
Abstract
Our health is closely related to our environment, such that a healthy environment brings healthy living and vice versa. Pollution due to air is a prime environmental aspect contributing to the burden of different diseases in human and also has considerable economic impact. The total air pollution accounts approximately 7 million deaths globally. Pollutants produced as combustion of particulate matter have demonstrated a time-series effect on human health. The size of inhalable particulate matter (PM10 and PM2.5) affects the mortality and morbidity upon short- and long-term exposure among all population, with highest effect on elderly individuals. Exposure to these pollutants produces the pathological alteration, such as increased inflammatory response, systemic oxidative stress, cardiovascular stress, and change in pulmonary autonomous nervous system activity. These molecular pathological events trigger several pulmonary and cardiovascular manifestations in human. From epidemiology point of view, it has been explored that among different air pollutants, particulate matter, ozone, carbon monoxide, nitrogen dioxide and sulfur dioxide are the major ones. The highest mortality is mainly observed in Asian populations as compared to Europeans and Americans. The top ten countries with the highest mortality are China, India, Pakistan, Bangladesh, Nigeria, the United States, Russia, Brazil, and Philippines, respectively. In this chapter, we reviewed different PM exposure-based epidemiological studies with more focus on high ambient Total Suspended Particulate (TSP) levels. It has also been found that overall absolute risk for mortality due to PM exposure is higher for cardiovascular compared to pulmonary disorders in case of both acute and chronic exposures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
8.1 Introduction
Human health is closely associated to the environment of its habitat and healthy habitat leads to healthy living (Seymour 2016). The damage done to the current environmental condition of our planet is quite noticeable. Climate change and air pollution due to different pollutants in the air is one of the major concerns all around the world. It has been estimated that a large number leading to premature deaths and adverse health effects are linked to air pollution. According to WHO reports, air pollution is the global, massive, single, and most significant environmental health risk. Health complications as a result of frequent exposure to air pollutants have high considerable economic impact, consequently increasing health care costs and premature deaths (Kelly and Fussell 2015). Pollutants that subsidize to air pollution can be divided into primary and secondary. Primary air pollutants are those which have their own origin such as carbon monoxide, nitrogen oxides, volatile organic compounds (VOC), sulfur dioxide, and particulate matter. Secondary air pollutants are those which are the outcome of primary air pollutants such as ozone and smog (Admassu et al. 2005).
Due to a drastic increase in urbanization and industrialization all over the world, there is a steep rise in the concentrations of various air pollutants. This has led to adverse impact on human existence in various forms like climate change, global warming, and flooding (Admassu et al. 2004). Inefficient pollution control methods, inadequacy of regulations enforcement, uncontrolled vehicular emissions, and increasing deforestation are components responsible for rising environmental air pollutants (McCarthy et al. 2009; Aggarwal and Jain 2015). Inhalation of fine particles causes severe lung disorders due to its high ambient TSP levels along with elevated levels of particulate matters (PM) PM10 and PM2.5 (Carrico et al. 2003; Begum et al. 2008). The most significant contributor of particulate matter is mainly vehicle exhaust (Agarwal et al. 2006). In most of the developing countries and cities, a distinct population of particulate matter is mostly found that are having deleterious impact on different categories of populations. The effect of particulate matter on human health can only be reduced when there is sharp decline in vehicular or construction-based activities (World Bank 2004). The adverse health impact of PM is directly proportional to its size, where PM2.5 and PM0.1 have the most hazardous impact as compared to PM10 (Dockery et al. 1993; Pope et al. 2002). Premature death from heart and lung disease, chronic bronchitis, asthma attacks and respiratory illness are topmost health effects of PM (Smith 2002). Various epidemiological studies have estimated the possible health impacts resulting from different categories of particulate matter locally, regionally, and globally. World health report (2016) also states that ambient particulate matter pollution is capable of 1.4% total annual global mortality with an estimated death of about 0.8 million people.
8.2 Air Pollution and Human Health
Air pollution is known as contagion mixture of both indoor and outdoor surroundings caused by any chemical, biological, or physical agents which tend to alter the air quality (Ji et al. 2017). The substances, either natural or anthropogenic, that contaminate the environment are known as pollutant. Air pollution could be categorized as natural or man-made and stationary or mobile on the basis of source of emissions. Natural sources include volcanic eruption, fires, storm, fog, and mist while man-made sources include vehicular exhaust, industrial emissions, crop residue burning, biomass burning, mining, and domestic activities (Barnes et al. 1999). On the basis of origin, air pollution sources can be of different types like point, area, and line. Point sources are those which have single known source of pollution from which pollutants are discharged such as factory smokestack, pipe, and ditch. Area sources are those sources of pollution which emit a substance from a particular area, for example, open burning and forest fires and evaporation losses from large spills of volatile liquids. Line sources are idealized geometric emitter that can be represented by an emission source consisting of straight line which may be of finite or infinite length, for example, roadway air pollution, aircraft emissions, noise pollution, etc. In 2005, WHO released “WHO Air quality guidelines” that has set up various permissible limits for different air pollutants that directly impact the human health. These guidelines help to reduce air pollutants to a certain level by regular monitoring and evaluation of their concentrations in the air. With the implementation of PM10 guidelines by WHO, there is significant improvement in its concentration from 70 to 20 μg/m3 and subsequently mortality rates were reduced to approximately 15%. This guide code applied worldwide is established through expert appraisal of scientific evidence for particulate matter (PM): limit for PM2.5: 10 μg/m3 annual mean; 25 μg/m3 24-h mean, limits for PM10: 20 μg/m3 annual mean; 50 μg/m3 24-h mean (WHO 2016). Comprehensive infinite risk for mortality due to PM vulnerability is greater for cardiovascular disease (CDV) compared to pulmonary diseases in respect to short- as well as long-term exposures. Even at identical acute relative risk elevations estimated between cardiovascular and pulmonary mortality, CVD account rises by 69%.
Air pollution is regarded as one of the dominant killers worldwide, responsible for 7 million deaths per year, out of which 600,000 are children (Yang et al. 2017). WHO reported that around 300 million children have been affected due to outdoor air pollution at global level. Air pollution is also spreading at a very higher rate in both urban and rural areas, mainly on low and middle income countries. South East Asia and Western Pacific regions had population-based burden of 3.3 million and 2.6 million death toll rate due to indoor and outdoor pollution, respectively (WHO 2012) (Table 8.1). Stronger link between both indoor and outdoor air pollution is associated with increased cardiovascular disease (Endes et al. 2017; Kelly and Fussell 2017; Bhatia et al. 2017), hypertension, diabetes (Vora et al. 2014), rheumatoid arthritis (De Roos et al. 2014), pulmonary diseases like asthma, lung cancer (Dominici et al. 2006; Machado et al. 2014; Bai et al. 2018) oxidative stress, physical disability (Weuve et al. 2016) and inflammation (Møller et al. 2014). Among all the air pollution-associated diseases, cardiovascular tops the chart with the highest incidence of 69% death toll rate. WHO also suggested that the concentrations of particulate matter can be reduced by adopting right policy measures due to which 15% of the lives can be saved at worldwide level.
Among different air pollutants, PM, ozone (O3), carbon monoxide (CO), nitrogen dioxide (NO2), and sulfur dioxide (SO2) are the major ones (Fröhlich 2017) (Table 8.2). The total air pollution including particulate matter (PM), O3, CO, SO2, NOx, and VOCs accounts for loss of approximately 7 million lives globally. The highest mortality is mainly in Asian countries. Top ten countries with the highest mortality rate due to air pollution are China followed by India, Pakistan, Bangladesh, Nigeria, the United States, Russia, Brazil, and Philippines, respectively.
8.2.1 Particulate Matter (PM)
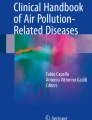
Particulate matter (PM) is the mixture of solid and liquid droplets suspended in the air and differentiated on the basis of different particle sizes (Manigrasso et al. 2017; Olatunji et al. 2018; Voidazan et al. 2018). PM not only evolves from natural sources such as volcanic eruptions but also through human actions such as burning of fossil fuels, waste disposal, and metal extraction activities. Both natural and artificial sources may emit either precursors like SO2, NO2, VOCs along with favorable meteorological conditions forming PM or can directly emit in the atmosphere through vehicular exhaust and industrial emissions (Olopade et al. 2017; Rahman et al. 2017). Coarse dust particles (PM10) are those having particle size of less than or equal to 10 μm in diameter and are inhalable particles (Fig. 8.1). The main sources for coarse dust particles are large-scale crushing or grinding activities during construction and suspension of road dust due to vehicular activities. It can deposit in thoracic or upper trachea-bronchial region causing severe health problems (Yin et al. 2017). Fine particles (PM2.5) are those having aerodynamic diameter size of 2.5 μm or smaller which are generally invisible and can only be observed using high-resolution microscopes. The prime source includes various types of combustion, motor vehicles, wood burning, and industrial processes (You et al. 2017b) as shown in Fig. 8.1. These are soot particles and are linked to various health impacts and are deposited in deeper lungs.

