
Abstract
Using data from the National Family Health Survey (NFHS) of India, the authors examine the impact of fertility gap on child nutritional outcomes, focused on whether a child is stunted, wasted or anemic. They find that the odds of having malnourished children who are stunted, wasted or anemic are higher for women who exceed their fertility target compared to those who have achieved or underachieved it. The authors build on the literature that has emphasized the importance of lower fertility on development, and thus calls for policies that are aimed at achieving this.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

1 Introduction
Fertility decisions have long been associated with human capitalaccumulation, which is a main driver of economic growth (Barro & Becker, 1989; Becker, Murphy, & Tamura, 1990). Consequently, economic development has been accompanied by significant declines in fertility, a phenomenon referred to as the demographictransition (Doepke & Tertilt, 2018). Beyond studies that examine the role of fertility in economic growth (see, e.g., Ashraf, Weil, & Wilde, 2013; Brander & Dowrick, 1994; Wang, Yip, & Scotese, 1994), a large body of literature examines various aspects of fertility given that fertility is considered an important factor in the development process. Along these lines, economists and demographers have expressed interest in understanding the determinants and effects of fertility rates. This interest has led to a large body of literature that examines such factors as education (e.g., Kravdal, 2002; Rindfuss, Morgan, & Offutt, 1996), urbanization (e.g., Gries & Grundmann, 2018; Guo, Wu, Schimmele, & Li, 2012), culture, religion and peer effect (e.g., Khan & Raeside, 1997; McQuillan, 2004; Mishra & Parasnis, 2017), income (e.g., Herzer, Strulik, & Vollmer, 2012; Klawon & Tiefenthaler, 2001) and labor market choices (e.g., Hondroyiannis, 2010), among others as determinants of fertility.
Another strand of literature examines the effects fertility on such development outcomes as education (e.g., Becker, Cinnirella, & Woessmann, 2010; Lloyd & Gage-Brandon, 1994), wellbeing (e.g., Cáceres-Delpiano & Simonsen, 2012; Kohler, Behrman, & Skytthe, 2005; Schultz, 2005) and labor force participation (e.g., Chun & Oh, 2002), among others. This chapter contributes to this body of literature by examining the impact of fertility gap on child nutrition in India. We examine the relationship between two important variables that are relevant for development and consequential in the development process. Fertility gap is the difference between a woman’s preferred number of children and her actual number of children. The decisions on how many children to have are among the most consequential in developing countries, and, in this study, we hypothesize the potential effects of these decisions on child nutrition. Child nutrition represents an important development agenda and has been identified as a major global priority over the past two decades. Child nutrition first formed part of the recently ended millennium development goals (MDGs) and has continued to remain a global priority on the post-2015 development agenda. Thus, understanding factors that influence this development goal is important.
India makes for an important case study to examine the impact of the fertility gap on child nutrition for several reasons. First, India introduced a nationalfamily planning program in the 1950s, making it one of the first countries in the world to introduce such a program on a national scale. The initiation of this program, coupled with several other fertility-related changes across Indian states over the years, has led to persistent demographictransitions characterized by declining fertility and mortality rates (Drèze & Murthi, 2001). Since the 1980s, India’s fertility rate has halved with the current rate recorded at 2.3 per woman. This figure of 2.3 represents a decline of more than 50% in the fertility rate of approximately 5 recorded in the late 1970s to early 1980s. This fertility trend has been argued to defy prevailing trends of developing countries especially given that such low fertility rates are only achieved at higher levels of income and economic growth in other parts of the world (UNPF, 2018).
Second, evidence suggests that the fertility gap in India has been persistent. In an analysis based on the National Family Health Survey (NFHS), Mishra and Parasnis (2018) show that for the period 2005–2006, there is evidence of a fertility gap in India and this gap has remained persistent for over a decade for most women.
Third, the incidence of malnutrition in India is very high. According to statistics from the United Nations Children’s Fund (UNICEF), one in five children (approximately 20%) of children under the age of five in India suffer from acute undernutrition and 48% of them suffer from chronic undernutrition. More than 40% of children in India under the age of the five are underweight and over 30% of the world’s children who suffer from acute undernutrition or are wasted live in India. Similarly, India accounts for more than 30% of stunted children in the world.
