type AAV capsid. Approximately 80% of the population show the presence of nAbs (neutralizing antibody) to wild-type AAV2 capsid [48,49,50]. Retina has an immune privilege due to the existence of the blood–retina barriers; therefore, vector administration via the subretinal route has a much reduced risk of negative immune response due to previous exposure to AAV. This is supported by the observation that subretinal readministration of virus led to repeated successful transduction even in the presence of nAbs to AAV in the serum [51, 52].
Post subretinal delivery of AAV2/8 vectors in a canine model, systemic distribution of AAV may occur in other parts such as the brain probably due to trans-synaptic transport to the neurons. This may not necessarily lead to further effects of the transgene if expressed under retinal cell-specific promoters as reported by Stieger et al. [53]. Several years post successful subretinal transfer of AAV 2, 4, and 5, in dogs and primates, existing AAV particles were observed in the outer plexiform layer (OPL) and in all other layers of the retina [54]. Dosage of virus in most of the in vivo gene therapy studies use a range of 108–1013 vg copies/ml in a single dose. Since the subretinal space can accommodate merely a few microliters, hence a higher viral tier is dosed thereby raising a risk for local tissue reactions, but the currently used injection methods have been shown to be relatively safe with the edema resolving uneventfully in most cases. Other general cellular toxicities arising due to the nature of transgene and transcriptional elements have to be assessed for morphology, physiology and inflammation status in preclinical models before proceeding to clinical trials [38].
30.3 Alternate Methods of Gene Delivery
Apart from AAV, a variety of other vectors have been used to treat retinal diseases which are compiled in Table 30.4. In 1997, lentiviral vectors (LV) carrying GFP driven by CMV or rhodopsin promoter were subretinally injected to the retina of newborn and adult rats and expression followed over 12 weeks. CMV promoter resulted in GFP expression in both photoreceptors and RPE, whereas rhodopsin promoter-driven expression was restricted to the photoreceptors. Due to lack of interphotoreceptor space, expression in adult rat retina was observed only at the site of injection, unlike newborn animals. This long-term expression of the transgenes in photoreceptors could be due to stable integration of the transgene into the genome of the host cell as demonstrated before [55]. The transduction efficiency of LV was similar to adenovirus (Ad)-based vectors [56, 57]. AAV performed better in transducing retina compared to LVs and Ads [58, 59]. Integrase deficient lentiviral vectors (IDLVs) have shown sustained gene expression in vitro and in vivo [60]. These episomal IDLVs are suitable for delivering large genes and transducing nondiving cells in the retina and neural retina without risks of insertional mutagenesis. In 2006, successful use of second-generation self-inactivating (SIN)-IDLVs delivered subretinally in adult rodent models of retinal degeneration (Rpe65rd12/rd12 mouse and Mertk-deficient rat) showed long-term (9 and 3 months’ follow-up in mice and rats, respectively) eGFP expression in adult RPE cells. Thus, IDLVs are potential candidate vectors for gene therapy of retinal dystrophies.
Nanoparticles (NPs) such as polymers, liposomes, peptide compacted DNA have been tested as gene delivery systems for retinal diseases [61, 62]. The advantage of using NPs is the ease in manipulating its chemical properties to suite DNA delivery, low cost of manufacturing, and transferring large vectors without any immune reactions. Critical steps in gene transfer via NPs involve uptake by target cells, escape endosomal degradation in the cytosol, and transport of genetic cargo to the nucleus without causing cytotoxicity and should be biodegradable in the human body [63]. NPs are taken up by RPE cells by either endocytosis [62]. NPs enter photoreceptors and glial cells by different methods of endocytosis depending on their shape, size, charges, and amount of DNA load they carry [64]. Measures to aid critical processes for efficient gene transfer and expression are considered for prospective human applications. Numerous types, modifications, or customizations of NPs are being studied to make them efficient carriers. The PLGA (poly lactic-co-glycolic acid) and PEG (polyethylene glycol) compacted DNA NPs are the forerunners for safe delivery of genes to photoreceptor cells and the RPE [65]. Cationic liposomes were first used for gene transfer to rat eye via subretinal or intravitreal injections resulting in expression of the lacZ reporter transgene in ganglion cells and RPE alone with no expression observed in photoreceptor cells. This could be due to the phagocytic process of RPE actively taking in most of the NPs compared to less efficient endocytosis by rods and cones [66]. A detailed review of various NPs for ocular gene therapy can be found in Adijanto and Naash’s article [64].
30.4 Gene Therapy of Congenital Retinal Degenerations
IRDs are inherited in the family in either autosomal dominant, autosomal recessive, or X-linked manner. The presence of mutational heterogeneity in autosomal dominant conditions is a challenge for gene therapy due to the toxic “gain of function” of the mutant allele. Such conditions lead to the death of photoreceptor cells [67]. The approach to treat a dominant-negative condition typically involves silencing of the dominant allele that is detrimental for the cell, followed by replacement with a codon optimized version of the gene resistant to the silencing. Ribozymes or small interfering RNA (siRNA) are used for silencing the defect. Some common inherited retinal conditions, preclinical studies, and recent clinical trials will be discussed in the following subsections.
30.4.1 Retinitis Pigmentosa (Rod–Cone Dystrophies)
Retinitis pigmentosa (RP) is a progressive rod–cone degeneration (RCDs) caused by mutations in more than 200 genes identified thus far, which affects 1 in 4000 individuals. RP is inherited as autosomal dominant (30–40%) (for example RHO gene; 25% of adRP), autosomal recessive (50–60%) (for example, USH2A gene; 20% of arRP), X-linked conditions (5–15%) (for example, RPGR gene; 70% of XLRP) or some rare forms such as mitochondrial diseases [68, 69]. Mutations in genes responsible for loss of photoreceptors leads to early signs such as difficulty in dark adaptation and night blindness as the rods get affected first. This is followed by a gradual decrease in the visual field (tunnel vision) progressing to complete loss of vision. Electroretinogram (ERG) usually shows a decline in photoreceptor activity in patients with RP. Phenotype and age of onset are highly variable with individuals.
