
Abstract
Human trichomoniasis is a sexually transmitted disease of global concern with millions of cases reported worldwide. The causative agent is Trichomonas vaginalis, a flagellated protozoan, which primarily resides in the genitourinary tract of affected women and men. Apart from causing discomfort due to malodourous discharge, vaginal irritation, and dysuria, it can also cause complications such as infections of the adjoining glands and endometrium, premature labor in pregnant women, and even cervical dysplasia. The diagnosis can be made on clinical examination, wet mount microscopy, stained smear examination, and antigen detection using commercial kits. Rapid nucleic acid amplification-based platforms are also available which demonstrate high sensitivity and specificity for detection of T. vaginalis. The management primarily consists of administration of 2 g of a single dose of oral metronidazole or tinidazole, with concomitant treatment of the sexual partner. Prevention of infection in high-risk individuals can be ensured by using condoms, microbicidal vaginal suppositories, and hydrogels containing antimicrobial peptides. Vaccination has shown promise in animal trichomoniasis; however, identification of candidates for human use and subsequent development of vaccines for humans are still in the pipeline.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Hydrogels
- Microbicidal vaginal suppositories
- Sexually transmitted disease
- Trichomoniasis
- Trichomonas vaginalis
1 Introduction
Human trichomoniasis is perhaps the most common sexually transmitted infection (STI) after viral STI’s in the world. Even though various serious health-related consequences can result from this infection, it still remains underrecognized, underreported, and largely ignored. This disease is caused by Trichomonas vaginalis, an anaerobic, flagellated parasite, and its trophozoite stage commonly resides in the genital and urinary tract of men and women. The trophozoite multiplies in the host and is transmitted via unprotected sexual intercourse. Although commonly asymptomatic, particularly in men, unusual genital discharge, burning or pain during micturition, and genital irritation are the most common clinical symptoms. Trichomoniasis has been linked to the facilitation of the HIV pandemic and can also result in pelvic inflammatory disease and poor outcomes in pregnant women if not recognized as a public health concern by clinicians and healthcare authorities. Global estimates suggest that there are an estimated 143 million cases of trichomoniasis, and approximately 90% of these infections are prevalent in patients from resource-limited settings (WHO 2008; Newman et al. 2015).
2 Epidemiology
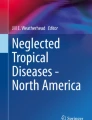
The true epidemiology of trichomoniasis is largely unknown due to lack of surveillance programs. However, there is considerable variability depending on patient population, the region of study, and diagnostic test used. While studies in women from the United States (USA) have described prevalence rates of 2–3% in the 14–49 age group, studies from African patients show a particularly higher prevalence rate (Kissinger 2015). Screening studies in women attending antenatal clinics have been used to indicate the trends of prevalence in the general population, and using this approach, prevalence rates ranging from 3.2% to 52% were noted in resource-limited settings, while they were much lower at 7.6–12.6% in the developed countries like the United States (Johnston and Mabey, 2008). The region-wise global distribution of trichomoniasis is depicted in Fig. 6.1.

WHO region-wise global estimates of trichomoniasis as per systematic review and global analysis in 2015 (Newman et al. 2015)
A prevalence of trichomoniasis ranging from 3.6% to 31% has been documented in Indian studies, the details of which are described in Table 6.1. It has been noted that the annual years of healthy life lost per 100,000 people due to trichomoniasis in Indian women has risen by 4% since 1990 at rate of 0.2% healthy life lost per year (Global Disease Burden 2017).
Risk factors associated with the development of trichomoniasis include commercial sex work, use of intravenous drugs, older age, African descent, and bacterial vaginosis. Among Indian women, it has been noted that those with infection are more likely to have lower levels of education, be married to an uneducated partner, belong to poor socioeconomic status, and report having sexual relations with more than one partner (Madhivanan et al. 2009).
