
Abstract
Age and apolipoprotein E (ApoE) are the mightiest risk factors for dementia and cardiovascular diseases, but the underlying mechanisms remain unclear. In human, ApoE has three isoforms, ApoE2, ApoE3, and ApoE4, which are expressed by the polymorphic alleles: ɛ2, ɛ3, and ɛ4. Among the three polymorphic alleles, apoE ε4 is the most risk gene. ApoE is the main ligand for the low-density lipoprotein (LDL) receptor and the LDL receptor-related protein (LRP), functioning as the component of plasma lipoproteins in the transportation of lipids. Physiologically, ApoE is a multifunctional protein with central roles in lipid metabolism; it transports lipids, including cholesterol, through the cerebrospinal fluid (CSF) and plasma. ApoE expression regulation and apoE gene polymorphism have an important connection with neurological or neurodegenerative diseases such as Alzheimer’s disease (AD), Parkinson’s disease (PD), ischemic stroke, and other diseases.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
5.1 Introduction
Aging is a complex of biological long-lasting processes that result being unavoidable. Aging and diseases are closely related as aging is the largest risk factor for multiple chronic diseases. Increasing evidence suggests a certain degree of heritability of lifespan. Recently, genome-wide association studies (GWAS) candidate gene studies (CGAS) have identified variation in two genes (Fortney et al. 2015; Johnson et al. 2015), fork head box O3 (FOXO3) and apolipoprotein E (ApoE), to be consistently associated with human longevity, while some other genes have inconsistence (Blanche et al. 2001; Deelen et al. 2011; Schachter et al. 1994; Zhang et al. 1998). Furthermore, ApoE, which is involved in lipoprotein metabolism, is the only age-related gene confirmed in human (Bao et al. 2014; Fortney et al. 2015).
ApoE is a 34 kDa lipid-binding protein which was first discovered by Shore in 1973 in very-low-density lipoprotein (VLDL) (Shore and Shore 1974). It is mainly distributed in VLDL, chylomicron (CM), and their wreckage. ApoE plays an important role in lipoprotein metabolism. It not only can bind to LDL receptor but also bind to the hepatic cell membrane chylomicrons (CM), VLDL debris, and some HDL (which contains ApoE) receptors. The function of ApoE is transportation of triglycerides and cholesterol in multiple tissues (Bu 2009; Leduc et al. 2010; Puglielli et al. 2003; Wang et al. 2006).
Based on the pivotal role of ApoE protein in lipoprotein metabolism in the brain and in the periphery, its expression regulation and expression types have an important connection with Alzheimer’s disease (AD), Parkinson’s disease (PD), multiple sclerosis (MS), vascular dementia (VD), cardiovascular diseases (CVD), type 2 diabetes mellitus (T2DM), and other diseases (Fig. 5.1).

Diseases associated with ApoE
5.1.1 The Structure and Physical Functions of ApoE
The molecular weight of ApoE is 34 kDa, consisting of 299 amino acid residues, rich in arginine with a single glycosylation site at threonine-194 (Lee et al. 2010; Rall et al. 1982; Weisgraber 1994). The secondary structure of ApoE was constituted of α-helix, β-turn β-sheet, and a “hinge region” which divides ApoE into two independent domains: the N-terminal domain (amino acids 1–191), two thirds of ApoE, contains the lipoprotein receptor-binding region (amino acids 136–150), and the C-terminal domain (amino acids 225–299) contains the lipid-binding region (amino acids 244–272) (Rasmussen 2016; Weisgraber 1994). X-ray crystallography solved the tertiary structure of the N-terminal domains of ApoE which consists of four helices arranged in antiparallel fashion (Weisgraber 1994), the lipoprotein receptor-binding region (amino acids 136–150) is in the fourth helix.
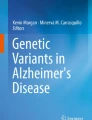
In contrast to other mammals, humans present three isoforms of ApoE, named ApoE2, ApoE3, and ApoE4, which are expressed by the polymorphic alleles: ɛ2, ɛ3, and ɛ4 (Tudorache et al. 2017). The substitution of Arg and Cys, two amino acid residues at positions 112 and 158 of the ApoE amino acid sequence, determines the type of isoforms: ApoE4 is Arg at both positions; ApoE2 is Cys; Cys at position 112 and Arg at position 158 are ApoE3 subtypes. The isoforms of ApoE display preferences for specific classes of lipoproteins, and ApoE4 prefers large, triglyceride-rich VLDL particles, whereas ApoE3 and ApoE2 associate preferentially with the small, phospholipid-rich HDL (Huang and Mahley 2014). The strange thing is the residues that differ the ApoE isoforms are in the N-terminal (E4, arginine 112; E3 and ApoE2, cysteine 112). However, the lipid-binding region is in the C-terminal (amino acids 244–272). This suggests that there may be a domain interaction between the N- and C-terminal domains in ApoE4; arginine 112 may orient the side chain of arginine 61 into the aqueous environment and then interact with glutamic acid 255, which determines the preference of ApoE4 for VLDL and of ApoE3 and ApoE2 for HDL (Huang and Mahley 2014) (Fig. 5.2).

Schematic illustration of structures of ApoE isoforms and its functional regions. The structure of ApoE constituted of two independent domains: the N-terminal domain (amino acids 1–191) contains the lipoprotein receptor-binding region (amino acids 136–150), and the C-terminal domain (amino acids 225–299) contains the lipid-binding region (amino acids 244–272). In ApoE4, two amino at position 112 and 158 differs the type of ApoE. The two arginines at position 112 and 158 in the N-terminal domain form a domain interaction with glutamic at position 255, which may determine the prior choice of ApoE4 for VLDL
In the 1970s, scientists found that ApoE is a component of a key modulator of lipoprotein, plasma lipoprotein, and cholesterol concentrations. Up to 75% of ApoE in plasma is synthesized by hepatic parenchymal cells (Mahley 1988); however, there are other organs and tissues producing a large amount of ApoE, most notably the brain, as well as the spleen, kidney, macrophages, and adipocytes (Ang et al. 2008; Getz and Reardon 2009; Williams et al. 1985). Physically, ApoE acts as cholesterol transporter, the key regulator to redistribute cholesterol within cells and to mobilize cholesterol between cells. These functions of ApoE transport cholesterol are essential for keeping myelin and neuronal membranes maintain both in the central and peripheral nervous systems (Leduc et al. 2010).