Particulate matter size classification: Comparative analysis of PM10 and PM2.5. Size determines the behavior of atmospheric particle, where PM10 has quintuple diameter to hair and PM2.5 quaternary smaller than PM10
(a) Coarse Particles (PM10)
Coarse particles are one of the primary air pollutants (solid and liquid particles floating) that are respirable and thus can penetrate deep into the respiratory system. These PM are 5–7 times smaller in diameter compared to human hair (50–70 μm diameter) (Fig. 8.1). The particular matter composition, shape, size, presence of additional pollutants, and metrological factors determine its toxicity and concentration (Patton et al. 2014; Kelly and Fussell 2015). PM10 is one of the significant air pollutants which is the biggest threat to all living organisms. When compared from the era of industrialization to the present time, coarse particles have become a significant air pollutant in urban, suburban, rural, and remote parts of the globe (Fang et al. 2013; Li et al. 2015; Yang et al. 2019). In urban cities of most countries, PM10 level is above the WHO and their respective countries standard (WHO 2016). PM10 lead to inflammatory responses, congenital heart failure, ischemic heart disease, respiratory and circulatory fatality, birth risk, and cancer risk (Hemminki and Pershagen 1994; Zhang et al. 2014; Agay-Shay et al. 2013; Silbajoris et al. 2011). Larger particular matter of and around 10 μm endures solely in the nose and throat part and smaller particles of and around 1 μm easily accumulate in the lower regions of the lungs. The intermediate sizes greater than 1 μm and less than 10 μm reside between the upper part of the respiratory tract. Setiawan et al. (2014) reported the positive strong correlation between higher concentrations of PM10 and their harmful impacts on human beings. As per the global data statistics, prominent higher concentration of PM10 is reported in Asia, followed by Africa and European countries. Moreover, according to 2016 data, top ten polluted countries around the globe are Cameron, Egypt, Mauritania, Niger, Nigeria, Pakistan, Qatar, Saudi Arabia, Tajikistan, and United Arab Emirates, respectively, as shown in Fig. 8.2.

Exposure to PM10 air pollution (2016): World Map showing annual mean exposure of population weighted exposure to ambient PM10 pollution throughout the globe on country basis
(b) Fine Particles (PM2.5)
Very tiny particles in the atmosphere of and around 2.5 mm wide are denoted as fine particles or PM2.5. These particles originate from dust, dirt, soot, and smoke, very tiny enough and are easily inhaled (Luo et al. 2018). According to Liu et al. (2018), it has been found that PM2.5 have shown stronger correlation with respect to their size range and human health effects. Infants and elderly population are at highest risk due to the inhalation of PM2.5 particles and most susceptible to pulmonary and heart diseases. Vulnerability to fine particulate matter (2.5 μm aerodynamic diameter) contributes to a predicted loss of 915,900 lives in China alone each year. Among these number of deaths, around 15% are attributable to PM2.5 due to transportation activities (Arashiro et al. 2018; Luyts et al. 2018). Severe health risks are associated with ultrafine particles (<0.1 μm) and composing PM2.5 and their main source is vehicular exhaust (Li et al. 2017; Hou et al. 2018; Kim et al. 2018; Kumar et al. 2018). Ultrafine particles can travel extensively deep into the lungs (Baldauf et al. 2016; Fonceca et al. 2018; Boogaard and van Erp 2019) as well as associated with the biomarkers of cardiovascular diseases leading to DNA hypomethylation and mortality (Atkinson et al. 2016; Kim et al. 2016; Simonetti et al. 2018; He et al. 2018; Louwies et al. 2018). PM2.5 components such as black carbon (BC) also have been associated with cardiorespiratory impacts (Donaldson et al. 2001; He et al. 2018). Since research on UFP and BC is not sufficient compared to PM as a whole, their effects are usually not included in mortality estimates (You et al. 2017a; Vreeland et al. 2017).
The annual risk of PM2.5 is increasing with years resulting in 3.0 million deaths (5.2% of global deaths in 2016). More than 50% occur in China and India. Comparative analysis showed that PM2.5 attributed to the increase in deaths by 68% from 1990 to 2016. World data clearly indicates that prominent higher concentration of PM10 is found in Asian followed by African and European countries. According to 2016 data, top ten polluted countries around the globe are Burkina Faso, Cameron, Egypt, Kuwait, Mauritania, Niger, Nigeria, Qatar, Saudi Arabia, and United Arab Emirates, respectively, as shown in Fig. 8.3.

Exposure to PM2.5 air pollution (2016): World Map showing annual mean exposure to PM2.5 pollution throughout the globe on country basis
The nature of particulate matter in the atmosphere determines the entry, absorption potential, and deposition of particles in the lungs (Clark et al. 2010). Particles which are larger than PM10 never reach the lungs as they get trapped within the nose and throat. Particles ranging from 10 μm in diameter or less become the most burdensome to the human health. Particles size smaller than 5 μm can be transported to bronchial tubes, while particles size of 2.5 μm or smaller can reside into the lung’s deepest portion (Prospero 1999; Mahowald et al. 2014).
8.2.2 Ozone (O3)
Ozone is the important component of photochemical smog and one of the greenhouse gases (Shi et al. 2016; Tham et al. 2017). It is a highly reactive, oxidative gas responsible for severe lung diseases, cardio-attacks and strokes all around the globe (Nuvolone et al. 2018). Ozone concentrations are mostly higher in summer season due to its photochemical nature and favorable meteorological conditions like high temperature and high solar radiation. Ozone is a secondary pollutant which is formed by its precursors like nitrogen oxides, carbon monoxide, and volatile organic compounds present in the atmosphere (Kan et al. 2012). Moreover, when hydroxyl radical (OH) reacts with trace gases, it leads to high concentration of ozone and hence becomes responsible for global warming. The increasing O3 level gives rise to serious health outcomes like inflammation, respiratory injury, and decreased lung activity (Kinney 1999; Koken et al. 2003).
8.2.3 Carbon Monoxide (CO)
CO is an outcome of carbon-containing fuels formed by mechanism of incomplete combustion (Yang et al. 2016). CO has the property to readily combine with hemoglobin due to its high affinity (200–250 times) as compared to oxygen and forms carboxyhemoglobin (COHb) (Gorman et al. 2003). When concentrations of COHb increases rapidly, oxygen level also sharply decreases and leads to morbidity and mortality (Graber et al. 2007; Pissuwan et al. 2016). CO is regarded as the most toxic inhalable gas which is both outdoor as well as indoor air pollutant and leads to sudden illness and death (Von Burg 1999). CO arises mainly from oxidation of fossil fuels like coal, kerosene, wood, and natural gases. Various forms of tobacco smoke and automobile exhaust also contain large concentration of CO. The level of CO ranges from 0.5 to 100 parts per million (ppm) both in indoor and outdoor environment. The standard range of indoor CO levels ranges from 0.5 to 5 ppm. This value exceeds the standard range in the presence of tobacco smoke in environment, incompetent heating, and ventilation up to 100 ppm (Penney et al. 2010), whereas, in urban zones, levels are typically from 20 to 40 ppm. In the periphery around highways and heavy construction site, the range of CO becomes much higher (Raub 1999). As it reaches to peak or exceeds standard range, the chance of CO poisoning initially shows the acute symptoms of headache, dizziness, and shortness of breath (Gorman et al. 2003; Piantadosi 1999). Further increase in exposure of level from acute to chronic leads to neurotoxicity, unconsciousness, cognitive and visual impairment and ultimately death. Research around years have determined chronic CO exposure as a risk factor for cardiovascular disease (Samoli et al. 2007). The underlining mechanisms for cardiotoxicity are associated with chronic CO risk identified to be directly or indirectly associated with activation and modulation of various intracellular signaling mechanisms. These mechanisms probably include CO-dependent regulation of cell proliferation, lipid-raft associated signaling protein caveolin-1, and modulation of NADPH oxidase (Taillé et al. 2005).
8.2.4 Nitrogen Oxides
The primary source of NO is fossil fuel combustion in motor vehicles and industrial emissions particularly from power generation plants. NO has the ability to react with ammonia, moisture, and other compounds to give rise to small particles (Ibeneme et al. 2016). These tiny particles can aggravate existing severe cardiovascular disease and asthma (Latza et al. 2009; Zhang et al. 2016). NO2 is a one of the criteria pollutant, which is the outcome of lightning, volcanic eruption, oxidation of NO to NO2, power houses, motor vehicles, bacterial source and combustion of fossil fuels (more than 70% of NO2 Production) (WHO). NO2 can affect human health mostly at higher or even at low concentrations. Epidemiological studies show that atmospheric NO2 attributes about 5–7% lungs cancer disease in both smokers and nonsmokers (Goudarzi et al. 2012; Omidi et al. 2016). It has severe acute effects followed by chronic effects like pulmonary as well as chronic obstructive pulmonary diseases (COPD), infant mortality chronic cough, bronchitis, infant mortality, and visibility (Barnett et al. 2005). According to WHO, the annual mean value of NO2 is 40 μg/m3 with respect to human health; however, even short-term exposure to NO2 leads to cardiovascular-related risks to exposed population (Brook 2008).