More than 150 mutations in the rhodopsin (RHO) gene belong to the G-protein coupled receptor family and present on chromosomal location 3q22.1, which leads to adRP. The structure and function of rhodopsin was described in 1994 [70] The rhodopsin protein is bound to 11-cis retinal (vitamin A) which gets activated upon light stimulation. This event initiates a chain of chemical reactions to produce an electric signal which is sent to the brain and perceived as vision. Gene therapies for RHO adRP were either focused on minimizing the expression of the toxic mutant allele or designing a mutation-independent strategy. In a recent gene therapy study, the authors developed a highly efficient shRNA that is specific to human and canine RHO in a mutation-independent manner. This vector design also involved the human RHO cDNA, codon-optimized to make it resistant to RNA interference, with both the shRNA and the RHO gene being expressed from a single AAV virion. This vector was tested in a spontaneously occurring dog model of RHO-adRP. The native canine RHO RNA was completely inactivated via subretinal vector delivery leading to expression up to 30% of normal cellular expression. OCT imaging and histopathology of the treated area showed normal structure and presence of normal RHO protein in the remaining transduced photoreceptors. Long-term follow-up of greater than 8 months by OCT and ERG showed reversal of phenotype and a stable maintenance of photoreceptor structure and function. This successful animal model study can be applied to treat patients with this form of adRP by gene therapy [71].
Rare XLRPs are caused by mutations in RP2 and OFD1 gene. RPGR gene present on chromosomal position: Xp11.4 was identified to cause XLRP in 1996 [72]. This encodes for retinitis pigmentosa GTPase regulator that is necessary for cells’ ciliary function aiding vision and is the most common form of XLRP. Along with few naturally occurring [73] and genetically modified mouse models [74], canine models with RPGR mutations such as the Siberian husky reported in 1999, which a spontaneous model of XLRP that mimics the human disease [75]. A recently reported model with a deletion of exons 1–4 in RPGR gene is the Weimaraner dog, a naturally occurring model for XLRP [76]. RPGR gene is a purine-rich gene which is prone to genetic instability, making it difficult to manipulate [77]. In a 2012 preclinical study, rAAV2/5 vector carrying RPGR cDNA driven either by a human photoreceptor-specific IRBP (interstitial retinol-binding protein) or GRK1 (rhodopsin kinase) promoter and was delivered at a dosage of 1013 vector genome/ml (vg/ml) via the subretinal route. This was not successful as the mice developed toxicity to the mutated therapeutic cDNA [78, 79]. A different report described an RPGR vector strategy where the purine-rich region was deleted in frame resulting in long (deletion of 314 codons) and short (deletion of 126 codons) forms in AAV8.GRK1.RPGRORF15 vectors. The long form showed functional restoration of the photoreceptors in the Rpgr-null mouse, whereas the short version did not fare well. This could be due to the maximal glutamylated status of the protein which is required for full therapeutic activity of the protein in the full-length RPGR which may have decreased in proteins formed from reduced sequences [80]. These challenges were overcome by using a codon-optimized version of the gene which is highly stable. AAV.coRPGRORF15 was used to treat Rpgr-null and Rd9 mice mouse models which showed reversal of the phenotype without any toxic side effects, thereby establishing the first successful proof-of-concept leading to three clinical trials initiated in 2017 and 2018 [81]. First clinical trial by Nightstar Therapeutics using AAV8.GRK1.RPGRORF15 (NCT03116113), second by MeiraGTx UK Ltd. using AAV2/5.hRKp.RPGR (NCT03252847), and the third by Applied Genetic Technologies Corp (AGTC) using AAV2/2(YF).GRK1.RPGRORF15 (NCT03316560) [82].
An example of autosomal recessive RP caused by mutations in the MERTK gene resulted in the accumulation of outer segment debris due to defective RPE phagocytosis, which is necessary for the renewal of photoreceptor outer segment [83]. In a preclinical study, rats were treated with subretinal injection of AAV-MERTK vectors that demonstrated significant improvements in response to ERG [84]. Six patients with confirmed mutations in MERTK were treated by gene therapy in a phase 1 clinical trial. Three out of the six patients had shown improvements in vision and had no signs of systemic toxicity in long-term follow-ups of over 2 years [85]. A 2019 gene therapy phase 2 clinical trial reported final outcomes of six male patients across different age groups affected with choroideremia who had received subfoveal injection of AAV2-REP1 at 1011 vg/0.1 mL. These subjects who had documented a reduction in the vision now demonstrated improvements in visual acuity without any adverse toxic effects [86].
30.4.2 Cone–Rod Dystrophies
Gene therapy for retinitis pigmentosa GTPase regulator interacting protein 1 (RPGRIP1)- in a canine model of severe cone–rod dystrophy (CRD) was performed using AAV5 and AAV8. Cone and rod functions were restored and RPGRIP1 was stably expressed over a period of 2 years in all treated eyes. This large animal model of CRD provides hope toward the treatment of patients [87]. Achromatopsia is caused by mutations in cyclic nucleotide-gated channel alpha 3 (CNGA3) (other genes causing similar phenotype are CNGB3, GNAT2, PDE6C, PDE6H, and ATF6) (http://www.sph.uth.tmc.edu/RetNet/) resulting in poor visual acuity, photophobia, and inability to recognize colors due to cone dysfunctions. The presence of a naturally occurring CNGB3-sheep model facilitated the study of treatment strategies [88]. In a 2011 study, sheep deficient in CNGA3 were treated unilaterally with AAV5 vectors carrying either the mouse or the human CNGA3 driven by a cone-specific 2.1-Kb red/green opsin promoter [89]. Follow-up studies after 6 years showed the animals had normal vision restored and were measured as demonstrated by ERG and other functional tests. This led to the initiation of clinical trials in CNGA3 achromatopsia patients (NCT02935517 and NCT02610582) [39].
30.4.3 LCA
Leber Congenital Amaurosis (LCA), first described by Theodore Leber in 1869, encompasses a set of autosomal recessive congenital rod–cone dystrophies (RCDs). The prevalence ranges from 2 to 3 in every 100,000 newborns and is the major cause of blindness in children. Around 15 genes (IMPDH1, AIPL1, CRB1, CEP290, CRX, GUCY2D, LRAT, RD3, RDH12, MERTK, RPGRIP1, TULP1, SPATA5, RPE65, and LCA5) (http://www.sph.uth.tmc.edu/RetNet/) that are required for normal vision are involved whose mutation result in LCA early in childhood. These genes are responsible for the development of photoreceptor cells, phototransduction and phagocytic processes in normal retina. Other structures such as cilia are needed for the perception of vision. Mutations in CEP290 (15%), AIPL1(12%), GUCY2D (12%), and RPE65 (8%) genes are the most common with other gene mutations accounting for a small percentage (5%) of LCA patients.
