
Abstract
The chapter deals with the relationship between global demographic change and the improvement in health, a core aspect of wellbeing and quality of life, over the period 1950–2100. The global change in population is closely related to the process of demographic transition with declining levels of fertility and mortality. While low fertility is a precondition for limiting global population growth, it also results in smaller birth cohorts, which contribute to the ageing of the population. The increasing life expectancy, in itself an indicator of improving physical health conditions at all ages and thus of wellbeing, also contributes to ageing. Furthermore, older populations are in general more prone to health risks – attendant with the epidemiological transition in the burden of diseases. The chapter depicts the development of global health using selected indicators of the Millennium Development Goals (MDGs) and the Global Burden of Disease (GBD) as measures. The increase in life expectancy at birth in all regions and at all levels of development shows the improvement and convergence of health conditions at a global scale in its contribution to global wellbeing.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- World population
- Demographic transition
- Ageing
- Epidemiologic transition
- Millennium Development Goals
- Global Burden of Disease
- Mortality
- Life expectancy
- Health indicators
- Wellbeing
Introduction
The World population already surpassed the 7th billion thresholds in 2011, and an additional billion will be added to the world population within the next 13胢years, according to the recent medium variant projection of the UN World Population Prospects (UN 2010). The assumptions underlying the medium variant projections predict a convergence of the different country fertility rates at a replacement level of about 2.1 births per woman around the end of the century. Alternative projections with a slightly higher or lower target level of fertility and a slower or faster adaptation to this level produce highly diverging projection results. Global population trends, with an accelerating growth or a population maximum at around mid-century followed by a long-term decline (Reher 2007), describe the extent of potential outcomes of the demographic transition currently taking place. Nevertheless, annual population growth rates have been continually decreasing since their all time high in the 1970s, and it is most likely that the decline will continue over the next decades. The theoretical explanation of the current global population development is closely related to the model of the demographic transition (cf. Notestein 1950, 1952; see Caldwell 2004; Weeks 2008: 89–96), which describes a causal link between declining levels of mortality and fertility and associated changes of the population growth and structure (see Bongaarts 2003, 2009; Canning 2011; Population Reference Bureau 2004 for an introduction to demographic concepts). Early empirical evidence of demographic transition processes at work was gathered when industrialised countries, since the beginning of the eighteenth century, experienced distinctive changes in their mortality trends for the first time. The usually high and highly variable mortality levels year after year, beginning with the infant and child mortality rates, began to fall due to improved nutrition, better hygiene, enhanced medical services followed by the availability of vaccinations and new treatments. With a time lag, often of approximately one generation or more, the decline in the formerly also high and erratic fertility rates followed soon after (cf. Woods 1982). Meanwhile, the population growth rates started to increase and reached unprecedentedly high levels. The respective changes in population development are depicted in Fig.胢2.1 which covers the secular trend and projection of population growth over the time span 400 BCE to 2300. Europe’s increased health and wellbeing and related pace of population growth since the start of industrialisation lead to a growing share in the world population until the first half of the twentieth century (Caldwell and Schindlmayr 2002; Gould 2009: 22f; Klein Goldewijk 2005; Kremer 1993; Maddison 2001; McEvedy and Jones 1978). As in the developed regions the demographic transition continued, and the gap between mortality and fertility rates finally narrowed, the growth rates returned to their previously low levels. By the mid-twentieth century, most developing countries had also followed the demographic transition process and had already improved their mortality conditions with rising growth rates as a result. Following this, Fig.胢2.1 shows that in recent decades, the global growth is concentrated in the less developed regions of the world – with Africa as a late comer in the demographic transition – and is expected to continue to grow beyond the twenty-first century. As predicted, according to the model of the demographic transition theory, the decline in fertility showed a time lag in the developing regions, too. Currently, in almost all developing countries, a decline in fertility has at least set in. However, the fertility decline did not progress as fast as expected, based on past experiences, in all developing countries, and some countries even show a stagnation of fertility reduction above the replacement level (Bongaarts 2008; Moultrie et al. 2012; Schoumaker 2009).

While low fertility is a precondition for limiting global population growth under conditions of low mortality, it also results in smaller birth cohorts, which add to the ageing of the population from the bottom of the age distribution. In addition to that, the increasing life expectancy triggered by lower mortality – in itself an indicator of improving physical health conditions at all ages – also contributes to ageing at the top of the age distribution, as it comprises lower mortality at higher ages as well. The characteristic succession of declining mortality and fertility rates and the inverse u-shaped trajectory of the population growth rate during the demographic transition causes a long-term change of the age distribution of a population. The median age of the population continually grows, and the initially young population with a large share of children goes through a process, where first, the share of the working age group grows, before finally, the share of the population in the older age groups rises. Sub-replacement fertility below about 2.1 children per women, prevailing in most industrialised countries today, increases the speed of population ageing and in the long run leads to a continuous natural population decline.
The aforementioned demographic transition theory clearly establishes the causal relationship between core demographic processes and the physical health conditions of a population (cf. Olshansky and Ault 1986). Increasing physical health conditions of a population directly affect the ageing of a population through lower mortality and rising life expectancy. Low mortality and especially infant and child mortality rates, which increase the chance that children survive into adulthood, are thought to indirectly influence the reproductive decisions made by individuals (cf. Weeks 2008: 99). In this regard, better health is a precondition for limited procreation. Fewer births per woman are sufficient to secure the intended number of children, if survival conditions improve. Not at least sexual and reproductive health and rights (SRHR) exercise an impact on demographic processes, because without access to family planning measures limiting fertility cannot be accomplished (cf. UN 1995, 2011a). In addition, older populations are generally more prone to health risks, such as chronic or degenerative diseases. Thus, ageing is one of the main demographic trends which affects the physical health conditions of a population and requests an adaptation of the health system (cf. Frenk et al. 1991). The shift of the main causes of death from communicable to chronic or degenerative diseases and the delay of such diseases to higher ages during the epidemiological transition shapes the relationship between physical health and wellbeing in the path of the development process (cf. Olshansky and Ault 1986; Omran 1971, 1998; Salomon and Murray 2002).