5.1.2 The Polymorphism of apoE Gene
The human apoE gene, 3.6 kb long, is located on the long arm of chromosome 19 and consists of four exons (Weisgraber 1994). Utermann first observed the polymorphism of apoE in 1975. Subsequent confirmation of the cDNA sequence directly tested revealed that there are three isoforms of apoE gene: ε2, ε3, and ε4. Some people only contain one major subtype, which is homozygous; some people can contain two main subtypes, namely, heterozygotes. Thus, there are six different phenotypes in the population, and all were readily detectable in human subjects: three homozygous phenotypes (ε4/4, ε3/3, and ε2/2) and three heterozygous phenotypes (ε4/3, ε3/2, and ε4/2) (Utermann et al. 1978, 1979a, b; Utermann and Beisiegel 1979).
In natural populations, apoE ɛ3 allele is the most common (77.9%), ɛ2 allele the least common (8.4%), and ɛ4 in the medium (13.7%) (Farrer et al. 1997). The gene frequencies of ApoE in Chinese population are 0.88, 0.05, and 0.06. At the same time, ApoE is also involved in the normal growth of the nervous system and repair process after injury; the nervous system has a wide range of physiological and pathological effects. Because ɛ3 appears to have the highest frequency, it is considered “wild type,” apoE 2 and apoE 4 are due to its mutation, variant receptor binding than “wild type” decreased, ApoE2 receptor-binding activity was reduced to 1% of the activity of ApoE3, and the decrease in ApoE2 receptor binding is closely related to inherited lipid disorders. The mutation of the gene apoE is involved in the pathogenesis of some of the primary cases of Alzheimer’s disease. apoE 2 has protective effects on vascular integrity; apoE 3 is moderate, while apoE 4 causes a fivefold increase in vascular inflammatory factor CypA, making blood vessels brittle, and also increases the risk of getting Alzheimer’s disease. However, people who have this genetic variant do not necessarily have Alzheimer’s disease. On the contrary, those who do not have this genetic variant are equally likely to have Alzheimer’s disease. So apart from genes, scientists suspect there must be more environmental factors that contribute to the development of Alzheimer’s disease.
5.2 ApoE and Alzheimer’s Disease
5.2.1 Alzheimer’s Disease
Alzheimer’s disease (AD) is a common neurodegenerative disease among elder people which cannot be cured. The most adverse effects are cognitive decline and memory loss. Approximately 13% of elder people over the age of 65 and 45% over the age of 85 presently are affected by AD (Assoc, A 2012). There are at least 30 million AD patients around the world, and it will reach 131 million in 2050 (ADI 2016; Hung et al. 2016). Due to an increasing elder population, AD becomes one of the greatest health issues of this century (Hickman et al. 2016) and is definitely the sixth leading cause of death in the USA (Assoc, A 2015). In 2016, the total health-care costs including long-term care and hospice services, for people aged over 65 years with dementia, are estimated to be $236 billion, and this number will be doubled in 2030 (Association 2016) .
Compared with the healthy brain, AD patients’ brain has severe shrinkage, especially in the hippocampus. Histopathology shows that extracellular senile plaques and intracellular neurofibrillary tangles are two hallmarks of AD pathology (Kanekiyo et al. 2014). Senile plaque involves amyloid-β peptide’s (Aβ) abnormal accumulation and aggregation between the neurons and later forms depositions in the gray matter of the brain, mainly in the hippocampus (which involves in new memory formation) and neocortex (Luo et al. 2017), while neurofibrillary tangles are associated with tau hyper-phosphorylation. However, due to the complex genetic, epigenetic, and environmental factors that may influence the development of AD, the mechanisms of AD have not been fully studied. Strong evidence suggest that human apoE gene is the strongest genetic risk factor for LOAD known so far. Among the three isoforms, ε2, ε3, and ε4, the risk ranking of suffering AD is ε4 > ε3 > ε2. ApoE ε4 increases AD risk about ~3 (single allele)- and 15-fold (double allele), respectively, while ApoE ε2 can decrease the possibility of AD (Kim and Tsai 2009; Koffie et al. 2012; Saunders et al. 1993).
5.2.2 Role of ApoE in Alzheimer’ Disease
Amyloid cascade hypothesis (ACH) has been proposed in 1992. The hypothesis mainly stands for the point of view that the deposition of Aβ, which is the major component of the senile plaques formed in AD patients’ brains, is the upstream initiation factor of AD pathology. Aβ deposition finally induces neurofibrillary tangles, neuronal loss, cell death, and dementia (Hardy and Higgins 1992). Currently, a new modified ACH has been proposed by Karran E (Karran and De Strooper 2016). The modified ACH suggests that tau dysfunction may run in parallel with the deposition of Aβ, but the key event in AD pathology is still Aβ deposition (Ricciarelli and Fedele 2017). However, others proposed different views: Moir suggests Aβ plaque may not be responsible for AD occurrence; on the contrary, Aβ wraps harmful pathogens to prevent them from infecting the brain, it is like the body’s immune response, rather than the killer (Kumar et al. 2016).
Abundance of evidences has suggested apoE gene is the strongest genetic risk factor for LOAD, but the role ApoE plays in AD hasn’t been fully explained. ApoE is primarily produced by the liver and macrophages in peripheral tissues, while it is produced by astrocyte or glia cells in the brain (Liu et al. 2013), both in humans and animals, and serves as a cholesterol carrier and mediates the uptake of lipoprotein particles (Hirsch-Reinshagen et al. 2009). ApoE mediates cholesterol metabolism in an isoform-dependent manner (Kanekiyo et al. 2014). It was demonstrated that ApoE4 has preference to very-low-density lipoproteins (VLDL), while ApoE3 and ApoE2 have a preference for small high-density lipoproteins (HDLs) due to their different structure sequence (Huang and Mahley 2014; Mahoney-Sanchez et al. 2016).
In human, compared to ε2 and ε3, the presence of ε4 is associated with increased risk for suffering both EOAD and LOAD, especially LOAD. Studies reveal that there is a clear relevance between apoE ε4 and the neural disorder pathology in AD (Mahley et al. 2006). Genetic studies demonstrate that, among persons who inherit double ε4 alleles, the risk of suffering from AD by 85 years of age is 50–90%, and among persons with one ε4 allele is 45% (Xu et al. 2006).
