
Abstract
The dominant frequency (DF) of atrial electrogram was claimed by researchers as to be correlated to the electrical activation of the atrial fibrillation (AF). By assessing the DF of AF data of 5 patients with persistent AF, this paper presented some AF signal analysis done to study the performance of the raw data, which is the data without QRS-T subtraction, data with QRS-T subtraction and rectification. The resultant data were mapped in 3-dimensional shapes of respective patients left atrium (LA), showing the DF activity changes during 21 s data recorded. The maps are useful for further analysis to justify which of the mentioned signal processing step is more reliable and also to study the relation between particular sites on the LA with the source (sites) of activation of AF.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Atrial fibrillation (AF) is a common arrhythmia which more often than not leads to stroke [1, 2]. AF happens when the heart beats abnormally, in fast and irregular rhythm in the atria [3]. There are three types of AF: paroxysmal, persistent and permanent [4,5,6]. Paroxysmal AF only occurs once in a while, i.e. spontaneously terminated within 7 days, while persistent AF is one that does not stop by itself, i.e. sustained more than 7 days, but will stop if medication or cardioversion is given to help the heart return to its normal rhythm [7]. The permanent AF is however present all the time and cannot be fixed with either medication or cardioversion [7]. Hence, AF increases in criticality from paroxysmal to persistent and finally the permanent type.
1.1 AF Treatment
There are three main methods for AF treatment today. The first one is medication. This is simply done by giving antiarrhythmic drugs to the patient to regulate the heart activity into normal rhythm [7, 8]. The second treatment is through surgical procedure. AF patients will be implanted with pacemaker or implantable defibrillator which invasively helps the patient heart to regulate normally [1, 9]. The third main treatment for AF is by non-surgical procedures. This type of treatment includes electrical cardioversion and the catheter-based radiofrequency (RF) ablation. Electrical cardioversion is commonly done by applying a certain amount of electricity on the patient chest by using a paddles or patches to help reset the electrical conduction of the heart [5].
In this research, we are interested on the catheter ablation procedure. Catheter ablation has widely been used in the treatment procedure for paroxysmal or persistent AF [4, 10, 11]. However, the ablation is considerably a random burnt of patient left atrium (LA) tissue if it is done by delivering the RF energy throughout the cardiac tissue of the left atrium (LA) wall with no accurately identifiable site of AF activation source on the atrium wall as the specific ablation target. Furthermore, to minimize the risk of infection or death to the patients, the sites for ablation should be determined accurately within a short time [4, 12]. Hence, extended study on the signal of the atrial electrogram data is requisite to help improve the current treatment procedure.
1.2 AF Activation Sites and Correlation with Dominant Frequency
Researchers believed that AF is maintained by sites with high frequency, thus known as the activation source of AF [4, 13,14,15,16]. The main sites of activation include the left atrium (LA) roof, LA septum, LA posterior wall as well as the pulmonary vein’s area [16, 17]. Since AF activity consists of signal which is random and often chaotic, the frequency domain analysis is preferable compare to the time domain analysis [4, 13, 15]. Dominant frequency (DF) is the commonly determined parameter in the frequency domain analysis which defined as the frequency with highest magnitude or power [4, 13, 18].
This paper will present the signal processing of the atrial electrogram to obtain the 3-dimensional mapping of the AF data using the raw data, data after QRS-T subtraction, and data after QRS-T subtraction being rectified. The study is significant to evaluate the signal processing steps which might contribute to time reduction in selecting the sites for ablation by understanding the correlation between the electrical activation of AF and its dominant frequency estimation.
2 Methodology
Figure 1 shows the methodology flow chart for the research. We proposed the raw data undergo QRS-T subtraction and rectification processing steps before the 3D DF mapping.

Methodology flowchart
2.1 Subjects and Data Collection
The research focused on data of a total of five patients with persistent AF. The raw data were collected when the subjects underwent catheter ablation guided by contact mapping using Ensite, NavX 6.0, St. Jude Medical (Glenfield Hospital, University of Leceister), performed in 20-s long continuous segments of each of the 2048 non-contact unipolar electrograms during AF.
