
Abstract
Bangladesh is a low-income country where 49% of its citizens live below the poverty line and earn less than US$1 a day. They also receive inadequate healthcare, education and social security services, suffer from low employment and are highly exposed to natural disasters (World Bank 2015). From an estimate population of 170 million, 17 million (10%) people are living with a disability, and makeup one of the most vulnerable groups in the country (CDD, 2015). There is a lack of public policy and private initiatives to address the disability issue due to the negative stigma associated with disability. Hence, there is insufficient resources and a lack of knowledge of disabilities and understanding the basic needs of the disabled. Social work is the scientific discipline of helping to address these problems and bring about the desired changes at the individual, family, society, organisational and international levels. Since its inception, social work is working with poor, sick, children, homeless, disabled, the elderly and marginalised in society. This chapter discusses relevant intervention strategies and approaches for rehabilitating disabled people within the framework of social work. Social workers can empower the disabled by streamlining resource redistribution to empower them and enhance their living standard.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
Introduction
Bangladesh is a low-income country located in South Asia. Form the country’s 170 million population, a reported 45% are living below the poverty line and earn under USD 1 a day (World Bank 2015). The country is facing severe poverty, where people have minimal access to education and medical care. Furthermore, Bangladesh is facing an unemployment crisis, lack of social security systems and is highly exposed to natural disasters (World Bank 2015). In the meantime, persons living with some form of disability account for about 20% of the world’s population (WHO and World Bank 2015). “Persons with Disability” (PWD) in Bangladesh comprises people living with physical disabilities, visual impairment, hearing impairment, speech impairment, mental disability (cognitive disability or mental retardation) and mental illness, characterised by either part or full injury or loss of intellectual poise. The Disability Welfare Act states that PWD comprises of persons with multiple disabilities, whether the reason for the infirmity is inherited or a result of abuse, illness, accident or additional causes. The Act also classifies that disabled persons have a disability and are incapable of leading a normal life either partly or wholly due to the infirmity or psychological deficiency (Disability Welfare Act 2001).
An estimated 10% of Bangladesh’s population, or approximately 17 million people, are living with disability (CDD 2015). Out of this number, a majority (41.5%) have physical disabilities, 19.6% have speech and hearing, 19.7% have visual disabilities, 7% have cerebral palsy, 7.4% have intellectual disabilities, 4.4% have multiple disabilities and 2.4% have a mental illness (World Bank 2015). Meanwhile, 70% of the PWD are illiterate, 68.9% of PWD have no access to medical assistance or rehabilitation due to economic hardship and 96.7% of PWD do not receive help from any organisation (Mostafa 2013).
PWD in Bangladesh are regularly ignored, deprived of basic needs, excluded from most public development policy initiatives and have difficulties accessing education, housing, medical care and basic living facilities (Park et al. 2002; Bowe 2006; Parish and Cloud 2006).
Global political instability, in recent years, has threatened peace and security, weakened economic recovery, delayed economic growth and poverty eradication. It has resulted in a lack of political will, poor governance, poor human rights, and lack of priority towards other social issues among women and children in difficult circumstances, people with AIDS, the elderly and drug users. These issues have contributed to the marginalisation of PWD. In this light, public development agencies and service providers have frequently ignored PWD. There are also cases where “special” programmes were implemented to effectively exclude PWD from mainstream society (Yeo and Moore 2003).
Social work is the scientific discipline that focuses on addressing problems and bringing about the desired changes at the individual, family, society, organisational and international levels (Ali and Hatta 2014). Since its inception, social work in infirmity services has transformed several of its important functions. Standard social services are focused on providing psychotherapy, information and referral, resource acquirement and case support (Beaulaurier and Taylor 2001). However, some PWD question the efficacy of social work based on their expectations of the role of social workers. These attitudes emerged in the 1970s–1980s where changes in numerous social work aspects were conducted in large measures to support the efforts to protect the civil rights of PWD (Beaulaurier and Taylor 2001). Other initiatives were campaigned to increase facilities for PWD so that they are capable of living in the society without institutional help and of creating positive attitudes and acknowledgement of their rights. The scope of disabilities creates an exclusive opportunity for social workers to collaborate with others to develop understanding and share expertise (CASW 2015). The PWD is known to experience higher living risk, thus increasing the need for advocacy, services and supports that can be provided by a social worker (Chaplin 2004). Social workers can undertake significant roles in resource relocation to assist and enable the disabled to be more autonomous and to create earnings opportunity in Bangladesh.
The Scenario of People with Disabilities in Bangladesh
The rights of PWD is one of the least understood issues in the area of development in Bangladesh. Issues concerning PWD have not been addressed widely in mainstream human rights, women’s rights, child rights, religious minorities’ rights or indigenous peoples’ rights organisations (Ackerman et al. 2005). It is also historically evident that disability rights are one of the most neglected and forgotten development areas by the governments and NGOs. The government and other development agencies have not realised that a close relationship exists between disability and development and believed that disability is a welfare issue. PWD are considered recipients of charity and welfare in Bangladesh. Most parents with disabled children in Bangladesh are not ready to address the issue faced by their disabled children in front of the public due to negative perceptions of having a disabled child as a curse and sentence from the Creator (God) (Ackerman et al. 2005).
