
Abstract
Chinese herbal medicine (CHM) has been used for several thousands of years to treat human illness, which makes CHM the best source to provide valuable and unique information for modern drug discovery and development. Development of CHM products as adjunct therapies to augment the efficacy and offset the toxicity of Western medicine is an excellent approach for rapid advancement into US FDA-approved new drugs. Developing CHM products as high-quality dietary supplements must particularly emphasize standardization through qualitative and quantitative quality controls on single herbs and multiple herbs of the prescription formulas by using the most advanced scientific technology, especially toxicity profile testing. A combination of advanced medicinal chemistry and natural products chemistry, coupled with cutting-edge life science technology, will play a very important role for converting CHM products, especially the pure single active principles, through modification and synthesis into clinical trial candidates very efficiently and effectively. This chapter presents ten case studies of promising new drug discovery resulting from CHM-derived products: compounds from Curcuma longa (Jiang Huang), Antrodia camphorata (Chang-ku), Apium graveolens (Han Qin), Momordica charantia (Ku Gua), Monascus purpureus (Hong Chi), Astragalus membranaceus (Huang Chi), Scutellaria decoction (Huang Chin Tang), Eucommia ulmoides (Tu Chung), Ligusticum wallichii (Chuan Chiung), and Lycium barbarum (Kou Chi Tzu).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Chinese herbal medicine (CHM)
- Drug discovery and development
- Disease prevention and treatment
- Medicinal chemistry
- Natural products chemistry
- Traditional Chinese medicine (TCM)
1.1 Introduction
Generations of Chinese people have used Chinese herbal medicine (CHM), the most important medicine of traditional Chinese medicine (TCM), for thousands of years for disease prevention and treatment. CHM and their active principles and derivatives provide a broad and profound base for the discovery of effective and safe dietary supplements, in addition to new medicine for the prevention or treatment of diseases affecting quality of life. The symbiotic relationship between the ancient practice of CHM, with its thousands of years of experience, and the modern technology and scientific advancements of today has proven to be the key to effective new drug discovery and development.
The knowledge base of CHM is both vast and diverse. Chinese medicines are all derived from natural products, with roughly 90 % coming from plants. Approximately 5000 plant species with therapeutic value have been identified, many of them used as Min Chien Yao, or folk drugs. About 500 of them are commonly prescribed by doctors of Chinese medicine based on a series of systemic and self-contained theories (Chung Yao, Chinese Materia Medica). This systematic approach is necessary because most CHM-derived products involve multicomponent processed herbal formulations. Although CHM does not provide the same scale and scope of modern-day clinical trials, they no doubt offer a vast knowledge base from which to gain valuable insights relevant to current chronic health issues. The combination of CHM and modern scientific practices has the potential to lead to both new clinical trial candidates and adjunct therapies for current Western medicine treatments (Lee et al. 2013).
In 2013, the authors detailed several case studies of modern drug discovery from CHM, including ephedrine/pseudoephedrine from Ephedra sinica (Ma Huang), indirubin from Indigofera tinctoria (Qing Dai – Dang Gui Long Hui Wan), and artemisinin from Artemisia annua (Qing Hao) (Lee et al. 2013). It should be noted that Tu Youyou from the China Academy of Chinese Medical Sciences, Beijing, was recognized in 2011 with the Lasker-DeBakey Clinical Medical Research Award and in 2015 together with Drs. Satoshi Ōmura and William C. Campbell, with the Nobel Prize in Physiology or Medicine, based on her outstanding contribution for the discovery of artemisinin in malaria therapy. Tu Youyou is credited with the inspiration and diligence to probe the ancient CHM literature for an applicable solution to malaria, which ultimately led to the identification of artemisinin/qinghaosu as the effective active principle. Dr. Yi Zhao of Guangxi Traditional Chinese Medical University, China, also made a significant contribution with regard to the elucidation of the pharmacological effect, as well as the mechanism of action of artemisinin/qinghaosu as evidenced in his academic papers entitled Studies on Artemisia annua L./Qinghaosu (Zhao et al. 1986, 1987; Zhao 2011). Overall, the discovery of artemisinin serves as the best example of producing a world-class new drug from ancient CHM via modern medicinal chemistry studies.
1.1.1 Current Areas of Interest for CHM-Derived Drugs
Chronic diseases such as diabetes, arthritis, heart disease, high blood pressure, etc. can be debilitating to patients and can drastically alter their quality of life. CHM has the potential to offer solutions to many of these modern chronic diseases. Some of the current areas of interest for scientists focusing on CHM-derived drug discovery are as follows: antioxidant and antiaging activity, blood pressure-lowering effects, hypolipidemic action, blood sugar-lowering effects, antiallergic functions, and antiarthritis properties. While we highlight quite a few CHM-derived drugs in our case studies, there are other notable discoveries concerning the treatment and prevention of these devastating chronic diseases.
In the coming years, CHM will lead to many new clinical trial drug candidates. The ancient practices of CHM combined with modern scientific evidence have clearly demonstrated that CHM can be a promising treatment modality for chronic diseases to greatly improve quality of life for patients. This combination of ancient and modern-day principles may also lead to a higher probability of success and a more efficient scientific process. This chapter presents ten case studies of promising new drug discovery resulting from CHM-derived products: compounds from Curcuma longa (Jiang Huang), Antrodia camphorata (Chang-ku), Apium graveolens (Han Qin), Momordica charantia (Ku Gua), Monascus purpureus (Hong Chi), Astragalus membranaceus (Huang Chi), Scutellaria decoction (Huang Chin Tang), Eucommia ulmoides (Tu Chung), Ligusticum wallichii (Chuan Chiung), and Lycium barbarum (Kou Chi Tzu).
1.2 Bringing TCM to Mainstream
1.2.1 Obstacles for Bringing TCM to Mainstream
Lack of standardization is a major obstacle to the development of CHM as world-class dietary supplements and new medicines. Unless herbal products can be guaranteed to be efficacious and safe with validated quality and consistency, they cannot be patented or tested in clinical trials. Even their commercialization and marketing as dietary supplements are weakened without such assurances. Four issues to be addressed in bringing CHM products into the mainstream pharmaceutical market are as follows: high quality, high consistency, high safety, and high efficacy. Good methods of quality control should be applied at all stages, including plant growth, production, processing, and storage. In addition, the products should be validated as being from the correct plant species, plant strain, and plant part as well as uniform from manufacturer to manufacturer and from batch to batch. The products must be free of toxicity and contaminants (e.g., heavy metals) with all of their constituents characterized. Possible interactions with other drugs must be determined, and controlled clinical trials should be performed to prove efficacy.
1.2.2 Methods for Bringing TCM to Mainstream
Two main areas for development of CHM products are as adjunct therapies to Western medicine and for prevention or treatment of diseases that are difficult to be treated satisfactorily with Western medicine. Strategies for development of CHM-based world-class new drugs should emphasize using medicinal chemistry approaches to study the active principals of CHM and to modify the lead compound into suitable clinical trial candidates. Furthermore, mechanism of action studies on active principles, active extracts, and effective formulas of CHM can provide needed scientific proof and future directions for new drug research. Also, it would be extremely helpful to establish international collaborative platforms for development of CHM-based new drugs.
Two examples of new botanical drugs already approved by the US FDA are Veregen (MediGene, Germany) in October 2006 and Fulyzaq (Salix Pharmaceuticals, USA) in December 2012. These products were indicated for use against human papilloma virus (HPV) and noninfectious diarrhea in adult patients with HIV/AIDS on antiretroviral therapy, respectively. Their major constituents are kunecatechins (component mixture from a green tea extract) and crofelemer (an extract from Croton lechleri), respectively.
A national program for developing world-class new botanical drugs was initiated by the Ministry of Economic Affairs (MOEA), Taiwan, during 2000–2005 (Lee 2015). The seven-person committee (Committee for Promotion of Chinese Herbal Medicine Industry and Technology) received FDA approval for four Investigational New Drug (IND) applications for partially purified Chinese herbal medicine products for clinical trials, established a platform technology to produce high-quality herbal medicine products with cutting-edge methodology for quality control, and founded excellent preclinical and IND-related infrastructures, including good agriculture, laboratory, manufacturing, and clinical practice (GAP, GLP, GMP, and GCP). Both the software and hardware of these infrastructures were set up to international standards (Lee 2015).
Medicinal chemistry is the art of combining chemistry and biology for optimal drug discovery, and these two research areas are complementary, just like yin and yang of TCM. The discovery of new bioactive compounds depends on valid biological assays, and new chemistry can make the discovery of new biological targets possible.
CHM-derived world-class new drugs and high-quality dietary prescriptions can come from three sources: herbal formulas, extract fractions, and single herbs. As mentioned above, the quality control of herbal formulas is critical, while any modification and improvement should be followed by reevaluation of efficacy and toxicity. In all cases, herbal formulas should continue to be used according to the conformation dictated by TCM diagnosis and principles. Both herbal formulas and single herbs from those formulas can be subjected to pharmacological testing as well as bioactivity-directed fractionation and isolation (BDFI) to discover active fraction mixtures and active single natural product lead compounds, respectively. After the structures of the active lead compounds are elucidated, an optimized lead can be pursued through an iterative cycle that includes the design of modified analogs, synthesis of these analogs, bioactivity screening, and analysis of results. Various preclinical studies to discern mechanism of action and other pharmacological properties (solubility, pharmacokinetics, etc.) are important to make sure that a lead is a viable clinical trial candidate. The goals of the lead development process are to improve pharmacological profiles by increasing activity, decreasing toxicity, or circumventing metabolic, pharmacokinetic, solubility, or drug-resistance problems. The following case studies will highlight the rationale, diversity, and strength of these processes as well as introduce several examples of CHM-derived drugs used now or in the future to treat or prevent diseases affecting quality of life.
1.3 Case Studies Highlighting CHM-Derived Drugs Used to Treat/Prevent Diseases Affecting Quality of Life
1.3.1 Curcuma longa (Turmeric)
1.3.1.1 Introduction
Curcuma longa (Chinese: Jiang Huang 薑黃) is a rhizomatous herbaceous perennial member of the Zingiberaceae family. More commonly known as turmeric, it is native to tropical Southeast Asia and now cultivated in the tropical and subtropical regions of the world, especially in India and China. Turmeric has a long historical use as a traditional medicine. In Ayurveda medicine, turmeric is primarily used as a treatment for inflammatory conditions. In TCM, it is used to treat biliary disorders, anorexia, cough, diabetes, wounds, hepatic disorders, and rheumatism. It has also been used as a sinusitis stimulant, aspirant, carminative, emmenagogue, astringent, detergent, and diuretic (Gupta et al. 2015). Besides its medicinal use, turmeric has long been part of the daily diet in Asian countries and has not been shown to cause any toxicity. Turmeric powder and many other extracts from the rhizomes were found to possess versatile bioactivity, including wound-healing, anti-inflammatory, hypolipidemic, cytotoxicity, antiprotozoan, antibacterial, antifungal, and antifertility effects (Chattopadhyay et al. 2004).
1.3.1.2 Chemical Constituents
To date, over 200 compounds have been identified from turmeric. These compounds belong to various structural types including diarylheptanoids (curcuminoids), diarylpentanoids, phenylpropene, phenolic compounds, monoterpenes, sesquiterpenes, diterpenes, triterpenoids, alkaloid, sterols, and fatty acids (Anonymous 1999b).
Curcuminoids with an aryl-C7-aryl skeleton, include curcumin (curcumin I, 1, Table 1.1), demethoxycurcumin (curcumin II, 2, Table 1.1), bisdemethoxycurcumin (curcumin III, 3, Table 1.1), p,p′-dihydroxydicinnamoyl methane, p-hydroxycinnamoyl-feruloylmethane, dihydrocurcumin, etc. Sesquiterpenes include ar-turmerone (4, Table 1.1), a-turmerone (5, Table 1.1), β-turmerone (6, Table 1.1), curlone, etc. Dried turmeric rhizomes usually contain 1.5–5 % essential oils. Compounds 4–6 are the major sesquiterpenes of the essential oils, and these compounds may account for at least 40 % of essential oils of turmeric rhizomes.
