
Abstract
Liver resection is based on a sound understanding of segmental anatomy which essentially defines the relationship between elements of the vasculobiliary tree and its associated parenchyma, made largely of organized cords of hepatocytes. Carl Langenbuch is credited with performing the first elective liver resection in 1888. The initial approaches focussed on directly splitting the parenchyma by mechanical means (finger ‘fracture’ or ‘Kelly-clysis’) with bleeding controlled by sutures as it arose. Pringle, in 1908, reported temporary occlusion of vascular inflow at the porta as a means of reducing blood loss while transecting the liver.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


9.1 Introduction
Liver resection is based on a sound understanding of segmental anatomy which essentially defines the relationship between elements of the vasculobiliary tree and its associated parenchyma, made largely of organized cords of hepatocytes. Carl Langenbuch is credited with performing the first elective liver resection in 1888. The initial approaches focussed on directly splitting the parenchyma by mechanical means (finger ‘fracture’ or ‘Kelly-clysis’) with bleeding controlled by sutures as it arose. Pringle, in 1908, reported temporary occlusion of vascular inflow at the porta as a means of reducing blood loss while transecting the liver.
During the early days of liver surgery, perioperative mortality from major liver resections, which was performed only in selected specialized centres, was in the range of 50%. In modern surgical practice, this has been dramatically reduced to less than 5%. Advances in anaesthesia, asepsis, transfusion medicine and perioperative intensive care have all had a vital contribution in making resection safe and more widely available. From the surgical point of view, three factors have changed both surgeon performance and patient outcomes: (1) better patient risk profiling leading to better patient selection and preoperative optimization; (2) refinement and standardization of the techniques of vascular control, haemostasis and transection; and (3) technological advances that have made a wide array of gadgets available that assist, directly or indirectly, a quick and safe resection.
For the purpose of this review, technical adjuncts are those that are either specialized modifications of standard surgical steps or conditions under which surgery is performed. Technological adjuncts cover those that use special gadgets or interventions that make liver surgery safe, quick or precise (Table 9.1). However, the combination of resection and ablative techniques, such as RFA, for bilobar lesions, although could be construed as adjuncts is beyond the remit of this review. Similarly, the advances in preoperative imaging and the various techniques of screening for bile leak at the end of the transection are not discussed.
9.2 Technical Adjuncts
9.2.1 Vascular Control
9.2.1.1 Vascular Inflow Occlusion
Mass clamping the portal triad at the hepatoduodenal ligament which shuts both the portal venous and hepatic arterial flow (vascular inflow occlusion) is a useful adjunct in liver resection. This was first described by Hogarth Pringle from Glasgow in 1908, who applied this, in the setting of liver trauma. The Pringle manoeuvre could be applied in a continuous or intermittent fashion and in both normal and cirrhotic livers. The technique involves encircling the hepatoduodenal ligament with a tape, the free ends of which pass through a piece of rubber tubing which gently tightens the loop snugly around the hepatic pedicle.
Although the maximum recorded ischaemic times for continuous and intermittent Pringle in noncirrhotic livers are 90 min and 348 min, respectively, a more conservative approach is used in actual practice [1, 2]. The maximum reported cumulative ischaemic time after intermittent Pringle in a cirrhotic liver is 204 min [3].
Intermittent Pringle, employed in consecutive cycles of occlusion and release, is the most widely used technique. The most common practice is to use intermittent clamping (ischaemia) for 15 min followed by a declamping (reperfusion) interval of 5 min. There is, however, a wide variation in the period of ischaemia (10–30 min) and the reperfusion (3–10 min) used in practice. Continuous Pringle may be used for up to 90 min in healthy livers (noncirrhotic, nonsteatotic, noninflammed, non-cholestatic) and up to 50 min in diseased livers (including cirrhotic) [4].
The consensus is that intermittent Pringle is better tolerated than continuous Pringle, especially in diseased livers. Ischaemic preconditioning (IPM), in which a short period of ischaemia (10 min) followed by reperfusion (10 min) is performed before an intended longer period of ischaemia (<75 min of continuous Pringle), protects the liver by attenuating the reperfusion injury [4, 5]. Cirrhotic livers and steatotic livers benefit more from IPM.
9.2.1.2 Total Vascular Exclusion (TVE)
Tumours involving the confluence of hepatic veins or the cava are not usually resectable by conventional techniques, as this requires a complete asanguinous field and often involves vascular reconstruction. TVE makes this feasible and involves a controlled occlusion of inflow as well as the outflow. The inflow occlusion is as for a standard Pringle. The outflow occlusion has two variants—(1) with caval occlusion which involves clamping the supra and infrahepatic cava and (2) without caval occlusion, which involves clamping the hepatic veins. Caval occlusion needs a veno-venous bypass to preserve haemodynamic stability. The portal flow is also diverted by a portosystemic venous bypass. The safe time up to which the liver tolerates ischaemia during TVE is about 60 min [4].
9.2.1.3 Total Vascular Exclusion + In Situ Cold Perfusion
The limitation of TVE alone is that hepatic warm ischaemia beyond 60 min exponentially increases the risks of post hepatectomy liver failure (PHLF) and influences mortality. The cytoprotective effects of core visceral hypothermia when combined with TVE results in the extension of the safe time available by a few hours, as cold ischaemia is better tolerated than warm ischaemia. In situ cold perfusion is accomplished by cannulating the gastroduodenal artery for arterial perfusion and the portal vein for portal perfusion. There also needs to be a caval vent as an outlet to drain the effluent. Systemic and portal veno-venous bypass should be in place.
9.2.1.4 TVE + Ante Situm Resection
Ante situm resection is a technique which disconnects the outflow while retaining continuity of the inflow. After infrahepatic caval control, the suprahepatic cava is cut below a clamp, and this allows the liver to be delivered close to the wound. The inflow control, cold perfusion and veno-venous bypass are standard. The advantage of this technique is that it provides the much needed mobility and access to the liver while keeping the inflow structures in continuity. Elimination of the need to transect and later anastomose the inflow structures reduces morbidity.
9.2.1.5 Ex Vivo Resection
This is an extension of the above techniques and involves an explant of the liver with or without the cava. Cold perfusion with a preservation solution protects the liver when the resection is being carried out on the bench. The liver is later autotransplanted applying the transplant techniques. Morbidity and mortality of ex vivo resection are high, as often the remnant is small and involves vascular and biliary reconstruction. There should be a backup plan of salvage liver transplantation when contemplating ex vivo resection.
9.2.2 Low Central Venous Pressure (CVP)
Although the practice of maintaining a low CVP in liver surgery has not been directly linked to a reduced morbidity, it is known that perioperative blood transfusion is associated with adverse postoperative and oncological outcomes after liver resection [6]. Maintaining a low central venous pressure (CVP) of under 5 mmHg, during parenchymal transection, reduces blood loss and need for blood transfusion. This is often done by a combination of strategies by the anaesthetist, including fluid restriction, reverse Trendelenburg position, glyceryl trinitrate infusion and diuresis (mannitol/frusemide). Caval clamping and hepatic inflow occlusion are also surgical techniques that may occasionally be used to achieve a lower CVP. The ideal method to lower CVP and the ideal range of pressure has not been established.
9.2.3 Associating Liver Partition and Portal vein ligation for Staged hepatectomy (ALPPS)
The technique of associating liver partition and portal vein ligation for staged hepatectomy, known as the ALPPS procedure, is a short interval, two-staged liver resection which involves an open right portal vein ligation and in situ parenchymal transection in the right trisectionectomy plane in the first stage [7]. The second stage performed 1–2 weeks later involves a right trisectionectomy. Compared to PVE, ALPPS produces an accelerated hypertrophy of the future liver remnant (FLR) in a much shorter time span. The main downside of ALPPS is the high morbidity and mortality in most reported series. Salvage ALPPS may have a place in patients who do not show an adequate hypertrophy response to PVE. It is a relatively new technique whose place in the surgical armamentarium will be defined with accumulating global experience.
9.3 Technological Adjuncts
9.3.1 Devices to Aid Transection
Several techniques and instruments have been developed in the past few decades to aid liver transection in order to improve safety, reduce bleeding, save time and attain good bilio- and haemostasis. The basic principle on which most of these instruments work is by removing the liver parenchyma and leaving behind vessels and ducts intact to be ligated separately or using energy to seal all the structures completely. The former is the preferred mechanism as it allows selective ligation of vessels and ducts and reduces both bleeding and bile leaks. Also, as it is under vision, it prevents inadvertent injury to the adjacent intraparenchymal structures. Devices that seal directly (termed precoagulation) run the risk of bleeding or bile leak in the event of incomplete coagulation as also lateral thermal damage. Often, more than one energy source and technological adjuncts are used during transection. The list of the technological adjuncts used in hepatic resections is long and ever growing. This itself is a testimony to the fact that no single instrument has been able to fulfil all the requirements uniformly in all the situations. The commonly used technological adjuncts have been summarized in Table 9.1.
