
Abstract
Anhedonia is a cardinal symptom of major depressive disorder yet has not received significant attention in the research domain. A major contributor to this disproportionality is the limited understanding of anhedonia. Traditionally conceptualized as a “loss of pleasure”, it is clear that anhedonia includes additional facets including interest, motivation and reward learning. With the construct of anhedonia expanded, the development of new assessment tools, including self-report scales and behavioural tasks, has greatly improved our understanding of the underlying neurobiology. Deficits in nucleus accumbens activity have historically been tied to anhedonia due to its attribution as a “pleasure centre” in the brain. However, it is now known that many other brain regions are involved in the processing of reward. Furthermore, many first-line antidepressant options focus primarily on potentiating serotonin levels, despite dopamine playing an essential role in anhedonia. A greater understanding of anhedonia may allow for more personalized treatment strategies and heavily reduce the significant burden associated with depression. This chapter will review the neurobiology, measurement and treatment of this core symptom of MDD.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Major depressive disorder (MDD) currently remains one of the leading causes of global disability and has significant personal, societal and economic burden (Lam et al. 2016; World Health Organization 2017). MDD can be defined by a myriad of symptoms; however, at least one of two core symptoms must be present. The first of these core symptoms, “a low mood or a feeling of sadness” is a defining symptom of MDD for many. The second of these symptoms is the presence of anhedonia , historically characterized as a “loss of pleasure”. More recently, anhedonia has received increased recognition due its potential contribution to the prediction of MDD diagnosis , treatment response and remission (McMakin et al. 2012; Rawal et al. 2013; Uher et al. 2012). This chapter will provide an update on the current literature of anhedonia in the context of MDD. Specifically, this chapter will highlight the neurobiology , measurement and treatment of this core symptom of MDD.
Traditionally, conceptualizations of anhedonia have focused on the consummatory aspect of pleasure; however, this simplified definition leads to difficulties in the precise measurement and study of anhedonia (Rizvi et al. 2016). Increasing neuroscientific evidence suggests anhedonia is a more multi-faceted construct that involves interest, anticipation , motivation , effort , expectation and consummatory pleasure (Rizvi et al. 2016; Treadway and Zald 2011). In line with this, there has been an emphasis towards refining the construct of anhedonia and to integrate the underlying neurocircuitry involved in the processing of rewarding stimuli. Ultimately, any deficit in the neural processing of reward could lead to the clinical symptom of anhedonia .
2 Reward Processing Models
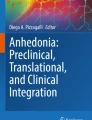
Reward processing models describe the facets of reward-seeking behaviour and their interactions. One conceptualization of reward processing is the Positive Valence System (PVS) from the Research Domain Criteria (RDoC) , a National Institute of Mental Health framework for biomarker research in mental disorders (Insel et al. 2010). The goal of RDoC is to utilize a dimensional approach across “units of analysis” (genes, brain circuits, self-reports) to evaluate causes of mental illness rather than a single predictor in isolation (Hess et al. 2016; Vengeliene et al. 2017). The PVS is not a model of reward processing, per se, but a suggested starting point for the constructs pertinent to a reward processing model which include the ability to make a reward-stimulus association, motivation , effort , expectation and consummatory pleasure. A model based on Kring and Barch (2014) has been put forth to depict the associations among these constructs (Fig. 7.1) (Rizvi et al. 2016). It is important to note that, while reward processing is depicted as a linear process, the facets may act in parallel or vary according to the situation.

Model of reward processing (Modified from Kring and Barch 2014)
Based on the Fig. 7.1 model, the reward process is described as initially building a stimulus-reward association, which then leads to interest/desire, anticipation , motivation , effort , hedonic response and feedback integration . After a reward-stimulus association has been established, an interest in the rewarding stimulus can then develop. Importantly, interest in reward is important to be able to anticipate it or to develop a “wanting” for a reward (Rizvi et al. 2016). The brain also needs to calculate the energy required to obtain the reward. Motivation describes the initial energy expenditure to obtain a reward, and effort describes the sustained energy expenditure. In other words, motivation is required to start the process of reward obtainment, and effort is required to continue this process.
Outcome following reward can be negative, positive (pleasurable) or neutral. Consummatory pleasure describes the pleasure experienced by an individual as they directly interact with a stimulus. Based on the outcomes from previous stimulus-reward associations, individuals develop expectations of reward. These expectations may relate to whether a reward will be present, the likelihood of attainment and magnitude of experienced pleasure or the effort required to obtain it. Reward expectations may influence other facets of reward such as the level of anticipation experienced or motivation to attain a reward (Rizvi et al. 2016). In particular, expectation can also affect the original stimulus-reward association through feedback integration , which is the ability to utilize new information to update existing knowledge of a potential reward. This reward learning ability is crucial to maintain accurate expectations and associations of the stimuli for future encounters. For example, there may be only certain contexts where a stimulus is rewarding or a stimulus may no longer be rewarding at all. In addition, the value one places on a stimulus can vary considerably by several factors including the time to attainment and the magnitude of the reward. MDD patients demonstrate deficits across these facets (reviewed in Rizvi et al. 2016; Treadway and Zald 2011; Tremblay et al. 2005), although the specific factors and conditions that contribute to these deficits need further exploration. Understanding the neurobiology associated with the reward facets can help to elucidate this knowledge gap.
3 The Neurobiology of Anhedonia
Understanding the underlying neurobiological underpinnings of MDD is essential to identifying subtypes , biomarkers and targeted treatments. Deficits in reward processing have been found to correlate with the clinical symptom of anhedonia (reviewed in Rizvi et al. 2016) and the above described reward facets may have shared and distinct neurobiological mechanisms. In support of this idea, Whitton et al. (2015) reported that separate neurobiological pathways may partially govern the activity of each reward facet. These pathways are superimposed over brain regions that are primarily in the frontal lobe, although other regions are also important.
The nucleus accumbens has long been acknowledged as the “pleasure centre” of the brain and has historically been tied to anhedonia (Wong et al. 1991). However, we now have a deeper understanding of the role of other brain regions in reward processing , which include the prefrontal cortex (orbitofrontal cortex , ventromedial prefrontal cortex , anterior cingulate cortex), amygdala, dorsal and ventral striatum and the insula (reviewed in Der-Avakian and Markou 2012; Treadway 2015). The prefrontal cortex , in particular, is involved in higher cognitive processing of reward, including reward valuation , decision making, context integration and cost-benefit analysis (Elliott et al. 2000; Grabenhorst and Rolls 2011). The orbitofrontal cortex, dorsolateral prefrontal cortex and ventromedial prefrontal cortex are particularly involved in these processes (reviewed in Treadway 2015). In addition, evidence suggests that once a stimulus has been identified as pleasurable, the anterior cingulate cortex (ACC) is a region involved in cost-benefit analysis and effort-related functions required to obtain reward (Salamone et al. 2009; Treadway and Zald 2011; Der-Avakian and Markou 2012). Using this information, the ventromedial PFC (vmPFC) may be responsible for executing the decision to carry out the reward-directed behaviour (Grabenhorst and Rolls 2011). Furthermore, the vmPFC, ACC, orbitofrontal cortex and striatum may also be involved in reward processing by monitoring the rewarding properties of a stimulus (Elliott et al. 2000; Seo and Lee 2007).
