
Abstract
Evidence for adverse effects of brominated flame retardants (BFRs) in humans is reviewed, with a focus on polybrominated diphenyl ethers (PBDEs). BFRs may easily leach out during manufacture or the use of consumer products, and enter the environment. Food consumption or ingestion of contaminated dust is among the major pathways of human exposure to BFRs. Epidemiological and experimental reports suggest that exposure to BFRs may induce adverse neurodevelopmental, metabolic, and reproductive effects.
The sex hormone-related effects of BRFs include those related to birth outcomes, growth, and reproductive system. Moreover, several other health consequences such as neurodevelopmental and behavioral disorders, thyroid hormone system, and obesity were identified as endocrine effects of BRFs. Some studies reported conflicting observations; however, their thyroid hormone disruption and neurodevelopmental toxicities have been demonstrated frequently. The use of certain BFRs is banned worldwide, however, BFRs are persistent in the ecosystem and are accumulating in human because of their lipophilicity. Thus, active epidemiological and mechanistic studies, especially on the susceptible populations, are warranted.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Flame retardants
- PBDEs
- Birth outcomes
- Congenital malformation
- Neurodevelopmental toxicity
- Reproductive toxicity
- Thyroid hormone disruption
- Obesity
- Diabetes
1 Background
Brominated flame retardants (BFRs) are a group of brominated chemicals that have been used as flame retardant. When heated, BFRs release free bromine atoms and respond to free radicals generated during burning, and thus delay the combustion process. Because of this property, this group of compounds have been widely used in various consumer products such as electronics, furnishing, textiles, building materials, and polyurethane foams, to enhance ignition resistance. The use of BFRs has led to frequent detection of several major BRFs, such as tetrabromobisphenol A (TBBPA), polybrominated diphenyl ethers (PBDEs), polybrominated biphenyls (PBBs), and hexabromocyclododecanes (HBCDs), in the environmental matrices and humans [1].
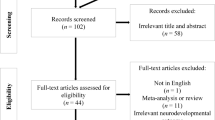
PBDEs are an important group of BFRs which have been used in a huge amount worldwide. The total production of PBDE commercial mixtures from 1970 to 2005 is estimated between 1.29 and 1.47 million tonnes worldwide [2]. PBDEs can be classified by the degree of bromination, and depending on the degree and location of bromination, a total of 209 congeners are possible. Among them, the most commonly used commercial PBDE mixtures are in forms of penta-, octa-, and deca-BDE. The most abundant PBDE congeners detected in biota and environment are BDE-47, -99, -100, -153, and -209 (Fig. 14.1).

Chemical structures of some major PBDE congeners and thyroxine
Because of their structural similarity to T4, it is hypothesized that PBDEs might interfere with thyroid hormone transport and metabolism [3, 4]. Animal experimental studies support the thyroid disrupting effects of PBDEs [5]. As a possible consequence of thyroid disruption, their neurodevelopmental toxicity has been also suggested in both experimental organisms and humans [6]. Owing to the health concerns and their persistent nature, some PBDEs such as hexabromodiphenyl ether and heptabromodiphenyl ether (hexa- and hepta-BDE), tetrabromodiphenyl ether, penta-bromodiphenyl ether (tetra- and penta-BDE), and most recently, deca-BDE were listed in Annex A of the Stockholm Convention as persistent organic pollutants (POPs). Therefore, global efforts have been implemented to eliminate the production and the use of PBDEs. However, given the widespread use of this group of compounds and their persistent nature, PBDEs in the environment and biota are expected to be a lingering public health threat for decades to come.
Unlike reactive flame retardants (FRs) such as TBBPA, which are covalently bonded into the polymer matrix, PBDEs are additive FRs, which are mixed with the polymer and do not form chemical bonds with the materials [1]. Both additive and reactive FRs can be easily leached out during manufacture or the use of consumer products and subsequently enter the environment. Humans are exposed to PBDEs through ingestion or inhalation of contaminated media. Intake of PBDEs is believed to occur primarily from food consumption, and to a lesser extent through air inhalation and dermal absorption [7,8,9,10]. Owing to their bio-accumulative characteristics, PBDEs are expected to be high in seafood, and hence humans with high seafood consumption tend to be exposed more [11]. Dust is another important route of oral exposure [8, 12,13,14,15]. In a recent Korean study, it was reported that incidental dust ingestion was major in children while food was more important source of exposure in adults [16].
The developing fetus may be exposed to PBDEs through the placenta [17]. For breastfed infants, breast milk is the most critical source of PBDE exposure [17, 18]. Because many plastic-made toys contain PBDEs, toys may be an important source of exposure to PBDEs in toddlers and young children [19, 20]. Specific behavior patterns of young children, like sucking and crawling, can increase the amount of exposure to PBDEs from the toys [19, 21]. Consequently, several PBDEs were detected at higher concentrations in the serum of toddlers compared to those of adults [22].
2 Human Toxicity of Brominated Chemicals
Knowledge about the human toxicity of PBDEs has accumulated in the last two decades. The extent of bromination appears to determine the toxicity of PBDEs, with more brominated congeners being less toxic. Thus, PBDEs found in the environment are likely to be more toxic than the forms which were applied to the products, because debromination occurs when they are released into the environment. Epidemiological evidence suggests an association between endocrine disruption and the developmental effects of PBDEs, even though, often, the observations are not consistent and the underlying etiology is not fully understood. Of particular concern is their association with adverse outcomes in neurobehavioral development among children.
This chapter describes what has been documented as human toxicity for PBDEs in detail, with a focus on endocrine disruption effects. Underlying toxicity mechanisms suggested for these outcomes are also briefly described.