The raw data collected for the research consist of wave (ECG) and virtual (atrial electrogram) signal recorded for a total of 21 s (7 s per recoding). The subjects’ data files were named as a1, a2, a3, a4 and a5 respectively.
2.2 QRS-T Subtraction
The QRS-T components are signals caused by the ventricular activity of the heart which range between 10–30 Hz [19,20,21,22]. Hence, it is somehow irrelevant in this study of AF which mainly occurred in the left atrium. Meanwhile, studies show that AF range between 5–12 Hz [21]. Therefore, subtracting the QRS-T components from the atrial electrogram data might help improve the result of the analysis because the frequency overlapping will be eliminated [21, 23].
In this study, the interest data is the atrial electrogram (labeled as virtual) data. However, the ECG data recorded is useful as a reference to initially identify the location of the frequency of the QRS-T components to be subtracted later from the atrial electrogram data. This is because the normal ECG waveform is a basic repeating signal pattern with P, Q, R, S and T waves as shown in Fig. 2, therefore allowed easier detection of QRS and T components to be subtracted. Conversely, the AF waveform is rather random and irregular, so it is difficult to identify the QRS and T components from the AF graph.

General waveform for ECG signal
Flat interpolation method has been applied to replace the subtracted QRS-T waves with a base value.
2.3 Rectification
Rectification is another proposed signal processing for the data. This enables justification on the necessary of rectification on the data to improve the signal analysis. Rectification is used to transform biphasic waveform into monophasic waveform by using the absolute value function in Matlab [15]. According to some researchers, rectification can cause the peak and troughs of a signal become correspond with a sinusoid signal [15]. This information is essential especially for local recording of atrial electrogram which either using unipolar or bipolar electrode, because of its typical sharp biphasic waveform which requires signal preprocessing steps [15, 20, 24]. The more similar a signal pattern is to the sinusoid signal (in time domain), the lesser the error existed when using Fourier transform method for frequency domain analysis [15]. Similarly, the closer the atrial electrogram waveform being approximated to a sinusoidal function, the better the DF analysis could reflect the activation rate of AF.
2.4 Fast Fourier Transform
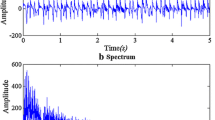
As mentioned earlier, DF is the main parameter determined to study the nature of the electrical activation of AF in frequency domain. Fast Fourier Transform (FFT) method has been chosen to obtain the dominant frequency of each of the 2048 point data for 21 s after the QRS-T subtraction and rectification. FFT method is claimed as fast and accurate in estimating the DF compare to methods such as autoregressive (AR), Blackman Tukey (BT) and the multiple signal classification (MUSIC) method [12].
2.5 3-Dimensional (3D) DF Mapping
The dominant frequencies of the data were also represented visually in 3-dimensional maps of left atrium wall for respective subjects. Different subjects have distinctive shapes of left atrium as shown in Fig. 3. Matlab coding is used to plot the 3-dimensional maps showing their particular frequency which keep on changing during the 21 s recording.

Subjects (a1), (a2), (a3), (a4) and (a5) respective 3D LA shapes
3 Result and Continuous Work
3D maps in default view were obtained as the result after the 3D DF mapping procedure. For each subject, 21 figures were obtained and saved to visualize the changes of DF on the maps per second. This will be used for visual observation and comparison of the DF changes for the raw data, data with QRS-T subtraction as well as the one with rectification. Figure 4 shows the example of 3D DF maps obtained for subject a1 for the 21 s consecutive AF.





