
Abstract
The aim of this review is to diagnose the nutrition transition in Sri Lanka with special emphasis on the nutrition profile of the country. The estimates reported in peer-reviewed journal articles and relevant national surveys conducted by the government agencies from 1977 to 2017 were synthesized. The estimates were summarized using tabular analysis, and trends over time were estimated using meta-regression models. The synthesis revealed that a considerably higher proportion of Sri Lankan population suffers from at least one form of malnutrition and the problem of undernutrition and hidden hunger is overlapping with the increasing threat of overnutrition despite the better performance shown by the economy as per various social and health indicators. The results of the meta-regression analysis revealed declining trends in many forms of undernutrition, particularly among females, over time. While the estate sector is more vulnerable to undernutrition among preschool children, the urban sector is more vulnerable to rising level of overnutrition across all age cohorts. The society is on the verge of entering into the fourth stage of nutrition transition, which is characterized by the consumption of energy-dense food, overweight and obesity, and rising non-communicable diseases (NCDs). It is recommended to make food systems more nutritionally sensitive through appropriate research, pricing, trade, food and nutrition policies to promote production and consumption of nutritious and healthy foods.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
The existing body of literature documents two-way interrelationship between nutrition and economic development (Ranis et al. 2000; Suri et al. 2011). Better nutritional status of the population is considered as an end as well as a critical input to an economic development (Strauss and Thomas 1998; Ranis et al. 2000; Bhargava et al. 2001; Smith and Haddad 2002; Bloom et al. 2004; Well 2007; Narayan et al. 2010). Evidence from Sri Lanka indicates a strong causal relationship between the nutritional status and school achievement (Wisniewski 2010) and labor productivity (Sahn and Alderman 1988) reinforcing the importance of nutrition as an input to formation of human capital and in turn economic growth. Hartwig (2010) reported that the importance of nutrition to economic development is more important to middle-income countries as their marginal productivity of health is higher than that in the high-income countries.
Coexisting to this literature, Popkin (1994, 1998, 1999, 2001, 2002, 2003, 2004) illustrated a dynamic nature of the relationship between income growth and nutritional status of the people. It has been argued that as the income of a country rises and the rate of urbanization increases, its people enter into different stages of consumption and physical activity levels (Fig. 2.1). The term used to classify this phenomenon is “nutrition transition.” When the income of a country rises, people will replace their traditional diet, which is low in fat and high in cereal with more fruit and vegetable and products of animal origin. However, when income further rises, diet of the people shifts more toward high-fat, more sugar, and processed foods which are low in fiber. The outcome of this shift is an epidemiological transition where people move away from nutrient deficiency diseases (undernutrition) toward higher rates of non-communicable diseases (NCDs) and overnutrition. With further rise in income and changes in life style, people will realize the adverse health effects of the high-fat, high-sugar diet and consequently will move toward a simple diet based on grains, vegetables, and fruits. It is further argued that at the presence of inequality in socioeconomic status across different geographical and socioeconomic sub-groups in a country, it is possible that different sub-communities will be at different stages of the transition. The outcome of this unequal rate of transformation is the coexistence of undernutrition and overnutrition at a cross section of time. Since inequality in economic development is a norm rather than an exception, this overlapping of phases is a common phenomenon in both developing and transitional economies.

Nutrition transition (Source: Adopted from Popkin (various years))
It is evident that many developing and transitional economies have undergone nutrition transition in varying degrees. For example, in China, consumption has shifted more toward a diet high in fat resulting in increased overweight and obesity (Bell et al. 2001; Popkin 2001). In South Korea, consumption of animal-based food and vegetable and fruits has increased over the years, but the total fat consumption was maintained at a steady level. Thus the prevalence of overweight and obesity has not changed (Lee et al. 2002). As reported by Baker and Friel (2014), the consumption of fat, sugar, and salt has increased in the recent past in many Asian countries due to the tendency toward consuming more processed foods. Accounting for the demographic and epidemiological changes in Sri Lanka, it is apparent that the country, too, has a conducive environment for a nutrition transition and its consumption pattern is changing (Wijesekere 2015; Weerahewa et al. 2018a, b).
Against this background, the aim of this chapter is to examine the nature of nutrition transition of Sri Lanka. More specifically, this review (i) synthesizes the published literature on undernutrition, overnutrition, and dietary pattern of Sri Lanka for the time period from 1977 to 2017 with a view to examine the nature of nutrition transition of Sri Lanka, and (ii) documents the empirical evidence on the underlying causes of the undernutrition and overnutrition problems in Sri Lanka. The review attempts to inform policy makers on the areas where interventions are required and to inform researchers on the gaps in literature. Furthermore, the analysis will enable to track the process of achieving the second and third Sustainable Development Goals (SDGs) on Zero hunger, and Global Health and Wellbeing, respectively.
The chapter is organized as follows. The next section sets the background of the study summarizing the economic situation, food policies, safety net programs, and diet transformation in the country. Section 3 introduces the methodology of the review paper, while Sect. 4 presents the results of review. Section 5 describes the nutrition transition in Sri Lanka and the final section concludes the paper with a way forward.
2.2 Contextual Background
2.2.1 Key Characteristics of the Sri Lankan Economy
Sri Lanka is a lower middle-income country with a per capita GDP of USD 4065 in 2017 (Central Bank of Sri Lanka 2017). It is evident that the country’s economy has been shifted toward industry- and service-oriented economy over the years, from a predominant agriculture base. Despite the declining role of agriculture sector to the economy, the sector provided direct employment to 26.1% of the labor force in 2017. However, due to low labor productivity in the agriculture sector, the share of the agriculture sector in total GDP is three times less than its share in the labor force.
Sri Lanka has experienced a remarkable increase in per capita GDP over the last few decades. In line with this economic growth, the rate of poverty has declined to a level of 4.1% in 2016 from being 26.1 in 1990/1991 (DCS 2017). Over the same period, the quality of the human capital, in terms of education and health, has increased. However, despite these achievements in the social sphere, Sri Lanka has continued to struggle to combat food insecurity and malnutrition. A considerable proportion of women and children in Sri Lanka still suffers from malnutrition (DCS 2017).
The percentage of the population living in urban areas has been stagnant in Sri Lanka, and approximately 18% of the population live in urban areas (World Bank 2018). However, there is a rapid increase in the expansion of urban areas in Sri Lanka that has led to an increase in population surrounding major urban areas (Ellis and Roberts 2015). Unlike in many South Asian countries, Sri Lanka has been able to alleviate urban poverty in a significant manner. The poverty incidences in urban areas reduced from 16.3% in 1990/1991 to 1.9% in 2016 (DCS 2016).
As in many developing countries, government intervenes in food systems, food pricing, and nutritional programs in Sri Lanka. Thus, for a better understanding of the changes in diet and malnutrition, one needs to have a better idea about the food and nutrition policies, food assistance programs, and nutritional interventions carried out by the government in the country. A brief description of those interventions is presented below.
2.2.2 Food and Nutrition Policy Framework During 1977–2017
With the liberalization of the economy in 1977, Sri Lanka shifted its policy orientation from protectionist to outward. Subsidies on many food commodities were removed and taxes on imports were cut down. However, country continued to protect the rice producers. To boost the local paddy production, huge public investments were made on irrigation projects. This open economic policy continued for two decades and in 2005, a major shift in outward-oriented policy took place with the change in political regime in the country. Several trade-related taxes were imposed on imports, though essential goods were levied from import tax. Several national-level programs were implemented during this period to promote home gardening and local food production. “Api wawamu rata nagamu” (“Let us grow and uplift our nation”) is one such programs (Weerahewa et al. 2017).
Extensive bodies of empirical research have been focused on the evolution of food and nutrition policy framework in Sri Lanka during the past several years. Among them, Edirisinghe (1987), Bhalla (1991), Ellis et al. (1997), Shekar et al. (2007), and Weerahewa et al. (2017, 2018a, b) provided detailed reviews, and the following subsections provide some salient features in those literature.
2.2.2.1 Food Assistance and Safety Net Programs
Sri Lanka has a long history of food assistance programs. At its inception was “Universal rice ration scheme,” which covered everyone in the country. However, most of the food assistance programs implemented after 1970 were targeted interventions. One of the earliest of this sort was the food stamp program. The next salient change to food assistance program was the replacement of direct food assistance program with social safety net program, which included food assistance as a main component. “Janasaviya,” which was in operation from 1989 to 1994 was the first of such kind. Later in 1995, this program was replaced by another income transfer program called “Samurdhi.”