3 Etiological Agent
The causative agent of trichomoniasis in humans is Trichomonas vaginalis, a flagellated protozoan. It has a primarily anaerobic lifestyle and is present extracellular to the genital and urinary tract epithelium (Kissinger 2015). Typically it exists in a trophozoite form which is pyriform in shape but can occasionally be amoeboid. It is approximately 10–20 μm in length and 2–14 μm in width with four flagella projecting from the anterior end and one flagellum extending posteriorly toward the middle of the trophozoite to form an undulating membrane. An axostyle can be seen extending from the posterior aspect of the trophozoite. The illustrated diagram and scanning electron microscopy image of T. vaginalis trophozoite are shown in Fig. 6.2a, b, respectively.

(a) Illustrated diagram of T. vaginalis; (b) scanning electron microscopy image of T. vaginalis. (Source : Adapted from Korean J Parasitol Vol. 51, No. 2: 243-246, April 2013 BRIEF COMMUNICATION http://dx.doi.org/10.3347/kjp.2013.51.2.243)
Apart from trophozoites, pseudocyst forms of T. vaginalis have also been found in animals and could have relevance in humans. The flagella in the pseudocyst form are located inside endocytic vacuoles and remain beating, the axostyle is present in a curved shape, and a distinct mitotic process has also been described (Pereira-Neves et al. 2003). The pseudocyst is round, shows no motility, and does not have a true cyst wall on light microscopy (Afzan and Suresh 2012). Cyst forms of T. vaginalis have not been demonstrated to date.
4 Pathogenesis
T. vaginalis is an obligate parasite which infects the squamous epithelium of the genital tract. It resides and replicates in the lower female genital tract and the male urethra and prostate. It is a predatory parasite which can phagocytose vaginal epithelial cells, bacteria, as well as erythrocytes for nutrition. Since no cyst form is present, the parasite cannot survive in the external environment. However, in a moist environment outside the human body, reports of surviving up to 3 h have been documented (Burch et al. 1959). Humans are its only known hosts, and transmission among them is primarily by sexual intercourse. Although rare, there is evidence of nonsexual transmission, with reports of transmission via fomites and possibly water (Crucitti et al. 2011).
5 Clinical Features
The incubation time for trichomoniasis is generally between 4 and 28 days, although most of the women (85%) and men (77%) with infection are asymptomatic. Some studies even suggest that asymptomatic women can harbor T. vaginalis in their genital tract for as many as 3–5 years. This could be due to the type of infecting strain, variations in genitourinary anatomy, or merely lack of imperfect tools for screening (Swygard et al. 2004). Among the asymptomatic women, nearly a third of them become symptomatic after 6 months.
The most commonly infected sites in women include the vagina, the urethra, and lastly the endocervix. The chief presenting complaint is most commonly vaginal discharge, noted in >50% cases, followed by itching and dysuria. Irritation of the vulvar region and abdominal pain may also be present. Per speculum examination reveals vaginal discharge which is characteristically frothy green and malodorous (Swygard et al. 2004). The vaginal pH is often markedly increased, often to more than five. Cervical pathology can be observed in the form of “colpitis macularis” also called “strawberry cervix,” which can be seen in 5% of women. When a colposcopic examination is carried out, it may be observed in as high as 50% of the infected women. It results from microscopic, punctate hemorrhages over the cervix causing the cervix to appear erythematous, edematous, and friable. Cervical mucopurulent discharge and other complications such as infections of the adnexa, Skene and Bartholin glands, and even the endometrium can occur.
There are reports of the pseudocyst forms of this agent being described from patients suffering from cervical neoplasia and may potentially play a role in exacerbating cervical cancer (Afzan and Suresh 2012). However, it is too early to come to such a conclusion with the currently available data. It has been noted that T. vaginalis infection has a significant association with the risk of developing pelvic inflammatory disease particularly in women with HIV infection (Moodley et al. 2002). Association between preterm labor and T. vaginalis infection has also been demonstrated in pregnant women (Hosney et al. 2017).
Information regarding trichomoniasis in men is limited, and they may often be asymptomatic. Common symptoms include urethral discharge (often less profuse and purulent than women) and dysuria. Seroepidemiologic evidence indicating an association of T. vaginalis with prostate cancer has emerged suggesting that infection may increase the risk of more aggressive cancer. However, most recent studies have found no associations between the two (Marous et al. 2017; Shui et al. 2016).