2.1 Birth Outcomes
Several epidemiological studies reported the associations between prenatal exposure to PBDEs and birth outcomes [23,24,25,26,27,28,29,30,31,32]. Most studies used PBDE levels detected in maternal or cord blood serum to indicate prenatal exposure, and the levels measured in breast milk to represent postnatal exposure.
The associations between PBDE exposure and birth outcomes have been frequently reported worldwide. In many populations, prenatal exposure to PBDEs has been associated with adverse birth outcomes. In a Spanish cohort study, the sum of PBDE concentrations in cord serum was negatively associated with abdominal circumference and the fetal weight estimated at gestational week 12 [23]. In addition, negative associations of maternal serum PBDE concentrations in the first trimester with head circumference and birth weight were reported in the same cohort [23]. Similar observations were reported in China, e.g., negative associations between maternal BDE-28/-100 concentrations and birth length, and BDE-28 concentrations and birth weight [24]. More recently, cord blood concentrations of PBDEs have been shown to be associated with increased head circumference in Chinese prospective birth cohort [25]. In the US general population (N = 234), the association between maternal and paternal PBDE concentrations measured before conception and birth size has been reported. Interestingly, a significant association of both maternal and paternal PBDEs with lower birth weight was found among female infants, whereas paternal concentrations of PBDEs were associated with higher birth weight in boys [26]. In a cohort of pregnant mothers in the USA (N = 286), negative associations were observed between major PBDEs including BDE-47, 99, and 100 and birth weight, even though the significance disappeared when the maternal weight gain was added to the association model [27]. However, in the same study, prenatal exposure to PBDE did not show an association with birth length, head circumference, or gestational duration [27].
Lactational exposure to PBDEs was associated with reduced birth weight, birth length, and chest circumference in a Taiwanese women population [28]. In the USA, weak associations between early-life PBDE exposures via breast milk and anthropometric measurements were shown. However, in this population, weight-to-height z-scores were inversely associated with PBDEs in breast milk among boys; on the contrary, weight-for-height z-scores were positively associated with PBDEs, except for BDE-153, among girls [29]. In a Swedish cohort (1996–2010), maternal breast milk concentrations of PBDEs (sum of BDE-47, 99, 100 and 153) showed an inverse association with birth weight, and the associations became stronger among boys [30]. In Northern Tanzania, BDE-47, -99, -100, and -153 concentrations measured in colostrum were significantly correlated with birth weight and birth length [31].
The associations with preterm birth or gestational age are seldom investigated. One report suggests that high levels of maternal BDE-47 might increase the risk of preterm birth [32]. On the contrary, cord blood concentrations of PBDEs were associated with increased gestational age in Chinese birth cohort, i.e., 0.73 weeks increase for 1 log unit increase of PBDEs [25]. It is not clear whether PBDEs are associated with the gestational period, because only a small number of studies have been conducted, and the directions of the association are conflicting.
Despite accumulating evidence from epidemiological and cross-sectional studies, mechanisms underlying the association between PBDEs and birth outcome are not well understood. For example, maternal BMI or weight gain during pregnancy has been associated with fetal growth, and these maternal somatic characteristics can be influenced by various factors other than PBDEs. Further research is needed to study whether PBDEs affect fetal growth independently, apart from maternal BMI and weight gain during pregnancy. Moreover, biological mechanisms underlying different responses by the infant sex are not known, and warrant further experimental studies.
2.2 Cryptorchidism and Hypospadias
Incidences of congenital malformation among male infants, including cryptorchidism and hypospadias, have been increasing significantly. It is suspected that cryptorchidism and hypospadias may share common risk factors [33]. Chemical-induced sex hormone disruption is one reason for these malformations, as it depends on the fetal conversion of testosterone to dihydrotestosterone, binding of dihydrotestosterone to the androgen receptor, and proper subsequent androgen receptor signaling [34]. The epidemiological studies have suggested associations of flame retardant exposure with genital malformation. Breast milk PBDE concentrations were found to be significantly higher in the boys with cryptorchidism than in controls, in a prospective Danish-Finnish study, 1997–2001 [35]. In a case–control study of Canada, concentrations of BDE-99, 100, and 154 in maternal hair were found to be significantly higher in the cases [36]. In another Canadian population, in utero exposure to PBDEs, as measured in maternal hair, was found to be higher by 48% in mothers who gave birth to infants with hypospadias [37]. Exposure to PBDEs that were measured in cord plasma samples also has been shown to be inversely associated with anogenital distance at birth, 6 months, 12 months, and 48 months of age in Shanghai birth cohort [38]. Considering the anti-androgenic potentials of PBDEs, not only congenital malformation but also adverse consequences in later life stages, warrant further investigations.
2.3 Neurodevelopment and Neurobehavioral Disorders
Prenatal exposure to PBDEs has been associated with alterations in behavioral domains, especially motor activity and cognitive function in later stages of life. This association was first reported in a US based study, which showed that children with higher cord serum concentrations of PBDEs scored lower mental and physical test scores at 12–48 and 72 months of age [39]. Subsequently, a number of epidemiological studies of similar design have been published. Maternal serum BDE-47 levels were associated with internalizing and externalizing problems in the Child Behavior Checklist, in toddlers of 18–24 months of age, in Korea [40]. In a Chinese population, cord serum BDE-99 and BDE-47 concentrations were observed to be significantly associated with lower language developmental index and social developmental index, respectively, at 24 months of age, but not at 12 months [41]. In a US population, prenatal exposure to BDE-47 was also shown to be associated with attention problems at 3–7 years of age [42].