The main part of the chapter comprises two key sections. The first describes global population change with a focus on the ageing of the population, based on the estimates and projections of the recent revision of the UN World Population Prospects and introduces related concepts in demography. The second section depicts the development of global health concentrating on selected indicators of the Millennium Development Goals (MDGs) as measures and draws on the UN Millennium Development Goal Report, as well as the UNAIDS Report on the Global AIDS Epidemic. A short summary on the health impacts of the epidemiological transition in the Global Burden of Disease (GBD) is based on the The Global Burden of Diseases, Injuries, and Risk Factors Study 2010. The final section aims to summarise the development of global health conditions in the light of the targets set by the MDGs and to assess the past and projected increase of life expectancy at birth on a global scale as an important indicator of wellbeing.
Data Sources and Population Projections
The data used for the analysis of global population trends in this chapter are derived from the United Nations World Population Prospects 2010 Revision (UN 2010, see also O’Neill et al. 2001; O’Neill and Balk 2001). The estimates and projections are biennially published by the UN Population Division and cover all countries of the world as well as major regions and groups of countries according to their level of development. Industrialised countries comprise Europe, Northern America, Australia, New Zealand and Japan (more developed region). All other (developing) countries belong to the less developed region. Among them, 48 countries are defined by the UN as least developed countries, based on a set of development indicators, 33 in Africa, 9 in Asia, 5 in Oceania plus one in Latin America and the Caribbean. Data from the United Nations World Population Prospects given in this chapter exclude the 48 least developed countries from the aggregate data for the less developed region. Data from the MDG-Reports include the least developed countries in the aggregate for developing regions, i.e. less developed regions. The estimates are population figures collected by the UN Population Division and adjusted for the consistency of time series. Projections are based on assumptions on the future development of mortality, fertility and migration (UN Population Division 2011c). The assumptions on the future of country specific fertility trajectories are derived from past time series of fertility decline using a probabilistic method that combines a double-logistic function as a model of fertility decline with a random term based on the variation in time series of past fertility declines. Once a country reaches the replacement level of a Total Fertility Rate (TFR) of 2.1 or below, a time series model is used to let the future fertility trajectory oscillate around this level. Sub-replacement countries are expected to converge to replacement fertility in the long run (cf. Goldstein et al. 2009). For each country 100,000 random trajectories are generated and the median of this distribution is used as the medium variant fertility assumption. High and low variants are 0.5 children above or below the medium variant. Assumptions for the development of the life expectancy are based on the analysis of past increases in longevity, which is expected as a general trend for all countries, and take decreasing additional gains in life expectancy into account once a country proceeds towards low age specific mortality rates (Büttner and Zlotnik 2005; Oeppen and Vaupel 2002). For countries with a high HIV prevalence, different assumptions for the transformation of future mortality levels are made, which reflect the increased general mortality risk and predict a slower increase in life expectancy. For 48 countries with a HIV prevalence of more than 2胢% between 1980 and 2009, a loss of more than 2胢years of life expectancy or with more than 700,000 people living infected with HIV, the specific impacts of HIV are included in the population projection model with individual country assumptions for the future spread of the infection and the development of the survival rates. The assumptions for the patterns of international migration are set with regard to the migration policies declared by sending and receiving countries and reflect existing net migration flows as the most likely trajectory, while in general the level of net migration is expected to gradually decrease until the end of the century. Detailed description of data sources, projections methods and alternative variants are available online from http://esa.un.org/unpd/wpp/index.htm. Additional data, divided into urban and rural populations as well as major agglomerations, are provided by the biennially World Urbanization Prospects online at http://esa.un.org/unpd/wup/index.htm. Data from this source are congruent with the World Population Prospects and the corresponding methods and assumptions.
The physical health indicators in this chapter are derived from the UN Millennium Development Goals Report (UN 2011b, see also UN 2013). In 2000, the UN adopted eight development goals in their millennium declaration, of which six are directly related to the health dimension and affect population processes either directly, due to impacts on fertility (through education, gender equality and access to sexual and reproductive health), or indirectly through improved living conditions and reduced mortality and thus increasing life expectancy:
-
Goal 1: Eradicate extreme poverty and hunger
-
Goal 2: Achieve universal primary education
-
Goal 3: Promote gender equality and empower women
-
Goal 4: Reduce child mortality
-
Goal 5: Improve maternal health
-
Goal 6: Combat HIV/AIDS, malaria and other diseases
The last two development goals are related to aspects of the sustainability of development and international development cooperation and are therefore not dealt with any further in this chapter. The MDGs are monitored, using a set of more than 60 statistical indicators and progress reports indicating the gains of developing countries in implementing the targets. MDG data is published annually online at http://www.devinfo.info/mdginfo/. There, information on data sources and methodical aspects of data collection are documented as well.
The section on HIV/AIDS additionally draws on the UNAIDS Report on the Global AIDS Epidemic (UNAIDS 2010) with epidemiological data on the pandemic collected by UNAIDS and WHO. HIV prevalence is estimated using statistical models with confidence ranges depending on the reliability of the epidemiological data available for each country. Larger confidence ranges are associated with uncertainty resulting from insufficient data quality, especially the lack of representative population based surveys of HIV testing. In this publication only the mid points of the prevalence ranges are depicted for reason of clarity. UNAIDS data with additional indicators are available online at http://www.aidsinfoonline.org.
Data on additional indicators of the change of the Global Burden of Disease (GBD) and causes of death during the epidemiological transition (cf. WHO 2008, 2009; Institute for Health Metrics and Evaluation 2012) are available from WHO. GBD data are published at http://www.who.int/research/en/ and the GBD 2010 at http://www.healtmetricsandevaluation.org/ghdx/gbd-2010-data-downloads. The GBD is calculated in years of healthy life lost by胢disability-adjusted life years (DALY), a measure which combines the years lost due to premature mortality (YLL) and years lived with disability (YLD). The health adjusted life expectancy (HALE) represents the actual life expectancy less the YLD. The GBD and mortality is differentiated by three major groups of causes: communicable (contagious) diseases (including maternal, neonatal, and nutritional disorders), non-communicable diseases (chronic or degenerative and man-made diseases), and injuries, including accidents, homicides, and suicides (Institute for Health Metrics and Evaluation 2012).