The PWD in rural Bangladesh are perceived negatively and experience wide-spread misconception and mistreatment making their lives miserable. The dependence and inability contribute to few facilities open to PWD and decrease their role in their family, society and nation (Morales and Sheafor 2004). The mistreatment of PWD is a culturally embedded and socially accepted form of oppression against PWD (Ackerman et al. 2005; Chiterika 2010). Moreover, the lack of experience in addressing the needs of this cohort may result in negative attitudes towards PWD from healthcare professionals who may struggle with communicating at appropriate developmental levels in Bangladesh (Ward et al. 2010). The PWD seems to be sidelined from mainstream national policies due to the public’s negative impression of them, inadequate knowledge of policymakers and planners, shortage of resources, insufficient knowledge and skills to address the needs of PWD in Bangladesh (Alam et al. 2005).
Bangladesh has ratified the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) and has a Disability Welfare Act-2001. The Government of Bangladesh (GB) and its concerned ministries, directorates, national and international agencies are aware of the situation of PWD. These agencies are working together for the development of PWD in the country. While the Ministry of Social Welfare (MSW) has provided a special allocation for PWD in its yearly budget, the allocation is undoubtedly inadequate to address the immediate needs of millions of PWD in the country (DRRA 2012). Nonetheless, all of these efforts could cover only 20% of the total disability in Bangladesh (DRRA 2012). The programme covered a few PWD in the country, but a major part of the PWD population cannot access these services in Bangladesh. Despite the Welfare Act 2001, no other laws allow PWD to claim and establish their rights in society (DRRA 2012).
The government provides monthly financial support to registered PWD. However, the cash grant amount is only sufficient to cover the expenses for a week, making them dependent on their families and other cash handouts from charities. Limited resources have restrained agencies from initiating and expanding rehabilitation and other services for PWD. Only a handful of PWD are involved in mainstream employment activities due to the lack of necessary expertise (Alam et al. 2005). Many international organisations are involved in disability rehabilitation in Bangladesh. Nevertheless, PWD is hardly engaged in the formulation of policy for these institutions, which makes it very hard to form actual policies for full inclusion of PWD (Yeo and Moore 2003).
There is also a lack of understanding and skills among development institutions to involve PWD with their policy and planning. Moreover, training organisations have inadequate capacity to train rehabilitation workers in Bangladesh, as well as inadequate professional facilities for sign language, braille and speech therapy that restrict the inclusion of PWD. The majority of the organisations are unwilling to employ PWD due to inexperience and lack of knowledge and expertise on the needs of PWD, negative perceptions, and the lack of intention to adopt a PWD-friendly working atmosphere in Bangladesh. Moreover, the PWD in most communities around the world are given little opportunity to become involved as a development partner due to the common perception that they are incapable of performing duties (Mostafa 2013).
There is still a general lack of acceptance of PWD in Bangladesh. The PWD is still frequently pitied, socially shunned, humiliated and discriminated against (Zastrow 2004). This vulnerable condition makes it more challenging and occasionally difficult for them to claim their political, social and financial rights. The voices of the disabled are not heard in Bangladesh. They are a disadvantaged group in society and live in poverty. In this regard, along with ethnic minorities, the elderly and women, they are facing constant discrimination (Brantlinger 2001; Das and Addlakha 2001; Larkin et al. 2003). Studies have argued that depriving policies, legislations, programmes and cultural rights contribute to a situation that denies people control over their lives (Chiterika 2010).
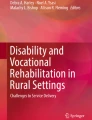
The MSW, Department of Social Services (DSW) and Foundation for the Development of PWD are working with other ministries and agencies to support the implementation of the laws and provisions. Hundreds of non-government agencies are working to address disability issues and encourage their inclusion in mainstream development. There is an apparent goal among the stakeholders working with PWD. However, many initiatives benefited only a small number of PWD in remote and urban areas, and there is a lack of cooperation between agencies (Mostafa 2013). In this light, PWD are vulnerable due to the lack of self-organisation, limited knowledge of their basic rights, low confidence, lack of respect from the society, lack of education facilities, limited social contact, weak leadership and limited advocacy in Bangladesh (Chiterika 2010) (Fig. 20.1).

The vicious circle of poverty and disability. (Source: Yeo and Moore 2003)
Legislation and Institutional Frameworks on Disability Issues in Bangladesh
In the 1970s, therights of PWD were recognised as the main agenda of the United Nations (UN) Agreement on the Civil Rights of the Mentally Retarded in 1975 (IFSW 2012). The government of Bangladesh accepted the rights of the PWD in 1993, with the establishment of the National Coordination Committee on Disability under the Social Welfare Ministry. The Constitution of Bangladesh specifically emphasised the equality, human dignity and social justice for the people of Bangladesh as stated in Articles 10, 11, 15, 17, 19, 20, 21, 27, 28, 29, 31, 32, 36. In this regard, the government of Bangladesh has guaranteed the rights and self-esteem of all citizens of Bangladesh, equally and without any prejudice (DRRA 2012).
