
Abstract
Hepatitis E virus (HEV) is globally prevalent with relatively high percentages of anti-HEV immunoglobulin G-positive individuals in the populations of developing and developed countries. There are two distinct epidemiologic patterns of hepatitis E. In areas with high disease endemicity, primarily developing countries in Asia and Africa, this disease is caused mainly by genotype 1 or 2 HEV, both of which transmit predominantly through contaminated water and occur as either outbreaks or as sporadic cases of acute hepatitis. The acute hepatitis caused by either of these two genotypes has the highest attack rate in young adults, and the disease is particularly severe among pregnant women. In developed countries, sporadic cases of locally acquired genotype 3 or 4 HEV infection are observed. The reservoir of genotype 3 and 4 HEV is believed to be animals, such as pigs, with zoonotic transmission to humans. The affected persons are often elderly, and persistent infection has been well documented among immunosuppressed persons. A subunit vaccine has been shown to be effective in preventing clinical disease and has been licensed in China.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
3.1 Introduction
Serological and molecular studies have shown that hepatitis E virus (HEV) is globally distributed and is the leading cause of enterically transmitted viral hepatitis illness worldwide. HEV infection has been reported in most countries of the world. Large annual epidemics are attributed to HEV in endemic areas, and sporadic cases are increasingly reported in developed countries. It is estimated that two billion people worldwide are infected with HEV every year with 14 million symptomatic cases and 300,000 deaths [87].
3.2 Worldwide HEV Serological Prevalence in the Human Population
Anti-HEV antibodies appear following HEV infection and can persist for several years [3, 4]. Thus, the detection of anti-HEV antibodies in blood from an individual is taken to indicate their prior exposure to HEV, and the prevalence of these antibodies may provide an epidemiological marker of the frequency of HEV exposure in a population. The prevalence of anti-HEV antibodies has been studied in various populations worldwide, and the results indicate that anti-HEV antibodies are present in persons living in all geographical areas. Tables 3.1, 3.2, 3.3, and 3.4 summarize the results reported from studies involving the collection of samples that are more or less representative of the general population of countries or regions from Asia, Europe, Africa, and the Americas.
Developing countries in Asia and Africa frequently displayed high HEV prevalence rates. In Asia, rates higher than 30 % were found among adults from India, Bangladesh, China, and Malaysia, while low rates (less than 10 % among adults) were consistently reported from Japan (Table 3.1). The anti-HEV-positive rates in most African countries are higher than 30 % (Table 3.2). In contrast, these rates are less than 20 % in most European countries (Table 3.3). The divergent anti-HEV immunoglobulin (Ig)G seroprevalence among different countries may roughly represent the geographical variations in the burden of hepatitis E infection. The prevalence of anti-HEV IgG is high in developing countries, reflecting the endemic nature of the disease in this setting.
HEV seroprevalence differs between rural and urban areas. In the general population, the positive rate of anti-HEV IgG was significantly higher in rural areas (41.7 %) than in urban areas (22.7 %) of China and in eastern Japan (5.6 %) than in western Japan (1.8 %) and varied greatly between different states/regions of the USA (range, 1.2–21.3 %) and Europe (range, 0.26–52.5 %) [31]. A difference in seroprevalence between rural and urban residents is also observed in Egypt, Mexico, and South Africa, with the seroprevalence being higher in rural areas [8, 110]. Conversely, one study in Gabon found that the HEV prevalence in urban areas (13.5 %) was over twice as high as that in rural areas (6.4 %) [20]. The population density, absence of sewer systems, consumption of bush meat, and presence of excreta from peri-domestic animals near habitations, all of which contribute to the precarious sanitary conditions in this area, might be risk factors for HEV spread.
In some countries, the seroprevalence of anti-HEV IgG has remained stable over time. The rate was approximately 5 % from 2007 to 2012 in Japan; approximately 3 % from 2000 to 2012 in Brazil, from 1999 to 2010 in Spain, and from 1994 to 2012 in Italy; and approximately 18 % from 1997 to 2013 in the USA, according to a review by [73]. In contrast, the anti-HEV IgG seroprevalence has increased over time in other countries: in Germany, from 5.5 % in 2010 to 15.5 % in 2013; in Greece, from 0.26 % in 1998 to 9.43 % in 2013; and in the Midi-Pyrénées region of France, from 16.6 % in 2008 to 52.5 % in 2011 [73]. Investigations in Pune, India [11], and Ankara, Turkey [12], showed no or minor increases in rates of HEV seropositive over time. However, a study from a tribal population of the Andaman and Nicobar Islands in India showed a significant rise in HEV seroprevalence, from 13 % in 1989 to 40 % in 1999 in children <15 years of age [79]. A few studies have addressed the issue of changing HEV seroprevalence over time in the same population, but the authors were unable to identify the specific factors responsible for this change [79].
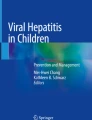
The seroprevalence of HEV seems to be higher in pregnant women than in the general population in Ghana, 28.7 % [2] vs. 4.6 % [74], and also in Gabon, 14.2 % [20] vs. 0 % [90]. In most disease-endemic areas, anti-HEV antibodies have been detected in as many as 5 % of children less than 10 years of age, and this ratio increases to 10–40 % among adults older than 25 years of age. India, Malaysia, and Southern China displayed the highest rates among children (up to 20–50 %) (Table 3.1). Overall, there appears to be a gradual increase in the anti-HEV IgG seroprevalence as the age of individuals rises (Table 3.6 and Fig. 3.1).

Anti-HEV IgG distribution in the general population of rural Durango, Mexico, according to age [7]
The wide variation in the anti-HEV antibody seroprevalence among the populations of various countries or within the same country may also be partly due to differences in the HEV antibody detection assays used to assess the seroprevalence (Table 3.5). The various commercially available tests show important differences in sensitivity. Further, the sensitivity and specificity of a test depend upon the prevalence, as well as on the viral genotype present in the study population. In a population-based cohort study, 1025 randomly selected participants were enrolled from Matlab, Bangladesh (2004–2005), and were tested for anti-HEV antibodies using an in-house enzyme immunoassay developed by the Walter Reed Army Institute of Research (WRAIR). In 2014, the banked sera of 1009 of those participants were retested using the Wantai anti-HEV IgG enzyme-linked immunosorbent assay (ELISA). The WRAIR assay estimated the overall population seroprevalence as 26.6 % (95 % confidence interval [CI], 24.0–29.5), whereas the Wantai assay produced a significantly higher estimated seroprevalence of 46.7 % (95 % CI, 43.5–49.8) (p < 0.001) [62]. Because these two tests produced nearly identical findings in those aged 5 years and below (n = 94) with a 98 % agreement between the tests [62], the different sensitivities of the two assays resulted in different seroprevalence. Thus, in the absence of standardized commercially available confirmatory assays, such as Western blots, differences in the seroprevalence rates between different populations must be interpreted with caution. Retesting populations with modern assays will be necessary to establish better population-level estimates of the HEV disease burden.