8.2.5 Sulfur Dioxide (SO2)
The main source of SO2 is from combustion of sulfur-containing fuels, especially in power plants and diesel engines, vehicular exhaust, and fossil fuel combustion (Silva et al. 2017). Sulfur dioxide majorly produces cytotoxic effect on retinal pigment of epithelial cells (Rall 1974; Bose et al. 2016). Short-term effect of SO2 on human health results in respiratory diseases in children (asthma, mainly in winter) (Pikhart et al. 2001; Heinrich et al. 2002) and registered a large number of both morbidity and mortality cases (Katsouyanni et al. 1997). SO2 leads to respiratory aggravation, bronchoconstriction, and most importantly cardiovascular disorders. Initial phase of cardiovascular abnormalities includes reduced heart rate vulnerability (Tunnicliffe et al. 2001). SO2 also causes respiratory symptoms such as shortness of breath, increased risk of asthma, and respiratory mortality (Clark et al. 2010; Chen et al. 2007; Zhao et al. 2008).
8.3 Air Pollution-Induced Cardiovascular Index and Their Consequences to Morbidity and Mortality
Pope and Dockery have highlighted the relationship between cardiovascular manifestation and air pollution. Their findings suggest that short-term daily exposure to particulate matter shows higher risk of cardiovascular-related mortality than all other diseases (Pope and Dockery 2006). Acute PM exposure contributes to 69% CVD-related deaths and 28% pulmonary-related manifestation (Brook et al. 2010). Some more critical studies have also been highlighted and give the addition prospective on exposure time and airborne pathogenesis.
Short-Term Exposure
Shorter exposure with a high level of pollutants is proportionally liked to the CVD-associated mortality. Increase in PM10 quantity by 10 μg/m3 promotes 1–2% surge in cardiovascular and pulmonary disease cases (Schwartz 2001). However, elevated exposure to PM2.5 by 10 μg/m3 increases the risk of myocardial infraction around 2.8%. Particulate matter-based morbidity and mortality are independent of other gaseous co-pollutants (i.e., NO2, SO2, O3, and CO). Acute exposure to O3 causes cardiopulmonary defect in middle-age person with no previous CVD (Bell et al. 2007). 1.0 μg/m3 increase of CO leads to 1.25% cardiovascular-related deaths, and short-term exposure to NO2 also promotes CVD pathogenesis (Samoli et al. 2006, 2007). The particulate matter-associated CVD risks appeared to be more in elderly person, while the younger population are more susceptible to NO2 exposure (Argacha et al. 2016).
Long-Term/Chronic Exposure
High PM level with prolonged exposure shows a greater magnitude than acute exposure. World Health Organization highlighted that constant exposure to PM2.5 leads to 800 thousand premature deaths per year and it ranked as the 13th leading cause of worldwide death (WHO 2002). Several other reports also suggest a strong association between chronic exposure to PM and cardiovascular mortality (Pope et al. 2004a). The annual increase of PM10 by 10 μg/m3 and PM2.5 by 5 μg/m3 promotes the risk of myocardial infarction by 10–13% (Cesaroni et al. 2014). Long-term exposure to PM2.5 causes premature arteriosclerosis and with traffic-related pollutants, it promotes coronary artery calcification (Kaufman et al. 2016). Chronic effect of airborne contaminants on mortality is examined in cohort studies. These studies involve exposure of pollutants and a large number of volunteers, and provide the data related to the impact of the pollutants on human life span (Künzli et al. 2001).
Air pollutants cause considerable alterations in cardiovascular indexes like heart rate, heart rate variability, arrhythmia, heart failure, cardiac arrest, ischemic heart disease, cerebrovascular disease (Stroke), blood pressure, vascular tone atherosclerosis, thrombosis, and coagulation (Table 8.3). These air pollution-induced cardiovascular indexes affect the viability of human life and increase mortality.
8.3.1 Heart Rate (HR) and Heart Rate Variability (HRV)
The increase of PM2.5 by 15.5 μg/m3 reduces the heart rate in old-aged people, while PM10 exposure (100 μg/m3) increases the heart rate by 5–10 beats per minute (POPE et al. 1999; Gold et al. 2000). Heart rate viability is strongly associated with the rate of exposure to particulate matter in both acute and chronic condition. Effect on HRV is correlated with the presence of nickel and iron in airborne particulate matter (Chang et al. 2007).
8.3.2 Arrhythmia, Heart Failure, and Cardiac Arrest
Cohort studies exhibit that arrhythmia, heart failure, and cardiac arrest are associated with increased exposure to PM2.5. Rise of PM2.5 by 10 μg/m3 increases heart failure cases by 1.28% (Dominici et al. 2006). Air pollutants also increase ventricular size and myocardial fibrogenesis that are the causes of cardiac arrhythmia and arrest (Wold et al. 2012).
8.3.3 Ischemic Heart Disease
Several studies have shown the relation between increased level of PM2.5 and ischemic heart disease. Coronary heart disease is a major cause of cardiovascular-related mortality and increase of PM2.5 by 10 μg/m3 promotes coronary heart disease cases (Pope et al. 2004a). PM2.5 along with PM10, NO2, and O3 are key causative factors for myocardial infarction, which is the first manifestation of ischemic heart disease. Patients aged 75 years or above acquire more ST-elevated myocardial infraction on exposure to PM10. However, younger population are more susceptible to fine and ultrafine particulate matter and NO2 exposure (Argacha 2017).
8.3.4 Thrombosis and Coagulation
Exposure of air pollutants to the cardiovascular system promotes hypercoagulability of blood. This physiological effect is either due to the entry of particulate matter into bloodstream or release of PM-induced circulating factors (Brook et al. 2010). Recent study reveals that exposure of concentrated ambient particulates (CAPs) to mice activates its pulmonary autonomous nervous system (ANS), which further stimulates the inflammatory responses and release of cytokines from alveolar macrophages to disseminate prothrombotic state (Chiarella et al. 2014).
8.3.5 Cerebrovascular Disease/Stroke
Data of 188 countries between 1990 and 2013 from Global Burden of Disease database shows 29% of air pollutant-induced cardiac manifestation are contributed only by stroke (Feigin et al. 2016). Many studies have found a positive association between air pollution, stroke, and mortality. Annual increase of air pollution by 5 μg/m3 enhances the risk of stroke up to 19% (Stafoggia et al. 2014). Time-series experiment has highlighted that increased air pollutants (notably PM, NO2, CO, and O3) level is associated with cerebrovascular disease. Air pollution-induced cardiac stroke has good correlation with ischemic, but not exactly with hemorrhagic stroke (Hong et al. 2002). Similar studies have also revealed that PM2.5 and CO-induced stroke mortality is predominant in warm season than the cold season (Kettunen et al. 2007). The short-term elevated level of the gaseous pollutants like O3, NO2, and CO also promotes the risk of stroke (Henrotin et al. 2010).
8.3.6 Blood Pressure, Vascular Tone, and Atherosclerosis
Increase exposure of PM2.5 by 10.5 μg/m3 enhances the diastolic pressure from 2.7 to 2.8 Hg in cardiac patients, and further increase of PM2.5 by 13.9 μg/m3 enhances diastolic pressure by 6.95 Hg without affecting systolic pressure (Zanobetti et al. 2004). Exposure to concentrated ambient particulates (CAPs) by 150 μg/m3 along with O3 (120 parts/billion) causes significant constriction of bronchial artery (up to 0.09 mm) (Brook et al. 2002). Higher exposure to PM2.5 and carbon particulates is correlated with increase in vascular constriction (O’Neill et al. 2005). However, chronic exposure to the fine and ultrafine particulate matter causes severe atherosclerosis. In human, 10 μg/m3 of PM2.5 promotes the carotid artery thickness by 5.9% (Suwa et al. 2002; Künzli et al. 2005). Long-term exposure to traffic-related PM2.5 (22.8 μg/m3) also promotes coronary artery calcification.
8.3.7 Hypertension
Long-term exposure to PM promotes the vascular oxidative stress, activation of ANS, inflammatory responses, increased sensitivity, and release of angiotensin II and endothelin which in turn develop systemic hypertension in animal (Brook et al. 2010; Ying et al. 2014). Controlled acute exposure to the concentrated ambient particles with ozone causes diastolic hypertension due to ANS imbalance (Urch et al. 2005).
8.4 Mechanism of Cardiovascular Toxicity Induced by Air Pollutants
The number of epidemiological studies strongly shows that air pollutants exposure causes a significant impact on the cardiovascular system. Association between cardiovascular complication and air pollution is now supported and asserted by the vast number of studies; however, the exact causative factors of pollutants and the molecular physiology by which airborne pollutants trigger cardiovascular abnormalities are understood to only some extent. Air pollutants which cause cardiovascular stress are gaseous and particulate in nature. Fine (PM2.5) and ultrafine (PM0.1) particulate matter are major components for manifestation of cardiovascular disease (Brook et al. 2010). The acute exposure to air pollutants leads to the development of myocardial infarction and change in heart viability, heart rate, blood pressure, blood coagulability, and vascular tone while prolonging exposure (chronic exposure) disseminates the progression of atherosclerosis (Brook et al. 2010).
Accumulating a number of evidences show that PM causes the chemical modification of oligonucleotides, resulting in the genetic and epigenetic changes which lead to aberrant genomic expression. Along with this it also induces oxidative stress and abnormal secretion of the stress-related hormone. To explain the mechanism of airborne pollutants-induced pathogenesis, three notable hypotheses were proposed, which explain the association between cardiovascular disease and air pollutants exposure (Fig. 8.4):
-
PM-induced pulmonary inflammatory responses promote oxidative and cardiovascular stress.