The GB has passed several Acts for PWD to improve their living standards, including the Disability Welfare Acts 2001 and 2012. The Disability Welfare Act 2001 is based on a medical, welfare and charity-based approach (Mostafa 2013). During the last decade, government agencies have also introduced legislation against disability discrimination (Ackerman et al. 2005). However, the implementations and effects of such legislations have been limited (Yeo and Moore 2003). While the national constitution prohibits any form of discrimination in the employment for the disabled, the full inclusion of PWD in employment or income generation activities in Bangladesh has yet to materialise (DRRA 2012). It ignores the development and rights components of development cooperation and regards the affair as a “welfare” issue (DRRA 2012). The Disability Welfare Act 2012 has failed to meet the goals due to the prime fact that this was anti-UNCRPD legislation. Hence, it failed to uphold the universal standards applicable in this field (Mizan and Sarwar 2012). In this light, the act is grounded on the Disability Welfare Act 2001action towards the universal modification of the education of disabled children. However, no financial costs were included in this plan.
The discussion above shows that the present policies and laws in Bangladesh concerning the rights of PWD do not effectively defend the rights to equality and non-discrimination. The majority of the programmes, legislations, practices and policies aim to address PWD are not suitable for community, are functionally inadequate and ineffective for the welfare of PWD in Bangladesh (Mostafa 2013). More comprehensive legislation is required in Bangladesh to guarantee the rights of PWD in all phases—civil, financial, social, cultural and political.
Organisations for Working with PWD in Bangladesh
The Ministry of Social Welfare (MSW), Department of Social Welfare (DSW) and National Foundation for Development of the Disabled Persons are the agencies responsible for fulfilling the needs of PWD in Bangladesh. Besides government agencies, many NGOs are working for PWD in Bangladesh. These NGOs include Action on Disability and Development (ADD) and Bangladesh Disability Welfare Association, Centre for Services and Information on Disability (CSID), Centre for the Rehabilitation of the Paralysed (CRP), Young Power in Social Action (YPSA), The National Federation of the Blind and National Federation of the Deaf Disabled Rehabilitationand Research Association (DRRA). Moreover, some international NGOs such as Christian Blind Mission (CBM), Sightsavers, Helen Keller International, Oxfam, Action Aid, ORBIS, Lillian Fonds, Handicap International and Leonard Cheshire Disability—International, Rotary International, Niktan, Eblis Foundation, The Canadian International Development Agency (CIDA) and other agencies are among the frontline NGOs that support the development of persons with disabilities in the country. Addressing disability issues is important in all facets of development: equality, empowerment, human rights, poverty and marginalisation (Lee 1999). There are several limitations in relying on NGOs to meet the needs of PWD. This includes low financial assistance, disorganised service delivery, too flexible and unregulated (Harriss-White 1999; Yeo and Moore 2003). Moreover, many mainstream development NGOs continue to claim that they are not “specialists” and therefore, do not want to consider disability issues (Yeo and Moore 2003). It is clear that most mainstream development NGOs do not fully include disabled people in their work in Bangladesh.
Social Work and Disability
In caringfor people with disabilities, social workers are generally responsible for working together with persons, groups and families who have several, difficult and co-existing personal and societal complications.
The main goal of social work is to enable PWD and their families to identify their needs, anxieties and aspirations, provide solutions and help them take control of their lives, avoid and cope with grief and catastrophe and ensure public involvement (Wilkinson 2015). Social work has existed as a discipline for over 100 years (Weaver 2006). During the Second World War, social casework has provided healthcare rehabilitation and social workers carried on more frequent interaction with PWD. In the golden age of social work in the 1970s and early the 1980s, the principal form of social work exercise has focused on personal casework with PWD (Langan 1992; Leece and Leece 2011). Besides that, the social casework methods were previously used for preparing individuals, family and society with a new disability outside of the hospital setting (Beaulaurier and Taylor 2001). The health rehabilitation task largely used a collective method that solely depends on the assistance of social workers (Berkowitz 1980).
The National Association of Social Workers (NASW) mentioned that social workers provide education, employment and skills development training, healthcare, affordable housing and mental support for PWD (NASW 2006a; Bean and Krcek 2012). Social workers help displaced, vulnerable people, elderly, children and PWD (Weaver 2006; NASW 2006b). In this light, the social workers as specialists could strengthen a person’s skills in adjusting to the environment, to rebuild a person’s relations with the community, while helping them to integrate into society, and promoting social functioning (Laima et al. 2003). Social workers have a responsibility to prepare future practitioners with the skills necessary to meet the needs of PWD (Robinson et al. 2012).