3.3 HEV Genotype Distribution Worldwide
In addition to humans, HEV infects many other wild and domestic animals, such as pigs, rabbits, rats, deer, mongoose, and chickens. The genomic sequences are different among HEV isolates from different hosts in different geographical areas. HEV is classified into the family Hepeviridae. A new proposed consensus for HEV classification [97] divides the Hepeviridae family in two genera: Orthohepevirus and Piscihepevirus. The latter currently includes only isolates from cutthroat trout. The genus Orthohepevirus is further subdivided into four species: Orthohepevirus A, with isolates from humans, pigs, wild boars, deer, mongoose, rabbits, and camels, and Orthohepevirus B, C, and D, with isolates from other mammals or from birds. Orthohepevirus A is additionally divided into at least seven genotypes (genotypes 1–7). Genotypes 1–4 are recognized to infect humans and can cause hepatitis E. Genotypes 1 and 2 are exclusively human HEV strains, whereas HEV genotypes 3 and 4 can also infect other animal species, particularly domestic pigs and wild boars. Each HEV genotype has a specific geographic distribution. The worldwide distribution of genotypes 1–4 is shown in Fig. 3.2.

Distribution of the HEV genotypes of viral isolates obtained from humans and animals (mainly pigs). The colors used for each country and the circle associated with it represent the predominant HEV genotypes of human and animal isolates, respectively, from that country (The figure is based on data from Okamoto [83] and Aggarwal [4])
3.3.1 Asia
The only HEV genotype that has been identified during the large waterborne outbreaks of HEV in India and in the neighboring South Asian countries, such as Nepal, Pakistan, and Bangladesh, is genotype 1. Additionally, HEV isolates from sporadic cases in these countries also belong to genotype 1. The nucleotide sequences of these isolates are highly homologous, indicating that genotype 1 is the dominant cause of hepatitis E disease in this region [98]. However, HEV isolates from pigs in India were identified as genotype 4 [13], indicating that different HEV genotypes can circulate in humans and pigs within the same country.
HEV strains isolated from the Xinjiang epidemic in 1988–1990, which were the first HEV strains analyzed in China, were assigned to genotype 1 [70]. Additionally, most of the HEV strains isolated prior to 2000 from regions across China also belong to genotype 1. However, genotype 4, which has been identified in most regions of China over the last 10 years, has overtaken genotype 1 in its frequency of isolation nationwide. Genotype 3 HEV strains have also been found in China and are thought to have been imported from Japan. Both genotypes 3 and 4 of HEV have been found in humans and pigs, and cross-species transmission of these two genotypes from pigs to humans may have occurred. Currently, HEV genotypes 1, 3, and 4 coexist in China, but genotype 4 is the predominant genotype in this country [70].
HEV genotypes 3 and 4 have been consistently dominant in East and Southeast Asian countries, such as Japan [58], Korea [54], and Singapore [102]. Hepatitis E shows a sporadic, non-endemic epidemiologic pattern in this area, and HEV strains of genotype 3 or 4 have been isolated from patients with autochthonous hepatitis E in these countries.
Large outbreaks and sporadic cases of hepatitis E have both been reported in Central Asia. The HEV strains isolated from outbreaks or sporadic cases in Turkmenistan were identified as belonging to genotype 1 [6]. In Kyrgyzstan, another Central Asian country, genotype 1 HEV strains were detected from patients during an outbreak, while the HEV strains detected from pigs in this country belong to HEV genotype 3 [71].
3.3.2 Africa
Data on the circulating HEV genotypes are available for nine African countries [61]. Based on these limited data, genotype 1 appears to be the most prevalent HEV genotype in Africa, as it was found in the Central African Republic [35], Sudan [82], Chad [82, 111], Egypt [15, 26], and Namibia [47]. Genotype 2 HEV, which was first reported in an outbreak in Mexico, was subsequently identified in patients in West Africa, Nigeria [18], Chad Nicand [35, 82], and Namibia [47, 72]. Genotype 3 HEV is rare in African countries and was found in one Egyptian child [57] and in one acute hepatitis patient in Mayotte (originally from France) [33]. Studies of Ghanaians suggest that the anti-HEV antibody seroprevalence among pig handlers is over 34 % and that the predominant HEV genotypes in Ghana may be of zoonotic origin [1, 2].
Notably, the HEV genotype distribution can differ between neighboring countries, as was demonstrated by one study in Sudan and Chad reporting that genotype 1 HEV was more common in Sudan, while genotype 2 HEV was more common in Chad [82].
3.3.3 America
Genotype 3 HEV was first identified in human cases of locally acquired hepatitis E in the USA [65, 92]. However, the incident rates of hepatitis E are relatively low in the USA and in Canada. Only a few of the reported acute hepatitis E cases were acquired domestically. All of the HEV strains isolated from patients without a history of travel to a foreign county were identified as genotype 3 [30, 106, 118]. Genotype 3 HEV is also prevalent in pigs in North America.
In Latin America, molecular characterization studies identified the prototype strain for genotype 2 HEV (M74506) on the basis of characterization of a single strain, but subsequent studies found that some cases in this area were caused by genotype 3 HEV strains [32]. Epidemic outbreaks and sporadic cases of hepatitis E were also reported from Cuba; the 23 HEV strains recovered from two outbreaks and from 12 sporadic cases were all clustered within genotype 1 in phylogenetic trees [114]. In recent studies performed in Venezuela, the sequences of two strains of HEV genotype 1 and of one strain of HEV genotype 3 were detected in three sporadic cases. Genotype 3 HEV RNA was also found in samples from hepatitis E patients in Argentina, Brazil, Uruguay, and Southwest Bolivia [29, 76, 78]. These data confirm the co-circulation of HEV genotypes 1 and 3 in the Caribbean region. However, additional findings are still needed to confirm the presence of HEV genotype 2 in Mexico.
3.3.4 Europe
Since the 1990s, travel-associated imported cases of HEV infection have been reported in many European countries: in the UK from India and Saudi Arabia; in the Netherlands from Bangladesh, Somalia, and the Middle East; and in Sweden and Turkey [67]. The clinical features of these patients were similar to those in HEV-endemic countries, and all of the HEV strains linked to these imported infections belong to genotype 1. In contrast, most of the hepatitis E cases in European countries, such as the UK, Germany, Dutch, Spain, Sweden, Czech Republic, and France, in which the infection was acquired from within Europe, rather than from travel outside of this area, are caused by HEV genotype 3 [9, 67]. Therefore, genotype 3 HEV is considered to be the autochthonous type in Europe.
In 2008, a genotype 4 HEV infection was reported in a German patient with no travel history [117]. A genotype 4 HEV strain was then detected in Belgian swine in 2011 [44], and the first autochthonous genotype 4 infection was reported in France [105], followed by two other cases in southern France associated with the consumption of uncooked pork liver sausage [23]. In 2011, 280 HEV RNA-positive infections were identified by the National Reference Centre for HAV and HEV, including nine infections due to HEV genotype 4 [53]. During 2011, five persons in the area of Lazio, Italy, were infected with a strain of HEV genotype 4 that showed high sequence homology with HEV isolates from swine in China [40]. These patients all lived in the same area and did not travel to disease-endemic areas, and epidemiologic information was unable to identify the transmission route. Strong sequence similarity (>96 %) was observed between the HEV isolates from human cases in northern and southern France and the strain isolated from swine in Belgium [16]. Overall, HEV genotypes 3 and 4 overlap in Europe, but genotype 3 seems to be more prevalent.