Using data from the fourth wave of the National Family Health Survey (NFHS-4) of India, we measure the fertility gap as a dummy variable taking the value 1 if a woman exceeds her fertility target and 0 otherwise. The outcome variable, child nutrition, also takes the form of binary variable taking the value 1 if a woman has at least one child who is stunted/wasted/anemic and 0 otherwise. By focusing on these three measures, and particularly on stunted and wasted children, our study captures chronic and acute cases of malnutrition, respectively. Our results suggest that the odds of having malnourished children who are stunted, wasted or anemic are higher for women who exceed their fertility target compared to those who have achieved or underachieved it. These results are consistent with the literature that has emphasized the importance of lower fertilityrate on development outcomes, and thus lends support to the need for policies that promote lower fertility rates.
While our empirical evidence is for India, similar fertility trends across developing countries suggest that our findings have relevance for other developing countries as well. Across both developed and developing countries, children have been used as instruments to secure support of parents in old age. This phenomenon, referred to in the literature as the old-age security hypothesis (Caldwell, 1976; Neher, 1971), proposes that an important reason behind fertility decision or parents’ choice of having many children is the transfer from children to parents. Since Neher (1971) and Caldwell (1976), several authors have theoretically and empirically explored and validated the old-age security hypothesis and its role in shaping fertility decisions (Bental, 1989; Nugent, 1985; Zhang & Nishimura, 1993). Despite the benefits of fertility as proposed by the old-age security hypothesis, it is important to also bring into purview the potential negative effects on outcomes such as child nutrition. Fertility thus may generate costs or benefits for society, and this may either be captured through direct impacts within a family or significant externality that influence the welfare of society in general (Schultz, 2005). Our findings thus prompt policymakers on the need to take a more holistic perspective on the effects of fertility when devising policy.
2 Related Literature
Very limited literature exists on the fertility gap, especially on developing countries because of data availability issues. Several studies, however, examine lifetime fertility intentions, completed fertility and the estimated gap between them using European and North American data. Studies on the United Kingdom (e.g., Berrington & Pattaro, 2014; Smallwood & Jefferies, 2003), the United States (e.g., Freedman, Freedman, & Thornton, 1980; Morgan & Rackin, 2010) and Norway (e.g., Noack & Østby, 2002) have found evidence suggesting that couples tend to have fewer children than planned with a persisting gap.
In the United Kingdom, Smallwood and Jefferies (2003) show a gap of 0.2–0.3 birth per woman for birth intentions between ages 21 and 23 and actual birth, for birth cohorts 1957 to 1959. In the United States, an earlier study by Freedman et al. (1980) showed that the gap was one child per woman for women who were first interviewed in early adulthood in 1962, while Morgan and Rackin (2010), on the other hand, show that the gap between birth intentions at the age of 24 and actual birth was 0.25 per woman for birth cohorts 1957–1964. In Norway, Noack and Østby (2002) demonstrated a fertility gap of 0.3 identifying that women aged between 20 and 24 (birth cohorts 1953–1957) intended to have an average of 2.4 children, but ended up with an average of 2.1 actual births by their 40s.
In a more recent study, Beaujouan and Berghammer (2019) examine the aggregate fertility gap between intended and actual fertility in 19 European countries and the United States. They focus on women aged between 20 and 24 who were born in the early 1970s. They find that the fertility gap is widest in German-speaking countries and Southern European countries, but smallest in Central and Eastern European countries. Further analysis which takes into account educational level suggests that in most countries, the fertility gap is largest among highly educated women. This finding is consistent with previous studies that examine how fertility intentions and their realization differ by education attainment. This body of literature suggest that the fertility gap widens with education (Berrington & Pattaro, 2014), and compared to their less educated counterparts, highly educated women tend to reach smaller completed family sizes. This pattern is more apparent in Central and Eastern European countries and states such as Austria, Germany, Spain and Italy, where families receive little institutional support to take for their citizens (Beaujouan & Berghammer, 2019; Neyer & Hoem, 2008).