Global Demographic Trends
Population Growth and Demographic Change
In 1950, the first year for which consistent data from the UN World Population Prospects time series are available, the world population was roughly 2.5 billion and the Total Fertility Rate (TFR) 5 children per women (Fig.胢2.2). At the beginning of the 1950s, the population was growing at an average of 48 million or an equivalent of 1.8胢% per year on average between 1950 und 1955 (Fig.胢2.3). Following this, estimates of the global population recorded an accelerating growth, with the 3rd billion registered in 1959, the 4th in 1974 und the 5th in 1987. The time interval for an additional billion declined from 15胢years for the 4th to 13胢years for the 5th billion, and the annual population growth reached, unprecedented in world history, a maximum level of 2胢% per year around 1970. At the end of the 1980s, population growth reached its all time high in absolute numbers with an average annual increase of 89 million people per year during the period of 1985/90. The 6th billion consequently came in 1999 after only 12胢years, and population growth was again placed on the political agenda, returning to previous perceptions of “over-population” as a threat for quality of life, development, and – as a new aspect – sustainability (Pearce 2010). In most contemporary analyses, the anti-natalist notion of population growth and fertility as being too high prevailed. The idea that high growth rates or soaring population densities are, in general, detrimental to the generation of economic wealth and wellbeing is often being blamed as the underlying cause for shortcomings in development efforts, despite the fact that the causal linkage is still contested in research (cf. Dyson 2010; Gould 2009). Nevertheless, growth was the most imminent population trend in the second half of the twentieth century.

World population and total fertility rate (TFR) 1950–2100 (Source: UN World Population Prospects 2010 Revision, translated from Swiaczny and Henning 2011: 56)

Total fertility rate and population growth rate by level of development (Source: UN World Population Prospects 2010 Revision, Medium Variant, translated from Swiaczny and Grünheid 2012: 49)
However, when the population growth started to take up pace, fertility had already started to decline at that time, too (Bongaarts 2003, 2008). During the second half of the 1980s, the fertility was less than 3.5 children per woman and today, the global figure is down to around 2.5. The secular trend, in accordance with the demographic transition model introduced in the preceding section, shows that efforts to promote the limitation of family size and to give access to family planning measures were successful. However, it is now thought that population policies in certain countries have put undue pressure on individuals and their right to decide freely and without coercion on timing and spacing as well as the desired number of children (cf. Pearce 2010: 53–65). Meanwhile, in many industrialised countries, the fertility has fallen below the replacement level of 2.1 (Fig.胢2.3), in general due to the modernisation of (western) societies, which improved the position of women, in particular their higher education attainments, labour market participation and gender equality. This Second Demographic Transition (SDT) to sub-replacement fertility (van de Kaa 1987) has recently spread to a number of developing countries as well and is an indicator for the prospect that the decline of the global fertility level will continue, as assumed by the UN population projections’ medium variant. Only the group of the least developed countries retains high fertility levels and shows only limited progress in lowering the family size, with recent stagnation in fertility decline recorded in some Sub-Saharan African countries (Bongaarts 2008; Moultrie et al. 2012; Schoumaker 2009). As a consequence, growth rates in the least developed countries belong to the highest in the world and will supposedly remain high for the next decades. Also there is no causal relationship between population growth and development with both, high and low growth countries among the best performing developing countries, high growth is posing an additional challenge to development efforts towards the quality of life and wellbeing. As a consequence the least developed high fertility countries will increase their share in the world population, and as most of the least developed countries are in Sub-Saharan Africa, this region will increase its weight compared to other regions.
Given that global fertility will have levelled off at 2.1 by the end of the century, the future population growth will slow down and begin to stabilise slightly above 10 billion. According to the medium variant projection in Fig.胢2.2, the time interval until the next additional billion of the world population will increase from 13胢years for the 7th billion, reached in 2011, to 14 and 18胢years for the 8th and 9th billion respectively, expected in 2025 and 2043. The growth rate, currently at about 1胢% per year, will be close to zero growth at the end of the century, and the 10th billion will finally be reached after 40胢years in 2083 (UN Population Division 1999, 2011a).
The growth path of the world population until the end of the century, as projected by the UN, depends primarily on the development of fertility as its core impact factor. A trajectory of 0.5 children per woman above or below the medium variant will result in completely different global population trends (Fig.胢2.2). A slower fertility reduction in high fertility countries, which would mean a slightly increasing global TFR levelling off at 2.6 at the end of the century, would result in a much slower reduction of the population growth rate, with still 0.8胢% per year at the end of the century. Due to the demographic momentum (Blue and Espenshade 2011; Bongaarts 1994, see below) of the age composition, the average annual growth will increase to 119 million at the end of the century in this scenario and continue to grow for some time beyond the turn of the century. Under such conditions, population would be close to 16 billion in 2100 and still growing further. A faster decline of fertility and a level continually below replacement from 2020 onwards, reaching 1.6 at the end of the century, will result in an increasingly declining population growth rate that will turn negative at mid-century with a culmination of the world population slightly above eight billion at this time. In the light of this population projection results and the impact that fertility shows thereon, unmet needs for family planning (i.e. SRHR) gain additional significance for global development.
As set out in the introductory section, the decline of fertility during the demographic transition is not only related to population growth, but also associated with the ageing of the population (cf. Haupt and Kane 2004; McFalls 2003). A reduced fertility rate in births per woman initially triggers smaller birth cohorts. A smaller number of children born immediately reduces the annual increment added to the existing population and therefore has a negative effect on the growth rate at that time. It also reduces the share of the younger age group within a population, as a smaller birth cohort replaces a somewhat larger cohort born the year before. This means, if compared to the population in the working age group, a shift in the dependency ratio or, related to the age of the population, a higher median age. An additional secondary effect of reduced fertility is, however, delayed by the demographic momentum of the age structure. While smaller cohorts are already being born, in young populations large and sometimes (depending on the age structure) even growing cohorts will continue to enter the reproductive age and increase the number of potential mothers for some time to come. Only when the smaller cohorts are at last and with a time lag entering the reproductive age, they will finally start to decrease the number of births and subsequently population growth. As long as the number of potential mothers is still growing, owing to the demographic momentum of the age structure of a young population, high growth rates and annual growth in absolute numbers of a population will prevail, while the number of children on the individual level (TFR) has already started shrinking (Fig.胢2.3). A fast and intense fertility decline generally has strong secondary effects on the birth level and consequently increases the pace and extent of the ageing process in the long run. The effect of the aforementioned demographic momentum on the change of the age structure during the demographic transition will be analysed in the following section.