3.3.5 New Zealand and Australia
In New Zealand, HEV genotype 3 was isolated from four patients with unexplained hepatitis [25]. In Australia, there are few reported cases of locally acquired HEV; cases of hepatitis E are mainly travelers returning from disease-endemic countries [96]. Data from the Commonwealth Department of Health in Australia indicate that there were 378 reported HEV cases from 1999 to 2013, with an average of 25 cases per year, but the genotypes of the HEV strains responsible for these cases were not defined [96].
3.4 Epidemiologic Patterns of HEV Infection
HEV is considered hyperendemic in many developing countries, such as India, Bangladesh, Egypt, Mexico, and China. According to the Centers for Disease Control and Prevention, USA, hyperendemic countries carry a prevalence of 25 % of all non-A, non-B acute hepatitis cases or have experienced a major waterborne outbreak of hepatitis E; in contrast, HEV is considered endemic in places with a quantifiable prevalence of all reported non-A, non-B acute hepatitis that is less than 25 % [121]. Endemic countries and regions include much of Western Europe, the USA, New Zealand, many countries in South America, much of Asia, and the Middle East [121]. In these places, HEV infection is infrequent and occasionally occurs as sporadic cases [86].
Distinctly different epidemiologic patterns have been observed in the geographical regions where hepatitis E is hyperendemic compared with those in areas where it is endemic. These two distinct patterns seem to correlate with the distribution of HEV genotypes, disease prevalence, frequencies of various transmission routes, affected population groups, and clinical characteristics of the disease (Table 3.7).
3.4.1 The Epidemiologic Patterns of Infection with HEV Genotypes 1 and 2
Hepatitis E in hyperendemic areas, located in tropical and subtropical regions with poor sanitation, has characteristic epidemiological features. Namely, it occurs as both an epidemic and a sporadic disease, affects a large part of the population, and is largely due to genotype 1 or genotype 2 HEV strains.
3.4.1.1 Reservoirs of HEV Genotypes 1 and 2 in Endemic Regions
In hyperendemic countries, hepatitis E is a waterborne infection caused mainly by genotype 1 or genotype 2 HEV. Because neither HEV genotype 1 nor HEV genotype 2 has ever been isolated from animals and both of these genotypes failed to infect pigs in experimental studies, zoonotic transmission appears unlikely to be responsible for the prevalence of HEV of these two genotypes. Their potential reservoir may be a continuously circulating pool of individuals with clinical or subclinical HEV infection. Punctuated by occasional dramatic outbreaks involving thousands or tens of thousands of cases, sporadic HEV cases occur throughout the year, and together these infections likely contribute to the HEV reservoir that is responsible for maintaining the disease in a given population [4].
The detection of HEV genotypes 1 and 2 in sewage indicates that it may play an important role as an environmental reservoir of HEV [49]. Studies of cynomolgus macaques experimentally infected with HEV found that infection in this model produces protracted viremia and prolonged fecal shedding of HEV [5, 46]. Similar fecal shedding of the virus by persons with subclinical HEV infection could lead to the continuous maintenance of a source of infection in a disease-endemic area. This pool of infection could, in turn, lead to periodic contamination of drinking water supplies.
3.4.1.2 Outbreaks of Hepatitis E
Outbreaks of hepatitis E have been documented exclusively in resource-limited countries or in regions undergoing a humanitarian emergency, where there were overcrowding and limited access to potable water, proper sanitation, and hygiene. Hepatitis E outbreaks have been reported in Asia, the Middle East, North and West Africa, and Central America (Mexico), which are all considered to be hyperendemic areas of HEV infection. HEV outbreaks can generally be traced back to contaminated water sources and may affect several hundreds to several thousands of individuals. The occurrence and magnitude of outbreaks are strongly associated with the hygienic conditions and population density (Table 3.8).
The first retrospectively (serologically) confirmed HEV outbreak occurred in New Delhi, India, in 1955–1956 with more than 29,000 symptomatic jaundiced persons [115]. In India, HEV is responsible for large outbreaks, and the source of infection is usually a contaminated water supply. According to the surveillance across all Indian states conducted by the National Integrated Disease Surveillance Programme (IDSP) in India [63], 291 hepatitis outbreaks were reported to the IDSP during 2011–2013. Twenty-three (65.7 %) of the 35 states in India reported at least one hepatitis outbreak, and five states reported more than 20 outbreaks. Among the 163 reported outbreaks with known etiology, 78 (48 %) were caused by hepatitis E, and 19 (12 %) were caused by both hepatitis A and E. Additionally, contaminated drinking water was identified as the cause for 72 % (109 of 151) of the hepatitis A and E outbreaks and was implicated in 49 (38 %) of the 128 outbreaks for which laboratory confirmation was not available. More outbreaks were reported from rural areas (199/291, 68 %) than from urban areas (92/291, 32 %). The large number of hepatitis A and E outbreaks in India might be explained in part by the lack of adequate sewage and sanitation systems; defecation in open fields, which can contaminate surface drinking water sources, remains a common practice in this region [63].
The first documented outbreak of HEV infection in Africa likely occurred in 1950 in Tunisia, and HEV outbreaks have been detected in 11 African countries since the 1980s [103]. In recent years, some hepatitis E outbreaks have been reported from areas in Africa with conflict, violence, and major human displacement [61, 103]. Several HEV outbreaks have occurred in refugee camps. From April 2014 to January 2015, a total of 1117 suspected cases of HEV, with 21 (1.9 %) deaths, were reported among refugees residing in the Gambella region [17]. The limited availability of facilities for safe drinking water or for the proper disposal of human feces in refugee camps appears to have been the main cause for the spread of HEV infection [17].
In North America, two outbreaks of hepatitis E took place in two Mexican villages in 1986–1987. In the village of Huitzila, 94 icteric cases were found among their 1157 residents; of these, two patients died. In Telixtac, 129 icteric cases were recorded among their 2194 inhabitants, with death reported in one patient [112]. Hepatitis E has not been reported since from Mexico; nevertheless, the country is considered hyperendemic for HEV [59].
Hepatitis E incidence in South Asia has been characterized by marked seasonality, with outbreaks occurring during the rainy or monsoon seasons. These epidemics have been documented in April and October in countries such as India, Bangladesh, and Nepal [22, 42, 63].
During outbreaks, HEV mainly targets young to middle-aged adults, generally 15–40 years of age, with a significantly lower seroprevalence in individuals <10 years old. Overall the attack rates during hepatitis E outbreaks range from 1 to 15 %, with males generally outnumbering females (male/female ratio = 2–3:1), suggesting that males are more likely to be affected by hepatitis E than females. In outbreaks in Pakistan and Nepal, the ratios of patients with mild anicteric symptoms to patients with severe jaundice were 4:1 and 3:1, respectively [99].
The clinical symptoms of HEV infection are typical of acute viral hepatitis and include jaundice, malaise, anorexia, nausea, abdominal pain, fever, and hepatomegaly; anicteric hepatitis is also observed [80]. The disease is self-limiting, and no chronic sequelae are generally reported. A unique clinical feature of HEV infection is its increased incidence and severity in pregnant women, with mortality rates of 15–20 % [60]. Pregnant women with jaundice and acute viral hepatitis due to HEV showed higher mortality rates and worse obstetric and fetal outcomes than those with other types of viral hepatitis [85].