Gene therapy for RPE65 in a naturally occurring canine model of RPE65 with visual impairments similar to that observed in human LCA type II were treated with subretinal injection of rAAV-RPE65. The dogs demonstrated improvements in that visual function establishing a proof-of-concept to treat LCA [90]. A long-term follow-up of over 3 years showed stable expression of RPE65 in target areas of the treated eyes and recovered significant retinal function as demonstrated by ERG and other tests [91]. In 2007, the first clinical trial (later two additional trials followed) for LCA had begun with reports of the initial phase of clinical trials in 2008 stating that AAV-RPE65 used were safe and effective over a follow-up of 1 year post treatment in patients [92, 93]. Thereafter, successful Phase I to III clinical trials of gene therapy of RPE65 using Luxturna were reported leading to its approval by the FDA for commercial use in 2017 [94, 95].
30.4.4 Stargardt Disease
Stargardt disease (STGD1) is a juvenile macular degeneration with a prevalence of 1 in 8000–10,000 individuals [96]. However, the age of onset could be during adolescence or any time in adulthood [96]. During the visual cycle, all-trans-retinal is transported out of the discs into the cytosol by ATP binding cassette subfamily A member 4 (ABCA4) transmembrane transporter in the photoreceptors where it gets converted to all-trans-retinol by dehydrogenases (RDH8). Phototransduction results in the formation of bisretinoid A2E (fluorophore of lipofuscin), a by-product that is toxic. The ABCA4 protein is responsible for the removal of these substances out of the cell. A nonfunctional ABCA4 results in the accumulation of these toxic substances causing the death of photoreceptor and atrophy of surrounding RPE cells [97]. Patients with mutations in the ABCA4 gene experience progressive central vision loss leading to blindness due to death of the photoreceptor cells [98, 99]. Currently, there is no cure for ABCA4 mutation related to Stargardt disease. ABCA4 cDNA is large (6.8 kb) which would require a suitable vector system such as dual AAVs, IDLVs, or compacted DNA nanoparticles for efficient gene delivery and expression (refer Sect. 30.2 of this chapter). ABCA4 null mice exhibit phenotypic expression similar to humans [100]. Nanoparticles have been studied in STGD1 mice models where CK30PEG carrying human ABCA4 cDNA and human interphotoreceptor retinoid-binding protein (IRBP) or mouse opsin (MOP) promoters were tested. Expression of ABCA4 was observed at 2 and 8 months post injection and had rescued the phenotype [101]. Traditional AAV vectors are not efficient in the packaging and transduction of large genes [102]. Ghosh lab in India [3] and MacLaren lab in the UK are involved in strategies to package ABCA4 as split gene into dual AAV vector systems toward treatment for STGD1. Recently, therapeutic levels of ABCA4 were achieved using the overlapping AAV strategy and which showed the first proof-of-concept in ABCA4 knockout murine model. Truncated proteins that are formed due to dual vector strategies were reduced by optimizing recombination. Functional ABCA4 protein was observed in photoreceptor outer segments of the mice retina with a successful reversal of the phenotype [103]. This approach could thus be applied to a large animal model followed by clinical trials for gene therapy of Stargardt disease using dual AAVs.
30.4.5 X-Linked Juvenile Retinoschisis
X-linked juvenile retinoschisis (XLRS) is early-onset macular degeneration occurring in males with a prevalence of 1:5000 to 25,000 males worldwide. This condition results from mutations in (RS1) gene encoding retinoschisin 1 protein required for cell adhesion, organization, and structural maintenance of the retina. Patients experience poor vision, accompanied by congenital nystagmus, strabismus, vitreous hemorrhage, retinal detachment leading to blindness in severe forms [104]. Preclinical gene therapy studies for retinoschisis were carried out in rabbits and the RS1 knockout mice, where intravitreal administration with self-complementary AAV8-scRS/IRBPhRS showed rescue of the disease phenotype [105, 106]. These successful results led to the initiation of clinical trials and recent reports of phase I/IIa are reported by Cukras et al., [107].
30.5 Gene Therapy of Retinal Neovascularization
Certain retinal pathological conditions like diabetic retinopathy (DR) [108] and age-related macular degeneration (AMD) [109] are caused due to hypertrophic, neovascular formations in the retina and choroid. These are relatively common conditions leading to age-related progressive blindness. AMD affects individuals of age 50 and above. Currently, FDA-approved treatment for these conditions are repeated intravitreal injections of antibodies against VEGF (vascular endothelial growth factor). AAV mediated gene therapy for DR involves strategies to protect nerves and blood vessels from damage or by inhibiting the neovascular networks and vascular hyperpermeability. Antibody approaches targeting sFlt-1, Flt23k, and PEDF have been studied on small and large animal models [110,111,112,113,114]. Other targets to inhibit angiogenesis that are being tested are endostatin, angiostatin, and metalloproteinase-3 [115,116,117]. Gene therapy to prevent neovascular formations in the case of wet AMD involves AAV2 vectors carrying sFLT-1 and sFLT01 that have been studied in animal models as well as phase 1 and 2 clinical trials. Reports of these studies have demonstrated the treatment approach to be safe and effective in correcting the vision of the majority of patients in clinical trials [118,119,120,121,122].
30.6 Gene Therapy of Syndrome-Associated Retinal Degenerations
Usher syndrome type I is caused by mutations in the myosin VIIa gene (MYO7A), present in the RPE. Patients with this syndrome experience early-onset RP phenotype and hearing loss by birth. A murine model, the shaker1 (Myo7ash1-4626SB) mouse, has been extensively used for preclinical studies [123]. In 2007, the first gene therapy study using third-generation self-inactivating LVs encoding a CMV promoter-driven MYO7a gene were administered subretinally in the eyes of the shaker1 mice. The reversal of the phenotype was observed as the ciliary function was restored [124]. A recent study used subretinal injection of an equine infectious anemia virus (EIAV) vector system carrying the MYO7A gene driven by CMV promoter, which led to the production of the protein and restoration of vision in knockout mice. Safety was assessed in monkeys which consequently led to the development of UshStat, for clinical trials of Usher type 1B syndrome gene therapy [125].