Social workers are responsible for meeting the needs of this population and can be integral to providing solutions (Robinson et al. 2012). Social workers are in an ideal position to work with PWD because they are highly trained to address the needs of people with disability (Hanley and Parkinson 1994; Bean and Krcek 2012). Furthermore, social workers value rights, dignity, individual uniqueness, self-determination and clients’ access to resources (NASW 2006a). At the micro and macro levels, social workers are focused primarily on the social well-being of individual clients and their families, equally valued with the importance of their physical, mental and spiritual well-being. At the macro level, they establish a better capability to look beyond the ill health and medical care, to treat them as human beings and to take care of the political and social concerns of PWD (CASW 2015). Social workers assisting PWD at individual levels, assist families who have family members or children with infirmity, as well as with societies in local and international levels. The PWD and their families are served by social work providers in traditional service delivery systems and in social service agencies (Parish and Lutwick 2005). These scopes include research, advocacy and counselling, policy practices, casework, community development and direct exercise. Social workers play important roles in the field of disability to develop policies, programmes and legislation to extend support to PWD in Bangladesh. Besides, social workers assisting PWD and families often encourage social inclusion, working opportunity, society living, rehabilitation and family care (IFSW 2012). Consequently, social workers help to improve the human function and efficacy of the social structure by offering wealth and facilities for PWD, clients and service recipients (DuBois and Miley 2005). Social work also addresses the issue of grief, loss and bereavement associated with a mental and physical disability.
The targeted outcomes of social work intervention include accepting and recognising PWD. Social workers are the change agents concentrating their involvements on the social connections between persons and community, as social work is about strategic change (Tan and Envall 2004). Social work is a scientific profession that helps clients to change them, their environment or accepts aspects of themselves (Adams et al. 2002; Leece and Leece 2011). Social workers can build on their connection with users and develop roles through advocacy, group work and counselling with PWD (Kirkpatrick et al. 1998; Leece and Leece 2011). In working with PWD, social workers’ are required to make appropriate referrals, provide supportive counselling, offer advocacy and to engage in group work, service coordination, team building and direct services (Andrews and Wikler 1981).
Role of Social Workers for Rehabilitation in Bangladesh
Social workers play a vital role in disability services offered by NGOs and government agencies. This is because they have vast knowledge in identifying both personal and logical dimensions of support and motivation, play a significant role in evaluation, case management and planning across all kind of service delivery (Wilkinson 2015). The principal mission of social work is to enhance their full potential, improve their living standard and avoid malfunctions in the communities (Hossain and Mathbor 2014). The role of social workers include:
Advocacy Services
Disability doesnotjust affect individuals, but also the family and community surrounding them. Social workers play an important role in meeting the needs of PWD in Bangladesh, as they provide assessment, intervention and advocacy for people with PWD and their families. However, there is a serious shortage of social workers caring for PWD, as well as other disadvantaged groups, such as the elderly (Robinson et al. 2012). Social workers are involved in social planning, policy development, inspire and encourage community to engage in social action in order to influence social policy and financial improvement of PWD in Bangladesh (IFSW 2012; Hossain and Mathbor 2014). Social workers should also be involved with social justice to advocate for people who are facing various injustices in Bangladesh. Furthermore, they need to ensure that the engagement of service recipients and develop roles of advocacy, counselling and collective work in Bangladesh (Kirkpatrick et al. 1998).
Medical Social Work
The DSW operateshospital social service programmes in Bangladesh. Medical social workers in Bangladesh are responsible for supplying medicine, familiarising the patients with the hospital environment, provide healthy food and other healthcare provisions for the poor, rehabilitation of PWD and new patients. Medical and psychiatric social workers in hospitals in Bangladesh collaborate with doctors, nurses and other therapists in the diagnosis and treatment planning process of disabled people (Hossain and Mathbor 2014). As a member of in-patient or out-patient interdisciplinary team in the hospital, social workers are responsible for supporting the rehabilitation process so that PWD have the highest freedom and self-sufficiency in various areas of his or her functioning, (CASW 2015). Social workers encourage PWD to know their status and seek appropriate treatment from hospitals in Bangladesh. In these settings, medical social workers might visit the PWD and their families in their homes and are responsible for providing proper information, treatment or training, and provide adequate support for PWD, family and community members in Bangladesh (Chiterika 2010).
Counselling Services
Social workers providecounselling to PWD to support and encourage the inclusion of PWD in the community in Bangladesh. The counselling sessions could address individuals, family and interpersonal issues to empower the education of PWD and increase their economic opportunities. In rehabilitation settings, social workers may serve as a mediator between family and the agency to discuss issues pertaining to rehabilitation and other essential services and plans (Zastrow 2009). This procedure involves the family, clients and society. The social worker assists the clients and their family to cope with vulnerable situations, concerns and reliance to one of increased self-reliance and hope, through diagnosis and interventions in the areas of psychosocial functioning (CASW 2015). This can also be linked to the advocacy role whereby social workers can lobby the government to implement legislation specifically targeting PWD in Bangladesh properly. The social workers could effectively guide the government concerning the inclusion of disability in all legislation, policies and programmes in Bangladesh (Yeo and Moore 2003). In this regard, the Code of Ethics calls for social workers at the macro level to advocate for changes in policy and law to improve social settings to meet social needs and enhance social justice for PWD (NASW 2006a).