The pharmaceutical products of turmeric are dried whole rhizomes, ground turmeric, turmeric oils, turmeric oleoresin, and curcumin. The quality control of turmeric has been thoroughly reviewed (Li et al. 2011). Curcuminoids are the main active compounds. They are primarily accumulated in turmeric rhizomes (3–15 %) with curcumin (1, Table 1.1) as the principal constituent. The contents of curcuminoids in turmeric rhizomes often vary with varieties, locations, sources, and cultivation conditions. According to the Indian Pharmacopoeia in 1996, dried turmeric rhizomes should contain not less than 1.5 % of curcumin (1) (w/w) (India 1996). The Pharmacopoeia of the People’s Republic of China (2005) requires no less than 1.0 % of curcumin (1) content (w/w) in dried turmeric rhizomes (Anonymous 2005). The Thai Herbal Pharmacopoeia recommended that dried turmeric should contain no less than 6 % of turmeric oil (v/w) and 5 % of total curcuminoids (w/w) (Thaikert and Paisooksantivatana 2009). The WHO (World Health Organization) suggests that not less than 4.0 % of volatile oil, and not less than 3.0 % of curcuminoids should be present in turmeric (Anonymous 1999d). The quality control of rhizomes, powders, and extract products was reported through defining and verifying the presence of curcumin (1), demethoxycurcumin (2), and bisdemethoxycurcumin (3) and determining their concentrations by HPLC chromatogram (Li et al. 2011). Turmeric oils and oleoresins with various promising activities have been marketed globally. To control the quality of these products, Ar-turmerone (5), turmerone (6), and β-turmerone (7) are usually employed as chemical markers, for example, a minimum of 40 % of these compounds in turmeric oils and oleoresins are required (Li et al. 2011).
1.3.1.3 Bioactivity
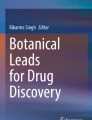
The primary active compound of turmeric is curcumin (1, Table 1.1), which is also responsible for turmeric’s vibrant yellow color. Curcumin was isolated in 1815, obtained in crystalline form in 1870, and ultimately identified as 1,7-bis-(4-hydroxy-3-methoxyphenyl)-1,6-heptadiene-3,5-dione-(1E,6E) (Miłobdzka and Lampe 1910). Chemically, curcumin is a diarylheptanoid, in which two ferulic acid fragments are connected by a methylene bridge. The β-diketone moiety of curcumin can undergo keto–enol tautomerism (Fig. 1.1) and exists entirely in the enol form in both solution and solid phases (Pedersen et al. 1985).

Tautomerism of curcumin and design of different analogs
Extensive studies have indicated that curcumin possesses versatile bioactivity, including anticarcinogenic, immunomodulatory, antioxidant, anti-inflammatory, anti-angiogenesis, anticancer, chemopreventive, anti-Alzheimer’s disease, antithrombotic, antimalarial, anti-rheumatoid arthritis, anti-HIV, wound healing, antihepatotoxic, anti-psoriasis, hypoglycemic, and antihyperlipidemic effects. Thus, curcumin has therapeutic potential against a wide range of diseases, such as inflammatory, lung, neurological, liver, metabolic, autoimmune, and cardiovascular diseases, as well as cancers. Nowadays, around 65 clinical trials are ongoing using curcumin for various diseases, especially for anti-inflammatory, chemoprevention, or cancer therapy (Bairwa et al. 2014; Goel et al. 2008; Hsu and Cheng 2007).
Curcumin has been testified to be nontoxic even at high dosages. To date, no toxicity has been found in any animal and human studies of curcumin. It has been classified as “generally recognized as safe” (GRAS) by the National Cancer Institute (Anand et al. 2007; Sharma et al. 2001). However, several pharmacokinetic and pharmacodynamic studies on curcumin have indicated that it is rapidly metabolized, conjugated in the liver, and excreted in the feces, thus having limited systemic bioavailability (Cheng et al. 2000; Ireson et al. 2001). Research studies have shown that the administration doses as high as 8 g of curcumin per day to human subjects resulted in only an average peak serum concentration of ~1.77 μM of curcumin (Anand et al. 2007; Sharma et al. 2001).
1.3.1.3.1 Curcumin Is a Multi-target Natural Compound
Curcumin’s versatile activities come from its ability to influence multiple signaling molecules. Numerous studies have shown that curcumin can bind directly to many signaling molecules, enzymes, protein kinases, protein reductases, carrier proteins, metal ions, etc. Various biophysical tools were employed to study interactions of curcumin with its targets. These tools are spectrophotometry, Fourier transform infrared (FTIR), circular dichroism (CD) spectroscopy, fluorescence quenching, Förster-type fluorescence resonance energy transfer (FRET), surface plasmon resonance, competitive ligand binding, radiolabeling, site-directed mutagenesis, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), immunoprecipitation, phage display biopanning, electron microscopy, 1-anilino-8-naphthalene-sulfonate (ANS) displacement, and co-localization techniques. Moreover, most of these studies have utilized molecular docking as a computational tool to study the mode and site of binding (Gupta et al. 2011).
Curcumin’s direct targets on signaling molecules and the different forces that bind the curcumin–protein complex have been well reviewed (Gupta et al. 2011). According to this review, the targets of curcumin fall into the following groups:
-
1.
Inflammatory molecules: tumor necrosis factor (TNF)-α, cyclooxygenase (COX)-1, COX-2, human a1-acid glycoprotein (AGP), and myeloid differentiation protein 2 (MD-2);
-
2.
Enzymes: histone acetyltransferases, histone deacetylases, glyoxalase I, xanthine oxidase, proteasomes, sarco (endo)plasmic reticulum Ca2+ ATPase, human immunodeficiency virus type 1 (HIV-1) integrase and HIV-1 protease, DNA methyltransferase 1, DNA polymerase l, ribonuclease A, lipoxygenase, matrix metalloproteinases, and lysozyme;
-
3.
Protein kinases: protein kinase C, viral sarcoma, glycogen synthase kinase-3β, ErbB2 (HER2/neu), and phosphorylase kinase;
-
4.
Protein reductases: thioredoxin reductase and aldose reductase;
-
5.
Carrier proteins: casein, albumin, fibrinogen, β-lactoglobulin, and immunoglobulin;
-
6.
Other proteins: cell survival proteins such as Bcl-2, cytoskeletal proteins such as FtsZ, and homotetrameric proteins such as transthyretin; and
-
7.
Tubulin.
1.3.1.3.2 Chemical Modification Study on Curcumin
With an aim to improve the bioactivity as well as bioavailability while retain a similar safety profile to curcumin, numerous curcumin analogs have been obtained through total synthesis or semi-synthesis (Bairwa et al. 2014; Lin et al. 2006a, b). Based on the structural features of curcumin, the modifications can be grouped into two series. In series I (Fig. 1.1), modifications were focused on the phenyl moiety. Various groups were substituted on the phenyl ring, or the phenyl rings were replaced by various heterocycles. In series II (Fig. 1.1), various linkers were used to connect the two phenyl ring moieties. According to the different type of the linkers, the modifications could be further grouped as: substitutions on the 1,6-heptadiene moiety (IIa, IIb, IIc, Fig. 1.1), forming a heterocycle on the 1,6-heptadiene moiety (IId, Fig. 1.1), altering the conjugation of the 1,6-heptadiene moiety (IIe, Fig. 1.1), and changing the β-diketone to a monocarbonyl moiety (IIf, IIg, IIh, Fig. 1.1). The analogs produced were assayed for their antioxidant, anti-inflammatory, cytotoxic, anti-malarial, anti-HIV, antitrypanosomal, or antileishmanial effects. The results showed that the modifications can affect the bioactivity, and some new derivatives have exhibited improved activity as well as drug profile. However, no common structure–activity relationship (SAR) correlations could be concluded from these modifications.
1.3.1.3.3 Preclinical and Clinical Research on Curcumin and Its Derivatives in the Areas of Inflammation, Chemoprevention, and Cancer
Extensive research conducted on cell cultures, animal models, and clinical trials indicated that curcumin may have potential as a therapeutic agent in inflammatory bowel disease, pancreatitis, arthritis, and chronic anterior uveitis. Research shows that curcumin can interact with numerous molecular targets involved in inflammation. Curcumin modulates the inflammatory response by downregulating the activity of cyclooxygenase-2 (COX-2), lipoxygenase, and inducible nitric oxide synthase (iNOS) enzymes, inhibiting the production of the inflammatory cytokines tumor necrosis factor-alpha (TNF−α), interleukin (IL)-1, -2, -6, -8, and -12; monocyte chemoattractant protein (MCP); and migration inhibitory protein and downregulating mitogen-activated and Janus kinases.
Several clinical trials of curcumin were conducted for various inflammatory conditions, including postoperative inflammation, arthritis, uveitis, inflammatory pseudotumors, dyspepsia, irritable bowel syndrome, inflammatory bowel disease, pancreatitis, and Helicobacter pylori infection. Most studies have been promising and warranted further research on curcumin’s therapeutic value for treatment of inflammatory conditions (Jurenka 2009). For example, studies proved curcumin to be superior to phenylbutazone and placebo in reducing spermatic cord edema, which resulted from surgery for inguinal hernia or hydrocele (Satoskar et al. 1986). In a preliminary double-blind, randomized, controlled trial (RCT), curcumin given at 1,200 mg daily was effective in improving joint swelling, morning stiffness, and walking time (Deodhar et al. 1980). In a clinical trial involving 32 patients with anterior uveitis, after administrating 375 mg curcumin for 12 weeks, visual acuity and aqueous flare improvements and decrease in keratic precipitates were observed (Lal et al. 1999). Curcumin was also used for idiopathic orbital inflammatory pseudotumors (IOIP). In a small study of eight patients with IOIP, 375 mg curcumin three times daily was given for 6–22 months, until complete regression of symptomology was achieved. Patients were followed for 2 years and assessed at 3-month intervals. Only five patients completed the study, but four completely recovered on curcumin therapy (Lal et al. 2000). Moreover, in several clinical trials and a pilot study, curcumin demonstrated anti-inflammatory activity and therapeutic benefit in various gastrointestinal conditions, including dyspepsia, Helicobacter pylori infection, peptic ulcer, irritable bowel syndrome, Crohn’s disease, and ulcerative colitis. Besides the examples mentioned above, numerous clinical trials are ongoing to explore the effect of curcumin on various inflammatory conditions. Jurenka has published an excellent review on this topic (Jurenka 2009).
It is well acknowledged that proinflammatory states are related to tumor promotion. Accordingly, the chemopreventive activity of curcumin has also been widely explored. Preclinical cancer research has shown that curcumin can inhibit carcinogenesis in various cancer types, such as colorectal, pancreatic, gastric, prostate, hepatic, breast, and oral cancers, as well as leukemia, and at various stages of carcinogenesis (Aggarwal et al. 2003). Several animal studies demonstrated that curcumin can inhibit all three stages of carcinogenesis: initiation, promotion, and progression. In the initiation and promotion stages, curcumin modulates transcription factors controlling phases I and II detoxification of carcinogens; downregulates proinflammatory cytokines, free-radical-activated transcription factors, and arachidonic acid metabolism via cyclooxygenase and lipoxygenase pathways; and scavenges free radicals. In the promotion and progression stages of carcinogenesis, curcumin decreases frequency and size of tumors and induces apoptosis via suppression of NF-kB and AP-1 in several cancer types (Chan 1995; Hong et al. 2004; Jurenka 2009; Kawamori et al. 1999; Singh and Aggarwal 1995). Currently, there are at least three ongoing clinical trials exploring the preventive benefits of curcumin as therapy to treat patients with adenomatous polyps at risk for colorectal cancer (Jurenka 2009).
In cancer therapy clinical trials, curcumin alone, as well as combinations with other agents such as bioperine and ashwagandha, was used to treat rectal cancer, pancreatic cancer, multiple myeloma cancer, osteosarcoma, or oral mucositis (Jurenka 2009). For example, one clinical trial indicated that curcumin can stabilize disease progression in patients with advanced pancreatic cancer. Twenty-one patients received 8 g of curcumin daily until the disease progressed. One patient achieved disease stabilization for 18 months (Dhillon et al. 2008).
