
Abstract
The treatment of pediatric cataracts includes surgical and conservative interventions. The ultimate goal of both treatment strategies is to improve visual functions of pediatric patients to the maximum extent and thereby enhance their quality of life. This chapter briefly reviews the history of pediatric cataract surgeries, indicating that the operative methods are constantly evolving with the development of surgical techniques and devices. However, surgery is not the only treatment option for pediatric cataracts. Conservative treatment may be considered for pediatric patients when the lens opacity is mild or the visual axis is not affected. For premature infants or children complicated with developmental disorders or systemic diseases, conservative treatment should also be considered. This chapter also introduces lens regeneration as a treatment of infantile cataracts—a new approach in pediatric cataract management.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
7.1 Evolution of Pediatric Cataract Surgical Techniques
The therapeutic strategies for pediatric cataract include surgery and conservative treatment. The ultimate goal of both treatments is to improve the visual function of children with cataract as much as possible and further enhance their quality of life.
In the early days, due to the limitations of surgical equipment and techniques, pediatric cataract surgery often resulted in a high incidence of complications, poor restoration of visual function, and in the worst cases, blindness. Therefore, the majority of earlier ophthalmologists were inclined to a conservative approach when it came to the treatment of pediatric cataract. In the last 20 years, with the rapid development of microsurgical techniques in cataract surgery, major progress has also been made in pediatric cataract surgery, which has led to better surgical outcomes, much fewer complications, and improved quality of life for pediatric patients. However, surgery is not the only option for children with cataract. If the opacity in the lens is not large, dense, or situated in a vital optical area, a conservative strategy including optical correction, regular follow-ups, and amblyopia management may be sufficient to improve visual function and prevent amblyopia. On the other hand, when surgery is needed, the selection of proper surgical timing and approach is very important. In this chapter, an overview will be given on the evolution of pediatric cataract treatments, the surgical timing, as well as indications of pediatric cataract extraction and intraocular lens implantation.
Since the first recorded pediatric cataract surgery in the early nineteenth century, the surgical techniques have undergone the following changes.
7.1.1 Cataract Discission/Needling
Cataract discission was the first recorded technique of pediatric cataract extraction. Since the procedure was simple and easy to follow, it prevailed in the early twentieth century. There are three surgical approaches in discission/needling, i.e., anterior discission, posterior discission, and through-and-through discission [1, 2]. The rationale of such a surgery is that the nucleus within pediatric cataracts is soft and the lens tissue is mainly composed of soluble proteins. Therefore, it was believed that after discission of the capsule, the effused lens material would be gradually absorbed within the eye over the following weeks and months. However, the large amount of lens proteins that enters into the aqueous humor or the vitreous body might be erroneously recognized as foreign proteins by the immune system, invoking a violent immune response that would lead to a series of serious complications like refractory uveitis and secondary glaucoma. As a result, most patients ended up blind. Hence, this type of surgery was abandoned.
-
1.
Anterior discission
An incision was made on the anterior capsule using various techniques so as to disperse the lens material into the aqueous humor to be gradually absorbed.
-
2.
Posterior discission
The posterior capsule was incised from the rear of the lens to disperse the lens tissue into the vitreous body to be better absorbed.
-
3.
Through-and-through discission
Both the anterior and the posterior capsules were incised so as to disperse the lens proteins into both the aqueous humor and the vitreous body in the hope of promoting complete absorption.
7.1.2 Optical Iridectomy
The serious complications of pediatric cataract discission prompted ophthalmologists to consider a “safer” surgical method, and thus, optical iridectomy came into being. Optical iridectomy was used for the treatment of lamellar cataract, nuclear cataract, and anterior or posterior polar cataract when the opacity was small and located at the visual axis with peripheral transparent areas and visual improvement after pupil dilation. Optical iridectomy aimed to improve vision by allowing light to pass through the peripheral transparent areas while keeping the lens intact [3]. According to the extent of resection, optical iridectomy could be divided into the following three types:
-
1.