30.7 Conclusion
The genetic basis of a disease and phenotypic variance were discovered and described by scientists and clinicians from the 1800s (refer Fig. 30.1) There has always been hope to cure or correct the mutations that lead to hereditary disorders. Over the past two decades, gene therapy has developed from ideation to proof-of-concept to clinical trials being conducted across the world. Of all diseases, gene therapy for monogenic inherited diseases, retinal diseases in particular have reached clinical trials early and have now been approved for treatment in many countries. Viral and nonviral methods have been explored for their gene delivery efficiencies to treat various dystrophies. Strategies to overcome and assess adverse immune reactions, toxicities, insertional mutagenesis without compromising gene delivery and expression efficacies are key to a successful gene therapy. Proof-of-concept in vitro and in vivo animal model studies are the initial supportive data that are essential for a treatment approach to achieve clinical approval. With successful clinical reports of patients treated with gene augmentation therapies for retinal dystrophies, “future looks brighter” indeed for other ocular disorders.
References
Auricchio A, Kobinger G, Anand V, Hildinger M, O’Connor E, Maguire AM, et al. Exchange of surface proteins impacts on viral vector cellular specificity and transduction characteristics: the retina as a model. Hum Mol Genet. 2001;10(26):3075–81.
Lebherz C, Maguire A, Tang W, Bennett J, Wilson JM. Novel AAV serotypes for improved ocular gene transfer. J Gene Med. 2008;10(4):375–82.
Ghosh A, Yue Y, Duan D. Efficient transgene reconstitution with hybrid dual AAV vectors carrying the minimized bridging sequences. Hum Gene Ther. 2011;22(1):77–83.
Williams DS, Fisher SK. Prevention of rod disk shedding by detachment from the retinal pigment epithelium. Invest Ophthalmol Vis Sci. 1987;28(1):184–7.
Wensel TG. Chapter 51 – Molecular biology of vision. In: Brady ST, Siegel GJ, Albers RW, Price DL, editors. Basic neurochemistry. 8th ed. New York: Academic Press; 2012. p. 889–903.
Gal A, Li Y, Thompson DA, Weir J, Orth U, Jacobson SG, et al. Mutations in MERTK, the human orthologue of the RCS rat retinal dystrophy gene, cause retinitis pigmentosa. Nat Genet. 2000;26(3):270–1.
Daya S, Berns KI. Gene therapy using adeno-associated virus vectors. Clin Microbiol Rev. 2008;21(4):583–93.
Pereira DJ, McCarty DM, Muzyczka N. The adeno-associated virus (AAV) rep protein acts as both a repressor and an activator to regulate AAV transcription during a productive infection. J Virol. 1997;71(2):1079–88.
Harper SQ, Hauser MA, DelloRusso C, Duan D, Crawford RW, Phelps SF, et al. Modular flexibility of dystrophin: implications for gene therapy of Duchenne muscular dystrophy. Nat Med. 2002;8(3):253–61.
Duan D, Yue Y, Yan Z, Engelhardt JF. A new dual-vector approach to enhance recombinant adeno-associated virus-mediated gene expression through intermolecular cis activation. Nat Med. 2000;6(5):595–8.
Yan Z, Zhang Y, Duan D, Engelhardt JF. Trans-splicing vectors expand the utility of adeno-associated virus for gene therapy. Proc Natl Acad Sci U S A. 2000;97(12):6716–21.
Ghosh A, Yue Y, Lai Y, Duan D. A hybrid vector system expands adeno-associated viral vector packaging capacity in a transgene-independent manner. Mol Ther. 2008;16(1):124–30.
Maddalena A, Tornabene P, Tiberi P, Minopoli R, Manfredi A, Mutarelli M, et al. Triple vectors expand AAV transfer capacity in the retina. Mol Ther. 2018;26(2):524–41.
Hanen K, Chloé C, Laure P, Sylvain F, Deniz D. Dosage thresholds and influence of transgene cassette in adeno-associated virus–related toxicity. Hum Gene Ther. 2018;29(11):1235–41.
Wiley LA, Burnight ER, Kaalberg EE, Jiao C, Riker MJ, Halder JA, et al. Assessment of Adeno-associated virus serotype tropism in human retinal explants. Hum Gene Ther. 2018;29(4):424–36.
Petrs-Silva H, Dinculescu A, Li Q, Min SH, Chiodo V, Pang JJ, et al. High-efficiency transduction of the mouse retina by tyrosine-mutant AAV serotype vectors. Mol Ther. 2009;17(3):463–71.
Zhong L, Li B, Mah CS, Govindasamy L, Agbandje-McKenna M, Cooper M, et al. Next generation of adeno-associated virus 2 vectors: point mutations in tyrosines lead to high-efficiency transduction at lower doses. Proc Natl Acad Sci U S A. 2008;105(22):7827–32.
Petrs-Silva H, Dinculescu A, Li Q, Deng W-T, Pang J-J, Min S-H, et al. Novel properties of tyrosine-mutant AAV2 vectors in the mouse retina. Mol Ther. 2011;19(2):293–301.
Hickey DG, Edwards TL, Barnard AR, Singh MS, de Silva SR, McClements ME, et al. Tropism of engineered and evolved recombinant AAV serotypes in the rd1 mouse and ex vivo primate retina. Gene Ther. 2017;24:787.
Kay CN, Ryals RC, Aslanidi GV, Min SH, Ruan Q, Sun J, et al. Targeting photoreceptors via intravitreal delivery using novel, capsid-mutated AAV vectors. PLoS One. 2013;8(4):e62097.
Lei B, Zhang K, Yue Y, Ghosh A, Duan D. Adeno-associated virus serotype-9 mediated retinal outer plexiform layer transduction is mainly through the photoreceptors. Adv Exp Med Biol. 2010;664:671–8.
Stieger K, Cronin T, Bennett J, Rolling F. Adeno-associated virus mediated gene therapy for retinal degenerative diseases. Methods Mol Biol (Clifton, NJ). 2011;807:179–218.
Allocca M, Mussolino C, Garcia-Hoyos M, Sanges D, Iodice C, Petrillo M, et al. Novel adeno-associated virus serotypes efficiently transduce murine photoreceptors. J Virol. 2007;81(20):11372–80.
Weber M, Rabinowitz J, Provost N, Conrath H, Folliot S, Briot D, et al. Recombinant adeno-associated virus serotype 4 mediates unique and exclusive long-term transduction of retinal pigmented epithelium in rat, dog, and nonhuman primate after subretinal delivery. Mol Ther. 2003;7(6):774–81.
Yang GS, Schmidt M, Yan Z, Lindbloom JD, Harding TC, Donahue BA, et al. Virus-mediated transduction of murine retina with adeno-associated virus: effects of viral capsid and genome size. J Virol. 2002;76(15):7651–60.