JC-9 (7, also known as ASC-J9, Table 1.1), a synthetic derivative of curcumin, exhibited potent activity against PC-3 (IC50 1.1 μM) and LNCaP (IC50 1.3 μM) cell lines (Lin et al. 2006a, b). Furthermore, JC-9 was found to be active in vivo against hepatocellular carcinoma and bladder cancer (Ma et al. 2008; Miyamoto et al. 2007). The mechanism of action study indicated that JC-9 enhances androgen receptor degradation (Shi et al. 2009). Another study indicated that JC-9 and its derivatives can overcome EGFR-TKI lung adenocarcinoma drug resistance and reduce EGFR-TKI-induced GI adverse effects (Wada et al. 2015). Therefore, JC-9 is a potential clinical trial candidate for treating prostate cancer, liver cancer, bladder cancer, and other cancers. JC-9 was licensed by AndroScience Corp. (San Diego, CA) and succeeded in phase 2 clinical trials against acne in 2014. Moreover, antiprostate clinical trials with JC-9 are being planned (Itokawa et al. 2008; Lee et al. 2008).
1.3.1.4 Conclusion
Turmeric has been used in traditional medicine since ancient times with a wide spectrum of therapeutic areas. Enormous amounts of data from preclinical and clinical research have confirmed turmeric’s benefits as described in traditional medicine. However, clinical applications of turmeric as a botanical drug can be made only after extensive research on its bioactivity, mechanism of action, pharmacotherapeutics, and toxicity, as well as developing standard QC. Curcumin is the major biologically active constituent of turmeric. In spite of numerous reports showing its putative mechanism(s), multiple molecular targets, and wide range of therapeutic applications, curcumin has not yet been approved for treatment of any human disease, even though it has been reported to be safe for humans at gram dosages. The main obstacle to utilizing curcumin therapeutically is its poor systemic bioavailability. Also, because curcumin can bind to multiple signaling molecules, it is rather difficult to determine which target is causing the desired effect in a certain disease. Therefore, further study should be focused on designing additional different curcumin analogs that will be more effective and better absorbed, as well as on developing a clearer understanding of the actual functional meaning of direct interactions of curcumin with various specific targets. Such discoveries will help to elevate this fascinating natural product as a therapeutic agent for the treatment of human diseases.
1.3.2 Antrodia camphorata
1.3.2.1 Introduction
Antrodia camphorata (syn. Antrodia cinnamomea, Taiwanofungus camphoratus) is a unique basidiomycete fungus of the Fomitopsidaceae family. It is a parasite that affects the inner cavity of Cinnamomum kanehirae Hayata (Lauraceae) (bull camphor tree), which grows only in Taiwan with a distribution in broad-leaved forests at an altitude of 200–2,000 m (Chang and Chou 1995). A. camphorata, also called “Niu-chang-chih” (牛樟芝), “Chang-chih,” “Niu-chang-ku,” or “Chang-ku” in Taiwan, is used to lessen the discomforts caused by alcohol drinking or exhaustion and is believed to be beneficial to preserve human vitality and promote longevity. Moreover, it has been used in TCM to treat a number of illnesses including diarrhea, abdominal pain, hypertension, itchy skin, viral infection, stomatitis, diabetes mellitus, nephritis, proteinuria, liver cirrhosis, hepatoma, influenza, car sickness, heat-related fever, and motion sickness (Geethangili and Tzeng 2011; Wu and Ryvarden 1997). Therefore, in Taiwan, A. camphorata is also called as “ruby in mushroom.”
Production of A. camphorata can occur by gathering mature fruiting bodies of wild A. camphorata, wood or solid-state cultivation, and liquid-state fermentation. Mature fruiting bodies of the wild A. camphorata are now close to extinction due to their very slow growth rate (1 or more years) and overharvesting (Huang et al. 2012).
1.3.2.2 Chemical Constituents
Currently, around 200 compounds have been identified from A. camphorata. These compounds have been summarized in four reviews (Ao et al. 2009; Geethangili and Tzeng 2011; Huang et al. 2012; Lu et al. 2013). Generally, the compounds isolated from A. camphorata include triterpenoids, diterpenoids, monoterpenes, steroids, lignans, benzoquinones, benzenoids, maleic/succinic acid derivatives, fatty acids and their esters, polysaccharides, etc. Terpenoids are the main chemical constituents of fruiting bodies of A. camphorata. Among the over 40 isolated terpenoids, most of them are lanostane (III, Fig. 1.2) and ergostane (IV, Fig. 1.2) triterpenes.

Most common triterpene skeletons found in Antrodia camphorata
1.3.2.3 Pharmacological Effects
Various crude extracts of A. camphorata, such as ethanol/methanol, chloroform, ethyl acetate, and aqueous extracts, have been tested for their pharmacological effects in vivo and in vitro in different modes. These research efforts indicated that A. camphorata possesses versatile bioactivities, including anticancer activity, anti-inflammatory and immunomodulatory effects, inhibition of hepatitis B virus (HBV) replication, antioxidant properties, antimicrobial activity, hepatoprotective effects, prevention of liver fibrosis, neuroprotective activity, antihypertensive effects, vasorelaxation properties, antihyperlipidemic activity, and cardiovascular effects (Ao et al. 2009; Geethangili and Tzeng 2011; Huang et al. 2012; Lu et al. 2013).
Beside the crude extract, various pure natural products from A. camphorata have also been widely studied and found to exhibit cytotoxic, neuroprotective, anti-inflammatory, anti-insecticidal, anti-HBV, and anti-HCV effects. For example, several triterpenoids, such as camphoratins B–F and zhankuic acid A, showed moderate to potent cytotoxicity, with EC50 values ranging from 0.3 to 3 μM against KB and KB-VIN human cancer cell lines. Moreover, camphoratins F and J, as well as zhankuic acid A and their related compounds, were also found to exhibit anti-inflammatory NO production inhibition activity with IC50 values of less than 5 μM and were more potent than the nonspecific NOS inhibitor nitro-l-arginine methyl ester (Shi et al. 2011; Wu et al. 2010).
Antroquinonol (8, Table 1.1), antroquinonol B, antroquinonol C, and related compounds are ubiquinone derivatives isolated from mycelia, fruiting bodies, or both of A. camphorata. Antroquinonol was reported to exhibit cytotoxic activities against cancer cell lines MCF-7, MDA-MB-231, Hep 3B, Hep G2, DU145, and LNCaP with IC50 values ranging from 0.13 to 6.09 μM (Lee et al. 2007). Golden Biotechnology Corp. of Taiwan patented the application of antroquinonol and its related compounds for inhibiting the growth of breast, lung, hepatic, and prostate cancers (Liu et al. 2008). Antroquinonol (Hocena®) has completed a phase 1 study in the USA (https://clinicaltrials.gov/ct2/show/NCT01134016), and a phase 2 study is planned to treat non-small cell lung cancer (https://clinicaltrials.gov/ct2/show/NCT02047344). It was granted Orphan Drug Designation by the US FDA for pancreatic cancer (January 21, 2015), acute myeloid leukemia (April 30, 2015), and hepatocellular cancer (July 23, 2015).
1.3.2.4 Conclusion
The pharmacological effects of an extract or isolates from A. camphorata have been widely studied for decades. However, most studies have been performed in vitro and in vivo with animals. Next, more clinical studies are expected to confirm the therapeutic benefit of A. camphorata. Although over 200 compounds have been isolated, little research regarding modification and synthesis of active compounds has been conducted. Therefore, continued medicinal chemistry study on A. camphorata may help to provide more promising leads for drug development. Also, it is urgent to establish standard quality control and methods for developing the crude extract of A. camphorata as a botanical drug that could be accepted worldwide.
1.3.3 Apium graveolens
1.3.3.1 Introduction
Apium graveolens Linn. (celery, Han Qin, 旱芹, Umbelliferae), belonging to the family Apiaceae, is a common annual herb widely cultivated in temperate zones. Its leaf stalks are consumed as a popular vegetable. In various forms, such as fresh herb, stalk, leaves, seeds, seed oil, and oleoresin, celery is used to flavor foods. Celery stalks have shown a broad bioactivity spectrum, including antihyperlipidemic, antihypertensive, and memory enhancement effects (Anonymous 2009). Its seeds are used for treatment of bronchitis, asthma, and diseases of the liver and spleen (Satyavati and Raina 1976).
1.3.3.2 Chemical Constituents
The chemical constituents of the whole herb are represented by psoralen, bergapten, isopimpinellin, luteolin, apiin, chrysoeriol, apigenin, quercetin, and volatile oils including d-limonene, myrcene, isobutyric acid, valeric acid, 3-isobutylidenephthalide, 3-isovalidenephthalide, and cis-3-hexen-1-yl-pyruvate. Celery seeds contain various bioactive compounds, including phthalides, coumarins, flavonoids, sesquiterpenoids, and aromatic glucosides. The seed oil is a valuable product in both the flavor and fragrance industries. 3-n-Butylphthalide, 3-n-butyl-4,5-dihydrophthalide (sedanenolide), and sedanolide are reported to be the major flavor components of the seed oil. The volatile oils of the leaves were reported to contain octene-4,5-dione, 2-isopropyloxyethane, sabinyl acetate, 1,4-butanediol, seselin, rutaretin, celereoin, celeroside, apiumoside, isoquercitrin, vellein, apiumetin, nodakenin, myristic acid, 8-hydroxy-5-methoxypsoralen, umbelliferone, and nodakenetin (Anonymous 1999a).
1.3.3.3 Bioactivity
Celery has been used as a medicinal plant for its aphrodisiac, anthelmintic, antispasmodic, carminative, diuretic, laxative, sedative, stimulant, and tonic effects. The medicinal parts of the plant are the roots, leaves, and seeds. Products of celery are also used for blood purification, for regulating bowel movements for evacuation, for glandular stimulation, and as a cure for gallstones and kidney stones. Celery seeds are implicated in arthritic pain relief and for treating rheumatic conditions and gout. Celery is also effective at lowering blood pressure due to the 3-n-butyl phthalide constituent, which has been demonstrated to relax the smooth muscles that line blood vessels (Anonymous 1999a).
Various extracts or fractions of celery were reported to possess antioxidant activity, anti-inflammatory effect, hepatoprotective activity, antimicrobial activity, and inhibition of blood platelet aggregation. Coumarins isolated from celery were reported to help prevent free radicals from damaging cells, thus decreasing the mutations that increase the potential for cells to become cancerous (Sowbhagya 2014).
S-(-)-3-n-butylphthalide [S-(-)-3-butyl-1(3H)-isobenzofuranone, S-(-)-NBP, 9, Table 1.1] was isolated from celery seeds. Pharmacological studies indicated that s-(-)-NBP, as well as synthesized (±)-NBP, has anti-ischemic effects. When stroke-prone spontaneously hypertensive rats were pretreated with (±)-NBP, the onset of stroke was delayed, life span was prolonged, and the neurological deficit score was decreased. (±)-NBP was also reported to ameliorate brain edema and blood–brain barrier damage in middle cerebral artery-occluded rats. (±)-NBP may have neuroprotective effects, since it improved mitochondria dysfunction. S-(-)-NBP and (±)-NBP also exhibited an inhibitory effect on thrombus formation in rats (Zhu et al. 2004). (±)-NBP has been developed as an anti-cerebral ischemic drug and has completed or is ongoing in phase 2–4 clinical trials in China (https://clinicaltrials.gov/ct2/show/NCT02149875, NCT01405248, NCT00724724, and NCT02594995). The results from the completed clinical trials confirmed its effect for treatment of mild and moderate acute ischemic stroke. In phase 2 trials, the total rate of efficacy was 70.3 % among the 91 effective cases. Phase 3 trials indicated that, in 282 effective cases, the total rate of efficacy was 63.9 %. In phase 4 trials, among the two groups with 305 and 1,147 effective cases, the efficacy ratios in the two groups were 78.4 % and 78.2 %, respectively. (±)-NBP was approved by the State Food and Drug Administration (SFDA) of China in 2005 for the treatment of ischemic stroke.
1.3.3.4 Conclusion
Celery and the natural products isolated from celery have exhibited great health benefits. The approval of (±)-NBP by the China SFDA for treating ischemic stroke is an excellent accomplishment. Nevertheless, further study on (±)-NBP-related compounds is still needed for meeting the approval from the US FDA, so that the world-class anti-stroke drugs can be obtained.