The only study on fertility gap that focuses on a developing country, of which we are aware, is Mishra and Parasnis (2018). They examine the fertility gap distribution in India and factors that could explain trends in this gap. Their results suggest that the preference for sons as influenced by Indian culture plays an important role in influencing the actual number of family, and by extension contributes to the trends in fertility gap.
This chapter contributes to the discourse on fertility gap in India but deviates from Mishra and Parasnis (2018) in that we do not seek to understand factors influencing the fertility gap in India, but we examine the role of fertility gap in shaping development outcomes, specifically child nutrition. In this regard, we contribute to the rather limited literature on the impact of fertility gap, and more narrowly the literature on the interplay between fertility, fertility choices and child nutrition (e.g., Blau, 1984, 1986; Horton, 1986).
3 Data and Estimation Strategy
3.1 Data and Variables
We use data from the National Family Health Survey (NFHS) conducted by the International Institute for Population Sciences (IIPS) under the Ministry of Health and Family Welfare (MOHFW), Government of India. This large-scale, multi-round survey is conducted in a representative sample of households throughout India. We employ the latest round: NFHS 4, conducted in 2015–2016. While the survey covers all 29 states of India, we include 17 states in this present analysis.Footnote 1 The survey provides detailed information on fertility for women aged 15–49. We restrict our sample to those women who have at least one child below the age of 5 years as information on nutritional parameters of children used in this study is only available for children below 5 years of age. Using this restricted sample and removing other outliers, we are left with a working sample of 138,009 women nationally, out of which 29,972 (21.7%) reported negative fertility gap (exceeding the desired number of children) and the remaining 108,037 (78.3%) reported ‘no to positive fertility gap’ (achieving or underachieving the desired number of children).
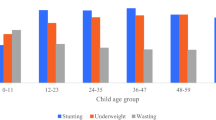
Our outcome variable captures the nutritional status of children who are in the age group of 0 to 5 years. The nutritional status is measured by one long term (i.e., stunted or not) and two short term (wasted or not, and anemic or not) health parameters. A child is considered ‘stunted’ if his/her ‘height for age’ z-score is below 2 standard deviations from the reference median as prescribed by World Health Organization (WHO hereafter); ‘wasted’ if his/her ‘weight for age’ z-score is below 2 standard deviations from the reference median as prescribed by WHO; and ‘anemic’ if a child suffers from ‘severe’ to ‘moderate’ anemia. Information on these variables is directly available in NFHS-4.
The main explanatory variable is fertility gap, defined as the difference between a woman’s ideal number of children and her actual number of children. A woman is said to have a (1) negative fertility gap if she exceeds her ideal family size, (2) positive, if she does not achieve her desired number of children and (3) zero fertility gap if the actual number of children is equal to her stated ideal. We work with the underlying hypothesis that women who have more children than desired may face greater constraints on their time as well as material and health resources, thus, resulting in poorer health outcomes for the children. To test this hypothesis, our measure of fertility gap takes the form of a dummy variable that takes the value 0 for women with no (i.e., achieved the ideal number of children) or positive fertility gap (i.e., has fewer children than ideal), and 1 for women with negative fertility gap (i.e., have more children than desired).
We control for potential factors that are likely to influence child nutrition outcomes. These control variables include mother’s age and years of education, religion (i.e., dummy variable equals to one if respondent is Hindu and zero if otherwise), economic status, location (rural vs. urban), and health status (i.e., Body Mass Index (BMI) and anemic status).
3.2 Empirical Strategy
We estimate an empirical equation of the form:
Here, outcome variable \( \left({Y}_i\right) \) is a binary variable, which takes the value 0 if a woman has no stunted/wasted/anemic children below the age of 5 years and 1 if woman has at least one child who is stunted/wasted/anaemic. \( {F}_i \) is the main explanatory variable, representing the fertility gap outcome for woman \( i \) as explained above. \( {X}_i \) is a set of control variables capturing individual characteristics. We also control for geographical (or regional) fixed effects. \( {e}_i \) is an error term.
Given that our outcome variable is binary in nature, we use logistic regression to estimate the equation above.