6 Diagnosis
The appropriate clinical specimens for diagnosis of trichomoniasis include urine, vaginal fluid, or endocervical swabs in women and in men; urethral discharge, urethral scrapings, urine, prostate secretions or semen may be used. Testing multiple sites is advisable especially in men (Swygard et al. 2004). Vaginal secretions can be obtained from the fornices and the lateral vaginal wall using a plastic loop or swab. They may be collected by the patients themselves or collected by the concerned physician. The self-collection of samples tends to have better acceptability among patients and has a similar performance when compared to clinician acquired samples.
-
1.
Direct microscopic examination: For the wet mount preparation, collected secretions are suspended in normal saline and subjected to light microscopic examination under high-power field (40×). Diagnosis relies on visual detection of viable trophozoites of T. vaginalis which can be identified based on their appearance and characteristic motility. The size of the trichomonas trophozoite is comparable to a lymphocyte (10–20 μm), and it may, therefore, be difficult to identify in case the motility is lost. Motility depends on the ambient temperature and moisture in the sample, and since it can be lost quickly, the specimen must be examined within 10–20 min of sample collection. Although it is quick and inexpensive, the sensitivity of direct microscopy varies from 38% to 82% and depends on the inoculum size (should be >104 organisms/mL), the time interval between sample collection and examination, and the experience of the microbiologist (Garber 2005; Schwebke and Burgess 2004).
-
2.
Isolation: Culture has been traditionally considered as the gold standard for diagnosing T. vaginalis infection. It can detect as low as 102 organisms/mL in the sample, and results are also easy to interpret (Garber 2005). Several media are available for culture, such as Diamond’s TYI liquid broth media, cysteine-peptone-liver-maltose (CPLM), Feinberg and Whittington’s medium, and self-contained culture systems (InPouch TV kit). Culture techniques have 100% specificity and a higher sensitivity (75–85%) compared to microscopy as a much lower concentration of parasite is needed for culture positivity (Pattullo et al. 2009). The drawbacks are higher cost and long turnaround time for diagnosis (3–7 days). Hence, screening for trichomoniasis using the only culture may not be a convenient approach. Cultivation of T. vaginalis on cell cultures has an even higher sensitivity and enables diagnosis form samples containing as few as three parasites/mL (Garber 2005). However, this technique is expensive and impractical and is highly prone to contamination by vaginal flora.
-
3.
Nucleic acid amplification tests (NAAT): Molecular tests have become common for diagnosing infection with T. vaginalis and can detect as low as one organism. Polymerase chain reaction has been performed most notably on vaginal fluids and urine. Urine-based PCR detection of T. vaginalis was performed with sensitivity and specificity of 64–90.8% and 93.4–100%, respectively, in women (Lawing et al. 2000) and 92.7% and 88.6%, respectively, in men (Kaydos-Daniels et al. 2003). The PCR amplification of 18S rRNA and pfoB gene of T. vaginalis has also been shown to have a specificity of 95.1% and 94.8%, respectively, in symptomatic subjects and 90.2% and 88.5% in asymptomatic patients, while a sensitivity of 100% has been noted in all cases (Sonkar et al. 2016). Dot-blot hybridization has also been used, employing a 2.3 kb T. vaginalis DNA fragment as a probe. The APTIMA® Trichomonas vaginalis assay is an amplification-based assay for T. vaginalis cleared by the USFDA which utilizes target capture followed by transcription-mediated amplification and chemiluminescent probe hybridization to detect T. vaginalis ribosomal RNA. Endocervical or vaginal swabs and urine can be tested, and a sensitivity and specificity of 95% and 98%, respectively, have been documented (Chapin and Andrea 2011). GeneXpert platform for the detection of T. vaginalis, the assay has also been evaluated and found to be 95% sensitive and 95–100% specific for diagnosing trichomoniasis when compared to NAAT (Badman et al. 2016). Additional advantages of GeneXpert include small platform requirement and rapid (<1 h) and direct detection from self-collected vaginal swabs and urine (Gaydos et al. 2017).
-
4.