3.4.1.3 Sporadic Hepatitis E in High-Endemic Regions
In HEV-endemic areas, epidemics of hepatitis E are more frequent and are usually separated by a few years. A periodicity of 5–10 years has been suggested for recurring HEV epidemics in India, China, and certain Central Asian republics of the former Soviet Union. Cyclic outbreaks have been documented in the tropics of Asia and Africa. In hyperendemic regions, hepatitis E continues to occur between epidemics in the form of sporadic hepatitis, irrespective of the age group [4]. In India, although the peak incidence occurs during the rainy season, low levels of HEV infection continue through the winter [9]. In the high-endemic regions, the sporadic patients and those patients during hepatitis E outbreaks share several epidemiological and clinical characteristics, such as predominant affliction of adolescents and young adults, the association between pregnancy and severe disease, and clinical presentation as acute hepatitis.
3.4.2 Epidemiologic Pattern of HEV Infection in Industrialized Countries
In contrast to the larger epidemics and outbreaks of genotype 1 and genotype 2 HEV in developing countries, autochthonous hepatitis E in industrialized countries is considered prevalent but is only limited to sporadic cases caused by HEV genotype 3 or genotype 4. Pigs, and likely many other animals, are natural reservoirs of HEV genotypes 3 and 4, and most infections are related to zoonotic transmission (details in Chap. 6).
HEV genotypes 3 and 4 seem to be much less virulent in humans than HEV genotypes 1 and 2. In immunocompetent individuals, HEV infections are usually asymptomatic and have no consequences. A careful investigation performed on people involved in an outbreak of genotype 3 HEV infection associated with shellfish intake among the passengers of a cruise ship found 11 cases of acute hepatitis and 22 asymptomatic infections [91]. A large prospective vaccination study in China showed that fewer than 5 % of those exposed to genotype 4 HEV develop signs of acute hepatitis E [124]. Another study reported that, as in adults, hepatitis E caused by genotype 3 HEV is very rarely symptomatic in children [116]. Additionally, in agreement with the typical male-to-female infection rate for HEV, an analysis of sporadic cases of acute hepatitis due to genotype 3 HEV found that the likelihood of infection was significantly higher among men than among women [91].
In recent years, the number of reported HEV cases in many developed countries has risen sharply, whereas the detected prevalence of antibodies against HEV in serum has remained fairly constant [88]. This observation suggests that the increase in cases of hepatitis E reported to the Robert Koch Institute likely arises from an increased awareness, rather than an increased incidence, of this disease [88]. An increase in the number of HEV infections acquired in developed countries and the discovery of chronic hepatitis E in immunosuppressed individuals have dispelled the perception of hepatitis E as merely an acute tropical illness, thus lending new importance to this infectious disease.
3.4.3 The Shifting Epidemiologic Pattern of Hepatitis E in China
China is generally considered to be an HEV-endemic area. The extended waterborne outbreak of 1989 in Xinjiang Province, northwestern China, resulted in 120,000 cases. The outbreak was caused by HEV genotype 1 and affected mainly young adults. Since then, a couple of outbreaks of different scales caused by genotype 1 HEV have been reported in different geographical areas. However, since 2000, hepatitis E has mainly occurred as sporadic cases and occasional food-borne outbreaks, and no HEV outbreaks have been reported in recent years, suggesting a transition from a high-endemicity pattern to a low-endemicity pattern. Currently, the predominant circulating HEV genotype is genotype 4, with only occasional genotype 1 cases, and the sporadic cases of hepatitis E are more common in elderly men [41, 70]. This pattern of infection is similar to that seen in Europe with genotype 3 HEV.
The trend of diminishing numbers of HEV outbreaks is in accordance with the shift in the prevalence of HEV genotypes over the past 20 years that has been observed in China and some other countries. The reason for this shift toward genotype 4 HEV as the predominant genotype in China is unclear, but it might reflect the improvements in water supply and sanitary conditions in China over the past few decades, allowing zoonotically transmitted genotype 4 HEV to become dominant in the human population.
3.5 HEV Prevention and Control
As an enterically transmitted virus, HEV is primarily transmitted by the contamination of drinking water and undercooked meat products. Proper disposal of human feces, consumption of clean water, sanitary handling and proper cooking of meat products, and education about personal hygiene help prevent this disease.
Passive immunoprophylaxis with antibodies against HEV capsid was successful in treating hepatitis E in cynomolgus monkeys [108]. Although there are four HEV genotypes, all known HEV strains share common epitopes on their capsid genes, suggesting that they belong to a single serotype [93]. Therefore, a protective vaccine against a broad spectrum of HEV isolates should be possible. Various recombinant capsid proteins expressed in insect cells and Escherichia coli were reported to be successful recombinant vaccines conferring protection against both homologous and heterologous HEV strains [33, 69, 109]. Two subunit vaccines have been developed against HEV infection and have been shown to be highly protective against clinical hepatitis E in clinical trials [95, 124]. The first of these vaccines is a 56-kDa protein encoded by the ORF2 of a genotype 1 HEV strain that is expressed in insect cells. In a trial among 2000 volunteer Nepalese soldiers, three doses of 20 μg of the 56-kDa protein (at 0, 1, and 6 months) achieved 100 % seroconversion and a protective efficacy of up to 95.5 % (95 % CI, 85.6–98.6 %) during a 2-year follow-up [95]. The second vaccine, a 26-kDa protein encoded by the ORF2 of a genotype 1 HEV strain, is expressed in E. coli and occurs as viruslike particles of 23 nm in diameter [124]. In the phase II study and the phase III trial, this vaccine was found to be safe and immunogenic, and it conferred protection against HEV infection [122, 124]. This vaccine has been licensed with the commercial name of Hecolin for use in China since 2012. A study addressing the long-term efficacy of this vaccine was carried out over 4.5 years in which the efficacy, immunogenicity, and safety of the vaccine were evaluated in a vaccinated group of 56,302 participants in comparison with a control group of 56,302 participants. In this study, 60 cases of hepatitis E were identified, of which only seven belonged to the vaccinated group, revealing that the efficacy of this vaccine is 87 %. No issues concerning the safety of the vaccine were observed [123]. The use of the vaccine should be considered to mitigate or prevent outbreaks of hepatitis E infection, especially in high-risk groups, such as pregnant women.
3.6 Conclusion
Hepatitis E is highly endemic in several developing countries in Asia and Africa where contamination of water supplies and lack of adequate sanitation are frequent. In developed countries, autochthonous cases of HEV infection are sporadic, and the importance of animal reservoirs has become clear. The clinical and epidemiological characteristics of hepatitis E in hyperendemic and endemic countries are summarized as follows:
In Developing Countries
-
Hepatitis E occurs as outbreaks or sporadic cases.
-
Outbreaks are generally caused by genotype 1 or genotype 2 HEV strains through water contamination.
-
The highest attack rate appears to be among individuals between 15 and 40 years of age.