4 Empirical Results
4.1 Summary Statistics
Table 5.1 reports the mean values for the control variables by fertility gap status. These summary statistics reveal that there are significant differences in mothers’ characteristics between the two sub-groups. Compared to women with negative fertility gaps, women with positive or no fertility gap are approximately 4 years younger, and have, on average, 3 more years of education. We also observe some significant economic and locational differences between the two sub-groups of women. We find that more women with negative fertility gaps belong to poorer economic status and reside in rural areas. On the health front, women with positive to no fertility gap are marginally healthier using the BMI and anemic status as indicators of health.
Table 5.2 presents an overview of the share of women associated with various nutritional statuses for children. We find that women with a negative fertility gap have a higher number of children alive compared to those with no or positive fertility gap. More than 87% of the women in the sample with negative fertility gap have three or more children, while for the women with no or positive fertility gap, this proportion is only about 15%. We also observe that women with no or positive fertility gap are younger, and thus a relatively large proportion (approximately 98%) of them have one or two children below the age of 5 years. Similarly, majority of the women without stunted or anemic children are those with no or positive fertility gap.
This preliminary data investigation points to some notable differences in child health status between the women who are exceeding their desired fertility compared to the women achieving/underachieving it. In the next section, we will present the results from formal empirical investigation of this relationship.
4.2 Multi-variate Regression Results
Table 5.3 reports logistic regression results (coefficients/odds ratios) for the relationship between child nutritional status and mother’s outcome for fertility gap.
The results suggest that the odds of having stunted children are 1.3 times higher for women with a negative fertility gap over women with a no to positive fertility gap with an estimated coefficient of 0.255. This indicates that women with more than desired children are more likely to have children with poor long-term health outcomes. Likewise, looking at the short-term health parameters, children from the women ‘overshooting’ their desired fertility are more likely to be ‘wasted’ and ‘anemic’. The corresponding odds are approximately 1.2 times higher for women with a negative fertility gap compared to those with a no to positive fertility gap. Here, the estimated coefficients, which are positive and statistically significant at the 1% significance level, are 0.198 for ‘wasted children’ and 0.189 for ‘anemic’ children.
Coefficients on control variables suggest that mother’s education and economic status are important and relevant factors for improving the odds of poor health outcomes for children both in the short term and in the longer term. These results, therefore, support conclusions from existing studies which suggest that an increase in mother’s years of education lowers the odds of having stunted/wasted/anemic children (see, e.g., Smith & Haddad, 2015). Likewise, the women from relatively affluent sections of the society have lower odds of having stunted/wasted/anemic children compared to the women who belong to the poorer strata.
Other findings suggest that age of a mother affects the nutritional outcomes for children only in the short term but not in the long term. Specifically, the coefficient of age is statistically insignificant in the model examining stunted growth but an increase in age of the mother, marginally lowers the odds of having ‘wasted’ and ‘anemic’ children. This finding is consistent with the literature which has shown that childbirth at relatively younger ages is associated with poorer nutritional outcomes for children (see, e.g., Martorell & Young, 2012).Footnote 2
The odds of stunting and wasting in children are 1.8 times higher for women residing in rural areas compared to those residing in urban areas. This may be explained by the lack of quality and sufficient diets as well as good sanitation often associated with individuals living in poor rural areas, which have been found to contribute to stunted and wasted growth (Smith & Haddad, 2015; Martorell & Young, 2012). However, location does not seem to affect the odds of anemia in children.
In addition to the various control variables discussed above, mother’s health has also been hypothesized to influence children nutritional outcomes. The existing literature shows that undernutrition and vitamin deficiencies in mothers can lead to fetal growth restriction and sub-optimal breast feeding, which consequently contributes to stunting and wasting in children (Black et al., 2013). We take into account these findings, and thus extend our model to include indicators that capture the health of mothers. We adopt two indicators to capture mother’s health: BMI and anemic status of mothers. BMI associated with poor health of a mother is defined by the range <18.5 kg/meter2 or > 30 kg/meter2. Anemic status of a mother is measured by hemoglobin levels and levels below 10 grams/deciliter (g/dl) are taken as poor health parameters. In the sample used, approximately 29% of women are considered unhealthy per the BMI standard and 15% are considered anemic.