Postnatal exposure also has been found to be associated with neurodevelopmental indices in several studies. In a Taiwanese infant population (N = 70), elevated PBDE levels in breast milk were shown to be associated with developmental delays in cognition [43]. In a North Carolina study cohort (N = 222), lactational PBDE exposure was observed to be correlated with increased activity and impulsive behavior in early childhood [29]. However, there are conflicting observations as well. In a prospective birth cohort in Spain (N = 88 for cord blood samples, and N = 244 for serum at age 4), no association was seen between PBDE body-burden and motor or cognitive alteration in 4-year-old children [44]. In Belgium adolescents (N = 515), no significant association was observed between serum PBDEs, HBCD, and TBBPA concentrations and attention, visual scanning, or working memory test scores. The only exception is the motor function scores in the finger tapping test which were shown to only be significantly associated with serum PBDEs levels in this population, showing a decrease in the number of taps by 5.31, by a two-fold increase of the sum of serum PBDEs [45].
In a California birth cohort, which was conducted in highly contaminated regions of the USA, both prenatal and childhood PBDE exposures were shown to be associated with poor attention, fine motor coordination, and cognition (Full-Scale IQ) at 7 years of age [46]. Several other studies have reported significant associations of prenatal and postnatal PBDE exposure with neurodevelopmental indices in the Health Outcomes and Measures of the Environment (HOME) Study. In the HOME study, maternal serum BDE-28 concentrations were associated with autistic behavior at 4–5 years of age [47], and BDE-47 concentrations were observed to be associated with a decrease in intelligence quotient (IQ) at 5 years of age [48]. However, neither psychomotor nor mental indices of the Bayley Scales of Infant Development-II (BSID-II) at ages 1, 2, and 3 years were shown to be significantly associated with prenatal PBDEs exposure in this cohort [48]. Recently, a follow-up of the HOME study showed that PBDEs concentrations measured in children of 8 years old were significantly associated with poorer emotional and impulse control [49], but those measured in children of 1, 2, 3, and 5 years old did not show an association. The results of the HOME study suggest that at the environmentally relevant levels of exposure, potential of neurodevelopmental toxicity cannot be ignored among children.
The exact mechanisms underlying PBDE neurotoxicity are unclear, but generally, two modes of action affecting brain development have been suggested [6]. One mode of action is a capacity of PBDEs to alter thyroid hormone homeostasis which can eventually result in brain development. The other possibilities include the oxidative stress potential of PBDEs, disruption of calcium signal transduction, and decrease in neural and oligodendrocyte differentiation, thereby affecting nervous system cells directly.
2.4 Reproductive Systems
Toxicities of PBDEs on the human reproductive system have not thoroughly studied, and, therefore, there remain gaps in knowledge. Among various reproductive dysfunction indicators, menstruation characteristics and age at puberty have been studied among female population. In Taiwan, PBDE concentrations in breast milk were not associated with maternal menstruation characteristics (N = 20), even though their concentrations were shown to be significantly related to the birth size of infants [28]. In another study conducted in Taiwanese women (N = 46), higher concentrations of PBDEs were shown to be significantly associated with prolonged length of menstrual cycle and irregular menstruation periods [50]. Menstruation characteristics are closely related to fertility. Age at puberty is also an important indicator of reproductive system toxicity in humans. One longitudinal study in the USA explored the association between pubertal timing and PBDE exposure. In this study, the age at pubertal transition was observed to be significantly higher among girls with greater PBDE levels [51]. Among a small male population recruited through a US infertility clinic (N = 62), positive associations of house dust penta- and octa-PBDE concentrations with hormone levels of estradiol, and sex hormone binding globulin (SHBG), luteinizing hormone (LH) and testosterone were observed, although an inverse association of deca-BDE concentrations with testosterone was seen [52].
2.5 Thyroid Hormones
Thyroid hormones play a crucial role in the maintenance and activation of metabolic function, neurodevelopment, and cognitive function. Moderate changes in thyroid hormone levels during pregnancy may be associated with adverse outcomes in offspring [53, 54]. For example, significantly lower IQ scores were found in children of women with thyroid deficiency during pregnancy, even though hormone levels were found within the reference range [55].
Significant associations between PBDEs exposure and thyroid hormone levels among adults are summarized in Table 14.1. Thyroid hormone disruptive effect of PBDEs has been suggested in diverse populations including the general population, fish consumers, and workers [56,57,58]. In recent studies, hypothyroidism, i.e., low T4 and high TSH, was shown to be associated with higher PBDE concentrations [59]. One study reported significant associations between PBDE concentrations and low status of free T3, total T3, free T4, and TSH simultaneously, but the participants were recruited from highly contaminated and occupational exposure conditions (e-waste site) [60]. Similarly, one large population study based on Inuit adults showed that exposure to BDE-47 was positively associated with total T3 [61].
Among pregnant women, the associations between PBDEs and subclinical hypothyroidism or hyperthyroidism were reported in several studies. For example, higher PBDE exposure were associated with lower TSH [62] or higher thyroid hormone levels without lower TSH [63, 64] in pregnant women. Significant disruption of thyroid hormone homeostasis by PBDEs exposure was shown in other studies based on pregnant women as well [65, 66].
The adverse effects of prenatal expsoure in newborn infants have been documented. Herbstman et al. [67] found significant association between cord serum PBDEs and lower T4 or higher TSH among babies born by spontaneous vaginal delivery. Although evidence showing otherwise is often found [68], most studies with neonatal population show significant associations between PBDEs exposure and hypothyroidism, e.g., a decrease in thyroid hormones or increased TSH (Table 14.2). Prenatal PBDE exposure was inversely associated with cord blood free T4 and total T4 in a large population-based study (N = 260) [65]. In addition, PBDEs exposure was inversely associated with free T3 and total T3 in cord blood serum in a small population-based study (N = 50) [69]. In both studies, however TSH was not influenced by PBDE level. In Korean general population, however, PBDE exposure as measured in cord blood serum was associated with increased TSH in newborn infants without change in T3 and T4 [70].