Finger Fracture
Though strictly not a technological adjunct, we discuss the finger fracture technique here as it was amongst the first techniques proposed to improve the safety of hepatic resections by reducing blood loss and bile leaks [8]. Introduced by Lin in 1954, it consisted of crushing the liver parenchyma between the thumb and finger of the operator. This left behind vessels and bile ducts which could be safely ligated and divided. Though this was an improvement over the sharp transection, especially when combined with a Pringle manoeuvre, it was nevertheless still associated with significant blood loss from small vessels which avulsed in the process and led to persistent bleeding. Also, this technique led to loss of parenchyma owing to the blunt and wide area of dissection. Hence, it did not gain widespread acceptance. Further, with advancements in instruments available for liver resection, this technique is rarely used today.
Kelly-Clysis
Kelly-clysis or the clamp crush technique was also introduced by Lin in 1974 as an improvement over his previously proposed technique of finger fracture [9]. It has since then become a commonly practiced technique which does not require any expensive gadgets. It consists of using a Kelly or artery forceps to crush the parenchyma between the jaws of the instrument, which leaves the vessels and biliary radicles intact for ligation and division under vision, thereby reducing the blood loss and bile leak rates. Given the simplicity of the technique and the associated advantages of low cost, speed and safety, this technique has become the standard against which all other techniques are compared. The technique has stood the test of time, and none of the randomized trials or meta-analysis performed till date have been able to prove the superiority of other techniques or gadgets over this technique [10, 11].
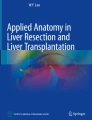
CUSA (Cavitron Ultrasonic Surgical Aspirator) (Fig. 9.1)
This uses ultrasonic energy to fragment the liver parenchyma, leaving behind vascular and biliary structures. The transducer oscillates at a frequency of 23 kHz. A hollow conical tip is attached to it which transmits this ultrasonic energy and fragments the parenchyma. The high water content of hepatocytes renders them susceptible to the ultrasonic energy, whereas the vessels and ducts are spared owing to the high content of connective tissue which is poor in water and rich in intracellular bonds. The continuous flow of water cools the tip, and the suction and aspiration technology removes the fragmented parenchyma from the field providing a clear vision. Further suction technology also helps in drawing the tissue towards the tip of the probe, providing a coupling effect. The suction pressure, irrigation speed and the amplitude can be changed to suit the requirements. The vascular and biliary ducts can then be ligated and divided separately. Unipolar or bipolar diathermy is often used for division of smaller structures, while the larger ones are either clipped or suture ligated before division. It fragments the parenchyma within a distance of 1–2 mm. CUSA machines with integrated electrocoagulation function are also available. CUSA probes that oscillate at different frequencies are available for application in various tissues. Further, CUSA can also be used without the need for vascular control. However, because of the need to separately ligate and divide even small structures, transection using CUSA becomes time consuming. Moreover, in cirrhotic livers, CUSA is not very useful as the fibrosis prevents easy parenchymal transection. Also CUSA has been reported to be associated with greater risks of venous air embolism, though there were no haemodynamic consequences [12]. Additionally, there is a learning curve associated with the device, which is rather cumbersome to use.

(a) CUSA in liver resection. (b) CUSA machine
Fan et al. reported their experience with CUSA and compared it with their own historical controls and found a significantly lower rate of blood loss, transfusion requirement, complications and mortality [13]. However, these results have not been reproduced in randomized trials. Takayama et al. compared CUSA with the clamp crush technique in a randomized trial and failed to show any significant reduction in blood loss [14]. However, vascular occlusion was used in both arms which could have been responsible for reduction in blood loss in the clamp crush arm. Moreover, the standard transection technique of the group was clamp crush, which could have resulted in superior results in the clamp crush arm. Nevertheless, a UK national survey revealed that CUSA was used by over half the liver surgeons to aid transection [15]. It is one of the most popular techniques to help transection, possibly because of its ability to clearly see structures before division and avoidance of vascular occlusion.
Waterjet (Fig. 9.2)
This works on a principle similar to CUSA, but instead of ultrasonic waves, it uses the kinetic energy of a pressurized jet of water to fragment the soft liver parenchyma. Rau et al. reported in their experimental studies that a pressure of 30–40 bar through a nozzle of 0.1 mm is adequate for fragmentation of normal parenchyma. They also found that cirrhotic livers required a pressure of 10 bars more than normal livers [16]. Similar to CUSA, the vascular and biliary structures need to be ligated separately. This too has an irrigation and suction technology integrated into the device to provide a clear field. The pressure of the water can be adjusted according to the nature of the liver. Cirrhotic livers are fibrotic and require a higher pressure for parenchymal disruption. However, this also places these livers at a higher risk of bleeding owing to disruption of small vessels. Newer models are also integrated with a diathermy machine, to provide the electrocoagulation function without needing to switch instruments. This saves time but both functions cannot be used simultaneously. A potential advantage of the waterjet system is the negligible necrosis that occurs at the margin. Further it allows dissection near the major hepatic veins and IVC also. One of the important drawbacks of the waterjet technique is splashes and spillage with potential for contamination. There may be a potential for spread of tumour cells as well exposure of the operator to the infective particles.

(a) Waterjet in liver resection. (b) Waterjet dissection machine and applicators (Reproduced with permission from in.erbe-med.com)
Rau et al. reported their experience with the use of waterjet in 350 patients and demonstrated reduced blood loss, lower transfusion requirements, faster resection and reduced need of Pringle manoeuvre [16]. However, most of the experience with waterjet has also come from this group alone.
Ultrasonic Scalpel (Harmonic®) (Fig. 9.3)
This is an energy device that coagulates and cuts using ultrasonic energy. It is effective in sealing vessels 2–3 mm in diameter. The generator produces a frequency of 55.5 kHz at which the blades vibrate. The ultrasonic vibration of blades produces heat and denatures the proteins in the parenchyma forming a coagulum. Further saw-like motion of the blades then divides the tissue. Since very high temperatures are not attained, lateral thermal damage is limited. However, it is not capable of sealing large blood vessels, and hence this is not useful deep in the parenchyma where large vessels are likely to be encountered. Further, this may not be very effective at sealing bile ducts though the data regarding this is conflicting. Kim et al. reported high bile leak rates of up to 24% with the use of Harmonic shears [17]. However, Mbah et al. found it to be relatively safe in their study [18]. This device may be used alone only for resections of superficial lesions. They are usually combined with other instruments for other resections. They are useful in both laparoscopic and open settings. Primary advantages include ease of application, being smokeless, less lateral spread and lack of need for grounding.

(a) Ultrasonic scalpel in liver resection. (b) Ultrasonic dissection machine
Focus or Fusion Technology
An advancement over the harmonic scalpel has been the development of Harmonic Focus. This has blades like the Kelly clamp, and the nonactivated instrument is used to crush the parenchyma. The residual vessels and ducts are then sealed using activated Focus depending on their size. This technique is proposed to increase speed, and reduce bleeding and postoperative biliary fistulae both [19].
Bipolar Vessel Sealing Device (LigaSure®) (Fig. 9.4)
This device uses bipolar radiofrequency energy to achieve parenchymal transection and sealing of vessels and ducts. It is capable of sealing vessels up to 7 mm in diameter. It acts by denaturing the collagen and elastin fibres in the vessel walls and sealing the vessel. It has found its use primarily in laparoscopic liver resections, where peripheral liver lesions can be resected using LigaSure alone. LigaSure can be used directly for achieving coagulation of the parenchyma followed by transection or can be used in conjunction with the clamp crush technique. A clamp may be used to crush the parenchyma, and LigaSure is then used for sealing the vessels and transection. Similar to the Fusion Technology with Harmonic, LigaSure Precise is available with a clamp-like structure, which can be used to crush the tissue before sealing [20, 21]. LigaSure can also be used without vascular occlusion. The radius of coagulation is around 1 mm, hence reducing the tissue loss.

(a) Bipolar vessel sealing device being used for laparoscopic liver resection. (b) Bipolar vessel sealing device and its laparoscopic probe
LigaSure has been found to increase the speed of transection, reduce blood loss and reduce complications [22]. Romano et al. reported a 17% rate of transfusions and complications with no bile leaks. Though some authors have reported it to be safe even in livers with cirrhosis, they found that its utility was reduced in patients with cirrhosis where it fails to achieve reliable sealing of vessels [23, 24]. They postulated that the fibrotic liver prevented adequate compression and also caused dispersal of the energy resulting in ineffective sealing of vessels and bleeding. Cost and availability are major factors affecting its routine usage. Also, a randomized trial failed to show any benefit of LigaSure over the clamp crush technique [25].