1.3.4 Momordica charantia
1.3.4.1 Introduction
In TCM, plants with a bitter flavor and cold property have long been used in the treatment of diabetes and high blood sugar (Chen et al. 2015). Momordica charantia (Chinese: ku gua 苦瓜), known as bitter melon or bitter cucumber, is a common edible vegetable, although all parts of the plant have also been used medicinally. The plant is a tropical and subtropical vine belonging to the family Cucurbitaceae, which produces a warty or ridged oblong fruit. Although it is bitter, the rind of the green fruit is often eaten cooked in stir fries in Chinese cooking or curries in Southeastern dishes. When the fruit is fully ripe, the rind is extremely bitter, but the red pith is sweet. In Japanese Kampo medicine, bitter melon is used for the depletion of yin and, thus, to treat yin stages of chronic diseases such as diabetes (Rister 1999). Indeed, the antidiabetic potential of this plant species has gained significant scientific attention (Broadhurst et al. 2000; Chaturvedi 2012; Grover and Yadav 2004; Horax et al. 2010; Hsu et al. 2011; Wang et al. 2012), particularly regarding the hyperglycemic effects of various chemical components.
1.3.4.2 Chemical Constituents
Components of this plant include flavonoids, isoflavones, anthroquinones, glucosinolates, steroidal saponins, glycol alkaloids, cucurbitane triterpenoids (e.g., charantin (10, Table 1.1)), and polypeptides (e.g., polypeptide-p) (Hamid et al. 2015; Hung et al. 2012; Kaur et al. 2016; Medagama and Bandara 2014; Snee et al. 2011; Tan et al. 2008). As many of these compounds have a bitter taste (Drewnowski and Gomez-Carneros 2000), studies have been conducted to determine how to best mask the bitter taste, if wider acceptance and consumption of M. charantia is to be promoted for medicinal value (Snee et al. 2011). The phytochemistry of the plant, particularly regarding antidiabetic constituents, has been well reviewed (Grover and Yadav 2004; Joseph and Jini 2013; Raman and Lau 1996).
1.3.4.3 Bioactivity
Bitter melon has been used as a folk medicine for numerous conditions, including stomach and gastrointestinal disorders (e.g., to treat colic in infants and peptic ulcers in adults as well for carminative, laxative, or purgative effects) (Grover and Yadav 2004). However, in traditional uses and modern medical studies (Joseph and Jini 2013; Raman and Lau 1996), the plant has been mostly appreciated for its ability to relieve diabetes by improving glucose metabolism (Hasan and Khatoon 2012; Leung et al. 2009), although it has also been studied for anticancer, antiviral (including HIV, herpes, polio), analgesic, anti-inflammatory, and hypotensive effects (Grover and Yadav 2004; Snee et al. 2011).
Among the compounds listed above, cucurbitane-type triterpenoids have been linked to AMP-activated protein kinase activity as a possible hypoglycemia mechanism (Tan et al. 2008), while polypeptide-p mimics the action of human insulin and might be used as a plant-based insulin replacement (Paul and Raychaudhuri 2010).
An exciting recent development is the discovery of a potential novel antidiabetic protein. Momordica charantia insulin receptor (IR)-binding protein (mcIRBP) is a novel insulin receptor (IR)-binding polypeptide with a distinct binding site from that of insulin (Lin et al. 2014). However, mcIRBP also enhances glucose uptake in cells and clearance in normal and diabetic mice, likely via stimulation of similar biopathways as insulin and regulation of genes affecting glucose and lipid metabolism (Lin et al. 2014).
1.3.4.4 Conclusion
Momordica charantia offers an alternative treatment to both injectable insulins, the only treatment for type 1 diabetes and current oral type 2 antidiabetic drugs, including sulfonylureas/insulinotropics, biguanides, α-glucosidase inhibitors, thiazolidinediones, and gliptins. Further studies and strictly controlled clinical trials are needed to evaluate thoroughly the potential of mcIRBP to treat diabetes, a life-altering metabolic disease, which can lead to blindness, renal disease, lower extremity amputations, and even death.
1.3.5 Monascus purpureus
1.3.5.1 Introduction
Red mold rice (RMR) is produced from ordinary rice by fermentation with the yeast species Monascus purpureus (Chinese: 紅麴). In East Asia, RMR is used to flavor, color, and preserve food and medicinally to improve blood circulation and digestion, as well as to treat diabetes (Heber et al. 1999; Li 1596).
1.3.5.2 Chemical Constituents
The fermentation process produces various secondary polyketide metabolites (Li 1596; Ma et al. 2000), including monascin (11, Table 1.1), ankaflavin (12, Table 1.1), and several monacolins.
1.3.5.3 Bioactivity
The hypolipidemic and hypocholesterolemic effects of these compounds have been noted for many years (Endo 1979; Lee et al. 2010). Indeed monacolin K (13, Table 1.1) is the same compound now widely marketed as the cholesterol-lowering drug lovastatin. RMR has also been studied for its anti-obesity effects, which have been linked to its lipolytic activity and subsequent prevention of body fat accumulation (hypertrophy and hyperplasia of adipose tissue), as well as mild appetite suppression (Chen et al. 2008). Finally, RMR fermented with M. purpureus strain NTU 568 [found to produce a higher content of the active components (Shi and Pan 2011)] has been developed as a commercial functional food to prevent Alzheimer’s disease (AD) (Lee and Pan 2011a, b).
1.3.5.4 Conclusion
These fermented products hold promise for preventive medicine, particularly decreasing heart disease risk. Continued studies are aimed at identification of the neuroprotective metabolites in RMR, further evaluation of their mechanism of action, and structural modifications to improve pharmacological profiles as potential drugs for neurodegenerative disorders, including AD and Parkinson’s disease (Lin et al. 2015).
1.3.6 Astragalus membranaceus
1.3.6.1 Introduction
The roots of Astragalus membranaceus (Chinese: Huang Chi 黃耆) (known in TCM for sweet flavor, slightly warm property) are used in various TCM formulas to counteract symptoms associated with a deficiency of chi, e.g., low energy, lack of strength, anorexia, slow healing, etc. (Batch 2010). As the authors have previously provided a detailed description of this herb (Lee et al. 2013), this section will focus only on the studies of PG2, an IV injection used to alleviate cancer-related fatigue and improve the quality of life for cancer patients.
1.3.6.2 Chemical Constituents
Polysaccharide immunostimulatory principles were developed as PG2 by Pharmagenesis in the USA and PhytoHealth Corporation of Taiwan based on the initial advice of Dr. K.H. Lee (Lee et al. 1993).
1.3.6.3 Bioactivity
In a randomized, double-blind placebo-controlled phase 2/3 clinical study (https://clinicaltrials.gov/ct2/show/NCT00523107), patients with advanced cancer who experienced moderate to severe cancer-related fatigue (CRF) had a higher response rate when they received PG2 compared with patients who received a placebo (normal saline). This study concluded that PG2 could be effective and safe for managing CRF in advanced cancer patients, without major or irreversible toxicities (Chen et al. 2012). Subsequently, PG2 was approved for clinical use in treating CRF by the Taiwan Department of Health in April 2011, particularly in cancer patients who developed severe fatigue after receiving chemotherapy. In another clinical trial, a combination treatment with PG2 and platinum-based chemotherapy in non-small cell lung cancer patients led to improved quality of life indices, including management of fatigue, nausea, vomiting, pain, and appetite loss (Kuo et al. 2015). Recruitment is currently ongoing for a phase 4 clinical trial (https://clinicaltrials.gov/ct2/show/NCT01720550) to evaluate the use of different doses of PG2 treatment for fatigue improvement in advanced cancer patients who are under standard palliative care in a hospice setting. Currently, all clinical studies have been performed with an IV injectable form of PG2.
1.3.6.4 Conclusion
In addition to the clinical studies, gene expression profiling showed that PG2 product batches were of high quality and consistency as well as functionally equivalent regarding their effects on the immune and hematopoietic systems (Kuo et al. 2015). A bioinformatics-based approach provided a quantitative measurement for the quality and consistency of herbal medicines and revealed new roles (e.g., immune modulation) for PG2 in cancer treatment. In the same study, PG2 and doxorubicin acted synergistically on induced cell death in HL-60 cells, raising the possibility of a novel antitumor function for PG2. Also, clinical trials (http://www.phytohealth.com.tw/upimages/newarrival1121228011612.pdf) are being performed with PG2 in Taiwan for potential use in treating stroke, both hemorrhagic and ischemic.
1.3.7 Huang Chin Tang
1.3.7.1 Introduction
Huang Chin Tang (or Scutellaria decoction) has been used as a Chinese herbal medicine for over 1,800 years to treat various GI issues, including diarrhea, nausea, vomiting, and abdominal cramps, as well as fever and headaches.
1.3.7.2 Chemical Constituents
Huang Chin Tang contains the four herbs shown below in a 3:2:2:2 ratio.
-
Scutellaria baicalensis (Chinese: Huang Qin 黃芩) (common: skullcap): part used – root, main purpose – to regulate digestive and intestinal functions
-
Paeonia lactiflora (Chinese: Bai Shao 芍藥) (common: white peony): part used – root, main purpose – combines with Glycyrrhiza to relax abdominal cramps
-
Glycyrrhiza uralensis (Chinese: Zhi Gan Cao 炙甘草) (common: licorice): part used – root, main purpose – combines with Paeonia to relax abdominal pain and cramps as well as to harmonize all ingredients and diminish side effects due to the more harsh components, such as Scutellaria
-
Ziziphus jujuba (Chinese: Da Zao 大棗) (common: jujube, Chinese date): part used – fruit, main purpose – to stimulate digestive functions
Thus, this Chinese medicine formulation is a complex mixture containing numerous compounds, unlike Western drugs, which usually contain only a single compound. Liquid chromatography and tandem mass spectrometry have been used to identify various chemicals, including flavonoids, triterpene saponins, and monoterpene glycosides, as well as assign them to the four individual herbs from PHY906, a carefully prepared, consistent, quality-controlled formulation of Huang Chin Tang for cancer therapy (Ye et al. 2007). Flavonoids, such as baicalein (14, Table 1.1), are major active compounds from Scutellaria.
1.3.7.3 Bioactivity
While cancer chemotherapeutic drugs can lengthen the life of a cancer patient, their toxicities and side effects can also severely diminish the quality of that life. PHY906 showed promising results in phase 1 clinical trials in 2010 (Saif et al. 2010) and provided relief from chemotherapy-induced gastrointestinal toxicity, especially severe diarrhea. While PHY906 did not affect the initial intestinal DNA damage caused by irinotecan, it did encourage regeneration of the intestinal progenitor or stem cells and several signaling components, ultimately restoring the intestinal epithelium. Other simultaneous action modes were also evident (Lam et al. 2010). Notably, in addition to reducing irinotecan-induced toxicities, PHY906 could potentiate the drug’s anticancer activity and exert favorable actions in multiple cancers treated with numerous chemotherapy drugs acting by different mechanisms (Liu and Cheng 2012). In a 2014 phase 2 clinical trial, a combination of PHY906 and capecitabine, a prodrug of 5-FU, was found to be a viable option for patients with advanced pancreatic cancer treated previously with gemcitabine (Saif et al. 2014). In the small cohort, quality-of-life indices of hand-to-foot syndrome and diarrhea were improved, and median overall survival was extended, especially in two patients with partial responses (69 and 83 weeks) compared with the previously reported 2 months for other second-line salvage therapies (Kang and Saif 2008). In a recently reported study, PHY906 potentiated the anti-hepatoma activity of the drug sorafenib by multiple mechanisms, particularly attraction of macrophages with a higher M1/M2 (tumor rejection) expression (Lam et al. 2015).
1.3.7.4 Conclusion
Based on the studies above, this CHM formula shows great promise as an adjuvant cancer therapy.
1.3.8 Eucommia ulmoides
1.3.8.1 Introduction
Eucommia ulmoides (Chinese: Tu Chung 杜仲) is a unique tree called the hardy or hard rubber tree and originating in central China. The most medically useful plant parts are the stem bark and leaves, used to make Tu Chung tea. This tea is considered to be useful in blood pressure regulation and weight control, as well as to rejuvenate skin elasticity and strengthen the lower back and knees. Eucommia is, thus, known as a “longevity herb” with its continued use thought to slow the aging process by improving body metabolism and strengthening the muscular skeletal system. Eucommia is well known in the traditional medicines of China, Japan, and Korea and is mentioned in the Chinese classic Shennong Bencaojing Yang (1998). It has analgesic (especially for pain in the lower back and knees), tonic (particularly for right kidney yang), and hypotensive actions. Regarding the former action, Eucommia is likely best known as part of the TCM arthralgia remedy Duhuo Jisheng Tang and is used to treat rheumatoid arthritis, rheumatic back pain, and sciatica (Dharmananda 1999, 2000). In most traditional formulations, Eucommia is a relatively minor ingredient in a large combination of herbs, e.g., it is 7 % of Duhuo Jisheng Tang; however, together with Dipsacus asperoides, it is a major component of Duzhong Wan, a TCM for treating lower back pain during pregnancy (Huang et al. 2014).