Local iris sphincterectomy
The purpose of local iris sphincterectomy was to dilate the pupil, and thus, the amount of light that enters the pupil could be increased. The surgery was suited to small cataracts that were centrally located. During a local sphincterectomy, the pupillary margin of the iris was grasped and pulled out with forceps through an incision at the corneal limbus, and a 1-mm-long piece of iris was resected with scissors. Then, the remaining iris was repositioned in the eye, giving formation of a semilunar notch in the iris (Fig. 7.1a).
Fig. 7.1 
Schematic diagram of optical iridectomy. (a) Local iris sphincterectomy. (b) Medium-width iridectomy. (c) Segmental iridectomy
-
2.
Medium-width iridectomy
The indication of a medium-width iridectomy was the same as that of sphincterectomy, but the resected area was larger (Fig. 7.1b).
-
3.
Segmental iridectomy
Segmental iridectomy, also known as sector iridectomy, involved an even larger area of resection compared with the former two approaches. It would remove a complete sector of the iris tissue, including both dilator and sphincter (Figs. 7.1c and 7.2).
Fig. 7.2 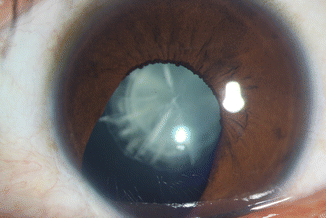
Slit-lamp microscopic image of segmental iridectomy in a 16-year-old boy


Optical iridectomy was previously considered to have the following advantages: (1) The surgical techniques were relatively simple and safe. (2) As the lens was left intact, the postoperative inflammatory response was mild, which might be associated with a much lower incidence of secondary membranes and glaucoma. (3) Accommodation was preserved after the surgery. However, the surgery also had several important limitations, which included: (1) The light came from the off-axis area, resulting in poor imaging quality; thus, the postoperative visual results in most pediatric patients were not satisfactory. (2) The barrier function of the iris was damaged during the surgery, and it would be difficult to perform subsequent operations and optic corrections in the future. (3) It was of poor efficacy in treating unilateral cataracts. (4) It was futile in cases of total cataracts. For these reasons, optical iridectomy was abandoned as well.
7.1.3 Linear Cataract Extraction
In the first half of the twentieth century, the procedure of linear cataract extraction was proposed based on surgical principles of discission. During the surgery, pressure was exerted on the surface of the cornea with a surgical device after cataract discission. In the meantime, irrigation was performed to flush out lens materials from the anterior chamber through the corneal or scleral incision [4]. This surgical technique had undergone many modifications. The removal of lens substance with irrigation was sometimes performed at the same time as the discission/needling procedure (one-stage procedure) or after about a week later (two-stage procedure). Compared with discission/needling alone, linear cataract extraction was associated with lower incidences of postoperative inflammatory reaction, secondary membranes, and secondary glaucoma. However, most pediatric patients still ended up blind, and this technique was also abandoned.
7.1.4 Cataract Aspiration
In the early 1960s, cataract aspiration, a more effective approach to removing the lens material than anterior chamber irrigation, was adopted and continually modified by pediatric ophthalmologists [5]. This technique involved an anterior capsulotomy approximately 2 mm in diameter and aspiration of the lens material with a syringe through the capsulotomy, leaving most of the lens capsule intact. Limitations of cataract aspiration were as follows: (1) The cortex removal was usually incomplete; (2) the collapsed capsular bag and fibrous adhesion of anterior and posterior capsule provided a scaffold for lens fiber regeneration, often resulting in a thick secondary membrane. Although the procedure of cataract aspiration alone is no longer employed, it did lay the foundation for cataract irrigation and aspiration.
7.1.5 Intracapsular Cataract Extraction
As the surgical approaches that preserve the lens capsule would inevitably lead to secondary opacification of the posterior capsule, intracapsular cataract extraction, previously performed only in adults, was also conducted in pediatric patients. However, because the zonule of pediatric patients was resilient and the surgery gave rise to multiple complications, this surgical approach did not find acceptance among pediatric ophthalmologists [5].
7.1.6 Cataract Irrigation and Aspiration
Restoring transparency of the visual axis was the principal purpose of pediatric cataract surgery. In the mid-1960s, a double-barreled cannula was introduced, which was a critical breakthrough in the development of cataract extraction. The dual irrigation and aspiration technique, especially after the introduction of phacoemulsification, enabled the ophthalmologists to maintain the anterior chamber depth during cataract aspiration, which made the removal of the lens material safer, more complete, and more effective. At present, cataract irrigation and aspiration are among the most favored surgical techniques for pediatric cataract extraction.