-
Exposure to PM leads to autonomic nervous system (ANS) imbalance and pathological alterations.
-
Inhaled air pollutants directly translocate in the circulatory system and perturb the distant cell and tissue components of the cardiovascular system.

Pathological mechanism of cardiovascular toxicity associated with increasing air pollutants
8.4.1 PM-induced Pulmonary Inflammatory Responses Promote Oxidative and Cardiovascular Stress
Air pollutants initiate a number of inflammatory reactions as soon as they come in contact with the lungs (GHIO et al. 2000). Particulate matter is a mixture of a wide range of particles (0.1–10 μm); these particles are typically composed of combustion originated carbon center, peripheral metal, and hydrocarbon. Larger and fine particulate matter (PM10 and PM2.5) are the major cause of pulmonary stress. PM induces the oxidative stress, inflammation, and pulmonary cell toxicity in the lungs (Donaldson and Stone 2003). Administration of aqueous PM induces the generation of reactive oxygen species (ROS), which increases bronchoalveolar localization of macrophages. Alveolar-localized macrophages release cytokines, interleukins, and TNF and start the inflammatory response. These PM also increase the bronchoalveolar lavage alpha-1 antitrypsin and fibronectin level that are the symptoms of pulmonary necrosis (GHIO and DEVLIN 2001). Prolonged exposure to polycyclic aromatic hydrocarbon-related PM2.5 rises the level of 8-hydroxy-2-deoxyguanosine and etheno-DNA adducts, which are the biomarker for oxidative DNA damage. These DNA adducts are predominant in road traffic workers (Bagryantseva et al. 2010). Air pollutant-induced elevated oxidize plasma LDL, IL-1&6 and TNF modulate the signaling of the cardiovascular system, which leads to the sympathovagal imbalance (Jacobs et al. 2011; Bind et al. 2012).
8.4.2 Exposure of PM Leads to Autonomic Nervous System (ANS) Imbalance and Pathological Alterations
Diesel exhaust (DE) particulate matter increases the heart rate and reduces the heart rate viability; it extends the ventricular depolarization and shortens repolarization, which lead to the development of arrhythmia. DE air pollutants alter the activity of TRP channels of the airway sensory neurons, present in the respiratory system. Functional alteration in these channels stimulates the midbrain which further excites the cortex and preganglionic autonomic neuron, resulting in the imbalance of autonomic nervous system, blood pressure, and heart rate (HR) (Hazari et al. 2011). A recent study has showed that exposure to the concentrated ambient particles (CAPs) stimulates the sympathetic nervous system and induces the secretion of catecholamine which further activates β2-adrenergic receptor of alveolar macrophages. Active β2-adrenergic receptor promotes the release of IL-6 that initiates the hypercoagulability of blood (prothrombotic state) (Chiarella et al. 2014).
8.4.3 Inhaled Air Pollutants Directly Translocate in the Circulatory System and Perturb the Distant Cell and Tissue Components of the Cardiovascular System
Ultrafine particulate matter (UFP) (PM0.1) and gaseous pollutants are directly translocated in the circulatory system and affect the distance organs (e.g., heart) (Nemmar et al. 2002). Injection of isolated UFP from ambient air promotes the left ventricle ejection fraction (LVEF) without affecting the heart rate (HR). UFP exhibits the potentially harmful impact on preexisting coronary disease patients (Wold et al. 2006). UFP-mediated direct acute response triggers the production of ROS, which gives rise to myocardial and endothelial dysfunction (Przyklenk and Kloner 1989). Exposure to PM0.1 also induces the level of circulatory c-Protein and inflammatory factor, which are responsible for increasing blood coagulability, vasoconstriction, and myocardial ischemia (Peters et al. 1997; Brook et al. 2002; Pope et al. 2004b).
8.5 Epidemiology of Air Pollution and Cardiovascular Disease
Ninety-one percent of the global population is living in the area where the air index is below the WHO recommended limits. Level of air pollutants like SO2, NOx, O3, CO, and particulate matter (PM2.5 and PM10) increased with the time, which created a range of harmful effect over human health, vegetation, ecosystem, and climate. Industrial development has been marked as a key transition for the increase in SO2 emission; sulfur pollution was first viewed in Europe, followed by North America. These two continents contribute highest to the emission of sulfur dioxides in the atmosphere; North America’s SO2 emission pick was around 37.7 million tons in 1970 and around 71.2 million tons in Europe in 1980. Though industrial development in Asia and Africa started much later, these regions began SO2 emission in the late twentieth century (Klimont et al. 2013). Another air pollutant NOx (nitrogen oxide), emitted from the combustion of fossil fuel and biomass burning, also contributes to air pollution-induced health problem; NOx emission has been seen high in developing countries. North America and Europe were emitting around 7.0 metric tons of NO2 in the early nineteenth century. However, Asian and African continents had started the emission of NO in the late nineteenth century (Dignon and Hameed 1989). Ozone is another noxious atmospheric pollutant, and its global emission level increased by 7.2% from 1990 to 2015 (0.0568 ppm to 0.0609 ppm). In the most polluted country, i.e., Bangladesh, Brazil, China, India, and Pakistan, the level of ozone was enhanced from 14% to 25% between 1990 and 2015, although exposure of ozone has decreased in the United States and Indonesia by 0.0037 ppm and 0.0065 ppm, respectively (Cohen et al. 2017). These gaseous pollutants work as a precursor for the creation of particulate matter. Level of particulate matter (PM2.5) has increased from 31.5 μg/m3 (1990) to 35.02 μg/m3 (2016), and its concentration has increased more rapidly in highly polluted cities. Level of PM2.5 has remained stable in India and Pakistan, but its concentration in another South Asian country (Bangladesh) has increased since 2010. The highest surge of PM2.5 has been found in Nigeria (African country) after 2015. However, there has been a significant reduction in PM2.5 level reported in China, and a slight decrease in Brazil, Russia, and the United States. Higher concentration of PM2.5 in 2016 was reported in Nigeria (203 μg/m3), Saudi Arabia (187·8 μg/m3), Qatar (148·2 μg/m3), Egypt (126·7 μg/m3), Bangladesh (101·04 μg/m3), Mauritania (123.6 μg/m3), Nepal (78·0 μg/m3), India (75·3 μg/m3), and China (56·4 μg/m3), whereas the lowest PM2.5 exposure in 2016 is reported in Pacific Island countries and territories (PM2.5 ≤ 8·0 μg/m3). The analysis of global PM2.5 air pollution data to different geographical regions shows that the African continent has the highest PM2.5 burden than Asia and North America. However, Europe has the lowest level of PM2.5 (Fig. 8.5).

Trends of PM2.5 exposure in different geographical regions and globally polluted countries
About 7 million deaths (4.2 million outdoor pollution and 3.8 million household pollution) had happened in the year 2016 due to low air quality. Air pollutants attribute to many diseases like cardiovascular disease, lung cancer, and pulmonary disease, which cause premature death in the population. Most of the airborne-associated mortalities are due to cardiovascular pathogenesis. Particulate matter, SO2 and NOx are the major contaminants, causing the deleterious effect on human cardiovascular system. Studies done in more than 30 different European cities show that elevated level of SO2 and NOx are associated with increased cardiovascular abnormalities and mortality (Katsouyanni et al. 1997; Samoli et al. 2006). Increase in short-term exposure of SO2 and NO2 by 10 ppb enhance the risk of heart disease by 2.36 and 1.70, respectively (Newby et al. 2015). Myocardium is the most sensitive organ for SO2 and its exposure affects the cytochrome c oxidase activity of myocardial mitochondria, which leads to cardiovascular manifestation (Qin et al. 2016). American Heart Association in 2010 had stated that an increase of cardiovascular manifestation is associated with long-term exposure to PM2.5. Increased level of PM2.5 has elevated the mortality rate by 0.7 million (3.5 M to 4.2 M) between 1990 and 2015. Air pollution contributes to 7.5% global mortality and is ranked as the fifth global risk factor for deaths. Air pollutants exposure causes cardiovascular disease (58.4%), lung cancer (16.5%), and lower respiratory infection (24.7%). Cardiovascular disease is the major contributor to death associated with air pollution. PM2.5 exhibits sever effect on male compared to female (1018.6 deaths per 100,000 males, and 703.4 deaths per 100,000 females), and it also displays more impact on older people (aged >70 years) than younger ones (aged ≤5 years) (GBD 2016).
Cardiovascular disease (CVD) is the illness of the heart and blood vessels. It is one of the leading diseases in global health burden, which contributes around 31% of all global deaths. CVD plays a part in deaths of approximately 17.9 million people every year and out of this 80% of CVD deaths occurred due to heart attack and stroke. Air pollution is the major factor for cardiovascular-related abnormalities, and alone it had contributed to around 7 million deaths in 2016. More than 90% of these deaths had occurred in lower-income or middle-income countries. Asian countries (i.e., China, India, Pakistan, and Bangladesh) had highest pollutant-related mortality (2.25 million deaths), in which China was the top contributor with 0.94 million followed by India with 0.84 million deaths. The African region had 0.17 million CVD-associated deaths, in which Nigeria had the highest incident rate. American continent had 0.18 million air pollution-related causalities in 2016, in which the United States, Mexico, and Brazil were the major contributors. In Europe around 0.23 million deaths were reported in 2016 due to air pollution, in which Ukraine had carried the higher burden. Remaining casualties had occurred in Middle East (70,096), Oceania (5872), and Caribbean region (11,484) (Fig. 8.6) (WHO 2016).