-
HEV infection is self-limited and has no chronic sequelae.
-
Hepatitis E occurs more often in pregnant women than in nonpregnant women or men, and pregnant women with hepatitis E have a high mortality rate (10–25 %).
In Developed Countries
-
Hepatitis E is mostly caused by HEV of genotype 3 or 4.
-
The main routes of HEV transmission are probably zoonotic and food-borne; person-to-person transmission is rare.
-
The estimated HEV infection incidence varies among different age groups, and the males of aged 50 years or older account for most of the total patients.
-
Chronic HEV infections have been observed in immunocompromised individuals.
Abbreviations
- ELISA:
-
Enzyme-linked immunosorbent assay
- HEV:
-
Hepatitis E virus
References
Adjei AA, Tettey Y, Aviyase JT, Adu-Gyamfi C, Mingle JA, Nartey ET (2010) Unexpected elevated alanine aminotransferase, aspartate aminotransferase levels and hepatitis E virus infection among persons who work with pigs in accra. Ghana Virol J 7:336
Adjei AA, Tettey Y, Aviyase JT, Adu-Gyamfi C, Obed S, Mingle JA et al (2009) Hepatitis E virus infection is highly prevalent among pregnant women in Accra. Ghana Virol J 6:108
Aggarwal R (2013) Diagnosis of hepatitis E. Nat Rev Gastroenterol Hepatol 10(1):24–33
Aggarwal R (2013) Hepatitis E: epidemiology and natural history. J Clin Exp Hepatol 3(2):125–133
Aggarwal R, Kamili S, Spelbring J, Krawczynski K (2001) Experimental studies on subclinical hepatitis E virus infection in cynomolgus macaques. J Infect Dis 184(11):1380–1385
Albetkova A, Drobeniuc J, Yashina T, Musabaev E, Robertson B, Nainan O et al (2007) Characterization of hepatitis E virus from outbreak and sporadic cases in Turkmenistan. J Med Virol 79(11):1696–1702
Alvarado-Esquivel C, Sanchez-Anguiano LF, Hernandez-Tinoco J (2014) Seroepidemiology of hepatitis E virus infection in general population in rural durango, Mexico. Hepat Mon 14(6):e16876
Alvarado-Esquivel C, Sanchez-Anguiano LF, Hernandez-Tinoco J (2015) Seroepidemiology of hepatitis E virus infection in mennonites in Mexico. J Clin Med Res 7(2):103–108
Aniţă A, Gorgan L, Aniţă D, Oşlobanu L, Pavio N, Savuţa G (2014) Evidence of hepatitis E infection in swine and humans in the east region of Romania. Int J Infect Dis 29:232–237
Arankalle VA, Chobe LP, Jha J, Chadha MS, Banerjee K, Favorov MO et al (1993) Aetiology of acute sporadic non-A, non-B viral hepatitis in India. J Med Virol 40(2):121–125
Arankalle VA, Tsarev SA, Chadha MS, Alling DW, Emerson SU, Banerjee K et al (1995) Age-specific prevalence of antibodies to hepatitis A and E in Pune, India, 1982 and 1992. J Infect Dis 171(2):447–450
Atabek ME, Fýndýk D, Gulyuz A, Erkul I (2004) Prevalence of anti-HAV and anti-HEV antibodies in Konya, Turkey. Health Policy 67(3):265–269
Begum N, Polipalli SK, Husain SA, Kar P (2010) Molecular analysis of swine hepatitis E virus from north India. Indian J Med Res 132:504–508
Bernal W, Smith HM, Williams R (1996) A community prevalence study of antibodies to hepatitis A and E in inner-city London. J Med Virol 49(3):230–234
Blackard JT, Rouster SD, Nady S, Galal G, Marzuuk N, Rafaat MM et al (2009) Genotypic characterization of symptomatic hepatitis E virus (HEV) infections in Egypt. J Clin Virol 46(2):140–144
Bouamra Y, Gérolami R, Arzouni JP, Grimaud JC, Lafforgue P, Nelli M et al (2014) Emergence of autochthonous infections with hepatitis E virus of genotype 4 in Europe. Intervirology 57(1):43–48
Browne LB, Menkir Z, Kahi V, Maina G, Asnakew S, Tubman M et al (2015) Notes from the field: hepatitis E outbreak among refugees from South Sudan-Gambella, Ethiopia, April 2014-January 2015. MMWR Morb Mortal Wkly Rep 64(19):537
Buisson Y, Grandadam M, Nicand E, Cheval P, van Cuyck-Gandre H, Innis B et al (2000) Identification of a novel hepatitis E virus in Nigeria. J Gen Virol 81(Pt4):903–909
Burans JP, Sharp T, Wallace M, Longer C, Thornton S, Batchelor R et al (1994) Threat of hepatitis E virus infection in Somalia during Operation Restore Hope. Clin Infect Dis 18(1):100–102
Caron M, Kazanji M (2008) Hepatitis E virus is highly prevalent among pregnant women in Gabon, central Africa, with different patterns between rural and urban areas. Virol J 5:158
Chiu DM, Chan MC, Yeung AC, Ngai KL, Chan PK (2013) Seroprevalence of hepatitis E virus in Hong Kong, 2008–2009. J Med Virol 85(3):459–461
Clayson ET, Vaughn DW, Innis BL, Shrestha MP, Pandey R, Malla DB (1998) Association of hepatitis E virus with an outbreak of hepatitis at a military training camp in Nepal. J Med Virol 54(3):178–182
Colson P, Romanet P, Moal V, Borentain P, Purgus R, Benezech A et al (2012) Autochthonous infections with hepatitis E virus genotype 4, France. Emerg Infect Dis 18(8):1361–1364
Corwin AL, Kheim HB, Clayson ET, Pham KS, Vo TT, Vu TY et al (1996) A waterborne outbreak of hepatitis E virus transmission in southwestern Vietnam. Am J Trop Med Hyg 54(6):559–562
Dalton HR, Fellows HJ, Gane EJ, Wong P, Gerred S, Schroeder B et al (2007) Hepatitis E in new zealand. J Gastroenterol Hepatol 22(8):1236–1240
Delarocque-Astagneau E, Abravanel F, Moshen A, Le Fouler L, Gad RR, El-Daly M et al (2012) Epidemiological and virological characteristics of symptomatic acute hepatitis E in Greater Cairo, Egypt. Clin Microbiol Infect 18(10):982–988
Dell’Amico MC, Cavallo A, Gonzales JL, Bonelli SI, Valda Y, Pieri A et al (2011) Hepatitis E virus genotype 3 in humans and Swine, Bolivia. Emerg Infect Dis 17(8):1488–1490
Ditah I, Ditah F, Devaki P, Ditah C, Kamath PS, Charlton M (2014) Current epidemiology of hepatitis E virus infection in the United States: low seroprevalence in the National Health and Nutrition Evaluation Survey. Hepatology 60(3):815–822
dos Santos DR, Vitral CL, de Paula VS, Marchevsky RS, Lopes JF, Gaspar AM et al (2009) Serological and molecular evidence of hepatitis E virus in swine in Brazil. Vet J 182(3):474–480