Palfi A, Chadderton N, O’Reilly M, Nagel-Wolfrum K, Wolfrum U, Bennett J, et al. Efficient gene delivery to photoreceptors using AAV2/rh10 and rescue of the Rho(−/−) mouse. Mol Ther Methods Clin Dev. 2015;2:15016.
Klimczak RR, Koerber JT, Dalkara D, Flannery JG, Schaffer DV. A novel adeno-associated viral variant for efficient and selective intravitreal transduction of rat Muller cells. PLoS One. 2009;4(10):e7467.
Dalkara D, Kolstad KD, Guerin KI, Hoffmann NV, Visel M, Klimczak RR, et al. AAV mediated GDNF secretion from retinal glia slows down retinal degeneration in a rat model of retinitis pigmentosa. Mol Ther. 2011;19(9):1602–8.
Boshart M, Weber F, Jahn G, Dorsch-Hasler K, Fleckenstein B, Schaffner W. A very strong enhancer is located upstream of an immediate early gene of human cytomegalovirus. Cell. 1985;41(2):521–30.
Schorpp M, Jager R, Schellander K, Schenkel J, Wagner EF, Weiher H, et al. The human ubiquitin C promoter directs high ubiquitous expression of transgenes in mice. Nucleic Acids Res. 1996;24(9):1787–8.
Niwa H, Yamamura K, Miyazaki J. Efficient selection for high-expression transfectants with a novel eukaryotic vector. Gene. 1991;108(2):193–9.
Esumi N, Oshima Y, Li Y, Campochiaro PA, Zack DJ. Analysis of the VMD2 promoter and implication of E-box binding factors in its regulation. J Biol Chem. 2004;279(18):19064–73.
Nicoletti A, Kawase K, Thompson DA. Promoter analysis of RPE65, the gene encoding a 61-kDa retinal pigment epithelium-specific protein. Invest Ophthalmol Vis Sci. 1998;39(3):637–44.
Busskamp V, Duebel J, Balya D, Fradot M, Viney TJ, Siegert S, et al. Genetic reactivation of cone photoreceptors restores visual responses in retinitis pigmentosa. Science. 2010;329(5990):413–7.
Wang Y, Macke JP, Merbs SL, Zack DJ, Klaunberg B, Bennett J, et al. A locus control region adjacent to the human red and green visual pigment genes. Neuron. 1992;9(3):429–40.
Khani SC, Pawlyk BS, Bulgakov OV, Kasperek E, Young JE, Adamian M, et al. AAV-mediated expression targeting of rod and cone photoreceptors with a human rhodopsin kinase promoter. Invest Ophthalmol Vis Sci. 2007;48(9):3954–61.
Zhu X, Ma B, Babu S, Murage J, Knox BE, Craft CM. Mouse cone arrestin gene characterization: promoter targets expression to cone photoreceptors. FEBS Lett. 2002;524(1–3):116–22.
Xiong W, Wu DM, Xue Y, Wang SK, Chung MJ, Ji X, et al. AAV cis-regulatory sequences are correlated with ocular toxicity. Proc Natl Acad Sci U S A. 2019;116(12):5785–94.
Gootwine E, Abu-Siam M, Obolensky A, Rosov A, Honig H, Nitzan T, et al. Gene augmentation therapy for a missense substitution in the cGMP-binding domain of ovine CNGA3 gene restores vision in day-blind sheep. Invest Ophthalmol Vis Sci. 2017;58(3):1577–84.
Reichel FF, Dauletbekov DL, Klein R, Peters T, Ochakovski GA, Seitz IP, et al. AAV8 can induce innate and adaptive immune response in the primate eye. Mol Ther. 2017;25(12):2648–60.
Bainbridge JW, Mehat MS, Sundaram V, Robbie SJ, Barker SE, Ripamonti C, et al. Long-term effect of gene therapy on Leber’s congenital amaurosis. N Engl J Med. 2015;372(20):1887–97.
Dimopoulos IS, Hoang SC, Radziwon A, Binczyk NM, Seabra MC, MacLaren RE, et al. Two-year results after AAV2-mediated gene therapy for Choroideremia: the Alberta experience. Am J Ophthalmol. 2018;193:130–42.
Pacak CA, Sakai Y, Thattaliyath BD, Mah CS, Byrne BJ. Tissue specific promoters improve specificity of AAV9 mediated transgene expression following intra-vascular gene delivery in neonatal mice. Genet Vaccines Ther. 2008;6(1):13.
Xue K, Groppe M, Salvetti AP, MacLaren RE. Technique of retinal gene therapy: delivery of viral vector into the subretinal space. Eye (London, England). 2017;31(9):1308–16.
Kotterman MA, Yin L, Strazzeri JM, Flannery JG, Merigan WH, Schaffer DV. Antibody neutralization poses a barrier to intravitreal adeno-associated viral vector gene delivery to non-human primates. Gene Ther. 2015;22(2):116–26.
Boye SE, Alexander JJ, Witherspoon CD, Boye SL, Peterson JJ, Clark ME, et al. Highly efficient delivery of Adeno-associated viral vectors to the primate retina. Hum Gene Ther. 2016;27(8):580–97.
Song H, Bush RA, Zeng Y, Qian H, Wu Z, Sieving PA. Trans-ocular electric current in vivo enhances AAV-mediated retinal gene transduction after Intravitreal vector administration. Mol Ther Methods Clin Dev. 2019;13:77–85.
Wobus CE, Hügle-Dörr B, Girod A, Petersen G, Hallek M, Kleinschmidt JA. Monoclonal antibodies against the adeno-associated virus type 2 (AAV-2) capsid: epitope mapping and identification of capsid domains involved in AAV-2-cell interaction and neutralization of AAV-2 infection. J Virol. 2000;74(19):9281–93.
Blacklow NR, Hoggan MD, Rowe WP. Serologic evidence for human infection with adenovirus-associated viruses. J Natl Cancer Inst. 1968;40(2):319–27.
Erles K, Sebokova P, Schlehofer JR. Update on the prevalence of serum antibodies (IgG and IgM) to adeno-associated virus (AAV). J Med Virol. 1999;59(3):406–11.
Bennett J, Maguire AM, Cideciyan AV, Schnell M, Glover E, Anand V, et al. Stable transgene expression in rod photoreceptors after recombinant adeno-associated virus-mediated gene transfer to monkey retina. Proc Natl Acad Sci U S A. 1999;96(17):9920–5.