The adverse effects of PBDEs on thyroid function have also been reported in children and post-menopausal women. In children of China, serum PBDE concentrations were associated with increased T3 [71]. Unlike previous reports, the direction of thyroid hormone change is toward hyperthyroidism, and hence this observation warrants further validations in other children populations. Because thyroid hormones are in apparent crosstalk with estrogens [72], menopausal status of women may influence thyroid hormone disruption by exogenous chemicals, due to the difference in estrogen reserves. One study based on the NHANES data suggested that general adult women with higher PBDE concentrations exhibited increased odds of having thyroid disease. In stratified analysis, this association became stronger in post-menopausal population, suggesting enhanced effects of PBDEs on thyroid signaling by the lowered estrogen levels [73]. In contrast, but partly supporting the crosstalk between thyroid and sex hormones, pre-menopausal adult women aged between 30 and 50 years of age showed stronger associations between PBDE exposure levels and prevalence of hypothyroidism, compared to older women aged between 51 and 79 years old [59].
PBDEs share structural similarity with T4 (Fig. 14.1) and cause thyroid hormone disruption through alteration of transport and metabolism/deactivation of thyroid hormones. UDP-GT induction catalyzes the glucuronidation of T4, eventually leading to the clearance of circulating T4 [74, 75]. Circulating T4 hormone may competitively binds to the thyroid hormone transport protein [76] and thyroid hormone receptor [77], and therefore has a potential to interfere with the normal transport of thyroid hormones to peripheral tissues, and inhibits cellular uptake of thyroid hormones in thyroid hormone-sensitive cells.
2.6 Obesity and Diabetes
Obesity, diabetes and other metabolic dysfunctions are closely related to the thyroid hormone system. Obesity and related diseases are therefore associated with chemicals disrupting thyroid function, e.g., BFRs including PBDEs. The associations of PBDEs and PBBs with diabetes and metabolic syndrome have been reported in a population participating in the US NHANES 2003–2004 [78]. In mothers, who participated in the Salinas birth cohort (N = 468), positive associations with BMI were observed for BDE-47, while BDE-153 was shown to be inversely associated [79]. Most recently, a very large French cohort (N = 71,415) showed that HBCD and PBDEs exposure were associated with type 2 diabetes (T2D) risk [80]. Among children of a California birth cohort (N = 224), prenatal exposure to total PBDEs showed positive associations with BMI z-score in boys, while a negative association in girls at age 7 years was observed [81]. However, children’s serum BDE-153 concentrations were inversely associated with BMI [81]. Similar negative associations were also observed in the HOME study. PBDEs during pregnancy were shown to be associated with anthropometric measures in children aged 1–8 years (N = 318), while maternal serum PBDEs were shown to be associated with lower BMI z-score, decreased waist circumference, and lower percent body fat [82]. In HOME study participants, at age 8 years, (N = 206), BDE-153 concentrations in children’s serum were shown to be inversely associated with adiposity measures, but no significant association was found for BDE-28, -47, -99, and -100 [83]. In both studies, negative associations between BDE-153 concentrations and adiposity measures were clear [82, 83]. For BDE-153, the mechanisms involved in reduction of adipose tissue are unknown. For example, a significant increase in serum BDE-153 levels has been shown after weight loss treatments in a group of 94 obese adolescents, without changes in BDE-47 and -100 [84]. BDE-153 has a longer half-life than BDE-47, -99, and -100 [85], leading to greater storage of PBDEs in the adipose tissue of person with higher adiposity. Thus, while experimental studies suggest obesogenic effects of PBDEs [86, 87], reverse causality may be observed in cross-sectional studies.
3 Conclusions
Epidemiological evidence indicating endocrine disruption by PBDEs are accumulating, even though inconsistent observations are also reported. PBDEs are associated with thyroid hormone disruption and negative neurodevelopmental outcomes in many populations including newborn children and pregnant women. However, their associations with sex hormone disruption or obesity are less studied and uncertain. Studies on populations at high levels of exposure such as e-waste disposal site residents or people with occupational BFR exposure are also warranted.
References
de Wit CA, Herzke D, Vorkamp K. Brominated flame retardants in the Arctic environment-trends and new candidates. Sci Total Environ. 2010;408(15):2885–918.
UNEP (2010) Supporting document for technical review of the implications of recycling commercial pentabromodiphenyl ether and commercial octabromodiphenyl ether. Stockholm Convention document for 6th POP Reviewing Committee meeting (UNEP/POPS/POPRC.6/INF/6). Available at http://chm.pops.int/Default.aspx?tabid=783 [Accessed 31 March 2019].
Birnbaum LS, Staskal DF. Brominated flame retardants: cause for concern? Environ Health Perspect. 2004;112(1):9–17.
McDonald TA. A perspective on the potential health risks of PBDEs. Chemosphere. 2002;46(5):745–55.
Boas M, Feldt-Rasmussen U, Main KM. Thyroid effects of endocrine disrupting chemicals. Mol Cell Endocrinol. 2012;355(2):240–8.
Costa LG, de Laat R, Tagliaferri S, Pellacani C. A mechanistic view of polybrominated diphenyl ether (PBDE) developmental neurotoxicity. Toxicol Lett. 2014;230(2):282–94.
Allen JG, McClean MD, Stapleton HM, Nelson JW, Webster TF. Personal exposure to polybrominated diphenyl ethers (PBDEs) in residential indoor air. Environ Sci Technol. 2007;41(13):4574–9.