Although there is a clear correlation between apoE ε4 gene and the elevated risk of AD, the mechanism for effect of ApoE in AD is complex and multi-angled. ApoE is associated with many aspects of AD (Arbor et al. 2016), both in Aβ-dependent and Aβ-independent ways, including Aβ metabolism, Aβ plaque formation, cytoskeletal structure and mitochondrial function impairment, synaptic plasticity loss, and blood-brain barrier (BBB) integrity impairment (Fig. 5.3).

Aβ metabolism in the brain and Aβ-dependent/Aβ-independent effects of ApoE on Alzheimer’s disease. (1) Non-amyloid metabolic pathway of amyloid precursor protein (APP); (2) amyloid metabolic pathway of APP produces amyloid-β peptide (Aβ); (3) Aβ is degraded by insulin-degrading enzyme (IDE) and neprilysin (NEP). (4) The major Aβ clearance pathways include receptor (LRP/LDLR)-mediated uptake into astrocyte/microglia cell or through the blood-brain barrier (BBB). (5) Extreme Aβ accumulation and aggregation can promote Aβ oligomers and Aβ plaque formation which leads to AD. (6) Apolipoprotein E (ApoE) is mainly produced by astrocyte in the brain. (7–9) Aβ-dependent effects of ApoE on AD: (7) ApoE directly interacts with Aβ and interferes Aβ clearance. (8) ApoE4 competes with Aβ for the same receptor LRP and LDLR, which interferences the cellular uptake pathways of Aβ. (9) ApoE4 inhibits Aβ-degrading enzymes to downregulate Aβ degradation. (10–12) Aβ-independent effects of ApoE on AD: (10) ApoE4 can directly damage neuron and leads to AD; (11) C-terminal of ApoE4 enters cytosol causing mitochondrion dysfunction; (12) ApoE4 impairs blood-brain barrier (BBB) integrity
5.2.2.1 APOE4 Affects AD in Aβ-Dependent Way
Aβ production and clearance disturbance may play a central role in AD pathogenesis. Obviously, ApoE relates to Aβ metabolism in AD in isoform-dependent manner. There are evidences to indicate that levels of soluble Aβ are increased with ApoE4, providing a potential mechanism of ApoE4-induced AD risk (Tai et al. 2014). However, the pathways by which ApoE4 may increase Aβ levels are unclear. Based on the existing evidences, ApoE may affect Aβ by the pathways of forming complexes, interfering Aβ clearance, altering Aβ degradation enzyme, and facilitating Aβ plaque formation.
Some research suggest that ApoE can directly interact with Aβ. Histological analyses of AD patients’ brains show that ApoE is co-deposited with Aβ in amyloid plaques (Namba et al. 1991). Epitope mapping demonstrates that residues 144–148 in the ApoE N-terminal region can interact with residues 13–17 in Aβ, forming the ApoE/Aβ complexes (Cho et al. 2001) which interfere Aβ uptake ways. Purified ApoE4 can bind to Aβ with a higher affinity than ApoE3 and E2 (Ladu et al. 1994). Researches have shown that ApoE increases the level of Aβ oligomers in an isoform-dependent manner (E4 > E3 >E2) (Hashimoto et al. 2012; Youmans et al. 2012). Moreover, blocking the ApoE/Aβ interaction can relieve Aβ-related pathology including brain Aβ accumulation, co-accumulation of ApoE within Aβ plaques, and neurodegeneration in both APP/E2 and APP/E4 mice (Pankiewicz et al. 2014).
ApoE can also modulate Aβ clearance way as a competitor. All three isoforms of ApoE can bind to the receptors and transporters such as low-density lipoprotein (LDL) receptor-related protein (LRP) in astrocytes that supposed to bind Aβ, which form a competition of Aβ cellular uptake pathway (Verghese et al. 2013). Interestingly, compared to ApoE4, ApoE2 and ApoE3 cleared more Aβ in transgenic mice (Dodart et al. 2005; Hudry et al. 2013).
Our previous research has shown that ApoE can also regulate Aβ metabolism by affecting its degrading enzyme IDE extracellularly. ApoE4 significantly downregulates the expression of IDE, while ApoE3 could rescue these effects in ApoE knockout mice (Du et al. 2009a). Keeney’ research also demonstrated that ApoE4 mice exhibited downregulated peroxisome proliferator-activated receptor (PPARγ) levels and IDE expression (Keeney et al. 2015). In another research of our lab, we suggest that PPARγ could transcriptionally activate IDE gene expression (Du et al. 2009b). These results indicate that ApoE4 may decrease IDE expression by inhibiting PPARγ.
Furthermore, some studies suggest that ApoE isoforms on AD pathogenesis are through plaque formation. Holtzman’s researches provide evidences that APPsw mice carried two apoE (+/+) and one (+/−) presented more Aβ plaques than no copies (−/−) of normal mice apoE gene (Holtzman et al. 2000b). In addition, they further demonstrate that these effects of ApoE are isoform specific (E4>E3) (Holtzman et al. 2000a).
5.2.2.2 APOE4 Affects AD in Aβ-Independent Way
In addition, both in vivo and in vitro studies also suggest ApoE may affect AD in Aβ-independent ways in parallel with Aβ-independent ways, including synaptic plasticity, BBB integrity, cytoskeletal structure and mitochondrial function impairment, synaptic plasticity loss, and blood-brain barrier (BBB) integrity impairment.
ApoE4 causes neuronal and behavioral deficits in the absence of Aβ accumulation in transgenic mice. Transgenic mice expressing human ApoE3 or ApoE4 and lacking endogenous mouse ApoE have been established (Buttini et al. 1999; Raber et al. 1998). Among all these models, Aβ levels do not accumulate; however, ApoE4 mice show deficits in vertical exploratory behavior and impairment of spatial learning and memory, while ApoE3 mice and wild-type mice show no significant change, and these impairments of learning and memory are gender specific (female>male) (Buttini et al. 1999; Raber et al. 1998).