Stained smears: Examination of Papanicolaou (Pap) smear has shown a low sensitivity (61%) for detection of T. vaginalis. Since T. vaginalis resides primarily in the vagina, ectocervical smears have better utility compared to endocervical smears. In a meta-analysis of the performance of Pap smear compared to wet mount preparation, it has been seen that in high prevalence populations, a positive Pap smear had a positive predictive value (PPV) of 83%, whereas it decreased in lower prevalence populations requiring a confirmatory culture for T. vaginalis (Wiese et al. 2000). The use of acridine orange and periodic acid-Schiff have been shown to be valuable by some investigators.
-
5.
Antigen detection tests: A rapid antigen detection-based test by Sekisui Diagnostics called the OSOM Trichomonas rapid test can be applied as a point of care test. It is based on the use of immunochromatographic capillary flow dipstick technology. The results are available in nearly 10 min. A high sensitivity and specificity of 82–95% and 97–100%, respectively, have also been noted (Meites et al. 2015). The details of rapid tests for diagnosis of T. vaginalis are depicted in Table 6.2.
-
6.
Indirect evidence: These include antibody-based methods which include complement fixation, gel diffusion techniques, hemagglutination, and ELISA to detect anti-trichomonas antibodies (Garber 2005). These, however, cannot be used to differentiate recent and remote infections as they are certainly not specific and could even reflect host interaction with nonpathogenic or commensal trichomonas and have thus been abandoned.
-
7.
Others: Presence of pus cells in the vaginal fluid and an elevated pH (>4.5) can indicate infection. The whiff test which is carried out by adding potassium hydroxide to the vaginal fluid for olfactory detection of amines gives variable results.
7 Treatment
In a resource-challenged setting, the screening for cases of trichomoniasis may be difficult and therefore the WHO promotes adopting the syndromic approaches for managing STIs. However, some experts suggest that this approach of managing trichomoniasis has minimal impact on the actual disease prevalence in endemic regions and may, in fact, lead to overtreatment of many cases (Bowden and Garnett 2000). A more fulfilling approach may thus be screening for trichomoniasis followed by treatment of the positive cases.
The treatment of T. vaginalis infection is essential as it reduces the clinical symptoms and prevents further transmission. At present, the only class of antimicrobial agents with known activity against T. vaginalis is nitroimidazoles such as metronidazole and tinidazole. According to the Centers for Disease Control and Prevention (2015), the recommended treatment regimen for trichomoniasis is 2 g of oral metronidazole or tinidazole provided as a single dose. Cure rates of approximately 84–98% and 92–100% have been documented in trials using the recommended metronidazole and tinidazole regimens, respectively. Generally, tinidazole is more expensive than metronidazole, but it reaches higher concentrations in the serum and genitourinary tract and also has a longer half-life and fewer side effects. The comparison of single-dose (2 g) metronidazole versus tinidazole suggests that tinidazole has equal or rather superior activity in achieving clinical relief and parasitological cure (O-Prasertsawat and Jetsawangsri 1992; Anjaeyulu et al. 1977). A 500 mg twice daily administration of metronidazole for 7 days has been found to be more effective than the traditional 2 g single dose in treating trichomoniasis in women with concomitant HIV infection (Kissinger et al. 2010). Gel formulations of metronidazole are available for topical application, but therapeutic levels of metronidazole are seldom reached in the urethra and perivaginal glands, and therefore the topical application of gels is not commonly used for treatment. However, high dose of intravaginal metronidazole (750 mg) with miconazole combination can be given as a vaginal suppository twice a day for 7 days and has been shown to offer well-tolerated treatment avoiding the systemic adverse effects of nitroimidazoles (Schwebke et al. 2013).
Another patient group of concern is pregnant and symptomatic women, who regardless of the stage of pregnancy must be tested and treated. The transmission of trichomoniasis in the perinatal period is uncommon. It is a yet to be proven if treatment of trichomoniasis reduces the risk of preterm labor in pregnant women as many studies with conflicting results are available (Stringer et al. 2010; Mann et al. 2009). The patient should be counseled by the treating physician regarding the potential benefits of treatment. Metronidazole does cross the placenta, but there is no evidence of mutagenicity or teratogenic effects in infants (Meites et al. 2015). The treatment is similar as in nonpregnant women (2 g metronidazole single dose). However, during breast feeding, 500 mg three times daily for 7 days is considered more compatible since it produces lower drug levels in breast milk.