(a) Total deaths attribution associated with air pollution in all the countries of the globe. (b) Graphical representation of death number in different regions of the world and (c) represent percentage distribution of mortality in the same
8.6 Summary and Recommendations
This chapter summarized the association between prevalence of major air pollutants and cardiovascular manifestation in the population. As per WHO report, four major components of air pollution are PM, O3, NOx, and SO2. Particulate matter is a critical component of air pollution and it contains all the hazardous organic and inorganic constituents. PM exposure causes more sever morbidity and mortality than other pollutants at any concentration. Even though WHO has recommended threshold level of 20 μg/m3 for PM10 and 10 μg/m3 for PM2.5 annually, other gaseous air pollutants like O3, NO2, and SO2 are also very crucial for increased airborne illness. Combination of these gaseous pollutants with particulates matter creates more harmful impact. WHO has also recommended the threshold level for these gaseous pollutants as 100 μg/m3 of O3 for 8 h, 40 μg/m3 of NOx annually, and 20 μg/m3 of SO2 for 24 h. Air pollution is a crucial environmental risk factor for human health and by reducing the air pollution level, countries can reduce disease and socioeconomic burdens. Outdoor pollution in both urban and rural areas caused around 4.2 million deaths in 2016. The case-crossover study done in Germany, the United States, Europe, and China shows that increased exposure to PM10 by 10 μg/m3 induces the 1.0–1.50% increase of cardiovascular cases. In further study on teen and adult population (0.5 million) with 16 years of follow-up shows that consequence of cardiovascular mortality increased by 8–18% for every 10.5 μg/m3 increase of PM2.5 level. Similarly, case-crossover studies done in China and the United States show that increase exposure to SO2 and NO2 by 10 μg/m3 elevates 2.0–3.0% arrhythmia and blood pressure cases. Ozone is also an important component of air pollution; several European studies reported that daily heart-related mortality increases by 0.4 per 10 μg/m3 rise of ozone. To tackle this issue many environment protection and health associated agencies have given the recommendation and guidelines. WHO has given the recommendation to the industries, power generation plant, municipal, agricultural waste management and transport to use clean technology that reduces the industrial emission, use of clean and heavy duty diesel vehicle, fuel with reduced sulfur content, renewable combustion free power source (light, water, and wind) and strict system to reduce the open garbage and biomass burning. Other agencies like EPA have set the limit for the emission of air pollutant from chemical plant, vehicle, and other industries. The European Environment Agency, with a network of 33 countries, gathered the data and made the assessment and policy for environment protection.
As specific therapy for air pollution illness is difficult to pinpoint due to diverse health consequences. The detrimental health impact of pollutants is not confined to the source site, since fine particles can travel further and can therefore affect the health of people living and working in the surrounding areas. Basic and fundamental new directions can enable better predictions for future conditions and scenarios. Joining hands among individuals along with NGOs in coordination with government can implement strong policy to reduce pollutant exposure using environmental education, safe clean technologies, and limiting pollution exposure strategies.
References
Admassu M, Wuhshet M, Tilaye T (2004) Sanitary survey in Gondar town. Ethiop J Heal Dev 18:39–42. https://doi.org/10.4314/ejhd.v18i1.9864
Admassu M, Wubshet M, Gelaw B (2005) A survey of bacteriological quality of drinking water in North Gondar. Ethiop J Heal Dev 18:112–115. https://doi.org/10.4314/ejhd.v18i2.9946
Agarwal R, Jayaraman G, Anand S, Marimuthu P (2006) Assessing respiratory morbidity through pollution status and meteorological conditions for Delhi. Environ Monit Assess 114:489–504. https://doi.org/10.1007/s10661-006-4935-3
Agay-Shay K, Friger M, Linn S et al (2013) Air pollution and congenital heart defects. Environ Res 124:28–34. https://doi.org/10.1016/j.envres.2013.03.005
Aggarwal P, Jain S (2015) Impact of air pollutants from surface transport sources on human health: a modeling and epidemiological approach. Environ Int 83:146–157. https://doi.org/10.1016/j.envint.2015.06.010
Arashiro M, Lin Y-H, Zhang Z et al (2018) Effect of secondary organic aerosol from isoprene-derived hydroxyhydroperoxides on the expression of oxidative stress response genes in human bronchial epithelial cells. Environ Sci Process Impacts 20:332–339. https://doi.org/10.1039/C7EM00439G
Argacha J-F (2017) Air pollution and myocardial infarction. Eur Heart J 38:141–141. https://doi.org/10.1093/eurheartj/ehw622
Argacha JF, Collart P, Wauters A et al (2016) Air pollution and ST-elevation myocardial infarction: a case-crossover study of the Belgian STEMI registry 2009–2013. Int J Cardiol 223:300–305. https://doi.org/10.1016/J.IJCARD.2016.07.191
Atkinson RW, Analitis A, Samoli E et al (2016) Short-term exposure to traffic-related air pollution and daily mortality in London, UK. J Expo Sci Environ Epidemiol 26:125–132. https://doi.org/10.1038/jes.2015.65
Bagryantseva Y, Novotna B, Rossner P et al (2010) Oxidative damage to biological macromolecules in Prague bus drivers and garagemen: impact of air pollution and genetic polymorphisms. Toxicol Lett 199:60–68. https://doi.org/10.1016/J.TOXLET.2010.08.007
Bai K-J, Chuang K-J, Chen J-K et al (2018) Investigation into the pulmonary inflammopathology of exposure to nickel oxide nanoparticles in mice. Nanomedicine 14:2329–2339. https://doi.org/10.1016/j.nano.2017.10.003
Baldauf RW, Devlin RB, Gehr P et al (2016) Ultrafine particle metrics and research considerations: review of the 2015 UFP workshop. Int J Environ Res Public Health 13:1054. https://doi.org/10.3390/ijerph13111054
Barnes J, Bender J, Lyons T, Borland A (1999) Natural and man-made selection for air pollution resistance. J Exp Bot 50:1423–1435. https://doi.org/10.1093/jxb/50.338.1423
Barnett AG, Williams GM, Schwartz J, Neller AH, Best TL, Petroeschevsky AL, Simpson RW (2005) Air pollution and child respiratory health. Am J Respir Crit Care Med 171(11):1272–1278
Begum BA, Biswas SK, Hopke PK (2008) Assessment of trends and present ambient concentrations of PM2.2 and PM10 in Dhaka, Bangladesh. Air Qual Atmos Heal 1:125–133. https://doi.org/10.1007/s11869-008-0018-7
Bell ML, Kim JY, Dominici F (2007) Potential confounding of particulate matter on the short-term association between Ozone and mortality in multisite time-series studies. Environ Health Perspect 115:1591–1595. https://doi.org/10.1289/ehp.10108
Bhatia S, Bhatia S, Mears J et al (2017) Seasonal periodicity of ischemic heart disease and heart failure. Heart Fail Clin 13:681–689. https://doi.org/10.1016/j.hfc.2017.05.004
Bind M-A, Baccarelli A, Zanobetti A et al (2012) Air pollution and markers of coagulation, inflammation, and endothelial function: associations and epigene-environment interactions in an elderly cohort. Epidemiology 23:332–340. https://doi.org/10.1097/EDE.0b013e31824523f0
Boogaard H, van Erp AM (2019) Assessing health effects of air quality actions: what’s next? Lancet Public Heal 4:e4–e5. https://doi.org/10.1016/S2468-2667(18)30235-4
Bose K, Lakshminarasimhan H, Sundar K, Kathiresan T (2016) Cytotoxic effect of ZnS nanoparticles on primary mouse retinal pigment epithelial cells. Artif Cells Nanomed Biotechnol 44:1764–1773. https://doi.org/10.3109/21691401.2015.1102739
Brook RD (2008) Cardiovascular effects of air pollution. Clin Sci 115(6):175–187
Brook RD, Brook JR, Urch B et al (2002) Inhalation of fine particulate air pollution and ozone causes acute arterial vasoconstriction in healthy adults. Circulation 105:1534–1536
Brook RD, Rajagopalan S, Pope CA et al (2010) Particulate matter air pollution and cardiovascular disease. Circulation 121:2331–2378. https://doi.org/10.1161/CIR.0b013e3181dbece1
Carrico CM, Kus P, Rood MJ et al (2003) Mixtures of pollution, dust, sea salt, and volcanic aerosol during ACE-Asia: radiative properties as a function of relative humidity. J Geophys Res 108:8650. https://doi.org/10.1029/2003JD003405