Table 5.4 presents the results in which we include mother’s health status as additional covariates. We find that the inclusion of information on mother’s health only slightly improved the overall explanatory power of the model and does not alter the effect of the fertility gap on the nutritional status of children. We do find that mothers’ anemic status positively influences the odds of a child having poor nutritional outcomes, with the strongest association observed in the case of children being anemic. Mother’s BMI status does not significantly affect the odds of being stunted but influences the odds of being wasted and anemic. Given that being wasted and anemic are associated with short-term health factors, this finding suggests that BMI of a mother tends to affect the nutritional status of children only in the short term but not over the longer term.
We also investigate the effect of the interaction between a mother’s health condition and fertility gap on her child’s nutritional outcomes. Specifically, we attempt to understand if mothers with poor health and negative fertility gap are likely to have children with poorer nutritional status. We achieve this by including two interaction terms between (1) mother’s BMI and fertility gap and (2) mother’s anemic status and fertility gap. These interaction terms are statistically insignificant.
5 Conclusion
This chapter examines the effects of the fertility gap on child nutrition in India. Child nutrition is one of the key indicators of development and one of the most important millennium and sustainable development goal. The importance of child nutrition is reflected in the fact that it is not just an independent development outcome, but it is instrumental in achieving the goals of poverty, poor health and inadequate social conditions. Specifically, good nutrition plays an important role in achieving the development goals of health, education and economic growth because of the importance of human capital in the development process. Child nutrition is crucial for the human capital components of economic development and good health. Good nutrition enables children benefit from education, it reduces mortality among children and mothers, and, more importantly, it contributes to the development of resilient communities. Accordingly, malnourishment can be linked with poor development and productivity.
Using a nationally representative data from India, we examine the association between fertility gaps and child nutrition with a specific focus on stunted growth, wasted growth and anemia. Fertility gap, defined as the difference between a woman’s ideal number of children and her actual number of children, is measured using a dummy variable. The dummy variable that takes the value 0 for women with no (i.e., achieved the ideal number of children) or positive fertility gap (i.e., has fewer children than ideal), and the value 1 for women with negative fertility gap (i.e., have more children than desired). Our results show that the odds of having malnourished children that are stunted, wasted or anemic are higher for women who exceed their fertility target compared to those who have achieved or underachieved it.
The findings from this research emphasize the importance of policies that promote low fertility. In the Indian context, where fertility period begins relatively early in life for most women, making it more likely for them to exceed their fertility targets, it is important to promote the awareness of family planning programs and contraception methods. This will ensure that the early onset of fertility cycle observed in India does not lead to more children than desired. Policies promoting the education of women are also important given the finding that education is associated with better fertility decisions.
Notes
- 1.
The 17 major states included in our analysis account for roughly 90% of India’s population and make up around 87% of India’s GDP. The remaining 11 states, not included in the analysis, were small with missing or unreliable data points. The states not included are Chhattisgarh, Jharkhand, Uttrakhand, Goa, Mizoram, Sikkim, Arunachal Pradesh, Meghalaya Jammu, Kashmir and Nagaland.
- 2.
These results must be contextualized in an Indian setting where most of the women start their fertility rather early in life. The median age of first marriage is still very low in India. As per NFHS 4 survey report, the median age at first marriage is 19 years among women aged 20–49 and 40% of women aged 20–49 marry before the legal minimum age for marriage of 18 years (Indian National Family Health Survey NFHS 4, 2015–16, Chapter 6, page number 157).
References
Ashraf, Q. H., Weil, D. N., & Wilde, J. (2013). The effect of fertility reduction on economic growth. Population and Development Review, 39(1), 97–130.