Radiofrequency-Assisted Transection (Fig. 9.5)
This uses the same principle as in radiofrequency ablation of tumours, to ablate and divide the liver parenchyma along the desired plane of transection to achieve a rapid and bloodless resection. This was first described by Weber et al. in 2002 [26]. The technique involves marking the margins of the tumour on the surface of liver parenchyma using intraoperative ultrasound. After this, another line is marked on the liver capsule at a distance of 1 cm from the tumour. Early in their experience, the authors ensured a margin of 2 cm which was later reduced to 1 cm. The probe is positioned with the help of ultrasound.

Radiofrequency device (Habib 4×) being used for resection. (Reproduced with permission from Acharya M, Panagiotopoulos N, Bhaskaran P, Kyriakides C, Pai M, Habib N. Laparoscopic resection of a giant exophytic liver haemangioma with the laparoscopic Habib 4× radiofrequency device. World J Gastrointest Surg. 2012 Aug 27; 4(8): 199–202)
The earliest probes used were monopolar probes which were the same as those designed for the purpose of tumour ablation. Currently multipronged bipolar probes are available which reduce the skin burns, lateral thermal damage and time [27]. However, the tissue necrosis in the remnant liver still remains significant. The primary disadvantage of this technique is that it ablates the entire parenchyma along with the vessels and ducts. Hence, inadvertent injuries to large ducts or vessels are possible. This is reflected in the results of a randomized trial which showed a higher incidence of postoperative complications in the radiofrequency arm (33%) compared to the clamp crush technique (none) [28]. Most surgeons also avoid its use near the hilum or hepatic veins where major structures are likely to be encountered. Also due to the significant tissue necrosis that it produces, there is loss of parenchyma, and this may be problematic in patients with cirrhosis and marginal volume. Further, large vessels may not be coagulated and sealed effectively leading to troublesome bleeding. The other issue is that it is time consuming. Further, its use near the hilum is discouraged owing to the risk of incomplete coagulation because of the heat sink effect.
Most of the experience with this technique has come from a single group. Pai et al. reported on the experience with bipolar radiofrequency device (Habib 4X) in 604 liver resections (206 major and 398 minor). The median blood loss was only 155 mL, with a blood transfusion rate of 12.5%. The morbidity rate was 23.5%, and mortality rate was 1.8%, which is similar to that with other techniques [29]. However, as stated earlier, a randomized trial did not show any benefit but instead a higher rate of complications. Whether lack of adequate experience was responsible for inferior results is unclear.
Microwave
The use of microwave energy in liver surgery was described first in 1981 [30]. Similar to the radiofrequency-assisted transection, this uses microwaves to achieve coagulative necrosis along the proposed line of transection. The needle probe is attached to the generator through a handpiece. The needle is inserted into the liver parenchyma, preferably under ultrasound guidance. The microwaves produce heat that causes denaturation of proteins and coagulative necrosis. Once the parenchyma changes colour to greyish white, the needle is removed and advanced. The radius of coagulation achieved is 5 mm.
Initial reports suggested that though it increased the speed of transection and reduced blood loss, it led to increased postoperative complications in the form of bile leak, collections and fever [31]. Part of it was related to inability of microwaves to seal the biliary channels effectively and partly to the necrotic surface of the remnant liver. Further its use near the hilum remains controversial owing to the high risk of injury to major structures. However, a recent study reviewing 1118 liver resections did not bear this out [32]. The median intraoperative blood loss was 250 mL, and bile leak was noted in 3% and collections in 3.3%. They reported successful use of microwave tissue coagulator even near the hilum. Bile leak rates were comparable to other techniques. However, this could be due to the fact that majority of the resections carried out were minor and nonanatomical. One of the main advantages of this technique however is the fact that no inflow occlusion is required, making it attractive in cirrhotics. Further most patients in this study had diseased livers, thus demonstrating the efficacy of this technique even in cirrhosis. However, the main deterrent to its widespread application remains tissue loss of the remnant liver and the high incidence of bile leaks and collections apart from issues of availability.
Saline-Linked Radiofrequency Sealing Device (Aquamantys®, TissueLink®)
This combines the principle of bipolar electrocoagulation with irrigation. The bipolar cautery coagulates the tissue but restricts the current flow to between the two prongs of forceps. This therefore prevents both skin burns and lateral damage. The continuous irrigation prevents the burnt tissue from sticking to the forceps and cools the area preventing eschar formation. Aquamantys is a commercially available disposable sealer that has a fixed flow of saline and fixed distance between the tips to ensure the same coagulant effect in each use. This is termed as the Transcollation technology that uses saline to improve the tissue sealing effect. Once adequate coagulation is achieved, the tissue can be divided using scissors or cautery. If a sharp tip is being used, it can be used to divide the tissue by gentle traction with the tip itself. The side of the tip is also useful for achieving cut surface coagulation and haemostasis. The device is capable of sealing vessels 3–6 mm in diameter. Larger vessels need to be clipped or ligated. This can be used either as the primary technique for parenchymal transection or in conjunction with other techniques. Curro et al. studied it in 12 cirrhotic patients and found it to be safe, feasible and associated with low blood loss and minimal tissue loss [33]. Kaibori et al. studied its use with CUSA and compared it with a standard bipolar cautery with CUSA and found it to be superior in terms of speed, blood loss and requirement of ties [34]. However, it is a relatively new technique, and safety issues are yet to be resolved completely. A study comparing irrigated bipolar sealer to monopolar cautery found a significantly higher rate of cut surface complications including abscess formation [35]. Though a few studies have shown that it reduces the bleeding and reperfusion injury, it is very time consuming. Xia et al. showed significantly less blood loss and reperfusion injury in cirrhotic livers while using TissueLink when compared to clamp crush technique [36].
Staplers (Fig. 9.6)
Staplers may be used either for division of major vascular pedicles, liver parenchyma or both. The use of staplers for division of portal and hepatic veins was proposed over 20 years ago and has become standard during both open and laparoscopic procedures. Endovascular staplers are also being used for parenchymal transection in both major and minor resections. They are especially useful in left lateral sectionectomy or minor resections where the thickness of parenchyma to be transected is less. In major hepatectomies, the parenchyma is first crushed and fragmented with a clamp, to reduce the thickness and allow application of the stapling device. They can effectively seal both blood vessels and biliary radicles and allow for rapid and safe division of parenchyma. After completion of transection, the surface haemostasis is performed as usual using mono- or bipolar electrocautery and/or argon plasma beam coagulation.

Stapler being used for division of vascular pedicle in laparoscopic liver resection
In a retrospective review of 1174 patients undergoing parenchymal transection using a stapler device (77% major resections and 23% minor resections), the median operating time was 206 min, and blood loss was 300 mL. Only 11% required blood transfusions, and the overall morbidity and mortality were 14% and 3.2%. The safety profile is further validated by the median length of hospital stay of only 7 days. Rare instances (1.1%) of stapler misfire were noted which resulted in bleeding and mortality [37]. Further advantages include the lack of need for vascular control. This is especially useful in patients with liver disease or cirrhosis who tolerate vascular exclusion poorly [38]. Further, staplers are extremely useful in laparoscopic liver resections and have in fact increased in popularity with increasing utilization of minimally access approach for hepatectomy. They are easy to learn and add to the speed and safety. A large database study of 1499 laparoscopic liver resections compared the use of staplers (746 resections) for parenchymal transection with other methods (735 resections) and found significantly shorter operative times, less blood loss and reduced transfusion requirements. Though surgical margins were found to be less in this study in the stapler arm, there were no clinical implications as both groups had similar recurrence and overall and disease free survival rates [39]. Further battery-powered staplers such as iDrive are available today, which make the use of staplers in all locations, angles and tissue thickness ergonomically convenient, easy and safe.
One of the main drawbacks of using staplers is the high cost associated with these devices. However, some authors believe that the reduction in operating time, reduced transfusions and complications offset the direct costs [38]. Also, some authors have raised concerns of bile leak with staplers, but large studies have not uniformly demonstrated this risk [37, 40].
Electrocoagulation
This includes the routinely used monopolar and bipolar diathermy. This is used in conjunction with other devices for dividing small vessels and ducts and fibrous tissue. In addition, these are also used for achieving surface haemostasis. They may also be used for obtaining biopsies from surface lesions or attaining haemostasis thereafter.
Choosing Between the Technologies
The plethora of gadgets to aid transection makes it difficult to choose one. Evidence to support any single device is sparse. The quality of trials available to test these ever increasing devices is poor, with a high risk of bias and significant heterogeneity in inclusion criteria. Further, continuous advancements, modifications and improvements in available devices make it difficult to draw conclusions from the trials.