1.3.8.2 Chemical Constituents
Numerous chemical constituents and pharmacological activities of Eucommia ulmoides have been described (Deyama et al. 2001; Lee et al. 2012). The main chemical components of interest about the traditional use of Tu Chung are iridoid glycosides, including geniposidic acid and aucubin, and lignans, such as pinoresinol glucoside and diglucoside.
1.3.8.3 Bioactivity
Various lignans have been linked to antihypertensive and vasodilating effects (Deyama et al. 2001; Luo et al. 2010; Sih et al. 1976). In mechanistic studies (Jin et al. 2008), the vasodilation induced by an aqueous extract of Eucommia ulmoides was found to depend on endothelium-derived hyperpolarizing factor (EDHF) with the activation of K+ channels. In addition, muscarinic Ach receptor agonists could also play a role in lowering blood pressure via vasodilation. Geniposidic acid (15, Table 1.1) also has antihypertensive effects (Deyama et al. 2001), while aucubin (16, Table 1.1) and other iridoids are likely responsible for the anti-inflammatory effects of Eucommia. Aucubin inhibits the arachidonic acid pathway, TNF-α-induced responses, and NF-kB activation (Benito et al. 2000; Park 2013), which may partly explain the herbal use in the treatment of arthritis (Wang et al. 2015b), as well as indicate a potential for improving obesity-induced atherosclerosis (Park 2013). Aucubin and geniposidic acid promoted collagen synthesis (Li et al. 1998), and geniposidic acid increased the skin moisture content of UV-damaged skin in hairless mice (Jimbo et al. 2015). Due to the important pharmacological effects of geniposidic acid and aucubin, a high-performance liquid chromatography – tandem mass spectrometry method has been developed to determine these two compounds in rat plasma, particularly for the pharmacokinetic study after oral administration of Eucommia herbal tea (Zhang et al. 2014). Due to its medicinal values, geniposidic acid is used as a food additive in Japan (Zhang et al. 2014).
Neuroprotective properties have also been ascribed to Eucommia ulmoides aqueous bark extracts, implying potential application in the prevention or treatment of Alzheimer’s and other neurodegenerative diseases (Kwon et al. 2012, 2014). Eucommia leaves have also been made into a health beverage (Yue et al. 1999).
1.3.8.4 Conclusion
Eucommia ulmoides is a TCM recommended for vitality enhancement and longevity. In addition to fairly common plant flavonoids, it also contains less common lignans and iridoid compounds. More scientific studies are needed to verify the plant’s suggested role as a “longevity herb” in preventing bone loss, inducing fat loss, and reducing elevated blood pressure and triglycerides. However, its potential as a nutritional supplement is fairly high, because, unlike many other plants, it is active at relatively low oral dosages.
1.3.9 Ligusticum wallichii (or Cnidium officinale)
1.3.9.1 Introduction
In TCM, the rhizomes from Ligusticum wallichii or L. chuanxiong (Chinese: Chuan Chung or Chuan Xiong 川芎), plant species in the carrot family (Umbelliferae), are well known for both medicinal (to treat/prevent disease) and edible (to provide nutrition) uses. In Japanese Kampo medicine, the roots of Cnidium officinale are used for the same purposes. Commonly, the plant is known as a lovage root and is particularly used as an important herb in blood tonics, for treating pain from headache, rheumatic arthralgia, or traumatic injury and to relieve gynecological problems. Si Wu Tang (four-substance decoction) is one of the most famous gynecological TCM formulas containing Ligusticum, as well as Angelica sinensis (Dang Gui), Rehmannia (Sheng Di Huang), and Paeonia alba (Bai Shao) (Zhou and Qu 2009). This formula is used for treating menstrual disorders, such as amenorrhea and dysmenorrhea.
1.3.9.2 Chemical Constituents
Ligusticum roots contain other important bioactive compounds, including alkaloids, particularly tetramethylpyrazine; phthalides, such as ligustilide and senkyunone; organic acids, such as ferulic acid; anthraquinones, such as chrysophanic acid; polysaccharides; ceramides; and cerebrosides (Li et al. 2012b).
1.3.9.3 Bioactivity
Pharmacological studies have shown that Ligusticum TCM formulas and particularly its antihypertensive constituent tetramethylpyrazine (17, Table 1.1), also known as ligustrazine or chuanxiongzine, can increase coronary circulation and decrease oxygen consumption, increase myocardial contractility and decrease heart rate, and cause vasodilation and lower blood pressure (Lee 2015). A review (Ran et al. 2011) compiled the current scientific research on the chemistry and pharmacology of L. chuanxiong, pointing out its valuable therapeutic properties as well as medical potential. The pharmacological targets and pharmacokinetics of L. chuanxiong, as well as other TCM formulas used for the treatment of cardiovascular and cerebrovascular disease, have been studied with the aims of clarifying the traditional uses and modernizing these herbal medicines (Li et al. 2012a; Zeng et al. 2013).
1.3.9.4 Conclusion
As Ligusticum is widely used in TCM for treating migraine, the herb’s effects on the blood–brain barrier have been studied (Wang et al. 2015a). The alkaloid tetramethylpyrazine has also shown in vivo nootropic and neuroprotective effects in rat models (Kong et al. 2015; Lu et al. 2014; Wu et al. 2013), as well as in vitro actions against neuro-inflammation (Kim et al. 2014), giving it a possible use in treatment of Alzheimer’s or other neurodegenerative diseases, which could greatly improve quality of life for many elderly adults.
1.3.10 Lycium barbarum
1.3.10.1 Introduction
Lycium barbarum (Chinese: Kou Chi Tzu 枸杞子) is a species of boxthorn in the family Solanaceae. It produces a bright red-orange oblong fruit, known as a wolfberry or goji berry. In China, these sweet-tasting berries are celebrated in an annual festival each August in Ningxia province, China, the main location of their cultivation. The berries can be eaten either raw or dried; made into juice, wine, or tea; or processed into powders, tablets, and tinctures (Cheng et al. 2015). In TCM, the berries (Fructus lycii) are regarded to benefit the liver and kidney, replenish vital essence (chi), and improve eyesight. The root bark (Cortex lycii) is also used to alleviate fever and to treat night sweats, pneumonia, and cough (Potterat 2010; Yao et al. 2011).
1.3.10.2 Chemical Constituents
L. barbarum fruits are rich in polysaccharides/proteoglycans (5–8 % of the dried fruit), termed LBPs, from six carbohydrates: galactose, glucose, rhamnose, arabinose, mannose, and xylose. Other major compounds are the coumarin scopoletin and glycosylated vitamin C (2-O-β-d-glucopyranosyl-l-ascorbic acid) (Tang et al. 2012). Water-soluble LBPs can be separated by an extraction process to remove more lipid-soluble constituents, including carotenoids such as zeaxanthin (Cheng et al. 2015). The LBPs are considered to be the most important, bioactive components (Shan et al. 2011). Other components in the fruit are carbohydrates, carotenoids, flavonoids, betaine, cerebroside, β-sitosterol, amino acids, trace elements, vitamins, etc. (Amagase and Farnsworth 2011). Detailed phytochemical reviews are available (Potterat 2010; Yao et al. 2011).
1.3.10.3 Bioactivity
In TCM, plants from the genus Lycium, including L. barbarum and the related species L. chinense, have been used for tonic, aphrodisiac, hepatoprotective, antiseptic, hypotensive, and hypoglycemic properties (Anonymous 1999c; Potterat 2010; Yao et al. 2011). The traditional “yin”-nourishing effect can be associated with immunoregulating actions. The LBPs exert both indirect effects on immune modulation and direct effects on cytoprotection, antiaging, and neuromodulation (Chang and So 2008). Such scientific evidence provides some support for the folk medicine use of wolfberries to increase longevity (Potterat 2010; Yao et al. 2011). Also, a recent report found that wolfberries can enhance the protective effect of influenza vaccine in older mice (Du et al. 2014). Similar support has also been found for the eye health benefits, e.g., LBPs have shown neuroprotective effects on retinal ganglion cells (Mi et al. 2013). LBPs have also been linked to immune-enhancing effects by increasing expression of interleukin-2 and tumor necrosis factor-alpha (Gan et al. 2003), as well as anticancer effects, such as apoptotic induction, stimulating interest in Lycium as a cancer therapy agent/adjuvant (Tang et al. 2012). The scientific studies related to the above bioactivities, as well as metabolism stimulation, cardiovascular benefits, diabetes, and antioxidant effects, have been well described in several reviews (Amagase and Farnsworth 2011; Cheng et al. 2015; Jin et al. 2013).
1.3.10.4 Conclusion
L. barbarum undoubtedly has nutritional value for public health, and its chemical components have shown various biological effects in cellular and animal studies, as well as some human clinical studies. Indeed, the Natural Standard Research Collaboration recently reported an evidence-based review to compile folkloric precedent with consolidated safety and efficacy data from the scientific literature (Ulbricht et al. 2015). However, further studies should be performed to truly clarify detailed mechanisms, possible synergistic effects, and ensured safety profiles, such as contraindication with other food and medications. The general public needs to be told about not only the potential health benefits but also the difference between health claims and structure–function claims regarding the potential of Lycium, as well as other products, as a functional food (Lasekan 2014).
1.4 Summary
Chinese herbal medicine (CHM) has been used for many thousands of years to both treat and prevent human disease. This invaluable knowledge makes CHM the best resource for modern scientists in their efforts to develop new drug research and future clinical trial candidates. Chronic disease seriously affects the quality of life of patients, and many ancient CHM-derived remedies could hold the answer to alleviating many of those diseases’ most debilitating symptoms, as well as preventing those diseases at the outset and treating the disease once contracted. Development of CHM products as adjunct therapies to augment the efficacy and offset the toxicity of Western medicine is an excellent approach for rapid advancement into US FDA-approved new drugs. Developing CHM products as high-quality dietary supplements must particularly emphasize standardization through qualitative and quantitative quality controls. A combination of advanced medicinal chemistry and natural products chemistry, coupled with cutting-edge life science technology, will play a very important role for converting CHM products, especially the pure single active principles, through modification and synthesis into clinical trial candidates very efficiently and effectively. This mixture of current Western medicine and the ancient therapies of CHM could indeed hold promising answers for the treatment of chronic diseases to greatly improve quality of life of patients, making CHM of the upmost importance in future drug discovery and development. As evidenced by the ten case studies outlined above, the active principles of CHM have been elucidated. Accordingly, there is a major need to develop these compounds into world-class medicines with great efficacy and low toxicity, making them superior to the current Western medicine therapies currently available.