(a) Subjects a1 3D DF maps for 1–3 s, (b) subjects a1 3D DF maps for 4–8 s, (c) subjects a1 3D DF maps for 9–13 s, (d) subjects a1 3D DF maps for 14–18 s, (e) subjects a1 3D DF maps for 19–21 s
These resultant 3D DF maps will further being used for proving relation between sites of LA (PV, MV, LAA and non DF areas) with the existence of electrical activation sources and also to study the reliability of QRS-T subtraction and rectification steps for better study of the AF electrogram data. For instance, DF activity on the known sites on LA such as the pulmonary veins (PV), left atrium appendage (LAA), and mitral valve (MV) areas might show significant irregular DF activity within the 21 s recording. If this happens, it can be inferred that the particular site do contribute or act as the main activation sites for AF as claimed by some researchers.
Another method to study the 3D DF maps is by using the organization index (OI) calculation. OI is defined as the ratio between power of DF and its harmonics (area of graph under the DF and its harmonics) to the total power. By knowing the OI value, we can relate the organization of particular sites on the LA with DF variability and thus the electrical activation of DF. The higher the OI value (>0.5), the more regular the frequency activity of the particular sites, and hence indicates low DF variability or low possibility of electrical activation source for AF on that particular area of LA.
The evaluation of sites on LA can be compared with OI analysis to justify their relatability as the sites of electrical activation source for AF. Similarly, OI analysis result will also be used together with visual observation of the 3D DF maps to infer the importance of using the preprocessing steps: QRS-T subtraction and rectification, on AF electrogram data studies.
4 Conclusion
This research is exploring pre-processing approaches which included both with and without rectification and filtering using QRS-T subtraction for DF estimation. The modelling of the electrophysiological data of AF in 3D DF maps form is a credible method to study the correlation between the DF activity of AF and its electrical activation attributes.
We believed that the QRS-T subtraction is a significant preprocessing step for the AF data. It is also expected that the DF activity in particular sites of LA, such as the PV, MV and LAA sites are more relevant to the AF electrical activation source compare to the non DF sites. However, in order to accurately study the behavior of AF and its relation with the DF, more subjects and data are desired in future.
References
Chugh, S.S., Roth, G.A., Gillum, R.F., Mensah, G.A.: Global burden of atrial fibrillation in developed and developing nations. Global Heart 9, 113–119 (2014)
Chugh, S.S., Havmoeller, R., Narayanan, K., Singh, D., Rienstra, M., Benjamin, E.J., Gillum, R.F., Kim, Y.-H., McAnulty, J.H., Zheng, Z.-J.: Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 study. Circulation 129, 837–847 (2013)
Nattel, S., Shiroshita-Takeshita, A., Brundel, B.J., Rivard, L.: Mechanisms of atrial fibrillation: lessons from animal models. Progress Cardiovasc. Dis. 48, 9–28 (2005)
Colilla, S., Crow, A., Petkun, W., Singer, D.E., Simon, T., Liu, X.: Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am. J. Cardiol. 112, 1142–1147 (2013)
Zoni-Berisso, M., Filippi, A., Landolina, M., Brignoli, O., D’Ambrosio, G., Maglia, G., Grimaldi, M., Ermini, G.: Frequency, patient characteristics, treatment strategies, and resource usage of atrial fibrillation (from the Italian Survey of Atrial Fibrillation Management [ISAF] study). Am. J. Cardiol. 111, 705–711 (2013)
Fukaya, H., Niwano, S., Sasaki, T., Kiryu, M., Kurokawa, S., Hatakeyama, Y., Sato, D., Yumoto, Y., Moriguchi, M., Niwano, H.: Attenuating effects of anti-arrhythmic agents on changes in fibrillation cycle length in very early phase paroxysmal atrial fibrillation—spectral analysis of fibrillation waves in surface ECG. J. Arrhythm. 25, 135–141 (2009)