In a landmark trial, Lesurtel et al. randomized 100 patients to one of the four techniques of clamp crush, CUSA, waterjet or dissecting sealer [41]. They found that the clamp crush technique was the best in terms of resection time, blood loss, transfusion requirement and cost. However, vascular occlusion was used only along with the clamp crush technique, which may bias the result in its favour. Arita et al. compared the clamp crush technique with the saline-linked radiofrequency coagulator and found similar results with no benefit for the sealing device [42]. A randomized trial however did find lower blood loss and faster transection when energy devices were used in liver resections compared to using silk ties. Here the transection in both groups was carried out by CUSA or clamp crush [43]. Rahbari et al. conducted a meta-analysis of seven randomized trials and found no benefit of any device over the clamp crush technique [11].
A recently published meta-analysis concluded that none of the special devices offers any benefit in terms of blood loss, transfusion requirement, morbidity or mortality [10]. What they did note was a higher incidence of adverse events with radiofrequency dissecting sealer, whose use should therefore be restricted to clinical trials.
The final choice of the device used to aid in transection depends on the personal choice of the surgeon, their experiences, knowledge of devices, location of the tumour, the proposed surgical procedure, availability of instruments, their potential complications and cost considerations. Currently, most surgeons use a combination of these devices in transection, to reduce blood loss and increase speed.
9.3.2 Haemostasis
Despite the plethora of gadgets and techniques available to aid the transection of liver parenchyma, bleeding from the cut surface still remains a major issue which ultimately determines the outcomes. Therefore, surgeons continue to rely on a mix of systemic and topical agents which can aid in the haemostasis and biliostasis.
9.3.2.1 Systemic
Several drugs have been tried systemically in an attempt to enhance and aid haemostasis after liver resections. These include tranexamic acid, aprotinin, antithrombin III, recombinant factor VIIa and desmopressin. The use of these agents in liver resections is an extrapolation of their utility in other surgical procedures such as orthopaedic or cardiovascular ones. Of these currently only tranexamic acid is routinely used. Others have been forgone due to either lack of efficacy, cost or side-effects [44,45,46]. It is postulated that liver resection creates a state of accelerated fibrinolysis or hyperfibrinolysis. In addition, a significant proportion of resections involve diseased livers which also add to this fibrinolytic state. Therefore, it was postulated that antifibrinolytic agents like aprotinin and tranexamic acid would reduce bleeding. The role of aprotinin has been studied in only 1 randomized trial in 1999 with 97 patients which showed that it reduces blood loss and transfusion requirements in liver resections [47]. However, no further trials have been conducted to test its utility and safety profile. Furthermore, a higher risk of renal failure, thromboembolic events and mortality was noted in patients undergoing cardiac surgery, which has discouraged its use. Additionally cost considerations have also impeded its use. Tranexamic acid has also been tested in only one randomized trial in 2006 and found to significantly reduce the blood loss and transfusion requirements and operating time [48]. However, tranexamic acid is believed to be associated with a risk of thromboembolic events. Its safety profile needs further elucidation in prospective trials.
Data regarding the utility of systemic agents in liver resections is sparse. Limited data is available in favour of tranexamic acid and aprotinin. However, good-quality trials are needed before their routine use can be recommended [49]. At present, selective use of these agents based on the thromboelastographic profile of the patient may be prudent.
9.3.2.2 Topical Haemostatic Agents
As the name states, these are applied topically to the cut surface of the liver to produce haemostasis. These include surface application of energy or pharmacological agents.
Energy Devices
These include surface application of electrocautery or argon plasma coagulation. Electrocoagulation has previously been discussed.
Argon Plasma Coagulation (Fig. 9.7)
Here, a beam of argon gas is directed from the tip of the probe to aid in the conduction of the radiofrequency energy to the tissue. The energy is delivered through ionized gas, and hence, the probe does not touch the tissue, preventing sticking of the tissue also. Further, the beam is ionized and autodirected towards the tissue with area of least resistance. As it dessicates and chars, the resistance rises, and the beam gets redirected to the raw uncoagulated area. It is faster than other coagulation systems and provides a more superficial and uniform coagulation, reducing deeper tissue damage. Further, it is smokeless and produces less charring. However, its use should be avoided in laparoscopic resections as it increases the risk of gas embolism. Helium plasma coagulator has also been introduced with the same principle using helium gas.

Argon plasma coagulation of cut surface
Pharmacological Agents
These consist of either directly acting agents which form the clot to achieve haemostasis or a matrix which stimulates endogenous clot production. The final step in the common pathway to clot formation is the formation of fibrin from fibrinogen by thrombin and polymerization of fibrin to form a stable clot. The directly acting agents generally contain fibrinogen and thrombin in separate vials which can be mixed and applied to the surface. These are also available bound to a matrix, resulting in a carrier-bound fibrin sealant. Several different formulations are available that differ in the percentages of these components and the presence of additional substances like antifibrinolytic agents, calcium, etc.
Some of the commonly used agents consist of:
-
1.
Those that mimic endogenous coagulation:
-
(a)
Fibrin sealants: Tisseel®, Hemaseel®, Quixil®
-
(b)
Carrier-bound fibrin sealants
-
Collagen fleece coated with fibrinogen and thrombin: TachoSil®, TachoComb®
-
Gelatin and thrombin: FloSeal®
-
Collagen and thrombin: CoStasis®
-
-
(a)
-
2.
Those that provide a matrix for endogenous coagulation:
-
(a)
Cellulose: Surgicel®, Nu-knit®
-
(b)
Gelatin: Gelfoam®, Spongostan®
-
(c)
Collagen: Tissuefleece®, Duracol®
-
(a)
Studies on the efficacy of topical haemostatic agents have shown a statistically significant reduction in the time to haemostasis. The clinical relevance of this finding remains unclear. Since the transfusion requirement is primarily determined by the loss occurring during transection rather than from the cut surface, the clinical relevance with regard to haemostatic potential remains unclear. The other function for which these agents are used is biliostasis. The effect of bile on these agents has been the subject of a few experimental studies. Bile salts have anticoagulant effects and have been shown to prevent the conversion of fibrinogen to fibrin [50]. This could potentially interfere with the biliostatic effect of these agents. However, Fonouni et al. conducted an animal experiment on a porcine model comparing the biliostatic potential of two commercially available sealants with control when applied to the cut surface. They found that the sealant group showed a significant reduction in the incidence of bile leakage [51]. Regardless, most other in vitro experimental studies have failed to reproduce these results. Further, other in vivo studies have also not shown a consistent benefit as far as biliostasis is concerned. Though a small study by Noun et al. showed a significant reduction in the drain output and drain fluid bilirubin, a well powered randomized trial failed to show any difference in bile leak rates [52, 53].
Recent meta-analysis has concluded that though the topical haemostatic agents reduced time to haemostasis, they did not reduce transfusion requirements, collections or bile leak rates [54, 55]. Hence, there seems to be inadequate evidence to support the routine use of topical haemostatic agents. However, surveys amongst liver surgeons reveal that they are popular and used by majority of surgeons with an intent to reduce bleeding, bile leak and collections [56, 57].
Chemical Cauterization
Chemical cauterization of the cut surface has been studied in rat models using ferric sulphate and ferric chloride. This has been found to be useful in achieving haemostasis in a significantly shorter time [58, 59]. However, the efficacy in vivo and adverse effect profile needs to be studied before this can be brought into routine practice.
9.4 Miscellaneous
9.4.1 Portal Vein Embolization
The limits of resection are dictated by the probability of leaving behind a safe volume of functional liver, which has an adequate vascular inflow, venous outflow and biliary drainage. Preoperative portal vein embolization (PVE) is the elective obliteration of portal blood flow to a selected portion of the liver, a few weeks prior to intended major liver resection, with the intention of eliciting a hypertrophic response in the non-embolized portion. Haemodynamic and humoral factors are involved in the hypertrophic response. The purpose is to augment the volume and potentially the function of the future liver remnant (FLR) beyond a safe threshold, so that the risk of post hepatectomy liver failure and its attendant complications including sepsis, multi-organ failure and mortality are avoided or minimized. This usually takes the form of a right portal vein embolization, performed in preparation of a planned future major right-sided resection such as an extended right hepatectomy (in a normal liver) or a right hepatectomy (in a cirrhotic liver). Very rarely, a left portal vein embolization may be indicated before a left-sided resection. The percutaneous PVE can be performed by a transhepatic or transjugular route. The direct transhepatic puncture of the portal vein under image guidance is the classical and most commonly performed technique. There are two minor but important variations, the ipsilateral (same side as the tumour/intended resection) and the contralateral approach, depending on which portal vein is punctured. Embolization of the portal vein branches to segment IV increases the volume of hypertrophy in the remnant in a planned right trisectionectomy.