Population Ageing and Age Structure
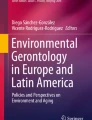
The age structure of the world population is changing due to reduced fertility, as described in the section above, and shown in Fig.胢2.4 (cf. Rowland 2012). In 1950, the population share of the younger age groups below 15胢years was 34.3胢% and the share of 65胢years and older only 5.2胢%. By 2010, the share of the younger age group had declined to 26.8胢% and the older age group was still small with 7.6胢%. The share of the working age group between 15 and 64胢years increased its share from 60.5胢% to 65.6胢% in this period respectively, and it will only slightly decrease over the next decades. In 2100, the world population will show an inverted age structure. The younger age group with 17.9胢% will then be less numerous than the group of 65 plus with 22.3胢% (7.8胢% for the group 80胢years and older), while working age population with 60胢% will still be only slightly below its 1950-share.

World population by age group 1950–2100 (Source: UN World Population Prospects 2010 Revision, Medium Variant, translated from Swiaczny and Grünheid 2012: 49)
The increasing share of the working age population emerging during the demographic transition is associated with a “demographic dividend” (Bloom et al. 2003). While a large share of working age population prevails, the dependency ratio on national levels, necessary to support the declining younger cohorts and a still small group in the pension age, reaches historically low levels. The dependency ratio is measured by the number of youth 14 and younger plus seniors 65 and older per 100 persons in the working age of 15–64胢years. Demographic change thus allows investment in development, and the economy can profit from a growing labour force, given that conditions allow profitable investment and gainful employment. Due to further ageing, i.e. larger cohorts entering the pension age, when demographic transition continues, the phase of demographic dividend comes to an end and the “window of opportunity” closes. On a global scale, this will be the case around 2045. In many industrialised countries, the demographic dividend is already fading out and some of the larger developing countries, for example China, will catch up soon. The dependency ration in China was approximately 77 between 1960 and 1975. At that time the TFR declined from around 6 children per woman before the 1970s to 2.6 during the 1980s as a result of the so called one-child policy. The dependency ratio improved as a result to 38 per 100 working age population between 2010 and 2015. With a sub replacement fertility of less than 2.1 since the second half of the 1990s the dependency ratio is projected to rise to more than 70 in 2055 and approximately 80 from 2065 onwards. According to the UN Population Division the “window of opportunity” of China will last from 1990 until 2025, compared to a much longer period in India lasting from 2010 to 2050 as a result of the later onset and slower decline of the TFR (Swiaczny and Henning 2011; UN Population Division胢2004b: 75).
Taking the median age as a measure, the age which divides a population into two equal halves, Fig.胢2.5 shows the global population ageing process with continually increasing median ages across the globe. The industrialised countries were the forerunners, but less developed countries are catching up fast and projections predict a closing of the ageing gap within the coming decades. On a global scale, the median age increased from 22.1胢years in 1970 to 29.2胢years in 2010, and in 2035, the median age will surpass the 35-year threshold, if current trends in fertility decline and improving mortality conditions continue. The gap between industrialised countries and the less developed region was 7.2胢years in 1950 and has now increased to 11.5胢years in 2010, due to the rapid ageing in the developed world. Nevertheless, a future convergence is inherent in the demographic transition process with a gap of only 5胢years remaining at mid-century and further declining. A special situation has to be conceded for the least developed countries. They are currently considerably younger than the world average, and the increase in median age will be rather limited during the next decades, a development correlating to the slow reduction of fertility and the high growth rates, as described in the previous section. Nevertheless, in 2010 a considerable number of developing countries showed median ages of less than 20胢years and almost all developing countries were below 30胢years, while at the same time the group of industrialised countries had a median age higher than 35胢years. In 2060, only a few remaining developing countries, mostly least developed countries in Sub-Saharan Africa, will remain below a median age of 35胢years (Fig.胢2.6).

Median age by level of development 1950–2100 (Source: UN World Population Prospects 2010 Revision, Medium Variant)

Median age 2010 and 2060 (Source: UN World Population Prospects 2010 Revision, Medium Variant, Map: ESRI, Cartography: F. Swiaczny/N. Ahmed, translated from Swiaczny and Henning 2011: 58)
The ageing process can be followed best in detail using population pyramids to analyse the age structure differentiated by birth cohort and sex, as depicted in Fig.胢2.7 for the population of industrialised, developing and least developed countries as well as for the world for the years 2010, 2060 and 2100. The population diagrams presented here have been standardised for population size, so that the age structure of the different populations for the three development categories can be directly compared. The age structures depicted by the different diagrams represent different stages of the ageing process, as related to the demographic transition. The least developed countries, which in 2010 are still in the earliest stage of the transition, show the typical shape of a pyramid (bottom line left). The population is young and expanding. In 2060, the dynamic of the expansion will have started to reduce, the youngest cohorts will be only slightly broader than the previously born (bottom line middle). The population is on the brink of a reversal that follows and leads to a population structure in 2100 that shows first signs of contraction at the stem of the population pyramid (bottom line right). The less developed countries are a stage ahead in 2010, with an age structure similar to that of the least developed countries in 2060. In 2060, their age structure will have entered into a phase of contraction. The smaller younger age groups at the bottom are a sign that fertility decline and ageing will have been persisting for some time. In 2100, the further advancement of ageing will have reshaped the population pyramid in direction of an even broader top and smaller stem. The age structure will be characterised by a dominance of the middle cohorts of working age (second line). The age structure of the industrialised countries is again one stage ahead in the transformation and ageing process. In 2010, the broader top of the age group 65 plus is an indicator of the low mortality and high survival rates at higher ages that are achieved in the industrialised countries today (third line). In the long run, the population in the industrialised countries will transform into a stable population where the shape of the age pyramid is no longer changing, as the comparison between 2060 and 2100 shows. A stable population always emerges when fertility and mortality levels are kept stable over a long time, as it is the case in the assumptions of the population projections used for the population diagrams in the figure (cf. Woods 1982: 46–85). Under such conditions, the shape of the population pyramid remains constant and the population growth or decline is determined by the relationship between births and deaths only. The long-term trend of population ageing, according to the UN population projection, is determined by the assumption that the increase of the life expectancy (i.e. reduced mortality levels) will level out as it reaches high values and that fertility will in the long run converge to replacement level. Thus, the world population, when all countries have passed through the demographic transition, will take on a shape quite similar to the one presented for the industrialised countries in 2100 (top line right). The long-term global population structure will resemble not only a stable population with low mortality and high life expectancy, but in fact a stationary population with zero growth due to the assumption of a fertility converging at replacement level.