ApoE impairs synaptic plasticity in an isoform-dependent manner. As compared to ApoE3, ApoE4 decreases dendritic spine density in transgenic and gene-targeted mice (Jain et al. 2013). ApoE3 promotes neurite outgrowth and increases neuronal sprouting (Kim et al. 2014). However, the effect of ApoE4 on synaptic plasticity is inconsistent. A study reported that ApoE4 had prejudicial effects on neurite outgrowth (Teter et al. 2002), while another study suggested ApoE4 even had stimulating effects in the absence of Aβ (Puttfarcken et al. 1997).
Moreover, it has also been demonstrated that the C-terminal fragments of ApoE4 can enter the cytosol and cause neurotoxicity by disrupting the cytoskeleton (Huang et al. 2001). ApoE4 fragment also target the neuron mitochondrion, leading to mitochondrial dysfunction. Brodbeck’s research later demonstrate that ApoE decreases mitochondrial mobility in an isoform-specific manner (E4 fragment > E4 > E3) (Brodbeck et al. 2011; Chang et al. 2005).
On the other hand, ApoE also exhibits isoform-specific effects on BBB integrity in mouse models (Bell et al. 2012). In both human apoE gene knock-in and glial fibrillary acidic protein promoter transgenic mice, ApoE4 expression increases the susceptibility of BBB to injury in the absence of Aβ. It has been reported that pericytes express ApoE (Xu et al. 2006), which might lead to BBB damage in the context of ApoE4.
5.3 ApoE and Other Neurodegenerative Diseases
Although the linkage is not as strong as with AD, ApoE also associates with progression in other neurological or neurodegenerative diseases, including Parkinson’s disease (PD), vascular dementia (VD), multiple sclerosis (MS), traumatic brain injury (TBI), ischemic stroke (IS), etc.
5.3.1 ApoE and Parkinson’s Disease
Though PD has some clinical and neuropathological features that are similar with AD, there are still lots of inconsistent features. Compared to AD, PD progresses slowly in most people, affecting less of the population older than 65 years of age (PD 2% vs AD 13%) (Hughes et al. 1993). Until now, the association between ApoE and PD is still controversial. Hardy’s research notice a strong association between the apoE ɛ4 allele and AD but no association between the apoE ɛ4 allele and PD (Hardy et al. 1994). Also, apoE ɛ4 does not aggravate AD lesion in patient with PD (Egensperger et al. 1996). Li and Pulkes’s researches, however, demonstrate the association between ApoE and PD in CNS (Li et al. 2004; Pulkes et al. 2011). Another research demonstrate apoE ɛ2 is associated with higher risk of PD development (Huang et al. 2004). So far, the role of ApoE in PD remains a lot of inconclusive.
5.3.2 ApoE and Vascular Dementia
VD is a severe cognitive impairment caused by brain damage from impaired blood hypoperfusion in the brain and usually happens after suffering ischemic stroke, hemorrhagic stroke, and cerebrovascular diseases (Roman 2004). VD is one of the second common causes of dementia after Alzheimer’s disease, causing around 15% of cases (O’Brien and Thomas 2015). Clinically, VD presents pathological features such as the amyloid plaques, neurofibrillary tangles, and white matter lesions, same as AD (Kalaria 2003). There are many risk factors of VD, including hypertension, ischemic stroke, hemorrhagic stroke, atherosclerosis, and other metabolic disorders; in addition to the above, ApoE is also considered as an important risk factor for VD, but the conclusions are conflicting. Some studies demonstrate there is a positive association between apoE ɛ4 allele and increased risk of VD (Baum et al. 2006; Chuang et al. 2010; Yin et al. 2012); on the contrary, Kawamata’s research find no obvious association between apoE ɛ4 allele and VD in Japanese (Kawamata et al. 1994).
5.3.3 ApoE and Multiple Sclerosis
MS is the most common demyelinating disease of the central nervous system. MS usually occurs between the ages of 20 and 50 and more common in women than men. The lesions are characterized by multiple lesions, remissions, and recurrences in the optic nerve, spinal cord, and brain stem (Zephir 2018). So far, some researches demonstrate a negative association between apoE ɛ4 allele or ɛ2 allele and MS (Carmona et al. 2011; Ghaffar et al. 2010; Ramagopalan et al. 2007; Xuan et al. 2011; Zwemmer et al. 2004) or MS patients’ cognitive impairment (Portaccio et al. 2009), while some researches indicate apoE ɛ4 carriers with MS have worsening progression of cognitive deficits than noncarriers (Oliveri et al. 1999; Shi et al. 2011). In summary, the possible relationship between the apoE ɛ4 allele and cognitive dysfunction in MS patients is small and on balance suggests a link.
5.3.4 ApoE and Ischemic Stroke
Stroke is a medical condition in which poor blood flow to the brain results in cell death. There are two main types of stroke: ischemic stroke (IS), due to lack of blood flow, and hemorrhagic stroke (HS), due to bleeding. Due to the association between apoE ɛ4 allele and increased levels of LDL and cholesterol, ApoE may have an impact on IS occurrence; several meta-analyses report a significant association between IS and the apoE ɛ4 allele.(Das et al. 2016; McCarron et al. 1999; Wang et al. 2006; Xu et al. 2016). It has been demonstrated that apoE ɛ4 carrier patients have significantly greater risk of IS occurrence (Treger et al. 2003). Also, apoE ɛ4 allele is related to increasing carotid intima-media thickness, which is associated with IS (Paternoster et al. 2008). IS is a result of combination interactions between environmental and various genetic factors: mthfr, apoE, pon1, pde4d, etc. (Wei et al. 2017), and influence of each gene is not as strong as in AD but is expected to be modest. The influence of genetic factors may be obscured by the acquired risk factors in IS. However, apoE gene seems to be a strong candidate for studying the interplay between genetic and acquired risk factors (Van Giau et al. 2015).
5.4 Conclusion
ApoE is a kind of apolipoprotein closely related to the nervous system. Its genetic polymorphism is not only closely related to lipid metabolism but also closely related to various neurological or neurodegenerative diseases and cardiovascular diseases, such as AD, PD, VD, MS, and IS. This review highlighted the association between ApoE and neurodegenerative diseases. The association between ApoE (especially ApoE4) and AD is strong and has been known for decades; several theories have been proposed how ApoE plays its roles, both in Aβ-dependent and Aβ-independent pathways. On the contrary, the linkage between ApoE and other neurological or neurodegenerative diseases is not as strong as AD, the effect of ApoE expression and ApoE polymorphism is also controversial, and this may be explained by the complex of the influences of genetic factors and environment factors (acquired factors). In summary, the association between ApoE and the risk of pathogenesis is still not clear, but ApoE is a definite essential factor for diagnosis, risk assessment, prevention, and treatment of disease in humans.