Barro, R. J., & Becker, G. S. (1989). Fertility choice in a model of economic growth. Econometrica, 57(2), 481–501. https://doi.org/10.2307/1912563
Beaujouan, E., & Berghammer, C. (2019). The gap between lifetime fertility intentions and completed fertility in Europe and the United States: A cohort approach. Population Research and Policy Review. https://doi.org/10.1007/s11113-019-09516-3
Becker, G. S., Murphy, K. M., & Tamura, R. (1990). Human capital, fertility, and economic growth. Journal of Political Economy, 98(5, Part 2), S12–S37.
Becker, S. O., Cinnirella, F., & Woessmann, L. (2010). The trade-off between fertility and education: Evidence from before the demographic transition. Journal of Economic Growth, 15, 177–204.
Bental, B. (1989). The old age security hypothesis and optimal population growth. Journal of Population Economics, 1(4), 285–301.
Berrington, A., & Pattaro, S. (2014). Educational differences in fertility desires, intentions and behaviour: A life course perspective. Advances in Life Course Research, 21, 10–27. https://doi.org/10.1016/j.alcr.2013.12.003
Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z., Christian, P., de Onis, M., … Webb, P. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet, 382, 427–477.
Blau, D. M. (1984). A model of child nutrition, fertility, and women’s time allocation: The case of Nicaragua. Research in Population Economics, 5, 113–135.
Blau, D. M. (1986). Fertility, child nutrition, and child mortality in Nicaragua: An economic analysis of interrelationships. The Journal of Developing Areas, 20(2), 185–202.
Brander, J. A., & Dowrick, S. (1994). The role of fertility and population in economic growth. Journal of Population Economics, 7(1), 1–25.
Cáceres-Delpiano, J., & Simonsen, M. (2012). The toll of fertility on mothers’ wellbeing. Journal of Health Economics, 31(5), 752–766. https://doi.org/10.1016/j.jhealeco.2012.05.006
Caldwell, J. C. (1976). Toward a restatement of demographic transition theory. Population and Development Review, 2(3/4), 321–366. https://doi.org/10.2307/1971615
Chun, H., & Oh, J. (2002). An instrumental variable estimate of the effect of fertility on the labour force participation of married women. Applied Economics Letters, 9(10), 631–634.
Doepke, M., & Tertilt, M. (2018). Women’s empowerment, the gender gap in desired fertility, and fertility outcomes in developing countries. Paper presented at the AEA Papers and Proceedings.
Drèze, J., & Murthi, M. (2001). Fertility, education, and development: Evidence from India. Population and Development Review, 27(1), 33–63.
Freedman, R., Freedman, D. S., & Thornton, A. D. (1980). Changes in fertility expectations and preferences between 1962 and 1977: Their relation to final parity. Demography, 17(4), 365–378.
Gries, T., & Grundmann, R. (2018). Fertility and modernization: The role of urbanization in developing countries. Journal of International Development, 30(3), 493–506.
Guo, Z., Wu, Z., Schimmele, C. M., & Li, S. (2012). The effect of urbanization on China’s fertility. Population Research and Policy Review, 31(3), 417–434. https://doi.org/10.1007/s11113-012-9230-0
Herzer, D., Strulik, H., & Vollmer, S. (2012). The long-run determinants of fertility: One century of demographic change 1900–1999. Journal of Economic Growth, 17(4), 357–385. https://doi.org/10.1007/s10887-012-9085-6
Hondroyiannis, G. (2010). Fertility determinants and economic uncertainty: An assessment using European panel data. Journal of Family and Economic Issues, 31(1), 33–50. https://doi.org/10.1007/s10834-009-9178-3
Horton, S. (1986). Child nutrition and family size in the Philippines. Journal of Development Economics, 23(1), 161–176. https://doi.org/10.1016/0304-3878(86)90086-6
International Institute for Population Sciences (IIPS) & ICF. (2017). National family health survey (NFHS-4), 2015–16. Mumbai: IIPS.
Khan, H. T. A., & Raeside, R. (1997). Factors affecting the most recent fertility rates in urban-rural Bangladesh. Social Science & Medicine, 44(3), 279–289. https://doi.org/10.1016/S0277-9536(96)00076-7
Klawon, E., & Tiefenthaler, J. (2001). Bargaining over family size: The determinants of fertility in Brazil. Population Research and Policy Review, 20(5), 423–440. https://doi.org/10.1023/A:1013337201896
Kohler, H. P., Behrman, J. R., & Skytthe, A. (2005). Partner+ children= happiness? The effects of partnerships and fertility on well-being. Population and Development Review, 31(3), 407–445.