Omar, R., Teo, W.S., Foo, D., Han, C.K., Jamaluddin, A.N., Low, L.P., Ong, T.K.: Atrial fibrillation in Singapore and Malaysia: current trends and future prospects. J. Arrhythm. 27, 171–185 (2011)
Kim, Y.H., Lim, H.E., Pak, H.N.: Use of three-dimensional mapping systems in the catheter ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 17, S16–S22 (2006)
Ching, C.K., Patel, D., Natale, A.: Catheter ablation of atrial fibrillation. J. Arrhythm. 23, 85–101 (2007)
Ahmad, A., Schlindwein, F.S., Ng, G.A.: Comparison of computation time for estimation of dominant frequency of atrial electrograms: fast fourier transform, blackman tukey, autoregressive and multiple signal classification. J. Biomed. Sci. Eng. 3, 843 (2010)
Ahmad, A., Buyamin, S., Senin, N.: Frequency analysis for surface electrocardiogram of atrial fibrillation. J. Teknol. 64 (2013)
Traykov, V.B., Pap, R., Sághy, L.: Frequency domain mapping of atrial fibrillation-methodology, experimental data and clinical implications. Curr. Cardiol. Rev. 8, 231 (2012)
Ng, J., Goldberger, J.J.: Understanding and interpreting dominant frequency analysis of AF electrograms. J. Cardiovasc. Electrophysiol. 18, 680–685 (2007)
Sanders, P., Berenfeld, O., Hocini, M., Jaïs, P., Vaidyanathan, R., Hsu, L.-F., Garrigue, S., Takahashi, Y., Rotter, M., Sacher, F.: Spectral analysis identifies sites of high-frequency activity maintaining atrial fibrillation in humans. Circulation 112, 789–797 (2005)
Jalife, J.: Rotors and spiral waves in atrial fibrillation. J. Cardiovasc. Electrophysiol. 14, 776–780 (2003)
Lin, Y.-J.: The frequency analysis and the atrial fibrillation. J. Biocatal. Biotransform. (2012)
Saini, I., Singh, D., Khosla, A.: QRS detection using K-Nearest Neighbor algorithm (KNN) and evaluation on standard ECG databases. J. Adv. Res. 4, 331–344 (2013)
Corino, V.D.A., Sassi, R., Mainardi, L.T., Cerutti, S.: Signal processing methods for information enhancement in atrial fibrillation: spectral analysis and non-linear parameters. Biomed. Signal Process. Control 1, 271–281 (2006)
Ahmad, A., Salinet Jr., J.L., Brown, P., Tuan, J.H., Stafford, P., Ng, G.A., Schlindwein, F.S.: QRS subtraction for atrial electrograms: flat, linear and spline interpolations. Med. Biol. Eng. Comput. 49, 1321–1328 (2011)
Yeh, Y.-C., Wang, W.-J.: QRS complexes detection for ECG signal: the difference operation method. Comput. Methods Programs Biomed. 91, 245–254 (2008)
Corino, V.D., Rivolta, M.W., Sassi, R., Lombardi, F., Mainardi, L.T.: Ventricular activity cancellation in electrograms during atrial fibrillation with constraints on residuals’ power. Med. Eng. Phys. 35, 1770–1777 (2013)
Ng, J., Kadish, A.H., Goldberger, J.J.: Technical considerations for dominant frequency analysis. J. Cardiovasc. Electrophysiol. 18, 757–764 (2007)
Acknowledgement
The authors would like to thank the Ministry of Higher Education and Universiti Teknologi Malaysia for supporting this research under Q.J130000.2523.15H29.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Nature Singapore Pte Ltd.
About this paper
Cite this paper
Mei, P.S.C., Subha, N.A.M., Ahmad, A. (2017). Modelling Electrophysiological Data in Persistent Atrial Fibrillation Studies Using the Evolution of 3-Dimensional Dominant Frequency Mapping. In: Mohamed Ali, M., Wahid, H., Mohd Subha, N., Sahlan, S., Md. Yunus, M., Wahap, A. (eds) Modeling, Design and Simulation of Systems. AsiaSim 2017. Communications in Computer and Information Science, vol 752. Springer, Singapore. https://doi.org/10.1007/978-981-10-6502-6_14
Download citation
DOI: https://doi.org/10.1007/978-981-10-6502-6_14
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-6501-9
Online ISBN: 978-981-10-6502-6
eBook Packages: Computer ScienceComputer Science (R0)