
Abstract
Air pollution is a complex mixture of gaseous, volatile, and particulate matter (PM) containing inorganic and organic species. There is now abundant evidence in epidemiological and toxicological studies that air pollution contributes to the development and exacerbation of diseases of respiratory, cardiovascular, and other organs, and associated mortality. Studies showed that equal masses of PM could induce disparate health effects, suggesting that particle sizes and components may be at fault. The fine and ultrafine PM is considered to be particularly important because the small particles can be easily inhaled. Possible biological mechanisms of action leading to adverse effects include the production of inflammatory mediators in the lung causing systemic inflammation, interaction with neural receptors causing interference with the central nervous system regulation of cardiovascular function, and particle translocation via the bloodstream to other organs. This chapter reviews whether some components of the PM mixture are of a greater public health concern than others, and presents compelling evidence that trace elements are most strongly linked to the adverse effects. Air pollution has wide-ranging and harmful effects on human health and is a major issue for the global community. Further research should explore the effects of source-specific PM with more advanced approaches to exposure modeling, measurements, and statistics, which would lead to more effective legislation and interventions for greater benefits to public health.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

1 Background on PM2.5: Global Pollution Hotspots, Multi-facets of PM2.5 in Physical, Chemical, and Biological Dimensions, and Key Review Question: The Importance of Trace Metals in Exposure and Effects of PM2.5
Numerous epidemiological and laboratory studies linked particulate matter (PM) exposure to health effects (Pope et al. 2002; Lippmann 2014; Kim et al. 2015; Thurston et al. 2017) and subsequently led to worldwide regulations on air pollution. Air pollution particles penetrate deep into the lungs and cardiovascular system, causing conditions including stroke, heart disease, lung cancer, chronic obstructive pulmonary diseases and respiratory infections like pneumonia. Additionally, fine particulate matter is responsible for environmental effects such as corrosion, exterior building erosion, damage to vegetation and reduced visibility.
World Health Organization (WHO) states that outdoor and indoor air pollution is the biggest environmental risk to health as it affects practically all countries in the world, and is responsible for about one in every nine deaths annually (WHO 2016). Using the data derived from satellite measurements, air transport models and ground station monitors for more than 3000 locations, both rural and urban, the report estimated that only one-tenth of the urban population lives in areas that comply with the WHO air quality guidelines. The highest ambient air pollution levels are in the Eastern Mediterranean Region and in South-East Asia, with annual mean levels often exceeding more than 5 times WHO limits, followed by low and middle-income cities in Africa and the Western Pacific. In 2018, air pollution contributed to approximately 24% of all adult deaths from heart disease, 25% from stroke, 43% from chronic obstructive pulmonary disease and 29% from lung cancer (WHO 2018). The more recent Global Burden of Diseases, Injuries, and Risk Factors Study 2015 further updated the annual mortality due to PM2.5 (PM with an aerodynamic diameter less than 2.5 µm) exposures to about 4.2 million per year (Cohen et al. 2017). This study also confirmed that while the global rate of mortality due to PM2.5 decreased since 1990, the absolute number of deaths increased due to population growth and increased pollution in the south and east Asia.
Generally, ambient airborne PM is grouped as coarse, fine, and ultrafine particles (UFPs) with aerodynamic diameters within between 10 and 2.5 μm, less than 2.5 μm (PM2.5), and less than 0.1 μm (PM0.1), respectively. The current mass-based PM standards by the World Health Organization (WHO), U.S. Environmental Protection Agency (EPA), and European Environment Agency (EEA) apply to PM10 and PM2.5. Contrastingly, the UFPs are not a criteria pollutant and thus are not routinely monitored. The reason for the specific size range standards is based on human physiology—coarse PM is mainly deposited along the conductive airways in the thorax, while nearly all of PM2.5 penetrates into the gas-exchange region in bronchi where particle retention times are much longer. Both PM10 and PM2.5 are removed mainly by mucociliary clearance and phagocytosis. The UFPs deposit at much higher rates in the bronchioles and alveoli, where, due to their small size, they can then penetrate biological membranes, pass into the systemic circulation, overcome the placental barrier and finally diffuse into all organ systems including the brain and nervous system (Ohlwein et al. 2019; Heinzerling et al. 2015).
A 2016 review of air quality standards in 194 countries by Kutlar et al. showed that only 39 countries worldwide have a PM2.5 24-hr (mean of 24 h) standard and 101 countries have PM10 24-hr standard. These standards vary greatly between the countries and regions, with the largest differences in air quality standards seen between high and low-income countries. A small selected subset of PM standards is shown in Table 1. Among countries with standards for 24-h averaging times for PM2.5 and PM10, 21% and 46%, respectively, met the WHO guideline values (Kutlar et al. 2017).
The concentration, composition, and size distribution of atmospheric aerosol particles are temporally and spatially variable. Generally, ambient PM is a very complex mixture of different size particles from different origins, and therefore, of different composition. Major sources of outdoor PM include fuel combustion from motor vehicles (e.g., cars and heavy-duty vehicles), heat and power generation (e.g., oil and coal power plants), industrial facilities (e.g., manufacturing factories, mines, and oil refineries), municipal and agricultural waste sites and waste incineration/burning, residential use of fuels (cooking, heating, and lighting). In some regions, additional, if not main, sources of ambient pollution are desert dust, waste burning and deforestation (WHO 2018). Furthermore, air quality is also affected by natural elements such as geographical (e.g., mountain ranges and valleys that obstruct natural air flow), meteorological and seasonal factors (e.g., amount of sunshine that enhances photochemistry and contributes to secondary aerosol formation, and relative humidity that contributes to particle growth and formation of acidic aerosols).
Although regulatory standards are mass-based, there is an overwhelming agreement that the human health effects should not be attributed simply to the total mass concentration but various PM components causing toxicities (Lippmann 2010; Lippmann et al. 2013; Cassee et al. 2013). The type and extent of health effects are investigated on their dependence on both chemical composition (such as transition metals, organic compounds, and other combustion-produced particles) and physical properties (size, particle number, and surface area). For monitoring purposes, the main constituents of PM are inorganic salts (sulfates, nitrates, ammonium, sodium chloride), organic compounds, black carbon, and mineral dust, including trace elements and metals (Adams et al. 2015). This composition is size-dependent: coarse PM is produced by abrasive physical events such as weathering, crushing, and grinding and is therefore mostly composed of minerals, bioaerosols (bacteria, pollen, fungi, vegetation litter), black smoke, and large sea salt particles. The coarse particles usually contribute the largest proportion of PM mass but little to the particle number. PM2.5 is derived mainly from combustion-related sources, and thus often includes particles with a carbon core that carries organic compounds and metals, as well as secondary particles chemically transformed from oxides of sulfur and nitrogen.
Recently, there has been an increased interest in human exposure to ultrafine particles (UFPs, smaller than 0.1 μm). In the ambient atmosphere, UFPs originate broadly from two sources: as a submicrometer fraction of fine particle emissions, and from engineered nanomaterials. For the first group, vehicle emissions, are the primary source of the submicron ultrafine particles by both internal combustions and by operational mechanical friction in motors. The potential for exposure to these sources is very large—in the United States, approximately 45 million people live, work, or attend schools within 300 feet of a major road, airport or railroad (EPA 2014). Additionally, an average American spends about an hour in daily travel or commute, most of which takes place on major roadways. Emitted primary ultrafine particles are transformed rapidly due to coagulation, adsorption, and secondary particle formation, especially in the areas with high potential for photochemical reactions. Therefore, ultrafine particles have greater spatial and temporal variability than fine particles. The second type of sub-micron ultrafine particles, engineered nanoparticles, have become more widely used in manufactured goods and consumer products, such as food additives, pharmaceuticals, and drug delivery systems, cosmetics, as well as in materials for optical and electronic devices. The increasing popularity is due to the particle size which brings unique advantages to the products. For example, titanium or zinc oxide nanoparticles in new sun-blocks do not cause skin to appear with a white coating, as these particles do not reflect visible light. These new products eventually enter the environment through sewage (for example, washed off sunblock or silver particles from hand sanitizers) or as refuse waste. Less than 3% of incinerated nanomaterial is thought to enter the atmosphere (Keller and Lazareva 2014), which would lead to inhalation exposure to these particles as well as their combustion byproducts.
2 From Occurrence to Exposure
2.1 A Global Overview of Chemical Compositions of PM2.5 and the Share of Trace Metals
A substantial fraction of fine and ultrafine particles is composed of primary emissions of various combustion processes such as fossil fuel combustion and high-temperature industrial processes, as well as the secondary transformation of organic volatiles from natural and anthropogenic sources. While the specific physical and chemical properties of particles, as well as the sources of these particles, are under constant investigation, it is unlikely that any single chemical component of PM is responsible for all adverse health outcomes. Many investigations prefer to focus on types of chemicals—namely ultrafine particles, bioaerosols, polycyclic aromatic compounds, and transition metals—known to have specific health effects (induction of inflammation and oxidative stress).
The chemical composition of PM2.5 offers valuable information to identify the contributions of specific sources and to understand aerosol properties and processes that could affect air quality index and health. While more than 4300 cities in 108 countries have some sort of monitoring devices and contribute to WHO’s ambient air quality database, Africa and some of the Western Pacific have a serious lack of air pollution data (WHO 2018). The lack of PM2.5 and chemical speciation monitors is attempted to be supplemented with satellite remote sensing technology and modeling. This approach demonstrates that the addition of even a few ground-based PM monitors to more globally continuous aerosol optical depth satellite data can yield valuable improvements to PM2.5 characterization on a global scale. Van Donkelaar et al. (2016) estimated that global annual average PM2.5 concentration for 2010 was 32.6 μg m−3, or three times higher than the 10 μg m−3 WHO guideline, with typical concentrations 20-70 μg m−3 in South and East Asia. Using a population density model, they reported that only 13% of the global population lived in areas below the 10 μg m−3 WHO guideline, with 52% of the high-income North America population living in cleaner air, compared to 1% or less of South Asia, East Asia, and North Africa/Middle East.
Depending on location and season, the PM2.5 chemical components could vary by more than an order of magnitude between sites. For example, the SPARTAN study of the global chemical composition of PM2.5 (Snider et al. 2016) involved 12 globally dispersed, densely populated urban locations in a variety of geographic regions including partial desert (Ilorin, Rehovot, Kanpur), coastline (Buenos Aires, Singapore), and developing megacities (Dhaka). The geographical variability resulted in the PM2.5 mass concentrations spanning an order of magnitude, from under 10 μg m−3 (e.g., Atlanta) to almost 100 μg m−3 (Kanpur). The SPARTAN analysis of global chemical composition of PM2.5 over periods of 2–26 months between 2013 and 2016 tabulated the major constituents as follows (relative contribution ± SD): ammoniated sulfate (20% ± 11%), crustal material (13.4% ± 9.9%), equivalent black carbon (11.9% ± 8.4%), ammonium nitrate (4.7% ± 3.0%), sea salt (2.3% ± 1.6%), trace element oxides (1.0% ± 1.1%), water (7.2% ± 3.3%) at 35% RH, and residual matter (40% ± 24%). The crustal material was defined as elements Mg, Fe, and Al; trace elements included Zn, V, Ni, Cu, As, Se, Ag, Cd, Sb, Ba, Ce, and Pb. The “residual matter” was most likely not fully characterized as an organic fraction, some components of which are known to be toxic to humans or the environment. For example, it may contain persistent organic pollutants, a category that encompasses pesticides and polycyclic aromatic hydrocarbons, among other toxic species. Curiously, at all sites the ratio of coarse- and fine-PM mass fraction was about 1:1, thus indicating the importance of both anthropogenic and natural sources of the pollution. It was found that ammonium sulfate correlated well with PM2.5 mass while other components had much higher spatial and temporal variability: nitrate absolute values range over 30-fold with additional variability attributed to season; crustal material did not show a clear pattern and was attributed to regional dust as well as (up to 80% in some urban locations) local dust; mass fractions of elemental black carbon ranged from 4% (Singapore) to 25% (Manila); trace elements and sea salt contributions were generally very small. The residual mass (mostly organic) contributed from 30 to 60% mass depending on location.
One of the persuasive studies of the spatial and temporal variation in PM in the United States comes from Bell (2012) who analyzed data on PM2.5 total mass and on the mass of 52 chemical components of PM2.5 for 187 counties in the continental U.S. for the period 2000–2005. In this study, Bell has shown that concentrations of PM2.5 components vary across counties and regions of the United States as well as over seasons. Her analysis of the seven components making up most of the PM2.5 mass found patterns similar to those in other studies. Organic carbon matter, nitrate, and elemental carbon were generally higher in the West than in the East, with some seasonal differences; sulfate was higher in the East, particularly in summer; and sodium ion appeared most prominently along the coasts. Additionally, Bell has demonstrated that relationships between daily PM2.5 total mass concentrations and hospitalizations for cardiovascular and respiratory disease also vary over season and region. Hospitalizations for respiratory disease were most pronounced on the second day after exposure to PM2.5 total mass and seasonally were largest in the winter with same-day PM2.5 exposures. Cardiovascular admissions in the main models were associated with same-day exposures to PM2.5 total mass were largest in winter and these increases were greatest across the Northeast U.S., while the seasonal model increases in cardiovascular admissions were observed only for the Northeast region and in all seasons.
Furthermore, the PM toxicity varies depending on its size distribution and chemical composition—properties associated with specific sources—and the PM health effects research is increasingly focused on source-apportionment of PM using chemical speciation data. Source-apportionment receptor models provide estimates of the contributions of various source categories to ambient air pollution at a given location at a given time. Various sources are distinguishable by the source apportionment because they have distinctive tracers and correlations that are closely associated with each source profile.