The percentage increase of standardized FLR (i.e. FLR/estimated total liver volume) that could be expected after PVE at 4–6 weeks ranges from 8 to 13%, although some studies have reported higher rates [60,61,62,63,64]. When expressed as a percentage augmentation from the baseline FLR, this would be a 40–62% increase [64].
PVE is indicated when the FLR is deemed inadequate or unsafe, and there is a reasonable prospect of an increase in the volume of FLR to an extent that would shift the FLR to a zone that would permit safe resection. Though there is no universal consensus on what would be an ideal minimum FLR, most experts would agree on the following broad practical guidelines for considering PVE [65,66,67]:
-
1.
In an otherwise normal liver (unusual in clinical practice):
-
(a)
A standardized FLR of <20%
-
(b)
FLR to body weight ratio of <0.5% [Truant criterion] [68]
-
(a)
-
2.
In the presence of significant steatosis/cholestasis/chemotherapy-associated steatohepatitis/chronic hepatitis (most patients would fall in this category):
-
(a)
A standardized FLR of <30%
-
(b)
FLR to body weight ratio of <0.8%
-
(a)
-
3.
In the presence of cirrhosis (Child A):
-
(a)
A standardized FLR of <40%
-
(b)
FLR to body weight ratio < 1.4%
-
(c)
FLR of <250 mL/m2 [Shirabe criterion] [69]
-
(a)
The volume increase may further be augmented by addition of TACE beforehand, concomitant segmental arterial occlusion, hepatic venous occlusion, stem cell transplantation and branched-chain amino acid supplementation. PVE is well tolerated with a mortality risk of 0.1% and major morbidity risk of 2–3%. The dropout rate of patients who have PVE but do not proceed to resection is up to 25% [70].
9.4.2 Biliary Drainage
Jaundice from biliary obstruction has a wide range of adverse effects which may impact postoperative outcomes. There is experimental evidence for increased bacterial translocation, endotoxemia, reduced Kupffer cell function, increased pro-inflammatory cytokines (TNFα/IL-6) and suppressed cell-mediated immunity [71]. Clinically, liver resection is associated with higher morbidity in jaundiced patients [72]. Poorer oncological outcomes have been recorded in distal obstructions needing a pancreaticoduodenectomy, when the serum bilirubin levels are >18 mg/dL, although there is no conclusive evidence along those lines in liver resections [73]. Biliary drainage, on the other hand, reduces pro-inflammatory cytokines [74] and causes hypertrophy of the liver remnant, when it is drained. The downside of drainage is procedure-related cholangitis, re-intervention rates, prolonged hospital stay, cost, delays in time to surgery and an increase in the risk of tumour seeding.
The volume and functional quality of FLR and the presence of cholangitis are two of the key determinants of PHLF [75]. Although absolute bilirubin level alone has not been shown to be an independent predictor of PHLF, most surgeons would prefer to have the bilirubin less than 5 mg/dL (or 3 mg/dL) before embarking on a major hepatectomy. However, there are centres which have reported safe upfront major liver resections in cohorts of patients with a median bilirubin in the range of 18 mg/dL [76]. If reduction in bilirubin is the goal, then drainage of as little as 30% of the liver would suffice. Major liver resection without drainage has been associated with increased perioperative infective complications and bile leak [72]. The mortality also increases if the FLR is <50% and the obstructed biliary system is undrained [72, 76].
In summary, preoperative biliary drainage when used selectively could be a useful adjunct to liver resection. The indications are summarized in Table 9.2.
9.4.3 Ultrasound-Directed Parenchymal Sparing Resection (Torzilli Technique)
Torzilli has pioneered an intraoperative ultrasound-guided, parenchymal sparing technique which is especially useful in multiple bilobar metastases as seen in colorectal cancer [77]. Two-staged resections which are the standard for bilobar metastasis have a dropout rate of up to 40% which can be avoided by this parenchymal sparing technique [78]. The key principles which set this technique apart from the standard resections are an adequate exposure and mobilization of the liver (with a thoracoabdominal approach, if necessary); a detailed mapping of the lesions under contrast-enhanced ultrasound; accepting minimal (even zero mm) margins; shaving lesions off veins; and resection and reconstruction of hepatic veins, if necessary. Perioperative outcomes (blood loss; general and liver specific morbidity) are better, and oncological outcomes have been shown to be at least on par with conventional two-staged resections [78].
9.4.4 Real-Time Functional FLR Assessment and Fluorescence-Guided Navigation Surgery
The kinetics of indocyanine green (ICG), a fluorescent dye, which is taken up by the liver and excreted in the bile with no enterohepatic circulation, has some unique properties which make it a clinically useful measure of liver function. The ICG plasma disappearance rate (ICG PDR) and retention at 15 min (ICG-R15) are the two commonly used parameters. The normal PDR is >18%/min and the normal ICG-R15 is <10% (or up to 14%). These may be calculated by measurement of the concentration of the dye on serial blood samples or non-invasively by finger spectrophotometry using appropriately calibrated machines. Although ICG has been in clinical use for many years now, for the preoperative stratification of liver function, and this has been incorporated into patient selection algorithms, the intraoperative real-time functional assessment of the liver remnant using ICG is a relatively new concept. ICG PDR after trial clamping of the inflow to the liver being resected has been shown to correlate well with the post resection ICG PDR as well as the incidence of PHLF and hospital stay [79, 80]. Lau et al. have coined the acronym ALIIVE for this technique, which stands for assessment of liver remnant using ICG clearance intraoperatively during vascular exclusion [80]. This technique simulates a post resection-state liver function, at a final intraoperative checkpoint, just before vascular ligation, which would be the point of no return. This increases the margin of safety and makes it possible to make critical decisions even at an advanced stage of the operation. For example if in a planned right trisectionectomy, the intraoperative ICG estimation points to an inadequate functional FLR, then one may resort to an ALPPS procedure; or on the other hand, in a planned ALPPS procedure, if the ICG predicts an adequate functional remnant, then a one-stage resection could be done. Currently, the clinical experience is limited, and more data is needed to draw safe and consistent cut-offs for intraoperative ICG kinetics that could be used reliably in decision-making.
As an extension, the optical properties of ICG-laden tissues have been used to develop systems, which have a number of practical applications in liver resection. Fluorescence imaging using ICG has been in clinical use in other branches of medicine since the 1970s, but its application in liver surgery is a relatively recent development. ICG emits fluorescence when excited by near infra-red light. This needs a specialized imaging system such as the photodynamic eye (PDE; Hamamatsu Photonics; Japan).
Applications in liver surgery include liver mapping for segmental resections, tumour visualization and intraoperative cholangiography. For mapping of liver segments, a 5 mg dose of ICG is injected in the portal vein branch of interest and imaged with a PDE-type system. Repeat injection with or without arterial clamping or even a Pringle manoeuvre may be required to prevent washout and cross-contamination from systemic circulation, if prolonged imaging is required.
Well-differentiated HCC has impaired biliary excretion and hence retains ICG. Poorly differentiated HCCs and metastasis do not take up ICG but compress surrounding normal parenchyma resulting in a rim-type fluorescence. Sensitivity is best for tumours within 5 mm of the surface. The interval between ICG injection and imaging should ideally be at least 2 days, and a single dose of 0.5 mg/kg administered within 14 days of surgery is sufficient to visualize tumours [81].
ICG fluorescence cholangiography offers a road map of the biliary tree while avoiding irradiation and the need for a C-arm. It is also useful in identifying cut surface bile leaks that may be missed by other techniques [82]. For cholangiography the recommended dose is 2.5 mg ICG about half an hour before induction or 10 mg, 24 h before surgery [81].
9.5 Summary
Liver resections are complex surgical procedures, fraught with issues of bleeding, bile leaks, prolonged surgery, inadequate liver remnant and postoperative liver failure. Advances made in the surgical and anaesthetic techniques and technology are increasingly allowing rapid and safe resection with minimal bleeding and few postoperative complications. Further these may help in achieving resection of tumours in central locations or overcoming the issue of insufficient volume. The first step to achieving better outcomes has been an improvement in our understanding of the anatomy of the liver and its vasculobiliary tree. Surgical and anaesthetic techniques that have been developed to reduce bleeding include modifying the vascular inflow and/or outflow and lowering the central venous pressure. Though these are not required for every resection, an understanding of these measures and their effects is paramount for the liver surgeon to safely complete resection in difficult situations.
The other potential target for improving outcomes is the technique of parenchymal transection itself and treatment of the cut surface. Though several devices have been developed to reduce blood loss during transection and decrease postoperative complications, no single technique has shown uniformly consistent results. The age-old technique of clamp crush appears to be best in terms of blood loss, speed, safety and complications. The cut surface can be managed with electrocoagulation or argon plasma coagulation beam or through the use of topical haemostatic agents. Again, no single technique has emerged as superior to the others. In general, surgeons use a mix of all available techniques in different permutations and combinations to achieve a safe resection and good outcome.