Sexual intercourse must be avoided by all patients until they and their sexual partners are treated and testing for other STDs including HIV must be carried out concomitantly. Abstinence from alcohol, at least for 24–72 h after completion of treatment, is advised to prevent severe side drug-related side effects known as “disulfiram reaction” after metronidazole administration.
Following the treatment, retesting is recommended within 3 months for all patients who are sexually active (CDC 2017).Recurrent or persistent infection can occur most commonly due to reinfection from an untreated sexual partner or occasionally due to antimicrobial-resistant T. vaginalis.
8 Drug Resistance and Antimicrobial Susceptibility Testing
Because most organisms are susceptible to the drug of choice, i.e., metronidazole, antimicrobial susceptibility testing (AST) is not performed routinely. However, there are rising reports of women having clinically resistant T. vaginalis with studies showing clinical resistance to metronidazole in 4–10% cases and tinidazole resistance in 1% (Schwebke and Barrientes 2006; Cudmore and Garber 2010). Some studies suggest that the presence of Mycoplasma hominis symbionts might be associated with the metronidazole resistance of T. vaginalis although concrete evidence is still warranted (Wang and Xie 2012). These reports of resistance are concerning since very few alternatives to the standard treatment are available. If needed, AST can be performed using micro-broth dilution methods or shell vial cultures to determine the minimal inhibitory drug concentration. There are, however, no standardized protocols or proficiency testing available for the same. In drug-resistant cases, a higher dose (2–3 g) of tinidazole can be given for 14 days, often with intravaginal tinidazole or intravaginal paromomycin (CDC 2017; Tayal et al. 2010).
9 Prevention of T. vaginalis Infection
The most reliable protection against sexually transmitted infections such as trichomoniasis is barrier methods, particularly condoms. Other preventive strategies include male circumcision, local application of intravaginal microbicide formulations, and vaccines (Bouchemal et al. 2017). Intravaginal microbicides can be self-administered by women before sexual intercourse, and hydrogels of hydroxyethyl cellulose with antimicrobial peptides or metronidazole have been investigated and found effective in mice models (Bouchemal et al. 2017).
The strategies to combat STIs such as trichomoniasis focus on the following main directions: firstly, knowing the extent of the epidemic by monitoring case counts and infection distribution by region and in time; secondly, by providing a good coverage of quality health services; thirdly, making available adequate funds to minimize the financial constraints of patients requiring services; and finally, innovation and development of technology for rapid diagnosis, effective treatment, and prophylactic strategies to combat this disease (Klausner and Broutet 2017).
10 Vaccine
The development of a vaccine against T. vaginalis could reduce the medical and societal costs associated with trichomoniasis (Cudmore and Garber 2010). The use of T. foetus, a natural pathogen of cattle, in vaccines have shown promise in reducing the duration of bovine infection, and similarly, efforts are ongoing to create a vaccine for human trichomoniasis (Smith and Garber 2014). Establishing good animal models, studies on the T. vaginalis immunity and details of cross-isolate protection are all warranted to accelerate this process. Determining the appropriate components of a vaccine is problematic and may be elucidated following more genomic and proteomic studies on T. vaginalis. These can contribute valuable information to the identification of unique proteins of T. vaginalis that can in future be potential vaccine targets.