2.2.2.2 Nutritional Interventions
In parallel to food assistance and social safety net programs, nutritional intervention programs were implemented even before 1977 in the country to combat both macro and micronutrient deficiencies among preschool children, primary school children, and pregnant mothers. Among them, Thriposha program and school midday meal program were the oldest. Salt iodization program to control Iodine Deficiency Disorders (IDD), provision of iron supplements to pregnant mothers and preschool children, provision of Poshana Malla (“nutrition bag”), a package containing nutritious food to pregnant women, are more recent interventions that the government has launched. Moreover, a program to provide a nutrition allowance of Rs. 20,000 to pregnant and lactating mothers was introduced in 2015 with the aim of minimizing the number of low birthweight babies in Sri Lanka. Its mode of implementation changed in May 2016 where a new voucher was introduced to replace the coupons.
With all these changes in the economy, social sphere and in policy arena, diet of the people has transformed, and the next section will outline these diet transformations in a nut shell.
2.2.3 Diet Transformation
This section depicts the dietary shift in terms of the intake of calorie, protein, and fat and the sources of these macro-nutrients focusing on the change in food basket of consumers. It examines the changes in the share of dietary energy, protein and fat coming from animal-origin foods. Change in vegetable and fruit consumption and sugar consumption are the indictors used in depicting the shift in diet.
2.2.3.1 Dietary Nutrient Intake
In the absence of continuous data series on dietary energy, protein, and fat intake, The FAO food balance sheet data, which provides time series data on per capita availability of calorie, protein, and fat till 2013, were extracted to present how availability of major nutrients has changed during 1977–2013. The per capita availability of dietary energy in Sri Lanka has increased from 2199 to 2539 kcal per capita per day from 1977 to 2013. This is higher than the recommended intake of 2030 kcal per day in 2002 as given by the DCS (recommended figure for recent years is unavailable). The FAO indicated that Sri Lankans still derive more than 90% of their dietary energy from plant origin foods, though the share has slightly decreased from 96% to 93% during this period. During the period 1977–2013, the per capita supply of dietary energy from animal-origin product has increased from 95 to 167 kcal per capita per day.
Per capita availability of protein for a Sri Lankan has increased from 46.05 g to 59.71 g from 1977 to 2013. Even though 72% of the total protein is still derived from food of plant origin, over the years, protein derived from food of animal origin has more than doubled (7.44 g to 16.31 g per capita per day) from 1977 to 2013. The share of food of animal origin to total protein intake has increased from 16.16% in 1977 to 27.32% in 2013. According to household Income and expenditure Surveys (HIES), this increased share of food of animal origin to total protein has come from the increased consumption of egg, fish, and meat (DCS 2018).
There was a marginal increase in the daily per capita availability of fat in Sri Lanka. It has increased from 42.18 g in 1977 to 49.71 g in 2013 (Fig. 2.2). Although the availability of fat from foods of plant and animal origin has increased over the study period, the major contribution has come from food of plant origin. The share of food of animal origin in total daily fat has increased from 12.92% to 17.24% from 1977 to 2013.

Changing availability of major nutrients in Sri Lanka (Source: FAOSTAT)
In summary, it can be concluded that the Sri Lankan diet has transformed to accommodate more calories, more protein, and more fat during the past few decades (Fig. 2.2). In terms of the changes in the contribution of food commodity to total energy during late 1970s, little over 60% of the calorie comes from starch, cereal, and tuber crops. According to Bogahawatte and Kailasapathy (1986), by 1970, the starchy staples had provided 75% of the total calorie requirement of the population. However, over the years, their contribution has declined to 56% (FAOSTAT). In 1980, the most important food commodities in Sri Lankan diet were rice and coconut (Sahn 1988). However, analysis of data from HIES suggests that, with time, consumption of rice, coconut as well as wheat has decreased and that of protein-rich commodities such as pulses, meat, fish, and egg has increased. The consumption of fresh milk was an exception, which has declined over the years, due to increased consumption of powdered milk.
In some geographical areas, e.g., Colombo (which houses one-tenth of the population), people are moving away from cereal-based diet (rice- and wheat-based) to more vegetable-, meat-, and fish-based diets (FAO 2016). Less than 30% of the weight of their diet is comprised of rice and wheat. In contrast, closer to 60% of the diet of Nuwara Eliya consumers is from rice and wheat.
2.2.3.2 Vegetable and Fruit Consumption
The intake of vegetable by an average Sri Lankan has remarkably increased over the years as 16.89 kg per capita per year in 1977 to 46.24 kg per capita per in 2013. However, the consumption of fruit has decreased over the study period from 64 kg per capita per annum (1970) to 36 kg per capita per annum (2013). With these opposite trends, the intake of vegetables and fruits as one category has only shown a marginal increase over the years (Fig. 2.3).

Fruit and vegetable consumption in Sri Lanka from 1977 to 2014 (Source: FAOSTAT)
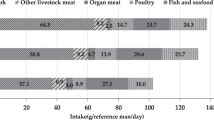
2.2.3.3 Meat and Fish Consumption
There was a considerable increase in meat intake by a Sri Lankan though the consumption of certain meat types such as bovine meat, mutton, goat meat, and pork has decreased. Increase in per capita availability of poultry meat has increased the per capita availability of meat from 3.62 in 1977 to 6.48 in 2013 kg per capita per year. Fish consumption also has more than doubled during the same period where the consumption has increased from 10.09 to 25.65 kg per capita per year during 1977 to 2013. Similarly, the marine fish consumption and fresh water fish consumption also have increased from 0.9 to 3.2 kg per capita per year.
2.2.3.4 Sugar and Salt Intake
Sugar and sweetener intake has increased over the study period (1977–2013), from 8.67 to 26.34 kg per capita per year. As a percentage, the energy intake from sugar was 0.39% of the total energy intake in 1977 and 10.47% in 2013, surpassing the WHO recommended level, which is below 10%.
There was no national figure available for salt intake. The WHO (2012) recorded the level of salt intake by Sri Lankan as 9–11 g per day, while a national survey conducted by Jayawardena (2014) reported sodium intake, which is the main component of salt, as 3.26 g for male and 2.51 g for female. Salt intake in 1970 was recorded as 7 g per day per capita, suggesting that even five decades ago, salt intake by a Sri Lankan was higher than the recommended level of 5 g per capita per day. With the time salt intake has further diverged from the recommended intake. As the WHO step survey indicates (WHO 2015) this may be due to the increased consumption of processed foods, which are high in sugar and salt.
With this general background of the country, the methodology adopted in this review to diagnose the nutrition transition in Sri Lanka is presented next, with special emphasis on nutritional status.
2.3 Methodology
2.3.1 Approach
In achieving the objectives of the study, the review synthesized the published literature focusing on the key features of each stage of nutrition transition (Fig. 2.1). In particular, the study utilized indicators of undernutrition (stunting, wasting, and underweight), overnutrition (overweight and obesity), and micronutrient deficiencies (iron deficiency anemia and vitamin A deficiency) in exploring the trend of the prevalence rate. Table 2.1 provides the definitions of the parameters. In determining the causal linkage between socioeconomic condition and malnutrition, the study hypothesized that poverty, sector of residence, gender of the child, age of the child, and education level of the mother are strongly associated with the incidence of malnutrition, and it was tested using a meta-regression. The stage of nutrition transition was determined using the characteristics associated with each stage as mentioned in Fig. 2.1.
2.3.2 Meta-Database and Eligibility Criteria
A general Google search was run to obtain key relevant research in the areas of nutrition and food consumption. Key terms and phrases included in the search were malnutrition, child malnutrition, overweight and obesity, nutrition transition, food consumption behavior, anthropometric measures of nutrition, nutritional status of preschool children, nutritional status of adolescents, nutritional status of adults, dietary diversity, micronutrient deficiency, and anemia. In addition to the search in the Google Scholar, the study scanned the reference lists of newly included studies and previous review studies (Rajapaksa et al. 2011; Bandara and Weerasinghe 2015). The database included Well-Being and Social Policy Journal, Obesity Reviews, Asia Pacific Journal of Public Health, Tropical Agricultural Research, Food and Nutrition Bulletin, Poverty and Economic Policy Network, BMC Public Health, European Journal of Preventive Medicine, Sri Lanka Journal of Diabetes Endocrinology and Metabolism, International Journal of Environmental Research and Public Health, Ceylon Journal of Medical Sciences, Ceylon Medical Journal, Preventive Medicine, Galle Medical Journal, Public Health Nutrition, Gerodontology, BMC Pediatrics, Asia Pacific Journal of Clinical Nutrition, and BMC Obesity. Apart from the original research articles, a number of national study reports were added to the meta-sample. These included reports of Demographic and Health Survey (DHS) for various years, annual reports of the Family Health Bureau, and various health reports published by the DCS, Sri Lanka.