Other adjuncts help in improving the quantity and quality of the future liver remnant to reduce chances of postoperative liver failure. A preoperative portal vein embolization can be used to increase future liver remnant volumes. An upcoming alternative is ALPPS which can be used either directly or after a failed PVE. Preoperative biliary drainage is advocated in jaundiced patients to improve the quality of the remnant liver and render resections safer.
To conclude technical and technological advances have made liver resection safe and feasible in most patients. A proper surgical planning utilizing the available options judiciously in the preoperative and intraoperative period is essential for achieving the best results.
Editorial Comments
Liver surgery has become safer than in the past due to a better understanding of the surgical anatomy and a number of technological advances. The improved resectability of liver tumours (both primary and secondary) has led to improved survival. Apart from technical innovations, advances have taken place in technology facilitating safe liver surgery. The authors have adequately dealt with both these aspects in their review. I would like to add the following:
-
1.
Hemihepatic or sequential vascular occlusion selectively blocks the inflow to the tumour-bearing liver or its segment. It thus preserves blood supply to the remaining liver. Moreover, it prevents splanchnic congestion. Haemodynamic instability too is minimized or avoided with this technique. Sometimes, when the tumour infiltrates the hepatic vein or inferior vena cava, there can be substantial backflow, and total vascular occlusion may be required. An alternative to total vascular occlusion is extra-parenchymal control of the hepatic vein and/or the suprahepatic vena cava [83].
-
2.
Acute normovolemic haemodilution. Major bleeding can be a problem during hepatectomy requiring multiple blood transfusions. This is undesirable because it hampers postoperative recovery and affects the oncological outcome. The haemodilution technique has been shown in a randomized study by Maithel and Jarnagin [84] to not increase the requirement for blood transfusion and being as effective as standard management.
-
3.
VIO soft coagulation system. This is a new coagulation device used in hepatic resection. All standard electrosurgical systems produce sparks and cause carbonization and adherence of the electrodes to the liver tissue. As a result haemostasis is not complete causing persistent bleeding. The VIO soft coagulation system avoids these because only joule heat is generated with a voltage limit of 200 v. As a result the coagulation with this device is superior to standard coagulation devices [85].
-
4.
Cryoablation [86]. As with radiofrequency ablation, cryoablation expands the boundaries of liver resection. It is especially useful in metastatic bilobar disease due to colorectal malignancies. For cryoablation of liver tumours, vacuum-insulated coaxial probes are placed during resection under ultrasound guidance. Initially a spinal needle is placed under intraoperative ultrasound guidance, and then probe(s) are placed in the tract thus created. The lesion is then ablated, and it is monitored by the appearance of an iceball (cryoablated tissue) which is hyperechoic with posterior acoustic shadowing. Apart from the tumour, 1 cm circumferential margin of normal tissue surrounding the tumour is also ablated. Once the tissue is frozen, the probes are rewarmed and quickly removed. The needle tract is plugged with a haemostatic agent. Though rare, cryoshock may occur. It is attributed to release of cytokines from tumours which may cause organ failure and disseminated intravascular coagulation. Raised transaminases and a low platelet count are harbingers of this. However, it occurs only when a large amount of tissue is cryoablated. Other cryo-related complications are liver abscess, bile leak, bleeding and pleural effusion. These problems are commonly seen during simultaneous colorectal resection including cryoablation of liver secondaries along with colorectal resection.
-
5.
3D visualization during laparoscopic liver resection. This improves depth perception and helps identify intraparenchymal blood vessels and bile ducts. 3D technology also helps surgeons to complete a hepatectomy faster [87].
-
6.
Augmented reality guidance system. Preoperative CT is routinely used for staging and surgical planning for liver cancers. However, identifying important structures within the liver parenchyma can still be a challenge. The augmenting reality guidance system has been developed to provide real-time intraoperative fluoroscopic ‘C’-arm cone beam CT images. The images projected on a screen can help surgeons navigate easily during surgery and identify vital structures [88].
-
7.
Laparoscopic liver surgery with robotic instruments. Laparoscopic liver resection has been in practice for some years now. One of the problems is the limited movement of the rigid instruments. This compromises the surgeon’s movements and often leads to musculoskeletal pain. To avoid these and improve laparoscopic liver resection, robotic instruments are being developed which will improve ergonomics and surgical skill [89].
-
8.
Robotic liver surgery. Liver resection by robotic surgery is in the evolving phase. There are a number of benefits. It avoids the limitations of laparoscopic liver resection mentioned above. This in turn improves tissue handling and suturing. In robotic surgery the surgeon sits at a console unlike in laparoscopic surgery where the surgeon is struggling with the instruments. The camera and the retractors are controlled by the surgeon, while in laparoscopy it is in the hands of the assistants. A distinct advantage is a short learning curve. The results of robotic liver surgery are similar to laparoscopic liver surgery in terms of operating time, blood loss, bile leak, morbidity and hospital stay. The cost of the robotic procedure is high, and this is hampering its wider use [90].
References
Delva E, Camus Y, Nordlinger B, Hannoun L, Parc R, Deriaz H, et al. Vascular occlusions for liver resections. Operative management and tolerance to hepatic ischemia: 142 cases. Ann Surg. 1989;209(2):211–8.
Procopio F, Torzilli G. Forty-nine colorectal cancer liver metastases in one-stage hepatectomy with cumulative Pringle time lasting 348 min. Updat Surg. 2012;64(3):241–3.
Wu C-C, Hwang C-R, Liu T-J, P’eng F-K. Effects and limitations of prolonged intermittent ischaemia for hepatic resection of the cirrhotic liver. Br J Surg. 1996;83(1):121–4.
van Riel WG, van Golen RF, Reiniers MJ, Heger M, van Gulik TM. How much ischemia can the liver tolerate during resection? Hepatobiliary Surg Nutr. 2016;5(1):58–71.
Clavien PA, Yadav S, Sindram D, Bentley RC. Protective effects of ischaemic preconditioning for liver resection performed under inflow occlusion in humans. Ann Surg. 2000;232(2):155–62.
Hughes MJ, Ventham NT, Harrison EM, Wigmore SJ. Central venous pressure and liver resection: a systematic review and meta-analysis. HPB. 2015;17(10):863–71.
Schnitzbauer AA, Lang SA, Goessmann H, Nadalin S, Baumgart J, Farkas SA, et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg. 2012;255(3):405–14.
Lin TY. Results in 107 hepatic lobectomies with a preliminary report on the use of a clamp to reduce blood loss. Ann Surg. 1973;177(4):413–21.
Lin T-Y. A simplified technique for hepatic resection: the crush method. Ann Surg. 1974;180(3):285–90.
Moggia E, Rouse B, Simillis C, Li T, Vaughan J, Davidson BR, et al. Methods to decrease blood loss during liver resection: a network meta-analysis. Cochrane Database Syst Rev. 2016;10:CD010683.
Rahbari NN, Koch M, Schmidt T, Motschall E, Bruckner T, Weidmann K, et al. Meta-analysis of the clamp-crushing technique for transection of the parenchyma in elective hepatic resection: back to where we started? Ann Surg Oncol. 2009;16(3):630–9.
Koo BN, Kil HK, Choi J-S, Kim JY, Chun DH, Hong YW. Hepatic resection by the Cavitron Ultrasonic Surgical Aspirator increases the incidence and severity of venous air embolism. Anesth Analg. 2005;101(4):966–70, table of contents.
Fan ST, Lai EC, Lo CM, Chu KM, Liu CL, Wong J. Hepatectomy with an ultrasonic dissector for hepatocellular carcinoma. Br J Surg. 1996;83(1):117–20.
Takayama T, Makuuchi M, Kubota K, Harihara Y, Hui AM, Sano K, et al. Randomized comparison of ultrasonic vs clamp transection of the liver. Arch Surg. 2001;136(8):922–8.
Lochan R, Ansari I, Coates R, Robinson SM, White SA. Methods of haemostasis during liver resection—a UK national survey. Dig Surg. 2013;30(4–6):375–82.
Rau HG, Duessel AP, Wurzbacher S. The use of water-jet dissection in open and laparoscopic liver resection. HPB. 2008;10(4):275–80.
Kim J, Ahmad SA, Lowy AM, Buell JF, Pennington LJ, Soldano DA, et al. Increased biliary fistulas after liver resection with the harmonic scalpel. Am Surg. 2003;69(9):815–9.
Mbah NA, Brown RE, Bower MR, Scoggins CR, McMasters KM, Martin RCG. Differences between bipolar compression and ultrasonic devices for parenchymal transection during laparoscopic liver resection. HPB. 2012;14(2):126–31.
Jagannath P, Chhabra DG, Sutariya KR, Shah RC. Fusion technique for liver transection with Kelly-clysis and harmonic technology. World J Surg. 2010;34(1):101–5.