Neurotransmitter imbalances in reward processing have historically focused on the role of dopamine , due to its high level of expression in the nucleus accumbens (Salamone et al. 2003). The ventral tegmental area (VTA) is a group of dopaminergic neurons which supplies dopamine to other areas in the mesocorticolimbic pathway including the nucleus accumbens and ventral striatum. Reduced dopamine activity can result in impaired reward function (Malhi and Berk 2007; Salamone et al. 2003). Exposure to pleasant stimuli increases dopamine activity in the ventral striatum; however, this dopamine activity may be reduced in MDD patients (Dunlop and Nemeroff 2007). Interestingly, this reduced dopamine activity in the ventral striatum is correlated with anhedonia severity, but not necessarily depressive symptom severity (Treadway 2015). Furthermore, anhedonia was found to correlate with reduced ventral striatal grey matter, which highlights its role in reward function (Sternat and Katzman 2016). However, preclinical findings have helped to elucidate the role of dopamine as being more linked to anticipation and motivation rather than consummatory pleasure (Salamone et al. 2003; Schultz 1998). For example, animals with reduced levels of dopamine may still experience pleasure, but prefer low cost-low reward options rather than high cost-high rewards. Treadway (2015) also reported that dopamine activity in the insula and ventral striatum had different effects on effort-based decision making. Increased dopamine activity in the ventral striatum was correlated with increased effort in a dose-dependent manner; however, the opposite trend was observed in the insula .
While substantial evidence has supported dopamine’s role in anticipation , expectation , motivation and effort of reward processing , the role of other neurotransmitter systems is less clear. However, recent studies indicate that dopamine does not act in isolation and that serotonin, gamma-aminobutyric acid (GABA) , glutamate and opioids may play an important role in reward (McCabe et al. 2010; Wassum et al. 2009; Wong et al. 1991). Reduced serotonin activity has been implicated in the preference for immediate smaller reward than delayed greater reward in MDD. Some studies have suggested this may be due to increased impulsivity and desire for short-term gratification (Der-Avakian and Markou 2012).
GABA is one of the most abundant neurotransmitters in the brain and has a variety of functions. In the context of reward, GABA has demonstrated modulation of dopamine activity and indirect effects on serotonin and noradrenergic activity (Wong et al. 1991). Importantly, some neuroimaging studies have identified lowered GABA concentrations in the anterior ACC and occipital cortex of depressed patients (Gabbay et al. 2012; Kugaya et al. 2003; Sanacora et al. 1999). Interestingly, when depressed patients were grouped according to the presence of anhedonia , only those with anhedonia had reduced GABA levels (Gabbay et al. 2012).
Opioids have primarily been studied in the context of pain , although there has been an increased interest in opioid receptors in MDD. The μ-opioid receptors found in the ventral tegmental area are implicated in the disinhibition of dopamine in the nucleus accumbens (Johnson and North 1992). Further, μ-opioid receptors in the amygdala may mediate the evaluation of a stimulus’ incentive properties (Wassum et al. 2009). MDD patients with reduced opioid activity were prone to lower social motivation after rejection and lower pleasure during positive interactions (Hsu et al. 2015). This motivation was positively correlated with opioid release in the nucleus accumbens in healthy controls. Taken together, these findings suggest that opioids may mediate motivation and pleasure responses; however, further studies are needed to confirm its role in reward processing .
While anhedonia is a core symptom of MDD, it is important to recognize that it also plays a significant role in schizophrenia and bipolar disorder (Zhang et al. 2016). Several studies have attempted to elucidate the underlying neurobiology of anhedonia in each of these patient groups (Sharma et al. 2017; Whitton et al. 2015; Zhang et al. 2016). However, a transdiagnostic neurobiological profile of anhedonia has yet to be completely elucidated. In order to identify a common functional connectivity pattern associated with anhedonia across disorders, Sharma et al. (2017) assessed a sample of MDD, schizophrenia and bipolar disorder patients. The authors performed a whole-brain resting state analysis and examined its relationship with the reward responsivity measure on the behavioural activation scale (BAS). Reduced reward responsivity was associated with a specific pattern of dysconnectivity surrounding the nucleus accumbens, which was common to MDD, schizophrenia and bipolar disorder , and characterized by hypoconnectivity with the default mode network (DMN). The DMN is primarily active during internally directed forms of cognition , including memory, prospection and facets of reward processing (Sharma et al. 2017). Some studies have noted that increased connectivity in the DMN was related to anhedonia (Hamilton et al. 2011). The specific regions in the DMN with diminished connections to the nucleus accumbens included the anterior and dorsal prefrontal cortex and the posterior cingulate cortex, which are heavily involved in reward processing (Sharma et al. 2017). Therefore, it is reasonable to expect deficits in reward processing and anhedonia when hypoconnectivity between the DMN and nucleus accumbens is present.
In contrast to the hypoconnectivity with the DMN, the nucleus accumbens was found to demonstrate hyperconnectivity with the cingulo-opercular network, in particular with the insular cortex (Sharma et al. 2017). While the role of the insula in reward is unclear, some evidence has suggested that it is involved with the effort to acquire rewards (Prevost et al. 2010; Treadway 2015). Interestingly, imaging studies have suggested that decreased insula activation, as a result of decreased dopamine release, may be associated with the selection of high effort reward options (Prevost et al. 2010; Treadway 2015). In summary, several key brain regions and connections have been identified in reward processing , particularly within the prefrontal cortex . It is possible that a neural dysfunction in any aspect of reward processing could lead to the clinical symptom of anhedonia .
4 Assessment of Anhedonia
Currently, measurement of anhedonia in clinical populations is primarily through self-report scales and behavioural tasks. While both tools allow for the assessment of anhedonia, each provides a unique but equally important perspective on this core symptom. In line with this, Treadway and Zald (2011) strongly assert that both measures should be used in tandem to obtain a more complete understanding of anhedonia. In this section, current scales and behavioural tasks will be described, along with their benefits and limitations.