Anand V, Chirmule N, Fersh M, Maguire AM, Bennett J. Additional transduction events after subretinal readministration of recombinant adeno-associated virus. Hum Gene Ther. 2000;11(3):449–57.
Stieger K, Colle MA, Dubreil L, Mendes-Madeira A, Weber M, Le Meur G, et al. Subretinal delivery of recombinant AAV serotype 8 vector in dogs results in gene transfer to neurons in the brain. Mol Ther. 2008;16(5):916–23.
Stieger K, Schroeder J, Provost N, Mendes-Madeira A, Belbellaa B, Le Meur G, et al. Detection of intact rAAV particles up to 6 years after successful gene transfer in the retina of dogs and primates. Mol Ther. 2009;17(3):516–23.
Miyoshi H, Takahashi M, Gage FH, Verma IM. Stable and efficient gene transfer into the retina using an HIV-based lentiviral vector. Proc Natl Acad Sci U S A. 1997;94(19):10319–23.
Bennett J, Wilson J, Sun D, Forbes B, Maguire A. Adenovirus vector-mediated in vivo gene transfer into adult murine retina. Invest Ophthalmol Vis Sci. 1994;35(5):2535–42.
Li T, Adamian M, Roof DJ, Berson EL, Dryja TP, Roessler BJ, et al. In vivo transfer of a reporter gene to the retina mediated by an adenoviral vector. Invest Ophthalmol Vis Sci. 1994;35(5):2543–9.
Ali RR, Reichel MB, Thrasher AJ, Levinsky RJ, Kinnon C, Kanuga N, et al. Gene transfer into the mouse retina mediated by an adeno-associated viral vector. Hum Mol Genet. 1996;5(5):591–4.
Flannery JG, Zolotukhin S, Vaquero MI, LaVail MM, Muzyczka N, Hauswirth WW. Efficient photoreceptor-targeted gene expression in vivo by recombinant adeno-associated virus. Proc Natl Acad Sci U S A. 1997;94(13):6916–21.
Philippe S, Sarkis C, Barkats M, Mammeri H, Ladroue C, Petit C, et al. Lentiviral vectors with a defective integrase allow efficient and sustained transgene expression in vitro and in vivo. Proc Natl Acad Sci U S A. 2006;103(47):17684–9.
Chen J, Patil S, Seal S, McGinnis JF. Rare earth nanoparticles prevent retinal degeneration induced by intracellular peroxides. Nat Nanotechnol. 2006;1(2):142–50.
del Pozo-Rodriguez A, Delgado D, Solinis MA, Gascon AR, Pedraz JL. Solid lipid nanoparticles for retinal gene therapy: transfection and intracellular trafficking in RPE cells. Int J Pharm. 2008;360(1–2):177–83.
Han Z, Conley SM, Naash MI. AAV and compacted DNA nanoparticles for the treatment of retinal disorders: challenges and future prospects. Invest Ophthalmol Vis Sci. 2011;52(6):3051–9.
Adijanto J, Naash MI. Nanoparticle-based technologies for retinal gene therapy. Eur J Pharm Biopharm. 2015;95:353–67.
Read SP, Cashman SM, Kumar-Singh R. A poly(ethylene) glycolylated peptide for ocular delivery compacts DNA into nanoparticles for gene delivery to post-mitotic tissues in vivo. J Gene Med. 2010;12(1):86–96.
Masuda I, Matsuo T, Yasuda T, Matsuo N. Gene transfer with liposomes to the intraocular tissues by different routes of administration. Invest Ophthalmol Vis Sci. 1996;37(9):1914–20.
Mendes HF, van der Spuy J, Chapple JP, Cheetham ME. Mechanisms of cell death in rhodopsin retinitis pigmentosa: implications for therapy. Trends Mol Med. 2005;11(4):177–85.
Hartong DT, Berson EL, Dryja TP. Retinitis pigmentosa. Lancet (London, England). 2006;368(9549):1795–809.
Daiger SP, Bowne SJ, Sullivan LS. Perspective on genes and mutations causing retinitis pigmentosa. Arch Ophthalmol. 2007;125(2):151–8.
Kaushal S, Khorana HG. Structure and function in rhodopsin. 7. Point mutations associated with autosomal dominant retinitis pigmentosa. Biochemistry. 1994;33(20):6121–8.
Cideciyan AV, Sudharsan R, Dufour VL, Massengill MT, Iwabe S, Swider M, et al. Mutation-independent rhodopsin gene therapy by knockdown and replacement with a single AAV vector. Proc Natl Acad Sci U S A. 2018;115(36):E8547–e56.
Meindl A, Dry K, Herrmann K, Manson F, Ciccodicola A, Edgar A, et al. A gene (RPGR) with homology to the RCC1 guanine nucleotide exchange factor is mutated in X-linked retinitis pigmentosa (RP3). Nat Genet. 1996;13(1):35–42.
Thompson DA, Khan NW, Othman MI, Chang B, Jia L, Grahek G, et al. Rd9 is a naturally occurring mouse model of a common form of retinitis pigmentosa caused by mutations in RPGR-ORF15. PLoS One. 2012;7(5):e35865.
Hong DH, Yue G, Adamian M, Li T. Retinitis pigmentosa GTPase regulator (RPGRr)-interacting protein is stably associated with the photoreceptor ciliary axoneme and anchors RPGR to the connecting cilium. J Biol Chem. 2001;276(15):12091–9.
Zeiss CJ, Acland GM, Aguirre GD. Retinal pathology of canine X-linked progressive retinal atrophy, the locus homologue of RP3. Invest Ophthalmol Vis Sci. 1999;40(13):3292–304.
Kropatsch R, Akkad DA, Frank M, Rosenhagen C, Altmuller J, Nurnberg P, et al. A large deletion in RPGR causes XLPRA in Weimaraner dogs. Canine Genet Epidemiol. 2016;3:7.
Hong DH, Li T. Complex expression pattern of RPGR reveals a role for purine-rich exonic splicing enhancers. Invest Ophthalmol Vis Sci. 2002;43(11):3373–82.
Beltran WA, Cideciyan AV, Lewin AS, Iwabe S, Khanna H, Sumaroka A, et al. Gene therapy rescues photoreceptor blindness in dogs and paves the way for treating human X-linked retinitis pigmentosa. Proc Natl Acad Sci U S A. 2012;109(6):2132–7.