References
ADI (2016) World Alzheimer report
Ang LS, Cruz RP, Hendel A, Granville DJ (2008) Apolipoprotein E, an important player in longevity and age-related diseases. Exp Gerontol 43:615–622
Arbor SC, LaFontaine M, Cumbay M (2016) Amyloid-beta Alzheimer targets – protein processing, lipid rafts, and amyloid-beta pores. Yale J Biol Med 89:5–21
Assoc, A (2012) 2012 Alzheimer’s disease facts and figures. Alzheimers Dement 8:131–168
Assoc, A (2015) Alzheimer’s Association report 2015 Alzheimer’s disease facts and figures. Alzheimers Dement 11:332–384
Association, A.s (2016) 2016 Alzheimer’s disease facts and figures. Alzheimers Dement 12:459–509
Bao Q, Pan J, Qi HF, Wang L, Qian H, Jiang FZ, Shao ZR, Xu FZ, Tao ZP, Ma Q et al (2014) Aging and age-related diseases – from endocrine therapy to target therapy. Mol Cell Endocrinol 394:115–118
Baum L, Lam LC, Kwok T, Lee J, Chiu HF, Mok VC, Wong A, Chen X, Cheung WS, Pang CP et al (2006) Apolipoprotein E epsilon4 allele is associated with vascular dementia. Dement Geriatr Cogn Disord 22:301–305
Bell RD, Winkler EA, Singh I, Sagare AP, Deane R, Wu Z, Holtzman DM, Betsholtz C, Armulik A, Sallstrom J, Berk BC, Zlokovic BV.(n.d.) Nature Volume 485, Issue 7399, 24 May 2012, Pages 512–516
Blanche H, Cabanne L, Sahbatou M, Thomas G (2001) A study of French centenarians: are ACE and APOE associated with longevity? C R Acad Sci III 324:129–135
Brodbeck J, McGuire J, Liu ZP, Meyer-Franke A, Balestra ME, Jeong DE, Pleiss M, McComas C, Hess F, Witter D et al (2011) Structure-dependent impairment of intracellular apolipoprotein E4 trafficking and its detrimental effects are rescued by small-molecule structure correctors. J Biol Chem 286:17217–17226
Bu GJ (2009) Apolipoprotein E and its receptors in Alzheimer’s disease: pathways, pathogenesis and therapy. Nat Rev Neurosci 10:333–344
Buttini M, Orth M, Bellosta S, Akeefe H, Pitas RE, Wyss-Coray T, Mucke L, Mahley RW (1999) Expression of human apolipoprotein E3 or E4 in the brains of Apoe−/− mice: isoform-specific effects on neurodegeneration. J Neurosci 19:4867–4880
Carmona O, Masuet C, Santiago O, Alia P, Moral E, Alonso-Magdalena L, Casado V, Arbizu T (2011) Multiple sclerosis and cognitive decline: is ApoE-4 a surrogate marker? Acta Neurol Scand 124:258–263
Chang SJ, Ma TR, Miranda RD, Balestra ME, Mahley RW, Huang YD (2005) Lipid- and receptor-binding regions of apolipoprotein E4 fragments act in concert to cause mitochondrial dysfunction and neurotoxicity. Proc Natl Acad Sci USA 102:18694–18699
Cho HS, Hyman BT, Greenberg SM, Rebeck GW (2001) Quantitation of apoE domains in Alzheimer disease brain suggests a role for apoE in Abeta aggregation. J Neuropathol Exp Neurol 60:342–349
Chuang YF, Hayden KM, Norton MC, Tschanz J, Breitner JCS, Welsh-Bohmer KA, Zandi PP, Investigators CC (2010) Association between APOE epsilon 4 allele and vascular dementia: the Cache County Study. Dement Geriatr Cogn 29:248–253
Das S, Kaul S, Jyothy A, Munshi A (2016) Association of APOE (E2, E3 and E4) gene variants and lipid levels in ischemic stroke, its subtypes and hemorrhagic stroke in a South Indian population. Neurosci Lett 628:136–141
Deelen J, Beekman M, Uh HW, Helmer Q, Kuningas M, Christiansen L, Kremer D, van der Breggen R, Suchiman HE, Lakenberg N et al (2011) Genome-wide association study identifies a single major locus contributing to survival into old age; the APOE locus revisited. Aging Cell 10:686–698
Dodart JC, Marr RA, Koistinaho M, Gregersen BM, Malkani S, Verma IM, Paul SM (2005) Gene delivery of human apolipoprotein E alters brain Abeta burden in a mouse model of Alzheimer’s disease. Proc Natl Acad Sci U S A 102:1211–1216
Du J, Chang JL, Guo SX, Zhang Q, Wang Z (2009a) ApoE 4 reduces the expression of A beta degrading enzyme IDE by activating the NMDA receptor in hippocampal neurons. Neurosci Lett 464:140–145
Du J, Zhang L, Liu SB, Zhang C, Huang XQ, Li J, Zhao NM, Wang Z (2009b) PPAR gamma transcriptionally regulates the expression of insulin-degrading enzyme in primary neurons. Biochem Biophys Res Commun 383:485–490
Egensperger R, Bancher C, Kosel S, Jellinger K, Mehraein P, Graeber MB (1996) The apolipoprotein E epsilon 4 allele in Parkinson’s disease with Alzheimer lesions. Biochem Biophys Res Commun 224:484–486
Farrer LA, Cupples LA, Haines JL, Hyman B, Kukull WA, Mayeux R, Myers RH, Pericak-Vance MA, Risch N, van Duijn CM (1997) Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease – a meta-analysis. Jama-J Am Med Assoc 278:1349–1356
Fortney K, Dobriban E, Garagnani P, Pirazzini C, Monti D, Mari D, Atzmon G, Barzilai N, Franceschi C, Owen AB et al (2015) Genome-wide scan informed by age-related disease identifies loci for exceptional human longevity. PLoS Genet 11:e1005728
Getz GS, Reardon CA (2009) Apoprotein E as a lipid transport and signaling protein in the blood, liver, and artery wall. J Lipid Res 50:S156–S161
Ghaffar O, Reis M, Pennell N, O’Connor P, Feinstein A (2010) APOE epsilon4 and the cognitive genetics of multiple sclerosis. Neurology 74:1611–1618