-
1.
Manual irrigation and aspiration
The irrigation and aspiration of the lens material were conducted manually with a double-barreled cannula (Fig. 7.3). The cannula needle was mounted on a 5 ml syringe, which was filled with 1–2 ml of balanced salt solution (BSS). Then, the lens cortex, after being sucked onto the needle and gently pulled to the middle of the anterior chamber, was aspirated with the cannula.
Fig. 7.3 
A double-barreled cannula
-
2.
Automated irrigation/aspiration handpiece
The invention of phacoemulsification and the application of the automated noncutting irrigation/aspiration handpiece (Fig. 7.4a) made it possible to maintain the anterior chamber depth, increase the efficiency in removing the lens material with greater suction, and reduce frequency of surgical instruments entering into the anterior chamber. When these two techniques were incorporated with tunnel incision and continuous curvilinear capsulorhexis, most of the surgical maneuvers could be completed within the capsular bag, this leading to less disturbance of intraocular tissues, much lower incidences of postoperative inflammation and complications, and subsequently improved surgical outcomes greatly (Fig. 7.4b).
Fig. 7.4 
(a) An automated irrigation/aspiration handpiece. (b) Irrigation/aspiration of the lens cortex with an automated irrigation/aspiration handpiece


7.1.7 Lensectomy with Anterior Vitrectomy (LAV)
In the 1970s, the automated vitrector (Fig. 7.5a) was introduced into pediatric cataract surgery. The thick and gummy lens material found in children is more easily and efficiently aspired using this instrument as opposed to using a double-barreled cannula. Moreover, posterior capsulotomy and anterior vitrectomy (Fig. 7.5b) could also be performed at the same time, which lower the incidence of reopacification of the visual axis to some extent [6]. There are two approaches for LAV. One is through the pars plana, and it is a more efficient approach in removing the lens material. Since the operation is performed in the posterior chamber and the vitreous, it is associated with lower risks for endothelial loss of the iris and cornea. The other approach is through the limbus, and it is a more familiar surgical technique for anterior segment surgeons despite its lack of advantages compared to the pars plana approach. Apart from cataract irrigation and aspiration, LAV is another surgical technique that is still in use for pediatric cataract extraction.

(a) An automated vitrectomy handpiece. (b) Anterior vitrectomy with an automated vitrectomy handpiece
7.1.8 Phacoemulsification
In the 1970s, phacoemulsification was used in pediatric surgery for the first time [7]. Since a hard nucleus is seldom found in pediatric patients, the lens material can be eliminated merely by aspiration in most cases. If any hard material is encountered, ultrasound is available to help remove it. Moreover, the larger aspiration port of the phacoemulsification handpiece is more efficient than that of the irrigation/aspiration handpiece in aspirating the lens material. Phacoemulsification has become one of the routine options for pediatric cataract surgery due to its high efficiency and safety (Fig. 7.6).

(a) A phacoemulsification handpiece. (b) Phacoemulsification cataract extraction surgery
7.1.9 Pediatric Intraocular Lens Implantation
For pediatric patients with cataract, clearing the visual axis is just the beginning for restoring visual function, and the postoperative correction of refractive errors of the aphakic eyes is equally important. Intraocular lens (IOL) implantation is an ideal approach for aphakic correction in pediatric patients, and the details of the implantation will be elaborated in Chap. 15 (Fig. 7.7).

Intraocular lens implantation. (a) A foldable IOL is inserted into the eye. (b)The IOL unfolded in the capsular bag
To sum up, throughout the evolutionary history of pediatric cataract surgery, we have come to know more about the anatomy and physiological characteristics of pediatric eyes, the development of the eye and vision, and the mechanisms for the occurrence of surgical complications. Meanwhile, the surgical instruments and techniques have also improved. Now, pediatric cataract surgery is safer, less invasive, and associated with fewer complications than before.