Abbreviations
- Ach:
-
Acetylcholine
- AIDS:
-
Acquired immunodeficiency syndrome
- ANS:
-
1-anilino-8-naphthalene-sulfonate
- ATP:
-
Adenosine triphosphate
- BDFI:
-
Bioactivity-directed fractionation and isolation
- CD:
-
Circular dichroism
- CHM:
-
Chinese herbal medicine
- COX:
-
Cyclooxygenase
- CRF:
-
Cancer-related fatigue
- DNA:
-
Deoxyribonucleic acid
- EDHF:
-
Endothelium-derived hyperpolarizing factor
- EGFR-TKI:
-
Epidermal growth factor receptor tyrosine kinase inhibitor
- FDA:
-
Food and Drug Administration
- FRET:
-
Förster-type fluorescence resonance energy transfer
- FTIR:
-
Fourier transform infrared spectroscopy
- GAP:
-
Good agriculture practice
- GCP:
-
Good clinical practice
- GI:
-
Gastrointestinal
- GLP:
-
Good laboratory practice
- GMP:
-
Good manufacturing practice
- GRAS:
-
Generally recognized as safe
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- HIV:
-
Human immunodeficiency virus
- HIV-1:
-
Human immunodeficiency virus type 1
- HPLC:
-
High-pressure liquid chromatography
- HPV:
-
Human papilloma virus
- IC50 :
-
Half maximal inhibitory concentration
- IL:
-
Interleukin
- IND:
-
Investigational New Drug
- iNOS:
-
Inducible nitric oxide synthase
- IOIP:
-
Idiopathic orbital inflammatory pseudotumors
- IV:
-
Intravenous
- LBP:
-
Lycium barbarum polysaccharide
- MALDI-TOF MS:
-
Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry
- mcIRBP:
-
Momordica charantia insulin receptor (IR)-binding protein
- MCP:
-
Monocyte chemoattractant protein
- MOEA:
-
Ministry of Economic Affairs
- NBP:
-
3-n-butylphthalide
- NOS:
-
Nitric oxide synthase
- RCT:
-
Randomized controlled trial
- RMR:
-
Red mold rice
- SFDA:
-
State Food and Drug Administration
- TCM:
-
Traditional Chinese medicine
- TNF:
-
Tumor necrosis factor
- US:
-
United States
- WHO:
-
World Health Organization
References
Aggarwal BB, Kumar A, Bhari AC (2003) Anticancer potential of curcumin: preclinical and clinical studies. Anticancer Res 23:363–398
Amagase H, Farnsworth NR (2011) A review of botanical characteristics, phytochemistry, clinical relevance in efficacy and safety of Lycium barbarum fruit (Goji). Food Res Int 44:1702–1717. doi:10.1016/j.foodres.2011.03.027
Anand P, Kunnumakkara AB, Newman RA, Aggarwal BB (2007) Bioavailability of curcumin: problems and promises. Mol Pharm 4:807–818. doi:10.1021/mp700113r
Anonymous (1999a) State Administration of Traditional Chinese Medicine. Chinese Materia Medica, vol 5. Shanghai Scientific and Technical Publishers, Shanghai, pp 906–908
Anonymous (1999b) State Administration of Traditional Chinese Medicine. Chinese Materia Medica, vol 8. Shanghai Scientific and Technical Publishers, Shanghai, pp 631–498
Anonymous (1999c) State Administration of Traditional Chinese Medicine of the People’s Republic of China, ‘Chinese Herbs’, vol 19. Shanghai Science and Technology Press, Shanghai, p 267
Anonymous (1999d) WHO monographs on selected medicinal plants. World Health Organization, Geneva
Anonymous (2005) The Pharmacopoeia of People’s Republic of China. China, E.C.O.T.P.O.P.S.R.O. Chemical Industry Press, Beijing
Anonymous (2009) Dictionary of Chinese Traditional Medicine, vol 1. Scientific Technology Press, Shanghai, pp 1560–1561
Ao ZH, Xu ZH, Lu ZM, Xu HY, Zhang XM, Dou WF (2009) Niuchangchih (Antrodia camphorata) and its potential in treating liver diseases. J Ethnopharmacol 121:194–212. doi:10.1016/j.jep.2008.10.039
Bairwa K, Grover J, Kania M, Jachak SM (2014) Recent developments in chemistry and biology of curcumin analogues. RSC Adv 4:13946–13978. doi:10.1039/c4ra00227j
Batch PA (2010) Prescription for nutritional healing: a practical A-to-Z reference to drug-free remedies using vitamins, minerals, herbs and food supplements, 4th edn. Avery Penguin Putnam, New York
Benito PB, Díaz Lanza AM, Silván Sen AM, De Santos Galindez J, Fernandez Matellano L, Sanz Gómez A, Abad Martínez MJ (2000) Effects of some iridoids from plant origin on arachidonic acid metabolism in cellular systems. Planta Med 66:324–328
Broadhurst CL, Polansky MM, Anderson RA (2000) Insulin-like biological activity of culinary and medicinal plant aqueous extracts in vitro. J Agric Food Chem 48:849–852. doi:10.1021/jf9904517
Chan MMY (1995) Inhibition of tumor necrosis factor by curcumin, a phytochemical. Biochem Pharmacol 49:1551–1556. doi:10.1016/0006-2952(95)00171-U
Chang TT, Chou WN (1995) Antrodia cinnamomea sp. nov. on Cinnamomum kanehirai in Taiwan. Mycol Res 99:756–758
Chang RCC, So KF (2008) Use of anti-aging herbal medicine, Lycium barbarum, against aging-associated diseases. What do we know so far? Cell Mol Neurobiol 28:643–652. doi:10.1007/s10571-007-9181-x
Chattopadhyay I, Biswas K, Bandyopadhyay U, Banerjee RK (2004) Turmeric and curcumin: biological actions and medicinal applications. Curr Sci (Bangalore) 87:44–53
Chaturvedi P (2012) Antidiabetic potentials of Momordica charantia: multiple mechanisms behind the effects. J Med Food 15:101–107. doi:10.1089/jmf.2010.0258
Chen WP, Ho BY, Lee CL, Lee CH, Pan TM (2008) Red mold rice prevents the development of obesity, dyslipidemia and hyperinsulinemia induced by high-fat diet. Int J Obes 32:1694–1704. doi:10.1038/ijo.2008.156
Chen HW, Lin IH, Chen YJ, Chang KH, Wu MN, Su WH, Huang GC, Lai YL (2012) A novel infusible botanically-derived drug, PG2, for cancer-related fatigue: a phase II double-blind, randomized placebo-controlled study. Clin Invest Med 35:E1–E11
Chen H, Guo J, Pang B, Zhao L, Tong X (2015) Application of herbal medicine with bitter flavor and cold property on treating diabetes mellitus. Evid Based Complement Alternat Med 2015:529491. doi:10.1155/2015/529491
Cheng AL, Hsu CH, Lin JK, Hsu MM, Ho YF, Shen TS, Ko JY, Lin JT, Lin BR, Ming-Shiang W, Yu HS, Jee SH, Chen GS, Chen TM, Chen CA, Lai MK, PU YS, Pan MH, Wang YJ, Tsai CC, Hsieh CY (2000) Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or pre-malignant lesions. Anticancer Res 21:2895–2900
Cheng J, Zhou ZW, Sheng HP, He LJ, Fan XW, He ZX, Sun T, Zhang X, Zhao RJ, Gu L, Cao C, Zhou SF (2015) An evidence-based update on the pharmacological activities and possible molecular targets of Lycium barbarum polysaccharides. Drug Des Dev Ther 9:33–78. doi:10.2147/DDDT.S72892
Deodhar S, Sethi R, Srimal R (1980) Preliminary study on antirheumatic activity of curcumin (diferuloyl methane). Indian J Med Res 71:632–634
Deyama T, Nishibe S, Nakazawa Y (2001) Constituents and pharmacological effects of Eucommia and Siberian ginseng. Acta Pharmacol Sin 22:1057–1070
Dharmananda S (1999) Chinese herbal therapy for sciatica and lumbago. 1999, START Group Manuscripts, Portland
Dharmananda S (2000) An analysis of Chinese herb prescriptions for rheumatoid arthritis. 2000, START Group Manuscripts, Portland
Dhillon N, Aggarwal BB, Newman RA, Wolff RA, Kunnumakkara AB, Abbruzzese JL, Ng CS, Badmaev V, Kurzrock R (2008) Phase II trial of curcumin in patients with advanced pancreatic cancer. Clin Cancer Res 14:4491–4499. doi:10.1158/1078-0432.CCR-08-0024
Drewnowski A, Gomez-Carneros C (2000) Bitter taste, phytonutrients, and the consumer: a review. Am J Clin Nutr 72:1424–1435
Du X, Wang J, Niu X, Smith D, Wu D, Meydani SN (2014) Dietary wolfberry supplementation enhances the protective effect of flu vaccine against influenza challenge in aged mice. J Nutr 144:224–209. doi:10.3945/jn.113.183566
Endo A (1979) Monacolin K, a new hypocholesterolemic agent produced by a Monascus species. J Antibiot (Tokyo) 32:852–854. doi:10.7164/antibiotics.32.852
Gan L, Zhang SH, Liu Q, Xu HB (2003) A polysaccharide-protein complex from Lycium barbarum upregulates cytokine expression in human peripheral blood mononuclear cells. Eur J Pharmacol 471:217–222. doi:10.1016/S0014-2999(03)01827-2
Geethangili M, Tzeng YM (2011) Review of pharmacological effects of Antrodia camphorata and its bioactive compounds. Evid Based Complement Alternat Med 2011:212641. doi:10.1093/ecam/nep108
Goel A, Kunnumakkara AB, Aggarwal BB (2008) Curcumin as “Curecumin”: from kitchen to clinic. Biochem Pharmacol 75:787–809. doi:10.1016/j.bcp.2007.08.016
Grover JK, Yadav SP (2004) Pharmacological actions and potential uses of Momordica charantia: a review. J Ethnopharmacol 93:123–132. doi:10.1016/j.jep.2004.03.035
Gupta SC, Prasad S, Kim JH, Patchva S, Webb LJ, Priyadarsini IK, Aggarwal BB (2011) Multitargeting by curcumin as revealed by molecular interaction studies. Nat Prod Rep 28:1937–1955. doi:10.1039/c1np00051a
Gupta AK, Mishra R, Lal RK (2015) Genetic resources, diversity, characterization and utilization of agronomical traits in turmeric (Curcuma longa L.). Ind Crop Prod 77:708–712. doi:10.106/j.indcrop.2015.09.030
Hamid K, Alqahtani A, Kim MS, Cho JL, Cui PH, Li CG, Groundwater PW, Li GQ (2015) Tetracyclic triterpenoids in herbal medicines and their activities in diabetes and its complications. Curr Top Med Chem 15:2406–2430. doi:10.2174/1568026615666150619141940
Hasan I, Khatoon S (2012) Effect of Momordica charantia (bitter gourd) tablets in diabetes mellitus: type 1 and type 2. Prime Res Med (PROM) 2:72–74
Heber D, Yip I, Ashley JM, Elashoff DA, Elashoff RM, Go VL (1999) Cholesterol-lowering effects of a proprietary Chinese red-yeast rice dietary supplement. Am J Clin Nutr 69:231–236
Hong J, Bose M, Ju J, Ryu JH, Chen X, Sang S, Lee MJ, Yang CS (2004) Modulation of arachidonic acid metabolism by curcumin and related β-diketone derivatives: effects on cytosolic phospholipase A2, cyclooxygenases and 5-lipoxygenase. Carcinogenesis 259:1671–1679. doi:10.1093/carcin/bgh165
Horax R, Hettiarachchy N, Over K, Chen P, Gbur E (2010) Extraction, fractionation and characterization of bitter melon seed proteins. J Agric Food Chem 58:1892–1897. doi:10.1021/jf902903s
Hsu CH, Cheng AL (2007) Clinical studies with curcumin. In: Aggarwal BB, Surh YJ, Shishodia S (eds) The molecular targets and therapeutic uses of curcumin in health and disease. Springer, New York, pp 471–480
Hsu C, Hsieh CL, Kuo YH, Huang CJ (2011) Isolation and identification of Cucurbitane-type triterpenoids with partial agonist/antagonist potential for estrogen receptors from Momordica charantia. J Agric Food Chem 59:4553–4561. doi:10.1021/jf200418g
Huang CH, Chen YJ, Lin CC (2012) Antrodia cinnamomea (A. camphorata, Neu Chang Chin): an exceptional polypore mushroom with potential antitumor and immunomodulatory effects. Curr Top Nutraceuticals Res 10:61–74