Hardy JA, Higgins GA (1992) Alzheimer’s disease: the amyloid cascade hypothesis. Science 256:184–185
Hardy J, Crook R, Prihar G, Roberts G, Raghavan R, Perry R (1994) Senile dementia of the Lewy body type has an apolipoprotein-E Epsilon-4 allele frequency intermediate between controls and Alzheimers-disease. Neurosci Lett 182:1–2
Hashimoto T, Serrano-Pozo A, Hori Y, Adams KW, Takeda S, Banerji AO, Mitani A, Joyner D, Thyssen DH, Bacskai BJ et al (2012) Apolipoprotein E, especially apolipoprotein E4, increases the oligomerization of amyloid beta peptide. J Neurosci 32:15181–15192
Hickman RA, Faustin A, Wisniewski T (2016) Alzheimer disease and its growing epidemic risk factors, biomarkers, and the urgent need for therapeutics. Neurol Clin 34:941
Hirsch-Reinshagen V, Burgess BL, Wellington CL (2009) Why lipids are important for Alzheimer disease? Mol Cell Biochem 326:121–129
Holtzman DM, Bales KR, Tenkova T, Fagan AM, Parsadanian M, Sartorius LJ, Mackey B, Olney J, McKeel D, Wozniak D et al (2000a) Apolipoprotein E isoform-dependent amyloid deposition and neuritic degeneration in a mouse model of Alzheimer’s disease. Proc Natl Acad Sci U S A 97:2892–2897
Holtzman DM, Fagan AM, Mackey B, Tenkova T, Sartorius L, Paul SM, Bales K, Ashe KH, Irizarry MC, Hyman BT (2000b) Apolipoprotein E facilitates neuritic and cerebrovascular plaque formation in an Alzheimer’s disease model. Ann Neurol 47:739–747
Huang Y, Mahley RW (2014) Apolipoprotein E: structure and function in lipid metabolism, neurobiology, and Alzheimer’s diseases. Neurobiol Dis 72(Pt A):3–12
Huang Y, Liu XQ, Wyss-Coray T, Brecht WJ, Sanan DA, Mahley RW (2001) Apolipoprotein E fragments present in Alzheimer’s disease brains induce neurofibrillary tangle-like intracellular inclusions in neurons. Proc Natl Acad Sci U S A 98:8838–8843
Huang XM, Chen PC, Poole C (2004) APOE epsilon-2 allele associated with higher prevalence of sporadic Parkinson’s disease. Neurology 62:A89–A90
Hudry E, Dashkoff J, Roe AD, Takeda S, Koffie RM, Hashimoto T, Scheel M, Spires-Jones T, Arbel-Ornath M, Betensky R et al (2013) Gene transfer of human Apoe isoforms results in differential modulation of amyloid deposition and neurotoxicity in mouse brain. Sci Transl Med 5:212ra161
Hughes AJ, Daniel SE, Lees AJ (1993) The clinical features of Parkinson’s disease in 100 histologically proven cases. Adv Neurol 60:595–599
Hung ASM, Liang Y, Chow TCH, Tang HC, Wu SLY, Wai MSM, Yew DT (2016) Mutated tau, amyloid and neuroinflammation in Alzheimer disease-a brief review. Prog Histochem Cytochem 51:1–8
Jain S, Yoon SY, Leung L, Knoferle J, Huang Y (2013) Cellular source-specific effects of apolipoprotein (apo) E4 on dendrite arborization and dendritic spine development. PLoS One 8:e59478
Johnson SC, Dong X, Vijg J, Suh Y (2015) Genetic evidence for common pathways in human age-related diseases. Aging Cell 14:809–817
Kalaria RN (2003) Comparison between Alzheimer’s disease and vascular dementia: implications for treatment. Neurol Res 25:661–664
Kanekiyo T, Xu HX, Bu GJ (2014) ApoE and A beta in Alzheimer’s disease: accidental encounters or partners? Neuron 81:740–754
Karran E, De Strooper B (2016) The amyloid cascade hypothesis: are we poised for success or failure? J Neurochem 139(Suppl 2):237–252
Kawamata J, Tanaka S, Shimohama S, Ueda K, Kimura J (1994) Apolipoprotein E polymorphism in Japanese patients with Alzheimer’s disease or vascular dementia. J Neurol Neurosurg Psychiatry 57:1414–1416
Keeney JT, Ibrahimi S, Zhao L (2015) Human ApoE isoforms differentially modulate glucose and amyloid metabolic pathways in female brain: evidence of the mechanism of neuroprotection by ApoE2 and implications for Alzheimer’s disease prevention and early intervention. J Alzheimers Dis 48:411–424
Kim D, Tsai LH (2009) Bridging physiology and pathology in AD. Cell 137:997–1000
Kim J, Yoon H, Basak J, Kim J (2014) Apolipoprotein E in synaptic plasticity and Alzheimer’s disease: potential cellular and molecular mechanisms. Mol Cells 37:767–776
Koffie RM, Hashimoto T, Tai HC, Kay KR, Serrano-Pozo A, Joyner D, Hou S, Kopeikina KJ, Frosch MP, Lee VM et al (2012) Apolipoprotein E4 effects in Alzheimer’s disease are mediated by synaptotoxic oligomeric amyloid-beta. Brain 135:2155–2168
Kumar DK, Choi SH, Washicosky KJ, Eimer WA, Tucker S, Ghofrani J, Lefkowitz A, McColl G, Goldstein LE, Tanzi RE et al (2016) Amyloid-beta peptide protects against microbial infection in mouse and worm models of Alzheimer’s disease. Sci Transl Med 8:340ra372
Ladu MJ, Falduto MT, Manelli AM, Reardon CA, Getz GS, Frail DE (1994) Isoform-specific binding of apolipoprotein-E to Beta-amyloid. J Biol Chem 269:23403–23406
Leduc V, Jasmin-Belanger S, Poirier J (2010) APOE and cholesterol homeostasis in Alzheimer’s disease. Trends Mol Med 16:469–477
Lee Y, Kockx M, Raftery MJ, Jessup W, Griffith R, Kritharides L (2010) Glycosylation and sialylation of macrophage-derived human apolipoprotein E analyzed by SDS-PAGE and mass spectrometry. Mol Cell Proteomics 9:1968–1981