For example, further interpretation of the SPARTAN measurements with the global chemical transport model led to insights into seven sources affecting each site (Weagle et al. 2018): six primarily anthropogenic categories and one “other sources” category. The primary anthropogenic categories, which contribute 76% of global PM2.5 exposures are residential energy use (21%), industry (18%), power generation (15%), agriculture (9%), transportation (8%), and open fires (5%).
The importance of such investigations is that resolution of the composition of PM into components related to emission source categories and identification of the most causal source categories and/or specific PM components responsible for most of the adverse health effects would permit more focused control of those causal PM2.5 components. A recent review of 280 articles published in 1966–2016 on epidemiological evidence of health effects associated with exposure to PM air pollution from five common outdoor emission sources (traffic, coal-fired power stations, diesel exhaust, domestic wood combustion heaters, and crustal dust) failed to rank them in the order of harmfulness, but indicated that PM from traffic and coal-fired power station emissions may elicit greater health effects compared to PM from other sources (Hime et al. 2018). Understanding the components and sources of PM2.5 that are most harmful to human health is critical for the development of air pollution regulations and environmental policies that maximize health benefits. The mortality risk estimated in the Dutch mortality cohort study for PM2.5 was 6% per 10 µg m−3 for natural-cause mortality (Beelen et al. 2008), identical to the estimate from the American Cancer Society study (Pope et al. 2002), while rates of lung cancer associated with PM10 in 17 European cohorts were 22% per 10 µg m−3 (Ole Raaschou-Nielsen et al. 2013). Even a 20% reduction in global anthropogenic emissions could reduce premature deaths in Europe by 54000 and in the U.S. by 27500 (Im et al. 2018).
2.2 Geographical Fingerprints of Metal Profiles in PM2.5 and Implications for Site-Specific Human Exposure
A joint statement from the European Respiratory Society and American Thoracic Society seeks to further clarify a general framework for interpreting the adverse human health effects of air pollution (Thurston et al. 2017). The statement pointed out that most of the data from epidemiological studies of PM effects has been collected in Europe and North America. Even these studies, which aimed to identify which PM components and sources were associated with a variety of adverse health outcomes, met with mixed results; an unsurprising result when the differences between them are taken into account. These include variations in study time, differences in the selection of PM components and health outcomes of interest, and uncertainty regarding estimates that stem from small data sets on PM composition and sources.
There are only a few long-term epidemiological studies that included a PM components other than PM mass (Wyzga and Rohr 2015). A study by Bell (2012) of daily hospital admissions for cardiovascular- and respiratory-related illnesses for 1999–2005 Medicare enrollees aged 65 years or older showed that only variability in elemental carbon explained variation in PM2.5 mass effect estimates for hospitalization. For the remaining components studied, Bell reported that greater concentrations of Ni and V in PM2.5 were associated with larger PM2.5 total mass health effect estimates for both cardiovascular and respiratory hospitalizations. PM10 mass associations with total non-accidental mortality were also larger in regions and seasons with higher fractions of V and notably Ni in PM2.5. Lipfert et al. (2009) looked into correlations of total mortality among a group of U.S. male veterans with hypertension to several components of PM2.5, including some metals, elemental carbon (EC), anions, some organic compounds, and polycyclic organic matter. They found no significant association between PM2.5 mass and mortality, but significant associations with “diesel particulate matter,” nitrate, EC, Ni, Pb, formaldehyde, benzene, polycyclic organic matter, while sulfate showed a significant negative association with mortality. Ostro et al. (2010, 2011) in a study of female teachers in California found all measured PM components (PM2.5 mass, EC, organic carbon (OC), sulfate, Fe, K, Si, Zn) correlated with ischemic heart disease deaths; but only PM2.5 mass, sulfate, nitrate, and Si were significantly associated with cardiopulmonary deaths and no significant associations for all-cause and pulmonary mortality. The city–season specific Poisson regression of mortality in 75 U.S. cities for 2000–2006 found that Si, Ca, and S were associated with more all-cause mortality, whereas S was related to more respiratory deaths (Dai et al. 2014). Thurston et al. (2013) used two models to examine the association between mortality among a group of individuals in the American Cancer Society cohort and multiple components of PM2.5 (mass, many elements, EC, OC) as well as the sources of PM2.5 modeled by source apportionment. For all-cause mortality, significant associations were found for the traffic and coal combustion factors, PM2.5 mass, As, Se, EC, and S. Respiratory mortality was significantly associated with the traffic factor, PM2.5 mass, Ca, Si, and OC, while associations with Cl and Ni were significantly negative. Ischemic heart disease was significantly associated with metal, traffic, and coal combustion factors, PM2.5 mass, As, Cl, Fe, Pb, Ni, Se, Zn, EC, and S. Subclinical markers for cardiovascular disease were examined in the Multi-Ethnic Study of Atherosclerosis cohort with no previous history of cardiovascular disease in 6 U.S. cities (Vedal et al. 2013), and were found in significant associations with PM2.5 mass, S, OC, and Cu for carotid intima-media thickness, and with Ni, Cu, and Ca, or V, depending on the model, for coronary artery calcium marker. Among the PM2.5 components measured during 1998–2013 in the Atlanta area, water-soluble Fe had the strongest estimated effect on emergency department visits for cardiovascular diseases, while in 2008–2013, water-soluble V was associated with cardiovascular visits (Ye et al. 2018). Results from 19 European cohorts by Wang et al. (2014) found no associations between cardiovascular deaths and several measured trace elements (Cu, Fe, K, Ni, S, Si, V, and Zn). In one example of non-cardiovascular study, low birth weight of infants born to mothers living in California was associated with multiple components (including Br, Cl, Cu, EC, Fe, Pb, Mn, Ni, V, Ti, Zn, K, Na, ammonium, sulfate, and nitrate) and PM2.5 mass.
These studies demonstrated that metals, especially transition metals, can explain most, if not all of the health effects observed in epidemiological studies. As suggested by US EPA ISA for PM, reduction of this category of compounds would most likely lead to mitigating the health effects of air pollution (EPA 2009).
While several studies confirmed the public health benefits of clean air policies that improved air quality, the question remains on whether and what adverse effects occur at lower air pollution concentrations. As described before, the PM composition in the western hemisphere does not necessarily depict PM in other countries, for which such information is not widely available but modeled; thus, PM-health relationship derived in the developed world might not be directly applicable to the differing pollution composition and concentrations, as well as the differing demographics (e.g., age and income), of non-Western countries. To resolve such uncertainties in at least laboratory settings (sans demographic differences), several approaches could prove useful, such as a multi-cities comparison of air-volume based exposure, which would indicate the effects of PM by mass; alternatively, a multi-cities comparison of the mass-normalized health endpoints could also prove useful, indicating intrinsic PM composition effects.
For example, these approaches were used in measurements of biological oxidative potential (by macrophage reactive oxygen species (ROS) assay) associated with size-segregated airborne PM (PM10–2.5, PM2.5, PM0.25) in six urban areas of the world (Los Angeles, USA; Denver, USA; Beirut, Lebanon; Milan, Italy; Thessaloniki, Greece; Lahore, Pakistan) (Saffari et al. 2014). They found that larger ROS activity depended on mass concentration only for a coarse fraction but not for finer fractions, in which composition was more important. This was attributed to higher concentrations of water-soluble metals (most notably Fe—vehicular tracer, and Ni and V—residual oil combustion tracer, or both) and organic carbon in smaller sized PM. For coarse PM10–2.5 the ROS activity was generally lower, except when in presence of metals Cu, Co, and Mn from resuspended soil and dust, and vehicular abrasion.
Developed concentrator technology (Siotas et al. 1999; Gupta et al. 2004) for conducting inhalation exposure studies of concentrated ambient particles (CAPS) in laboratory animals (Maciejczyk et al. 2005), cell, and human volunteers created a new opportunity to quantitatively link the PM exposure to the biomarkers of health effects. Using a mouse model (ApoE−/− mice, bred to develop atherosclerotic plaque similar to that observed in humans with atherosclerosis) subchronically (6 h/d, 5d/wk, for 6 months) exposed to CAPS at locations with different PM2.5 compositions, Chen and Nadziejko (2005) demonstrated that components attributable to source categories for residual oil combustion (Ni, V, and S), coal combustion (S and Se), and traffic (EC, Al, and P) appeared to be the most influential in altering heart rate and heart rate variability in these mice. Follow-up CAPS studies were done at five different sites across the United States which represented ambient pollutant mixtures from diverse locations and dominated by different source categories, including coal combustion, wood smoke, and traffic. In terms of atherosclerotic plaque progression, it was notable that plaque progression occurred at the three sites with exposure to coal combustion emissions and was lacking at the two sites without such exposure (Lippmann et al. 2013).
Overall, it appears that the cardiovascular effects of ambient air PM2.5 are influenced, if not dominated, by their metal contents, especially the transition metals, and that nickel is likely to be a key component (Lippmann and Chen 2009).
2.3 Size-Specific Relative Enrichment of Anthropogenic Versus Crustal Metals Entails Implications for Element-Specific (Toxic vs. Non-toxic Metals) Exposure
While fine and ultrafine particles are mainly of anthropogenic combustion origin, coarse PM (PM10–2.5), besides some black smoke and some secondary particles, also includes the significant fraction of the mechanically generated particles from crustal sources such soil, dust from roads and building sites, and large sea salt particles. In epidemiological studies, the association between coarse PM10–2.5 and health are more difficult to find (WHO 2013) since PM10-2.5 is actually not measured but is calculated by subtracting measured PM2.5 from measured PM10. This difficulty in separating the possible contributing effect of PM2.5 increases the uncertainty in modeling the associations between coarse PM and hospital admissions. Nevertheless, EPA integrated science assessment for PM concluded that, in general, short-term coarse PM exposures had positive associations for cardiovascular and respiratory health effects and mortality (EPA 2009).
Exposure to coarse PM was linked to inflammatory effects in the lung (Wegesser et al. 2008), cardiovascular mortality (Malig and Ostro 2009), and decreased heart rate variability (Lipsett et al. 2006). Giannadaki et al. (2014) and Lelieveld et al. (2015) estimated that premature mortality attributable to natural dust is between 400 and 500 thousand per year, contributing ∼18% to the total premature mortality attributable to air pollution. Locally, the contribution of natural dust can reach up to 90% of the total premature mortality due to air pollution, mostly in countries located in and around the dust belt zone in Africa, the Middle East, and Asia. The causal effect of desert dust might not necessarily be due to mineral composition or overall load—at least two studies identified the presence of microorganisms and viable pathogens in Iraq, Kuwait, and African dusts (Godleski et al. 2011; Polymenakou et al. 2008).
Clinical studies have reported that coarse particles can be as toxic as PM2.5 on a mass basis (reviewed by Cassee et al. 2013). The difference in risk between coarse and fine PM may at least partially be explained by differences in intake and different biological mechanisms. However, toxicological studies on the effects of coarse particles are scarce. The few studies available usually collected PM on filters and used in vitro assays or intratracheal exposures for assessment, often in relation to the sources of emission. For example, coarse (PM10–2.5) and fine (PM2.5) PM samples from various locations in the New York City metropolitan area were assessed for their ROS response in the cell model and pro-inflammatory response in mice by oropharyngeal aspiration (Mirowsky et al. 2013). There, PM2.5 was found to elicit a greater in vitro ROS response compared to PM10–2.5. Endotoxin in the NYC samples was correlated only with a pro-inflammatory-related response in mice.
Contrasting results were reported from a study of coarse and fine PM samples collected at 5 diverse sites within California (Mirowsky et al. 2015), where PM10–2.5 elicited the greatest ROS response in the cells, especially for the urban locations, and also the greatest increase pro-inflammatory-related response in mice, with the exception of the rural ocean-side location. Elements associated with soil and traffic markers were most strongly linked to the adverse effects in vitro and in vivo. Interestingly, super-coarse PM (i.e., PM > 10 μm) produced as great, or more, of an inflammatory response in the mouse lung, a somewhat puzzling result since these super-coarse particles deposit largely in the upper respiratory tract. In contrast to Middle East desert dust studies, the California study only found associations between endotoxin and ROS response in the cell model failing to do so in the mouse model. Collectively this evidence points out that particle sources might be more influential than size when determining toxicity as trace elements.
3 From Exposure to Bioavailability
3.1 Defining Bioavailablity Based on Target Sites: Regional Deposition of Airborne Metals in Respiratory Tracts—Which Part of the Airway Is Vulnerable to Exposure to Inhalable Metals?
The assessment of adverse health effects of outdoor air pollution has historically focused on respiratory health outcomes. However, more recently, associations have also been reported for cardiovascular and other systemic or metabolic effects such as diabetes, neurological, and developmental outcomes. According to a joint ERS/ATC statement, the list of detectable air pollution health effects continues to expand, making a determination of the adversity of these numerous effects more and more important (Thurston et al. 2017). So the question is how do we go from respiration into multiple pathophysiological pathways that include systemic inflammation, oxidative stress, immune modulation, and epigenetic alteration? Different deposition patterns of fine and coarse particles were documented (ICRP 1994), with coarse particles having a higher deposition probability in the upper airways and the bronchial tree. Particles deposited in the upper airways are cleared rather rapidly from the respiratory tract via mucociliary clearance and macrophage transport. These deposition and clearance mechanisms explain the short-term health effects of PM10 and coarse PM. However, cardiovascular disease exacerbation could be activated by the autonomous nervous system via irritant receptors in the upper airways (Brook et al. 2010; Peters et al. 2006). Therefore, coarse particles may induce health effects by different mechanisms than fine and ultrafine particles and potentially relate to different health outcomes. Happo et al. (2010) intratracheal instilled mice (10 mg/kg) with size-segregated ambient PM samples collected in six European cities over various seasons and found the overall inflammatory activity of PM decreased with particle size, such that PM10–2.5 and PM2.5-1 had a higher potency than PM1–0.2 and PM0.2. The PM10-2.5 inflammatory response strongly correlated with source tracers for soil (K, Mg, Cu, Mn, Fe) and sea spray (Na, Cl, nitrate), while PM2.5-0.2 inflammatory response strongly correlated with oxidized organic compounds, transition metals (e.g., Fe and Cr), and source tracers for fuel oil combustion (Ni and V).