Huang YX, Liu EW, Wang L, Huo Y, Wang Q, Olaleye O, Wang T, Gao XM (2014) LC/MS/MS determination of pharmacokinetic studies of six compounds in rat plasma following oral administration of the single and combined extracts of Eucommia ulmoides and Dipsacus asperoides. Chin J Nat Med 12:0469–0476. doi:10.1016/S1875-5364(14)60073-X
Hung HY, Qian K, Morris-Natschke SL, Hsu CS, Lee KH (2012) Recent discovery of plant-derived anti-diabetic natural products. Nat Prod Rep 29:580–606. doi:10.1039/c2np00074a
India. Ministry of Health and Family Welfare (1996) Indian Pharmacopoeia, Controller of Publications: Delhi, 1996
Ireson C, Orr S, Jones DJ, Verschoyle R, Lim CK, Luo JL, Howells L, Plummer S, Jukes R, Williams M, Steward WP, Gescher A (2001) Characterization of metabolites of the chemopreventive agent curcumin in human and rat hepatocytes and in the rat in vivo, and evaluation of their ability to inhibit phorbol ester-induced prostaglandin E2 production. Cancer Res 61:1058–1064
Itokawa H, Shi Q, Akiyama T, Morris-Natschke SL, Lee KH (2008) Recent advances in the investigation of curcuminoids. Chin Med 3:1–13. doi:10.1186/1749-8546-3-11
Jimbo N, Kawada C, Nomura Y (2015) Herb extracts and collagen hydrolysate improve skin damage resulting from ultraviolet-induced aging in hairless mice. Biosci Biotechnol Biochem 79:1624–1628. doi:10.1080/09168451.2015.1046362
Jin X, Otonashi-Satoh Y, Sun P, Kawamura N, Tsuboi T, Yamaguchi Y, Ueda T, Kawasaki H (2008) Endothelium-derived hyperpolarizing factor (EDHF) mediates endothelium-dependent vasodilator effects of aqueous extracts from Eucommia ulmoides Oliv. leaves in rat mesenteric resistance arteries. Acta Med Okayama 62:319–325
Jin M, Huang Q, Zhao K, Shang P (2013) Biological activities and potential health benefit effects of polysaccharides isolated from Lycium barbarum L. Int J Biol Macromol 54:16–23. doi:10.1016/j.ijbiomac.2012.11.023
Joseph B, Jini D (2013) Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac J Trop Dis 3:93–102
Jurenka JS (2009) Anti-inflammatory properties of curcumin, a major constituent of Curcuma longa: a review of preclinical and clinical research. Altern Med Rev 14:141–153
Kang SP, Saif MW (2008) Optimal second line treatment options for gemcitabine refractory advance pancreatic cancer patients. Can we establish standard of care with available data? J Pancreas (Online) OP 9:83–90
Kaur P, Garg V, Gulait M, Singh SK (2016) Oral delivery of antidiabetic polypeptide-k: journey so far and the road ahead. Curr Drug Deliv 13(2):236–244
Kawamori T, Lubet R, Steele VE, Kelloff GJ, Kaskey RB, Rao CV, Reddy BS (1999) Chemopreventive effect of curcumin, a naturally occurring anti-inflammatory agent, during the promotion/progression stages of colon cancer. Cancer Res 59:597–601
Kim M, Kim SO, Lee, Lee JH, Jung WS, Moon SK, Kim YS, Cho KH, Ko CN, Lee EH (2014) Tetramethylpyrazine, a natural alkaloid, attenuates pro-inflammatory mediators induced by amyloid β and interferon-γ in rat brain microglia. Eur J Pharmacol 741:504–511. doi:10.1016/j.ejphar.2014.06.037
Kong X, Zhong M, Su X, Qin Q, Su H, Wan H, Liu C, Wu J, Shang H, Zhang Y, Lin N (2015) Tetramethylpyrazine promotes migration of neural precursor cells via activating the phosphatidylinositol 3-kinase pathway. Mol Neurobiol. doi:10.1007/s12035-015-9551-1
Kuo YL, Chen CH, Chuang TH, Hua WK, Lin WJ, Hsu WH, Chang PM, Hsu SL, Huang TH, Kao CY, Huang CY (2015) Gene expression profiling and pathway network analysis predicts a novel antitumor function for a botanical-derived drug, PG2. Evid Based Complement Alternat Med 2015:917345. doi:10.1155/2015/917345
Kwon SH, Kim MJ, Ma SX, You IJ, Hwang JY, Oh JH, Kim SY, Kim HC, Lee SY, Jang CG (2012) Eucommia ulmoides Oliv. bark protects against hydrogen peroxide-induced neuronal cell death in SH-SY5Y cells. J Ethnopharmacol 142:337–345. doi:10.1016/j.jep.2012.04.010
Kwon SH, Ma SX, Hong SI, Kim SY, Lee SY, Jang CG (2014) Eucommia ulmoides Oliv. bark attenuates 6-hydroxydopamine-induced neuronal cell death through inhibition of oxidative stress in SH-SY5Y cells. J Ethnopharmacol 152:173–182. doi:10.1016/j.jep.2013.12.048
Lal B, Kapoor AK, Asthana OP, Agrawal PK, Prasad R, Kumar P, Srimal RC (1999) Efficacy of curcumin in the management of chronic anterior uveitis. Phytother Res 13:318–322. doi:10.1002/(SICI)1099-1573(199906)13:4<318::AID-PTR445>3.0.CO;2-7
Lal B, Kapoor A, Agrawal OP, Asthana OP, Srimal RC (2000) Role of curcumin in idiopathic inflammatory orbital pseudotumours. Phytother Res 14:443–447. doi:10.1002/1099-1573(200009)14:6<443::AID-PTR619>3.0.CO;2-V
Lam W, Bussom C, Guan F, Jiang Z, Zhang W, Gullen EA, Liu SH, Cheng YC (2010) The four-herb Chinese medicine PHY906 reduces chemotherapy-induced gastrointestinal toxicity. Sci Transl Med 2:45ra59. doi:10.1126/scitranslmed.3001270
Lam W, Jiang Z, Guan F, Huang X, Hu R, Wang J, Bussom S, Liu SH, Zhao H, Yen Y, Cheng YC (2015) PHY906(KD018), an adjuvant based on a 1800-year-old Chinese medicine, enhanced the anti-tumor activity of Sorafenib by changing the tumor microenvironment. Sci Rep 5:9384. doi:10.1038/srep09384
Lasekan O (2014) Exotic berries as a functional food. Curr Opin Clin Nutr Metab Care 17:589–595. doi:10.1097/MCO.0000000000000109
Lee KH (2015) Chinese herbal medicine-derived products for prevention or treatment of disease affecting quality of life. Plenary lecture presented at the 2nd international conference of traditional and complementary medicine on health. Taipei, Taiwan, 26 October 2015
Lee CL, Pan TM (2011a) Composition and method for prevention and treatment of Alzheimer’s disease. Taiwan Patent I341204
Lee CL, Pan TM (2011b) Red mold fermented products and Alzheimer’s disease: a review. Appl Microbiol Biotechnol 91:461–469. doi:10.1007/s00253-011-3413-1
Lee KH, Tao-Wiedman TW, Wu H (1993) Pharmagenesis Advisory Board Meeting
Lee TH, Lee CK, Tsou WL, Liu SY, Kuo MT, Wen WC (2007) A new cytotoxic agent from solid-state fermented mycelium of Antrodia camphorata. Planta Med 13:1412–1415. doi:10.1055/s-2007-990232
Lee KH, Lin L, Shih CCY, Su CY, Ishida J, Ohtsu H, Wang HK, Itokawa H, Chang CS (2008) US Patent 7,355,081
Lee CL, Kung YH, Wu CL, Shu YW, Pan TM (2010) Monascin and ankaflavin act as novel hypolipidemic and high-density lipoprotein cholesterol-raising agents in red mold dioscorea. J Agric Food Chem 58:9013–9019. doi:10.1021/jf3042402
Lee KH, Morris-Natschke SL, Qian K, Dong Y, Yang X, Zhou T, Belding E, Wu SF, Wada K, Akiyama T (2012) Recent progress of research on herbal products used in traditional Chinese medicine: the herbs belonging to the divine husbandman’s herbal foundation canon (Shen Nong Ben Cao Jing). J Trad Compl Med 2:6–26
Lee KH, Morris-Natschke SL, Brattlie J, Xie J, Belding E (2013) Modern drug discovery from Chinese Materia Medica used in traditional Chinese medicine. In: Adams JD, Lien EJ (eds) Traditional Chinese medicine: scientific basis for its use. RSC Publishing, Cambridge, pp 81–134
Leung L, Birtwhistle R, Kotecha J, Hannah S, Cuthbertson S (2009) Anti-diabetic and hypoglycaemic effects of Momordica charantia (bitter melon): a mini review. Br J Nutr 102:1703–1708. doi:10.1017/S0007114509992054
Li SZ (1596) Pen Tsao Kang Mu (Compendium of Materia Medica Systematic Pharmacopoeia) China
Li Y, Kamo S, Metori K, Koike K, Che QM, Takhashi S (1998) The promoting effects of geniposidic acid and aucubin in Eucommia ulmoides Oliv leaves on collagen synthesis. Biol Pharm Bull 21:1306–1310
Li SY, Yuan W, Deng G, Wang P, Yang P, Aggarwal BB (2011) Chemical composition and product quality control of turmeric (Curcuma longa L.). Pharm Crop 2:28–54. doi:10.2174/2210290601102010028
Li B, Xu X, Wang X, Yu H, Li X, Tao W, Wang Y, Yang L (2012a) A systems biology approach to understanding the mechanism of action of Chinese herbs for treatment of cardiovascular disease. Int J Mol Sci 13:13501–13520. doi:10.3390/ijms131013501
Li W, Tang Y, Chen Y, Duan JA (2012b) Advances in the chemical analysis and biological activities of chuanxiong. Molecules 17:10614–10651. doi:10.3390/molecules170910614
Lin L, Shi Q, Nyarko AK, Bastow KF, Wu CC, Su CY, Shih CC, Lee KH (2006a) Antitumor agents. 250. Design and synthesis of new curcumin analogues as potential anti-prostate cancer agents. J Med Chem 49:3963–3972. doi:10.1021/jm051043z
Lin L, Shi Q, Su CY, Shih CC, Lee KH (2006b) Antitumor agents 247. New 4-ethoxycarbonylethyl curcumin analogs as potential antiandrogenic agents. Bioorg Med Chem 14:2527–2534. doi:10.1016/j.bmc.2005.11.034
Lin HY, Ho TY, Lin C, Li CC, Hsiang CY (2014) A novel insulin receptor-binding protein from Momordica charantia enhances glucose uptake and glucose clearance in vitro and in vivo through triggering insulin receptor signaling pathway. J Agric Food Chem 62:8952–8961. doi:10.1021/jf3042402
Lin CM, Lin YT, Lin RD, Huang WJ, Lee MH (2015) Neurocytoprotective effects of aliphatic hydroxamines from lovastatin, a secondary metabolite from Monascus-fermented red mold rice, in 6-hydroxydopamine (6-OHDA)-treated nerve growth factor (NGF)-differentiated PC12 cells. ACS Chem Neurosci 6:716–724. doi:10.1021/cn500275k
Liu SH, Cheng YC (2012) Old formula, new Rx: the journey of PHY906 as cancer adjuvant therapy. J Ethnopharmacol 140:614–623. doi:10.1016/j.jep.2012.01.047
Liu SY, Kuo MT, Wen WC (2008) US Patent No. 7,385,088
Lu MC, El-Shazly M, Wu TY, Du YC, Chang TT, Chen CF, Hsu YM, Lai KH, Chiu CP, Chang FR, Wu YC (2013) Recent research and development of Antrodia cinnamomea. Pharmacol Ther 139:124–156. doi:10.1016/j.pharmthera.2013.04.001
Lu C, Zhang J, Shi X, Miao S, Bi L, Zhang S, Yang Q, Zhou X, Zhang M, Xie Y, Miao Q, Wang S (2014) Neuroprotective effects of tetramethylpyrazine against dopaminergic neuron injury in a rat model of Parkinson’s disease induced by MPTP. Int J Biol Sci 10:350–357. doi:10.7150/ijbs.8366
Luo LF, Wu WH, Zhou YJ, Yan J, Yang GP, Ouyang DS (2010) Antihypertensive effect of Eucommia ulmoides Oliv. extracts in spontaneously hypertensive rats. J Ethnopharmacol 129:238–243. doi:10.1016/j.jep.2010.03.019
Ma J, Li Y, Ye Q, Li J, Hua Y, Ju D, Zhang D, Cooper R, Chang M (2000) Constituents of red yeast rice, a traditional Chinese food and medicine. J Agric Food Chem 48:5220–5225. doi:10.1021/jf000338c
Ma WL, Hsu CL, Wu MH, Wu CT, Wu CC, Lai JJ, Jou YS, Chen CW, Yeh S, Chang C (2008) Androgen receptor is a new potential therapeutic target for the treatment of hepatocellular carcinoma. Gastroenterology 135:947–955. doi:10.1053/j.gastro.2008.05.046
Medagama AB, Bandara R (2014) The use of complementary and alternative medicines (CAMs) in the treatment of diabetes mellitus: is continued used safe and effective? Nutr J 13:102. doi:10.1186/1475-2891-13-102