4.1 Self-Report Scales
MDD patients often display reduced interest in rewarding stimuli (Uher et al. 2008, 2012); therefore, self-report scales are particularly useful since they are able to directly assess anhedonic symptoms (Kringelbach et al. 2012; Rizvi et al. 2016). The measurement of the explicit components of anhedonia is particularly important due to the subjective nature of reward behaviour. Furthermore, specific activities that are perceived as rewarding and the motivation to obtain rewards vary between each patient. Therefore, self-report scales should ideally be generalizable across cultures and individuals. For the purposes of this chapter, current self-report scales of anhedonia will be grouped into “first-generation” and “second-generation” questionnaires to distinguish older versus more contemporary scales that have been developed in the last decade (Rizvi et al. 2016).
4.1.1 First-Generation Scales
The first-generation scales mostly measure consummatory pleasure, but some include motivational and effort components. The Snaith-Hamilton Pleasure Scale (SHAPS) is a 14-item scale designed to assess hedonic capacity and is the current gold standard of anhedonia measurement in MDD research (Snaith et al. 1995). The SHAPS presents participants with several examples of pleasurable situations that span the domains of hobbies, social life, sensory experiences and food/drink. The participants are instructed to select the degree to which they would enjoy situations over the past few days. As a measure of state anhedonia, the SHAPS has demonstrated its ability to detect acute changes in anhedonia, including treatment-related improvements. The scale has demonstrated good divergent and convergent validity in MDD populations. Furthermore, it has been shown to positively correlate with closely related measures such as quality of life and function. However, the SHAPS is a measure of consummatory pleasure and does not probe the other facets of reward processing life effort . In addition, while the items are generalizable across samples (“I would enjoy my favourite meal”), they may not be specific enough to elicit a strong hedonic reaction, thereby limiting the scale’s sensitivity. While the SHAPS continues to demonstrate its strength in the assessment of consummatory pleasure, its use in tandem with other measures of anhedonia should be considered.
A similar measure of anhedonia is the Fawcett-Clark Pleasure Capacity Scale (FCPCS) , which includes 36 items (Fawcett et al. 1983). Like the SHAPS, the FCPCS solely assesses consummatory pleasure on a scale between extreme displeasure to extreme pleasure. The FCPCS assesses pleasure across several domains including social activities, sensory experiences and the sense of mastery of difficult tasks. Like the SHAPS, the FCPCS has demonstrated good convergent and divergent reliability and as a measure of state anhedonia is capable of measuring acute changes in anhedonia due to treatment (Clark et al. 1984; Leventhal et al. 2006). However, the FCPCS suffers from a lack of generalizability due to several items possessing high cultural bias. Despite this, the FCPCS has been validated in MDD populations, and the items possess high internal consistency reliability (Leventhal et al. 2006).
Finally, the last two scales, the Revised Chapman Physical Anhedonia Scale (CPAS) and the Chapman Social Anhedonia Scale (CSAS) , are designed to measure various facets of reward including motivation , effort and consummatory pleasure in the context of physical anhedonia and social anhedonia, respectively (Chapman et al. 1976). Several criticisms of the CPAS and CSAS as measures of anhedonia in MDD have arisen due to its design. Both scales were developed for use in schizophrenia and thus have several items that are not applicable to MDD populations. Further, some items are not related to anhedonia, such as “I have often felt uncomfortable when my friends touch me”. With the large number of items for each scale, 61 on the CPAS and 40 on the CSAS , there is limited use in clinical settings. Furthermore, the construct and discriminant validity of the scales have been questioned, and some have asserted that the items are outdated (Leventhal et al. 2006). Both scales use a binary true or false answer format which hinders a more sensitive assessment of anhedonia. In contrast to the SHAPS and FCPCS , the CPAS and CSAS are measures of trait anhedonia as opposed to state anhedonia. Despite this, both measures can detect changes in anhedonia (Leventhal et al. 2006).
4.1.2 Second-Generation Scales
With the increased focus on expanding the construct of anhedonia beyond consummatory pleasure, there has been recent development of anhedonia scales to reflect these changes and to address the limitations of the “first-generation” scales. These new scales are designed to measure various facets of reward function in order to capture a more complete understanding of anhedonia (reviewed in Rizvi et al. 2016).
The Temporal Experience of Pleasure Scale (TEPS) was developed by Gard et al. (2006). Importantly, the TEPS was developed with two subscales that measure anticipatory and consummatory pleasure separately. In particular, the anticipatory items encompass reward responsiveness and imagery, while the consummatory items focus on appreciation of positive stimuli. The items are measured on a 6-point Likert scale which range from “very false for me” to “very true for me”. Selected items focus on physical anhedonia as the authors believed it would provide results that are more homogeneous and interpretable. Despite attempts at designing the TEPS to be more generalizable, some items are not applicable to all populations, such as “the sound of crackling wood in the fireplace is very relaxing”. While the convergent and discriminatory validity have demonstrated that the subscales are distinct, the anticipatory subscale had low internal consistency reliability. Furthermore, the TEPS has only been validated in bipolar, schizophrenia and opioid-dependent groups with limited studies in MDD populations (Gard et al. 2007; Garfield et al. 2016; Tso et al. 2014). Taken together, the TEPS may require additional validation studies to confirm the reliability of its psychometric properties and its use in MDD.
The Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS) is a 17-item scale designed to measure social anhedonia in schizophrenia and address the limitations of the CSAS (Gooding and Pflum 2014). The ACIPS uses a 6-point Likert scale as opposed to a binary outcome. The ACIPS also includes subscales for the anticipatory and consummatory facets of reward; however, factor analysis did not reveal distinct subscales. Nevertheless, when both the CSAS and ACIPS were assessed against the TEPS, the ACIPS demonstrated better correlation with the TEPS subscales than the CSAS . Finally, despite being developed as a substitute to the CSAS in schizophrenia, the ACIPS has not been validated in this population. On a similar note, the ACIPS has not been validated in MDD. Further validation studies are required to assess its utility in several psychiatric populations and to determine whether their measures of anticipation and consummatory pleasure are distinct constructs.
Lastly, the Dimensional Anhedonia Rating Scale (DARS) is the most recently developed scale by Rizvi et al. (2015). The DARS consists of 17-items on a 5-point Likert scale and was designed to specifically assess anhedonia in MDD patients. In order to increase the generalizability of the scale, participants are asked to fill in personal activities or experiences they perceive as enjoyable across the domains of hobbies, social activities, food/drink and sensory experiences. With the highly subjective nature of rewarding experiences, this feature may allow for a more sensitive measurement of anhedonia. While increasing generalizability, the DARS is designed to maintain specificity by having a specific set of items for each domain assessed. Within each of these domains, items to probe interest, motivation , effort and consummatory pleasure are measured based on how the respondent feels “now”. This measurement of state anhedonia has the benefit of increased sensitivity during assessment of treatment response. In contrast to the other “second-generation measures”, the reliability and validity of the DARS has been tested in a MDD population and demonstrated good convergent validity with the SHAPS. The DARS may also be useful in predicting subtypes as results from the validation study demonstrated its ability to predict treatment-resistant status over the SHAPS in MDD patients. While promising, further research into the use of the DARS is required to assess its test-retest viability and its use in the study of the neurobiology of anhedonia.