Financial and Equipment Support
Bangladesh is a low-income country where 49% of people live below the poverty line and earn less than US$1 a day. People are living with inadequate health, education and social security services, low employment and exposed to natural disasters (World Bank 2015). Poverty hinders parents from getting assistance and therapy that could ensure the proper growth and development of PWD. Moreover, poor parents are not in the position to purchase assistive devices for their disabled children. Social workers assist by providing their clients with various social service offices/agencies for welfare benefits, and assistive devices like wheelchairs, special seats, standing and walking devices and orthotics and prosthetics, as well as hearing aids, toys for activities of daily living, tricycles, tools and equipment for work, protective footwear, simple devices for braille reading. They also provide home services to increase accessibility.
Vocational Training and Empowerment
Currently, manystakeholders are working on behalf of disabled people. However, they have been working through exclusion, isolation and demeaning welfare programmes (Yeo and Moore 2003). In this light, providing charity becomes insufficient to address the issues of PWD and change the notion that PWD is inferior. Charity is not part of the development process, and PWD have not benefited from it. This is because the PWD desire to be treated equally, participate as equal citizens in their own communities with ordinary citizens with equal rights (Chiterika 2010; Suharto 2006). Thus, the empowerment perspective has encouraged social workers to develop collaborations with oppressed PWD and persons living in poverty (May 2005) as individuals with disabilities are becoming increasingly interested in gaining empowerment (Mackelprang and Salsgiver 1996; Beaulaurier and Taylor 2001).
Therefore, rehabilitation programmes need to empower the PWD to enhance their confidence and self-motivation by mutual discussion as a support group (Suharto 2006). The principal objectives of the rehabilitation programmes should aim to remove the barrier of disability while enhancing employment opportunities for self-reliance and freedom (Suharto 2006). PWD is one of the most disadvantaged and helpless groups in Bangladesh, as they have no or limited access to education, basic needs, employment opportunities, skills or vocational training. This has worsened their situation further. In this regard, social workers might provide training for PWD who lack the skills and qualification to venture into employment and provide employment opportunities for qualified PWD (IFSW 2012).
Professional Schools
Children andyouth with disabilities have limited access to education in Bangladesh. While providing educational opportunities for PWD is central to economic empowerment, however, access to education for PWD is very restricted due to the negative attitudes of community leaders, school authorities and village leaders who do not admit children with disabilities in Bangladesh. They do not include adequate hygiene (toilets), suitable infrastructure, educational materials, assistive devices like hearing and braille in Bangladeshi schools (Ackerman et al. 2005). School workers can directly assist individual children, groups or entire classrooms. Additionally, they might assist families to receive services that are required for them, consult with parents and teachers and others in the issue of children’s lives (NASW 2006b). In Bangladesh, the education of children with disabilities is dependent on NGOs due to minimal government programmes. Consequently, social workers may influence political, administrative and legislative changes through relevant proposals and submissions to government bodies for research, continuous professional development, education and training and promoting and facilitating the inclusion or integration of PWD within the broader community in Bangladesh.
At the same time, medical social workers might play a significant role in providing information on the available therapies, discuss treatment options with nurses and doctors, teaching health education and help create rapport with doctors and patients. The scope of social workers’ roles includes cooperating with other professionals, collaborating with community members, supporting PWD, developing healthcare model and resources, consulting for adequate services, changing policy to eradicate poverty, housing, employment and social justice and assisting the development of preventive programmes for PWD. Furthermore, social workers could facilitate the interference, support and increase access to services, information and individual and public teaching for PWD (CASW 2015). PWD are most likely to run their small businesses with profits to improve the living standard (Ackerman et al. 2005). Social workers play an increasingly prominent role in employee assistance programmes in addressing issues affecting PWD in the workplace in Bangladesh. The majority of PWD are mostly uneducated and receive no training. Hence, they are eventually unable to run their business with profits. In response, social workers could arrange need-based training on income generation activity (IGA) to enhance skills in the market promotion.
Lobbyists
Social workers could conduct collaborative, strengths-cantered activities to promote, support and advocate awareness of the rights and benefits of adaptive technology for PWD (DuBois and Miley 2005). There is a lack of self-organisation among PWD (Alam et al. 2005). Disabled people are socially excluded, as they often have little interaction with other disabled people in their home country and other parts of the world (Yeo and Moore 2003). Social workers can play the role as a lobbyist to strengthen self-help disability organisations particularly in the area of identifying and training of leaders, linking self-help groups with potential funding partners, training on operation and management of cooperatives, seminars on small business, development and management and training on advocacy and awareness-raising in Bangladesh. Disabled people are rarely involved in the policy-making at the national and international levels (Yeo and Moore 2003). Social workers can build collaboration and coordination as well as exchange information, knowledge, resource and services among the governmental and NGOs at both national and international levels in Bangladesh. The social workers could also help empower PWD through the formation of self-help groups and in rural areas and urban slums (Laima et al. 2003).