On the other end of the particle size spectrum, while larger particles such as PM10, PM10-2.5, and PM2.5 dominate mass-based metrics, ultrafine particles (smaller than 0.1 µm) contribute very little to PM mass. Recent toxicological studies showed that this size fraction acts through mechanisms not shared with larger particles, but their toxicity is depending on size, composition, surface area and surface charge (WHO 2013). The toxicity mechanism of the UFPs will be discussed later in the text.
3.2 Defining Bioavailability Based on Chemical Speciation: Insoluble, Soluble Metal-Ligand Complex, Freely-Dissolved—Which Form of the Inhaled Metals Are Mostly Available for Bio-Uptake?
The problem of toxicity is rooted in PM complexity: ambient particles come in a variety of sizes, shapes, and surface coatings, all of which affect their bioactivity. For example, sulfuric acid layered ultrafine ZnO particles have been shown to give a proportionally greater pulmonary response than conventionally generated sulfuric acid mist of comparable size (Amdur and Chen 1989), suggesting that transition metals dissolved in the acid layer may be made bioavailable and render their higher pulmonary toxic.
The initial surface chemistry of the particles clearly influences their fate and distribution in biological systems upon immersion into biological fluids. The toxicity of PM may not necessarily be the cumulative toxicity of its components, since at least some of the PM components cannot dissolve in bronchial fluid and ultimately penetrate the air/blood interface. Although redox-active transition metals generally account for a small fraction of the total PM mass (10%), they are among the major drivers of PM-induced oxidative potential. Water-soluble transition metals (e.g., Fe, Ni, Cu, Cr, Mn, Zn, and V) and water-soluble organic carbon showed consistent correlations with the oxidative potential of airborne PM across different urban areas and size ranges (Saffari et al. 2014). Compared to their insoluble counterparts, soluble metals are generally more likely to quickly enter into the systemic circulation and be translocated to other organs such as the heart upon uptake in the lung. However, the extent of the solubility of all constituents of ambient PM by lung fluids is not well determined, especially for organic substances.
One of the main problems is the lack of a standardized in vitro bioaccessibility method, as recently pointed out in an extensive review of 96 relevant articles (Wiseman 2015). The currently favored water extraction method is practical and cheap, yet might not be physiologically relevant, especially since it hardly accounts for the effect of temperature on metal ion solubility. The aqueous leaching of metals from PM could be further hampered from additional pH effects due to hydrolysis of the ions present. The bronchial alveolar fluid, on the other hand, contains surfactant proteins, phospholipids, ions, and other substances, all of which could affect the solubility of PM. For example, a comparison of four different Standard Reference Materials (SRMs): NIST 1648a (urban PM), BCR 038 (fly ash powder), NIES 8 (vehicle exhaust particulates) and NIST 2584 (indoor dust), reported mean increases of soluble elemental fractions in the amount of 40, 67, 39 and 59% for the SRMs extracted with a simulated biological fluid relative to water, respectively (Davies and Feddah 2003). Recognizing the limitations of aqueous extractions, the researchers rely on the use of two simulated biological fluids—Gamble’s solution and artificial lysosomal fluid (ALF). The electrolytic composition of Gamble’s solution was designed to be virtually identical to human interstitial lung fluid, while ALF was to simulate the acidic conditions which exist during phagocytosis by alveolar and interstitial macrophages (see review by Wiseman 2015, for variable compositions of both). Unfortunately, the different pH and composition of these leaching solutions make it difficult to cross-compare the extraction efficiencies used in different studies. For example, higher solubility of Ni, Cu, and Zn was observed in the modified Gamble’s solution containing cysteine and glutathione due to the formation of soluble complexes of these metals with thiol groups (Voutsa and Samara 2002). Further complications in comparison arise from differences in length of extraction, the ratio of PM to liquid, mechanical equipment used (shaking, sonication, etc.), and sensitivity of the follow-up chemical analysis method (Wiseman 2015; Leclercq et al. 2017).
Despite these difficulties, interesting metal bioavailability results appear from a comparison of dusts collected in different locations. In one such study, three SRMs: BCR-723 (road dust collected in Austria with a particle size fraction of <90 µm and a median value of 14.6 µm), NIST 2710a (soil particles collected in the USA with a particle size fraction of <74 µm), and NIST 1648a (urban atmospheric particulate matter collected in the city of St. Louis, MO, USA with a particle size fraction of <100 µm and a median value of 5.85 µm), were selected to assess bioaccessibility of metals using several dissolution media (PBS, Gamble’s solution, modified Gamble’s solution and ALF) (Pelfrêne et al. 2017). Total release of elements Ba, Cd, Cu, Mn, Ni, Pb and Zn in the three SRMs decreased according to the following sequence: ALF > Gamble’s solution > PBS. High variability of Co and Sr bioaccessibility was recorded between the three fluids and within each fluid, while Cr was only soluble less than 10% all across. In ALF (acidic pH), metal solubilities of NIST 1648a were Cu 55%, Mn 47%, and Ni 12%, while for BCR-723 they were 65%, 5%, and 24%, respectively. The different percentages of metallic elements release could be attributed to differences in the source (St. Louis ambient PM vs. Austria road dust), and chemical tendencies of metal to form soluble complexes and transformations in the lung environment. Metal oxides (possibly formed in high-temperature combustion, but also crustal), chlorides, carbonates can be generally easily dissolved in lung fluids, while metal sulfides, phosphates, and silicates (many of crustal origin) are common insoluble compounds. Sholkovitz et al. (2012) reflected on a remarkable systematic trend: an inherently higher solubility of Fe in aerosols derived from anthropogenic and natural combustion sources compared to lithogenic dust derived from arid continental soils. Their combined analysis for Fe total load and Fe solubility in ∼1100 samples collected by multiple researchers over the open ocean, the coastal ocean, and continental sites revealed the inverse trends for anthropogenic (low load – high solubility) and lithogenic (high load – low solubility) PM over regional and global scales despite significant differences in when and how the samples were collected and stored, and in leaching techniques and solutions that have been used to define ‘soluble’ iron. They also noted that the solubility of Fe (and thus, possibly of other metals) in lithogenic aerosols can increase when mixed with acidic anthropogenic aerosol (Sholkovitz et al. 2012).
In one of the few studies which examined multi-element solubility in field-collected airborne PM using simulated lung fluids, the soluble fractions of As, Ce, Co, Cr, Cu, Mn, Ni, Pb, Sb, Ti, and V were analyzed in airborne PM10, PM2.5 and PM1 from Frankfurt, Germany (Wiseman and Zereini 2014). Overall, filters extracted with the acidic ALF yielded more soluble metal fractions when compared to the neutral Gamble’s solution. Interestingly, Sb, Pb and As were observed to be the most soluble in all airborne PM fractions. For example, after 24 h in ALF, Pb (an element of well-established health concern) had a mean soluble fraction of 96% in PM10, 84% in PM2.5 and 78% in PM1. Among other metals in PM10, PM2.5, and PM2, the mean soluble fraction of Ni was 52%, 25%, and 35%, respectively, while for Cu, they were consistently more than 80% all across. Leclercq et al. (2017) found that LHC-9 culture medium appears to be a good physiological proxy to human respiratory mucus collected from COPD patients for most metals. They tested the in vitro pro-inflammatory responses of soluble, insoluble, and total PM2.5, and found that both soluble and insoluble fractions induced cell inflammatory responses although their cumulative response did not correspond to the one by the total fraction. The authors suggested that the inflammation could be not only linked to the presence of some of the metals contained in soluble and insoluble fractions of PM2.5, but also to the presence of organic chemicals in its insoluble fraction.
4 From Bioavailability to Toxicity
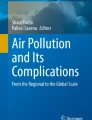
Air pollution plays an important role in the development and exacerbation of respiratory diseases, such as asthma, chronic obstructive pulmonary disease (COPD), and lung cancer (EPA 2009). In the past several decades, other adverse effects were documented, and the European Respiratory Society and the American Thoracic Society proposed a set of considerations of what constitutes an adverse health effect of air pollution (Thurston et al. 2017). A consensus document on behalf of the European Society of Cardiology reviewed the mechanisms and relationships between ambient air pollution and cardiovascular disease (Newby et al. 2015). Cascio (2018) succinctly summarized three principal pathways supported by epidemiological, clinical and toxicological data that explain the observed biochemical, physiological and clinical effects of PM exposure. Firstly, inhaled particulates can interact with the lung cells and initiate oxidative stress reactions leading to local and systemic inflammatory responses. For the cardiovascular system, these responses include decreased nitric oxide availability, oxidation, and alteration of the function of blood lipids, platelet activation, and prothrombotic changes in blood proteins that affect the function of blood vessels and clotting. Secondly, inhaled particulates can interact with neural receptors in the lung and activate a reflex of the autonomic nervous system that regulates blood pressure and heart rhythm. Thirdly, the UFPs can translocate across the alveolar membrane and move via bloodstream to other organs (e.g., heart, liver).
As mentioned earlier, trace elements constituents generally contribute only minimally to PM mass, yet these small amounts are biologically significant for the first proposed mechanism—activation of pro-inflammatory pathways and generation of reactive oxygen species. One of the most likely toxic components of PM2.5 are transition metals such as Fe, V, Ni, Cr, Cu, and Zn due to their oxidative potential, which is related to the redox activity and ability to generate ROS in biological tissues (Lippmann and Chen 2009), which can damage DNA and disrupt cell functioning via the oxidation of proteins and peroxidation of lipids. The increase in the level of oxidative stress occurs via a two-step catalytic conversion of hydrogen peroxide into the redox-active hydroxyl radical (Pratviel 2012), and the extent of this reaction is believed to be highly dependent on the oxidation state of the transition metal and conditions of the biological fluid (e.g., pH) (Saffari et al. 2014). The oxidative potential has been suggested to be a more health-relevant metric than PM mass, which may not adequately capture regional differences in biological activity (Weichenthal et al. 2016).
For the mechanistic understanding of aerosol health effects, cellular studies investigate how PM2.5 components can induce inflammation and oxidative stress. Common quantitative measures of oxidative stress are macrophage-based assay, dithiothreitol and ascorbic acid assays, iodometric spectrophotometry and electron paramagnetic/spin resonance spectrometry. However, a review by Shiraiwa et al. (2017) indicated that the relationship between the measured oxidative potential of PM and health endpoints is not established with certainty, and might depend on the type of assays and length of exposure. For example, the glutathione-related oxidative burden but not ascorbate-related oxidative burden was associated with lung cancer mortality in the Canadian Census Health and Environment Cohort (Weichenthal et al. 2016). Nevertheless, the macrophage-based ROS assay has been applied to ambient PM collected in various places in the world, showing that the ROS activities among the sites differ by more than 1 order of magnitude (Saffari et al. 2014). A greater PM redox activity was observed in developing areas of the world, which may be due to stronger emissions of fuel oil combustion, vehicle exhaust, and biomass burning. ROS activity levels were generally higher close to sources and urban sites compared to rural locations, except in summer when comparable ROS activity was observed at rural sites (Saffari et al. 2014). Concentrations of water-soluble transition metals (e.g., Fe, Ni, Cu, Cr, Mn, Zn, and V) showed positive correlations with the ROS activity of airborne PM across different urban areas and size ranges (Daher et al. 2012; Shafer et al. 2010). A large and systematic effort (Lippmann et al. 2013) to evaluate the relative toxicity of filter-collected PM found differences in the production of ROS in human epithelial and endothelial cell lines depending on location, season, and size fraction, with the highest ROS production for samples from New York City and Los Angeles. ROS responses to ultrafine PM samples from all sites were higher than responses to coarse and fine PM samples (on an equal mass basis); responses were higher in summer for fine and ultrafine samples but higher in winter for coarse samples. Strong correlations were observed between ROS production and Cu, Sb, V, Co, Be, and Ni. A Biosampler –collected PM2.5 from rural New York was studied for its oxidant generation capacity in vitro showed a relatively significant association Ni, and weaker but still significant correlations with Ba, Mn, and Fe. The single-source regression analysis showed a significant association with metal source only (Maciejczyk et al. 2010).
Ito et al. (2011) examined the effect of individual PM2.5 components on mortality in New York City, and in the cold season, the components associated with residual oil burning, Ni, V, and Zn, all showed the strongest effects at lag 3, while in the warm season, strong associations were observed for secondary aerosols including OC, sulfate, and Se, which are associated with transported coal emissions. In Seattle, the components associated with mortality during cold-season were traffic (EC), residual oil burning (Ni and V), and wood burning (K) (Zhou et al. 2011). In their review, Lippmann and Chen (2009) concluded that the cardiovascular effects of ambient air PM2.5 are greatly influenced, if not dominated, by their metal contents, especially the transition metals, and that nickel is likely to be a key component (Lippmann and Chen 2009).