7.2 Conservative Treatment for Pediatric Cataract
In the 1960s, Chandler and some researchers found that the surgery for many pediatric patients with congenital cataract usually resulted in poorer visual acuity or even vision loss. Therefore, they proposed that cataract surgery should not be recommended unless preoperative vision was extremely poor [8, 9]. With the development of medical technology, a consensus has been reached among ophthalmologists that the surgical treatment for pediatric cataracts that greatly hinder the development of visual function should be conducted as soon as possible to clear the visual axis and restore visual function [10–12]. In children with cataracts that are not dense (e.g., lamellar cataract) or not on the visual axis, follow-up observations are advisable since it preserves accommodation and a series of problems like secondary opacification can be avoided. In children with unilateral cataract, anisometropia should also be taken into consideration apart from accommodation; therefore, the treatment should tend to be more conservative. Moreover, for premature infants and children with systemic dysplasia or disorders, general anesthesia poses a high risk. In these patients, systemic abnormalities should be treated before the elective cataract surgery.
7.2.1 Indications of Conservative Treatment for Pediatric Cataract
Even though there is still no solid evidence for indications of conservative treatment of pediatric cataract, some consensus has been reached in clinical practice. They agree that the choice of treatment should be mainly based on the location, degree, and range of the lens opacity. Now, there are certain examination devices that can perform quantitative analysis of the range and degree of lens opacity to provide more scientific guidance for clinical practice (Fig. 7.8).

Quantitative evaluation of the degree of lens opacity by Pentacam
7.2.1.1 Nondense Lens Opacities on the Visual Axis
When nondense lens opacity (Fig. 7.9) is not dense enough to obscure the light passing through the visual axis and fundus observation, conservative treatment can be adopted. With optical correction and visual training, the visual function can be improved in children with localized nondense lens opacity. Meanwhile, the surgery-induced problems like loss of accommodation and anisometropia can be avoided.

Nondense lens opacity. (a) A representative image of nondense lens opacity from slit-lamp retroillumination. (b) An image of localized nondense lens opacity from slit-lamp oblique illumination
7.2.1.2 Off-Axis Lens Opacities
For opacities that do not involve the visual axis (Fig. 7.10), conservative treatment should be the first consideration. Even though the off-axis lens opacity is obviously dense, light can still pass through the visual axis and reach the retina, thus leading to no significant influence on the development of visual function. However, for opacity which makes lens shape abnormity, such as pyramidal cataract, surgical treatment will be required in case of irregular astigmatism that cannot be corrected.

Off-axis lens opacity. (a) Off-axis posterior subcapsular opacity. (b) Retro-illumination view of off-axis lens opacity
7.2.1.3 Dense Lens Opacities on the Visual Axis with a Diameter Smaller than 3 mm
For dense opacity on the visual axis with a diameter smaller than 3 mm, a cautious assessment should be performed before making a decision on the treatment strategy. When the opacity has no significant effect on the visual function and the child has good fixation ability, but without strabismus and nystagmus, conservative treatment, like dilation of the pupil and refractive errors correction, can be conducted, and the patients should also be put under long-term observation (Fig. 7.11). Conversely, for children with poor vision, inability of fixation, and presentation of strabismus and nystagmus, after careful refraction and fundus examinations to rule out poor unaided vision caused by refractive errors or fundus diseases, surgery should be performed as soon as possible.

Dense lens opacity on the visual axis with a diameter less than 3 mm. (a) Dense anterior capsular opacity. (b) Retro-illumination view of a dense opacity on the visual axis
7.2.1.4 Intolerance of General Anesthesia Due to Systemic Status
Pediatric cataract can be one of the clinical manifestations of a certain syndrome and is often associated with genetic or systemic disorders [13]. For infants with systemic abnormities, there are many complex and uncertain factors in their surgery and prognosis. As operations on young children all need to be performed under general anesthesia, the poor tolerance of the newborn, premature babies, and infants with immature vital organ system renders them vulnerable to anesthesia accidents that might be life-threatening [14, 15]. For these patients, life is the foremost priority over elective cataract surgery. Therefore, the systemic status of pediatric patients should be cautiously evaluated before surgery to rule out surgical contraindications. If a surgery is not performed in the short term, conservative treatments should be conducted first.