References
Afzan MY, Suresh K (2012) Pseudocyst forms of Trichomonas vaginalis from cervical neoplasia. Available from: http://repository.um.edu.my/29663/1/AfzanandSuresh.pdf
Anjaeyulu R, Gupte SA, Desai DB (1977) Single-dose treatment of trichomonal vaginitis: a comparison of tinidazole and metronidazole. J Int Med Res 5:438–441 Available from: http://www.ncbi.nlm.nih.gov/pubmed/590601
Arora BB, Maheshwari M, Devgan N, Arora DR (2014) Prevalence of trichomoniasis, vaginal candidiasis, genital herpes, chlamydiasis, and actinomycosis among urban and rural women of Haryana. Indian J Sex Transm Dis 29:1–5 Available from: http://www.hindawi.com/journals/jstd/2014/963812/
Badman SG, Causer LM, Guy R, Tabrizi SN, Francis F, Donovan B et al (2016) A preliminary evaluation of a new GeneXpert (Gx) molecular point-of-care test for the detection of Trichomonas vaginalis. Sex Transm Infect 92:350–352 Available from: http://sti.bmj.com/lookup/doi/10.1136/sextrans-2015-052384
Bouchemal K, Bories C, Loiseau PM (2017) Strategies for prevention and treatment of Trichomonas vaginalis infections. Clin Microbiol Rev 30:811–825 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28539504
Bowden FJ, Garnett GP (2000) Trichomonas vaginalis epidemiology: parameterising and analysing a model of treatment interventions. Sex Transm Infect 76:248–256 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11026878
Burch TA, Rees CW, Reardon L (1959) Diagnosis of Trichomonas vaginalis vaginitis. Am J Obstet Gynaecol 77:309–313. https://doi.org/10.1016/0002-9378(59)90232-7
Centres for Disease Control and Prevention (CDC). Trichomoniasis-2015 (2017) STD treatment guidelines [internet]. [Cited 2017, July 12]. Available from: https://www.cdc.gov/std/tg2015/trichomoniasis.htm
Chapin K, Andrea S (2011) APTIMA Trichomonas vaginalis, a transcription-mediated amplification assay for detection of Trichomonas vaginalis in urogenital specimens. Expert Rev Mol Diagn 11:679–688 Available from: http://www.tandfonline.com/doi/full/10.1586/erm.11.53
Crucitti T, Jespers V, Mulenga C, Khondowe S, Vandepitte J, Buvé A (2011) Non-sexual transmission of Trichomonas vaginalis in adolescent girls attending school in Ndola, Zambia. PLoS One 6:e16310 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21305023
Cudmore SL, Garber GE (2010) Prevention or treatment: the benefits of Trichomonas vaginalis vaccine. J Infect Public Health 3:47–53 Available from: http://www.ncbi.nlm.nih.gov/pubmed/20701891
Das A, Prabhakar P, Narayanan P, Neilsen G, Wi T, Kumta S et al (2011) Prevalence and assessment of clinical management of sexually transmitted infections among female sex workers in two cities of India. Infect Dis Obstet Gynaecol 2011:494769 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21747642
Deivam S, Rajalakshmi R, Priyadharshini S, Seethalaksmi R, Balasubramanian N, Brinda T et al (2017) Prevalence of Trichomonas vaginalis infection among patients that presented to Rural Tertiary Care Hospital in Tiruchirapalli, India in 2011 and 2013, vol 2, pp 255–260. Available from: http://www.pharmahealthsciences.net/pdfs/urgent/10_MS_1466.pdf
Dickinson B (2017) BD affirm™ VPIII microbial identification system [internet]. [Cited Jul 13]. Available from: http://moleculardiagnostics.bd.com/product/affirm/
Fule R, Fule S, Tankhiwale N (2012) Clinical and laboratory evidence of Trichomonas vaginalis infection among women of reproductive age in rural area. Indian J Med Microbiol 30:314 Available from: http://www.ijmm.org/text.asp?2012/30/3/314/99493
Garber GE (2005) The laboratory diagnosis of Trichomonas vaginalis. Can J Infect Dis Med Microbiol 16:35–38 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18159526
Gaydos CA, Klausner JD, Pai NP, Kelly H, Coltart C, Peeling RW (2017) Rapid and point-of-care tests for the diagnosis of Trichomonas vaginalis in women and men. Sex Transm Infect 93:S31–S35 [Internet]. Jul 6 [cited 2017 Jul 21];sextrans-2016-053063. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28684611
