
Abstract
Transcranial Doppler (TCD) ultrasound is an essential tool in clinical diagnosis to determine the occurrence of embolism in stroke patients. However, it requires manual attention and the accuracy will deteriorate due to fatigue factor. Instead of depending on human observer as a gold standard to detect the emboli, this study proposes an automated emboli detection system based on three detection methods i.e. time-domain intensity, frequency-domain intensity and time-frequency intensity hybrid. Experimental studies of 240 samples of six data sets were employed. The performance evaluations of each method are measured in term of accuracy percentage and processing speed while human observation is also done as the golden standard for accuracy comparison. The best result is achieved by the time-frequency intensity hybrid method where 90.74 % of the embolic signals and 100 % of the non-embolic signals were successfully identified. The performance of this method is promising as the accuracy achieved by human observation was 87.45 and 100 % for embolic signals and non-embolic signals, respectively.
Access provided by CONRICYT-eBooks. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
In 2014, the World Health Statistics provided by World Health Organization reports that stroke was the third leading cause of death. Despite the improvements of stroke treatments through medical advances, it remains the most important disease for permanent disability and the overall mortality from stroke has been increased from year 2000–2012 [1]. This indicates that the prevention of such disease remains as a serious public health challenge. Stroke is a condition where the brain cannot function normally due to severe restriction or complete cessation of blood flow to the brain cells. It is classified on the basis of its aetiology as either hemorrhagic or ischemic. Hemorrhagic stroke is produced by ruptured blood vessels in the brain while ischemic stroke is mainly caused by the presence of an obstruction in the blood vessels. According to American Stroke Association, ischemic stroke is more commonly appear without warning in 87 % cases of stroke [2]. One of the major complications of ischemic stroke can be caused by a blood clot that forms inside veins or arteries known as embolus. Depending on the severity of the ischemia, the emboli can be either solid or gaseous. These emboli, regardless of the type, might block the blood flow in the cerebral arteries in the brain and result in ischemic stroke.
In recent technology, an implementation of transcranial Doppler (TCD) in detection of emboli has gain the interest among researchers [3]. However, the current technique used requiring the human observer to do online assessment of the stationary patients equipped with the TCD ultrasound equipment which is hectic. Moreover, the ability to select, classify and abstract significance information by human observer is subjective due to his sense. Such methods are often proven to be costly, time-consuming and logically difficult. Hence, an automated detection of embolic signal for stroke prevention automatic has been introduced in this paper and it seems possible to replace the current technique where it provides a promising method for detection and classification of emboli event.
2 Methodology
2.1 Obtaining Data
The TCD was employed to represent the blood flow simulation of virtual patients for database collection. For each patient, 20 embolic signals and 20 non-embolic signals has been recorded from TCD simulator. The length of each signal is approximately around 10 s and total of 240 videos is saved for the different types of patients from different age groups which are 25 year-old male, 25 year-old female, 40 year-old female, 50 year-old male, 65 year-old male and 65 year-old female.
2.2 Automated Emboli Detection Method
Time-Domain Intensity. In this method, several steps are considered. The first step is framing the raw TCD data such that only emboli that exist in certain points of the signal can be evaluated at one time in short portion of the signal. Consequently, is the intensity of each frame is calculated by Eq. (1):
where A is amplitude of the signal, \( t_{start} \) is starting time of the frame and \( t_{end} \) is ending time of the frame. Next, the background blood flow intensity is calculated by using Eq. (2) so that it can be used as a reference level:
where \( I_{i} \) is intensity of frame index, i and n is total number of frames. The emboli-blood ratio (EBR) is the ratio of intensity of the frame to the intensity of background blood flow. The EBR of every frame is calculated by Eq. (3):
Finally, the EBR for each frame is compared to the threshold level set. If the EBR of any frame is higher than the threshold, that frame is considered to contain an embolus. In contrast, the frame is a non-embolic signal if the EBR is lower than the threshold. To choose the threshold value, the 120 non-embolic signals extracted earlier is used. The threshold level is set to be a little higher than the highest EBR value of the non-embolic signals.
Frequency-Domain Intensity. Similarly to the previous method, it is started with framing the raw TCD data. Next, each of the frames is multiplied with a window function so that both ends of the signal will fall to zero smoothly where the Hamming, Hanning and Bartlet window [4] are employed in this study. Subsequently, Fast Fourier Transform (FFT) is used to obtain the frequency response of the signal. FFT is given by Eq. (4):
where \( \omega_{N} = e^{ - 2\pi i/N} \), N is number of points of FFT, k is domain index of the FFT and j is index of data from original signal. Finally, the Frequency Components is compared to threshold. Here, two methods is used in order to obtain the reference level for the comparison. The first is interframe comparison where the comparison is done between different frames. The ratio of the magnitude of each frame and the average value of all the frames is found as in Eq. (5):
where K is the total number of frames, F is the frame number, n is the nth frequency component and \( \left| {X\left( f \right)} \right| \) is the magnitude of the frequency component.
The second method is intraframe comparison where the comparison is done only in each frame. The ratio between the frequency components with the highest magnitude and the average magnitude of other frequency components in the same frame is calculated according to Eq. (6):
where N is the total number of frequency component.
Time-Frequency-Domain Intensity Hybrid. There are a few considerations here. First of all, the processing speed is a concern as the processing time for both methods is stack up. Next, the frame length must be set to be the same so that this hybrid method can be applied. The optimum frame lengths for the time-domain intensity method and the frequency-domain intensity method might be different. Thus, a suitable frame length must be found by trying different values and comparing the results.
3 Result and Discussion
For all methods, the key performance area is the accuracy of detection. In this study the testing is done on the 120 embolic signals. In this study, the performance of this system was evaluated based on accuracy and processing time.
3.1 Result of Human Observation
The experiment was repeated thrice and the results of embolic detection based on human observation are tabulated in Table 1. In overall, only 425 out of 486 emboli can be detected and the percentage is 87.45 %. It was not surprising due to some emboli are very small and can be hardly detected. As expected, the performance percentage of human observation was drop over time due to loss of concentration and fatigues built after a long period of observation. This result proved that the ability to select, classify and abstract significance information by human observation is often to be costly, time-consuming and logically difficult.
3.2 Result of Time-Domain Intensity Method
Figure 1a and b show examples of embolic detected by using time-domain intensity method. The red and black lines in Fig. 1a are the threshold level and mean of the EBR, respectively. It was found in Fig. 1b that there was an emboli detected at 8.8 s of the TCD signal as it exceeded the threshold set earlier. On the other hand, Fig. 1c and d show when the EBR value of the signal will be very close to the average with smaller deviation, There is no crossing of threshold so the non-embolic signals were identified correctly.