4.2 Behavioural Tasks
Self-report scales provide direct insight into experiences of anhedonia and have demonstrated important utility in clinical settings; however, they possess several limitations. While many consider rewarding experiences and its associated pleasures, motivations , interests and anticipation , an entirely conscious experience, this may not be the case. Several lines of evidence suggest that these experiences, while often conscious, may include an unconscious component. Kringelbach et al. (2012) asserts that at times, we may be poor at identifying our current emotional states. Further, he suggests that this may lead to an unawareness of what motivates us, why we take interest or what brings us pleasure. Several studies have suggested that reward learning often occurs implicitly. A study by Pessiglione et al. (2008) utilized a behavioural task which presented healthy participants with two cues, one associated with a monetary reward and another associated with a “punishment”. As the task progressed, participants were more prone to selecting the cues associated with a reward without their awareness, supporting the occurrence of implicit reward processing . Where self-reports can provide great explicit information, behavioural tasks can tap into both the conscious and unconscious and as such are valuable objective measures in the study of anhedonia.
4.2.1 Reward Association
The ability to develop an association between a stimulus and reward is primarily assessed using reward response bias tasks, which are based on signal detection theory (Henriques and Davidson 2000; Pizzagalli et al. 2005). Specifically, these tasks measure the level of “response bias”, which is the tendency to select the stimuli associated with greater rewards. In general, these tasks involve the presentation of two or more different stimuli with specific reward contingencies, which can vary. Stimuli can range and include verbal or non-verbal cues. One stimulus may be neutral or associated with a punishment, or all stimuli can be associated with reward but vary in terms of frequency and/or magnitude. Oftentimes, the participants are not informed of the specific reward contingencies. These tasks assess the ability of individuals to discriminate between stimuli according to their rewarding properties. During behavioural tasks that assess stimulus-reward association, healthy individuals display a bias towards rewarding stimuli (Pechtel et al. 2013). However, several studies have noted that this bias is reduced in depressed individuals, which suggests an impaired ability to form this association (Henriques and Davidson 2000; Pechtel et al. 2013; Pizzagalli et al. 2008).
4.2.2 Reward Valuation
Several factors may influence the value of a reward, such as the size and time required to obtain it (Green et al. 1997). Delay discounting tasks manipulate these variables to assess how they affect the value one places on a reward (Kirby et al. 1999). Delay discounting describes the situation where the value of a reward drops as the time to obtain the reward increases (Green et al. 1997). Most delay discounting tasks have been developed with monetary rewards which may vary in size or may be fixed (Kirby et al. 1999; Pulcu et al. 2014; Richards et al. 1999). The more immediate reward is always associated with a smaller size. MDD patients often display greater discounting effects than healthy controls and value immediate rewards more highly despite being offered a larger, albeit relatively delayed reward, suggesting differences in reward valuation (Dombrovski et al. 2012; Pulcu et al. 2014).
4.2.3 Anticipation
Several reward tasks designed to probe the other facets of reward are often modified in order to measure anticipation (Knutson et al. 2008; reviewed in Rizvi et al. 2016). These tasks are commonly used in a neuroimaging environment. Changes in brain activity prior to the participant obtaining the reward are used as measures of anticipation (Knutson et al. 2008; Kumar et al. 2014). The monetary incentive delay task was designed to distinguish anticipatory and consummatory facets of reward processing (Knutson et al. 2008). This task is composed of three trial types, a reward trial, punishment trial and no-incentive trial. Each trial is composed of an incentive cue, target stimulus and then a feedback. The goal is to press the correct button associated with the trial type once the target stimulus has been presented to increase win money or to avoid losing money.
4.2.4 Expectation
Prediction error tasks assess brain activity associated with changes in dopaminergic activity in the ventral striatum in response to outcomes that are different than expected (Schultz 1998; reviewed in Rizvi et al. 2016; Schultz 2013). Outcomes that are better than predicted are associated with an increased burst of dopamine . In contrast, there is a decrease in dopamine signaling when the outcome is worse than predicted. No changes in activity occur when the result is accurately predicted. Many variations of the task have been created, but they all involve having participants learn a certain reward contingency, which changes and results in a greater or lesser reward than expected (Forbes et al. 2009; Kumar et al. 2008; reviewed in Rizvi et al. 2016). Cohen et al. (2009) developed a prediction error task which was composed of two phases: a learning phase and a choosing phase. In the learning phase, one of two stimuli is presented at one time to allow the participants to learn their reward contingencies. The “safe” stimulus is rewarded 100% of the time, whereas the “risky” stimulus has a chance of loss or gain. Once completed, the participants begin the choosing phase where they are presented with both stimuli and are asked to select one. MDD patients demonstrate reduced prediction error signal compared to healthy controls. There is also some evidence to suggest that MDD and schizophrenia patients have dysfunction in shared as well as disparate brain regions during prediction error tasks.
4.2.5 Motivation
Motivation can be assessed using a cued-reinforcement reaction time task which assesses reaction time speed (Chase et al. 2010; Cools et al. 2005; reviewed in Rizvi et al. 2016). Cools et al. (2005) developed this task in order to assess the impact of reduced serotonin levels on motivation. During the task, three circles are presented, with one arranged in a different orientation. The goal is to select the “out-of-place” circle as fast as possible, with faster responses rewarding more points. Prior to each trial, a coloured rectangle will be presented which will signify the probability of receiving a reward. MDD participants tend to be less affected by motivational cues, thus will respond with lower reaction times than healthy controls (Treadway 2015).
4.2.6 Effort
Effort to obtain a reward is necessary for reward decision making via a cost-benefit analysis. Consequently, Treadway et al. (2012) developed the effort-expenditure for rewards task to determine the effect of probability and reward size on effort-based decision making. This task is composed of two trial types, “easy” and “hard”. Prior to the start of the trial, the probability of receiving the reward upon successful completion and size of the reward is listed for each trial type. The goal of each trial is to press a button several times to fill a metre in a certain period. The time limit, finger selection and number of button presses required depend on the trial type. Prior to each trial, participants are to select either the low reward and low-cost “easy” trial or the high/low reward and high-cost “hard” trial. This was done in a limited amount of time to ensure that selection was based on effort calculations. As noted in several studies, MDD patients expend less effort to obtain rewards (Prevost et al. 2010; Salamone et al. 2003; Treadway et al. 2009). Treadway et al. (2012) also reported that anhedonia severity was negatively correlated with willingness to expend effort, especially when there was a low probability of a reward.