Population by age group and population structure by level of development 2010, 2060 and 2100 (Source: UN World Population Prospects 2010 Revision, Medium Variant)
Development of Health Indicators
The following sub-sections present a selection of indicators from the MDG: child mortality, maternal mortality, family planning and HIV/AIDS. The priority of these targets set by the MDGs and followed here to illustrate the development of global health conditions concern a very core aspect of human wellbeing and quality of life, namely the ability to live a life free of the risk of a premature death due to preventable causes (UN 2012b; UN Population Division 2011b). Longevity (life expectancy), through means of good physical health, is thus a major impact factor as well as an indicator of the wellbeing of a person (Sen and Nußbaum 1993; Streeten et al. 1981; UN Population Division 2012). However, wellbeing is not confined to physical health and comprises, among others, an economic, social, as well as psychological and emotional dimension too (Camfield and Skevington 2008; Strack et al. 1991; UNDP 1994; WHO 2004, see Veenhoven 1996: 1–4 for a review and appraisal of quality of life indicators). Moreover, the concept of health, as adopted by WHO in 1946, embraces a broad definition, not restricting health to the “absence of disease and infirmity” only, but includes the notion of “complete physical, mental and social wellbeing” as the basic definition (UN 1948).
The four indicators selected here represent different aspects of the health condition of a population and their respective impacts on the age specific mortality and fertility: mortality at a young age, mortality at the reproductive age of women, quality of care related to birth and morbidity and mortality of mother and child, control of one’s fertility through contraception, and finally the societal challenge of sexually transmitted diseases and their health impact and excess mortality. These indicators are specially targeted to mirror the morbidity and mortality conditions of developing countries at an early stage of epidemiological transition and are also relevant to different aspects of the health system. All four indicators relate to the issue of sexual and reproductive health and rights (SRHR), as defined by the International Conference on Population and Development (ICPD) in Cairo 1994: “Reproductive health is a state of complete physical, mental and social wellbeing and not merely the absence of disease of infirmity, in all matters related to the reproductive system and to its functions and processes. Reproductive health therefore implies that people are able to have a satisfying and safe sex life and that they have the capability to reproduce and the freedom to decide if, when and how often to do so” (UN 1995: 40). According to the Program of Action of the ICPD, adopted at the conference, this includes and is not limited to the access to family planning and the care of sexually transmitted diseases in order to enhance “life and personal relations” (sexual health) (UN 1995: 40).
The linkages between physical health, population development and wellbeing are complex and manifold (De Souza et al. 2003; Frenk et al. 1991; WHO 2009). Even small development efforts in poverty reduction or hygiene and basic health care provision have significant impacts on child mortality (UN Population Division 2011b). Improvement of maternal mortality, instead, requires a higher investment in the health care system, e.g. to provide nationwide qualified assistance at birth and after care. This requires, beside the physical infrastructure, a developed education system to train the highly qualified medical staff needed for the purpose. The improvement of sexual health by making family planning available through measures of contraception does not only require the universal provision of modern contraceptives especially to vulnerable groups, but also education on sexuality as well as societal changes which allow contraceptive practices to be considered as an option by individuals in need of family planning (by public health programs). Finally, sexually transmitted diseases such as HIV/AIDS pose a new challenge to public health in order to control the spread of the disease and to cope with a wide range of consequences of the infection. At the same time, the extremely costly treatment of the disease with anti retroviral drugs (ART) puts an additional strain on the limited capacities of the health care systems in developing countries and competes with resources needed e.g. for family planning or to fight other communicable diseases, such as malaria, tuberculosis or the group of neglected tropical diseases (Hotez 2011). In countries highly affected by HIV/AIDS, the excess mortality due to the pandemic has a direct demographic impact on development too, as young and often economically active people are dying of the disease and leave large numbers of orphans behind.
The following sub-section covers the impact of the epidemiological transition (Omran 1971, 1998) from communicable (infectious) to non-communicable chronic or degenerative diseases, such as cardiovascular diseases or cancer, on the change in the burden of disease of a population. The change of the main causes of death from famine and pandemics to man-made diseases is at a later stage also accompanied by a delay of morbidity and mortality. On average, ill health and death occurs later in life (cf. Olshansky and Ault 1986; Salomon and Murray 2002). The Global Burden of Disease (GBD) is assessed by WHO using disability-adjusted life years (DALY) and health adjusted life expectancy (HALE) as a measure (WHO 2009: 5, see section “Data sources and population projections”). This transition in health conditions which parallels the demographic transition and gains in importance for ageing populations, especially in more developed regions (see UN 2012a and UN Population Division 2012 for further reading). Nevertheless, the rising prevalence of chronic or degenerative diseases is not only a phenomenon of industrialised countries but affects more and more developing countries too (Gaziano 2011; Institute for Health Metrics and Evaluation 2013). This development is often attributed as a “double burden”, as the health systems are often not yet fit to deal with the common contagious diseases when at the same time the upcoming chronic or degenerative diseases are imposing new challenges (WHO 2009: V). Behavioural related diseases (Vallin and Meslé 2004), as for example obesity, associated with diabetes (Shetty and Schmidhuber 2011), or tobacco smoking which causes cardiovascular conditions and cancer, are on the rise in a number of developing countries due to changes in life style (WHO 2009: 3), despite the fact that malnutrition may prevail simultaneously in the respective countries (Mendez et al. 2005).
Alternative measures of quality of life are distributed along two dimensions: input (e.g. access to services or wealth as a condition for a happy life) versus output (e.g. life expectancy) measures as well as objective (e.g. DALY/HALE) versus subjective (e.g. self-reported happiness) measures. Veenhoven (2005: 61–63) argues against input based indicators firstly because they are not based on a “sound theory about human needs” and secondly because a “more” does not necessarily improve the quality of life for all indicators (e.g. income). His alternative to DALY uses self-reported subjective quality of life (compared to observable behavior) instead of the objective medical diagnosis applied for DALYs. The proposed happy life years (HLY, formerly Happy Life Expectancy) is based on the life expectancy at birth adjusted by a happiness index on a 0–10 scale derived from the World Database on Happiness (WDH) (Veenhoven 2005, see also Glatzer 1991 on objective versus subjective measurement).