4.1 Metal-Only Particle Toxicity: Evidence and Experience from Nanotoxicology
Several decades after the enactment of Clean Air Acts in U.S and U.K the urban pollution have visibly decreased but the epidemiological studies began to show the effects of small changes in PM concentrations on cardiovascular mortality and morbidity (Dockery et al. 1995; Pope et al. 1995; Pope et al. 2002). Ultrafine particles were hypothesized to be responsible for driving the cardiovascular effects of PM (Oberdörster et al. 1995). Unfortunately, most of the PM sampling, speciation campaigns, exposure studies and epidemiology studies that have taken place in the past two decades have lacked UFP samplers. Since UFPs do not contribute substantially to the mass, they are most commonly monitored by particle number counters, and thus are somewhat difficult to separate from the mass-modeled effects of PM2.5. A recent systematic review by Ohlwein (2018) of 85 epidemiologic studies pointed to adverse short-term associations with inflammatory and cardiovascular changes, some of which were attributed to UFPs or UFPs in combination with other pollutants. For the other studied health outcomes, the epidemiological evidence on independent health effects of UFP remains inconclusive or insufficient mostly due to small numbers of participants, a lack of consistent exposure information, and short intervals between exposure and effect.
The mechanistic role of UFP in cardiovascular, genotoxic and carcinogenic effects has been studied in laboratory-created aerosols of surrogate particles (e.g., carbon black, diesel engine soot, TiO2, ZnO, and Ni). Incidentally, engineered nanomaterial industries seem to be proactively trying to predict the possible adverse effect of new materials instead of “waiting to ‘count bodies’ on the introduction of a new hazard” (Donaldson and Seaton 2012). The nano-industry has yet to define what constitutes “particle reactivity”, and lacks a single parameter that would allow it to do so. To rectify this, the industry currently proposes a number of methods to measure this, such as measurement of ROS, pH and redox potential, band gap, and in vitro dissolution. The industry has refined the particle characterization methodology to go beyond mass and number concentrations and adopted well-recognized analytical methods that can provide reliable measurements in chemical composition, aggregation, surface area, crystal structure, and other parameters (Stone et al. 2017). A portable instrument for realistic safety testing of inhaled nanoparticles in vitro was recently developed and tested with an Ag and C particles (Geiser et al. 2017).
The mechanism of UFP toxicity that lead to cardiovascular effects (atherosclerosis, stroke, myocardial infarction) as well as the subsets of symptoms and diseases (Stone et al. 2017; Allen et al. 2017; Hamanaka and Munfu 2018) follows the same three main pathways as the inhalation and deposition of PM explained earlier in our text. First, particles interaction with neural receptors interferes with the central nervous system regulation of cardiovascular function. Second, lung inflammatory mediators cause systemic inflammation. Third, particle translocation to bloodstream carries them to other organs (e.g., heart, liver) (Stone et al. 2017; Cascio 2018).
Early work with health and safety of nanoparticles generally focused on single-component nanoparticles such as TiO2, Au, and carbon nanotubes. Some of the first studies with ultrafine TiO2 particles of different sizes demonstrated an increase of translocation of smaller particles into the lung interstitium compared to larger particles (Oberdörster et al. 1994). Occupational inhalation exposure to metal nano- and micro-sized particles, e.g., tungsten carbide-cobalt dust, in hard metal manufacturing facilities and mining and drilling industries is well documented to cause “hard metal lung disease” and an increased risk of lung cancer (Armstead and Li 2016). Looking ahead, the nanoparticle industry might face the problem of ambient UFPs—increasingly complex multicomponent systems that would need to be examined for health and ecological concerns in a greater detail than their individual constituent.
Some studies have shown that engineered nanoparticles do not exhibit ecotoxicity based on their chemical and macroscopic nature, but are toxic via similar mechanisms. For example, C60 fullerene and TiO2 nanoparticles have variable physicochemical properties but are both redox active and provoke oxidative stress in aquatic organisms. Furthermore, TiO2 has been reported to cause neurotoxicity in the brain tissue of various fish when entering into the brain and are subsequently phagocytosed by microglial cells, which then produce ROS (Hu and Gao 2010).
The majority of preclinical and clinical studies on environmentally relevant UFPs have been conducted with diesel exhaust and diesel exhaust particles, which are a rich source of UFPs. A comprehensive review by Stone et al. (2014) provides an extensive list of effects such as airway inflammation, changes in heart rate variability and arrhythmia, and a series of vascular dysfunctions, all of which promote cardiovascular disease. The cellular and biochemical mechanisms underlying these effects are wide-ranging, with oxidative stress and inflammation being key drivers (Miller et al. 2012).
4.2 The Fractional Contribution of Metals in PM2.5 Mixture Effects: How Do We Quantify It?
Lippmann and colleagues used source-apportionment techniques to evaluate which specific components and source categories might be contributing most to the health effects associated with exposure to PM (Lippmann HEI report 2013). Using a mouse model of cardiovascular disease, Chen and Lippmann (Study 1 of Lippmann’s HEI report 2013) observed that mice exposed to CAPS in 5 different locations in the US for 6 months showed greater plaque development in the arteries than mice exposed to filtered air, with samples collected at Manhattan (urban area with emissions from residual oil combustion, traffic, and secondary PM from coal-fired power plants) and Tuxedo (rural, mainly secondary PM from coal-fired power plants), New York, and East Lansing, Michigan (mid-west US with emissions from coal-fired power plants). In contrast, no differences between the control and CAPS-exposed mice were seen at Seattle, Washington (mainly traffic and wood smoke), and Irvine, California (mainly traffic). They found that CAPS exposures were associated with acute increases in heart rate and decreases in HRV at Manhattan and, to a lesser extent, at Tuxedo. Very few significant associations for HRV were seen at the other locations. The investigators concluded that the effects on plaque progression were most likely attributable to a coal combustion source category, and that the residual oil combustion, coal combustion, and traffic source categories contributed most to the observed acute cardiac effects. In terms of strength of associations, components attributable to source categories for residual oil combustion (Ni, V, and S), coal combustion (S and Se), and traffic (EC, Al, and P) appeared to be the most influential.
Using mouse in vivo and cultured cells (human lung epithelial cells and endothelial cells) in vitro exposures, Gordon and Chen (Study 2 of Lippmann’s HEI report 2013) reported that the production of reactive oxygen species (ROS) in human epithelial and endothelial cell lines were correlated with location, season, and size fraction, with the highest ROS production for samples from Manhattan and Los Angeles. In addition, on equal mass basis, ROS responses to ultrafine PM samples from all sites were higher than responses to coarse and fine PM samples; responses were higher in summer for fine and ultrafine samples but higher in winter for coarse samples. Strong correlations were observed between ROS production and Cu, Sb, V, Co, Be, and Ni. The investigators observed an increase lung inflammation in PM-exposed mice and the lung inflammation is larger to the coarse fraction of PM than to the fine and ultrafine fractions. Interestingly, there was no correlation between in vitro ROS production and in vivo lung inflammation for the same PM sample. The investigators concluded that the composition of PM samples pointed to the traffic and residual oil combustion source categories as contributors to the observed effects.
These studies consistently identified that coal combustion, residual oil combustion, traffic and metals source categories are associated with health effects, and that variables such as location, season, and size of PM pollution are influential in the strength of the associations.
5 Future Perspectives
5.1 Role of Metals in the Formation/Thriving of Other PM2.5-Associated Components: A Catalytic Role for Organic Transformation (E.G., Radical Generation, SOA Formation)?
Some of the early studies of the mixtures of UFPs and gases to reproduce aerosols typical of primary emissions from coal combustion or smelting operations demonstrated the capacity of metal-containing particles to oxidize reactive gases and produce ultrafine acid-coated particles. For example, a ZnO–SO2–H2O (mixed at 500 °C) system showed that oxidation of SO2 to H2SO4 was surface catalyzed, and the amount of soluble sulfur compounds present on the surface was dependent on the ZnO concentration and not on the SO2 concentration (Amdur et al. 1988). These acid-coated aerosols were used as a model of a type of primary emissions from smelters and coal combustors in the investigation of pulmonary effects in guinea pigs (Amdur and Chen 1989; Chen et al. 1992). Presence of acid in PM has been suggested as a major source of water-soluble Fe and other transition-metal ions in recent studies. For example, roadway emissions followed by secondary processing by acid were suggested as major contributors of water-soluble Fe, Cu, Mn, and Zn in Atlanta (Ye et al. 2018). Results from a series of toxicological studies designed to evaluate the health effects from various coal-fired power station emission scenarios suggest that the toxicity of PM from coal-fired power stations increases as the particles are atmospherically transformed, and transition metals play a critical role in these transformations. The amount and composition of the submicrometer aerosol depend on the source of fossil fuel used to produce electricity. For example, the dominant elements are Mg, Ca, and Fe for the lignite and Si, Fe, and Na for the bituminous coals, reflecting the differences in the composition of the mineral matter in coals of different origin (Amdur 1986). Metals such as As, Sb, Se, and Zn, which are volatile at combustion temperature, volatilize and condense preferentially on nanosized ultrafine particles (Amdur 1986). These ultrafine particles tend to be acidic and when inhaled produce decrement in pulmonary function, lung inflammation (Amdur and Chen 1989) and airway hyper responsiveness (Chen et al. 1992). Ambient concentrations of PM2.5-sulfate are considered a reliable marker of coal-fired power plants emissions.
Oxidative stress is a general term used to describe an imbalance in a cell’s redox state, such that pro-oxidant production overwhelms the endogenous antioxidant mechanisms of a cell. ROS refers to a family of molecules that are metabolites of oxygen and that, due to their high reactivity, are likely to participate in oxidation-reduction reactions (Lund 2010). While ROS form as natural by-products of a normal metabolic redox reaction, excess ROS is a response to environmental stress and can damage cellular lipids, proteins, or DNA, thus inhibiting signal transduction pathways and normal cellular functions.
Current knowledge suggests that transition metal-containing particles are the key factors in the formation of environmentally persistent free radicals (EPFR) that are formed when combustion byproducts interact with transition metal oxide on PM (Vejerano et al. 2018). During incineration of organic materials, emitted combustion byproducts recombine to form hydrocarbons and halogenated hydrocarbons while some condense to form nanoparticles. As the temperature cools off, soot and aromatic compounds (such as phenols and halogenated benzenes) are formed. At a temperature lower than 600 °C these organic aromatic precursors get adsorbed to particle surfaces where they are catalyzed by transition metal oxides to eventually form polychlorinated dibenzofurans (PCDFs), polychlorinated dibenzo-p-dioxins (PCDDs), and polycyclic aromatic hydrocarbons (nitro-PAHs and oxy-PAHs). However, the intermediate products of these surface-mediated reactions are long-lived surface bound radicals which are resistant to reaction with molecular oxygen, and thus, environmentally persistent. In a study, Louisiana PM2.5, Gehling and Dellinger (2013) used electron paramagnetic resonance for the EPFR decay measurements and reported a fast decay of 1/e lifetime 1–21 days (attributed to the phenoxyl radical), and slow decay 21–5028 days (attributed to the semiquinone radical). The primary sink for the EPFRs in the atmosphere is their reaction with molecular oxygen, which converts EPFRs to molecular species, and the rate of this reaction depends both on the properties of the organic molecules and metal oxide surface (Vejerano et al. 2018; Feld-Cook et al. 2017).
In contrast to gas-phase free radicals, the EPFRs are stabilized on the particle surface, and thus, due to their extended lifetime, present a higher risk of inhalation exposure. Yet the toxicity of EPFRs is not well studied, most likely due to lack of use of electron paramagnetic resonance instruments. Their contribution to PM toxicity most likely gets shifted to other species such as metals or organics, depending on what is measured. For example, Biswas et al. (2009) suggested that particle oxidative potential stems from the semivolatile PM fractions, based on a remarkable reduction in oxidative potential when the semivolatile fraction was removed from diesel aerosols. However, it could also be because of the decreased EPFR formation due to the lack of organic precursors. The toxicity studies that rely on the extraction of PM would be especially biased toward other components since when extracted EPFR react in solution to form multiple molecular reaction products including catechol, hydroquinone, phenol, chlorinated phenols, dibenzo-p-dioxin, and dibenzofuran (Truong et al. 2010). Unless TOF-MS techniques are used, the conventional approach to use solvent extracts in toxicity studies might modify the toxicity of PM and explain the discrepancies between inhalation and instillation studies.
There is evidence that transition metals can possibly chelate to carbonyls and organic acids in ambient particles and form metallo-organic compounds. Such complexes contribute to aqueous phase oxidation of organic compounds and the production of water-soluble organics (Singn and Gupta 2016).
5.2 Identifying the Relative Importance of Inhalation in Human Aggregate Exposure to Toxic Metals—Case Analysis for As, Cd, Cu, Pb; Understand the Underlying Biogeochemical Processes that Determine the Exposure Levels of Airborne Metals -> Enhance Human Health-Oriented Understanding of the Environmental Process of Trace Metals
In a variety of large population studies, various cardiovascular and pulmonary health effects have been significantly associated with long-term average concentrations of ambient air in terms of one or more of its particle size fractions and/or of its chemical components. These associations can be verified by studies in human volunteers by intratracheal instillation of particle suspensions of known compositions. Lay et al. (1998) and Ghio et al. (1998) instilled ~5-mg doses containing both soluble and insoluble 2.6 µm Fe particle agglomerates suspended in saline into the lungs of volunteer subjects to investigate oxidative stress. BALF samples were collected from 1 to 91 days later. After 1 day, Lay et al. (1998) reported inflammatory responses, and Ghio et al. (1998) reported decreased transferrin concentrations and increased concentrations of ferritin and lactoferrin. After 4 days, iron homeostasis was normal.