Nanashima A, Tobinaga S, Abo T, Nonaka T, Sawai T, Nagayasu T. Usefulness of the combination procedure of crash clamping and vessel sealing for hepatic resection. J Surg Oncol. 2010;102(2):179–83.
Patrlj L, Tuorto S, Fong Y. Combined blunt-clamp dissection and LigaSure ligation for hepatic parenchyma dissection: postcoagulation technique. J Am Coll Surg. 2010;210(1):39–44.
Nanashima A, Abo T, Arai J, Takagi K, Matsumoto H, Takeshita H, et al. Usefulness of vessel-sealing devices combined with crush clamping method for hepatectomy: a retrospective cohort study. Int J Surg. 2013;11(9):891–7.
Saiura A, Yamamoto J, Koga R, Seki M, Yamaguchi T. Liver transection using the LigaSure sealing system. HPB. 2008;10(4):239–43.
Romano F, Franciosi C, Caprotti R, Uggeri F, Uggeri F. Hepatic surgery using the Ligasure vessel sealing system. World J Surg. 2005;29(1):110–2.
Ikeda M, Hasegawa K, Sano K, Imamura H, Beck Y, Sugawara Y, et al. The vessel sealing system (LigaSure) in hepatic resection: a randomized controlled trial. Ann Surg. 2009;250(2):199–203.
Weber J-C, Navarra G, Jiao LR, Nicholls JP, Jensen SL, Habib NA. New technique for liver resection using heat coagulative necrosis. Ann Surg. 2002;236(5):560–3.
Ayav A, Jiao L, Dickinson R, Nicholls J, Milicevic M, Pellicci R, et al. Liver resection with a new multiprobe bipolar radiofrequency device. Arch Surg. 2008;143(4):396–401.
Lupo L, Gallerani A, Panzera P, Tandoi F, Palma GD, Memeo V. Randomized clinical trial of radiofrequency-assisted versus clamp-crushing liver resection. Br J Surg. 2007;94(3):287–91.
Pai M, Frampton AE, Mikhail S, Resende V, Kornasiewicz O, Spalding DR, et al. Radiofrequency assisted liver resection: analysis of 604 consecutive cases. Eur J Surg Oncol. 2012;38(3):274–80.
Tabuse K, Katsumi M. Application of a microwave tissue coagulator to hepatic surgery the hemostatic effects on spontaneous rupture of hepatoma and tumor necrosis. Nihon Geka Hokan. 1981;50(4):571–9.
Lau WY, Arnold M, Guo SK, Li AK. Microwave tissue coagulator in liver resection for cirrhotic patients. Aust N Z J Surg. 1992;62(7):576–81.
Sasaki K, Matsuda M, Hashimoto M, Watanabe G. Liver resection for hepatocellular carcinoma using a microwave tissue coagulator: experience of 1118 cases. World J Gastroenterol. 2015;21(36):10400–8.
Currò G, Lazzara S, Barbera A, Cogliandolo A, Dattola A, De Marco ML, et al. The Aquamantys® system as alternative for parenchymal division and hemostasis in liver resection for hepatocellular carcinoma: a preliminary study. Eur Rev Med Pharmacol Sci. 2014;18(2 Suppl):2–5.
Kaibori M, Matsui K, Ishizaki M, Sakaguchi T, Matsushima H, Matsui Y, et al. A prospective randomized controlled trial of hemostasis with a bipolar sealer during hepatic transection for liver resection. Surgery. 2013;154(5):1046–52.
Patrizi A, Jezequel C, Sulpice L, Meunier B, Rayar M, Boudjema K. Disposable bipolar irrigated sealer (Aquamantys(®)) for liver resection: use with caution. Updat Surg. 2016;68(2):171–7.
Xia F, et al. The use of saline-linked radiofrequency dissecting sealer for liver transection in patients with cirrhosis. J Surg Res. 2008;149:110. [cited 2018 Jul 27]. https://www.ncbi.nlm.nih.gov/pubmed/18541264.
Raoof M, Aloia TA, Vauthey J-N, Curley SA. Morbidity and mortality in 1,174 patients undergoing hepatic parenchymal transection using a stapler device. Ann Surg Oncol. 2014;21(3):995–1001.
Schemmer P, Friess H, Hinz U, Mehrabi A, Kraus TW, Z’graggen K, et al. Stapler hepatectomy is a safe dissection technique: analysis of 300 patients. World J Surg. 2006;30(3):419–30.
Buell JF, Gayet B, Han H-S, Wakabayashi G, Kim K-H, Belli G, et al. Evaluation of stapler hepatectomy during a laparoscopic liver resection. HPB. 2013;15(11):845–50.
Wang W-X, Fan S-T. Use of the Endo-GIA vascular stapler for hepatic resection. Asian J Surg. 2003;26(4):193–6.
Lesurtel M, Selzner M, Petrowsky H, McCormack L, Clavien P-A. How should transection of the liver be performed? Ann Surg. 2005;242(6):814–23.
Arita J, Hasegawa K, Kokudo N, Sano K, Sugawara Y, Makuuchi M. Randomized clinical trial of the effect of a saline-linked radiofrequency coagulator on blood loss during hepatic resection. Br J Surg. 2005;92(8):954–9.
Gotohda N, Yamanaka T, Saiura A, Uesaka K, Hashimoto M, Konishi M, et al. Impact of energy devices during liver parenchymal transection: a multicenter randomized controlled trial. World J Surg. 2015;39(6):1543–9.
Chavez-Tapia NC, Alfaro-Lara R, Tellez-Avila F, Barrientos-Gutiérrez T, González-Chon O, Mendez-Sanchez N, et al. Prophylactic activated recombinant factor VII in liver resection and liver transplantation: systematic review and meta-analysis. PLoS One. 2011;6(7):e22581. [cited 2018 Jul 28]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144913/.
Shimada M, Matsumata T, Kamakura T, Hayashi H, Urata K, Sugimachi K. Modulation of coagulation and fibrinolysis in hepatic resection: a randomized prospective control study using antithrombin III concentrates. Thromb Res. 1994;74(2):105–14.
Wong AYC, Irwin MG, Hui TWC, Fung SKY, Fan ST, Ma ESK. Desmopressin does not decrease blood loss and transfusion requirements in patients undergoing hepatectomy. Can J Anesth. 2003;50(1):14–20.
Lentschener C, Benhamou D, Mercier FJ, Boyer-Neumann C, Naveau S, Smadja C, et al. Aprotinin reduces blood loss in patients undergoing elective liver resection. Anesth Analg. 1997;84(4):875–81.
Wu C-C, Ho W-M, Cheng S-B, Yeh D-C, Wen M-C, Liu T-J, et al. Perioperative parenteral tranexamic acid in liver tumor resection. Ann Surg. 2006;243(2):173–80.
Gurusamy KS, Li J, Sharma D, Davidson BR. Pharmacological interventions to decrease blood loss and blood transfusion requirements for liver resection. Cochrane Database Syst Rev. 2009;(4):CD008085.
Haessler H, Stebbins MG. Effect of bile on the clotting time of blood. J Exp Med. 1919;29(5):445–9.
Fonouni H, Kashfi A, Stahlheber O, Konstantinidis L, Kraus TW, Mehrabi A, et al. Analysis of the biliostatic potential of two sealants in a standardized porcine model of liver resection. Am J Surg. 2017;214(5):945–55.
Figueras J, Llado L, Miro M, Ramos E, Torras J, Fabregat J, et al. Application of fibrin glue sealant after hepatectomy does not seem justified. Ann Surg. 2007;245(4):536–42.
Noun R, Elias D, Balladur P, Bismuth H, Parc R, Lasser P, et al. Fibrin glue effectiveness and tolerance after elective liver resection: a randomized trial. Hepato-Gastroenterology. 1996;43(7):221–4.
Sanjay P, Watt DG, Wigmore SJ. Systematic review and meta-analysis of haemostatic and biliostatic efficacy of fibrin sealants in elective liver surgery. J Gastrointest Surg. 2013;17(4):829–36.
Brustia R, Granger B, Scatton O. An update on topical haemostatic agents in liver surgery: systematic review and meta analysis. J Hepatobiliary Pancreat Sci. 2016;23(10):609–21.
Nakajima Y, Shimamura T, Kamiyama T, Matsushita M, Sato N, Todo S. Control of intraoperative bleeding during liver resection: analysis of a questionnaire sent to 231 Japanese hospitals. Surg Today. 2002;32(1):48–52.
Boonstra EA, Molenaar IQ, Porte RJ, de Boer MT. Topical haemostatic agents in liver surgery: do we need them? HPB. 2009;11(4):306–10.
Nouri S, Sharif MR. Use of ferric sulfate to control hepatic bleeding. Trauma Mon. 2015;20(1):e25257.