In general longevity measured as life expectancy at birth is not a good indicator for the quality of life, as a long life does not necessarily mean a healthy and happy life (see Veenhoven 2005: 65). However, in this chapter life expectancy is used as a central indicator because it links a central measure for the analysis of population processes with an essential component of most quality of life indicators and it is available for all countries allowing global comparisons. Furthermore, as Veenhoven concedes, “… happiness and longevity tend to go together…” (2005: 79). This is especially true for regions with high life expectancy (UN 2012b). But the correlation is not always straight forward, there are countries with a short life expectancy and high happiness rates (e.g. in some developing countries) or vice versa.
Consequently the final sub-section is dedicated to the development of life expectancy at birth. The life expectancy at birth is a key demographic measure, which provides a synthesis of the mortality conditions of a population through the life course at a given time (i.e. a period measure). Age specific death rates (the risk to die at a specific age) are collected for all age cohorts based on the deaths in a population occurring over a time period and collected in a “life table” (see Preston et al. 2001; Rowland 2006 for the method). The life expectancy at birth indicates the hypothetical average length of life, if a newborn faces the risk to die at a certain age throughout her further life which resembles the current age specific death rates of the base year or years. As long as mortality levels are declining (i.e. life expectancy is increasing) the life expectancy at birth of a cohort will be lower than the actual average age of death of that cohort (a cohort measure, to be calculated only after the complete cohort is dead). From a life table additional information can be obtained, e.g. the probability to survive from one age to another and the life expectancy at any age. As the age specific mortality rates are used to calculate the measure, the life expectancy at birth is a good indicator for the overall health conditions and physical wellbeing of a population. Deteriorating health conditions after the collapse of the former Soviet Union, for example, were expressed by an immediate contraction of the life expectancy in Russia (e.g. from 69胢years 1985/90 to 65 years 2000/05). The same applies to those countries most affected by HIV/AIDS, they too show a declining or stagnating life expectancy, after the death toll started to rise due to the infection (e.g. in South Africa from 61胢years 1990/95 to 51 years 2005/2010).
Life Expectancy at birth is also a key indicator of the Human Development Index (HDI), together with education and per capita income. A number of other indicators are derived from the HDI and include additional aspects of development. The Inequality-Adjusted HDI is adjusted for inequality in development outcomes, the Gender Inequality Index uses a combination of maternal mortality and adolescent fertility instead of life expectancy, and the Multidimensional Poverty Index uses child mortality and nutrition instead of life expectancy (see UNDP 2011: 167–173 for details on the computation). For a predecessor of the HDI see also the Physical Quality of Life Indicator by Morris (1979), using infant mortality, life expectancy and basic literacy. As an alternative to those output oriented indicators the World Bank proposes an input based Human Opportunity Indicator which measures equal access to a minimum standard set of services (see Molinas et al. 2009, 2010).
Child Mortality
Infant mortality within the first year after birth and mortality under the age of 5胢years per 1,000 live births are two indicators that represent the earliest stage in the demographic transition process and the change in health conditions of a population (Fig.胢2.8). Once health conditions improve, through reduced poverty or better health care provision, the mortality of younger age groups is usually declining first. Child mortality is furthermore closely connected to maternal mortality (see section “Maternal mortality”) and family planning (see section “Family Planning”). Better survival conditions of the mother and better medical management of pregnancy and child birth have crucial influence on the mortality risk in childhood as does timing and spacing of births (UN Population Division 2011b). In the industrialised countries the infant mortality rate was still at a relatively high level at the beginning of the 1950s, with 60 deaths per 1,000 live births or slightly less than the rate of the least developed countries today. Infant mortality was declining fast after World War II in the industrialised world to 15 at the beginning of the 1980s and 2010/15 it reached a very low level of 6 per 1,000 live births, leaving little room for further improvement. The under-five mortality (data available from 1980/85 in Fig.胢2.8) declined accordingly. Mortality between the age of 1 and 5胢years has been shrinking from only 3 per 1,000 in 1980/85 to 2 in 2010/15. Infant mortality in the less and least developed countries was extremely high in the beginning of the 1950s with 145 and 192 per 1,000. In 1980/85 the rate was still at 70 and 125. Today the mortality is at 38 and 73 which is equivalent to the infant mortality in the industrialised countries before WW II and around 1960. The mortality between 1 and 5胢years was still high in the beginning of the 1980s, 30 and 76 per 1,000; this represents 43 and 61胢% of the infant mortality. The mortality between 1 and 5胢years has been declining faster in the past decades than the infant mortality and is now down to a rate of 14 and 40 respectively, or 36 and 54胢% of the infant mortality level. The UN Population Division expects in their assumptions a further global convergence so that in 2100 both country groups will roughly equal the infant und under-five mortality levels of the industrialised countries as of the beginning of the 1980s. Figure胢2.9 shows the spatial pattern of the child mortality with high rates for both variables prevailing mostly in Sub-Saharan-Africa and Southern Asia. A comparison of both maps stresses again the precarious health conditions in most countries of Sub-Saharan-Africa, where not only the infant mortality belongs to the highest levels globally recorded but also the under-five mortality remains still in excess of 100 deaths per 1,000 live births.