4.2.7 Feedback Integration
Several probabilistic reversal learning tasks have been developed to assess the effect feedback has on reward learning (Hasler et al. 2009; Murphy et al. 2003; Taylor Tavares et al. 2008). These tasks always include the presentation of two stimuli simultaneously, both with an equal probability of being associated with a reward. The first stimulus a participant selects will subsequently be associated with a high probability of reward in future trials. Participants are told to select the stimulus most associated with reward despite any potential reward losses that may arise. However, participants are also told that the rules may reverse with the other stimulus being more rewarded and to then select this one. Learning may occur through positive feedback or negative feedback. For example, participants may obtain more correct answers by focusing on positive feedback or by avoiding negative feedback. MDD patients are more hypersensitive to negative feedback and will often switch their selection to the incorrect stimulus too soon (Thomson 2015). In line with this, Murphy et al. (2003) demonstrated that MDD patients are more likely to view a potentially rewarding stimulus as non-rewarding shortly after any negative association of the stimulus’ rewarding properties is received.
In summary, behavioural tasks can evaluate various aspects of reward processing including response bias and learning. Importantly, most tasks use monetary reward, instead of primary rewards (e.g. food, social reward). Levels of monetary reward may also be too small to elicit a strong reward response. Future research should evaluate different types of reward in the above described paradigms.
5 Treatment of Anhedonia
Currently, there are many treatment options available for MDD; however, the prevalence of treatment-resistant depression remains significantly high (Kennedy et al. 2016; Lam et al. 2016). The inadequacy of current treatment options are highlighted in the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study (Warden et al. 2007). In this study of over 3000 patients, participants initially received a first-line antidepressant. If the patient failed to achieve remission, they received an additional antidepressant . By the fourth treatment step, 30% of patients failed to achieve remission (Warden et al. 2007). Currently, the serotonin and norepinephrine systems remain the primary target of first-line antidepressants (Kennedy et al. 2016). Most of these first-line treatments are selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) . Since dopamine and other neurotransmitters play a significant role in the reward system (McCabe et al. 2010; Wassum et al. 2009; Wong et al. 1991; reviewed in Rizvi et al. 2016), this has important implications in MDD treatment since conventional antidepressants do not significantly target these systems. There has been substantial evidence linking anhedonia to poor treatment outcomes, including treatment resistance (Malhi and Berk 2007; Malhi et al. 2005; Rizvi et al. 2014a, b; Souery et al. 1999). This suggests that targeting the dopamine or other systems involved in anhedonia may benefit MDD treatment. Despite being a core symptom, there are not a significant amount of studies conducted on the effects of antidepressants on anhedonia.
While SSRIs have demonstrated effectiveness in the treatment of MDD, they have been reported to induce emotional blunting effects (McCabe et al. 2009). Healthy controls treated with citalopram had lowered emotional responses to aversive and rewarding stimuli which indicate that SSRIs can impact emotional range (McCabe et al. 2009). Interestingly, when participants were treated with the noradrenergic antidepressant reboxetine, they demonstrated greater response to rewarding stimuli and decreased response to aversive stimuli (McCabe et al. 2010). Norepinephrine is associated with increased attention and is synthesized from dopamine (McCabe et al. 2010). Further, preclinical studies in mice have demonstrated that SNRIs may be effective in minimizing the emotional blunting effects of serotonin while retaining its antidepressant activity (Dekeyne et al. 2002). While promising, further studies are required to confirm whether SNRIs are more favourable than SSRIs in the treatment of anhedonia.
Agomelatine , a melatonergic antidepressant, has demonstrated efficacy in depression (Kennedy and Rizvi 2010). In addition to action on the melatonin system, agomelatine disinhibits the release of norepinephrine and dopamine by acting as a 5-HT2c receptor antagonist. Demyttenaere et al. (2013) demonstrated that agomelatine treatment had a greater reduction in Hamilton depression rating scores relative to SSRIs. Gargoloff et al. (2016) took this further and assessed the effectiveness of agomelatine as a treatment of anhedonia. In this 8-week trial, 143 patients were given agomelatine , and anhedonia was assessed using the SHAPS. Gargoloff and colleagues reported a significant decrease in anhedonia as early as 1 week of treatment. Interestingly, patients who were also on concomitant treatments demonstrated a delayed improvement in anhedonia. The authors suggested that the increase in serotonin levels by SSRIs may dampen the activity of norepinephrine and dopamine , reducing their ability to improve anhedonia. Finally, the authors also performed a separate analysis which compared changes in anhedonia between patients experiencing their first episode to those who are experiencing recurrent episodes. Both groups demonstrated similar reductions in anhedonia.
In response to the high failure rate of first-line antidepressant monotherapy, there has been an increase use of adjunctive pharmacotherapy to target specific neurotransmitter systems, which include stimulants (e.g. methylphenidate, dextroamphetamine) (Kennedy et al. 2016). Rizvi et al. (2014a) conducted a secondary analysis of osmotic-release oral system methylphenidate (OROS-MPH) to determine whether early symptomatic improvements in apathy/anhedonia predicted increased likelihood of treatment response compared to placebo. Using the Apathy Evaluation Scale (AES) , the authors determined that early improvements in apathy predicted increased likelihood of treatment response only in the active drug group and not the placebo group. These results support the notion that a personalized treatment approach may be beneficial to alleviate specific symptoms experienced by a patient, including anhedonia.
Deep brain stimulation (DBS) is a neurosurgical procedure that has recently been adapted for use in MDD treatment and was originally used for the treatment of pain and movement disorders (Kennedy and Giacobbe 2007). Certain brain areas associated with reward have been selected as potential targets of DBS treatment in MDD. Currently, DBS use is experimental and only conducted in severely treatment-resistant patients as it is highly invasive. In 2005, Mayberg and colleagues were the first to study the use of DBS in the subcallosal cingulate gyrus (SCG), a region of the anterior cingulate cortex (ACC) which is responsible for emotion regulation. The SCG is directly connected to the ventral striatum, nucleus accumbens, rostral portions of the prefrontal cortex and the central nuclei of the amygdala , which are areas implicated in reward processing . Dopamine receptors are also expressed in these areas, which suggest that DBS may impact dopamine activity and subsequently anhedonia. Preliminary data suggest that DBS to the SCG and nucleus accumbens has a preferential effect on mood and anhedonia symptoms (Lipsman et al. 2014; Schlaephfer et al. 2008).
Conclusion
This chapter highlighted key updates in anhedonia research and how modern definitions affected the trajectory of this research. Past constructs of anhedonia were broad and focused primarily on consummatory pleasure, which limited our understanding of the underlying neurobiology and potential development of treatment strategies. Reward processing includes interest, anticipation , motivation , effort and pleasure; a deficit in any of these facets may result in the clinical symptom of anhedonia . Behavioural tasks in tandem with neuroimaging have identified that slightly distinct pathways govern the activity of each reward facet, which underscores that anhedonia is a multi-faceted construct. This has also been reflected in the development of contemporary self-report questionnaires. There are various treatments that target anhedonia symptoms due to their effect on the dopaminergic and noradrenergic systems; however, further research is needed to elucidate the effects of conventional antidepressants on anhedonia . As our understanding of anhedonia progresses, reward processing models may be refined and allow for more personalized treatment strategies.