7.2.2 Conservative Treatment for Pediatric Cataract
7.2.2.1 Dilation of the Pupil
If an opacity in the visual axis is small (less than 3 mm in diameter) and not dense, like a nuclear cataract or an anterior polar cataract, dilation of the pupil can be carried out to let more light pass through the transparent area of the lens to facilitate visual development in pediatric patients [16, 17]. Commonly used mydriatics include compound tropicamide 0.5–1 %, cyclopentolate 1 %, and atropine ointment. Glare and reduced accommodation may occur after dilation. Glare can be managed by wearing polarized or photo-gray spectacles to avoid strong light stimulation, and reduced accommodation can be controlled by wearing double-focus spectacles to aid near vision for reading. Moreover, mydriatics can also be prescribed to pediatric patients with cataracts that progress slowly or those who have postponed surgery due to various considerations like intolerance of general anesthesia, systemic risk factors, and social and economic issues.
7.2.2.2 Correction of Refractive Errors
Since the refractive status of pediatric patients is constantly changing along with eye development, pediatric cataracts are often associated with ametropia. Therefore, when conservative treatment is being conducted, refraction examination is carried out every 3–6 months to adjust the spectacle/contact lens prescription so as to avoid ametropic amblyopia. Due to poor compliance by pediatric patients during a vision examination, a retinoscopy can be performed under sedation or general anesthesia to determine refractive changes so as to timely adjust the prescription for either spectacles or contact lenses. As anisometropia often occurs in young children with unilateral cataract, contact lenses can be adopted under this circumstance to avoid the size difference between binocular retinal images induced by spectacles.
7.2.2.3 Treatment of Amblyopia
Ametropia and anisometropia as well as form deprivation are important causes for amblyopia in children with congenital cataracts [18, 19]. The therapeutic regimens should be tailored to the needs of these patients. For those with unilateral cataract, the affected eye is more susceptible to amblyopia due to competitive inhibition. Therefore, a well-designed occlusion therapy based on effective refractive correction is an important method of managing amblyopia in these children. Moreover, physiotherapies like He-Ne laser, pulse red light stimulation, afterimage stimulation, Haidinger’s brush (light brush) stimulation, and grating stimulation can also be part of the personalized treatment of amblyopia.
7.2.2.4 Regular Follow-Up
The key to successful treatment of pediatric cataract is early diagnosis and decision of surgical timing, since advancing lens opacity is likely to develop progressive vision impairment and other complications like amblyopia, strabismus, and nystagmus. As the cataractous eyes are still developing and especially their refractive status is constantly changing with the increase of the axial length [20], their refractive status should be regularly assessed in order to adjust the eyeglass prescription along with amblyopia management. Therefore, regular follow-up is of great significance during conservative treatment. However, children with congenital cataracts used to have a poor follow-up adherence in clinical practice. The statistics of Zhongshan Ophthalmic Center of Sun Yat-sen University shows that adherence to follow-up drops sharply as follow-up visits increase. It is estimated that attendance to visits drops from 87.8 to 33.3 % from the first visit to the fourth. In 2010, in order to improve the poor follow-up adherence, Zhongshan Ophthalmic Center of Sun Yat-sen University first provided the short message service based on the patient database to remind the parents of the pediatric patients of the follow-up visits in addition to patient education and explaining to parents the importance of scheduled visits. With a large-scale, randomized controlled trial, it has been found that, compared with the standard clinical practice of reminding parents of the scheduled visits, the short message reminder can effectively improve adherence by the parents and attendance, which has led to better visual prognosis [21]. In light of the introduction and popularization of smartphones, the center independently developed and established the follow-up system for pediatric patients with congenital cataract in 2014 (Fig. 7.12), which has, for the first time, made it possible to make accurate visit arrangements on the basis of the follow-up database of the pediatric patients. With this system, doctors can be reminded via the doctor app on cell phones of their daily scheduled visits. Meanwhile, notifications of upcoming visits can be sent via the patient app to parents in advance, and parents can also obtain the results of each visit promptly. This has led to better compliance by parents for follow-up treatment.