Mi XS, Zhong JX, Chang RCC, So KF (2013) Research advances on the usage of traditional Chinese medicine for neuroprotection in glaucoma. J Integr Med 11:233–240. doi:10.3736/jintegrmed2013037
Miłobdzka J, Lampe V (1910) Zur kenntnis des curcumins. Ber Deutsch Chem Ges 43:2163–2170
Miyamoto H, Yang ZM, Chen YT, Ishiguro H, Uemura H, Kubota Y, Nagashima Y, Chang YJ, Hu YC, Tsai MY, Yeh S, Messing EM, Chang C (2007) Promotion of bladder cancer development and progression by androgen receptor signals. J Natl Cancer Inst 99:558–568. doi:10.1093/jnci/djk113
Park KS (2013) Aucubin, a naturally occurring iridoid glycoside inhibits TNF-α-induced inflammatory responses through suppression of NF-kB activation in 3T3-L1 adipocytes. Cytokine 62:407–412. doi:10.1016/j.cyto.2013.04.005
Paul A, Raychaudhuri SS (2010) Medicinal uses and molecular identification of two Momordica charantia varieties – a review. eJBio 6:43–51
Pedersen U, Rasmussen PB, Lawesson SO (1985) Synthesis of naturally occurring curcuminoids and related compounds. Liebigs Ann Chem 8:1557–1569. doi:10.1002/jlac.198519850805
Potterat O (2010) Goji (Lycium barbarum and L. chinense: phytochemistry, pharmacology and safety in the perspective of traditional uses and recent popularity. Planta Med 76:7–19. doi:10.1055/s-0029-1186218
Raman A, Lau C (1996) Anti-diabetic properties and phytochemistry of Momordica charantia L. (Cucurbitaceae). Phytomedicine 2:349–362. doi:10.1016/S0944-7113(96)80080-8
Ran X, Ma L, Peng C, Zhang H, Qin LP (2011) Ligusticum chuanxiong Hort: a review of chemistry and pharmacology. Pharm Biol 49:1180–1189. doi:10.3109/13880209.2011.576346
Rister R (ed) (1999) Japanese herbal medicine: the healing art of Kampo. Avery Publishing Group, New York, p 31
Saif MW, Lansigan F, Ruta S, Lamb L, Mezes M, Elligers K, Grant N, Jiang ZL, Liu SH, Chang YC (2010) Phase I study of the botanical formulation PHY906 with capecitabine in advanced pancreatic and other gastrointestinal malignancies. Phytomedicine 17:161–169. doi:10.1016/j.phymed.2009.12.016
Saif MW, Li J, Lamb L, Kaley K, Elligers K, Jiang Z, Bussom S, Liu SH, Cheng YC (2014) First-in-human phase II trial of the botanical formulation PHY906 with capecitabine as second-line therapy in patients with advance pancreatic cancer. Cancer Chemother Pharmacol 73:373–380. doi:10.1007/s00280-013-2359-7
Satoskar R, Shah S, Shenoy S (1986) Evaluation of anti-inflammatory property of curcumin (diferuloyl methane) in patients with postoperative inflammation. Int J Clin Pharmacol Ther Toxicol 24:651–654
Satyavati GV, Raina MK (1976) Indian Council of Medical Research. In Medicinal plants of India, vol 1. New Delhi, p 107
Shan X, Zhou J, Ma T, Chai Q (2011) Lycium barbarum polysaccharides reduce exercise-induced oxidative stress. Int J Mol Sci 12:1081–1088. doi:10.3390/ijms12021081
Sharma RA, McLelland HR, Hill KA, Ireson CR, Euden SA, Manson MM, Pirmohamed M, Marnett LJ, Gescher AJ, Steward WP (2001) Pharmacodynamic and pharmacokinetic study of oral Curcuma extract in patients with colorectal cancer. Clin Cancer Res 7:1894–1900
Shi YC, Pan TM (2011) Beneficial effects of Monascus purpureus NTU 568-fermented products: a review. Appl Microbiol Biotechnol 90:1207–1217. doi:10.1007/s00253-011-3202-x
Shi Q, Shih CY, Lee KH (2009) Novel anti-prostate cancer curcumin analogues that enhance androgen receptor degradation activity. Anti Cancer Agents Med Chem 9:904–912. doi:10/2174/187152009789124655
Shi LS, Chao CH, Shen DY, Chan HH, Chen CH, Liao YR, Wu SJ, Leu YL, Shen YC, Kuo YH, Lee EJ, Qian K, Wu TS, Lee KH (2011) Biologically active constituents from the fruiting body of Taiwanofungus camphoratus. Bioorg Med Chem 19:677–683. doi:10.1016/j.bmc.2010.10.032
Sih CJ, Ravikumar PR, Huang FC, Tuckner C, Whitlock H Jr (1976) Isolation and synthesis of pinoresinol diglucoside, a major antihypertensive principle of Tu Chung (Eucommia ulmoides, Oliver). J Am Chem Soc 98:5412–5413. doi:10.1021/ja00433a070
Singh S, Aggarwal BB (1995) Activation of transcription factor NF-kB is suppressed by curcumin (diferuloylmethane). J Biol Chem 270:24995–25000. doi:10.1074/jbc.270.42.24995
Snee LS, Nerurkar VR, Dooley DA, Efird JT, Shovic AC, Nerurkar PV (2011) Strategies to improve palatability and increase consumption intentions for Momordica charantia (bitter melon): a vegetable commonly used for diabetes management. Nutr J 10:78. doi:10.1186/1475-2891-10-78
Sowbhagya HB (2014) Chemistry, technology, and nutraceutical functions of celery (Apium graveolens L.): an overview. Crit Rev Food Sci Nutr 54:389–398. doi:10.1080/10408398.2011.586740
Tan MJ, Ye JM, Turner N, Hohnen-Behrens C, Ke CQ, Tang CP, Chen T, Weiss HC, Gesing ER, Rowland A, James DE, Ye Y (2008) Antidiabetic activities of triterpenoids isolated from bitter melon associated with activation of the AMPK pathway. Chem Biol 15:263-–273. doi:10.1016/j.chembiol.2008.01.013
Tang WM, Chan E, Kwok CY, Lee YK, Wu JH, Wan CW, Chan RY, Yu PH, Chan SW (2012) A review of the anticancer and immunomodulatory effects of Lycium barbarum fruit. Inflammopharmacology 20:307–314. doi:10.1007/s10787-011-0107-3
Thaikert R, Paisooksantivatana Y (2009) Variation of total curcuminoids content, antioxidant activity and genetic diversity in turmeric (Curcuma longa L.) collections. Kasetsart J (Nat Sci) 43:507–518
Ulbricht C, Bryan JK, Costa D, Culwell X, Giese N, Isaac R, Nummy K, Pham T, Rapp C, Rusie E, Weissner W, Sindsor RC, Woods J, Zhou S (2015) An evidence-based systematic review of goji (Lycium spp.) by the Natural Standard Research Collaboration. J Diet Suppl 12:184–240. doi:10.3109/19390211.2014.904128
Wada K, Lee JY, Hung HY, Shi Q, Lin L, Zhao Y, Goto M, Yang PC, Kuo SC, Chen HW, Lee KH (2015) Novel curcumin analogs to overcome EGFR–TKI lung adenocarcinoma drug resistance and reduce EGFR–TKI-induced GI adverse effects. Bioorg Med Chem 23:1507–1514. doi:10.1016/j.bmc.2015.02.003
Wang X, Sun W, Cao J, Qu H, Bi X, Zhao Y (2012) Structures of new triterpenoids and cytotoxicity activities of the isolated major compounds from the fruit of Momordica charantia L. J Agric Food Chem 60:3927–3933. doi:10.1021/jf204208y
Wang Q, Shen L, Ma S, Chen M, Lin X, Hong Y, Liang X, Feng Y (2015a) Effects of Ligusticum chuanxiong and Gastrodia elata on blood-brain barrier permeability in migraine rats. Pharmazie 70:421–426
Wang SN, Xie GP, Qin CH, Chen YR, Zhang KR, Li X, Wu Q, Dong WQ, Yang J, Yu B (2015b) Aucubin prevents interleukin-1 beta induced inflammation and cartilage matrix degradation via inhibition of NF-kB signaling pathway in rat articular chondrocytes. Int Immunopharmacol 24:408–415. doi:10.1016/j.intimp.2014.12.029
Wu SH, Ryvarden L (1997) Antrodia camphorata (“niu-chang-chih”), new combination of a medicinal fungus in Taiwan. Bot Bull Acad Sin Taipei 38:273–276
Wu SJ, Leu YL, Chen CH, Chaho CH, Shen DY, Chan HH, Lee EJ, Wu TS, Wang YH, Shen YC, Qian K, Bastow KF, Lee KH (2010) Camphoratins A–J, potent cytotoxic and anti-inflammatory triterpenoids from the fruiting body of Taiwanofungus camphoratus. J Nat Prod 73:1756–1762. doi:10.1021/np1002143
Wu W, Yu X, Luo XP, Yang SH, Zheng D (2013) Tetramethylpyrazine protects against scopolamine-induced memory impairments in rats by reversing the cAMP/PKA/CREB pathway. Behav Brain Res 253:212–216. doi:10.1016/j.bbr.2013.07.052
Yang SZ (translator) (1998) The Divine Farmer’s Materia Medica. Blue Poppy Press, Boulder, CO
Yao X, Peng Y, Xu LJ, Li L, Wu QL, Xiao PG (2011) Phytochemical and biological studies of Lycium medicinal plants. Chem Biodivers 8:976–1010. doi:10.1002/cbdv.201000018
Ye M, Liu SH, Jiang Z, Lee Y, Tilton R, Cheng YC (2007) Liquid chromatography/mass spectrometry analysis of PHY906, a Chinese medicine formulation for cancer therapy. Rapid Commun Mass Spectrom 21:3593–3607. doi:10.1002/rcm.2832
Yue H, Hu X, Su K, Zhai W (1999) Development of healthy beverage from Eucommia ulmoides foliage. Chin Med Herbs 22:385–387
Zeng M, Pan L, Qi S, Cao Y, Zhu H, Guo L, Zhou J (2013) Systematic review of recent advances in pharmacokinetics of four classical Chinese medicines used for the treatment of cerebrovascular disease. Fitoterapia 88:50–75. doi:10.1016/j.fitote.2013.04.006
Zhang L, Ma YL, Liu Y, Zu YB (2014) Development and validation of high liquid performance chromatography-tandem mass spectrometry method for simultaneous determination of geniposidic acid and aucubin in rat plasma for pharmacokinetic study after oral administration of Du-zhong tea extract. J Chromatogr B Anal Technol Biomed Life Sci 963:62–69. doi:10.1016/j.jchromb.2014.04.033
Zhao Y (2011) Studies on Qinghao and the Qinghaosus. Traditional Chinese Medical College, China Press, Beijing
Zhao Y, Hanton WK, Lee KH (1986) Antimalarial agents. 2. Artesunate, an inhibitor of cytochrome oxidase activity in Plasmodium berghei. J Nat Prod 49:139–142. doi:10.1021/np50043a018
Zhao Y, Hall IH, Oswald CB, Yokoi T, Lee KH (1987) Antimalarial agents. III. Mechanism of action of artesunate against Plasmodium berghei infection. Chem Pharm Bull 35:2052–2061
Zhou J, Qu F (2009) Treating gynaecological disorders with traditional Chinese medicine: a review. Afr J Tradit Complement Altern Med 6:494–517
Zhu XZ, Li XY, Liu J (2004) Recent pharmacological studies on natural products in China. Eur J Pharmacol 500:221–230. doi:10.1016/j.ejphar.2004.07.027
Acknowledgments
The authors would like to acknowledge support from three NIH grants: CA017625 and CA177584 from the National Cancer Institute and AI033066 from the Institute of Allergy and Infectious Diseases awarded to K.-H. Lee. Support in part was also received from the Taiwan Ministry of Health and Welfare Clinical Trial Center of Excellence, Taiwan (MOHW103-TDU-B-212-113002).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Singapore
About this chapter
Cite this chapter
Lee, KH., Morris-Natschke, S.L., Zhao, Y., Musgrove, K. (2016). Chinese Herbal Medicine-Derived Products for Prevention or Treatment of Diseases Affecting Quality of Life. In: Tsay, HS., Shyur, LF., Agrawal, D., Wu, YC., Wang, SY. (eds) Medicinal Plants - Recent Advances in Research and Development. Springer, Singapore. https://doi.org/10.1007/978-981-10-1085-9_1
Download citation
DOI: https://doi.org/10.1007/978-981-10-1085-9_1
Published:
Publisher Name: Springer, Singapore
Print ISBN: 978-981-10-1084-2
Online ISBN: 978-981-10-1085-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)