Once the relevant peer-reviewed articles and national reports were complied, authors screened the abstracts of all relevant studies to decide whether to include them into the database. In constructing the meta-database, restriction was set to obtain original research studies carried out in Sri Lanka to assess the nutritional status and food consumption behaviors during the period from 1979 to 2018. The study included only the published peer-reviewed articles in economics, medicine, and nutritional disciplines. It excluded gray literature (working papers, conference proceedings, and technical reports) and studies that focused on nutritional status of patients. Only research articles written in English were included to the meta-database. All the primary studies included had either estimated malnutrition among preschool children, primary school children, adolescents, and adults or determinants of malnutrition in Sri Lanka. All entries have also assessed at least one of the following nutritional outcomes: stunting, wasting, underweight, micronutrient deficiencies, overweight, and obesity. The Prisma flow diagram is depicted in Fig. 2.4.

Prisma flow diagram
2.3.3 Tabular Analysis
Once the meta-database was constructed, authors extracted information from each research study, namely author, year of the study, population of interest, sample size, measure of malnutrition, micronutrient deficiencies, determinants of nutritional status, title of the article, and the journal. Then, the data were systematically tabulated for synthesis.
The stage of nutrition transition was diagnosed with a change in the prevalence rate of undernutrition (stunting, wasting, underweight, thinness), overnutrition (overweight and obesity), and the prevalence rate of anemia among preschool children, adolescents, and adults.
2.3.4 Regression Analysis
The regression analysis was performed to test the study hypothesis related to the causal factors of child malnutrition in Sri Lanka. The sector of the residence (x1), gender of the child (x2), age of the child (x3), income level of the household (x4), year of the survey (x5), and the education level of the mother (x6) were treated as explanatory variables in the regression model (Eq. (2.1). All the explanatory variables are dummy variables. Here, the ith subscript denotes the year of the survey.
where, the dependent variable of the model (Yi) is the rate of prevalence of malnutrition in the ith year, β0 is the constant term and βj are the estimated coefficients, and εi is the error term. The Eq. ((2.1) was tested for the pool sample as well as for each sector of residence and gender of the child. In total, ten econometric models were estimated.
In obtaining the published data on malnutrition to the regression analysis, the study only utilized the national-level findings published by DCS, Sri Lanka. Data available on Demographic and Health Survey (DCS 2007, 2016) report on “Nutritional status of preschool children in Sri Lanka by DCS, undated” and report on “Social Conditions of Sri Lanka” were extracted.
2.4 Results
2.4.1 Trends in Nutritional Status and Determinants
This section presents the findings of the review using tabular analysis. In this exercise, the result section is divided into three main sub themes: Undernutrition, prevalence of anemia, and overweight and obesity. In each subsection, the paper will first summarize the studies reviewed and then presents and discusses the findings. Each section will conclude with a review of studies carried out to determine specific nutritional problem.
2.4.1.1 Status of Undernutrition among Preschool Children
The review consisted of 29 published reviewed articles or national reports on child malnutrition in Sri Lanka. Out of them, nine studies are national representative studies (Gavan and Chandrasekera 1979; DCS 1988, 1995, 2002, 2009, 2017; FHB 2009, 2010, 2011). Six studies were exclusively on malnutrition among children between 0- and 5-year old (DCS 2009, 2017; FHB 2011; Perris and Wijesinghe 2011; Jayatissa et al. 2012a, b, c). Some studies have limited their focus to study malnutrition in children between the age of 3 and 60 months (DCS 2002; Jayasekera 2006). Some other studies have excluded the babies aged less than 6 months, 1 year, and 2 years old in studying child malnutrition in Sri Lanka (Thamilini et al. 2015; Kandeepan et al. 2016; Jayatissa and Wickramage 2016). This variation in the age group presented a difficulty in making comparison between studies. Though the DHS reports are available from 1988 to 2017, the difference in their target population makes it harder for a one-to-one comparison across figures. Except few (Malkanthi et al. 2007, Gavan and Chandrasekera 1979; Pathmeswaran et al. 2005), all the other national and sample surveys have estimated the prevalence of malnutrition through three widely used anthropometric measures: stunting, wasting, and underweight (Tables 2.2, 2.3 and 2.4).
All national studies have witnessed a snail pace in progress in tracking all forms of malnutrition in Sri Lanka. In fact, the prevalence of wasting has slightly increased in Sri Lanka over the study period (DCS 1988, 1995, 2002, 2017). However, there was a geographical inequality in the rate of change of malnutrition. In comparison to other two sectors, estate sector has shown a remarkable progress in curtailing the proportion of children who were stunted (DCS 1988, 2017; Gavan and Chandrasekera 1979). By 1988, two in every three children were stunted in the estate sector and by 2016, only one in three children were stunted.
In 2016, the prevalence of underweight among preschool children in Sri Lanka was 20.5% (DCS 2017), which was relatively higher as compared to stunting (chronic malnutrition) and wasting. The prevalence of stunting in Sri Lanka (17.3%) is less than the corresponding figure for South Asia and in the world (Tables 2.5 and 2.12). However, wasting (15.1%) is relatively high in Sri Lanka as compared to the World and South Asia (Table 2.5). Considering the regional disparities, prevalence of wasting among urban children is lower compared to estate and rural children (DCS 2017).
There were ten studies focusing on child malnutrition in sub-populations. One study has focused on the child malnutrition in farming communities (Malkanthi et al. 2007) and their reported value of stunting (19% in 2005) was higher than the closest national survey value of 13.5% reported by DCS in 2002 (DCS 2002). Prasanna (2015) also reported a higher stunting value of 23% for the fishing community. Those two studies reflect higher vulnerability of farming and fishing communities to chronic malnutrition. However, the prevalence of wasting (11.2%) in the fishing community was lower than the national average (15.1%) reported in DCS (2017). In contrast, Peiris and Wijesinghe (2011) reported that the prevalence of stunting was lower and that of wasting was far higher in the Weeraketiya area compared to the national average figure for the recent year. As wasting is an outcome of the recent lack of food or illness that prevents children from eating or absorbing nutrient and stunting is an indicator of chronic undernutrition, the latter is less surprising.
Another study reported that in state-operated foster care institutions, half of the children between the ages of 3 and 60 months were stunted, one-fourth was wasted and two-thirds were underweight (Jayasekera 2006). As expected, children in the war-affected areas were more malnourished than others with respect to all the three forms of malnutrition (Kandeepan et al. 2016). When the age range of children and the risk of malnutrition are considered, children less than 6 months of age seem to be at a minimum risk (Nanayakkara and Silva 2011). Further, the children in households having a migrant worker father were found to be less stunted (Jayatissa and Wickramage 2016).
2.4.1.2 Status of Undernutrition Among Adolescents and Adults
There is a dearth of research on malnutrition among school-age children and adults in Sri Lanka. However, as revealed by Jayatissa et al. (2002), the rate of malnutrition among primary school children was as same as preschool children in 2002 (Table 2.6). Malnutrition continued to prevail at the same rate among preschool and primary school children. However, a recent study signaled a rising rates of both underweight and stunting among primary school children (Naotunna et al. 2017). There was a marginally lower prevalence rate of stunting. The same study suggested that one in four of the primary school children are thin and that the proportion of boys who are thin was statistically higher than that of girls. Study of Pathmeswaran et al. (2005) revealed that none of the students in a selected private school were stunted. In another study, it was revealed that primary school children in Colombo had a relatively lower rate of malnutrition prevalence (Thilakarathne and Wijesinghe 2011).