References
Chapman LJ, Chapman JP, Raulin ML. Scales for physical and social anhedonia. J Abnorm Psychol. 1976;85:374–82.
Chase HW, Michael A, Bullmore ET, Sahakian BJ, Robbins TW. Paradoxical enhancement of choice reaction time performance in patients with major depression. J Psychopharmacol. 2010;24(4):471-479.
Clark DC, Fawcett J, Salazar-Grueso E, Fawcett E. Seven-month clinical outcome of anhedonic and normally hedonic depressed inpatients. Am J Psychiatry. 1984;141:1216–20.
Cohen MX, Axmacher N, Lernartz G, Baup N, Fossati P, Pessiglione M. Neuroelectric signatures of reward learning and decision-making in the human nucleus accumbens. Neuropsychopharmacology. 2009;34:1649–58.
Cools R, Blackwell A, Clark L, Menzies L, Cox S, Robbin TW. Tryptophan depletion disrupts the motivational guidance of goal-directed behaviour as a function of trait impulsivity. Neuropsychopharmacology. 2005;30:1362–73.
Dekeyne A, Gobert A, Auclair A, Girardon S, Millan M. Differential modulation of efficiency in a food-rewarded ‘differential reinforcement of low-rate’ 72-s schedule in rats by norepinephrine and serotonin reuptake inhibitors. Psychopharmacology. 2002;162:156–67.
Demyttenaere K, Corruble E, Hale A, Quera-Salva MA, Picarel-Blanchot F, Kasper S. A pooled analysis of six month comparative efficacy and tolerability in four randomized clinical trials: agomelatine versus escitalopram, fluoxetine, and sertraline. CNS Spectr. 2013;18(3):163–70.
Der-Avakian A, Markou A. The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci. 2012;35:68–77.
Dombrovski AY, Siegle GJ, Szanto K, Clark L, Reynolds CF, Aizenstein H. The temptation of suicide: striatal gray matter, discounting of delayed rewards, and suicide attempts in late-life depression. Psychol Med. 2012;42:1203–15.
Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry. 2007;64(3):327–37.
Elliott R, Friston KJ, Dolan RJ. Dissociable neural responses in human reward systems. J Neurosci. 2000;20:6159–65.
Fawcett J, Clark DC, Scheftner WA, Gibbons RD. Assessing anhedonia in psychiatric patients. Arch Gen Psychiatry. 1983;40:79–84.
Forbes EE, Hariri AR, Martin SL, Silk JS, Moyles DL, Fisher PM, Brown SM, Ryan ND, Birmaher B, Axelson DA, Dahl RE. Altered striatal activation predicting real-world positive affect in adolescent major depressive disorder. Am J Psychiatry. 2009;166:64–73.
Gabbay V, Mao X, Klein RG, Ely BA, Babb JS, Panzer AM, Alonso CM, Shungu DC. Anterior cingulate cortex γ-aminobutyric acid in depressed adolescents: relationship to anhedonia. Arch Gen Psychiatry. 2012;69:139–49.
Gard DE, Gard MG, Kring AM, John OP. Anticipatory and consummatory components of the experience of pleasure: a scale development study. J Res Pers. 2006;40:1086–102.
Gard DE, Kring AM, Gard MG, Horan WP, Green MF. Anhedonia in schizophrenia: distinctions between anticipatory and consummatory pleasure. Schizophr Res. 2007;93:253–60.
Garfield JB, Cotton SM, Lubman DI. Psychometric properties, validity, and reliability of the temporal experience of Pleasure Scale state version in an opioid-dependent sample. Drug Alcohol Depend. 2016;161:238–46.
Gargoloff PD, Corral R, Herbst L, Marquez M, Martinotti G, Gargoloff PR. Effectiveness of agomelatine on anhedonia in depressed patients: an outpatient, open-label, real-world study. Hum Psychopharmacol Clin Exp. 2016;31(6):412–8.
Gooding DC, Pflum MJ. The assessment of interpersonal pleasure: introduction of the Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS) and preliminary findings. Psychiatry Res. 2014;215:237–43.
Grabenhorst F, Rolls ET. Value, pleasure and choice in the ventral prefrontal cortex. Trends Cogn Sci. 2011;15:56–67.
Green L, Myerson J, McFadden E. Rate of temporal discounting decreases with amount of reward. Mem Cogn. 1997;25:715–23.
Hamilton JP, Furman DJ, Chang C, et al. Default-mode and task-positive network activity in major depressive disorder: implications for adaptive and maladaptive rumination. Biol Psychiatry. 2011;70:327–33.
Hasler G, Mondillo K, Drevets WC, Blair JR. Impairments of probabilistic response reversal and passive avoidance following catecholamine depletion. Neuropsychopharmacology. 2009;34:2691–8.
Henriques JB, Davidson RJ. Decreased responsiveness to reward in depression. Cognit Emot. 2000;14:711–24.
Hess JL, Kawaguchi DM, Wagner KE, Faraone SV, Glatt SJ. The influence of genes on “positive valence systems” constructs: a systematic review. Am J Med Genet B Neuropsychiatr Genet. 2016;171B(1):92–110.
Hsu DT, Sanford BJ, Meyers KK, Love TM, Hazlett KE, Walker SJ, Mickey BJ, Koeppe RA, Langenecker SA, Zubieta JK. It still hurts: altered endogenous opioid activity in the brain during social rejection and acceptance in major depressive disorder. Mol Psychiatry. 2015;20(2):193–200.
Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, Sanislow C, Wang P. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry. 2010;167(7):748–51.
Johnson SW, North RA. Opioids excite dopamine neurons by hyperpolarization of local interneurons. J Neurosci. 1992;12:483–8.
Kennedy SH, Giacobbe P. Treatment resistant depression—advances in somatic therapies. Ann Clin Psychiatry. 2007;19:279–87.
Kennedy SH, Rizvi SJ. Agomelatine in the treatment of major depressive disorder: potential for clinical effectiveness. CNS Drugs. 2010;24(6):479–99.
Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, Hasnain M, Jollant F, Levitt AJ, MacQueen GM, McInerney SJ, McIntosh D, Milev RV, Muller DJ, Parikh SV, Pearson NL, Ravindran AV, Uher R, CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacological treatments. Can J Psychiatry. 2016;61:540–60.
Kirby N, Petry NM, Bickel WK. Heroin addicts have higher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol Gen. 1999;128:78–87.
Knutson B, Bhanji J, Cooney R, Atlas L, Gotlib I. Neural responses to monetary incentives in major depression. Biol Psychiatry. 2008;63:686–92.