Li YJ, Hauser MA, Scott WK, Martin ER, Booze MW, Qin XJ, Walter JW, Nance MA, Hubble JP, Koller WC et al (2004) Apolipoprotein E controls the risk and age at onset of Parkinson disease. Neurology 62:2005–2009
Liu CC, Liu CC, Kanekiyo T, Xu H, Bu G (2013) Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol 9:106–118
Luo JH, Warmlander SKTS, Graslund A, Abrahams JP (2017) Cross-interactions between the Alzheimer disease amyloid-beta peptide and other amyloid proteins. A further aspect of the amyloid cascade hypothesis (vol 291, pg 16488, 2016). J Biol Chem 292:2046–2046
Mahley RW (1988) Apolipoprotein-E – cholesterol transport protein with expanding role in cell biology. Science 240:622–630
Mahley RW, Weisgraber KH, Huang YD (2006) Apolipoprotein E4: a causative factor and therapeutic target in neuropathology including Alzheimer’s disease. Proc Natl Acad Sci USA 103:5644–5651
Mahoney-Sanchez L, Belaidi AA, Bush AI, Ayton S (2016) The complex role of apolipoprotein E in Alzheimer’s disease: an overview and update. J Mol Neurosci 60:325–335
McCarron MO, Delong D, Alberts MJ (1999) APOE genotype as a risk factor for ischemic cerebrovascular disease – a meta-analysis. Neurology 53:1308–1311
Namba Y, Tomonaga M, Kawasaki H, Otomo E, Ikeda K (1991) Apolipoprotein-E immunoreactivity in cerebral amyloid deposits and neurofibrillary tangles in Alzheimers-disease and kuru plaque amyloid in Creutzfeldt-Jakob disease. Brain Res 541:163–166
O’Brien JT, Thomas A (2015) Vascular dementia. Lancet 386:1698–1706
Oliveri RL, Cittadella R, Sibilia G, Manna I, Valentino P, Gambardella A, Aguglia U, Zappia M, Romeo N, Andreoli V et al (1999) APOE and risk of cognitive impairment in multiple sclerosis. Acta Neurol Scand 100:290–295
Pankiewicz JE, Guridi M, Kim J, Asuni AA, Sanchez S, Sullivan PM, Holtzman DM, Sadowski MJ (2014) Blocking the apoE/A beta interaction ameliorates A beta-related pathology in APOE epsilon 2 and epsilon 4 targeted replacement Alzheimer model mice. Acta Neuropathol Commun 2:75
Paternoster L, Gonzalez NAM, Lewis S, Sudlow C (2008) Association between apolipoprotein E genotype and carotid intima-media thickness may suggest a specific effect on large artery atherothrombotic stroke. Stroke 39:48–54
Portaccio E, Goretti B, Zipoli V, Nacmias B, Stromillo ML, Bartolozzi ML, Siracusa G, Guidi L, Federico A, Sorbi S et al (2009) APOE-epsilon4 is not associated with cognitive impairment in relapsing-remitting multiple sclerosis. Mult Scler 15:1489–1494
Puglielli L, Tanzi RE, Kovacs DM (2003) Alzheimer’s disease: the cholesterol connection. Nat Neurosci 6:345–351
Pulkes T, Papsing C, Mahasirimongkol S, Busabaratana M, Kulkantrakorn K, Tiamkao S (2011) Association between apolipoprotein E genotypes and Parkinson’s disease. J Clin Neurosci 18:1333–1335
Puttfarcken PS, Manelli AM, Falduto MT, Getz GS, LaDu MJ (1997) Effect of apolipoprotein E on neurite outgrowth and beta-amyloid-induced toxicity in developing rat primary hippocampal cultures. J Neurochem 68:760–769
Raber J, Wong D, Buttini M, Orth M, Bellosta S, Pitas RE, Mahley RW, Mucke L (1998) Isoform-specific effects of human apolipoprotein E on brain function revealed in ApoE knockout mice: increased susceptibility of females. Proc Natl Acad Sci U S A 95:10914–10919
Rall SC, Weisgraber KH, Mahley RW (1982) Human apolipoprotein-E – the complete amino-acid-sequence. J Biol Chem 257:4171–4178
Ramagopalan SV, Deluca GC, Morrison KM, Herrera BM, Dyment DA, Orton S, Bihoreau MT, Degenhardt A, Pugliatti M, Sadovnick AD et al (2007) No effect of APOE and PVRL2 on the clinical outcome of multiple sclerosis. J Neuroimmunol 186:156–160
Rasmussen KL (2016) Plasma levels of apolipoprotein E, APOE genotype and risk of dementia and ischemic heart disease: a review. Atherosclerosis 255:145–155
Ricciarelli R, Fedele E (2017) The amyloid cascade hypothesis in Alzheimer’s disease: It’s time to change our mind. Curr Neuropharmacol 15:926–935
Roman GC (2004) Vascular dementia. Advances in nosology, diagnosis, treatment and prevention. Panminerva Med 46:207–215
Saunders AM, Strittmatter WJ, Schmechel D, George-Hyslop PH, Pericak-Vance MA, Joo SH, Rosi BL, Gusella JF, Crapper-MacLachlan DR, Alberts MJ et al (1993) Association of apolipoprotein E allele epsilon 4 with late-onset familial and sporadic Alzheimer’s disease. Neurology 43:1467–1472
Schachter F, Faure-Delanef L, Guenot F, Rouger H, Froguel P, Lesueur-Ginot L, Cohen D (1994) Genetic associations with human longevity at the APOE and ACE loci. Nat Genet 6:29–32
Shi J, Tu JL, Gale SD, Baxter L, Vollmer TL, Campagnolo DI, Tyry TM, Zhuang Y, Kuniyoshi SM (2011) APOE epsilon4 is associated with exacerbation of cognitive decline in patients with multiple sclerosis. Cogn Behav Neurol 24:128–133
Shore B, Shore V (1974) An apolipoprotein preferentially enriched in cholesteryl ester-rich very low density lipoproteins. Biochem Biophys Res Commun 58:1–7