Study on malnutrition among adolescents have given arise to a large range of estimates, starting from 16.4% (wasting) to 28.5% stunting and 47.2% underweight (Jayatissa and Ranbanda 2006; FHB 2015). The FHB (2012, 2015) reported stunting and wasting in children among different school grades, suggesting that over a period of 3 years, prevalence of both stunting and wasting has marginally increased, except among Grade 7 students. Only very few studies are available on the adult anthropometry and among them one indicates that 14.9% of women and 16.2% of the men between the age category of 18 and 59 are thin (Jayatissa et al. 2012a, b, c). Considering the regional disparities, 22% of the estate women were thin in 2016 (DCS 2017).
2.4.1.3 Determinants of Undernutrition
Fifteen studies examined the association or causal relationship between household income, mother’s nutritional status, socioeconomic status, feeding behavior, and child malnutrition in Sri Lanka. Of the 15, 5 reported a significant negative association between (causality) household income and/or wealth and child malnutrition (Ekanayake et al. 2003; Rathnayake and Weerahewa 2005a, b; Rannan-Eliya et al. 2013; Jayatissa and Wickramage 2016). Of these five studies, one study (Rathnayake and Weerahewa 2005b) has researched the association between mother’s income and child nutritional status (Table 2.7). The findings of this study indicate that when maternal employment generates extra income, the calorie intake of all individuals of the household increases, yet the allocation of calories to the children of the household is reduced.
Six of the 15 studies listed in Table 2.7 have investigated the association between mother’s knowledge and child malnutrition (Ekanayake et al. 2003; Rathnayake and Weerahewa 2005a, b; Jayawardena 2012, 2014; Prasanna 2015). Some studies have conceptualized the maternal knowledge about nutrition through their literacy rate (Prasanna 2015) and number of years of schooling (Rathnayake and Weerahewa 2005a, b; Jayawardena 2012), while Ekanayake et al. (2003) has specifically looked at awareness of the mother on nutritional aspects. Irrespective of the different conceptualization, except one almost all of the studies reported a significant negative causality between mother’s knowledge/education and child malnutrition. The association between mother’s nutritional status and age, and child malnutrition has been assessed in three studies using maternal height and maternal BMI as proxy for maternal nutritional status (Ekanayake et al. 2003; Rannan-Eliya et al. 2013; Ubeysekara et al. 2015). All three studies reported a positive association between age of the mother and the child malnutrition. The association between the maternal height and child malnutrition is negative (Rannan-Eliya et al. 2013).
The significant association between the feeding practices and child malnutrition was reported in four studies (Rannan-Eliya et al. 2013; Jayawardena 2014; Ubeysekara et al. 2015; Perkins et al. 2018). Examples of feeding practices included to the econometric models were, late introduction of fat and oil to child food, continuation of breastfeeding at the age of one, early initiation of breast feeding, and feeding with a low protein diet.
Apart from the above determinants, some reported studies have looked at the association between child malnutrition and alcoholism of the farther or smoking habit of the farther (Jayawardena 2014; Prasanna 2015), low birthweight, altitude, ethnicity, number of children in the family, and the household size. The effect of low birthweight will continue to hamper the growth of child in later state as well (Ekanayake et al. 2003; Jayawardena 2012; Rannan-Eliya et al. 2013; Jayatissa and Wickramage 2016).
2.4.2 Micronutrient Deficiencies
Nineteen studies included in this review have estimated the prevalence of anemia among preschool children, adolescents, and adults (Table 2.8). Among them, 12 were national-level surveys (Jayatissa (2009); Mudalige and Nestel 1996; Piyasena and Mahamithawa 2003; Pathmeswaran et al. 2005; Jayatissa and Ranbanda 2006; Hettiarachchi et al. 2006; DCS 2007; Jayatissa and Hossaine 2010; Jayatissa et al. 2012a, b, c; Naotunna et al. 2017; Allen et al. 2017). As per the findings of the national surveys conducted by the MRI in 1996, 45% of the preschool children in Sri Lankan were anemic (45%) (Jayatissa et al. 2012a, b, c). However, with the time, deficiency has declined to a level of 15.1% (Jayatissa et al. 2012a, b, c). By 1994, the prevalence rate of anemia among primary school children and adolescents was closer to 50% (Mudalige and Nestel 1996). According to DCS (2007), there was a marginal decrease in the prevalence rate in 2006/2007 for all age groups. However, even by mid of the 20th century closer to one-third of the preschool children and more than one-third of pregnant and nonpregnant women were anemic. An estimate coming from a geographic subgroup (Galle in the Southern Province of Sri Lanka) indicated that in 2003, the prevalence rate of anemia is as high as 54% among adolescents (Hettiarachchi et al. 2006). The prevalence rate among primary school children in 2014 in North Central province was only 17.3% (Allen et al. 2017; Naotunna et al. 2017). Many sample surveys carried out after 2006 indicated that the rate of anemia prevalence was less than 20% for several communities (Jayatissa et al. 2012a, b, c; Senadheera et al. 2017) except for Jaffna, which was a war-affected area (Kandeepan et al. 2016).
The prevalence of anemia among boys has been slightly higher than that among girls in both preschool children and primary school children (Pathmeswaran et al. 2005; DCS 2007; Jayatissa and Hossaine 2010; Jayatissa et al. 2012a, b, c). However, adolescent females had shown a higher prevalence compared to males (Hettiarachchi et al. 2006; Allen et al. 2017).
2.4.3 Overweight and Obesity
2.4.3.1 Overweight and Obesity Among Preschool Children
Twenty of the included studies examined overweight and obesity among Sri Lankan population (Table 2.9). Out of them, 11 had explored the prevalence of overweight among preschool children and adolescents (Pathmeswaran et al. 2005; Jayatissa and Ranbanda 2006; Thilakarathne and Wijesinghe 2011; Jayawardena et al. 2012; Jayatissa et al. 2012a, b, c; Rathnayake et al. 2014a, b; FHB 2015; DCS 2017), while the rest studied the prevalence of overweight and obesity among adults (Fernando et al. 1994; Katulanda et al. 2010; Fernando and Wijesinghe 2010; Jayatissa et al. 2012a, b, c; Perera and Ekanayake 2012; Rathnayake et al. 2014a, b; Jayawardena et al. 2012, 2013a, b, 2016, 2017; DCS 2017).
As per the survey findings, the prevalence of overweight and obesity is less than 3% among the preschool children (Jayatissa et al. 2012a, b, c; DCS 2017). Considering the inequality, only 1.3% of the preschool children in the estate sector are overweight as compared to the urban sector (2.9%; DCS 2017). Male children have a higher tendency to be overweight than females (Jayatissa et al. 2012a, b, c). Primary school children have shown a higher tendency to be overweight and obese than preschool children (Pathmeswaran et al. 2005; Jayatissa et al. 2012a, b, c; FHB 2015). However, the difference is not that high except for the primary school children enrolled in private schools (Pathmeswaran et al. 2005) and primary school children in Colombo area in the Western Province (Thilakarathne and Wijesinghe 2011). As reported in Pathmeswaran et al. (2005), 20% of the private school students in the studied sample were overweight. In many studies the prevalence of overweight was found to be higher than that of obesity. Among the adolescents, nearly 5% are overweight (Jayatissa et al. 2012a, b, c; FHB 2015). As observed, the prevalence of overweight and obesity is relatively higher among boys than girls among primary school children and adolescents.
2.4.3.2 Overweight and Obesity Among Adult Men and Women
Prevalence of overweight and obesity among adults are far higher than that of preschool children and school-age children (Table 2.10). Despite the range of values reported by different studies, the prevalence of overweight among adults is at least four times higher than that of preschoolers and adolescents.
One study using a nationally representative sample reported that the overweight and obesity statistics related to women were 31.9% and 13.3%, respectively, for the year 2016 (DCS 2017). However, as suggested by DCS (2007), the prevalence of overweight and obesity among women was lesser a decade ago, i.e., 24% in 2016 and 7.2% in 2006 (DCS 2007). As both the studies have been carried out by the same institute and the age group was similar, these statistics are comparable and they reflect the rising burden of overnutrition among adults in Sri Lanka. Another national survey suggested that the prevalence was slightly lower among male in which 22.8% and 6.6% are overweight and obese, respectively (Jayatissa et al. 2012a, b, c).
In terms of the geographic distribution of the prevalence of overnutrition, three national studies (DCS 2000, 2007, 2017) have provided evidence to the positive association between urban living and the prevalence of overweight. In urban sector, one in three women are overweight and one in five women are obese. In particular, urban women are twice likely to be overweight as compared to estate women. However, with the rapid increase in the incidence of overweight in the estate sector women, the gap between two sectors is getting narrowed.