Infant and under-five mortality by level of development 1950–2100 per 1,000 live births (Source: UN World Population Prospects 2010 Revision, Medium Variant. Figures for under-five mortality include infant mortality)

Infant and under-five mortality 2010/15 per 1,000 live births (Source: UN World Population Prospects 2010 Revision, Medium Variant, Map: ESRI, Cartography: F. Swiaczny and N. Ahmed. Figures for under-five mortality include infant mortality)
Maternal Mortality
The mortality of women during pregnancy or related to birth within 42胢days after the termination of a pregnancy is an important aspect of health as it is, together with HIV/AIDS, one of the most important causes of death in women at the reproductive age in developing countries (Institute for Health Metrics and Evaluation 2012). The risk for mother – and child (see section “Child mortality”) – increases in general with short inter-pregnancy intervals and the number of children born and is even higher for adolescents or at higher ages of the mother (UN 2011a). Reducing maternal mortality and improving the health conditions of mother and child plays an important role in the Millennium Development strategies and are regarded as a major contribution to development. Maternal mortality is closely related to reproductive health. Attended delivery and emergency obstetric care could prevent a large part of the current maternal mortality in developing countries and preventing unplanned and unwanted pregnancies would also contribute to the elimination of 20 up to 40胢% of the maternal deaths in developing countries (UN 2009). A comparison with the maternal mortality of the developed region with 26 per 100,000 live births in 1990 and only 17 in 2000 and beyond shows the large gap still existing in the developing parts of the world (Fig.胢2.10; WHO et al. 2012). In the two, in terms of maternal mortality, most advanced developing regions, Eastern Asia and Caucasus and Central Asia, maternal mortality is more than two or three times more prevalent than in the industrialised countries. In the least developed countries the prevalence of maternal mortality was 900 deaths per 100,000 live births in 1990 and up to 2008 the figure declined only by 35胢% to 590. The target set by the MDG to reduce maternal mortality by three quarters between 1990 and 2015 is thus still far ahead. Comparing the two regions with the highest prevalence, Sub-Saharan-Africa and Southern Asia, exemplifies the different pace in reaching the goal. While in Sub-Saharan-Africa the rate fell from 870 to 640 only between 1990 and 2008, or roughly one quarter, Southern Asia was more successful in reducing the rate from 590 to 280 during the same period of time at a double pace by one half. This resembles the different efforts made by the two depicted regions in improving the share of deliveries attended by skilled health personnel during the period of 1990–2009 (Fig.胢2.11). While the share increased in Southern Asia from 32 to 50胢%, the improvement in Sub-Saharan-Africa is more limited and increased only by 4 percentage points to 46胢% in 2009. Although many regions improved the access to skilled attendance at birth, the goal of universal access by 2015 is still not in sight in all the developing regions, with access of only 65胢% in 2009, up by 10 percentage points from 55胢% in 1990.

Maternal deaths per 100,000 live births by region 1990, 2000, 2008 (Source: MDG-Report 2011: 28 and Annex)

Deliveries attended by skilled health personnel in percentage by region around 1990 and 2009 (Source: MDG-Report 2011: 29)
Family Planning
Unmet need for family planning of women, who have the desire to delay or avoid pregnancy, but are not using any form of contraception, is one of the most imminent obstacles in securing sexual health and meeting the targets set by the MDGs. According to the UNFPA in 2012 more than 220 million women aged 15–49 years lack access to safe and effective contraception (Singh and Darroch 2012). As Fig.胢2.12 illustrates, the unmet need for family planning has been reduced in a number of regions, with figures close to 10胢% in 2008. In Eastern Asia, unmet need is even close to zero. Other regions, with an unmet need of roughly between 20 and 25胢%, i.e. Sub-Saharan-Africa, the Caribbean and South Asia, show different trajectories. While in Southern Asia the percentage of the unmet need declined from 20 to 15胢% between 1990 and 2008, there is no progress in Sub-Saharan-Africa. Sub-Saharan-Africa is also the region with the lowest percentage of use of any method of contraception, with 22胢% in 2008. At that time, the average for all developing regions had increased to 61胢%, compared to 72胢% in the developed regions. Furthermore, this correlates to the number of births per 1,000 adolescents aged 15–19 years, which is 122 in 2008 in Sub-Sahara Africa, more than twice the average figure for all developing regions (UN 2011b). As described before, the unmet need plays a role in the impairment of the health of mothers and children, especially for vulnerable groups as adolescents, and plays a role in high fertility and population growth rates. For those regions with large unmet needs and little improvement over the last two decades, the stress on development efforts will increase in future due to the young age structures and the large number of people growing into the reproductive age (demographic momentum, see section “Population growth and demographic change”). Even to keep the current levels of service provision the efforts must be increased to meet the increasing needs of the growing cohorts in the reproductive age. At the same time, the additional official development assistance to developing countries that is available for family planning has fallen behind the strongly increasing amount that is now spent to fight infectious diseases such as HIV/AIDS. In 2009 the share of the official development assistance to health available for family planning has fallen to 2.6胢% from 8.2胢% in 2000. The per capita assistance for family planning has declined in almost all receiving countries (UN 2011b: 35).

Unmet need for family planning in percent of women 15–49 years, married or in a union by region 1990, 2000, 2008 (Source: MDG-Report 2011: 33)
HIV/AIDS
In many developing countries, HIV/AIDS is one of the most substantial threats to health and development (Institute for Health Metrics and Evaluation 2012; UNAIDS 2010). The impact of HIV/AIDS related mortality on the life expectancy at birth exceeds in some cases even 10胢years, as of 2005/10 it is the case in Botswana, Lesotho, Malawi, South Africa, Swaziland, and Zimbabwe (UN Population Division 2011b). As Fig.胢2.13 shows, the highest prevalence rates of HIV/AIDS are located in one of the poorest parts of the world, Sub-Saharan Africa, as well as in Russia, with a prevalence rate of more than 5 or even 10胢% of the population between 15 and 49胢years old. The global pandemic has lead to 33.3 million people living with HIV/AIDS in 2009, which equals a prevalence rate of 0.8胢% of the total population. The number increased from 26.2 million in 1999, despite the fact that the incidence of new infections decreased by 19胢% between 1999 and 2009, from annually 3.1 million new infections in 1999 to 2.6 million in 2009. Since the peak of new infections in 1997, with an annual 3.2 million incidences, the number of new infections decreased by 21胢%. The rise in people living with HIV/AIDS, even though success in the reduction of new infections has been reached in recent years, is due to the fact that better care and access to antiretroviral treatment has improved the survival of people living with HIV/AIDS. In 2009, the global number of deaths due to HIV/AIDS was 1.8 million, down from 2.1 million during the peak year of 2004. However, although the trend in the number of HIV/AIDS related deaths has been reversed, the number of orphans due to the excess mortality of HIV/AIDS has mounted to more than 16 million in 2009, increasing from roughly 8 million in 1999 (UN 2011b: 36–42). The care for orphans is only one indirect effect of HIV/AIDS imposed on the development efforts in the most heavily affected countries. Others, e.g., relate to the parental investment in education, which is undermined by premature death in the prime working age due to HIV/AIDS. Between 2005 and 2010, an estimate for high HIV countries reveals that more than 85胢% of all death from HIV/AIDS affects those between 15 and 59胢years which undermines the livelihoods of affected families and respectively their ability to invest in health and education of children (UN Population Division 2011b: 21).