Cesaroni G, Forastiere F, Stafoggia M et al (2014) Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 348:f7412. https://doi.org/10.1136/bmj.f7412
Chang C-C, Hwang J-S, Chan C-C, Cheng T-J (2007) Interaction effects of ultrafine carbon black with iron and nickel on heart rate variability in spontaneously hypertensive rats. Environ Health Perspect 115:1012–1017. https://doi.org/10.1289/ehp.9821
Chen T-M, Kuschner WG, Gokhale J, Shofer S (2007) Outdoor air pollution: nitrogen dioxide, sulfur dioxide, and carbon monoxide health effects. Am J Med Sci 333(4):249–256
Chiarella SE, Soberanes S, Urich D et al (2014) β2-Adrenergic agonists augment air pollution–induced IL-6 release and thrombosis. J Clin Invest 124:2935–2946. https://doi.org/10.1172/JCI75157
Clark NA, Demers PA, Karr CJ et al (2010) Effect of early life exposure to air pollution on development of childhood asthma. Environ Health Perspect 118:284–290. https://doi.org/10.1289/ehp.0900916
Cohen AJ, Brauer M, Burnett R et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet (London, England) 389:1907–1918. https://doi.org/10.1016/S0140-6736(17)30505-6
De Roos AJ, Koehoorn M, Tamburic L et al (2014) Proximity to traffic, ambient air pollution, and community noise in relation to incident rheumatoid arthritis. Environ Health Perspect 122:1075–1080. https://doi.org/10.1289/ehp.1307413
Dignon J, Hameed S (1989) Global emissions of nitrogen and sulfur oxides from 1860 to 1980. JAPCA 39(2):180–186
Dockery DW, Pope CA, Xu X et al (1993) An association between air pollution and mortality in six U.S. cities. N Engl J Med 329:1753–1759. https://doi.org/10.1056/NEJM199312093292401
Dominici F, Peng RD, Bell ML et al (2006) Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 295:1127. https://doi.org/10.1001/jama.295.10.1127
Donaldson K, Stone V (2003) Current hypotheses on the mechanisms of toxicity of ultrafine particles. Ann Ist Super Sanita 39:405–410
Donaldson K, Stone V, Seaton A, MacNee W (2001) Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ Health Perspect 109:523–527. https://doi.org/10.1289/ehp.01109s4523
Endes S, Schaffner E, Caviezel S et al (2017) Is physical activity a modifier of the association between air pollution and arterial stiffness in older adults: the SAPALDIA cohort study. Int J Hyg Environ Health 220:1030–1038. https://doi.org/10.1016/j.ijheh.2017.06.001
Fang Y, Mauzerall DL, Liu J et al (2013) Impacts of 21st century climate change on global air pollution-related premature mortality. Clim Chang 121:239–253. https://doi.org/10.1007/s10584-013-0847-8
Feigin VL, Roth GA, Naghavi M et al (2016) Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol 15:913–924. https://doi.org/10.1016/S1474-4422(16)30073-4
Fonceca AM, Zosky GR, Bozanich EM et al (2018) Accumulation mode particles and LPS exposure induce TLR-4 dependent and independent inflammatory responses in the lung. Respir Res 19:15. https://doi.org/10.1186/s12931-017-0701-z
Fröhlich E (2017) Hemocompatibility of inhaled environmental nanoparticles: potential use of in vitro testing. J Hazard Mater 336:158–167. https://doi.org/10.1016/j.jhazmat.2017.04.041
GBD (2016). https://vizhub.healthdata.org/gbd-compare
GHIO AJ, DEVLIN RB (2001) Inflammatory lung injury after bronchial instillation of air pollution particles. Am J Respir Crit Care Med 164:704–708. https://doi.org/10.1164/ajrccm.164.4.2011089
GHIO AJ, KIM C, DEVLIN RB (2000) Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. Am J Respir Crit Care Med 162:981–988. https://doi.org/10.1164/ajrccm.162.3.9911115
Gold DR, Litonjua A, Schwartz J et al (2000) Ambient pollution and heart rate variability. Circulation 101:1267–1273
Gorman D, Drewry A, Huang YL, Sames C (2003) The clinical toxicology of carbon monoxide. Toxicology 187(1):25–38
Goudarzi G, Mohammadi MJ, Angali KA, Neisi AK, Babaei AA, Mohammadi B, Soleimani Z, Geravandi S (2012) Estimation of health effects attributed to NO2 exposure using AirQ model. Arch Hyg Sci 1:59–66
Graber JM, Macdonald SC, Kass DE et al (2007) Carbon monoxide: the case for environmental public health surveillance. Public Health Rep 122:138–144. https://doi.org/10.1177/003335490712200202
Hazari MS, Haykal-Coates N, Winsett DW et al (2011) TRPA1 and sympathetic activation contribute to increased risk of triggered cardiac arrhythmias in hypertensive rats exposed to diesel exhaust. Environ Health Perspect 119:951–957. https://doi.org/10.1289/ehp.1003200
He C, Song Y, Ichinose T et al (2018) Lipopolysaccharide levels adherent to PM2.5 play an important role in particulate matter induced-immunosuppressive effects in mouse splenocytes. J Appl Toxicol 38:471–479. https://doi.org/10.1002/jat.3554
Heinrich J, Hoelscher B, Frye C, Meyer I, Pitz M, Cyrys J, Wjst M, Neas L, Wichmann H-E (2002) Improved air quality in reunified Germany and decreases in respiratory symptoms. Epidemiology 13(4):394–401
Hemminki K, Pershagen G (1994) Cancer risk of air pollution: epidemiological evidence. Environ Health Perspect 102(Suppl 4):187–192. https://doi.org/10.1289/ehp.94102s4187
Henrotin J-B, Zeller M, Lorgis L et al (2010) Evidence of the role of short-term exposure to ozone on ischaemic cerebral and cardiac events: the Dijon Vascular Project (DIVA). Heart 96:1990–1996. https://doi.org/10.1136/hrt.2010.200337
Hong Y-C, Lee J-T, Kim H, Kwon H-J (2002) Air pollution: a new risk factor in ischemic stroke mortality. Stroke 33:2165–2169
Hou J, Sun H, Guo Y et al (2018) Associations between urinary monohydroxy polycyclic aromatic hydrocarbons metabolites and Framingham Risk Score in Chinese adults with low lung function. Ecotoxicol Environ Saf 147:1002–1009. https://doi.org/10.1016/j.ecoenv.2017.09.058
Ibeneme S, Egbosionu V, Ibeneme G et al (2016) Evidence of allergic reactions and cardiopulmonary impairments among traders operating from foodstuff warehouses. Biomed Res Int 2016:1–11. https://doi.org/10.1155/2016/1081258
Jacobs L, Emmerechts J, Hoylaerts MF et al (2011) Traffic air pollution and oxidized LDL. PLoS One 6:e16200. https://doi.org/10.1371/journal.pone.0016200
Ji J, Hedelin A, Malmlöf M et al (2017) Development of combining of human bronchial Mucosa models with XposeALI® for exposure of air pollution nanoparticles. PLoS One 12:e0170428. https://doi.org/10.1371/journal.pone.0170428
Kan H, Chen R, Tong S (2012) Ambient air pollution, climate change, and population health in China. Environ Int 42:10–19
Katsouyanni K, Touloumi G, Spix C, Schwartz J, Balducci F, Medina S, Rossi G, Wojtyniak B, Sunyer J, Bacharova L, Schouten JP, Ponka A, Anderson HR (1997) Short term effects of ambient sulphur dioxide and particulate matter on mortality in 12 European cities: results from time series data from the APHEA project. Air pollution and health: a European approach. BMJ 314(7095):1658–1663
Kaufman JD, Adar SD, Barr RG et al (2016) Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the multi-ethnic study of atherosclerosis and air pollution): a longitudinal cohort study. Lancet 388:696–704. https://doi.org/10.1016/S0140-6736(16)00378-0
Kelly FJ, Fussell JC (2015) Air pollution and public health: emerging hazards and improved understanding of risk. Environ Geochem Health 37:631–649. https://doi.org/10.1007/s10653-015-9720-1
Kelly FJ, Fussell JC (2017) Role of oxidative stress in cardiovascular disease outcomes following exposure to ambient air pollution. Free Radic Biol Med 110:345–367. https://doi.org/10.1016/j.freeradbiomed.2017.06.019
Kettunen J, Lanki T, Tiittanen P et al (2007) Associations of fine and ultrafine particulate air pollution with stroke mortality in an area of low air pollution levels. Stroke 38:918–922. https://doi.org/10.1161/01.STR.0000257999.49706.3b
Kim HH, Lee CS, Do YS et al (2016) Near-road exposure and impact of air pollution on allergic diseases in elementary school children: a cross-sectional study. Yonsei Med J 57:698. https://doi.org/10.3349/YMJ.2016.57.3.698
Kim H-J, Park SJ, Park CS et al (2018) Surface-modified polymer nanofiber membrane for high-efficiency microdust capturing. Chem Eng J 339:204–213. https://doi.org/10.1016/j.cej.2018.01.121
Kinney P (1999) The pulmonary effects of outdoor ozone and particle air pollution. Semin Respir Crit Care Med 20(06):601–607
Klimont Z, Smith SJ, Cofala J (2013) The last decade of global anthropogenic sulfur dioxide: 2000–2011 emissions. Environ Res Lett 8(1):014003