Apart from the nationally representative samples, several reports have presented overweight and obesity prevalence for a number of subgroups, e.g., adults in Colombo, women in Pannala and Negombo, institutionalized elders, men in Kandy (Fernando et al. 1994; Fernando and Wijesinghe 2010; Perera and Ekanayake 2012; Rathnayake et al. 2014a, b; Jayawardena et al. 2016; Jayawardana et al. 2017). The prevalence of obesity among cardiac patients, men in Kandy, and women in Pannala and Negombo is higher than the national-level statistics.
2.4.3.3 Determinants of Overweight and Obesity
There were eight studies, which have explored the association between overweight and obesity, and household income, physical activity level, leisure activities, and education level of adults (Arambepola et al. 2008; Katulanda et al. 2010; Jayatissa et al. 2012a, b, c; Perera and Ekanayake 2012; Rathnayake et al. 2014a, b; Jayawardana et al. 2017). Of these, five have reported a positive association between overweight and household income (Katulanda et al. 2010; Jayatissa et al. 2012a, b, c; Rathnayake et al. 2014a, b; Jayawardana et al. 2017), and three reported a negative association between physical activity level and overweight among adults (Rathnayake et al. 2014a, b; Jayawardena 2014). Two of these studies have found a positive relationship between urban living and overweight (Katulanda et al. 2010; Arambepola et al. 2008). The association between female gender and overweight and obesity was reported by Katulanda et al. (2010) and Perera and Ekanayake (2012). Surprisingly, three studies have reported a positive association between education level and the incidence of overweight, of which one has studied the overweight among preschool children (Jayatissa et al. 2012a, b, c), and the other has studied the overweight among adults (Katulanda et al. 2010). One study focusing on overweight and obesity among adolescents reported that lower fruit consumption, skipping of breakfast, and intake of high-energy dense food are positively associated with the overweight prevalence among adolescents (Rathnayake et al. 2014a, b; Table 2.11).
2.5 Diagnosis of Nutrition Transition
2.5.1 Key Trends, Patterns in Malnutrition and Its Determinants
As Table 2.12 indicates, child’s nutritional status has improved in Sri Lanka, while WRA anemia has declined over the last 40 years. However, there is a slight increase in obesity and overweight among adults. This contradicting sign indicates that Sri Lanka is facing double burden of malnutrition. In fact, more than one in ten preschool and school children in Sri Lanka suffer from at least one form of undernutrition. This proportion is even higher in the estate sector due to relatively higher rates of poverty and low level of maternal education, maternal nutrition level, and poor feeding practices.
As brought up in this review, income is one of the key determinants of undernutrition. People in the lowest income quartile consume monotonous cereal-based diets which lack some important macro and micronutrients. In contrast, people in the highest income quintile consume more diversified diets which are relatively high in animal-based foods. However, increase in income does not always lead to higher nutrient intake as part of the increased income is spent to buy nonnutritive attributes. Therefore, it is not the family income but the effective income allocated for the consumption of nutritious food that affect the nutritional outcome of the household. Any addiction that reduces the income allocated to food consumption will negatively influence the nutrition outcome of the household. Addiction to alcohol and smoking habit of the father are two such addictions that have prevented the child achieving its desired level of growth in estate sector and fishing community in Sri Lanka. This has become a determinant in the estate sector because estate sector dwellers are more likely to consume alcohol compared to urban and rural dwellers (Jayathilaka et al. 2016).
This review suggests two opposite relationships between women’s employment and child malnutrition. While many of the studies portray an inverse association between women’s employment and child nutrition, one study suggests a positive association between the two variables, probably due to the interlinkage between women’s income and caring. Though increase in women income can be used to improve the nutritional status of children, due to the increased time burden of women, growth of infants could be adversely affected by women employment (Johnston et al. 2018). However, older children are benefited by the income contribution of the mother. Similarly, Burroway (2017) also showed that although some jobs are capable of alleviating child malnutrition, malnutrition is high among people those who are engaged in agricultural jobs.
Income is a necessary but not a sufficient drive to alleviate child malnutrition. As indicated by the analysis of the available literature, nutritional status of the mother is a critical factor in determining the nutritional outcome of the child. Maternal height and BMI affect anthropometry of preschool children. This intergeneration vicious cycle needs to be broken down to improve child nutrition. Maternal height and BMI influence the birthweight and the nutritional outcome of the child. The chance of giving birth to a low weight baby is higher among malnourished mothers than other groups. The role of mother in determining the nutrition outcome goes beyond this intergenerational relationship. Mother’s knowledge on health and growth of a child plays a significant role in improving the child health (Glewwe 1999).
With respect to the determinants of overweight and obesity, unlike in some developing countries where overweight and obesity are associated with lower income groups and least education level (Drewnowski and Specter 2004), the opposite has been observed in the Sri Lankan context where obesity rates are higher among high-income and highly educated groups than the low-income and less-educated groups. This may be partly due to the difference in food consumption basket and physical activity of these groups.
2.5.2 Results of the Econometric Analysis
The results of the meta-regression analysis were consistent with our expectations and previous literature (Table 2.13). The results of the analysis indicate that over the years, both stunting and underweight in Sri Lanka have significantly reduced (models 1–9), while wasting has increased (Model 8). Regression results further witnessed a geographical inequality in child malnutrition where urban children are less undernourished and estate sector children are more undernourished (Models 1, 7 and 9). However, with respect to the prevalence of wasting, estate sector performs better than the other two sectors, where the prevalence of wasting is lower than the other two sectors. The results further suggest that all the sectors have been able to curtail the high prevalence rate of undernutrition, though the reduction is impressive in the estate sector as compared to other two sectors (Models 2–4).
High prevalence rate of malnutrition is associated with income quartile. As compared to the rate of child malnutrition in the first four income quartile, the rate of child malnutrition in the fifth income quartile is low. Though statistically insignificant at 10% level, the prevalence rate in the third and fourth income quartiles is low compared to the bottom two quintiles. The difference was statistically significant at 5% level only for the prevalence of wasting and underweight and not significant for stunting and overweight. Moreover, child malnutrition is inversely associated with the mother’s education level. The children who are born to mothers with no education or only with primary education are at a higher risk of being stunted or underweight, whereas children born to mothers who have completed school education or with higher education qualifications are at a lower risk. The association is not significant at 10% level for wasting and overweight. Similarly, it was found that children less than 6 months old are at a lower risk of being stunted or wasted and higher risk of being underweight, compared to other age groups. In contrast to this, children above the age of 1 and less than 2 have a higher risk of being stunted and wasted. This reinforces the finding, which implies better care at first few months and improper introduction of complementary food at the age of 1. Indicating the double burden of malnutrition, children between the ages of 6 months and 2 years show a higher risk of being overweight. One of the salient finding of this study is that none of the estimated models provide empirical evidence for the presence of gender inequality of malnutrition.
2.6 Summary, Conclusions, and Way Forward
2.6.1 Summary and Conclusions
Based on the findings of the previous section, this review assessed the degree of nutrition transition in Sri Lanka. As stated in Sect. 5, over these years, Sri Lankan diet has transformed toward more animal-based products as compared to cereal-based monotonous diet consume in the past. However, still the share of food of animal origin to total intake of calorie, protein, and fat remains relatively small in Sri Lanka. These facts suggest that Sri Lanka has not reached the fourth stage of the nutrition transition in which the diet includes more fat that comes from animal products. The consumption of sugar and salt also has increased in Sri Lanka to a far high level to be classified into the third stage of the nutrition transition.
Considering the regional disparities in food consumption, in some geographical locations in the country, still the consumption of products of animal origin remains low while the consumption of cereal-based products is high. Contrast to this in urban areas, consumption of cereal-based products has declined in favor of products of animal origin. Thus, it can infer that even though the stage of nutrition transition Sri Lanka is not clear, in terms of diet transformation, certain geographical communities (e.g., estate sector) are still at the food insecurity stageFootnote 1, while urban communities are at the Degenerative disease stage.
The national-level statistics on undernutrition and overnutrition among preschool children and adult women are used in this review in the absence of those for overnutrition and undernutrition of the whole population. Accordingly, it was found that child malnutrition has declined in Sri Lanka, and in some geographical subgroups (children in the estate sector) it has declined by leaps and bounds. This reduction in undernutrition in the estate sector has been accompanied by reduction in anemia status as well. This reduction of nutritional deficiencies is a characteristic of a receding famine stage. Though the estate sector was the most vulnerable sector to food insecurity four decades ago, this result provides strong evidence for an existence of a nutrition transition from the famine stage (food insecurity) to the “receding famine stage.”