When similar study protocols were applied to real-world PM samples, the observed clinical health effects, i.e., lung inflammation and injury, can be used to verify the adverse effects observed in human populations, such as those from the Utah Valley, where there was a 14-month- long strike at a steel mill complex. There were significantly lower rates of mortality and hospital admissions during the strike than in the preceding and following years (Pope et al. 1989, 1991, 1992). Analyses of the PM collected on air sampling filters during those 3 years indicated that the concentrations of many airborne metal PM components (Cu, Zn, Fe, Pb, Sr, As, Mn, and Ni) were also significantly lower during the strike interval than in the preceding and following years (Frampton et al. 1999; Ghio and Devlin 2001; Dye et al. 2001). Volunteers instilled with aqueous extracts of PM filters while the steel mill was open had significant increases in both lung inflammation and injury in contrast to those volunteers in- stilled with an equal mass of PM extract from filters collected while the mill was closed (Ghio and Devlin 2001). Water soluble components or ionizable metals, which accounted for 20% of the PM mass, were responsible for the adverse health effects (Molinelli et al. 2002). The PM dose (500 µg) used in these studies was high, making it difficult to interpret these finding in relation to the risk of inhaled ambient particles in general population.
5.3 Forward-Looking Perspective on the Emerging Inhalable Sub-micron Particles Issues
In urban air, most UFPs are produced in vehicle exhaust and are composed of a carbon core coated with a diverse range of chemical species including redox-active transition metals and organic hydrocarbons. There is great variability in ambient UFP numbers, ranging from 500–10,000 particles/cm3 in rural areas to 7500–25,000 particles/cm3 in the urban background (Putaud et al. 2010), and with a European mean concentration of 31,500 particles/cm3 on busy streets. Depending on the type of vehicle and meteorological conditions, the large reactive surface area of exhaust UFPs can provide a reaction platform for catalytic conversion of organic radicals, sulfur, and nitrogen species chemistry, and partitioning for volatile and semi-volatile hydrocarbons. Thus, looking for causation of health effects becomes challenging in multicomponent complex systems of PM in air pollution.
Wildfires are increasingly being recognized as an important public health issue due to their UFP production. In the Western U.S. and Canada, the annual number of fires, the length of wildfire season, and the total area burned have all increased at a rapid rate over the past 30 years. Smoke from wildfires, including particles and gases, is trapped into high surface winds associated with the hot convective updraft and travels great distances to degrade air quality for communities far downwind. In 2014, wildfires in the US contributed 16.5% of fine particulate emissions for all fire, mobile, and stationary sources combined (EPA 2018). According to Verisk’s (2017) Wildfire Risk Analysis, 4.5 million U.S. homes were identified at high or extreme risk of wildfire, with seven states with more than 13% of households at high or extreme risk from wildfire. Recent systematic reviews (Youssouf et al. 2014; Liu et al. 2015; Reid et al. 2016) conclude that a strong association exists between exposure to wildfire smoke or wildfire PM2.5 and all-cause mortality and respiratory morbidity (asthma and COPD, bronchitis and pneumonia). One meta-analysis of 10 studies of wildfire-related particle exposure and respiratory health outcomes found higher relative risk for females than for males of developing asthma and COPD, with this risk higher in adults than in children for all respiratory-related hospital or emergency departments’ admissions (Kondo et al. 2019). However, significant gaps in research remain to connect wildfires beyond acute respiratory effects, such as cardiovascular mortality and morbidity, the risk for the susceptible population, long-term health effects, and consequences of exposure in children (Black et al. 2017; Reid et al. 2016; Kondo et al. 2019). Several studies have reported associations between wildfire smoke exposure and cardiac outcomes including emergency visits for heart failure (Rappold et al. 2011), out of hospital cardiac arrest (Stanley et al. 2014; Dennekamp et al. 2015) and cardiac mortality (Analitis et al. 2012; Sastry 2002). In a recent study in Dhaka City, Bangladesh, the effects of PM2.5 on cardiac emergency department visits, hospitalization and mortality are larger at lower PM2.5 concentrations, but smaller, and non-significant at higher concentrations, where biomass (e.g. crop) burning dominates, suggesting exposure biomass burning PM2.5 as having a lower CVD effect per μg/m3 than fossil fuel combustion-related PM2.5 (Rahman and Thurston, ISEE2019 abstract).
The size for fresh smoke particles falls in the 0.10–0.16 µm range (a count median diameter), but fires also produce a variety of coarse mode particles, and very hot fires generate giant ash particles with diameters of up to a millimeter (Naeher et al. 2007; Reid et al. 2005). A toxicological study by Kim et al. (2014) of fine and coarse wildfire PM in mice provided direct evidence of the differential biological effects of the two size fractions of PM. The oropharyngeal aspiration of 100 µg coarse PM/mouse causes inflammatory effects in the lung attributed to endotoxin, while the same dose of fine PM did not produce pulmonary effects, but did produce cardiovascular effects. Besides fine and UF particulates, wildfire smoke contains many air pollutants of concern for public health, such as carbon monoxide, nitrogen dioxide, ozone, polycyclic aromatic hydrocarbons, and volatile organic compounds. The chemical make-up of wildfire smoke depends on the type of biomass burned (green vs. dead vegetation, brush vs. softwood vs. hardwood) and the conditions for burning (active fire vs. smoldering).
Worldwide, indoor/outdoor cooking and heating appliances that burn wood are a major source of air pollution. In Europe 15–25% (i.e. Sweden, Finland, Germany and Austria) and 50% of PM2.5 in the Alpine region originates from residential biomass (primarily wood) combustion, and will become the dominant source of fine PM by 2020 with a contribution of 38% of total emissions (see review by Sigsgaard et al. 2015). Rokoff et al. (2017) reviewed 36 studies in developed countries that reported associations of household wood stove use and/or community wood smoke exposure with pediatric health outcomes. While the use of wood stoves showed inconsistent associations with cough and wheeze and limited evidence for an association with other markers of respiratory health, there were consistent associations between higher community wood smoke and poor respiratory health in children. A conservative estimate of biomass smoke to premature mortality in Europe amounts to at least 40,000 deaths per year (Sigsgaard et al. 2015). The use of biomass, primarily for heating, is thought to be responsible for as much as 30% of PM pollution in winter in Delhi (Gordon et al. 2018). The use of traditional stoves throughout rural India and South Asia households contributes to extreme exposures well above the recommended WHO air quality guidelines.
6 Conclusions
a. Metals are minor contributors to total PM 2.5 mass globally, but play a multi-faceted role;
There is clearly emerging evidence that the inhalation of some components of ambient air PM are associated with adverse health effects at concentrations near or not much higher than current ambient PM2.5 mass concentrations. These components include EC, Ni, V, and Pb, and suggestive evidence exists for others, such as Al, Zn, and OC. Location, season, and size of PM are influential important variables that need to be considered when investigating the health effects of PM pollution. Many transition metals in PM are redox-active and lead to the production of reactive oxygen species in various cells in the lungs, blood and vascular tissues. This ROS production causes oxidative stress, which then leads to increased airway and systemic inflammation, and adverse cardiovascular responses. Metals also play a role in catalytic reaction leading to the formation of secondary organic aerosols, and conversion of gaseous pollutants (notably oxides of sulfur and nitrogen) to particulate phase. There is some evidence that adverse health effects are significantly associated with aerosol acidity originating from fossil fuel combustion, which could be due to its irritancy, or to its role in making metals bioavailable within the particles. Additional catalytic metal reactions lead to the formation and stabilization of long-lived organic radicals. Future studies can utilize pure materials as well as ambient air PM of mixed composition to obtain more information on the roles of specific PM components and their interactions and combined effects, and thereby identify those components most in need of control in order to reduce the health impacts of airborne PM.
b. Abundance and profiles of airborne trace metals infer geographical inhalation exposure disparities (exposure inequality);
Over the past several decades, a combination of the advancements in technology and effective policies have led to a decline in air pollution in North America. Specifically, since 2010 the mandate of low-sulfur diesel fuel and vehicle emission control for diesel truck and buses in the U.S. decreased the PM and nitrogen oxide emission by 90% (HEI 2015). However, there is evidence of the environmental inequality in North America, Asia, and Africa showing that low socioeconomic status communities face higher concentrations of criteria air pollutants (Hajat et al. 2015). The results for Europe are mixed, and rapidly developing nations like India and China are understudied. This air pollution inequality may have sizeable impacts for population health—nearly 90% of air-pollution-related deaths occur in low- and middle-income countries, with nearly 2 out of 3 occurring in WHO’s South-East Asia and Western Pacific regions (WHO 2016). The reasons for exposure inequality include economical (industries build factories on cheap land), political (poor communities lack political power to prevent construction of factories, landfills, and roads in close proximity), social (access to education and health services), demographic (population density and age), and other (affordability of newer cars, types of roads, etc.). Furthermore, the toxicity of particulates in different parts of the world is not necessarily the same, which might be most relevant for metals released from open-air smelting, trash burning, and less-stringently regulated industries, and for black and organic carbon compounds from combustion processes, including biomass burning and biofuel use for cooking and heating. While reported health burden estimates are based on studies conducted in North America and Europe, efforts are underway to generate locally relevant air quality and health data in developing countries (HEI 2019).
c. Size distribution and chemical speciation of airborne metals determines their respiratory deposition efficiency and pulmonary bioavailability and consequent toxic potencies;
Smaller size fractions are found to be generally associated with higher intrinsic ROS activity, which may be due to a higher abundance of water-soluble metals or organics. For the human distal regions of the lungs, neither macrophage-mediated long-term clearance kinetics data nor translocation data for UFP into the circulation are currently available. Particle clearance from the lungs can also occur via transport toward lymph nodes and translocation into the blood circulation, leading potentially to accumulation in secondary organs and tissues.
d. Metals are important toxicity contributors to PM 2.5 , but may not be as dominant as previously perceived.
When black carbon and PM2.5 are considered simultaneously for health effects, associations remained robust for black carbon. The review by Cassee et al. (2013) of the WHO REVIHAAP Project (2013) lists the growing evidence that links black carbon particles with cardiovascular health effects and premature mortality, for both short-term (24 h) and long-term (annual) exposures. Even when black carbon may not be the causal agent, it may operate as a universal carrier of a wide variety of combustion-derived chemical constituents of varying toxicity, including organic particles, not fully considered with PM2.5 mass. Lucking et al. (2011) has shown that removing the particles from diluted diesel engine exhaust prevented adverse effects on the cardiovascular system—explained by differences in particle composition, with black carbon particles (soot) in diesel exhaust enriched with (semi)volatile organic particles and metals. There is growing information on the associations of organic carbon with health effects, and carbonaceous primary emissions are one of the important contributors to the formation of secondary organic aerosols (a significant component of the PM2.5 mass). The evidence is insufficient to distinguish between the toxicity of primary and secondary organic aerosols link as a carrier of organic to metals and EPFRs in UFP or PM2.5. In the Los Angeles basin, it was found that both water-soluble and water-insoluble organic carbon as emitted by vehicular sources contribute substantially to the ROS activity of PM (Saffari et al. 2015).
e. The shift from intrinsic toxicity of metals alone to joint interactions and combined toxicity with other PM 2.5 components and gaseous pollutants (total air exposure).
A comprehensive meta-analysis of 100 studies of the association of ambient air pollution with hypertension and blood pressure (Yang et al. 2018) showed significant association of long-term exposures to PM2.5 to hypertension, and of PM10, PM2.5, and NO2 with diastolic blood pressure. However, any hypertension and blood pressure effects from short-term exposure to PM had to include a gaseous pollutant (SO2 or NO2 or both) to be significant. Acute exposure to gaseous ambient air pollution was associated with increases in morbidity and mortality within low and middle-income countries with greatest associations observed for cardiorespiratory mortality (Newell et al. 2018). Another systematic review and meta-analysis of 17 studies found positive and significant associations for air pollutants and pediatric pneumonia. While the most consistent association was for PM2.5, the highest excess risk was for SO2 followed by PM2.5, O3, PM10, NO2, and CO (Nhung et al. 2017). A series of identically designed subchronic exposure animal studies compared inhalation of simulated fresh emissions from coal combustion, diesel exhaust, gasoline exhaust, and wood smoke and found the least relative toxicity for the coal combustion (Mauderly et al. 2011). The follow-up analyses using compositional data of these exposure atmospheres pointed toward SO2, ammonia, NOx, and CO as most predictive of changes in inflammatory and vascular markers (Seilkop et al. 2012).
Reflecting on the results of the non-additive cell inflammatory responses described previously, Leclercq et al. (2017) hypothesized that the xenobiotic cell penetrance mechanisms may be different depending on how they are presented to the cells, in their soluble form or linked to particles. The relationship between chemical makeup of core particles and particle surface affects uptake, retention, translocation and the clearance within the lungs. Transition metals and PAHs are notably known to be associated with PM, either adsorbed on the surface or as an integral component of the particle core; thus, they can become bioavailable almost immediately by dissolving in somewhat neutral pH of lung fluid or somewhat later when digested by acidic phagocytosis. As a result, PM induces oxidative stress either directly via transition metals followed by inflammation by the subsequent secretion of proinflammatory mediators caused by undissolved particles, as well as by the reactive quinones arising from the metabolism of organic chemicals.