Deng WT, Dyka FM, Dinculescu A, Li J, Zhu P, Chiodo VA, et al. Stability and safety of an AAV vector for treating RPGR-ORF15 X-linked retinitis Pigmentosa. Hum Gene Ther. 2015;26(9):593–602.
Pawlyk BS, Bulgakov OV, Sun X, Adamian M, Shu X, Smith AJ, et al. Photoreceptor rescue by an abbreviated human RPGR gene in a murine model of X-linked retinitis pigmentosa. Gene Ther. 2016;23(2):196–204.
Fischer MD, McClements ME, Martinez-Fernandez De La Camara C, Bellingrath JS, Dauletbekov D, Ramsden SC, et al. Codon-optimized RPGR improves stability and efficacy of AAV8 gene therapy in two mouse models of X-linked retinitis Pigmentosa. Mol Ther. 2017;25(8):1854–65.
Martinez-Fernandez De La Camara C, Nanda A, Salvetti AP, Fischer MD, MacLaren RE. Gene therapy for the treatment of X-linked retinitis pigmentosa. Expert Opin Orphan Drugs. 2018;6(3):167–77.
Audo I, Mohand-Said S, Boulanger-Scemama E, Zanlonghi X, Condroyer C, Demontant V, et al. MERTK mutation update in inherited retinal diseases. Hum Mutat. 2018;39(7):887–913.
Conlon TJ, Deng W-T, Erger K, Cossette T. Pang J-j, Ryals R, et al. preclinical potency and safety studies of an AAV2-mediated gene therapy vector for the treatment of MERTK associated retinitis pigmentosa. Hum Gene Ther Clin Dev. 2013;24(1):23–8.
Ghazi NG, Abboud EB, Nowilaty SR, Alkuraya H, Alhommadi A, Cai H, et al. Treatment of retinitis pigmentosa due to MERTK mutations by ocular subretinal injection of adeno-associated virus gene vector: results of a phase I trial. Hum Genet. 2016;135(3):327–43.
Lam BL, Davis JL, Gregori NZ, MacLaren RE, Girach A, Verriotto JD, et al. Choroideremia gene therapy phase 2 clinical trial: 24-month results. Am J Ophthalmol. 2019;197:65–73.
Lhériteau E, Petit L, Weber M, Le Meur G, Deschamps J-Y, Libeau L, et al. Successful gene therapy in the RPGRIP1-deficient dog: a large model of cone–rod dystrophy. Mol Ther. 2014;22(2):265–77.
Ofri R, Averbukh E, Ezra-Elia R, Ross M, Honig H, Obolensky A, et al. Six years and counting: restoration of Photopic retinal function and visual behavior following gene augmentation therapy in a sheep model of CNGA3 Achromatopsia. Hum Gene Ther. 2018;29:1376.
Banin E, Gootwine E, Obolensky A, Ezra-Elia R, Ejzenberg A, Zelinger L, et al. Gene augmentation therapy restores retinal function and visual behavior in a sheep model of CNGA3 Achromatopsia. Mol Ther. 2015;23(9):1423–33.
Acland GM, Aguirre GD, Ray J, Zhang Q, Aleman TS, Cideciyan AV, et al. Gene therapy restores vision in a canine model of childhood blindness. Nat Genet. 2001;28(1):92–5.
Acland GM, Aguirre GD, Bennett J, Aleman TS, Cideciyan AV, Bennicelli J, et al. Long-term restoration of rod and cone vision by single dose rAAV-mediated gene transfer to the retina in a canine model of childhood blindness. Mol Ther. 2005;12(6):1072–82.
Bainbridge JW, Smith AJ, Barker SS, Robbie S, Henderson R, Balaggan K, et al. Effect of gene therapy on visual function in Leber’s congenital amaurosis. N Engl J Med. 2008;358(21):2231–9.
Maguire AM, Simonelli F, Pierce EA, Pugh EN Jr, Mingozzi F, Bennicelli J, et al. Safety and efficacy of gene transfer for Leber’s congenital amaurosis. N Engl J Med. 2008;358(21):2240–8.
Russell S, Bennett J, Wellman JA, Chung DC, Yu ZF, Tillman A, et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, phase 3 trial. Lancet (London, England). 2017;390(10097):849–60.
Bennett J, Wellman J, Marshall KA, McCague S, Ashtari M, DiStefano-Pappas J, et al. Safety and durability of effect of contralateral-eye administration of AAV2 gene therapy in patients with childhood-onset blindness caused by RPE65 mutations: a follow-on phase 1 trial. Lancet (London, England). 2016;388(10045):661–72.
Tanna P, Strauss RW, Fujinami K, Michaelides M. Stargardt disease: clinical features, molecular genetics, animal models and therapeutic options. Br J Ophthalmol. 2017;101(1):25–30.
Molday RS. Chapter twenty-four – insights into the molecular properties of abca4 and its role in the visual cycle and stargardt disease. In: Hejtmancik JF, Nickerson JM, editors. Progress in molecular biology and translational science, vol. 134. Amsterdam: Academic Press; 2015. p. 415–31.
Cideciyan AV, Aleman TS, Swider M, Schwartz SB, Steinberg JD, Brucker AJ, et al. Mutations in ABCA4 result in accumulation of lipofuscin before slowing of the retinoid cycle: a reappraisal of the human disease sequence. Hum Mol Genet. 2004;13(5):525–34.
Kennedy CJ, Rakoczy PE, Constable IJ. Lipofuscin of the retinal pigment epithelium: a review. Eye. 1995;9(6):763–71.
Weng J, Mata NL, Azarian SM, Tzekov RT, Birch DG, Travis GH. Insights into the function of rim protein in photoreceptors and etiology of Stargardt’s disease from the phenotype in abcr knockout mice. Cell. 1999;98(1):13–23.
Han Z, Conley SM, Makkia RS, Cooper MJ, Naash MI. DNA nanoparticle-mediated ABCA4 delivery rescues Stargardt dystrophy in mice. J Clin Invest. 2012;122(9):3221–6.
Lai Y, Yue Y, Duan D. Evidence for the failure of adeno-associated virus serotype 5 to package a viral genome > or = 8.2 kb. Mol Ther. 2010;18(1):75–9.
McClements ME, Barnard AR, Singh MS, Issa PC, Jiang Z, Radu RA, et al. An AAV dual vector strategy ameliorates the stargardt phenotype in adult Abca4−/− mice. Hum Gene Ther. 2019;30(5):590–600.