Drobeniuc J, Greene-Montfort T, Le NT, Mixson-Hayden TR, Ganova-Raeva L, Dong C et al (2013) Laboratory-based surveillance for hepatitis E virus infection, United States, 2005–2012. Emerg Infect Dis 19(2):218–222
Echevarría JM (2014) Light and darkness: prevalence of hepatitis E virus infection among the general population. Scientifica (Cairo) 2014:481016
Echevarría JM, González JE, Lewis-Ximenez LL, Dos Santos DR, Munné MS, Pinto MA et al (2013) Hepatitis E virus infection in Latin America: a review. J Med Virol 85(6):1037–1045
Emerson SU, Purcell RH (2001) Recombinant vaccines for hepatitis E. Trends Mol Med 7:462–466
Epelboin L, Nicand E, Roussin C, Lernout T, Pettinelli ME, Tesse S et al (2011) A sporadic case of genotype 3f acute hepatitis E in Mayotte. Med Mal Infect 41(7):392–394
Escriba JM, Nakoune E, Recio C, Massamba PM, Matsika-Claquin MD, Goumba C et al (2008) Hepatitis E, Central African Republic. Emerg Infect Dis 14(4):681–683
Faber MS, Wenzel JJ, Jilg W, Thamm M, Höhle M, Stark K (2012) Hepatitis E virus seroprevalence among adults, Germany. Emerg Infect Dis 18(10):1654–1657
Farshadpour F, Taherkhani R, Makvandi M (2015) Prevalence of Hepatitis E Virus among Adults in South-West of Iran. Hepat Res Treat 2015:759589
Fix AD, Abdel-Hamid M, Purcell RH, Shehata MH, Abdel-Aziz F, Mikhail N et al (2000) Prevalence of antibodies to hepatitis E in two rural Egyptian communities. Am J Trop Med Hyg 62(4):519–523
Fogeda M, Avellón A, Echevarría JM (2012) Prevalence of specific antibody to hepatitis E virus in the general population of the community of Madrid, Spain. J Med Virol 84(1):71–74
Garbuglia AR, Scognamiglio P, Petrosillo N, Mastroianni CM, Sordillo P, Gentile D et al (2013) Hepatitis E virus genotype 4 outbreak, Italy, 2011. Emerg Infect Dis 19(1):110–114
Geng Y, Zhao C, Fan J, Harrison TJ, Zhang H, Lian H et al (2013) Genotype analysis of hepatitis E virus from sporadic hepatitis E cases in northern China. Infect Genet Evol 20:413–417
Gurley ES, Hossain MJ, Paul RC, Sazzad HM, Islam MS, Parveen S et al (2014) Outbreak of hepatitis E in urban bangladesh resulting in maternal and perinatal mortality. Clin Infect Dis 59(5):658–665
Guthmann JP, Klovstad H, Boccia D, Hamid N, Pinoges L, Nizou JY et al (2006) A large outbreak of hepatitis E among a displaced population in Darfur, Sudan, 2004: the role of water treatment methods. Clin Infect Dis 42(12):1685–1691
Hakze-van der Honing RW, van Coillie E, Antonis AF, van der Poel WH (2011) First isolation of hepatitis E virus genotype 4 in Europe through swine surveillance in the Netherlands and Belgium. PLoS One 6(8):e22673
Haque F, Banu SS, Ara K, Chowdhury IA, Chowdhury SA, Kamili S et al (2015) An outbreak of hepatitis E in an urban area of Bangladesh. J Viral Hepat 22(11):948–956
Han J, Lei Y, Liu L et al (2014) SPF rabbits infected with rabbit hepatitis E virus isolate experimentally showing the chronicity of hepatitis. PLoS One 9(6):e99861
He J, Binn LN, Tsarev SA, Hayes CG, Frean JA, Isaacson M et al (2000) Molecular characterization of a hepatitis E virus isolate from Namibia. J Biomed Sci 7(4):334–338
Ibarra H, Riedemann S, Reinhardt G, Frieck P, Siegel F, Toledo C et al (1997) Prevalence of hepatitis E virus antibodies in blood donors and other population groups in southern Chile. Rev Med Chil 125(3):275–278
Ippagunta SK, Naik S, Sharma B, Aggarwal R (2007) Presence of hepatitis E virus in sewage in northern India: frequency and seasonal pattern. J Med Virol 79:1827–1831
Ijaz S, Vyse AJ, Morgan D, Pebody RG, Tedder RS, Brown D (2009) Indigenous hepatitis E virus infection in England: more common than it seems. J Clin Virol 44(4):272–276
Izopet J, Labrique AB, Basnyat B, Dalton HR, Kmush B, Heaney CD et al (2015) Hepatitis E virus seroprevalence in three hyperendemic areas: Nepal, Bangladesh and southwest France. J Clin Virol 70:39–42
Jacobs C, Chiluba C, Phiri C, Lisulo MM, Chomba M, Hill PC et al (2014) Seroepidemiology of hepatitis E virus infection in an urban population in Zambia: strong association with HIV and environmental enteropathy. J Infect Dis 209(5):652–657
Jeblaoui A, Haim-Boukobza S, Marchadier E, Mokhtari C, Roque-Afonso AM (2013) Genotype 4 hepatitis e virus in france: an autochthonous infection with a more severe presentation. Clin Infect Dis 57(4):e122–e126
Jeong SH (2011) Current status of hepatitis e virus infection in Korea. Gut Liver 5(4):427–431
Jia Z, Yi Y, Liu J, Cao J, Zhang Y, Tian R et al (2014) Epidemiology of hepatitis E virus in China: results from the Third National Viral Hepatitis Prevalence Survey, 2005–2006. PLoS One 9(10):e110837
Kamar N, Dalton HR, Abravanel F, Izopet J (2014) Hepatitis E virus infection. Clin Microbiol Rev 27(1):116–138
Kamel AH, Ali MA, El-Nady HG, Deraz A, Aho S, Pothier P et al (2011) Presence of enteric hepatitis viruses in the sewage and population of Greater Cairo. Clin Microbiol Infect 17(8):1182–1185
Kanayama A, Arima Y, Yamagishi T, Kinoshita H, Sunagawa T, Yahata Y et al (2015) Epidemiology of domestically acquired hepatitis E virus infection in Japan: assessment of the nationally reported surveillance data, 2007–2013. J Med Microbiol 64(7):752–758
Khuroo MS (2011) Discovery of hepatitis E: the epidemic non-A, non-B hepatitis 30 years down the memory lane. Virus Res 161(1):3–14
Khuroo MS (1980) Study of an epidemic of non-A non-B hepatitis; possibility of another human hepatitis virus distinct from post-transfusion non-A, non-B type. Am J Med 68(6):818–824
Kim JH, Nelson KE, Panzner U, Kasture Y, Labrique AB, Wierzba TF (2014) A systematic review of the epidemiology of hepatitis E virus in Africa. BMC Infect Dis 14:308
Kmush BL, Labrique AB, Dalton HR, Ahmed ZB, Ticehurst JR, Heaney CD et al (2015) Two generations of “gold standards”: the impact of a decade in hepatitis E virus testing innovation on population seroprevalence. Am J Trop Med Hyg 93(4):714–717