Kravdal, Ø. (2002). Education and fertility in sub-Saharan Africa: Individual and community effects. Demography, 39(2), 233–250. https://doi.org/10.1353/dem.2002.0017
Lloyd, C. B., & Gage-Brandon, A. J. (1994). High fertility and children’s schooling in Ghana: Sex differences in parental contributions and educational outcomes. Population studies, 48(2), 293–306.
Martorell, R., & Young, M. F. (2012). Patterns of stunting and wasting: Potential explanatory factors. Advances in Nutrition, 3, 227–233.
McQuillan, K. (2004). When does religion influence fertility? Population and Development Review, 30(1), 25–56.
Mishra, A., & Parasnis, J. (2017). Peers and fertility preferences: An empirical investigation of the role of neighbours, religion and education. Social Indicators Research, 134(1), 339–357.
Mishra, A., & Parasnis, J. (2018). Husband, sons and fertility gap: Evidence from India. Monash University Department of Economics Working Paper Series, 17/18, 1–37.
Morgan, S. P., & Rackin, H. (2010). The correspondence between fertility intentions and behavior in the United States. Population and Development Review, 36(1), 91–118.
Neher, P. A. (1971). Peasants, procreation, and pensions. The American Economic Review, 61(3), 380–389.
Neyer, G., & Hoem, J. M. (2008). Education and permanent childlessness: Austria vs. Sweden. A research note. In J. Surkyn, P. Deboosere, & J. Van Bavel (Eds.), Demographic challenges for the 21st century: A state of the art in demography (pp. 91–112). Brussels: Brussels University Press.
Noack, T., & Østby, L. (2002). Free to choose–but unable to stick to it? Norwegian fertility expectations and subsequent behaviour in the following 20 years. In E. Klijzing & M. Corijn (Eds.), Dynamics of fertility and partnership in Europe: Insights and lessons from comparative research (pp. 103–116). New York: United Nations.
Nugent, J. B. (1985). The old-age security motive for fertility. Population and Development Review, 11(1), 75–97. https://doi.org/10.2307/1973379
Rindfuss, R. R., Morgan, S. P., & Offutt, K. (1996). Education and the changing age pattern of American fertility: 1963–1989. Demography, 33(3), 277–290. https://doi.org/10.2307/2061761
Schultz, T. P. (2005). Effects of fertility decline on family well-being: Opportunities for evaluating population programs. New Haven: Yale University.
Smallwood, S., & Jefferies, J. (2003). Family building intentions in England and Wales: Trends, outcomes and interpretations. Population Trends, 112, 15–28.
Smith, L. C., & Haddad, L. (2015). Reducing child undernutrition: Past drivers and priorities for the post-MDG era. World Development, 68, 180–204.
UNPF. (2018). The state of world population 2018. New York: United Nations Population Fund.
Wang, P., Yip, C. K., & Scotese, C. A. (1994). Fertility choice and economic growth: Theory and evidence. The Review of Economics and Statistics, 76(2), 255–266. https://doi.org/10.2307/2109880
Zhang, J., & Nishimura, K. (1993). The old-age security hypothesis revisited. Journal of Development Economics, 41(1), 191–202. https://doi.org/10.1016/0304-3878(93)90047-Q
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Mishra, A., Awaworyi Churchill, S. (2020). Fertility Gap and Child Nutrition: Evidence from India. In: Awaworyi Churchill, S. (eds) Moving from the Millennium to the Sustainable Development Goals. Palgrave Macmillan, Singapore. https://doi.org/10.1007/978-981-15-1556-9_5
Download citation
DOI: https://doi.org/10.1007/978-981-15-1556-9_5
Published:
Publisher Name: Palgrave Macmillan, Singapore
Print ISBN: 978-981-15-1555-2
Online ISBN: 978-981-15-1556-9
eBook Packages: Economics and FinanceEconomics and Finance (R0)