Increase Awareness
Illiteracy is a major problem in Bangladesh, and illiterate parents mostly live in poverty. Subsequently, they are not aware of the constitutional facilities and basic rights of their disabled children and the education options available to them. Children with disabilities are often hidden as victims due to humiliation and potential teasing and ridicule from others (Alam et al. 2005). The print and electronic media have also given minimal attention to PWD. Therefore, social workers could work collaboratively to fulfil the requirements of PWD and increase the level of public awareness regarding their fundamental rights, and to create new levels of coordination into social life in Bangladesh. Social workers in their organisations work on behalf of their clients, and this includes efforts to influence other professionals to improve the living standard of PWD. Social workers could also provide counselling campaign for the provision of service, and establish social or public policies that benefit PWD and their caregivers (Parish and Lutwick 2005; Heller et al. 2007; Robinson et al. 2012).
Provide Health Education
Medical social workersare responsible for delivering education, knowledge, family planning and counselling, immunisation, food nutrition, maternal illness and healthcare for children in Bangladesh. However, most PWD is living in poverty and in rural areas without access to welfare programmes and services in Bangladesh. Healthcare services are scarce for disadvantaged people in Bangladesh, including PWD. The lack of nutritious food, hazardous working and housing conditions, lack of access to vaccination, poor sanitation and hygiene, insufficient information, and risk of war, conflict and natural disaster are significant issues for PWD in Bangladesh. This has generated a negative impact on family care, and primary interference is an important instrument to help people with disability. Hence, social workers need to empower their parents and family members with the knowledge and skills to understand and fulfil the requirement of PWD in Bangladesh (Ackerman et al. 2005).
PWD continue to be isolated from mainstream society due to their physical inability and negative stigmas regarding their competence in Bangladesh. While there are no laws that restrict PWD from participating in the society, social works in Bangladesh are still hindered by physiological obstacles and deprivation which made it hard for the disabled to be accepted by the community in Bangladesh (Beaulaurier and Taylor 2001). Negatives attitudes, prejudice, and employers’ reluctance to hire and accommodate PWD have somewhat significantly impacted their employment opportunities (Schartz et al. 2006a; Schartz et al. 2006b; Samant et al. 2009).
Professional social workers act as trainers, consultants and programme designers to assist engagement, maintenance, accommodation and training workers with disabilities (Straussner 1990). As counsellors and mentors, social workers could assist organisations to gain a better understanding of disability matters for employment, legislation and accommodating PWD (Samant et al. 2009). Therefore, social workers could develop a relationship with international development agencies to encourage the participation of PWD in their programmes and services and spread awareness so that the future generation accepts PWD as equal members of the community in Bangladesh.
Conclusion
Undoubtedly, PWD is one of the most discriminated minority groups in the world and have received constant systematic violations of their human rights. These violations result in worsening living conditions, degrading human treatment, lack of access to housing, healthcare and employment, social exclusion and even death. PWD are seen as perpetually dependent and unproductive. Some families tend to neglect their developmental needs. With a common perception that nothing can be expected from PWD, families do not care to invest for the education, healthcare and other needs of their family members with disabilities in Bangladesh. Inadequate and ineffective execution of the current laws and policies in the lack of attentive monitoring system and apathy of GOs and NGOs in imposing them due to the lower priority assigned to programmes regarding disability. Generally excluded from social, economic and political institutions and interactions, disabled people lack the power to exert an influence on policymakers in Bangladesh.
Advocacy of PWD is crucial to generate awareness of disability issues. Providing equal rights and chances for the disabled to get involved in finance and politics, as well as creating more social connections will contribute to the increase of living standards in Bangladesh (Yeo and Moore 2003). There is a dearth of professional social workers with the capability to work with PWD to address issues related to people with physical, visual, hearing and intellectual disability. Social workers can be the catalyst for change, as they are responsible for training, education, advocacy, and identification of needs on individual, community and state. In this regard, they can create and sustain the necessary partnerships to reduce the disparities experienced by PWD (Robinson et al. 2012). However, there are still many mountains to climb before equity and social inclusion can be a reality for PWD. Multi-sectoral collaboration efforts are needed to ensure the full integration of PWD. With unprecedented global efforts to improve living standard, PWD should be fully incorporated as a major target for substantial improvement to PWD living standards to become a reality.
References
Ackerman, P., Thormann, M. S., & Huq, S. (2005). Assessment of Educational Needs of Disabled Children in Bangladesh. Washington, DC: United States Agency for International Development (USAID).
Adams, R., Dominelli, L., & Payne, M. (2002). Social Work: Themes, Issues and Critical Debates (2nd ed.). Basingstoke: Palgrave Macmillan.
Alam, K. J., Bari, N., & Khan, M. A. (2005). Community Based Rehabilitation Practices and Alleviation of Poverty of People with Disabilities in Bangladesh. Retrieved from http://www.worldenable.net/cbr2005/paperbangladesh.htm.