The follow-up system for pediatric cataract patients at Zhongshan Ophthalmic Center of Sun Yat-sen University. This system consists of a computerized follow-up platform and two mobile apps. Both the doctor app and the patient app can be downloaded from the Apple App Store or various Android stores
7.2.3 Observation Indexes and Adjustment of Treatment Regimens in Conservative Treatment
Choosing conservative methods to treat pediatric cataract is a prudent decision after weighing the pros and cons. As a congenital cataract may be stationary or progressive, and the visual function of the pediatric patient is in close relation with the degree of lens opacity, regular follow-ups and timely adjustment of the treatment regimens are an indispensable link in conservative treatment. The follow-up system for pediatric cataract patients at Zhongshan Ophthalmic Center of Sun Yat-sen University collects and documents personal information and all follow-up data of each pediatric cataract patient (Fig. 7.13). For cataractous children under conservative treatment, we need to note the following observation indexes so as to evaluate the efficacy of the treatment and adjust the treatment strategies in a timely manner.

(a) Basic information of pediatric patients in the follow-up system at Zhongshan Ophthalmic Center. (b) Visual acuity, ocular alignment, anesthesia, and intraocular pressure of each patient are collected and documented using the follow-up system
7.2.3.1 Changes of Lens Opacity
Although most congenital cataracts are relatively stationary, it is also likely that the lens opacities will progress in a few cases. Therefore, observation of the lens opacities during follow-up visits should be prioritized. If possible, slit-lamp photographs of the anterior segment should be taken with the pupil dilated on each visit so as to sequential image data of the lens, which will in turn facilitate the comparative analysis of the progression of lens opacity (Fig. 7.14). When a cataract is found to be progressive through several visits, especially when its diameter increases to 3 mm or above and the opacity is close to the posterior pole and/or on the visual axis, surgery should be scheduled without delay [22–24].

Changes in degree of lens opacity. (a) and (b) Peripheral vacuolar lens opacity observed in a boy when he was 2 months old. (c) Total cataract developed when the same patient was 5 months old
7.2.3.2 Visual Function
During conservative treatment, examination of the visual function is of great significance in assessing the progression of cataract, for it can clearly demonstrate whether the visual function is altered due to the lens opacity. However, poor compliance in pediatric patients, especially infants, makes it challenging to assess their visual function, particularly their visual acuity. In children with bilateral cataracts, the effect of the cataracts on visual function can be judged from their daily activities. But in children with unilateral cataracts, there are few relevant visual symptoms. The assessment should be carried out with occlusion of the unaffected eye. In addition to the subjective visual acuity test, assessment of visual function can also include objective procedures like fixation test, visual electrophysiological examination, and preferential looking acuity cards. Currently, the most commonly used preferential looking acuity card in clinical settings is the Teller acuity card, which is used to measure the grating acuity of infants based on the preferential looking theory. This procedure has gained wider and wider acceptance among pediatric ophthalmologists and is often used in multicenter clinical trials of congenital cataract to evaluate the visual status of nonverbal infants [25].
7.2.3.3 Ocular Alignment, Fixation, and Fix and Follow
Whether the lens opacity has affected the visual acuity can be inferred by examining ocular “fix and follow” behavior of the pediatric patients of the pediatric patients. Bilateral examination should be performed before unilateral assessments in fix and follow. Fix and follow behavior is usually well developed in a normal infant that is 4 months old. However, if nystagmus and inability of fixation are present in a 4-month-old, significant form deprivation might have occurred. Once strabismus and nystagmus progress, amblyopia will become irreversible, and conservative treatment should be replaced by surgery as soon as possible. On the other hand, for children without strabismus and nystagmus, frequent follow-up observations should be kept, and ocular alignment, as well as fixation ability, should be documented during every follow-up visit.
7.2.3.4 Refractive Status
Effective correction of refractive errors is essential for the conservative treatment of pediatric cataract, and accurate refractive examination is fundamental to refractive correction. Therefore, it is advised that objective refraction be conducted every 3–6 months to monitor the changes of the refractive status. If the change in spherical is over 2.0 D or the change in cylinder is over 1.0 D, the refractive prescription of the pediatric patients should be adjusted.