Harrad S, Hazrati S, Ibarra C. Concentrations of polychlorinated biphenyls in indoor air and polybrominated diphenyl ethers in indoor air and dust in Birmingham, United Kingdom: implications for human exposure. Environ Sci Technol. 2006;40(15):4633–8.
Wu N, Herrmann T, Paepke O, Tickner J, Hale R, Harvey LE, La Guardia M, McClean MD, Webster TF. Human exposure to PBDEs: associations of PBDE body burdens with food consumption and house dust concentrations. Environ Sci Technol. 2007;41(5):1584–9.
Bramwell L, Glinianaia SV, Rankin J, Rose M, Fernandes A, Harrad S, Pless-Mulolli T. Associations between human exposure to polybrominated diphenyl ether flame retardants via diet and indoor dust, and internal dose: a systematic review. Environ Int. 2016;92-93:680–94.
Schecter A, Papke O, Tung KC, Staskal D, Birnbaum L. Polybrominated diphenyl ethers contamination of United States food. Environ Sci Technol. 2004;38(20):5306–11.
Jones-Otazo HA, Clarke JP, Diamond ML, Archbold JA, Ferguson G, Harner T, Richardson GM, Ryan JJ, Wilford B. Is house dust the missing exposure pathway for PBDEs? An analysis of the urban fate and human exposure to PBDEs. Environ Sci Technol. 2005;39(14):5121–30.
Zota AR, Rudel RA, Morello-Frosch RA, Brody JG. Elevated house dust and serum concentrations of PBDEs in California: unintended consequences of furniture flammability standards? Environ Sci Technol. 2008;42(21):8158–64.
Stapleton HM, Eagle S, Sjodin A, Webster TF. Serum PBDEs in a North Carolina toddler cohort: associations with handwipes, house dust, and socioeconomic variables. Environ Health Perspect. 2012;120(7):1049–54.
Lorber M. Exposure of Americans to polybrominated diphenyl ethers. J Expo Sci Environ Epidemiol. 2008;18(1):2–19.
Lee S, Kannan K, Moon HB. Assessment of exposure to polybrominated diphenyl ethers (PBDEs) via seafood consumption and dust ingestion in Korea. Sci Total Environ. 2013;443:24–30.
Shin MY, Kim S, Lee S, Kim HJ, Lee JJ, Choi G, Choi S, Kim S, Kim SY, Park J, Moon HB, Choi K, Kim S. Prenatal contribution of 2, 2′, 4, 4′-tetrabromodiphenyl ether (BDE-47) to total body burden in young children. Sci Total Environ. 2018;616-617:510–6.
Lee S, Kim S, Kim E, Lee IS, Choi G, Kim HJ, Park J, Jae Lee J, Choi S, Young Kim S, Kim S, Kim S, Choi K, Moon HB. Polybrominated diphenyl ethers (PBDEs) in breast milk of Korea in 2011: current contamination, time course variation, influencing factors and health risks. Environ Res. 2013;126:76–83.
Chen SJ, Ma YJ, Wang J, Chen D, Luo XJ, Mai BX. Brominated flame retardants in children’s toys: concentration, composition, and children’s exposure and risk assessment. Environ Sci Technol. 2009;43(11):4200–6.
Ionas AC, Dirtu AC, Anthonissen T, Neels H, Covaci A. Downsides of the recycling process: harmful organic chemicals in children’s toys. Environ Int. 2014;65:54–62.
Hoffman K, Webster TF, Sjodin A, Stapleton HM. Toddler’s behavior and its impacts on exposure to polybrominated diphenyl ethers. J Expo Sci Environ Epidemiol. 2017;27(2):193–7.
Toms LM, Sjodin A, Harden F, Hobson P, Jones R, Edenfield E, Mueller JF. Serum polybrominated diphenyl ether (PBDE) levels are higher in children (2–5 years of age) than in infants and adults. Environ Health Perspect. 2009;117(9):1461–5.
Lopez-Espinosa MJ, Costa O, Vizcaino E, Murcia M, Fernandez-Somoano A, Iniguez C, Llop S, Grimalt JO, Ballester F, Tardon A. Prenatal exposure to polybrominated flame retardants and fetal growth in the INMA cohort (Spain). Environ Sci Technol. 2015;49(16):10108–16.
Chen L, Wang C, Cui C, Ding G, Zhou Y, Jin J, Gao Y, Tian Y. Prenatal exposure to polybrominated diphenyl ethers and birth outcomes. Environ Pollut. 2015;206:32–7.
Chen L, Wang C, Zhang Y, Zhou Y, Shi R, Cui C, Gao Y, Tian Y. Polybrominated diphenyl ethers in cord blood and perinatal outcomes from Laizhou Wan Birth Cohort, China. Environ Sci Pollut Res Int. 2018;25(21):20802–8.
Robledo CA, Yeung E, Mendola P, Sundaram R, Maisog J, Sweeney AM, Barr DB, Louis GM. Preconception maternal and paternal exposure to persistent organic pollutants and birth size: the LIFE study. Environ Health Perspect. 2015;123(1):88–94.
Harley KG, Chevrier J, Aguilar Schall R, Sjodin A, Bradman A, Eskenazi B. Association of prenatal exposure to polybrominated diphenyl ethers and infant birth weight. Am J Epidemiol. 2011;174(8):885–92.
Chao HR, Wang SL, Lee WJ, Wang YF, Papke O. Levels of polybrominated diphenyl ethers (PBDEs) in breast milk from Central Taiwan and their relation to infant birth outcome and maternal menstruation effects. Environ Int. 2007;33(2):239–45.
Hoffman K, Adgent M, Goldman BD, Sjodin A, Daniels JL. Lactational exposure to polybrominated diphenyl ethers and its relation to social and emotional development among toddlers. Environ Health Perspect. 2012;120(10):1438–42.