Poon RT, Fan ST, Wong J. Liver resection using a saline-linked radiofrequency dissecting sealer for transection of the liver. J Am Coll Surg. 2005;200(2):308–13.
Goéré D, Farges O, Leporrier J, Sauvanet A, Vilgrain V, Belghiti J. Chemotherapy does not impair hypertrophy of the left liver after right portal vein obstruction. J Gastrointest Surg. 2006;10(3):365–70.
Imamura H, Shimada R, Kubota M, Matsuyama Y, Nakayama A, Miyagawa S, et al. Preoperative portal vein embolization: an audit of 84 patients. Hepatology. 1999;29(4):1099–105.
Leung U, Simpson AL, Araujo RLC, Gönen M, McAuliffe C, Miga MI, et al. Remnant growth rate after portal vein embolization is a good early predictor of post-hepatectomy liver failure. J Am Coll Surg. 2014;219(4):620–30.
Shindoh J, Truty MJ, Aloia TA, Curley SA, Zimmitti G, Huang SY, et al. Kinetic growth rate after portal vein embolization predicts posthepatectomy outcomes: toward zero liver-related mortality in patients with colorectal liver metastases and small future liver remnant. J Am Coll Surg. 2013;216(2):201–9.
Shindoh J, Vauthey J-N, Zimmitti G, Curley SA, Huang SY, Mahvash A, et al. Analysis of the efficacy of portal vein embolization for patients with extensive liver malignancy and very low future liver remnant volume, including a comparison with the associating liver partition with portal vein ligation for staged hepatectomy approach. J Am Coll Surg. 2013;217(1):126–33; discussion 133-134.
Abdalla EK, Adam R, Bilchik AJ, Jaeck D, Vauthey J-N, Mahvi D. Improving resectability of hepatic colorectal metastases: expert consensus statement. Ann Surg Oncol. 2006;13(10):1271–80.
Ribero D, Chun YS, Vauthey J-N. Standardized liver volumetry for portal vein embolization. Semin Interv Radiol. 2008;25(2):104–9.
Dixon E, Abdalla E, Schwarz RE, Vauthey J-N. AHPBA/SSO/SSAT sponsored consensus conference on multidisciplinary treatment of hepatocellular carcinoma. HPB. 2010;12(5):287–8.
Truant S, Oberlin O, Sergent G, Lebuffe G, Gambiez L, Ernst O, et al. Remnant liver volume to body weight ratio > or =0.5%: a new cut-off to estimate postoperative risks after extended resection in noncirrhotic liver. J Am Coll Surg. 2007;204(1):22–33.
Shirabe K, Shimada M, Gion T, Hasegawa H, Takenaka K, Utsunomiya T, et al. Postoperative liver failure after major hepatic resection for hepatocellular carcinoma in the modern era with special reference to remnant liver volume. J Am Coll Surg. 1999;188(3):304–9.
van Lienden KP, van den Esschert JW, de Graaf W, Bipat S, Lameris JS, van Gulik TM, et al. Portal vein embolization before liver resection: a systematic review. Cardiovasc Intervent Radiol. 2013;36(1):25–34.
Kimmings AN, van Deventer SJ, Obertop H, Rauws EA, Huibregtse K, Gouma DJ. Endotoxin, cytokines, and endotoxin binding proteins in obstructive jaundice and after preoperative biliary drainage. Gut. 2000;46(5):725–31.
Cherqui D, Benoist S, Malassagne B, Humeres R, Rodriguez V, Fagniez PL. Major liver resection for carcinoma in jaundiced patients without preoperative biliary drainage. Arch Surg. 2000;135(3):302–8.
Sauvanet A, Boher J-M, Paye F, Bachellier P, Sa Cuhna A, Le Treut Y-P, et al. Severe jaundice increases early severe morbidity and decreases long-term survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. J Am Coll Surg. 2015;221(2):380–9.
Padillo FJ, Muntane J, Montero JL, Briceño J, Miño G, Solorzano G, et al. Effect of internal biliary drainage on plasma levels of endotoxin, cytokines, and C-reactive protein in patients with obstructive jaundice. World J Surg. 2002;26(11):1328–32.
Ribero D, Zimmitti G, Aloia TA, Shindoh J, Fabio F, Amisano M, et al. Preoperative cholangitis and future liver remnant volume determine the risk of liver failure in patients undergoing resection for hilar cholangiocarcinoma. J Am Coll Surg. 2016;223(1):87–97.
Abdel Wahab M, El Hanafy E, El Nakeeb A, Hamdy E, Atif E, Sultan AM. Postoperative outcome after major liver resection in jaundiced patients with proximal bile duct cancer without preoperative biliary drainage. Dig Surg. 2015;32(6):426–32.
Torzilli G, Procopio F, Botea F, Marconi M, Del Fabbro D, Donadon M, et al. One-stage ultrasonographically guided hepatectomy for multiple bilobar colorectal metastases: a feasible and effective alternative to the 2-stage approach. Surgery. 2009;146(1):60–71.
Torzilli G, Viganò L, Cimino M, Imai K, Vibert E, Donadon M, et al. Is enhanced one-stage hepatectomy a safe and feasible alternative to the two-stage hepatectomy in the setting of multiple bilobar colorectal liver metastases? A comparative analysis between two pioneering centers. Dig Surg. 2018;35(4):323–32.
Thomas MN, Weninger E, Angele M, Bösch F, Pratschke S, Andrassy J, et al. Intraoperative simulation of remnant liver function during anatomic liver resection with indocyanine green clearance (LiMON) measurements. HPB. 2015;17(6):471–6.
Lau L, Christophi C, Nikfarjam M, Starkey G, Goodwin M, Weinberg L, et al. Assessment of liver remnant using ICG clearance intraoperatively during vascular exclusion: early experience with the ALIIVE technique. HPB Surg. 2015;2015:757052.
Majlesara A, Golriz M, Hafezi M, Saffari A, Stenau E, Maier-Hein L, et al. Indocyanine green fluorescence imaging in hepatobiliary surgery. Photodiagn Photodyn Ther. 2017;17:208–15.
Kaibori M, Ishizaki M, Matsui K, Kwon AH. Intraoperative indocyanine green fluorescent imaging for prevention of bile leakage after hepatic resection. Surgery. 2011;150(1):91–8.
Sgourakis G, Lantis S, Kontovounisios C, Korontzi M, Karaliotas C, Zacharioudakis K, et al. Hepatic vascular occlusion during liver resection. Hell J Surg. 2010;10:310–7.
Maithel SK, Jarnagin WR. Adjuncts to liver surgery: is acute normovolemic hemodilution useful for major hepatic resections? Adv Surg. 2009;43:259–68.
Hirokawa F, Hayashi M, Miyamoto Y, Iwamoto M, Tsunematsu I, Asakuma M, et al. A novel method using the VIO soft-coagulation system for liver resection. Surgery. 2011;149:438–44.
Ng KM, Chua TC, Saxena A, Zhao J, Chu F, Morris DL. Two decades of experience with hepatic cryotherapy for advanced colorectal metastases. Ann Surg Oncol. 2012;19:1276–83.
van der Vorst JR, Schaafsma BE, Hutteman M, Verbeek FP, Liefers GJ, Hartgrink HH, et al. Near-infrared fluorescence-guided resection of colorectal liver metastases. Cancer. 2013;119:3411–8.
Kenngott HG, Wagner M, Gondan M, Nickel F, Nolden M, Fetzer A, et al. Real-time image guidance in laparoscopic liver surgery: first clinical experience with a guidance system based on intraoperative CT imaging. Surg Endosc. 2014;28:933–40.
Hermon B, Zahraee AH, Szewczyk J, Morel G, Bourdin C, Verche J-L, et al. Ergonomic and gesture performance of robotized instruments for laparoscopic surgery. 2011 IEEE/RSJ International Conference on Intelligent Robots and Systems. https://doi.org/10.1109/IROS.2011.6094449.
Leung U, Fong Y. Robotic liver surgery. Hepatobiliary Surg Nutr. 2014;3:288–94.
Conflict of Interest Statement
The authors declare no conflicts of interest. The list of commercially available devices and products is by no means complete, and several other products may be available in each category which are beyond the scope of this review.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Indian Association of Surgical Gastroenterology
About this chapter

Cite this chapter
Kilambi, R., Kumar, S. (2019). Adjuncts to Liver Resection. In: Sahni, P., Pal, S. (eds) GI Surgery Annual. GI Surgery Annual, vol 25. Springer, Singapore. https://doi.org/10.1007/978-981-13-3227-2_9
Download citation
DOI: https://doi.org/10.1007/978-981-13-3227-2_9
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-3226-5
Online ISBN: 978-981-13-3227-2
eBook Packages: MedicineMedicine (R0)