It is still controversial whether the conservative treatment of pediatric cataract should be chosen. The current few consensus are mainly based on clinical experience, and there is a lack of guidelines based on rigorous studies. In general, when deciding whether surgery should be adopted, we must follow the principle of giving priority to life and also take into consideration the location, range, and severity of the lens opacity. Meanwhile, in developing countries, medical equipment, health-care quality, and skills of the surgeons in the resident regions of the pediatric patients should also be considered. Therefore, when choosing the treatment regimen for pediatric cataract, ophthalmologists should carry out a comprehensive evaluation and use integrated thinking to find a balance between timely surgery that removes form deprivation and conservative treatment that avoids serious complications caused by surgery.
7.3 Prospect: Lens Regeneration for Treatment of Infantile Cataracts
In the current clinical practice of infantile cataract treatment, the key techniques of the most common surgical procedure include removal of the cataract through a large anterior continuous circular capsulorhexis (ACCC), additional posterior capsulotomy, and anterior vitrectomy (Fig. 7.15a), which is followed by optic correction through IOL implantation, aphakic spectacles, or contact lenses. However, surgical complications, e.g., visual axis opacification, frequently occur among infant patients. Furthermore, other challenging issues including refractive correction of developing eyes and secondary glaucoma may give rise to a worse outcome. The current technique of capsulorhexis for infantile cataract surgery involves creating a large opening of a 6-mm diameter at the center of the anterior capsule, which leaves a broad wound area and destroys a significant amount of lens epithelial cells (LECs) (Fig. 7.15a). To address these issues and to facilitate lens regeneration, our team of investigators at Zhongshan Ophthalmic Center (Yizhi Liu’s team) created a new technique of capsulorhexis [26]. We first reduced the diameter of the capsulorhexis opening to 1.0–1.5 mm, which leaves a minimal wound of 1.2 mm2 on the capsule, only 4.3 % of the size of the wound created by the current technique. Furthermore, we moved the location of the capsulorhexis to the peripheral capsule instead of the central zone (Fig. 7.15b). A 0.9-mm phacoemulsification cannula was applicated to eliminate the lens materials and/or cortical opacities. These changes introduce substantial advantages. First of all, the technique greatly decreases the size of surgical injury, which is associated with a lower incidence of postoperative inflammation and much earlier healing. In addition, the scarring tissue formed after wound healing will be away from the visual axis, which provides increased visual axis transparency. Most importantly, a nearly intact transparent lens capsule and LECs are preserved. They possess regenerative potentials and are the critical prerequisites for the regeneration of a natural crystalline lens. We finished a clinical trial in children with cataracts who were ≤ 2 years to examine whether we could regenerate lenses in human eyes via minimally invasive surgery. Our approach is conceptually different from current practice of surgery in that endogenous LECs are preserved to a maximum as well as their natural environment and the regenerated lenses are able to improve visual functions [26].

(a) Diagrams of the traditional technique for pediatric cataract surgery. The routine anterior continuous curvilinear capsulorhexis (ACCC) for children creates an opening of a 6-mm diameter at the center of the anterior capsule, eliminates the lens epithelial cells (LECs) beneath it, and results in a large wound area of 28 mm2. The scars formed afterward frequently lead to postoperative visual axis opacification (VAO). In these cases, PCCC and anterior vitrectomy are usually performed during follow-up visits. (b) The new minimally invasive technique. The diameter of capsulorhexis is reduced to 1.0–1.5 mm, resulting in a small wound area of 1.2 mm2. The location of capsulorhexis is at the periphery of the lens capsule
7.4 Summary
Treatment of pediatric cataracts falls into two categories, i.e., surgical and conservative. Pediatric cataract surgery has been evolving for nearly two centuries. With growing knowledge of anatomical and physiological characteristics of pediatric eyes, mechanisms of visual development and surgical complications, as well as constant improvement of surgical techniques and devices, pediatric cataract surgery is becoming safer, less invasive, and associated with fewer complications. Indications and planning of conservative treatment are based on location, severity and size of the lens opacity, as well as the visual function and systemic condition of the affected child.
References
Taylor D. The Doyne lecture. Congenital cataract: the history, the nature and the practice. Eye. 1998;12:9–36.
Ziegler SL. Complete discission of the lens by the V-shaped method. JAMA. 1921;77:1100–2.