Lignell S, Aune M, Darnerud PO, Hanberg A, Larsson SC, Glynn A. Prenatal exposure to polychlorinated biphenyls (PCBs) and polybrominated diphenyl ethers (PBDEs) may influence birth weight among infants in a Swedish cohort with background exposure: a cross-sectional study. Environ Health. 2013;12:44.
Muller MH, Polder A, Brynildsrud OB, Lie E, Loken KB, Manyilizu WB, Mdegela RH, Mokiti F, Murtadha M, Nonga HE, Skaare JU, Lyche JL. Brominated flame retardants (BFRs) in breast milk and associated health risks to nursing infants in northern Tanzania. Environ Int. 2016;89-90:38–47.
Peltier MR, Koo HC, Getahun D, Menon R. Does exposure to flame retardants increase the risk for preterm birth? J Reprod Immunol. 2015;107:20–5.
Akre O, Lipworth L, Cnattingius S, Sparen P, Ekbom A. Risk factor patterns for cryptorchidism and hypospadias. Epidemiology. 1999;10(4):364–9.
Carmichael SL, Herring AH, Sjodin A, Jones R, Needham L, Ma C, Ding K, Shaw GM. Hypospadias and halogenated organic pollutant levels in maternal mid-pregnancy serum samples. Chemosphere. 2010;80(6):641–6.
Main KM, Kiviranta H, Virtanen HE, Sundqvist E, Tuomisto JT, Tuomisto J, Vartiainen T, Skakkebaek NE, Toppari J. Flame retardants in placenta and breast milk and cryptorchidism in newborn boys. Environ Health Perspect. 2007;115(10):1519–26.
Goodyer CG, Poon S, Aleksa K, Hou L, Atehortua V, Carnevale A, Koren G, Jednak R, Emil S, Bagli D, Dave S, Hales BF, Chevrier J. A case-control study of maternal polybrominated diphenyl ether (PBDE) exposure and cryptorchidism in Canadian populations. Environ Health Perspect. 2017;125(5):057004.
Poon S, Koren G, Carnevale A, Aleksa K, Ling J, Ozsarfati J, Kapur BM, Bagli D. Association of in utero exposure to polybrominated diphenyl ethers with the risk of hypospadias. JAMA Pediatr. 2018;172(9):851–6.
Luan M, Liang H, Yang F, Yuan W, Chen A, Liu X, Ji H, Wen S, Miao M. Prenatal polybrominated diphenyl ethers exposure and anogenital distance in boys from a Shanghai birth cohort. Int J Hyg Environ Health. 2019;222(3):513–23.
Herbstman JB, Sjodin A, Kurzon M, Lederman SA, Jones RS, Rauh V, Needham LL, Tang D, Niedzwiecki M, Wang RY, Perera F. Prenatal exposure to PBDEs and neurodevelopment. Environ Health Perspect. 2010;118(5):712–9.
Kim S, Eom S, Kim HJ, Lee JJ, Choi G, Choi S, Kim S, Kim SY, Cho G, Kim YD, Suh E, Kim SK, Kim S, Kim GH, Moon HB, Park J, Kim S, Choi K, Eun SH. Association between maternal exposure to major phthalates, heavy metals, and persistent organic pollutants, and the neurodevelopmental performances of their children at 1 to 2 years of age- CHECK cohort study. Sci Total Environ. 2018;624:377–84.
Ding G, Yu J, Cui C, Chen L, Gao Y, Wang C, Zhou Y, Tian Y. Association between prenatal exposure to polybrominated diphenyl ethers and young children’s neurodevelopment in China. Environ Res. 2015;142:104–11.
Cowell WJ, Lederman SA, Sjodin A, Jones R, Wang S, Perera FP, Wang R, Rauh VA, Herbstman JB. Prenatal exposure to polybrominated diphenyl ethers and child attention problems at 3–7 years. Neurotoxicol Teratol. 2015;52:143–50.
Chao HR, Tsou TC, Huang HL, Chang-Chien GP. Levels of breast milk PBDEs from southern Taiwan and their potential impact on neurodevelopment. Pediatr Res. 2011;70(6):596–600.
Gascon M, Vrijheid M, Martinez D, Forns J, Grimalt JO, Torrent M, Sunyer J. Effects of pre and postnatal exposure to low levels of polybromodiphenyl ethers on neurodevelopment and thyroid hormone levels at 4 years of age. Environ Int. 2011;37(3):605–11.
Kicinski M, Viaene MK, Den Hond E, Schoeters G, Covaci A, Dirtu AC, Nelen V, Bruckers L, Croes K, Sioen I, Baeyens W, Van Larebeke N, Nawrot TS. Neurobehavioral function and low-level exposure to brominated flame retardants in adolescents: a cross-sectional study. Environ Health. 2012;11:86.
Eskenazi B, Chevrier J, Rauch SA, Kogut K, Harley KG, Johnson C, Trujillo C, Sjodin A, Bradman A. In utero and childhood polybrominated diphenyl ether (PBDE) exposures and neurodevelopment in the CHAMACOS study. Environ Health Perspect. 2013;121(2):257–62.
Braun JM, Kalkbrenner AE, Just AC, Yolton K, Calafat AM, Sjodin A, Hauser R, Webster GM, Chen A, Lanphear BP. Gestational exposure to endocrine-disrupting chemicals and reciprocal social, repetitive, and stereotypic behaviors in 4- and 5-year-old children: the HOME study. Environ Health Perspect. 2014;122(5):513–20.
Chen A, Yolton K, Rauch SA, Webster GM, Hornung R, Sjodin A, Dietrich KN, Lanphear BP. Prenatal polybrominated diphenyl ether exposures and neurodevelopment in U.S. children through 5 years of age: the HOME study. Environ Health Perspect. 2014;122(8):856–62.