Ali, I., & Hatta, Z. A. (2014). Zakat as a Poverty Reduction Mechanism Among the Muslim Community: Case Study of Bangladesh, Malaysia, and Indonesia. Asian Social Work and Policy Review, 8(1), 59–70.
Andrews, S., & Wikler, L. (1981). Developmental Disabilities. Health and Social Work, 6(1), 62–68.
Bean, K. F., & Krcek, T. E. (2012). The Integration of Disability Content into Social Work Education: An Examination of Infused and Dedicated Models. Advances in Social Work, 13(3), 633–647.
Beaulaurier, R. L., & Taylor, S. H. (2001). Social Work Practice with People with Disabilities in the Era of Disability Rights. Social Work in Health Care, 32(4), 66–91.
Berkowitz, E. D. (1980). Rehabilitation: The Federal Government’s Response to Disability 1935–1954. New York: Arno Press.
Bowe, F. (2006). Disability in America. New York: Hofstra University.
Brantlinger, E. (2001). Poverty Class and Disability: A Historical, Social and Political Perspective. Focus on Exceptional Children, 33(7), 1–15.
Canadian Association of Social Work (CASW). (2015). The Role of Social Work in Mental Health. Retrieved November 1, 2015, from http://www.casw-acts.ca.
Centre of Disability in Development (CDD). (2015). Disability Situation in Bangladesh. Retrieved October 24, 2015, from http://www.cdd.org.bd.
Chaplin, R. (2004). General Psychiatric Services for Adults with Intellectual Disability and Mental Illness. Journal of Intellectual Disability Research, 48(1), 1–10.
Chiterika, C. (2010). People with Disabilities and the Role of Social Workers in Lesotho. International Journal of Social Work and Society, 8(1), 82–93.
Das, V., & Addlakha, R. (2001). Disability and Domestic Citizenship: Voice, Gender, and Making of the Subject. Public Culture, 13(3), 511–531.
Disability Welfare Act. (2001). Govt of Bangladesh.
Disabled Rehabilitation & Research Association (DRRA). (2012). Contextual Analysis of Socio-economic Situation of Persons with Disabilities in Bangladesh. Dhaka: Bangladesh.
DuBois, B., & Miley, K. (2005). Social Work: An Empowering Profession. Boston: Pearson.
Hanley, B., & Parkinson, C. B. (1994). Position Paper on Social Work Values: Practice with Individuals Who Have Developmental Disabilities. Mental Retardation, 32(6), 426–431.
Harriss-White, B. (1999). Onto a Loser: Disability in India. In B. Harriss-White & S. Subramanian (Eds.), Ill Fare in India: Essays on India’s Social Sector in Honor of S. Guhan (pp. 135–158). New Delhi: Sage Publications.
Heller, T., Caldwell, J., & Factor, A. (2007). Aging Family Caregivers: Policies and Practices. Mental Retardation and Developmental Disabilities Research Review, 13(2), 136–142.
Hossain, M. I., & Mathbor, G. M. (2014). Social Work Practice for Social Development in Bangladesh: Issues and Challenges. Asian Social Work and Policy Review, 8(2), 123–137.
International Federation of Social Work (IFSW). (2012). People with Disabilities. Retrieved from http://www.ifsw.org.
Kirkpatrick, I., Ackroyd, S., & Walker, R. (1998). The New Managerialism and Public Service Professions: Change in Health, Social Services and Housing. London: Palgrave Macmillan.
Laima, S., Ligija, S., & Jurate, G. (2003). The Role of Social Worker in Team of Rehabilitation: Methodological Approach. MEDICINA, 39(9), 889–833.
Langan, M. (1992). The Rise and Fall of Social Work. In J. Clark (Ed.), A Crisis in Care. London: Sage.
Larkin, V. M., Alston, R. J., Middleton, R. A., & Willson, K. B. (2003). Underrepresented Ethnically and Racially Diverse Ageing Populations with Disabilities: Trends and Recommendation. Journal of Rehabilitation, 69(2), 26–31.
Lee, H. (1999). Discussion Paper for Oxfam: Disability as a Development Issue and How to Integrate a Disability Perspective into the SCO. Oxford: Oxfam.
Leece, J., & Leece, D. (2011). Personalisation: Perceptions of the Role of Social Work in a World of Brokers and Budgets. British Journal of Social Work, 41(2), 204–223.
Mackelprang, R. W., & Salsgiver, R. O. (1996). People with Disabilities and Social Work: Historical and Contemporary Issues. Social Work, 41(1), 7–14.
May, G. E. (2005). Changing the Future of Disability: The Disability Discrimination Model. In G. E. May & M. B. Raske (Eds.), Ending Disability Discrimination: Strategies for Social Workers (pp. 82–98). Boston: Pearson Education, Allyn & Bacon.