One of the major obstacles for PM health effects research is that only small amounts of PM obtained via collection is usually available. For ambient PM, it is necessary to collect and extract PM from the collector (by scraping, sonicating, or chemically extracting from a filter), which may alter the state of the PM before its use in toxicology studies. Transformation and loss of toxicologically important semivolatile compounds during sampling is also an issue that must be taken into account when testing collected PM.
A number of studies have attempted to separate the role of PM and gaseous components in the health effects associated with ambient air pollution exposure by removing PM from the mixture using high-efficiency particle filters. In a cardiovascular study of mice in Sao Paulo urban air (mostly traffic and resuspended soil sources), mild but significant vascular structural alterations compared to filtered air group where 30% NO2, 50% PM2.5 (with PM0.3 filter), and 100% BC were removed (Akinaga et al. 2009). However, Barrett et al. (2011) reported that acute exposure to either whole (PM plus gaseous) or just gaseous phase of simulated downwind coal combustion emissions both exacerbated various features of allergic airway responses in mice.
Gordon et al. (2012) examined various cardio physiological changes that occur with gas-phase only components of diesel exhaust and compared that to whole exhaust in rats. They concluded that it is possible that the components of whole diesel exhaust might have a greater influence on the heart, while both filtered and whole exhaust similarly elevated pulmonary inflammation in animals. In another study in which diesel engine emission altered atherosclerotic plaque composition, the overall effect of the whole exhaust was substantial and exceeded the impact of PM alone (Campen et al. 2010). In a study that compared the effects of diluted whole diesel engine exhaust (WDE) with PM2.5 CAPS, Quan et al. (2010) exposed male ApoE−/− mice 5.2 h/day, 5 days/week, for 5 months to five different exposure atmospheres: (1) FA; (2) Tuxedo, NY, PM CAPS, (mean = 110 µg/m3); (3) WDE, containing diesel exhaust particles (DEP) at 436 µg/m3; (4) diesel exhaust gases (DEG, equivalent to gases in WDE; and (5) CAPS + DEG. Atherosclerotic plaques were quantified for brachiocephalic artery cross-sections after 3 and 5 months of exposure. The results indicated that (1) DEG did not exacerbate progression; (2) There were no interactive effects between DEG and CAPS; (3) CAPS, despite having a much lower PM concentration, caused more plaque development than WDE, indicating that some components in ambient PM, not present in WDE, are responsible for the exacerbation of plaque progression by CAPS. In a human clinical study of patients with heart failure, the use of particle filter reduced the adverse effects of whole diesel exhaust on endothelial function and BNP but otherwise had no improving effect on the 6-min walking distance and arterial stiffness (Vieira et al. 2016).
f. Future needs for holistic thinking of interactive behavior of metals, organics, and bioaerosols in atmospheric chemistry and human exposure/health; bridge biogeochemistry and environmental health for human aggregate exposure of trace metals.
Active comprehensive research of the toxicity of ambient PM components in last several decades has not identified a single culprit component or source category that is responsible in whole or in part for the observed health effects associated with PM2.5. In fact, all the evidence points that there could be a combination of particle sizes, particle and gaseous sources, concentrations, weather patterns, geographical locations, sociodemographic factors, and sensitive population. Thus, there is a great need for accumulated knowledge to be synthesized and integrated into a holistic approach to evaluate and resolve human exposure to ambient pollutants. The priorities for improved assessments should include (1) epidemiological studies and PM monitoring in regions where such studies have not yet been performed, especially in Asia and Africa; (2) comprehensive analysis of all components (organic, inorganic, bioaerosol) including gases; (3) studies of pollution intervention or sudden pollution episodes (for examples, fires, volcanos); (4) comprehensive studies involving personal exposure monitoring; and (5) improved statistical modeling. Enhanced understanding of these related factors will lead to better targeted public health protection.
References
Adams K, Greenbaum DS, Shaikh R, van Erp AM, Russell AG (2015) Particulate matter components, sources, and health: systematic approaches to testing effects. J Air Waste Manag Assoc 65(5):544–558. https://doi.org/10.1080/10962247.2014.1001884
Akinaga LMY, Lichtenfels AJ, Carvalho-Oliveira R, Caldini EG, Dolhnikoff M, Silva LFF, De Siqueira Bueno HM, Pereira LAA, Saldiva PHN, Garcia MLB (2009) Effects of chronic exposure to air pollution from Sao Paulo city on coronary of Swiss mice, from birth to adulthood. Toxicol Pathol 37(3):306–314
Allen JL, Oberdörster G, Morris-Schaffer K, Wong C, Klocke C, Sobolewski M, Conrad K, Mayer-Proschel M, Cory-Slechta DA (2017) Developmental neurotoxicity of inhaled ambient ultrafine particle air pollution: parallels with neuropathological and behavioral features of autism and other neuro developmental disorders. Neurotoxicology 59:140–154. https://doi.org/10.1016/j.neuro.2015.12.014
Amdur MO, Chen LC, Guty J, Lam, HF, Miller PD (1988) Speciation and pulmonary effects of acidic SOx formed on the surface of ultrafine zinc oxide aerosols. Atmos Environ 22(3):557–560 (1967). https://doi.org/10.1016/0004-6981(88)90199-0
Amdur MO, Chen LC (1989) Furnace-generated acid aerosols: speciation and pulmonary effects. Environ Health Perspect 79:147–150
Analitis A, Georgiadis I, Katsouyanni K (2012) Forest fires are associated with elevated mortality in a dense urban setting. Occup Environ Med 69:158–162
Armstead AL, Li B (2016) Nanotoxicity: emerging concerns regarding nanomaterial safety and occupational hard metal (WC-Co) nanoparticle exposure. Int J Nanomedicine 11:6421–6433
Banerjee A, Roychoudhury A (2019) Nanoparticle-induced ecotoxicological risks in aquatic environments. In: Nanomaterials in plants, algae and microorganisms. Elsevier
Barrett EG, Day KC, Gigliotti AP, Reed MD, McDonald JD, Mauderly JL, Seilkop SK (2011) Effects of simulated downwind coal combustion emissions on pre-existing allergic airway responses in mice. Inhalation Toxicol 23(13):792–804. https://doi.org/10.3109/08958378.2011.609917
Bell ML; HEI Health Review Committee. (2012) Assessment of the health impacts of particulate matter characteristics. Res Rep Health Eff Inst. (161):5-38.
Beelen R, Hoek G, van den Brandt PA, Goldbohm RA, Fischer P, Schouten LJ, Jerrett M, Hughes E, Armstrong B, Brunekreef B. (2008) Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ Health Perspect. 116(2):196-202. https://doi.org/10.1289/ehp.10767
Biswas S, Verma V, Sioutas C, Schauer JJ, Cassee FR, Cho AK (2009) Oxidative potential of semi-volatile and non volatile particulate matter (pm) from heavy-duty vehicles retrofitted with emission control technologies. Environ Sci Technol 43(10):3905–3912. https://doi.org/10.1021/es9000592
Black C, Tesfaigzi Y, Bassein JA, Miller LA. (2017) Wildfire smoke exposure and human health: Significant gaps in research for a growing public health issue. Environ Toxicol Pharmacol. 55:186-195. https://doi.org/10.1016/j.etap.2017.08.022.
Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD; American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism. (2010) Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation.121(21):2331-78. https://doi.org/10.1161/CIR.0b013e3181dbece1
Campen MJ, Lund AK, Knuckles TL, Conklin DJ, Bishop B, Young D, Seilkop S, Seagrave J, Reed MD, McDonald JD (2010) Inhaled diesel emissions alter atherosclerotic plaque composition in ApoE −/− mice. Toxicol Appl Pharmacol 242(3):310–317. https://doi.org/10.1016/j.taap.2009.10.021
Cascio WE (2018) Wildland fire smoke and human health. Sci Total Environ 624:586–595. https://doi.org/10.1016/j.scitotenv.2017.12.086
Cassee FR, Heroux M-E, Gerlofs-Nijland ME, Kelly FJ (2013) Particulate matter beyond mass: recent health evidence on the role of fractions, chemical constituents and sources of emission. Inhal Toxicol 25(14):802–812. https://doi.org/10.3109/08958378.2013.850127
Chen LC, Nadziejko C (2005) Effects of subchronic exposures to concentrated ambient particles (CAPs) in mice. V. CAPs exacerbate aortic plaque development in hyperlipidemic mice. Inhal Toxicol 17:217–224
Chen LC, Miller PD, Amdur MO, Gordon T (1992) Airway hyperresponsiveness in guinea pigs exposed to acid-coated ultrafine particles. J Toxicol Environ Health 35(3):165–174
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Forouzanfar MH (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet 389(10082):1907–1918. https://doi.org/10.1016/s0140-6736(17)30505-6
Daher N et al (2012) Characterization, sources and redox activity of fine and coarse particulate matter in Milan. Italy Atmos Environ 49:130–141
Dai L, Zanobetti A, Koutrakis P, Schwartz JD (2014) Associations of fine particulate matter species with mortality in the United States: a multicity time-series analysis. Environ Health Perspect 122:837–842. https://doi.org/10.1289/ehp.1307568
Davies NM, Feddah MR (2003) A novel method for assessing dissolution of aerosol inhaler products. Int J Pharm 255:175–187
Dennekamp M, Straney LD, Erbas B, Abramson MJ, Keywood M, Smith K, Sim MR, Glass DC, Monaco AD, Haikerwal A, Tonkin AM (2015) Forest fire smoke exposures and out-of-hospital cardiac arrests in Melbourne, Australia: a case-crossover study. Environ Health Perspect 123(10):959–964. https://doi.org/10.1289/ehp.1408436
Dockery DW, Pope CA III, Xu X, Spengler JD, Ware JH, Fay ME et al (1993) An association between air pollution and mortality in six U.S. cities. N Engl J Med 329:1753–1759. https://doi.org/10.1056/nejm199312093292401
Donaldson K, Seaton A (2012) A short history of the toxicology of inhaled particles. Part Fibre Toxicol 9:13. https://doi.org/10.1186/1743-8977-9-13
Dye JA, Lehmann JR, McGee JK, Winsett DW, Ledbetter AD, Everitt JI, Ghio AJ, Costa DL. (2001) Acute pulmonary toxicity of particulate matter filter extracts in rats: coherence with epidemiologic studies in Utah Valley residents. Environ Health Perspect. 109 Suppl 3:395-403. PMID: 11427389
EPA U.S. (2009) Integrated science assessment for particulate matter (final report). Washington, DC, United States Environmental Protection Agency. http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=216546#Download
EPA U.S. (2012) Provisional assessment of recent studies on health effects of particulate matter exposure. U.S. Environmental Protection Agency, Washington, DC, EPA/600/R-12/056. https://cfpub.epa.gov/ncea/isa/recordisplay.cfm?deid=247132
EPA U.S. (2014) Office of transportation and air quality. Near Roadway Air Pollution and Health: Frequently Asked Questions. EPA-420-F-14-044
EPA U.S (2018) 2014 National Emissions Inventory. https://gispub.epa.gov/neireport/2014/
Feld-Cook EE, Bovenkamp-Langlois L, Lomnicki SM (2017) Effect of particulate matter mineral composition on environmentally persistent free radical (EPFR) formation. Environ Sci Technol 51:10396–10402. https://doi.org/10.1021/acs.est.7b01521
Frampton MW, Ghio AJ, Samet JM, Carson JL, Carter JD, Devlin RB. (1999) Effects of aqueous extracts of PM(10) filters from the Utah valley on human airway epithelial cells. Am J Physiol. 277(5):L960-7. https://doi.org/10.1152/ajplung.1999.277.5.L960.
Gauderman WJ, Urman R, Avol E, Berhane K, McConnell R, Rappaport E, Chang R, Lurmann F, Gilliland F (2015) Association of improved air quality with lung development in children. N Engl J Med 372(10):905–913
Gehling W, Dellinger B (2013) Environmentally persistent free radicals and their lifetimes in PM2.5. Environ Sci Technol 47(15):8172–8178. https://doi.org/10.1021/es401767m
Geiser M, Jeannet N, Fierz M, Burtscher H (2017) Evaluating adverse effects of inhaled nanoparticles by realistic in vitro technology. Nanomaterials 7(2):49. https://doi.org/10.3390/nano7020049
Ghio AJ, Carter JD, Richards JH, Brighton LE, Lay JC, Devlin RB. (1998) Disruption of normal iron homeostasis after bronchial instillation of an iron-containing particle. Am J Physiol. 274(3):L396-403. https://doi.org/10.1152/ajplung.1998.274.3.L396.
Ghio AJ, Devlin RB. (2001) Inflammatory lung injury after bronchial instillation of air pollution particles. Am J Respir Crit Care Med.164(4):704-8. PMID: 11520740
Giannadaki D, Pozzer A, Lelieveld J (2014) Modeled global effects of airborne desert dust on air quality and premature mortality. Atmos Chem Phys 14(2):957–968
Godleski JJ et al (2011) Toxicological evaluation of realistic emission source aerosols (TERESA): summary and conclusions. Inhal Toxicol 23(Suppl. 2):95–103
Gordon CJ, Schladweiler MC, Krantz T, King C, Kodavanti UP. (2012) Cardiovascular and thermoregulatory responses of unrestrained rats exposed to filtered or unfiltered diesel exhaust. Inhal Toxicol. 24(5):296-309. https://doi.org/10.3109/08958378.2012.670811.