Examples of embolic and non-embolic detected by using time-domain intensity method. a EBR values of an embolic TCD signal. b Waveform of TCD signal with detected emboli in red. c EBR values of a non-embolic TCD signal. d Waveform of non-embolic TCD signal
3.3 Result of Frequency-Domain Intensity Method
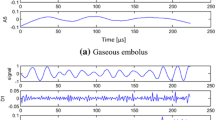
Although the time-domain intensity method is robust in detecting of embolic, this method is unable to perform well when the size of embolus is small (Fig. 2a). In contrast, by applying the frequency-domain intensity method, the embolic frame and non-embolic frame can be seen as in Fig. 2b and c, respectively. The TCD signals are mostly made up of frequency components with frequencies lower than 5 kHz. The magnitude of the frequency spectrum of non-embolic frame has smaller fluctuations and there is no obvious peak (Fig. 2c) while, a peak with high magnitude can be found in embolic frames (Fig. 2b). Moreover, there will be some embolic signal which has high time-domain intensity, but with non-outstanding magnitude in its frequency spectrum as shown in Fig. 3.

a An embolic signal with small embolus and weak time-domain intensity; b frequency spectrum of embolic frame; c non-embolic frame

a An embolic signal high time-domain intensity; b frequency spectrum of embolic frame; c non-embolic frame
3.4 Result of Time-Frequency-Domain Intensity Hybrid Method
In this experiment, the same ratio is used since the optimum frame overlapping ratios for both previous methods were 75 %. The best result was obtained when the frame length of 0.03 s was used (147/162, 90.74 %). From the result, it seems that the time-domain intensity method is the main contributor. However, by employing the frequency-domain intensity method together, the results are improved for all frame lengths. As expected, the processing time is higher than the previous two methods. However, the processing time is still much shorter than the original signal length (Fig. 4).

Emboli detection accuracy and processing time required versus frame length for time-frequency intensity hybrid method
3.5 Overall Performance Summary
Table 2 shows comparison of the detection of embolic and non-embolic signal achieved by using different methods in term of percentage of accuracy and processing time. The results show that except for time-domain intensity method, all methods are able to provide better results than human observation. Furthermore, it was found that all of the processing time is shorter than the actual length of the signal (around 20 min). This proves that the processing speed of all methods is fast enough, thus, it was not be considered while choosing the best method. Hence, it can be concluded that the time-frequency intensity hybrid method is the most suitable method in overall for this project.
4 Conclusion
In this paper, an automated detection of embolic signal for stroke prevention has been studied and successfully implemented. Three methods has been developed i.e. time-domain intensity, frequency-domain intensity and time-frequency intensity hybrid. The results show that the time-frequency domain intensity was the best method with 90.74 % of the embolic signal and 100 % of the non-emboli signal were identified correctly. As the performance of the proposed system was better than the human observation, the objective of developing an algorithm was achieved and the system is suitable for real-time application.
References
World Health Organization (2014) World health statistics 2014. http://www.who.int/gho/publications/world_health_statistics/2014/en/. Accessed 1 Jan 2015
American Stroke Association (2015). Ischemic strokes (Clots) [Online]. American Stroke Association. http://www.strokeassociation.org/STROKEORG/AboutStroke/TypesofStroke/IschemicClots/Ischemic-Strokes-Clots_UCM_310939_Article.jsp. Accessed 1 Jan 2015
Chung EM (2006) Transcranial doppler embolus detection: a primer. Ultrasound 14:202–210
Aydin N, Markus HS (2000) Optimization of processing parameters for the analysis and detection of embolic signals. Eur J Ultrasound 12:69–79
Acknowledgment
The authors would like to thank the financial support provided by FRGS, 203/PELECT/6071266 (USM).
Author information
Authors and Affiliations
Corresponding authors
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer Science+Business Media Singapore
About this paper
Cite this paper
Ibrahim, N.S., Duan, N.Y., Ramli, D.A., Jaafar, H. (2017). Automatic Detection of Embolic Signal for Stroke Prevention. In: Ibrahim, H., Iqbal, S., Teoh, S., Mustaffa, M. (eds) 9th International Conference on Robotic, Vision, Signal Processing and Power Applications. Lecture Notes in Electrical Engineering, vol 398. Springer, Singapore. https://doi.org/10.1007/978-981-10-1721-6_65
Download citation
DOI: https://doi.org/10.1007/978-981-10-1721-6_65
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-1719-3
Online ISBN: 978-981-10-1721-6
eBook Packages: EngineeringEngineering (R0)