Global-Disease-Burden (2017) Trichomoniasis in India – statistics, demographics affected [internet]. [Cited 2017 Jul 13]. Available from: http://global-disease-burden.healthgrove.com/l/25879/Trichomoniasis-in-India
Hosny AE-DMS, El-Khayat W, Kashef MT, Fakhry MN (2017) Association between preterm labour and genitourinary tract infections caused by Trichomonas vaginalis, Mycoplasma hominis, gram-negative bacilli, and coryneforms. J Chin Med Assoc 80:575–581 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28094234
Johnston VJ, Mabey DC (2008) Global epidemiology and control of Trichomonas vaginalis. Curr Opin Infect Dis 21:56–64 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18192787
Kaydos-Daniels SC, Miller WC, Hoffman I, Banda T, Dzinyemba W, Martinson F et al (2003) Validation of a urine-based PCR-enzyme-linked immunosorbent assay for use in clinical research settings to detect Trichomonas vaginalis in men. J Clin Microbiol 41:318–323 Available from: http://www.ncbi.nlm.nih.gov/pubmed/12517867
Kissinger P (2015) Trichomonas vaginalis: a review of epidemiologic, clinical and treatment issues. BMC Infect Dis 15:307 Available from: http://www.ncbi.nlm.nih.gov/pubmed/26242185
Kissinger P, Mena L, Levison J, Clark RA, Gatski M, Henderson H et al (2010) A randomized treatment trial: single versus 7-day dose of metronidazole for the treatment of Trichomonas vaginalis among HIV-infected women. J Acquir Immune Defic Syndr 55:565–571 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21423852
Klausner JD, Broutet N (2017) Health systems and the new strategy against sexually transmitted infections. Lancet Infect Dis 3099:9–10 Available from: http://linkinghub.elsevier.com/retrieve/pii/S1473309917303614
Lawing LF, Hedges SR, Schwebke JR (2000) Detection of trichomonosis in vaginal and urine specimens from women by culture and PCR. J Clin Microbiol 38:3585–3588 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11015368
Madhivanan P, Bartman MT, Pasutti L, Krupp K, Arun A, Reingold AL et al (2009) Prevalence of Trichomonas vaginalis infection among young reproductive age women in India: implications for treatment and prevention. Sex Health 6:339–344 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19917204
Malla N, Kaur S, Khurana S, Bagga R, Wanchu A (2008) Trichomoniasis among women in North India: a hospital based study. Indian J Sex Transm Dis AIDS 29:76 Available from: http://www.ijstd.org/text.asp?2008/29/2/76/48729
Mann JR, McDermott S, Zhou L, Barnes TL, Hardin J (2009) Treatment of trichomoniasis in pregnancy and preterm birth: an observational study. J Women’s Health 18:493–497 Available from: http://www.ncbi.nlm.nih.gov/pubmed/19361316
Marous M, Huang W-Y, Rabkin CS, Hayes RB, Alderete JF, Rosner B et al (2017) Trichomonas vaginalis infection and risk of prostate cancer: associations by disease aggressiveness and race/ethnicity in the PLCO trial. Cancer Causes Control 28:889–898 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28669054
Meites E, Gaydos CA, Hobbs MM, Kissinger P, Nyirjesy P, Schwebke JR et al (2015) A review of evidence-based care of symptomatic trichomoniasis and asymptomatic Trichomonas vaginalis infections. Clin Infect Dis 61(Suppl. 8):S837–S848 Available from: http://www.ncbi.nlm.nih.gov/pubmed/26602621
Moodley P, Wilkinson D, Connolly C, Moodley J, Sturm AW (2002) Trichomonas vaginalis is associated with pelvic inflammatory disease in women infected with human immunodeficiency virus. Clin Infect Dis 34:519–522 Available from: http://www.ncbi.nlm.nih.gov/pubmed/11797180
Muthusamy S, Elangovan S (2017) A study on the prevalence of genital trichomoniasis among female outpatients attending sexually transmitted infection clinic in a tertiary care hospital. J Lab Phys 9:16–19 Available from: http://www.ncbi.nlm.nih.gov/pubmed/28042211
Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N et al. 2015. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting (Meng Z (ed)). PLoS One 10:e0143304. Available from: http://dx.plos.org/10.1371/journal.pone.0143304