The proportion of preschool children who are undernourished is higher than the proportion of preschool children who are overweight. However, in some geographical sub-groups in Colombo in the western province, overweight among school children is higher than that of undernourished implying that these communities (urban has already shifted to the stage 4 of the nutrition transition) are at different stages of nutrition transition.
The incidence of overweight and obesity among Sri Lankan adults are higher than South Asian average and almost same as the world average. As the DHS (2006/2007, 2016) indicates, overweight among women has increased over a 10-year period, the prevalence is higher among urban dwellers than the rest. By 2016, the major nutritional problem faced by women is overweight. This high prevalence rate of overweight among adult is one of the characteristics of the stage 4 of the nutrition transition (Degenerative disease). However, in the estate sector, the prevalence of thinness among adults is higher than the prevalence of overweight. Thus, it is obvious that estate sector has not reached the fourth stage of the nutrition transition process.
The burden of NCDs has increased in Sri Lanka. Hospitalization due to diabetes mellitus, hypertensive disease, and ischemic heart disease has more than doubled during the last three decades (MoH 2011, Ministry of Health, Nutrition and Indigenous Medicine 2017). Around 70% of the disease burden in Sri Lanka is due to NCDs. Nearly 30% of the total hospital deaths are due to cardiovascular diseases, which are the first leading cause of death in Sri Lanka for the past few years (WHO 2015). The hospitalization for NCDs has accelerated after 1990, while those due to infectious diseases has rapidly declined after 1990 (DCS 2009).
In summary, it is evident that Sri Lanka on average has swung between stages 3 and 4 of the nutrition transition, while some communities have already shifted to stage, some others are still struggling to move away from the third stage. It can be concluded that Sri Lanka, as in many developing countries, experiences the duel burden of malnutrition characterized by coexisting undernutrition and overnutrition.
2.6.2 Way Forward
This review witnessed a nutrition transition in Sri Lanka similar to many developing and transitional economics where both undernutrition and overnutrition coexist. Poverty, low maternal nutritional status, and lack of maternal knowledge on nutrition hinder the success of alleviating malnutrition despite several attempts taken to combat the epidemics of undernutrition and micronutrient deficiencies among children and pregnant mothers in the country. Urbanization, change in food consumption pattern, and physical inactivity may have contributed to the emerging problem of overnutrition.
The findings from this review have important policy implications on several areas such as agriculture, nutrition and health, and education. Food policies, agricultural policies, and nutrition policies need to be integrated to combat the triple burden of malnutrition in Sri Lanka. Agricultural policies should be reoriented to diversify farm-level production. The existing policy framework of the country incentivizes paddy production at the expense of high-value agricultural products. To this end, the current land policy, which bans the use of paddy land for cultivation of other crops, could be relaxed. Agriculture research policies need to be directed to explore the possible ways of improving nutritive values of crop and animal-sourced food in addition to yield improvements.
Food policies of the country, government taxes, and subsides need to be reformulated to make nutritious food more affordable. Import taxes can be charged on unhealthy food item (i.e., energy dense and/or junk foods) to make them less affordable to the consumers. Legislations are required to transform the food processing industry to depict sugar and salt contents in processed foods through compulsory labeling requirements. Along with such changes, reformations in consumption pattern are required through attitudinal changes. Public awareness through campaigns on the food-based dietary guidelines is required. School children need to be educated and regulatory measures should be imposed on sales of food items within school premises.
As stated before, though there have been many attempts to combat undernutrition and micronutrient deficiencies, the need to prevent the rising tide of overnutrition has not been adequately emphasized in Sri Lanka. Thus, it is necessary to introduce programs and policies to curtail the rising epidemic of overnutrition in the country at this early phase.
More research is needed to provide more scientific evidence for in-depth understanding of the prevalence of malnutrition in Sri Lanka. As evident from the review, prevalence of certain forms of malnutrition is higher in certain communities. The studies conducted so far provide no evidence to explain such patterns. More research is needed to understand the determinants of multiple forms of malnutrition and their interconnections over the lifecycle. Further research is needed to synthesize the trends in physical activity and NCDs and their association with food consumption behavior and demographic changes in the society, which has not been covered in this review.
Given the trends in the nutritional outcomes, a sound national monitoring program to record the health and nutritional data of citizens of all age groups will be required to track the improvements in health and nutritional status.
Notes
- 1.
This condition mimics the stage as defined by Popkin (1999)
References
Allen A, Allen S, Rodrigo R, Perera L, Shao W, Li C, Premawardhena A (2017) Iron status and anaemia in Sri Lankan secondary school children: a cross-sectional survey. PLoS One 12(11):e0188110
Amarasinghe GS, Naottunna NPGCR, Agampodi TC, Agampodi SB (2017) Factors associated with anemia among Sri Lankan primary school children in rural North Central Province. BMC Pediatr 17(1):87
Arambepola C, Allender S, Ekanayake R, Fernando D (2008) Urban living and obesity: is it independent of its population and lifestyle characteristics? Trop Med Int Health 13(4):448–457
Baker P, Friel S (2014) Processed foods and the nutrition transition: evidence from Asia. Obes Rev 15(7):564–577
Bandara S, Weerasinghe MC (2015) Health and socio-economic determinants of malnutrition in the plantation sector of Sri Lanka: a review, Working Paper Series No. 21. Institute of Policy Studies of Sri Lanka, Colombo
Bell AC, Ge K, Popkin BM (2001) Weight gain and its predictors in Chinese adults. Int J Obes 25(7):1079
Bhalla S (1991) Sri Lanka. In: Krueger AO, Schiff M, Valdes A (eds) The political economy of agricultural pricing policy, volume 2: Asia. Johns Hopkins, Baltimore, MD, pp 195–235
Bhargava A, Jamison DT, Lau LJ, Murray CJ (2001) Modeling the effects of health on economic growth. J Health Econ 20(3):423–440
Bloom DE, Canning D, Sevilla J (2004) The effect of health on economic growth: a production function approach. World Dev 32(1):1–13
Bogahawatte C, Kailasapathy K (1986) The consumption patterns of food in Sri Lanka with special reference to protein-calorie nutrition. Agric Syst 22(4):289–303
Burroway R (2017) Are all jobs created equal? A cross-national analysis of women’s employment and child malnutrition in developing countries. Soc Sci Res 67:1–13
Central Bank (2017) Annual report, 2017. Central Bank, Colombo
Chathurani U, Dharshika I, Galgamuwa D, Wickramasinghe ND, Agampodi TC, Agampodi SB (2012) Anaemia in pregnancy in the district of Anuradhapura, Sri Lanka—need for updating prevalence data and screening strategies. Ceylon Med J 57(3):101–106
DCS (2002) Sri Lanka demographic and health survey 2000. Department of Census and Statistics in Collaboration with Ministry of Health, Nutrition and Welfare, Colombo
DCS (2009). Sri Lanka demographic and health survey 2006–07, Colombo: Department of Census and Statistics. http://www.statistics.gov.lk/samplesurvey/LFS_Annual%20Report_2016.pdf. Accessed 24 Jun 2018
DCS (2017) Sri Lanka demographic and health survey 2016. Department of Census and Statistics, Colombo
DCS (2018) Sri Lanka labour force survey annual report 2017. Department of Census and Statistics, Colombo
Department of Census and Statistics (1988) Sri Lanka demographic and health survey 1987. Ministry of Plan Implementation, Colombo