Kumar T, Shrivastava A, Kumar A, Laserson KF, Narain JP, Venkatesh S et al (2015) Viral hepatitis surveillance – India, 2011–2013. MMWR Morb Mortal Wkly Rep 64(28):758–762
Kuniholm MH, Purcell RH, McQuillan GM, Engle RE, Wasley A, Nelson KE (2009) Epidemiology of hepatitis E virus in the United States: results from the third national health and nutrition examination survey, 1988–1994. J Infect Dis 200(1):48–56
Kwo PY, Schlauder GG, Carpenter HA, Murphy PJ, Rosenblatt JE, Dawson GJ et al (1997) Acute hepatitis E by a new isolate acquired in the United States. Mayo Clin Proc 72(12):1133–1136
Labrique AB, Zaman K, Hossain Z, Saha P, Yunus M, Hossain A et al (2010) Epidemiology and risk factors of incident hepatitis E virus infections in rural Bangladesh. Am J Epidemiol 172(8):952–961
Lapa D, Capobianchi MR, Garbuglia AR (2015) Epidemiology of hepatitis E virus in European countries. Int J Mol Sci 16(10):25711–25743
Li RC, Ge SX, Li YP, Zheng YJ, Nong Y, Guo QS et al (2006) Seroprevalence of hepatitis E virus infection, rural southern People’s Republic of China. Emerg Infect Dis 12(11):1682–1688
Li SW, Zhang J, Li YM, Ou SH, Huang GY, He ZQ et al (2005) A bacterially expressed particulate hepatitis E vaccine: antigenicity, immunogenicity and protectivity on primates. Vaccine 23(22):2893–2901
Liu P, Li L, Wang L, Bu Q, Fu H, Han J et al (2012) Phylogenetic analysis of 626 hepatitis E virus (HEV) isolates from humans and animals in China (1986–2011) showing genotype diversity and zoonotic transmission. Infect Genet Evol 12(2):428–434
Lu L, Drobeniuc J, Kobylnikov N, Usmanov RK, Robertson BH, Favorov MO et al (2004) Complete sequence of a Kyrgyzstan swine hepatitis E virus (HEV) isolated from a piglet thought to be experimentally infected with human HEV. J Med Virol 74(4):556–562
Maila HT, Bowyer SM, Swanepoel R (2004) Identification of a new strain of hepatitis E virus from an outbreak in Namibia in 1995. J Gen Virol 85(Pt 1):89–95
Marano G, Vaglio S, Pupella S, Facco G, Bianchi M, Calizzani G et al (2015) Hepatitis E: an old infection with new implications. Blood Transfus 13(1):6–17
Meldal BH, Sarkodie F, Owusu-Ofori S, Allain JP (2012) Hepatitis E virus infection in Ghanaian blood donors – the importance of immunoassay selection and confirmation. Vox Sang 104(1):30–36
Minuk GY, Sun A, Sun DF, Uhanova J, Nicolle LE, Larke B et al (2007) Serological evidence of hepatitis E virus infection in an indigenous North American population. Can J Gastroenterol 21(7):439–442
Mirazo S, Ramos N, Russi JC, Gagliano G, Arbiza J (2011) Detection and molecular characterization of sporadic cases of acute human hepatitis E virus infection in Uruguay. Arch Virol 156(8):1451–1454
Mor O, Bassal R, Michaeli M, Wax M, Ram D, Cohen-Ezra O et al (2015) Prevalence of hepatitis E virus antibodies, Israel, 2009–2010. Emerg Infect Dis 21(4):692–694
Munné MS, Vladimirsky S, Otegui L, Castro R, Brajterman L, Soto S et al (2006) Identification of the first strain of swine hepatitis E virus in South America and prevalence of anti-HEV antibodies in swine in Argentina. J Med Virol 78(12):1579–1583
Murhekar MV, Sehgal SC, Murhekar KM, Padbhidri SB, Chitambar SD, Arankalle VA (2002) Changing scenario of hepatitis A virus and hepatitis E virus exposure among the primitive tribes of Andaman and Nicobar Islands, India over the 10-year period 1989–99. J Viral Hepat 9(4):315–321
Mushahwar IK (2008) Hepatitis E, virus: molecular virology, clinical features, diagnosis, transmission, epidemiology, and prevention. J Med Virol 80(4):646–658
Naik SR, Aggarwal R, Salunke PN, Mehrotra NN (1992) A large waterborne viral hepatitis E epidemic in Kanpur, India. Bull World Health Organ 70(5):597–604
Nicand E, Armstrong GL, Enouf V, Guthmann JP, Guerin JP, Caron M et al (2005) Genetic heterogeneity of hepatitis E virus in Darfur, Sudan, and neighboring Chad. J Med Virol 77(4):519–521
Okamoto H (2007) Genetic variability and evolution of hepatitis E virus. Virus Res 127(2):216–228
Park HK, Jeong SH, Kim JW, Woo BH, Lee DH, Kim HY et al (2012) Seroprevalence of anti-hepatitis E virus (HEV) in a Korean population: comparison of two commercial anti-HEV assays. BMC Infect Dis 12:142
Patra S, Kumar A, Trivedi SS, Puri M, Sarin SK (2007) Maternal and fetal outcomes in pregnant women with acute hepatitis E virus infection. Ann Intern Med 147(1):28–33
Pérez-Gracia MT, García M, Suay B, Mateos-Lindemann ML (2015) Current knowledge on hepatitis E. J Clin Transl Hepatol 2:117–126
Pérez-Gracia MT, Mateos Lindemann ML, Caridad Montalvo Villalba M (2013) Hepatitis E: current status. Rev Med Virol 23(6):384–398
Pischke S, Heim A, Bremer B et al (2011) Hepatitis E: an emerging infectious disease in Germany? Z Gastroenterol 49(9):1255–1257
Rab MA, Bile MK, Mubarik MM, Asghar H, Sami Z, Siddiqi S et al (1997) Water-borne hepatitis E virus epidemic in Islamabad, Pakistan: a common source outbreak traced to the malfunction of a modern water treatment plant. Am J Trop Med Hyg 57(2):151–157
Richard-Lenoble D, Traore O, Kombila M, Roingeard P, Dubois F, Goudeau A (1995) Hepatitis B, C, D, and E markers in rural equatorial African villages (Gabon). Am J Trop Med Hyg 53(4):338–341
Said B, Ijaz S, Kafatos G, Booth L, Thomas HL, Walsh A et al (2009) Hepatitis E outbreak on cruise ship. Emerg Infect Dis 15(11):1738–1744
Schlauder GG, Dawson GJ, Erker JC, Kwo PY, Knigge MF, Smalley DL et al (1998) The sequence and phylogenetic analysis of a novel hepatitis E virus isolated from a patient with acute hepatitis reported in the United States. J Gen Virol 79(Pt 3):447–456
Schlauder GG, Mushahwar IK (2001) Genetic heterogeneity of hepatitis E virus. J Med Virol 65(2):282–292
Seow HF, Mahomed NM, Mak JW, Riddell MA, Li F, Anderson DA (1999) Seroprevalence of antibodies to hepatitis E virus in the normal blood donor population and two aboriginal communities in Malaysia. J Med Virol 59(2):164–168