Gupta T, Demokritou P, Koutrakis P (2004) Development and performance evaluation of a high-volume ultrafine particle concentrator for toxicological studies. Inhal Toxicol 16:851–862
Hajat A, Hsia C, O’Neill MS (2015) Socioeconomic disparities and air pollution exposure: a global review. Curr Environ Health Rep 2(4):440–450. https://doi.org/10.1007/s40572-015-0069-5
Hamanaka RB, Mutlu GM (2018) Particulate matter air pollution: effects on the cardiovascular system. Front Endocrinol 9:680. https://doi.org/10.3389/fendo.2018.00680
Happo MS, Salonen RO, Halinen AI, Jalava PI, Pennanen AS, Dormans JA, Gerlofs-Nijland ME, Cassee FR, Kosma VM, Sillanpaa M, Hillamo R, Hirvonen MR (2010) Inflammation and tissue damage in mouse lung by single and repeated dosing of urban air coarse and fine particles collected from six European cities. Inhal Toxicol 22:402–416. https://doi.org/10.3109/08958370903527908
Heinzerling A, Hsu J, Yip F (2015) Respiratory health effects of ultrafine particles in children: a literature review. Water Air Soil Pollut 227:32. https://doi.org/10.1007/s11270-015-2726-6
HEI Review Panel on Ultrafine Particles (2013) Understanding the health effects of ambient ultrafine particles. HEI Perspectives 3. Health Effects Institute; Boston, MA
Health Effects Institute (2015) Executive Summary. The Advanced Collaborative Emissions Study (ACES). Health Effects Institute; Boston, MA
Health Effects Institute (2019) Update Winter 2019. www.healtheffects.org/system/files/UpdateWinter2019.pdf
Hime NJ, Marks GB, Cowie CT (2018) A comparison of the health effects of ambient particulate matter air pollution from five emission sources. Int J Environ Res Public Health 15(6):1206. https://doi.org/10.3390/ijerph15061206
Im U, Brandt J, Geels C, Hansen KM, Christensen JH, Andersen MS, Solazzo E, Kioutsioukis I, Alyuz U, Balzarini A, Baro R, Bellasio R, Bianconi R, Bieser J, Colette A, Curci G, Farrow A, Flemming J, Fraser A, Jimenez-Guerrero P, Kitwiroon N, Liang C-K, Nopmongcol U, Pirovano G, Pozzoli L, Prank M, Rose R, Sokhi R, Tuccella P, Unal A, Vivanco MG, West J, Yarwood G, Hogrefe C, Galmarini S (2018) Assessment and economic valuation of air pollution impacts on human health over Europe and the United States as calculated by a multi-model ensemble in the framework of AQMEII3. Atmos Chem Phys 18:5967–5989. https://doi.org/10.5194/acp-18-5967-2018
Ito K, Mathes R, Ross Z, Nádas A, Thurston G, Matte T (2011) Fine particulate matter constituents associated with cardiovascular hospitalizations and mortality in New York City. Environ Health Perspect 119:467–473. https://doi.org/10.1289/ehp.1002667
Keller AA, Lazareva A (2014) Predicted releases of engineered nanomaterials: from global to regional to local. Environ Sci Technol Lett 1(1):65–70
Kim KH, Kabir E, Kabir S.(2015) A review on the human health impact of airborne particulate matter. Environ Int. 74:136-43.
Kim YH, Tong H, Daniels M, Boykin E, Krantz QT, McGee J, Hays M, Kovalcik K, Dye JA, Gilmour MI. (2014). Cardiopulmonary toxicity of peat wildfire particulate matter and the predictive utility of precision cut lung slices. Part Fibre Toxicol. 11:29. https://doi.org/10.1186/1743-8977-11-29
Knol AB et al (2009) Expert elicitation on ultrafine particles: likelihood of health effects and causal pathways. Part Fibre Toxicol 6:19
Kutlar Joss M, Eeftens M, Gintowt E, Kappeler R, Künzli N (2017) Time to harmonize national ambient air quality standards. Int J Public Health 62(4):453–462. https://doi.org/10.1007/s00038-017-0952-y
Kondo MC, De Roos AJ, White LS, Heilman WE, Mockrin MH, Gross-Davis CA, Burstyn I. (2019) Meta-Analysis of Heterogeneity in the Effects of Wildfire Smoke Exposure on Respiratory Health in North America. Int J Environ Res Public Health. 16(6). pii: E960. https://doi.org/10.3390/ijerph16060960.
Lay JC, Bennett WD, Kim CS, Devlin RB, Bromberg PA. (1998) Retention and intracellular distribution of instilled iron oxide particles in human alveolar macrophages. Am J Respir Cell Mol Biol. 18(5):687-95. PMID: 9569239.
Leclercq B, Alleman LY, Perdrix E, Riffault V, Happillon M, Strecker A, Lo-Guidice J-M, Garçon G, Coddeville P (2017) Particulate metal bioaccessibility in physiological fluids and cell culture media: toxicological perspectives. Environ Res 156:148–157. https://doi.org/10.1016/j.envres.2017.03.029
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525(7569):367–371
Lipfert FW, Wyzga RE, Baty JD, Miller JP (2009) Air pollution and survival within the Washington University-EPRI Veterans cohort: risks based on modeled estimates of ambient levels of hazardous and criteria air pollutants. J Air Waste Manage Assoc 59:473–489. https://doi.org/10.1080/10473289.2009.10465740
Lippmann M, Chen LC (2009) Health effects of concentrated ambient air particulate matter (CAPs) and its components. Crit Rev Toxicol 39(10):865– 913
Lippmann M, Ito K, Hwang JS, Maciejczyk P, Chen LC (2006) Cardiovascular effects of nickel in ambient air. Environ Health Perspect 114(11):1662–1669. https://doi.org/10.1289/ehp.9150
Lippmann M, Chen L-C, Gordon T, Ito K, Thurston GD (2013) National Particle Component Toxicity (NPACT) initiative: integrated epidemiologic and toxicologic studies of the health effects of particulate matter components. Res Rep 177 Health Effects Institute, Boston, MA
Lippmann M. (2010) Targeting the components most responsible for airborne particulate matter health risks. J Expo Sci Environ Epidemiol. 20(2):117-8. https://doi.org/10.1038/jes.2010.1
Lippmann M (2014) Toxicological and epidemiological studies of cardiovascular effects of ambient air fine particulate matter (PM2.5) and its chemical components: coherence and public health implications. Crit Rev Toxicol 44(4):299–347. https://doi.org/10.3109/10408444.2013.861796
Liu JC, Pereira G, Uhl SA, Bravo MA, Bell ML (2015) A systematic review of the physical health impacts from non-occupational exposure to wildfire smoke. Environ Res 136:120–132
Lucking AJ, Lundback M, Barath SL et al (2011) Particle traps prevent adverse vascular and prothrombotic effects of diesel engine exhaust inhalation in men. Circulation 123:1721–1728
Lund AK (2010) Cardiovascular toxicology. In: Comprehensive toxicology, 2nd edn. McQueen, CA
Maciejczyk P, Zhong M, Li Q, Xiong S, Nadziejko C, Chen LC (2005) The design of a concentrated ambient particulate matter exposure system for biometric telemetry monitoring. Inhal Toxicol 17:189–197
Maciejczyk P, Zhong M, Lippmann M, Chen LC (2010) Oxidant generation capacity of source-apportioned PM2.5. Inhal Toxicol 2:29–36
Malig BJ, Ostro BD (2009) Coarse particles and mortality: evidence from a multi-city study in California. Occup Environ Med 66:832–839
Mauderly JL, Barrett EG, Gigliotti AP, McDonald JD, Reed MD, Seagrave J, Mitchell LA, Seilkop SK (2011) Health effects of subchronic inhalation exposure to simulated downwind coal combustion emissions. Inhal Toxicol 23(6):349–362
Miller MR, Shaw CA, Langrish JP (2012) From particles to patients: Oxidative stress and the cardiovascular effects of air pollution. Future Cardiol 8(4):577–602. https://doi.org/10.2217/fca.12.43
Mirowsky J, Hickey C, Horton L, Blaustein M, Galdanes K, Peltier RE, Chillrud S, Chen LC, Ross J, Nadas A, Lippmann M, Gordon T (2013) The effect of particle size, location and season on the toxicity of urban and rural particulate matter. Inhal Toxicol 25(13):747–757
Mirowsky JE, Jin L, Thurston G, Lighthall D, Tyner T, Horton L, Galdanes K, Chillrud S, Ross J, Pinkerton KE, Chen LC, Lippmann M, Gordon T (2015) In vitro and in vivo toxicity of urban and rural particulate matter from California. Atmos Environ 103:256–262. http://doi.org/10.1016/j.atmosenv.2014.12.051
Molinelli AR, Madden MC, McGee JK, Stonehuerner JG, Ghio AJ.(2002) Effect of metal removal on the toxicity of airborne particulate matter from the Utah Valley. Inhal Toxicol. 14(10):1069-86. PMID: 12396411
Naeher LP, Brauer M, Lipsett M, Zelikoff JT, Simpson CD, Koenig JQ, Smith KR (2007) Woodsmoke health effects: a review. Inhal Toxicol 19(1):67–106
Newby DE, Mannucci PM, Tell GS, Baccarelli AA, Brook RD, Donaldson K, Forastiere F, Franchini M, Franco OH, Graham I, Hoek G, Hoffmann B, Hoylaerts MF, Künzli N, Mills N, Pekkanen J, Peters A, Piepoli MF, Rajagopalan S, Storey RF (2015) ESC Working Group on Thrombosis, European Association for Cardiovascular Prevention and Rehabilitation, ESC Heart Failure Association, Expert position paper on air pollution and cardiovascular disease. Eur Heart J 36:83–93. https://doi.org/10.1093/eurheartj/ehu458
Newell K, Kartsonaki C, Lam K, Kurmi O (2018) Cardiorespiratory health effects of gaseous ambient air pollution exposure in low and middle income countries: a systematic review and meta-analysis. Environ Health 17(1):41. https://doi.org/10.1186/s12940-018-0380-3 A global access science source
Nhung NTT, Amini H, Schindler C, Kutlar Joss M, Dien TM, Probst-Hensch N, Perez L, Kunzli N (2017) Short-term association between ambient air pollution and pneumonia in children: a systematic review and meta-analysis of time-series and case-crossover studies. Environ Pollut 230:1000–1008. https://doi.org/10.1016/j.envpol.2017.07.063
Oberdörster G, Ferin J, Lehnert BE (1994) Correlation between particle size, in vivo particle persistence, and lung injury. Environ Health Perspect 102(Suppl 5):173–179
Oberdörster G, Gelein RM, Ferin J, Weiss B (1995) Association of particulate air pollution and acute mortality: involvement of ultrafine particles? Inhal Toxicol 7(1):111–124
Ohlwein S, Kappeler R, Kutlar Joss M et al. (2019) Health effects of ultrafine particles: a systematic literature review update of epidemiological evidence. Int J Public Health. https://doi.org/10.1007/s00038-019-01202-7
Ole Raaschou-Nielsen O, Andersen ZJ, Beelen R, Samoli E, Stafoggio M, Weinmayr G, Hoffmann B, Fisher P, Nieuwenhuijsen MJ, Brunekreef B, Xun WW, Katsouyanni K, Dimakopoulou K, Sommar J, Forsberg B, Modig L, Oudin A, Oftedal B, Schwarze PE, Nafstad P, De Faire U, Pedersen NL, Ostenson CG, Fratiglioni L, Penell J, Korek M, Pershagen G, Eriksen KT, Sørensen M, Tjønneland A, Ellermann T, Eeftens M, Peeters PH, Meliefste K, Wang M, Bueno-de-Mesquita B, Key TJ, de Hoogh K, Concin H, Nagel G, Vilier A, Grioni S, Krogh V, Tsai MY, Ricceri F, Sacerdote C, Galassi C, Migliore E, Ranzi A, Cesaroni G, Badaloni C, Forastiere F, Tamayo I, Amiano P, Dorronsoro M, Trichopoulou A, Bamia C, Vineis P, Hoek G (2013) Air pollution and lung cancer incidence in 17 European cohorts: prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol 14:813–822
Ostro B, Lipsett M, Reynolds P, Goldberg D et al (2010) Long-term exposure to constituents of fine particle air pollution and mortality: results from the California teachers study. Environ Health Perspect 118:363–369. https://doi.org/10.1289/ehp.0901181
Ostro B, Reynolds P, Goldberg D, Hertz A et al (2011) Erratum: assessing long-term exposure in the California teachers study. Environ Health Perspect 119:242–243
Pelfrêne A, Cave MR, Wragg J, Douay F (2017) In vitro investigations of human bioaccessibility from reference materials using simulated lung fluids. Int J Environ Res Pub Health 14(2):112
Peters A, Veronesi B, Calderón-Garcidueñas L, Gehr P, Chen LC, Geiser M, Reed W, Rothen-Rutishauser B, Schürch S, Schulz H. (2006) Translocation and potential neurological effects of fine and ultrafine particles a critical update. Part Fibre Toxicol. 3:13. PMID: 16961926
Polymenakou PN et al (2008) Particle size distribution of airborne microorganisms and pathogens during an intense African dust event in the eastern Mediterranean. Environ Health Perspect 116(3):292–296
Pope CA 3rd. (1989) Respiratory disease associated with community air pollution and a steel mill, Utah Valley. Am J Public Health. 79(5):623-8. PMID: 2495741
Pope CA 3rd. (1991) Respiratory hospital admissions associated with PM10 pollution in Utah, Salt Lake, and Cache Valleys. Arch Environ Health. 46(2):90-7. PMID: 2006899
Pope CA 3rd, Schwartz J, Ransom MR. (1992) Daily mortality and PM10 pollution in Utah Valley. Arch Environ Health. 47(3):211-7. PMID: 1596104
Pope CA III, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE et al (1995) Particulate air pollution as a predictor of mortality in a prospective study of US adults. Am J Respir Crit Care Med 151:669–674. https://doi.org/10.1164/ajrccm/151.3_pt_1.669
Pope CA III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K et al (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287:1132–1141. https://doi.org/10.1001/jama.287.9.1132
Pratviel G (2012) Chapter 7. Oxidative DNA damage mediated by transition metal ions and their complexes. In: Sigel A, Sigel H, Sigel RKO (eds) Interplay between metal ions and nucleic acids metal ions in life sciences, pp 201–216. Springer. https://doi.org/10.1007/978-94-007-2172-2_7
Putaud JP, Van Dingenen R, Alastuey A, Bauer H, Birmili W, Cyrys J et al (2010) A European aerosol phenomenology - 3: physical and chemical characteristics of particulate matter from 60 rural, urban, and curbside sites across Europe. Atmos Environ 44(10):1308–1320. https://doi.org/10.1016/jatmosenv.2009.12.011
Quan C, Sun Q, Lippmann M, Chen LC. (2010) Comparative effects of inhaled diesel exhaust and ambient fine particles on inflammation, atherosclerosis, and vascular dysfunction. Inhal Toxicol. 22(9):738-53. https://doi.org/10.3109/08958371003728057.