Koken PJM, Piver WT, Ye F, Elixhauser A, Olsen LM, Portier CJ (2003) Temperature, air pollution, and hospitalization for cardiovascular diseases among elderly people in Denver. Environ Health Perspect 111(10):1312–1317
Kumar P, Patton AP, Durant JL, Frey HC (2018) A review of factors impacting exposure to PM2.5, ultrafine particles and black carbon in Asian transport microenvironments. Atmos Environ 187:301–316. https://doi.org/10.1016/J.ATMOSENV.2018.05.046
Künzli N, Medina S, Kaiser R et al (2001) Assessment of deaths attributable to air pollution: should we use risk estimates based on time series or on cohort studies? Am J Epidemiol 153:1050–1055
Künzli N, Jerrett M, Mack WJ et al (2005) Ambient air pollution and atherosclerosis in Los Angeles. Environ Health Perspect 113:201–206. https://doi.org/10.1289/ehp.7523
Latza U, Gerdes S, Baur X (2009) Effects of nitrogen dioxide on human health: systematic review of experimental and epidemiological studies conducted between 2002 and 2006. Int J Hyg Environ Health 212:271–287. https://doi.org/10.1016/j.ijheh.2008.06.003
Li F, Liu Y, Lü J et al (2015) Ambient air pollution in China poses a multifaceted health threat to outdoor physical activity. J Epidemiol Community Health 69:201–204. https://doi.org/10.1136/jech-2014-203892
Li Z, Che W, Frey HC et al (2017) Characterization of PM2.5 exposure concentration in transport microenvironments using portable monitors. Environ Pollut 228:433–442. https://doi.org/10.1016/J.ENVPOL.2017.05.039
Liu W, Xu Y, Liu W et al (2018) Oxidative potential of ambient PM 2.5 in the coastal cities of the Bohai Sea, northern China: Seasonal variation and source apportionment. Environ Pollut 236:514–528. https://doi.org/10.1016/j.envpol.2018.01.116
Louwies T, Int Panis L, Provost E et al (2018) DNA hypomethylation in association with internal and external markers of traffic exposure in a panel of healthy adults. Air Qual Atmos Heal 11:673–681. https://doi.org/10.1007/s11869-018-0574-4
Luo M, Hou X, Gu Y et al (2018) Trans-boundary air pollution in a city under various atmospheric conditions. Sci Total Environ 618:132–141. https://doi.org/10.1016/j.scitotenv.2017.11.001
Luyts K, Van Den Broucke S, Hemmeryckx B et al (2018) Nanoparticles in the lungs of old mice: pulmonary inflammation and oxidative stress without procoagulant effects. Sci Total Environ 644:907–915. https://doi.org/10.1016/j.scitotenv.2018.06.301
Machado MN, Schmidt AC, Saldiva PHN et al (2014) Pulmonary functional and morphological damage after exposure to tripoli dust. Respir Physiol Neurobiol 196:17–24. https://doi.org/10.1016/j.resp.2014.02.007
Mahowald N, Albani S, Kok JF et al (2014) The size distribution of desert dust aerosols and its impact on the Earth system. Aeolian Res 15:53–71. https://doi.org/10.1016/J.AEOLIA.2013.09.002
Manigrasso M, Vitali M, Protano C, Avino P (2017) Temporal evolution of ultrafine particles and of alveolar deposited surface area from main indoor combustion and non-combustion sources in a model room. Sci Total Environ 598:1015–1026. https://doi.org/10.1016/j.scitotenv.2017.02.048
McCarthy MC, O’Brien TE, Charrier JG, Hafner HR (2009) Characterization of the chronic risk and hazard of hazardous air pollutants in the United States using ambient monitoring data. Environ Health Perspect 117:790–796. https://doi.org/10.1289/ehp.11861
Møller P, Danielsen PH, Karottki DG et al (2014) Oxidative stress and inflammation generated DNA damage by exposure to air pollution particles. Mutat Res Rev Mutat Res 762:133–166. https://doi.org/10.1016/j.mrrev.2014.09.001
Nemmar A, Hoet PHM, Vanquickenborne B et al (2002) Passage of inhaled particles into the blood circulation in humans. Circulation 105:411–414
Newby DE, Mannucci PM, Tell GS, Baccarelli AA, Brook RD, Donaldson K, Forastiere F, Franchini M, Franco OH, Graham I, Hoek G, Hoffmann B, Hoylaerts MF, Künzli N, Mills N, Pekkanen J, Peters A, Piepoli MF, Rajagopalan S, Storey RF (2015) Expert position paper on air pollution and cardiovascular disease. Eur Heart J 36(2):83–93
Nuvolone D, Petri D, Voller F (2018) The effects of ozone on human health. Environ Sci Pollut Res 25:8074–8088. https://doi.org/10.1007/s11356-017-9239-3
O’Neill MS, Veves A, Zanobetti A et al (2005) Diabetes enhances vulnerability to particulate air pollution-associated impairment in vascular reactivity and endothelial function. Circulation 111:2913–2920. https://doi.org/10.1161/CIRCULATIONAHA.104.517110
Olatunji AS, Kolawole TO, Oloruntola M, Günter C (2018) Evaluation of pollution of soils and particulate matter around metal recycling factories in Southwestern Nigeria. J Heal Pollut 8:20–30. https://doi.org/10.5696/2156-9614-8.17.20
Olopade CO, Frank E, Bartlett E et al (2017) Effect of a clean stove intervention on inflammatory biomarkers in pregnant women in Ibadan, Nigeria: a randomized controlled study. Environ Int 98:181–190. https://doi.org/10.1016/j.envint.2016.11.004
Omidi Y, Goudarzi G, Heidari AM, Daryanoosh SM (2016) Health impact assessment of short-term exposure to NO2 in Kermanshah, Iran using AirQ model. Environ Health Eng Manag 3(2):91–97
Patton AP, Perkins J, Zamore W et al (2014) Spatial and temporal differences in traffic-related air pollution in three urban neighborhoods near an interstate highway. Atmos Environ (1994) 99:309–321. https://doi.org/10.1016/j.atmosenv.2014.09.072
Penney D, Benignus V, Kephalopoulos S, Kotzias D, Kleinman M, Verrier A (2010) Carbon monoxide WHO guidelines for indoor air quality: selected pollutants
Peters A, Döring A, Wichmann H-E, Koenig W (1997) Increased plasma viscosity during an air pollution episode: a link to mortality? Lancet 349:1582–1587. https://doi.org/10.1016/S0140-6736(97)01211-7
Piantadosi CA (1999) Diagnosis and treatment of carbon monoxide poisoning. Respir Care Clin N Am 5:183–202
Pikhart H, Bobak M, Gorynski P, Wojtyniak B, Danova J, Celko MA, Kriz B, Briggs D, Elliott P (2001) Outdoor sulphur dioxide and respiratory symptoms in Czech and Polish school children: a small-area study (SAVIAH). Int Arch Occup Environ Health 74(8):574–578
Pissuwan D, Somkid K, Kongseng S et al (2016) Respiratory tract toxicity of titanium dioxide nanoparticles and multi-walled carbon nanotubes on mice after intranasal exposure. Micro Nano Lett 11:183–187. https://doi.org/10.1049/mnl.2015.0523
Pope CA, Dockery DW (2006) Health effects of fine particulate air pollution: lines that connect. J Air Waste Manage Assoc 56:709–742. https://doi.org/10.1080/10473289.2006.10464485
Pope CA III, Burnett RT, Thun MJ et al (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287:1132. https://doi.org/10.1001/jama.287.9.1132
Pope CAI, Dockery DW, Kanner RE et al (1999) Oxygen saturation, pulse rate, and particulate air pollution. Am J Respir Crit Care Med 159:365–372. https://doi.org/10.1164/ajrccm.159.2.9702103
Pope CA, Burnett RT, Thurston GD et al (2004a) Cardiovascular mortality and long-term exposure to particulate air pollution. Circulation 109:71–77. https://doi.org/10.1161/01.CIR.0000108927.80044.7F
Pope CA, Hansen ML, Long RW et al (2004b) Ambient particulate air pollution, heart rate variability, and blood markers of inflammation in a panel of elderly subjects. Environ Health Perspect 112:339–345. https://doi.org/10.1289/ehp.6588
Prospero JM (1999) Long-range transport of mineral dust in the global atmosphere: impact of African dust on the environment of the southeastern United States. Proc Natl Acad Sci USA 96:3396–3403. https://doi.org/10.1073/PNAS.96.7.3396
Przyklenk K, Kloner RA (1989) ‘Reperfusion injury’ by oxygen-derived free radicals? Effect of superoxide dismutase plus catalase, given at the time of reperfusion, on myocardial infarct size, contractile function, coronary microvasculature, and regional myocardial blood flow. Circ Res 64:86–96
Qin G, Wu M, Wang J, Xu Z, Xia J, Sang N (2016) Sulfur dioxide contributes to the cardiac and mitochondrial dysfunction in rats. Toxicol Sci 151(2):334–346
Rahman MM, Mazaheri M, Clifford S, Morawska L (2017) Estimate of main local sources to ambient ultrafine particle number concentrations in an urban area. Atmos Res 194:178–189. https://doi.org/10.1016/j.atmosres.2017.04.036
Rall DP (1974) Review of the health effects of sulfur oxides. Environ Health Perspect 8:97–121. https://doi.org/10.1289/ehp.74897