Vuong AM, Yolton K, Poston KL, Xie C, Webster GM, Sjodin A, Braun JM, Dietrich KN, Lanphear BP, Chen A. Childhood polybrominated diphenyl ether (PBDE) exposure and executive function in children in the HOME study. Int J Hyg Environ Health. 2018;221(1):87–94.
Chao HR, Shy CG, Wang SL, Chen SC, Koh TW, Chen FA, Chang-Chien GP, Tsou TC. Impact of non-occupational exposure to polybrominated diphenyl ethers on menstruation characteristics of reproductive-age females. Environ Int. 2010;36(7):728–35.
Windham GC, Pinney SM, Voss RW, Sjodin A, Biro FM, Greenspan LC, Stewart S, Hiatt RA, Kushi LH. Brominated flame retardants and other persistent organohalogenated compounds in relation to timing of puberty in a longitudinal study of girls. Environ Health Perspect. 2015;123(10):1046–52.
Johnson PI, Stapleton HM, Mukherjee B, Hauser R, Meeker JD. Associations between brominated flame retardants in house dust and hormone levels in men. Sci Total Environ. 2013;445-446:177–84.
Berbel P, Mestre JL, Santamaria A, Palazon I, Franco A, Graells M, Gonzalez-Torga A, de Escobar GM. Delayed neurobehavioral development in children born to pregnant women with mild hypothyroxinemia during the first month of gestation: the importance of early iodine supplementation. Thyroid. 2009;19(5):511–9.
Idris I, Srinivasan R, Simm A, Page RC. Maternal hypothyroidism in early and late gestation: effects on neonatal and obstetric outcome. Clin Endocrinol. 2005;63(5):560–5.
Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O’Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, Faix JD, Klein RZ. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341(8):549–55.
Bloom M, Spliethoff H, Vena J, Shaver S, Addink R, Eadon G. Environmental exposure to PBDEs and thyroid function among New York anglers. Environ Toxicol Pharmacol. 2008;25(3):386–92.
Turyk ME, Persky VW, Imm P, Knobeloch L, Chatterton R, Anderson HA. Hormone disruption by PBDEs in adult male sport fish consumers. Environ Health Perspect. 2008;116(12):1635–41.
Yuan J, Chen L, Chen D, Guo H, Bi X, Ju Y, Jiang P, Shi J, Yu Z, Yang J, Li L, Jiang Q, Sheng G, Fu J, Wu T, Chen X. Elevated serum polybrominated diphenyl ethers and thyroid-stimulating hormone associated with lymphocytic micronuclei in Chinese workers from an E-waste dismantling site. Environ Sci Technol. 2008;42(6):2195–200.
Oulhote Y, Chevrier J, Bouchard MF. Exposure to polybrominated diphenyl ethers (PBDEs) and hypothyroidism in Canadian women. J Clin Endocrinol Metab. 2016;101(2):590–8.
Wang H, Zhang Y, Liu Q, Wang F, Nie J, Qian Y. Examining the relationship between brominated flame retardants (BFR) exposure and changes of thyroid hormone levels around e-waste dismantling sites. Int J Hyg Environ Health. 2010;213(5):369–80.
Dallaire R, Dewailly E, Pereg D, Dery S, Ayotte P. Thyroid function and plasma concentrations of polyhalogenated compounds in Inuit adults. Environ Health Perspect. 2009;117(9):1380–6.
Chevrier J, Harley KG, Bradman A, Gharbi M, Sjodin A, Eskenazi B. Polybrominated diphenyl ether (PBDE) flame retardants and thyroid hormone during pregnancy. Environ Health Perspect. 2010;118(10):1444–9.
Stapleton HM, Eagle S, Anthopolos R, Wolkin A, Miranda ML. Associations between polybrominated diphenyl ether (PBDE) flame retardants, phenolic metabolites, and thyroid hormones during pregnancy. Environ Health Perspect. 2011;119(10):1454–9.
Vuong AM, Webster GM, Romano ME, Braun JM, Zoeller RT, Hoofnagle AN, Sjodin A, Yolton K, Lanphear BP, Chen A. Maternal polybrominated diphenyl ether (PBDE) exposure and thyroid hormones in maternal and cord sera: the HOME study, Cincinnati, USA. Environ Health Perspect. 2015;123(10):1079–85.
Abdelouahab N, Langlois MF, Lavoie L, Corbin F, Pasquier JC, Takser L. Maternal and cord-blood thyroid hormone levels and exposure to polybrominated diphenyl ethers and polychlorinated biphenyls during early pregnancy. Am J Epidemiol. 2013;178(5):701–13.
Kim S, Park J, Kim HJ, Lee JJ, Choi G, Choi S, Kim S, Kim SY, Moon HB, Kim S, Choi K. Association between several persistent organic pollutants and thyroid hormone levels in serum among the pregnant women of Korea. Environ Int. 2013;59:442–8.
Herbstman JB, Sjodin A, Apelberg BJ, Witter FR, Halden RU, Patterson DG, Panny SR, Needham LL, Goldman LR. Birth delivery mode modifies the associations between prenatal polychlorinated biphenyl (PCB) and polybrominated diphenyl ether (PBDE) and neonatal thyroid hormone levels. Environ Health Perspect. 2008;116(10):1376–82.
Chevrier J, Harley KG, Bradman A, Sjodin A, Eskenazi B. Prenatal exposure to polybrominated diphenyl ether flame retardants and neonatal thyroid-stimulating hormone levels in the CHAMACOS study. Am J Epidemiol. 2011;174(10):1166–74.