Rappold AG, Stone SL, Cascio WE et al (2011) Peat bog wildfire smoke exposure in rural North Carolina is associated with cardiopulmonary emergency department visits assessed through syndromic surveillance. Environ Health Perspect 119:1415–1420
Reid JS, Koppmann R, Eck TF, Eleuterio DP (2005) A review of biomass burning emissions part II: intensive physical properties of biomass burning particles. Atmos Chem Phys 5:799–825
Reid CE, Brauer M, Johnston FH, Jerrett M, Balmes JR, Elliott CT (2016) Critical review of health impacts of wildfire smoke exposure. Environ Health Perspect 124:1334–1343. https://doi.org/10.1289/ehp.1409277
Rokoff LB, Koutrakis P, Garshick E, Karagas MR, Oken E, Gold DR, Fleisch AF. (2017) Wood Stove Pollution in the Developed World: A Case to Raise Awareness Among Pediatricians. Curr Probl Pediatr Adolesc Health Care. 47(6):123-141. https://doi.org/10.1016/j.cppeds.2017.04.001.
Saffari A, Daher N, Shafer MM, Schauer JJ, Sioutas C (2014) Global perspective on the oxidative potential of airborne particulate matter: a synthesis of research findings. Environ Sci Technol 48(13):7576–7583
Saffari A, Hasheminassab S, Wang D, Shafer MM, Schauer JJ, Sioutas C (2015) Impact of primary and secondary organic sources on the oxidative potential of quasi-ultrafine particles (PM0.25) at three contrasting locations in the Los Angeles Basin. Atmos Environ 120:286–296
Sastry N (2002) Forest fires, air pollution, and mortality in southeast Asia. Demography 39:1–23
Seilkop SK, Campen MJ, Lund AK, McDonald JD, Mauderly JL (2012) Identification of chemical components of combustion emissions that affect pro-atherosclerotic vascular responses in mice. Inhal Toxicol 24(5):270–287
Shafer MM, Perkins DA, Antkiewicz DS, Stone EA, Quraishi TA, Schauer JJ (2010) Reactive oxygen species activity and chemical speciation of size-fractionated atmospheric particulate matter from Lahore, Pakistan: an important role for transition metals. J Environ Monit 12(3):704–715
Shiraiwa M, Ueda K, Pozzer A, Lammel G, Kampf CJ, Akihiro Fushimi, … Weber (2017) Aerosol health effects from molecular to global scales. Environ Sci Technol 51(23):13545–43567. https://doi.org/10.1021/acs.est.7b04417
Sholkovitz ER, Sedwick PN, Church TM, Baker AR, Powell CF (2012) Fractional solubility of aerosol iron: synthesis of a global-scale data set. Geochim Cosmochim Acta 89:173–189. https://doi.org/10.1016/j.gca.2012.04.022
Sigsgaard T, Forsberg B, Annesi-Maesano I, Blomberg A, Bølling A, Boman C, Bønløkke J, Brauer M, Bruce N, Héroux ME, Hirvonen MR, Kelly F, Künzli N, Lundbäck B, Moshammer H, Noonan C, Pagels J, Sallsten G, Sculier JP, Brunekreef B. (2015) Health impacts of anthropogenic biomass burning in the developed world. Eur Respir J. 46(6):1577-88. https://doi.org/10.1183/13993003.01865-2014.
Singh DK, Gupta T (2016) Role of transition metals with water soluble organic carbon in the formation of secondary organic aerosol and metallo-organics in PM1 sampled during post monsoon and pre-winter time. J Aerosol Sci 94:56–69. https://doi.org/10.1016/j.jaerosci.2016.01.002
Sioutas C, Kim S, Chang M (1999) Development and evaluation of a prototype ultrafine particle concentrator. J Aerosol Sci 30:1001–1012
Snider G, Weagle C, Murdymootoo K, Ring A, Ritchie Y et al (2016) Variation in global chemical composition of PM2.5: emerging results from SPARTAN. Atmos Chem Phys 16:9629–9653
Straney L, Finn J, Dennekamp M et al (2014) Evaluating the impact of air pollution on the incidence of out-of-hospital cardiac arrest in the Perth Metropolitan Region: 2000–2010. J Epidemiol Commun Health 68:6–12
Stone V, Miller MR, Clift MJD, Elder A, Mills NL, Moller P, … Cassee FR (2017) Nanomaterials versus ambient ultrafine particles: an opportunity to exchange toxicology knowledge. Environ Health Perspect 125(10):106002. https://doi.org/10.1289/ehp424
Thurston GD, Ito K, Lall R, Burnett RT, Turner MC, Krewski D, Shi, Y, Jerrett M, Gapstur SM, Diver WR, Pope CA III (2013) NPACT study 4 Mortality and long-term exposure to PM2.5 and its components in the American cancer society’s cancer prevention study II Cohort. In: National Particle Component Toxicity (NPACT) initiative: integrated epidemiologic and toxicologic studies of the health effects of particulate matter components. Res Rep 177. Health Effects Institute, Boston, MA
Thurston GD, Kipen H, Annesi-Maesano I, Balmes J, Brook RD, Cromar K et al (2017) A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. Eur Respir J 49(1):1600419. https://doi.org/10.1183/13993003.00419-2016
Truong H, Lomnicki S, Dellinger B (2010) Potential for misidentification of environmentally persistent free radicals as molecular pollutants in particulate matter. Environ Sci Technol 44(6):1933–1939. https://doi.org/10.1021/es902648t
van Donkelaar A, Martin RV, Brauer M, Hsu NC, Kahn RA, Levy RC, Lyapustin A, Sayer AM, Winker DM (2016) Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ Sci Technol 50(7):3762–3772
Vedal S, Kim SY, Miller KA, Fox JR, Bergen S, Gould T, Kaufman JD, Larson TV, Sampson PD, Sheppard L, Simpson SD, Szpiro AA (2013) Section 1. NPACT epidemiologic study of components of fine particulate matter and cardiovascular disease in the MESA and WHI-OS Cohorts. In: National particle component toxicity (NPACT) initiative report on cardiovascular effects. Res Rep 178. Health Effects Institute, Boston, MA
Vejerano EP, Rao G, Khachatryan L, Cormier SA, Lomnicki S (2018) Environmentally persistent free radicals: insights on a new class of pollutants. Environ Sci Technol 5:2468–2481
Verisk (2017) Wildfire risk analysis. https://www.verisk.com/insurance/visualize/key-findings-from-the-2017-verisk-wildfire-risk-analysis/?utm_source=Social&utm_medium=Twitter&utm_campaign=VeriskSM&utm_content=842017. Accessed 31 May 2019
Vieira JL, Guimaraes GV, de Andre PA, Cruz FD, Saldiva PHN, Bocchi EA (2016) Respiratory filter reduces the cardiovascular effects associated with diesel exhaust exposure: a randomized, prospective, double-blind, controlled study of heart failure: the FILTER-HF trial. JACC: Heart Failure 4(1):55–64 https://doi.org/10.1016/j.jchf.2015.07.018
Voutsa D, Samara C (2002) Labile and bioaccessible fractions of heavy metals in the airborne particulate matter from urban and industrial areas. Atmos Environ 36:3583–3590
Wang M, Beelen R, Stafoggia M Raaschou-Nielsen O, Andersen ZJ, Hoffmann B, Fischer P, Houthuijs D, Nieuwenhuijsen M, Weinmayr G, Vineis P0, Xun WW, Dimakopoulou K, Samoli E, Laatikainen T, Lanki T, Turunen AW, Oftedal B, Schwarze P, Aamodt G, Penell J, De Faire U, Korek M, Leander K, Pershagen G, Pedersen NL, Östenson CG, Fratiglioni L, Eriksen KT, Sørensen M, Tjønneland A, Bueno-de-Mesquita B0, Eeftens M, Bots ML, Meliefste K, Krämer U, Heinrich J, Sugiri D, Key T, de Hoogh K, Wolf K, Peters A, Cyrys J, Jaensch A, Concin H0, Nagel G, Tsai MY, Phuleria H, Ineichen A, Künzli N, Probst-Hensch N, Schaffner E, Vilier A, Clavel-Chapelon F, Declerq C, Ricceri F, Sacerdote C, Marcon A, Galassi C, Migliore E, Ranzi A, Cesaroni G, Badaloni C, Forastiere F, Katsoulis M, Trichopoulou A, Keuken M0, Jedynska A0, Kooter IM0, Kukkonen J, Sokhi RS, Brunekreef B, Katsouyanni K, Hoek G. (2014) Long-term exposure to elemental constituents of particulate matter and cardiovascular mortality in 19 European cohorts: results from the ESCAPE and TRANSPHORM projects. Environ Int. 66:97-106. https://doi.org/10.1016/j.envint.2014.01.026
Weagle CL, Snider G, Li C, van Donkelaar A, … and Martin RV. (2018). Global sources of fine particulate matter: interpretation of PM2.5 chemical composition observed by SPARTAN using a global chemical transport model. Environ Sci Technol 52(20):11670–11681 https://doi.org/10.1021/acs.est.8b01658
Weichenthal S, Crouse DL, Pinault L, Godri-Pollitt K, Lavigne E, Evans G, van Donkelaar A, Martin RV, Burnett RT (2016) Oxidative burden of fine particulate air pollution and risk of cause-specific mortality in the Canadian Census Health and Environment Cohort (CanCHEC). Environ Res 146:92–99. https://doi.org/10.1016/j.envres.2015.12.013
Wegesser TC, Pinkerton KE, Last JA (2009) California wildfires of 2008: coarse and fine particulate matter toxicity. Environ Health Perspect 117(6):893–897. https://doi.org/10.1289/ehp0800166
WHO Regional Office for Europe (2013) Review of evidence on health aspects of air pollution—REVIHAAP Project, Technical Report Copenhagen: WHO Regional Office for Europe. http://www.euro.who.int/__data/assets/pdf_file/0004/193108/REVIHAAP-Final-technical-report.pdf
WHO (2016) Ambient air pollution: a global assessment of exposure and burden of disease. World Health Organization. http://www.who.int
WHO (2018) 9 out of 10 people worldwide breathe polluted air, but more countries are taking action. News Release, 2 May 2018. http://www.who.int/news-room/detail/02-05-2018-9-out-of-10-people-worldwide-breathe-polluted-air-but-more-countries-are-taking-action
Wiseman C (2015) Analytical methods for assessing metal bioaccessibility in airborne particulate matter: a scoping review. Anal Chim Acta 877:9–18. https://doi.org/10.1016/j.aca.2015.01.024
Wyzga RE, Rohr AC (2015) Long-term particulate matter exposure: attributing health effects to individual PM components. J Air Waste Manag Assoc 65(5):523–543. https://doi.org/10.1080/10962247.2015.1020396
Yang BY, Qian Z, Howard SW, Vaughn MG, Fan SJ, Liu KK, Dong GH (2018) Global association between ambient air pollution and blood pressure: a systematic review and meta-analysis. Environ Pollut 235:576–588. https://doi.org/10.1016/j.envpol.2018.01.001
Ye D, Klein M, Mulholland JA, Russell AG, Weber R, Edgerton ES, Chang HH, Sarnat JA, Tolbert PE, Ebelt Sarnat S (2018) Estimating acute cardiovascular effects of ambient PM2.5 metals. Environ Health Perspect 126(2):027007. https://doi.org/10.1289/ehp2182
Youssouf H, Liousse C, Roblou L, Assamoi EM, Salonen RO, Maesano C, Banerjee S, Annesi-Maesano I (2014) Non-accidental health impacts of wildfire smoke. Int J Environ Res Pub Health 11:11772–11804
Zhou J, Ito K, Lall R, Lippmann M, Thurston G (2011) Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ Health Perspect 119:461–466. https://doi.org/10.1289/ehp.1002613
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Chen, LC., Maciejczyk, P. (2020). Size and Composition Matters: From Engineered Nanoparticles to Ambient Fine Particles. In: Jiang, G., Li, X. (eds) A New Paradigm for Environmental Chemistry and Toxicology. Springer, Singapore. https://doi.org/10.1007/978-981-13-9447-8_15
Download citation
DOI: https://doi.org/10.1007/978-981-13-9447-8_15
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-9446-1
Online ISBN: 978-981-13-9447-8
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)