Mizan, A. S., & Sarwar, M. G. (2012). In Pursuit of Deliverance: Critical Analysis of the Draft Rights of the Persons with Disabilities Act 2012. Retrieved from https://www.academia.edu/6615613/An_Overview_of_the_Rights_of_Persons_with_Disabilities_Act_2013.
Morales, A. T., & Sheafor, B. W. (2004). Social Work: A Profession of Many Faces. Boston, MA: Allyn & Bacon.
Mostafa, M. G. (2013). The Convention on the Rights of Persons with Disabilities: A Study on Bangladesh Compliance. National Human Rights Commission, Bangladesh (NHRCB). Dhaka: Bangladesh.
National Association of Social Workers (NASW). (2006a). How Do Social Workers Help the Families of Children with Disabilities. Retrieved from http://www.nasw.org.
National Association of Social Workers (NASW). (2006b). Assuring the Sufficiency of a Frontline Workforce: A National Study of Licensed Social Workers. Retrieved from http://www.workforce.socialworkers.org/studies/nasw_06_execsummary.pdf.
Parish, S. L., & Cloud, J. M. (2006). Financial Well-Being of Young Children with Disabilities and Their Families. Social Work, 51, 223–232.
Parish, S. L., & Lutwick, Z. (2005). A Critical Analysis of the Emerging Crisis in Long Term Care for People with Developmental Disabilities. Social Work, 50(4), 345–254.
Park, J., Turnbull, A. P., & Turnbull, H. R. (2002). Impacts of Poverty on Quality of Life in Families of Children with Disabilities. Exceptional Children, 68(2), 151–170.
Robinson, L. M., Dauenhauer, J., Bishop, K. M., & Baxter, J. (2012). Growing Health Disparities for Persons Who Are Aging with Intellectual and Developmental Disabilities: The Social Work Linchpin. Journal of Gerontological Social Work, 55(2), 175–190.
Samant, D., Soffer, M., Hernandez, B., Adya, M., Akinpelu, O., Levy, J. M., Repoli, E., Kramer, M., & Blanck, P. (2009). Corporate Culture and Employment of People with Disabilities: Role of Social Workers and Service Provider Organizations. Journal of Social Work in Disability & Rehabilitation, 8(3), 171–188.
Schartz, H., Hendricks, D. J., & Blanck, P. (2006a). Workplace Accommodations: Evidence-Based Outcomes. Work, 27, 345–354.
Schartz, H. A., Schartz, K. M., Hendricks, D. J., & Blanck, P. (2006b). Workplace Accommodations: Empirical Study of Current Employees. Mississippi Law Journal, 75, 917.
Straussner, S. L. A. (1990). Occupational Social Work Today. New York: Haworth.
Suharto, E. (2006). Role of Social Workers in Indonesia: Issues and Challenges in Rehabilitation People with Disabilities. Retrieved July 16, 2019, from http://www.policy.hu/suharto/Naskah%20PDF/CibinongDifableSocialWork.pdf.
Tan, N. T., & Envall, E. (2004). Social Work; Challenges in the New Millennium. In N. T. Tan & E. Envall (Eds.), Social Work Around the World. Bern, Switzerland: IFSW.
Ward, R. L., Nichols, A., & Freedman, R. (2010). Uncovering Health Care Inequalities Among Adults with Intellectual and Developmental Disabilities. Health and Social Work, 35(4), 280–290.
Weaver, H. N. (2006). Social Work Through an Indigenous Lens: Reflections on the State of Our Profession. In N. Hall (Ed.), Social Work: Making a World of Difference, Social Work Around the World 1V in the Year of IFSW’s 50th Jubilee (pp. 37–51). Berne: International Federation of Social Workers and Fafo.
Wilkinson, G. (2015). Social Work Practice Statement: The Contribution Social Work Can Make to the National Disability Insurance Scheme (NDIS). Retrieved from https://www.aasw.asn.au/document/item/7420.
World Bank. (2015). Bangladesh Country Profile. Retrieved from http://www.wb.org.
Yeo, R., & Moore, K. (2003). Including Disabled People in Poverty Reduction Work: “Nothing About Us, Without Us”. World Development, 31(3), 571–590.
Zastrow, C. (2004). Introduction to Social Work and Social Welfare: Empowering People (8th ed.). Belmont, CA: Brooks/Cole.
Zastrow, C. (2009). Introduction to Social Work and Social Welfare: Empowering People (10th ed.). Baltimore, MD: CENGAGE Learning.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Ali, I. et al. (2020). People with Disabilities: The Role of Social Workers for Rehabilitation in Bangladesh. In: Momen, M.N., Baikady, R., Sheng Li, C., Basavaraj, M. (eds) Building Sustainable Communities. Palgrave Macmillan, Singapore. https://doi.org/10.1007/978-981-15-2393-9_20
Download citation
DOI: https://doi.org/10.1007/978-981-15-2393-9_20
Published:
Publisher Name: Palgrave Macmillan, Singapore
Print ISBN: 978-981-15-2392-2
Online ISBN: 978-981-15-2393-9
eBook Packages: Economics and FinanceEconomics and Finance (R0)