Shrestha MP, Scott RM, Joshi DM, Mammen MP, Thapa GB Jr, Thapa N (2007) Safety and efficacy of a recombinant hepatitis E vaccine. N Engl J Med 356(9):895–903
Shrestha AC, Faddy HM, Flower RL, Seed CR, Keller AJ (2015) Hepatitis E virus: do locally acquired infections in Australia necessitate laboratory testing in acute hepatitis patients with no overseas travel history? Pathology 47(2):97–100
Smith DB, Simmonds P, International Committee on Taxonomy of Viruses Hepeviridae Study Group, Jameel S, Emerson SU, Harrison TJ et al (2014) Consensus proposals for classification of the family Hepeviridae. J Gen Virol 95(Pt 10):2223–2232
Sugitani M, Tamura A, Shimizu YK, Sheikh A, Kinukawa N, Shimizu K et al (2009) Detection of hepatitis E virus RNA and genotype in Bangladesh. J Gastroenterol Hepatol 24(4):599–604
Siddiqui AR, Jooma RA, Smego RA Jr (2005) Nosocomial outbreak of hepatitis E infection in Pakistan with possible parenteral transmission. Clin Infect Dis 40(6):908–909
Song DY, Zhuang H, Li Z (1992) Hepatitis E in Hetian city. Analysis of 562 cases. Zhonghua Nei Ke Za Zhi 31(5):275–277
Takahashi M, Tamura K, Hoshino Y, Nagashima S, Yazaki Y, Mizuo H et al (2010) A nationwide survey of hepatitis E virus infection in the general population of Japan. J Med Virol 82(2):271–281
Tan LT, Tan J, Ang LW, Chan KP, Chiew KT, Cutter J et al (2013) Epidemiology of acute hepatitis E in Singapore. J Infect 66(5):453–459
Teo CG (2012) Fatal outbreaks of jaundice in pregnancy and the epidemic history of hepatitis E. Epidemiol Infect 140(5):767–787
Teshale EH, Howard CM, Grytdal SP, Handzel TR, Barry V, Kamili S et al (2010) Hepatitis E epidemic, Uganda. Emerg Infect Dis 16(1):126–129
Tessé S, Lioure B, Fornecker L, Wendling MJ, Stoll-Keller F, Bigaillon C et al (2012) Circulation of genotype 4 hepatitis E virus in Europe: first autochthonous hepatitis E infection in France. J Clin Virol 54(2):197–200
Tohme RA, Drobeniuc J, Sanchez R, Heseltine G, Alsip B, Kamili S et al (2011) Acute hepatitis associated with autochthonous hepatitis E virus infection-San Antonio, Texas, 2009. Clin Infect Dis 53(8):793–796
Tsega E, Krawczynski K, Hansson BG, Nordenfelt E, Negusse Y, Alemu W et al (1991) Outbreak of acute hepatitis E virus infection among military personnel in northern Ethiopia. J Med Virol 34(4):232–236
Tsarev SA, Tsareva TS, Emerson SU, Govindarajan S, Shapiro M, Gerin JL et al (1994) Successful passive and active immunization of cynomolgus monkeys against hepatitis E. Proc Natl Acad Sci U S A 91:10198–10202
Tsarev SA, Tsareva TS, Emerson SU, Govindarajan S, Shapiro M, Gerin JL et al (1997) Recombinant vaccine against hepatitis E: dose response and protection against heterologous challenge. Vaccine 15:1834–1838
Tucker TJ, Kirsch RE, Louw SJ, Isaacs S, Kannemeyer J, Robson SC (1996) Hepatitis E in South Africa: evidence for sporadic spread and increased seroprevalence in rural areas. J Med Virol 50(2):117–119
van Cuyck-Gandre H, Juge F, Roques P (2003) Phylogenetic analysis of the first complete hepatitis E virus (HEV) genome from Africa. FEMS Immunol Med Microbiol 39(2):133–139
Velázquez O, Stetler HC, Avila C, Ornelas G, Alvarez C, Hadler SC et al (1990) Epidemic transmission of enterically transmitted non-A, non-B hepatitis in Mexico, 1986–1987. JAMA 263(24):3281–3285
Verhoef L, Koopmans M, Duizer E, Bakker J, Reimerink J, Van Pelt W (2012) Seroprevalence of hepatitis E antibodies and risk profile of HEV seropositivity in The Netherlands, 2006–2007. Epidemiol Infect 140(10):1838–1847
Villalba ML, Lay Lde L, Chandra V, Corredor MB, Frometa SS, Moreno AG et al (2008) Hepatitis E virus genotype 1, Cuba. Emerg Infect Dis 14(8):1320–1322
Viswanathan R, Sidhu AS (1957) Infectious hepatitis; clinical findings. Indian J Med Res 45(Suppl):49–58
Wedemeyer H, Pischke S, Manns MP (2012) Pathogenesis and treatment of hepatitis E virus infection. Gastroenterology 142(6):1388–1397
Wichmann O, Schimanski S, Koch J, Kohler M, Rothe C, Plentz A et al (2008) Phylogenetic and case-control study on hepatitis E virus infection in Germany. J Infect Dis 198(12):1732–1741
Wilhelm B, Muellner P, Pearl DL, Rajić A, Houde A, McEwen SA (2015) Preliminary molecular epidemiological investigation of hepatitis E virus sequences from Québec, Canada. Prev Vet Med 118(4):359–369
Yamada H, Takahashi K, Lim O, Svay S, Chuon C, Hok S et al (2015) Hepatitis E Virus in Cambodia: prevalence among the general population and complete genome sequence of genotype 4. PLoS One 10(8):e0136903
Yoon Y, Jeong HS, Yun H, Lee H, Hwang YS, Park B et al (2014) Hepatitis E Virus (HEV) seroprevalence in the general population of the Republic of Korea in 2007–2009: a nationwide cross-sectional study. BMC Infect Dis 14:517
Yugo DM, Meng XJ (2013) Hepatitis E virus: foodborne, waterborne and zoonotic transmission. Int J Environ Res Public Health 10(10):4507–4533
Zhang J, Liu CB, Li RC, Li YM, Zheng YJ et al (2009) Randomized controlled phase II clinical trial of a bacterially expressed recombinant hepatitis E vaccine. Vaccine 27(12):1869–1874
Zhang J, Zhang XF, Huang SJ, Wu T, Hu YM et al (2015) Long-term efficacy of a hepatitis E vaccine. N Engl J Med 372(10):914–922
Zhu FC, Zhang J, Zhang XF, Zhou C, Wang ZZ et al (2010) Efficacy and safety of a recombinant hepatitis E vaccine in healthy adults: a large-scale, randomised, double-blind placebo-controlled, phase 3 trial. Lancet 376(9744):895–902
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Geng, Y., Wang, Y. (2016). Epidemiology of Hepatitis E. In: Wang, Y. (eds) Hepatitis E Virus. Advances in Experimental Medicine and Biology, vol 948. Springer, Dordrecht. https://doi.org/10.1007/978-94-024-0942-0_3
Download citation
DOI: https://doi.org/10.1007/978-94-024-0942-0_3
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-024-0940-6
Online ISBN: 978-94-024-0942-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)