Kring AM, Barch DM. The motivation and pleasure dimension of negative symptoms: neural substrates and behavioral outputs. Eur Neuropsychopharmacol. 2014;24:725–36.
Kringelbach ML, Stein A, Van Hartevelt TJ. The functional human neuroanatomy of food pleasure cycles. Physiol Behav. 2012;106:307–16.
Kugaya A, Sanacora G, Verhoeff NP, Fujita M, Mason GF, Seneca NM, Bozkurt A, Khan SA, Anand A, Degen K, Charney DS, Zoghbi SS, Baldwin RM, Seibyl JP, Innis RB. Cerebral benzodiazepine receptors in depressed patients measured with [123I]iomazenil SPECT. Biol Psychiatry. 2003;54:792–9.
Kumar P, Waiter G, Ahearn T, Milders M, Reid I, Steele JD. Abnormal temporal difference reward-learning signals in major depression. Brain. 2008;131:2084–93.
Kumar P, Berghorst LH, Nickerson LD, Dutra SJ, Goer FK, Greve DN, Pizzagalli DA. Differential effects of acute stress on anticipatory and consummatory phases of reward processing. Neuroscience. 2014;266:1–12.
Lam RW, Wang J, Enns MW, Kolivakis T, Michalak EE, Sareen J, Song W, Kennedy SH, MacQueen GM, Milev RV, Parikh SV, Ravindran AV, CANMAT Depression Work Group. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 1. Disease burden and principles of care. Can J Psychiatry. 2016;61:510–23.
Leventhal AM, Chasson GS, Tapia E, Miller EK, Pettit JW. Measuring hedonic capacity in depression: a psychometric analysis of three anhedonia scales. J Clin Psychol. 2006;62:1545–58.
Lipsman N, Sankar T, Downar J, Kennedy SH, Lozano AM, Giacobbe P. Neuromodulation for treatment-refractory major depressive disorder. CMAJ. 2014;186(1):33–9.
Malhi GS, Berk M. Does dopamine dysfunction drive depression? Acta Psychiatr Scand. 2007;115(Suppl 433):116–24.
Malhi GS, Parker GB, Crawford J, Wilhelm K, Mitchell PB. Treatment-resistant depression: resistant to definition? Acta Psychiatr Scand. 2005;112(4):302–9.
Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C, Schwalb JM, Kennedy SH. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45:651–60.
McCabe C, Cowen PJ, Harmer CJ. Neural representation of reward in recovered depressed patients. Psychopharmacology. 2009;205:667–77.
McCabe C, Mishor Z, Cowen PJ, Harmer CJ. Diminished neural processing of aversive and rewarding stimuli during selective serotonin reuptake inhibitor treatment. Biol Psychiatry. 2010;67(5):439–45.
McMakin DL, Olino TM, Porta G, Dietz DJ, Emslie G, Clarke G, Wagner KD, Asarnow JR, Ryan ND, Birmaher B, Shamseddeen W, Mayes T, Kennard B, Spirito A, Keller M, Lynch FL, Dickerson JF, Brent DA. Anhedonia predicts poorer recovery among youth with selective serotonin reuptake inhibitor-treatment resistant depression. J Am Acad Child Adolesc Psychiatry. 2012;51(4):404–11.
Murphy FC, Michael A, Robbins TW, Sahakian BJ. Neuropsychological impairments in patients with major depressive disorder: the effects of feedback on task performance. Psychol Med. 2003;33:455–67.
Pechtel P, Dutra S, Goetz E, Pizzagalli D. Blunted reward responsiveness in remitted depression. J Psychiatr Res. 2013;47:1864–9.
Pessiglione M, Petrovic P, Daunizeau J, Palminteri S, Dolan RJ, Frith CD. Subliminal instrumental conditioning demonstrated in the human brain. Neuron. 2008;59:561–7.
Pizzagalli DA, Jahn AL, O’Shea JP. Toward an objective characterization of an anhedonic phenotype: a signal-detection approach. Biol Psychiatry. 2005;57:319–27.
Pizzagalli DA, Losifescu D, Hallett LA, Ratner KG, Fava M. Reduced hedonic capacity in major depressive disorder: evidence from a probabilistic reward task. J Psychiatr Res. 2008;43:76–87.
Prevost C, Pessiglione M, Metereau E, Clery-Melin ML, Dreher JC. Separate valuation subsystems for delay and effort decision costs. J Neurosci. 2010;30(42):14080–90.
Pulcu E, Trotter PD, Thomas EJ, McFarquhar M, Juhasz G, Sahakian BJ, Deakin JF, Zahn R, Anderson IM, Elliott R. Temporal discounting in major depressive disorder. Psychol Med. 2014;44:1825.
Rawal A, Collishaw S, Thapar A, Rice F. ‘The risks of playing it safe’: a prospective longitudinal study of response to reward in the adolescent offspring of depressed parents. Psychol Med. 2013;43:27–38.
Richards JB, Zhang L, Mitchell SH, de Wit H. Delay or probability discounting in a model of impulsive behavior: effect of alcohol. J Exp Anal Behav. 1999;71:121–43.
Rizvi SJ, Geraci J, Ravindran A, Kennedy SH. Predictors of response to adjunctive osmotic-release methylphenidate or placebo in patients with major depressive disorder: effects of apathy/anhedonia and fatigue. J Clin Psychopharmacol. 2014a;34(6):755–9.
Rizvi SJ, Grima E, Tan M, Rotzinger S, Lin P, McIntyre RS, Kennedy SH. Treatment-resistant depression in primary care across Canada. Can J Psychiatr. 2014b;59(7):349–57.
Rizvi SJ, Quilty LC, Sproule BA, Cyriac A, Michael Bagby R, Kennedy SH. Development and validation of the Dimensional Anhedonia Rating Scale (DARS) in a community sample and individuals with major depression. Psychiatry Res. 2015;229(1–2):109–19.
Rizvi SJ, Pizzagalli DA, Sproule BA, Kennedy SH. Assessing anhedonia in depression: potentials and pitfalls. Neurosci Biobehav Rev. 2016;65:21–35.
Salamone JD, Correa M, Mingote S, Weber SM. Nucleus accumbens dopamine and the regulation of effort in food-seeking behavior: implications for studies of natural motivation, psychiatry, and drug abuse. J Pharmacol Exp Ther. 2003;305:1–8.
Salamone JD, Farrar AM, Font L, Patel V, Schlar DE, Nunes EJ, Collins LE, Sagar TN. Differential actions of adenosine A1 and A2A antagonists on the effort-related effects of dopamine D2 antagonism. Behav Brain Res. 2009;201:216–22.