Raub J (1999) Carbon Monoxide, 2nd edn. World Health Organization, Geneva
Samoli E, Aga E, Touloumi G et al (2006) Short-term effects of nitrogen dioxide on mortality: an analysis within the APHEA project. Eur Respir J 27:1129–1138. https://doi.org/10.1183/09031936.06.00143905
Samoli E, Touloumi G, Schwartz J et al (2007) Short-term effects of carbon monoxide on mortality: an analysis within the APHEA project. Environ Health Perspect 115:1578–1583. https://doi.org/10.1289/ehp.10375
Schwartz J (2001) Is there harvesting in the association of airborne particles with daily deaths and hospital admissions? Epidemiology 12:55–61
Setiawan B, Kania N, Nugrahenny D et al (2014) Subchronic inhalation of particulate matter 10 coal dust induces atherosclerosis in the aorta of diabetic and nondiabetic rats. Biomarkers Genomic Med 6:67–73. https://doi.org/10.1016/j.bgm.2014.03.002
Seymour V (2016) The human-nature relationship and its impact on health: a critical review. Front Public Health 4:260. https://doi.org/10.3389/fpubh.2016.00260
Shi S, Zhu S, Lee ES et al (2016) Performance of wearable ionization air cleaners: Ozone emission and particle removal. Aerosol Sci Technol 50:211–221. https://doi.org/10.1080/02786826.2016.1139045
Silbajoris R, Osornio-Vargas AR, Simmons SO et al (2011) Ambient particulate matter induces interleukin-8 expression through an alternative NF-κB (nuclear factor-kappa B) mechanism in human airway epithelial cells. Environ Health Perspect 119:1379–1383. https://doi.org/10.1289/ehp.1103594
Silva AH, Locatelli C, Filho UP et al (2017) Visceral fat increase and signals of inflammation in adipose tissue after administration of titanium dioxide nanoparticles in mice. Toxicol Ind Health 33:147–158. https://doi.org/10.1177/0748233715613224
Simonetti G, Conte E, Perrino C, Canepari S (2018) Oxidative potential of size-segregated PM in an urban and an industrial area of Italy. Atmos Environ 187:292–300. https://doi.org/10.1016/j.atmosenv.2018.05.051
Smith KR (2002) Indoor air pollution in developing countries: recommendations for research. Indoor Air 12:198–207. https://doi.org/10.1034/j.1600-0668.2002.01137.x
Stafoggia M, Cesaroni G, Peters A et al (2014) Long-term exposure to ambient air pollution and incidence of cerebrovascular events: results from 11 European cohorts within the ESCAPE project. Environ Health Perspect 122:919–925. https://doi.org/10.1289/ehp.1307301
Suwa T, Hogg JC, Quinlan KB et al (2002) Particulate air pollution induces progression of atherosclerosis. J Am Coll Cardiol 39:935–942
Taillé C, El-Benna J, Lanone S, Boczkowski J, Motterlini R (2005) Mitochondrial respiratory chain and NAD(P)H oxidase are targets for the antiproliferative effect of carbon monoxide in human airway smooth muscle. J Biol Chem 280(27):25350–25360
Tham A, Lullo D, Dalton S et al (2017) Modeling vascular inflammation and atherogenicity after inhalation of ambient levels of ozone: exploratory lessons from transcriptomics. Inhal Toxicol 29:96–105. https://doi.org/10.1080/08958378.2017.1310333
Tunnicliffe WS, Hilton MF, Harrison RM, Ayres JG (2001) The effect of sulphur dioxide exposure on indices of heart rate variability in normal and asthmatic adults. Eur Respir J 17(4):604–608
Urch B, Silverman F, Corey P et al (2005) Acute blood pressure responses in healthy adults during controlled air pollution exposures. Environ Health Perspect 113:1052–1055. https://doi.org/10.1289/ehp.7785
Voidazan S, Moldovan H, Huţanu A et al (2018) Could fibrinogen and hsCRP be useful for assessing personal risk in workers exposed to a mixture of ultrafine particles and organic solvents? Rev Rom Med Lab 26:177–187. https://doi.org/10.2478/rrlm-2018-0011
Von Burg R (1999) Toxicology update. J Appl Toxicol 19(5):379–386
Vora R, Zareba W, Utell MJ et al (2014) Inhalation of ultrafine carbon particles alters heart rate and heart rate variability in people with type 2 diabetes. Part Fibre Toxicol 11:31. https://doi.org/10.1186/s12989-014-0031-y
Vreeland H, Weber R, Bergin M et al (2017) Oxidative potential of PM 2.5 during Atlanta rush hour: measurements of in-vehicle dithiothreitol (DTT) activity. Atmos Environ 165:169–178. https://doi.org/10.1016/j.atmosenv.2017.06.044
Weuve J, Kaufman JD, Szpiro AA et al (2016) Exposure to traffic-related air pollution in relation to progression in physical disability among older adults. Environ Health Perspect 124:1000–1008. https://doi.org/10.1289/ehp.1510089
WHO (2002) The World Health Report 2002: reducing risks, promoting healthy life. World Health Organization, Geneva
WHO (2012) Burden of disease from the joint effects of household and ambient air pollution for 2012. World Heal Organ
WHO (2016) Burden of disease from ambient air pollution for 2016
World Bank (2004) Reducing air pollution from urban transport
Wold LE, Simkhovich BZ, Kleinman MT et al (2006) In vivo and in vitro models to test the hypothesis of particle-induced effects on cardiac function and arrhythmias. Cardiovasc Toxicol 6:69–78
Wold LE, Ying Z, Hutchinson KR et al (2012) Cardiovascular remodeling in response to long-term exposure to fine particulate matter air pollution. Circ Heart Fail 5:452–461. https://doi.org/10.1161/CIRCHEARTFAILURE.112.966580
Yang B, Deng Q, Zhang W et al (2016) Exposure to polycyclic aromatic hydrocarbons, plasma cytokines and heart rate variability. Sci Rep 6:19272. https://doi.org/10.1038/srep19272
Yang L, Hou X-Y, Wei Y et al (2017) Biomarkers of the health outcomes associated with ambient particulate matter exposure. Sci Total Environ 579:1446–1459. https://doi.org/10.1016/j.scitotenv.2016.11.146
Yang B-Y, Guo Y, Morawska L et al (2019) Ambient PM1 air pollution and cardiovascular disease prevalence: insights from the 33 communities Chinese health study. Environ Int 123:310–317. https://doi.org/10.1016/J.ENVINT.2018.12.012
Yin Z, Xu H-J, Yao X-L et al (2017) Ambient fine particles (PM 2.5) attenuate collagen-induced platelet activation through interference of the PLCγ2/Akt/GSK3β signaling pathway. Environ Toxicol 32:530–540. https://doi.org/10.1002/tox.22257
Ying Z, Xu X, Bai Y et al (2014) Long-term exposure to concentrated ambient PM 2.5 increases mouse blood pressure through abnormal activation of the sympathetic nervous system: a role for hypothalamic inflammation. Environ Health Perspect 122:79–86. https://doi.org/10.1289/ehp.1307151
You S, Neoh KG, Tong YW et al (2017a) Variation of household electricity consumption and potential impact of outdoor PM2.5 concentration: a comparison between Singapore and Shanghai. Appl Energy 188:475–484. https://doi.org/10.1016/j.apenergy.2016.12.019
You S, Yao Z, Dai Y, Wang C-H (2017b) A comparison of PM exposure related to emission hotspots in a hot and humid urban environment: concentrations, compositions, respiratory deposition, and potential health risks. Sci Total Environ 599–600:464–473. https://doi.org/10.1016/j.scitotenv.2017.04.217
Zanobetti A, Canner MJ, Stone PH et al (2004) Ambient pollution and blood pressure in cardiac rehabilitation patients. Circulation 110:2184–2189. https://doi.org/10.1161/01.CIR.0000143831.33243.D8
Zhang Y, Li M, Bravo MA et al (2014) Air quality in Lanzhou, a Major Industrial City in China: characteristics of air pollution and review of existing evidence from air pollution and health studies. Water Air Soil Pollut 225:2187. https://doi.org/10.1007/s11270-014-2187-3
Zhang T, Gao B, Zhou Z, Chang Y (2016) The movement and deposition of PM2.5 in the upper respiratory tract for the patients with heart failure: an elementary CFD study. Biomed Eng Online 15:138. https://doi.org/10.1186/s12938-016-0281-z
Zhao Y, Wang S, Duan L, Lei Y, Cao P, Hao J (2008) Primary air pollutant emissions of coal-fired power plants in China: current status and future prediction. Atmos Environ 42(36):8442–8452
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Prasad, R.R., Paudel, S. (2020). Impacts of Air Pollution on Epidemiology and Cardiovascular Systems. In: Saxena, P., Srivastava, A. (eds) Air Pollution and Environmental Health. Environmental Chemistry for a Sustainable World, vol 20. Springer, Singapore. https://doi.org/10.1007/978-981-15-3481-2_8
Download citation
DOI: https://doi.org/10.1007/978-981-15-3481-2_8
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-3480-5
Online ISBN: 978-981-15-3481-2
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)