Foster J. Optical iridectomy, indications, method and value. Br J Ophthalmol. 1932;16(8):476–84.
Cordes FC. Linear extraction in congenital cataract surgery. Trans Am Ophthalmol Soc. 1960;58:203–18.
Ryan SJ, Blanton FM, von Noorden GK. Surgery of congenital cataract. Am J Ophthalmol. 1965;60:583–7.
Parks MM. Posterior lens capsulectomy during primary cataract surgery in children. Ophthalmology. 1983;90:344–5.
Hiles DA, Hurite FG. Results of the first year’s experience with phacoemulsification. Am J Ophthalmol. 1973;75:473–7.
Chandler PA. Surgery of congenital cataract. Trans Am Acad Ophthalmol Otolaryngol. 1968;72(3):341–54.
Chandler PA. Surgery of congenital cataract. Am J Ophthalmol. 1968;65(5):663–74.
Birch EE, Stager DR. The critical period for surgical treatment of dense congenital unilateral cataract. Invest Ophthalmol Vis Sci. 1996;37(8):1532–8.
Taylor D, Wright KW, Amaya L, et al. Should we aggressively treat unilateral congenital cataracts? Br J Ophthalmol. 2001;85(9):1120–6.
Zetterstrom C, Lundvall A, Kugelberg M. Cataracts in children. J Cataract Refract Surg. 2005;31(4):824–40.
Merin S, Crawford JS. The etiology of congenital cataracts. A survey of 386 cases. Can J Ophthalmol. 1971;6(3):178–82.
Williams AR, Conroy JM. The anesthetic management of the pediatric strabismus patient. J AAPOS. 1998;2(2):113–5.
Pun MS, Thakur J, Poudyal G, et al. Ketamine anaesthesia for paediatric ophthalmology surgery. Br J Ophthalmol. 2003;87(5):535–7.
Drummond GT, Hinz BJ. Management of monocular cataract with long-term dilation in children. Can J Ophthalmol. 1994;29(5):227–30.
Choi J, Kim JH, Kim SJ, et al. Clinical characteristics, course, and visual prognosis of partial cataracts that seem to be visually insignificant in children. J AAPOS. 2012;16(2):161–7.
Ceyhan D, Schnall BM, Breckenridge A, et al. Risk factors for amblyopia in congenital anterior lens opacities. J AAPOS. 2005;9(6):537–41.
Denion E, Dedes V, Bonne M, et al. Importance of occlusion therapy for amblyopia in partial unilateral congenital cataracts that are discovered late. J Fr Ophtalmol. 2004;27(9 Pt 1):1017–24.
Gordon RA, Donzis PB. Refractive development of the human eye. Arch Ophthalmol. 1985;103(6):785–9.
Lin H, Chen W, Luo L, et al. Effectiveness of a short message reminder in increasing compliance with pediatric cataract treatment: a randomized trial. Ophthalmology. 2012;119(12):2463–70.
Hamill MB, Koch DD. Pediatric cataracts. Curr Opin Ophthalmol. 1999;10(1):4–9.
Nelson LB, Wagner RS. Pediatric cataract surgery. Int Ophthalmol Clin. 1994;34(2):165–89.
You C, Wu X, Zhang Y, et al. Visual impairment and delay in presentation for surgery in chinese pediatric patients with cataract. Ophthalmology. 2011;118(1):17–23.
Lambert SR, Buckley EG, Drews-Botsch C, et al. A randomized clinical trial comparing contact lens with intraocular lens correction of monocular aphakia during infancy: grating acuity and adverse events at age 1 year. Arch Ophthalmol. 2010;128(7):810–8.
Lin H, Ouyang H, Zhu J, et al. Lens regeneration using endogenous stem cells with gain of visual function. Nature. 2016;531(7594):323–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Liu, X., Zhang, X., Ni, Y. (2017). Overview of Pediatric Cataract Treatments. In: Liu, Y. (eds) Pediatric Lens Diseases. Springer, Singapore. https://doi.org/10.1007/978-981-10-2627-0_7
Download citation
DOI: https://doi.org/10.1007/978-981-10-2627-0_7
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-2626-3
Online ISBN: 978-981-10-2627-0
eBook Packages: MedicineMedicine (R0)