Department of Census and Statistics (1995) Sri Lanka demographic and health survey 1993. Department of Census and Statistics, Colombo
Department of Census and Statistics (2000) Sri Lanka demographic and health survey 2000. Department of Census and Statistics, Colombo
Department of Census and Statistics (2007) Sri Lanka demographic and health survey 2006–2007. Department of Census and Statistics, Colombo
Department of Census and Statistics (2016) Sri Lanka demographic and health survey 2016. Department of Census and Statistics, Colombo
De Silva K, Liyanage C, Wijesinghe C, Perera B (2017) Nutritional status of elders in Galle district, Sri Lanka. Galle Med J 22(1):1–5
Drewnowski A, Specter SE (2004) Poverty and obesity: the role of energy density and energy costs. Am J Clin Nutr 79(1):6–16
Edirisinghe N (1987) The food stamp scheme in Sri Lanka: costs, benefits, and options for modification, vol 58. International Food Policy Research Institute, Washington, DC
Ekanayake S, Weerahewa J, Ariyawardana A (2003) Role of mothers in alleviating child malnutrition: evidence from Sri Lanka. In: Research report presented at the 3rd Poverty and Economic Policy (PEP), 16-20th June 2004, pp 1–20
Ellis F, Senanayake P, Smith M (1997) Food price policy in Sri Lanka. Food Policy 22(1):81–96
Ellis P, Roberts M (2015) Leveraging urbanization in South Asia: managing spatial transformation for prosperity and livability. The World Bank
Family Health Bureau (2011). Annual Report 2010, Family Health Bureau, Ministry of Health, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=com_phocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
Family Health Bureau (2012) Annual Report 2011, Family Health Bureau, Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=com_phocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
Family Health Bureau (2013). Annual Report 2012, Family Health Bureau, Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=com_phocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
Family Health Bureau (2014) Annual Report 2013, Family Health Bureau, Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=com_phocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
Family Health Bureau (2015) Annual Report 2014, Family Health Bureau, Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=comphocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
Family Health Bureau (2016) Annual Report 2015, Family Health Bureau, Ministry of Health, Nutrition and Indigenous Medicine, Sri Lanka. http://fhb.health.gov.lk/web/index.php?option=com_phocadownload&view=category&id=66:annual-reports&itemid=150&lang=en. Accessed 24 Jul 2018
FAO (2010) The state of food insecurity in the world 2004. Available at http://www.fao.org/3/y5650e/y5650e00.pdf
FAO (2016) City region food system situation analysis. Colombo, Sri Lanka. Working document
Fernando DJ, Siribaddana SH, Silva DR, Perera SD (1994) The prevalence of obesity and other coronary risk factors in a suburban Sri Lankan community. Asia Pac J Clin Nutr 3(4):155–159
Fernando WHKN, Wijesinghe DGNG (2010) Assessment of nutritional status and disease prevalence among elderly population in elderly homes in Kandy. Tropic Agri Res 21(3):229–237
FHB (2008) Family health bureau- annual report 2007. Ministry of Health, Colombo
FHB (2009) Family health bureau- annual report 2008. Ministry of Health, Colombo
FHB (2010) Family Health Bureau- Annual Report 2009. Ministry of Health, Colombo
FHB (2015) School health return. Family Health Bureau, Ministry of Health, Colombo
Gavan JD, Chandrasekera IS (1979) The impact of public food grain distribution on food consumption and welfare in Sri Lanka (No. 13). International Food Policy Research Institute, Washington, DC
Glewwe P (1999) Why does mother’s schooling raise child health in developing countries? Evidence from Morocco. J Hum Resour:124–159
Hartwig J (2010) Is health capital formation good for long-term economic growth?—Panel Granger-causality evidence for OECD countries. J Macroecon 32(1):314–325
Hawkes C, Fanzo J (2017) Nourishing the SDGs: Global nutrition report 2017. Development Initiatives, Bristol. Available from https://openaccess.city.ac.uk/id/eprint/19322. Accessed 11 Nov 1999
Hettiarachchi M, Liyanage C, Wickremasinghe R, Hilmers DC, Abrams SA (2006) Prevalence and severity of micronutrient deficiency: a cross-sectional study among adolescents in Sri Lanka. Asia Pac J Clin Nutr 15(1):56
Jayasekera CR (2006) Nutritional status of children under five in three state foster care institutions in Sri Lanka. Ceylon Med J 51:63–65
Jayathilaka R, Selvanathan S, Bandaralage JS (2016) Is there a link between alcohol consumption and the level of poverty? Appl Econ 48(22):2054–2063
Jayathissa R, Mahamithawa S, Ranbanda JM (2002) Nutritional problems among Sri Lankan primary schoolchildren aged 5–9 years. Department of Nutrition, Medical Research Institute. Colombo, Sri Lanka
Jayatissa R (2009) Micronutrient deficiencies in Sri Lanka–Are we on track? Presentation made at National fortification meeting. https://www.researchgate.net/profile/Renuka_Jayatissa/publication/280659815_Micronutrient_Deficiencies_in_Sri_Lanka_-_Are_we_on_Track/links/55c0e28608aed621de150343/Micronutrient-Deficiencies-in-Sri-Lanka-Are-we-on-Track.pdf. Accessed 11 Nov 2019
Jayatissa R, Bekele A, Kethiswaran A, De Silva AH (2012a) Community-based management of severe and moderate acute malnutrition during emergencies in Sri Lanka: challenges of implementation. Food Nutr Bull 33(4):251–260
Jayatissa R, Gunathilaka MM, Fernando DN (2012b) Anaemia among children aged 6–59 month. National nutrition and micronutrient survey. Part I. Ministry of Health and United Nations International Children’s Emergency Fund UNICEF, Colombo
Jayatissa R, Hossain SM, Gunawardana S, Ranbanda JM, Gunathilaka M, De Silva PC (2012c) Prevalence and associations of overweight among adult women in Sri Lanka: a national survey. Sri Lanka J Diabet Endocrinol Metab 2(2):61–68
Jayatissa R, Ranbanda RM (2006) Prevalence of challenging nutritional problems among adolescents in Sri Lanka. Food Nutr Bull 27(2):153–160
Jayatissa R, Hossaine SMM (2010) Nutrition and food security assessment in Sri Lanka 2009. Medical Research Institute, United Nations International Children’s Emergency Fund (UNICEF)[T1] and World Food Programme, Colombo
Jayatissa R, Wickramage K (2016) What effect does international migration have on the nutritional status and child care practices of children left behind? Int J Environ Res Public Health 13(2):218
Jayawardana NWIA, Jayalath WATA, Madhujith WMT, Ralapanawa U, Jayasekera RS, Alagiyawanna SASB, Kalupahana NS (2017) Lifestyle factors associated with obesity in a cohort of males in the central province of Sri Lanka: a cross-sectional descriptive study. BMC Public Health 17(1):27
Jayawardena P (2012) Socio-economic determinants and inequalities in childhood malnutrition in Sri Lanka. Well-Being Soc Policy J 8(1):1–22
Jayawardena P (2014) Underlying causes of child and maternal malnutrition in the estate sector of Sri Lanka. J South Asian Stud 2(3):241–255
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP (2012) The obesity epidemic in Sri Lanka revisited. Asia Pacific J Public Health 27(2):NP1298–NP1299
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Hills AP (2013a) Food consumption of Sri Lankan adults: an appraisal of serving characteristics. Public Health Nutr 16(4):653–658
Jayawardena R, Byrne NM, Soares MJ, Katulanda P, Yadav B, Hills AP (2013b) High dietary diversity is associated with obesity in Sri Lankan adults: an evaluation of three dietary scores. BMC Public Health 13(1):314
Jayawardena R, Punchihewa P, Ranathunga I, Lokunarangoda N, Pathirana AK, Santharaj WS (2016) Body weight perception among Sri Lankan cardiac patients. BMC Obes 3(1):32
Johnston D, Stevano S, Malapit HJ, Hull E, Kadiyala S (2018) Time use as an explanation for the agri-nutrition disconnect? Evidence from rural areas in low and middle income countries. Food Policy 76:8–18
Kandeepan K, Balakumar S, Arasaratnam V (2016) Nutritional status and food insecurity among the children in northern Sri Lanka. Procedia Food Sci 6:220–224
Katulanda P, Jayawardena MAR, Sheriff MHR, Constantine GR, Matthews DR (2010) Prevalence of overweight and obesity in Sri Lankan adults. Obes Rev 11(11):751–756