Lin SM, Chen FA, Huang YF, Hsing LL, Chen LL, Wu LS, Liu TS, Chang-Chien GP, Chen KC, Chao HR. Negative associations between PBDE levels and thyroid hormones in cord blood. Int J Hyg Environ Health. 2011;214(2):115–20.
Kim S, Park J, Kim HJ, Lee JJ, Choi G, Choi S, Kim S, Kim SY, Moon HB, Kim S, Choi K. Association between several persistent organic pollutants and thyroid hormone levels in cord blood serum and bloodspot of the newborn infants of Korea. PLoS One. 2015;10(5):e0125213.
Guo LC, Xiao J, Zhang Y, Yu S, Lin H, Su G, Liu T, Li X, Lv S, Rutherford S, Ma W. Association between serum polybrominated diphenyl ethers, new flame retardants and thyroid hormone levels for school students near a petrochemical complex, South China. Chemosphere. 2018;202:476–82.
Vasudevan N, Pfaff D. Molecular mechanisms of crosstalk between thyroid hormones and estrogens. Curr Opin Endocrinol Diabetes. 2005;12(5):381–8.
Allen JG, Gale S, Zoeller RT, Spengler JD, Birnbaum L, McNeely E. PBDE flame retardants, thyroid disease, and menopausal status in U.S. women. Environ Health. 2016;15(1):60.
Kodavanti PR, Coburn CG, Moser VC, MacPhail RC, Fenton SE, Stoker TE, Rayner JL, Kannan K, Birnbaum LS. Developmental exposure to a commercial PBDE mixture, DE-71: neurobehavioral, hormonal, and reproductive effects. Toxicol Sci. 2010;116(1):297–312.
Zhou T, Ross DG, DeVito MJ, Crofton KM. Effects of short-term in vivo exposure to polybrominated diphenyl ethers on thyroid hormones and hepatic enzyme activities in weanling rats. Toxicol Sci. 2001;61(1):76–82.
Meerts IA, van Zanden JJ, Luijks EA, van Leeuwen-Bol I, Marsh G, Jakobsson E, Bergman A, Brouwer A. Potent competitive interactions of some brominated flame retardants and related compounds with human transthyretin in vitro. Toxicol Sci. 2000;56(1):95–104.
Ren XM, Guo LH. Molecular toxicology of polybrominated diphenyl ethers: nuclear hormone receptor mediated pathways. Environ Sci Process Impacts. 2013;15(4):702–8.
Lim JS, Lee DH, Jacobs DR Jr. Association of brominated flame retardants with diabetes and metabolic syndrome in the U.S. population, 2003-2004. Diabetes Care. 2008;31(9):1802–7.
Warner M, Rauch S, Coker ES, Harley K, Kogut K, Sjodin A, Eskenazi B. Obesity in relation to serum persistent organic pollutant concentrations in CHAMACOS women. Environ Epidemiol. 2018;2(4):e032.
Ongono JS, Dow C, Gambaretti J, Severi G, Boutron-Ruault MC, Bonnet F, Fagherazzi G, Mancini FR. Dietary exposure to brominated flame retardants and risk of type 2 diabetes in the French E3N cohort. Environ Int. 2019;123:54–60.
Erkin-Cakmak A, Harley KG, Chevrier J, Bradman A, Kogut K, Huen K, Eskenazi B. In utero and childhood polybrominated diphenyl ether exposures and body mass at age 7 years: the CHAMACOS study. Environ Health Perspect. 2015;123(6):636–42.
Vuong AM, Braun JM, Sjodin A, Webster GM, Yolton K, Lanphear BP, Chen A. Prenatal polybrominated diphenyl ether exposure and body mass index in children up to 8 years of age. Environ Health Perspect. 2016;124(12):1891–7.
Vuong AM, Braun JM, Wang Z, Yolton K, Xie C, Sjodin A, Webster GM, Lanphear BP, Chen A. Exposure to polybrominated diphenyl ethers (PBDEs) during childhood and adiposity measures at age 8 years. Environ Int. 2019;123:148–55.
Malarvannan G, Van Hoorenbeeck K, Deguchtenaere A, Verhulst SL, Dirinck E, Van Gaal L, Jorens PG, Covaci A. Dynamics of persistent organic pollutants in obese adolescents during weight loss. Environ Int. 2018;110:80–7.
Staskal DF, Hakk H, Bauer D, Diliberto JJ, Birnbaum LS. Toxicokinetics of polybrominated diphenyl ether congeners 47, 99, 100, and 153 in mice. Toxicol Sci. 2006;94(1):28–37.
Fernie KJ, Laird Shutt J, Ritchie IJ, Letcher RJ, Drouillard K, Bird DM. Changes in the growth, but not the survival, of American kestrels (Falco sparverius) exposed to environmentally relevant polybrominated diphenyl ethers. J Toxicol Environ Health A. 2006;69(16):1541–54.
Kamstra JH, Hruba E, Blumberg B, Janesick A, Mandrup S, Hamers T, Legler J. Transcriptional and epigenetic mechanisms underlying enhanced in vitro adipocyte differentiation by the brominated flame retardant BDE-47. Environ Sci Technol. 2014;48(7):4110–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Choi, K., Kim, S. (2020). Brominated Flame Retardants (BFRs). In: Kishi, R., Grandjean, P. (eds) Health Impacts of Developmental Exposure to Environmental Chemicals. Current Topics in Environmental Health and Preventive Medicine. Springer, Singapore. https://doi.org/10.1007/978-981-15-0520-1_14
Download citation
DOI: https://doi.org/10.1007/978-981-15-0520-1_14
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-15-0519-5
Online ISBN: 978-981-15-0520-1
eBook Packages: MedicineMedicine (R0)