Sanacora G, Mason GF, Rothman DL, Behar KL, Hyder F, Petroff OA, Berman RM, Charney DS, Krystal JH. Reduced cortical gamma-aminobutyric acid levels in depressed patients determined by proton magnetic resonance spectroscopy. Arch Gen Psychiatry. 1999;56:1043–7.
Schlaepfer TE, Cohen MX, Frick C, Kosel M, Brodesser D, Axmacher N, Joe AY, Kreft M, Lenartz D, Sturm V. Deep brain stimulation to reward circuitry alleviates anhedonia in refractory major depression. Neuropsychopharmacology. 2008;33(2):368–77.
Schultz W. Predictive reward signal of dopamine neurons. J Neurophysiol. 1998;80:1–27.
Schultz W. Updating dopamine reward signals. Curr Opin Neurobiol. 2013;23:229–38.
Seo H, Lee D. Temporal filtering of reward signals in the dorsal anterior cingulate cortex during a mixed-strategy game. J Neurosci. 2007;27:8366–77.
Sharma A, Wolf DH, Ciric R, Kable JW, Moore TM, Vandekar SN, Katchmar N, Daldal A, Ruparel K, Davatzikos C, Elliot MA, Calkins ME, Shinohara RT, Bassett DS, Satterthwaite TD. Common dimensional reward deficits across mood and psychotic disorders: a Connectome-Wide Association Study. Am J Psychiatr. 2017;174:657–66.
Snaith RP, Hamilton M, Morley S, Humayan A, Hargreaves D, Trigwell P. A scale for the assessment of hedonic tone the Snaith-Hamilton Pleasure Scale. Br J Psychiatry. 1995;167:99–103.
Souery D, Amsterdam J, de Montigny C, Lecrubier Y, Montgomery S, Lipp O, Racagni G, Zohar J, Mendlewicz J. Treatment resistant depression: methodological overview and operational criteria. Eur Neuropsychopharmacol. 1999;9:83–91.
Sternat T, Katzman MA. Neurobiology of hedonic tone: the relationship between treatment-resistant depression, attention-deficit hyperactivity disorder, and substance abuse. Neuropsychiatr Dis Treat. 2016;12:2149–64.
Taylor Tavares JV, Clark L, Furey ML, Williams GB, Sahakian BJ, Drevets WC. Neural basis of abnormal response to negative feedback in unmedicated mood disorders. Neuroimage. 2008;42:1118–26.
Thomson KR. Measuring anhedonia: impaired ability to pursue, experience, and learn about reward. Front Psychol. 2015;6:1409.
Treadway MT. The neurobiology of motivational deficits in depression—an update on candidate pathomechanisms. Curr Top Behav Neurosci. 2015;27:337–55.
Treadway MT, Zald DH. Reconsidering anhedonia in depression: lessons from translational neuroscience. Neurosci Biobehav Rev. 2011;35(3):537–55.
Treadway MT, Buckholtz JW, Schwartzman AN, Lambert WE, Zald DH. Worth the ‘EEfRT’? The effort expenditure for rewards task as an objective measure of motivation and anhedonia. PLoS One. 2009;4:e6598.
Treadway MT, Bossaller N, Shelton RC, Zald DH. Effort-based decision-making in major depressive disorder: a translational model of motivational anhedonia. J Abnorm Psychol. 2012;121(3):553–8.
Tremblay LK, Naranjo CA, Graham SJ, Herrmann N, Mayberg HS, Hevenor S, Busto UE. Functional neuroanatomical substrates of altered reward processing in major depressive disorder revealed by a dopaminergic probe. Arch Gen Psychiatry. 2005;62:1228–36.
Tso IF, Grove TB, Taylor SF. Differential hedonic experience and behavioral activation in schizophrenia and bipolar disorder. Psychiatry Res. 2014;219:470–6.
Uher R, Farmer A, Maier W, Rietschel M, Hauser J, Marusic A, Mors O, Elkin A, Williamson RJ, Schmael C, Henigsberg N, Perez J, Mendlewicz J, Janzing JG, Zobel A, Skibinska M, Kozel D, Stamp AS, Bajs M, Placentino A, Barreto M, McGuffin P, Aitchison KJ. Measuring depression: comparison and integration of three scales in the GENDEP study. Psychol Med. 2008;38:289–300.
Uher R, Perlis RH, Henigsberg N, Zobel A, Rietschel M, Mors O, Hauser J, Dernovsek Z, Souery D, Bajs M, Maier W, Aitchison KJ, Farmer A, McGuffin P. Depression symptom dimensions as predictors of antidepressant treatment outcome: replicable evidence for interest-activity symptoms. Psychol Med. 2012;42(5):967–80.
Vengeliene V, Bespalov A, Robmanith M, Horschitz S, Berger S, Relo AL, Noori HR, Schneider P, Enkel T, Bartsch D, Schneider M, Behl B, Hansson AC, Schloss P, Spanagel R. Toward trans-diagnostic mechanisms in psychiatry: neurobehavioral profile of rats with a loss-of-function point mutation in the dopamine transporter gene. Dis Model Mech. 2017;10(4):451–61.
Warden D, Rush AJ, Trivedi MH, Fava M, Wisniewski SR. The STAR*D project results: a comprehensive review of findings. Curr Psychiatry Rep. 2007;9(6):449–59.
Wassum KM, Ostlund SB, Maidment NT, Balleine BW. Distinct opioid circuits determine the palatability and the desirability of rewarding events. Proc Natl Acad Sci U S A. 2009;106:12512–7.
Whitton AE, Treadway MT, Pizzagalli DA. Reward processing dysfunction in major depression, bipolar disorder and schizophrenia. Curr Opin Psychiatry. 2015;28(1):7–12.
Wong LS, Eshel G, Dreher J, Ong J, Jackson DM. Role of dopamine and GABA in the control of motor activity elicited from the rat nucleus accumbens. Pharmacol Biochem Behav. 1991;38:829–35.
World Health Organization. Depression fact sheet. 2017. http://www.who.int/mediacentre/factsheets/fs369/en/.
Zhang B, Lin P, Shi H, Ongur D, Auerbach RP, Wang X, Yao S, Wang X. Mapping anhedonia-specific dysfunction in a transdiagnostic approach: an ALE meta-analysis. Brain Imaging Behav. 2016;10:920–39.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer Nature Singapore Pte Ltd.
About this chapter
Cite this chapter
Chow, T.K., Kennedy, S., Rizvi, S.J. (2018). Anhedonia as a Crucial Factor of Depression: Assessment, Neurobiological Underpinnings and Treatment. In: Kim, YK. (eds) Understanding Depression. Springer, Singapore. https://doi.org/10.1007/978-981-10-6577-4_7
Download citation
DOI: https://doi.org/10.1007/978-981-10-6577-4_7
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-6576-7
Online ISBN: 978-981-10-6577-4
eBook Packages: MedicineMedicine (R0)