O-Prasertsawat P, Jetsawangsri T (1992) Split-dose metronidazole or single-dose tinidazole for the treatment of vaginal trichomoniasis. Sex Transm Dis 19:295–297 Available from: http://www.ncbi.nlm.nih.gov/pubmed/1411848
Pattullo L, Griffeth S, Ding L, Mortensen J, Reed J, Kahn J et al (2009) Stepwise diagnosis of Trichomonas vaginalis infection in adolescent women. J Clin Microbiol 47:59–63 Available from: http://www.ncbi.nlm.nih.gov/pubmed/18987174
Pereira-Neves A, Ribeiro KC, Benchimol M (2003) Pseudocysts in trichomonads – new insights. Protist 154:313–329 Available from: http://www.ncbi.nlm.nih.gov/pubmed/14658492
Pillay A, Lewis J, Ballard RC (2004) Evaluation of Xenostrip-Tv, a rapid diagnostic test for Trichomonas vaginalis infection. J Clin Microbiol 42:3853–3856 Available from: http://www.ncbi.nlm.nih.gov/pubmed/15297548
Schwebke JR, Barrientes FJ (2006) Prevalence of Trichomonas vaginalis isolates with resistance to metronidazole and tinidazole. Antimicrob Agents Chemother 50:4209–4210 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17000740
Schwebke JR, Burgess D (2004) Trichomoniasis. Clin Microbiol Rev 17:794–803 Available from: http://cmr.asm.org/content/17/4/794.short
Schwebke JR, Lensing SY, Sobel J (2013) Intravaginal metronidazole/miconazole for the treatment of vaginal trichomoniasis. Sex Transm Dis 40:710–714 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23949586
Shui IM, Kolb S, Hanson C, Sutcliffe S, Rider JR, Stanford JL (2016) Trichomonas vaginalis infection and risk of advanced prostate cancer. Prostate 76:620–623 Available from: https://insights.ovid.com/pubmed?pmid=26818005
Smith J, Garber GE (2014) Current status and prospects for development of a vaccine against Trichomonas vaginalis infections. Vaccine 32:1588–1594 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23916988
Sonkar S, Yadav S, Malla N, Dhanda R, Khurana S, Bagga R et al (2016) Evaluation of DNA based techniques for the diagnosis of human vaginal trichomoniasis in North Indian population. Br Microbiol Res J 17:1–12 Available from: http://www.sciencedomain.org/abstract/17070
Stringer E, Read JS, Hoffman I, Valentine M, Aboud S, Goldenberg RL (2010) Treatment of trichomoniasis in pregnancy in sub-Saharan Africa does not appear to be associated with low birth weight or preterm birth. S Afr Med J 100:58–64 Available from: https://pdfs.semanticscholar.org/4c44/f28a3a94532bca269390b3aa5a9c6ea4450e.pdf
Swygard H, Seña AC, Hobbs MM, Cohen MS (2004) Trichomoniasis: clinical manifestations. Diagn Manag Sex Transm Infect 80:91–95 Available from: http://sti.bmj.com/content/sextrans/80/2/91.full.pdf
Tayal SC, Ochogwu SA, Bunce H (2010) Paromomycin treatment of recalcitrant Trichomonas vaginalis. Int J STD AIDS 21:217–218 Available from: http://www.ncbi.nlm.nih.gov/pubmed/20215633
Wang P-J, Xie C-B (2012) Mycoplasma hominis symbiosis and Trichomonas vaginalis metronidazole resistance. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 30:210–213 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23072138
Wiese W, Patel SR, Patel SC, Ohl CA, Estrada CA (2000) A meta-analysis of the Papanicolaou smear and wet mount for the diagnosis of vaginal trichomoniasis. Am J Med 108:301–308 Available from: http://linkinghub.elsevier.com/retrieve/pii/S0002934399004660
World Health Organization (2008) Global incidence and prevalence of selected curable sexually transmitted infections – 2008. WHO. [Internet]. [cited 2017 Jul 10]. Available from: http://www.who.int/reproductivehealth/publications/rtis/stisestimates/en/
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Khurana, S., Singh, S. (2018). Human Trichomoniasis. In: Singh, P. (eds) Infectious Diseases and Your Health. Springer, Singapore. https://doi.org/10.1007/978-981-13-1577-0_6
Download citation
DOI: https://doi.org/10.1007/978-981-13-1577-0_6
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-1576-3
Online ISBN: 978-981-13-1577-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)