Molday RS, Kellner U, Weber BHF. X-linked juvenile retinoschisis: clinical diagnosis, genetic analysis, and molecular mechanisms. Prog Retin Eye Res. 2012;31(3):195–212.
Marangoni D, Wu Z, Wiley HE, Zeiss CJ, Vijayasarathy C, Zeng Y, et al. Preclinical safety evaluation of a recombinant AAV8 vector for X-linked retinoschisis after intravitreal administration in rabbits. Hum Gene Ther Clin Dev. 2014;25(4):202–11.
Bush RA, Zeng Y, Colosi P, Kjellstrom S, Hiriyanna S, Vijayasarathy C, et al. Preclinical dose-escalation study of Intravitreal AAV-RS1 gene therapy in a mouse model of X-linked Retinoschisis: dose-dependent expression and improved retinal structure and function. Hum Gene Ther. 2016;27(5):376–89.
Cukras C, Wiley HE, Jeffrey BG, Sen HN, Turriff A, Zeng Y, et al. Retinal AAV8-RS1 gene therapy for X-linked Retinoschisis: initial findings from a phase I/IIa trial by Intravitreal delivery. Mol Ther. 2018;26(9):2282–94.
Wang JH, Ling D, Tu L, van Wijngaarden P, Dusting GJ, Liu GS. Gene therapy for diabetic retinopathy: are we ready to make the leap from bench to bedside? Pharmacol Ther. 2017;173:1–18.
Moore NA, Bracha P, Hussain RM, Morral N, Ciulla TA. Gene therapy for age-related macular degeneration. Expert Opin Biol Ther. 2017;17(10):1235–44.
Pechan P, Rubin H, Lukason M, Ardinger J, DuFresne E, Hauswirth WW, et al. Novel anti-VEGF chimeric molecules delivered by AAV vectors for inhibition of retinal neovascularization. Gene Ther. 2009;16(1):10–6.
Haurigot V, Villacampa P, Ribera A, Bosch A, Ramos D, Ruberte J, et al. Long-term retinal PEDF overexpression prevents neovascularization in a murine adult model of retinopathy. PLoS One. 2012;7(7):e41511.
Lamartina S, Cimino M, Roscilli G, Dammassa E, Lazzaro D, Rota R, et al. Helper-dependent adenovirus for the gene therapy of proliferative retinopathies: stable gene transfer, regulated gene expression and therapeutic efficacy. J Gene Med. 2007;9(10):862–74.
Ideno J, Mizukami H, Kakehashi A, Saito Y, Okada T, Urabe M, et al. Prevention of diabetic retinopathy by intraocular soluble flt-1 gene transfer in a spontaneously diabetic rat model. Int J Mol Med. 2007;19(1):75–9.
Gehlbach P, Demetriades AM, Yamamoto S, Deering T, Xiao WH, Duh EJ, et al. Periocular gene transfer of sFlt-1 suppresses ocular neovascularization and vascular endothelial growth factor-induced breakdown of the blood-retinal barrier. Hum Gene Ther. 2003;14(2):129–41.
Auricchio A, Behling KC, Maguire AM, O’Connor EM, Bennett J, Wilson JM, et al. Inhibition of retinal neovascularization by intraocular viral-mediated delivery of anti-angiogenic agents. Mol Ther. 2002;6(4):490–4.
Biswal MR, Prentice HM, Dorey CK, Blanks JC. A hypoxia-responsive glial cell-specific gene therapy vector for targeting retinal neovascularization. Invest Ophthalmol Vis Sci. 2014;55(12):8044–53.
Le Gat L, Gogat K, Bouquet C, Saint-Geniez M, Darland D, Van Den Berghe L, et al. In vivo adenovirus-mediated delivery of a uPA/uPAR antagonist reduces retinal neovascularization in a mouse model of retinopathy. Gene Ther. 2003;10(25):2098–103.
Constable IJ, Pierce CM, Lai CM, Magno AL, Degli-Esposti MA, French MA, et al. Phase 2a randomized clinical trial: safety and post hoc analysis of subretinal rAAV.sFLT-1 for wet age-related macular degeneration. EBioMedicine. 2016;14:168–75.
Heier JS, Kherani S, Desai S, Dugel P, Kaushal S, Cheng SH, et al. Intravitreous injection of AAV2-sFLT01 in patients with advanced neovascular age-related macular degeneration: a phase 1, open-label trial. Lancet (London, England). 2017;390(10089):50–61.
Rakoczy EP, Lai CM, Magno AL, Wikstrom ME, French MA, Pierce CM, et al. Gene therapy with recombinant adeno-associated vectors for neovascular age-related macular degeneration: 1 year follow-up of a phase 1 randomised clinical trial. Lancet (London, England). 2015;386(10011):2395–403.
Lai CM, Estcourt MJ, Wikstrom M, Himbeck RP, Barnett NL, Brankov M, et al. rAAV.sFlt-1 gene therapy achieves lasting reversal of retinal neovascularization in the absence of a strong immune response to the viral vector. Invest Ophthalmol Vis Sci. 2009;50(9):4279–87.
Lai CM, Shen WY, Brankov M, Lai YK, Barnett NL, Lee SY, et al. Long-term evaluation of AAV-mediated sFlt-1 gene therapy for ocular neovascularization in mice and monkeys. Mol Ther. 2005;12(4):659–68.
Gibson F, Walsh J, Mburu P, Varela A, Brown KA, Antonio M, et al. A type VII myosin encoded by the mouse deafness gene shaker-1. Nature. 1995;374(6517):62–4.
Hashimoto T, Gibbs D, Lillo C, Azarian SM, Legacki E, Zhang XM, et al. Lentiviral gene replacement therapy of retinas in a mouse model for usher syndrome type 1B. Gene Ther. 2007;14(7):584–94.
Zallocchi M, Binley K, Lad Y, Ellis S, Widdowson P, Iqball S, et al. EIAV-based retinal gene therapy in the shaker1 mouse model for usher syndrome type 1B: development of UshStat. PLoS One. 2014;9(4):e94272.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Gopinath, C., Sarkar, S., Ghosh, A. (2021). Gene Therapy for Retinal Diseases. In: Prakash, G., Iwata, T. (eds) Advances in Vision Research, Volume III. Essentials in Ophthalmology. Springer, Singapore. https://doi.org/10.1007/978-981-15-9184-6_30
Download citation
DOI: https://doi.org/10.1007/978-981-15-9184-6_30
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-9183-9
Online ISBN: 978-981-15-9184-6
eBook Packages: MedicineMedicine (R0)