Tai LM, Mehra S, Shete V, Estus S, Rebeck GW, Bu GJ, LaDu MJ (2014) Soluble apoE/A beta complex: mechanism and therapeutic target for APOE4-induced AD risk. Mol Neurodegener 9:2
Teter B, Xu PT, Gilbert JR, Roses AD, Galasko D, Cole GM (2002) Defective neuronal sprouting by human apolipoprotein E4 is a gain-of-negative function. J Neurosci Res 68:331–336
Treger I, Froom P, Ring H, Friedman G (2003) Association between apolipoprotein E4 and rehabilitation outcome in hospitalized ischemic stroke patients. Arch Phys Med Rehabil 84:973–976
Tudorache IF, Trusca VG, Gafencu AV (2017) Apolipoprotein E – a multifunctional protein with implications in various pathologies as a result of its structural features. Comput Struct Biotechnol J 15:359–365
Utermann G, Beisiegel U (1979) Charge-shift electrophoresis of apolipoproteins from normal humans and patients with Tangier disease. FEBS Lett 97:245–248
Utermann G, Albrecht G, Steinmetz A (1978) Polymorphism of apolipoprotein E. I. Methodological aspects and diagnosis of hyperlipoproteinemia type III without ultracentrifugation. Clin Genet 14:351–358
Utermann G, Pruin N, Steinmetz A (1979a) Polymorphism of apolipoprotein E. III. Effect of a single polymorphic gene locus on plasma lipid levels in man. Clin Genet 15:63–72
Utermann G, Vogelberg KH, Steinmetz A, Schoenborn W, Pruin N, Jaeschke M, Hees M, Canzler H (1979b) Polymorphism of apolipoprotein E. II. Genetics of hyperlipoproteinemia type III. Clin Genet 15:37–62
Van Giau V, Bagyinszky E, An SSA, Kim S (2015) Role of apolipoprotein E in neurodegenerative diseases. Neuropsychiatr Dis Treat 11:1723–1737
Verghese PB, Castellano JM, Garai K, Wang YN, Jiang H, Shah A, Bu GJ, Frieden C, Holtzman DM (2013) ApoE influences amyloid-beta (A beta) clearance despite minimal apoE/A beta association in physiological conditions. Proc Natl Acad Sci U S A 110:E1807–E1816
Wang JM, Irwin RW, Brinton RD (2006) Activation of estrogen receptor alpha increases and estrogen receptor beta decreases apolipoprotein E expression in hippocampus in vitro and in vivo. Proc Natl Acad Sci U S A 103:16983–16988
Wei LK, Au A, Menon S, Griffiths LR, Kooi CW, Irene L, Zhao J, Lee C, Alekseevna AM, Hassan MRA et al (2017) Polymorphisms of MTHFR, eNOS, ACE, AGT, ApoE, PON1, PDE4D, and ischemic stroke: meta-analysis. J Stroke Cerebrovasc Dis 26:2482–2493
Weisgraber KH (1994) Apolipoprotein E: structure-function relationships. Adv Protein Chem 45:249–302
Williams DL, Dawson PA, Newman TC, Rudel LL (1985) Apolipoprotein E synthesis in peripheral tissues of nonhuman primates. J Biol Chem 260:2444–2451
Xu Q, Bernardo A, Walker D, Kanegawa T, Mahley RW, Huang Y (2006) Profile and regulation of apolipoprotein E (ApoE) expression in the CNS in mice with targeting of green fluorescent protein gene to the ApoE locus. J Neurosci 26:4985–4994
Xu M, Zhao J, Zhang Y, Ma X, Dai Q, Zhi H, Wang B, Wang L (2016) Apolipoprotein E gene variants and risk of coronary heart disease: a meta-analysis. Biomed Res Int 2016:3912175
Xuan C, Zhang BB, Li M, Deng KF, Yang T, Zhang XE (2011) No association between APOE epsilon 4 allele and multiple sclerosis susceptibility: a meta-analysis from 5472 cases and 4727 controls. J Neurol Sci 308:110–116
Yin YW, Li JC, Wang JZ, Li BH, Pi Y, Yang QW, Fang CQ, Gao CY, Zhang LL (2012) Association between apolipoprotein E gene polymorphism and the risk of vascular dementia: a meta-analysis. Neurosci Lett 514:6–11
Youmans KL, Tai LM, Nwabuisi-Heath E, Jungbauer L, Kanekiyo T, Gan M, Kim J, Eimer WA, Estus S, Rebeck GW et al (2012) APOE4-specific changes in A beta accumulation in a new transgenic mouse model of Alzheimer disease. J Biol Chem 287:41774–41786
Zephir H (2018) Progress in understanding the pathophysiology of multiple sclerosis. Rev Neurol (Paris)
Zhang JG, Ma YX, Wang CF, Lu PF, Zhen SB, Gu NF, Feng GY, He L (1998) Apolipoprotein E and longevity among Han Chinese population. Mech Ageing Dev 104:159–167
Zwemmer JN, van Veen T, van Winsen L, van Kamp GJ, Barkhof F, Polman CH, Uitdehaag BM (2004) No major association of ApoE genotype with disease characteristics and MRI findings in multiple sclerosis. Mult Scler 10:272–277
Acknowledgements
This work was financially supported by grants from the National Key R&D Program of China (2018YFD0400204), the Key International S&T Cooperation Program of China (2016YFE113700), the European Union’s Horizon 2020 Research and Innovation Program (633589) and the National Natural Science Foundation of China (81471396).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter

Cite this chapter
Yin, Y., Wang, Z. (2018). ApoE and Neurodegenerative Diseases in Aging. In: Wang, Z. (eds) Aging and Aging-Related Diseases. Advances in Experimental Medicine and Biology, vol 1086. Springer, Singapore. https://doi.org/10.1007/978-981-13-1117-8_5
Download citation
DOI: https://doi.org/10.1007/978-981-13-1117-8_5
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-13-1116-1
Online ISBN: 978-981-13-1117-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)