Lee MJ, Popkin BM, Kim S (2002) The unique aspects of the nutrition transition in South Korea: the retention of healthful elements in their traditional diet. Public Health Nutr 5(1a):197–203
Malkanthi RLDK, Chandrasekera GAP, Jayasinghe JMUK (2007) High prevalence of malnutrition and household food insecurity in the rural subsistence Paddy farming sector. Trop Agri Res 19:136–149
Ministry of Health (2017) Annual health bulletin. Ministry of Health, Nutrition and Indigenous Medicine, Colombo
MoH (2011) Non-communicable disease status Sri Lanka. Ministry of Health, Colombo
Mudalige R, Nestel P (1996) Combating iron deficiency. Ceylon J Med Sci 39(1):9–16
Nanayakkara GJM, Silva KDRR (2011) Association among maternal nutrition, birth characteristics, feeding practices, nutritional status and body composition of term infants. The Proceedings of the Nutrition Society, 70(OCE4)
Naotunna NPGCR, Dayarathna M, Maheshi H, Amarasinghe GS, Kithmini VS, Rathnayaka M, Agampodi TC (2017) Nutritional status among primary school children in rural Sri Lanka; a public health challenge for a country with high child health standards. BMC Public Health 17(1):57
Narayan S, Narayan PK, Mishra S (2010) Investigating the relationship between health and economic growth: empirical evidence from a panel of 5 Asian countries. J Asian Econ 21(4):404–411
Pathmeswaran A, Jayatissa R, Samarasinghe S, Fernando A, De Silva RP, Thattil RO, De Silva NR (2005) Health status of primary schoolchildren in SriLanka. Ceylon Med J 50(2):46–50
Peiris TDR, Wijesinghe DJGNG (2011) Nutritional status of under 5 year-old children and its relationship with maternal nutrition knowledge in Weeraketiya DS division of Sri Lanka. Trop Agric Res 21(4):330–339
Perera R, Ekanayake L (2012) Relationship between nutritional status and tooth loss in an older population from Sri Lanka. Gerodontology 29(2):566–570
Perkins JM, Jayatissa R, Subramanian SV (2018) Assessment of nutritional status and disease prevalence among elderly population in elderly homes in Kandy. Nutrition 55–56:76–83
Piyasena C, Mahamithawa AMASB (2003) Assessment of anaemia status in Sri Lanka 2001 [survey report]. Ministry of Health, Nutrition and Welfare, Department of Health Services, Medical Research Institute, Colombo, pp 40–46
Popkin BM (1994) The nutrition transition in low-income countries: an emerging crisis. Nutr Rev 52(9):285–298
Popkin BM (1998) The nutrition transition and its health implications in lower-income countries. Public Health Nutr 1(1):5–21
Popkin BM (1999) Urbanization, lifestyle changes and the nutrition transition. World Dev 27(11):1905–1916
Popkin BM (2001) The nutrition transition and obesity in the developing world. J Nutr 131(3):871S–873S
Popkin BM (2002) The shift in stages of the nutrition transition in the developing world differs from past experiences. Public Health Nutr 5(1A):205–214
Popkin BM (2003) The nutrition transition in the developing world. Develop Policy Rev 21(5–6):581–597
Popkin BM (2004) The nutrition transition: an overview of world patterns of change. Nutr Rev 62(suppl 2):S140–S143
Prasanna IWK (2015) Nutritional status of preschool children and its associates: a Sri Lankan experience of a fishing community. Eur J Prevent Med 3(2–1):31–35
Rajapaksa LC, Arambepola C, Gunawardena N, Rosa C, Opatha S (2011) Nutritional status in Sri Lanka, determinants and interventions: a desk review. UNICEF, Colombo
Ranis G, Stewart F, Ramirez A (2000) Economic growth and human development. World Dev 28(2):197–219
Rannan-Eliya RP, Hossain SMM, Anuranga C, Wickramasinghe R, Jayatissa R, Abeykoon ATPL (2013) Trends and determinants of childhood stunting and underweight in Sri Lanka. Ceylon Med J 58(1):10–18
Rathnayake IM, Weerahewa J (2005a) Maternal employment and income affect dietary calorie adequacy in households in Sri Lanka. Food Nutr Bull 26(2):222–229
Rathnayake IM, Weerahewa J (2005b) Determinants of nutritional status among pre-school children in Sri Lanka. Trop Agri Res 17:148–161
Rathnayake KM, Roopasingam T, Dibley MJ (2014a) High carbohydrate diet and physical inactivity associated with central obesity among premenopausal housewives in Sri Lanka. BMC Res Notes 7(1):564
Rathnayake KM, Roopasingam T, Wickramasighe VP (2014b) Nutritional and behavioral determinants of adolescent obesity: a case–control study in Sri Lanka. BMC Public Health 14(1):1291
Rathnayake KM, Wimalathunga MPPM, Weech M, Jackson KG, Lovegrove JA (2015) High prevalence of undernutrition and low dietary diversity in institutionalised elderly living in Sri Lanka. Public Health Nutr 18(15):2874–2880
Sahn DE (1988) The effect of price and income changes on food-energy intake in Sri Lanka. Econ Dev Cult Chang 36(2):315–340
Sahn DE, Alderman H (1988) The effects of human capital on wages, and the determinants of labor supply in a developing country. J Dev Econ 29(2):157–183
Senadheera D, Goonewardene M, Mampitiya I (2017) Anaemia and iron deficiency in pregnant women attending an antenatal clinic in a Teaching Hospital in Southern Sri Lanka. Ceylon Med J 62(3):175–183
Shekar M, Somanathan A, Du L (2007) Malnutrition in Sri Lanka: scale, scope, causes, and potential response. World Bank report. Report No. 40906-LK. World Bank, Washington, DC
Smith LC, Haddad L (2002) How potent is economic growth in reducing undernutrition? What are the pathways of impact? New cross-country evidence. Econ Dev Cult Chang 51(1):55–76
Strauss J, Thomas D (1998) Health, nutrition, and economic development. J Econ Lit 36(2):766–817
Suri T, Boozer MA, Ranis G, Stewart F (2011) Paths to success: the relationship between human development and economic growth. World Dev 39(4):506–522
Thamilini J, Silva KDRR, Jayasinghe JMUK (2015) Prevalence of stunting among pre-school children in food insecure rural households in Sri Lanka. Trop Agri Res 26(2):390–394
Thilakarathne RMLR, Wijesinghe DGNG (2011) Association between nutritional status and life style practices of primary school children in the Colombo District: a pilot study. Trop Agri Res 22(4):392–401
Ubeysekara NH, Jayathissa R, Wijesinghe CJ (2015) Nutritional status and associated feeding practices among children aged 6-24 months in a selected community in Sri Lanka: a cross sectional study. Eur J Prevent Med 3(2–1):15–23
Weerahewa J, Korale-Gedara PK, Kanthilanka H (2017) The evolution of food policy in Sri Lanka: 1948-2017. Reference Module in Food Sciences, pp 1–19
Weerahewa J, Korale-Gedara P, Wijetunga CS (2018b) Nutrition transition in Sri Lanka: a diagnosis. Ann Nutr Food Sci 2(2):1020
Weerahewa J, Wijetunga CS, Babu SC, Atapattu N (2018a) Food policies and nutrition transition in Sri Lanka: historical trends, political regimes, and options for interventions. IFPRI Discussion Paper 1727. International Food Policy Research Institute (IFPRI), Washington, DC. http://ebrary.ifpri.org/cdm/ref/collection/p15738coll2/id/132683. Accessed 24 Jul 2018
Well DN (2007) Accounting for the effect of health on economic growth. Q J Econ 122(3):1265–1306
WHO (2012) Report of expert meeting on population sodium reduction strategies for prevention and control of non-communicable diseases in the South Asian region. World Health Organization (WHO), Geneva
WHO (2015) Non-communicable disease country profile. World Health Organization (WHO), Geneva. http://apps.who.int/iris/bitstream/handle/10665/128038/9789241507509_eng.pdf;jsessionid=FAF005500BC47F41343C767CC74284DF?sequence=1. Accessed 24 Jul 2018
Wijesekere G (2015) Changing patterns of food consumption in Sri Lanka: 1985–2009. The Australian National University, Australia South Asia Research Centre, Canberra
Wisniewski SL (2010) Child nutrition, health problems, and school achievement in Sri Lanka. World Dev 38(3):315–332
World Bank (2018) World Bank Open Data. https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS. Accessed 24 Jul 2018
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Weerahewa, J., Korale-Gedara, P., Wijetunga, C.S. (2020). Nutrition Transition in Sri Lanka: A Meta-Analysis of the Nutrition Profile. In: Marambe, B., Weerahewa, J., Dandeniya, W. (eds) Agricultural Research for Sustainable Food Systems in Sri Lanka. Springer, Singapore. https://doi.org/10.1007/978-981-15-2152-2_2
Download citation
DOI: https://doi.org/10.1007/978-981-15-2152-2_2
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-2151-5
Online ISBN: 978-981-15-2152-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)