HIV prevalence, 15–49 years, and antiretroviral treatment (ART), CD4<350, in percentage 2009 (Source: UNAIDS and WHO. http://www.aidsinfoonline.org. Accessed 3 July 2012, Map: ESRI, Cartography: F. Swiaczny and N. Ahmed)
Globally, a total of 33 countries have seen a decrease of the incidence of HIV/AIDS infections by at least 25胢% between 2001 and 2009. Twenty-two of these countries are in Sub-Saharan Africa, where the number of new infections decreased from 2.2 million in 2001 to 1.8 million in 2009, while the number living with the disease increased from 20.3 million to 22.5 million respectively (UN 2011b: 36–42). At the same time Armenia, Bangladesh, Georgia, Kazakhstan, Kyrgyzstan, the Philippines, and Tajikistan showed an increase of the incidence of more than 25胢% between 2001 and 2009 (UNAIDS 2010: 61).
In 2009, Sub-Saharan Africa bore 68胢% of the global HIV/AIDS prevalence, but the region is also an example for the success of antiretroviral treatment. From 2004 onwards, the time when the expansion of antiretroviral treatment in Sub-Saharan Africa started (Fig.胢2.13), the number of deaths decreased by 310.000 or 20胢% over a 5胢year period. Despite the fast pace with which antiretroviral treatment was made available in recent years and the large share of development aid assigned for the task, the target of universal access by 2010 is not met (UN 2011b: 41). Beside HIV/AIDS, the treatment of other communicable diseases, such as malaria and tuberculosis, has also gained major advances (UN 2011b: 42–47).
Changes in the Global Burden of Disease
The aforementioned indicators of the MDGs are mainly targeting the health related aspects of the quality of live in the less and least developed regions. As they are still in the first stages of the epidemiological transition (cf. Olshansky and Ault 1986; Omran 1971, 1998; Salomon and Murray 2002), their global burden of disease of morbidity and mortality is determined by high disability-adjusted life years (DALY, see section “Data sources and population projections”) levels mostly due to a large impact of communicable diseases, such as infections and sexually transmitted diseases and conditions rising from maternal, neonatal, and nutritional disorders. Non-communicable, chronic or degenerative diseases and injuries (including accidents, homicides and suicides) are less frequent causes of ill health and death. With increasing levels of development the DALY level in general is shrinking and the share of the latter causes is increasing. In the more developed regions the major causes of morbidity and mortality are dominated by non-communicable diseases, mainly cardiovascular diseases and cancer. A final stage of the epidemiological transition comprises the delay of the prevalence of such diseases into higher ages, increasing the health adjusted life expectancy (HALE, see section “Data sources and population projections”). Ageing populations are also more prone to the development of a set of diseases such as dementia or Alzheimer’s disease with high prevalence in older ages only. Figure胢2.14 compares the development of the burden of disease measured according to the top 25 major causes of death for selected regions in developed and developing regions according to the results of the GBD 2010 (Institute for Health Metrics and Evaluation 2012). The selected regions encompass three regions with the highest incomes and three regions representing the lowest level of human development. While in the high income regions roughly 20 of the top 25 causes of death are both, in 1990 and 2010 related to non-communicable chronic and degenerative diseases the situation in the regions with lower human development shows a decrease of communicable and an increase in non-communicable diseases as major causes of death. In Central Sub-Saharan Africa, communicable disease represented 15 causes versus 6 non-communicable causes in 1990, in 2010 the situation changed in favour of the non-communicable diseases with 9 and communicable diseases with 12 of the top 25 causes of death. Nevertheless, in both years the top 5 causes of death were all due to infectious diseases. In Southeast Asia and Central Latin America the epidemiological change works in the same direction, but to a lesser degree, as in these regions the share of non-communicable diseases was already considerably higher in 1990. In these regions, all communicable causes of death within the top 25 ranking lost rank places between 1990 and 2010, except for HIV/AIDS which increased from rank 58 to 14 in Southeast Asia and from rank 26 to 11 in Central Latin America (Institute for Health Metrics and Evaluation 2012).

Top 25 causes of death, both sexes by selected region 1990, 2010 (Source: Institute for Health Metrics and Evaluation 2012: GBD 2010 Database. Accessed 21 January 2012)
Globally, the distribution of the causes of death between non-communicable and communicable diseases is more or less stable. Among the top 25 causes of death 13 belonged to the group of non-communicable diseases each in 1990 and 2010. However, a shift took place which lead to a loss of ranks of all communicable diseases among the top 25 causes of death, except for HIV/AIDS, which rose from rank 35 to 6 between 1990 and 2010. Measured in DALYs the global burden of disease also changed only slightly between 1990 and 2010, per capita the DALYs decreased by about 24胢%. In both years, 11 communicable causes were among the top 25 and 10 non-communicable in 1990 and 11 in 2010. Again all communicable causes lost ranks between 1990 and 2010, except HIV/AIDS, which increased from rank 33 to 5 and neonatal sepsis which increased by one rank. On the top lower respiratory infections, diarrheal diseases and preterm birth complication were replaced by ischemic heart disease, lower respiratory infections and stroke. Other non-communicable diseases which gained importance are low back pain (rank 11 to 6), major depressive disorder (15 to 11) and diabetes (21 to 14). The global HALE increased from 54.4胢years for males and 57.8胢years for females in 1990 to 58.3 and 61.8, respectively, in 2010. The increase took place in 19 of the 21 regions investigated by the GBD 2010 study. The exceptions were Sub-Saharan Africa, because of the impact of HIV/AIDS, and the Caribbean, due to the recent earthquake in Haiti. Compared to the life expectancy at birth, which increased by 4.7胢years for males and 5.1胢years for women between 1990 and 2010, the HALE at birth increased only by 3.9胢years and 4.0胢years, respectively. Some of the increased life expectancy at birth is consequently lost to periods spent in ill health (Institute for Health Metrics and Evaluation 2012, 2013; Salomon et al. 2012).
The change in the GBD along with the ageing of the population poses challenges to the health system as well as to family support networks. As more and more people in developing countries suffer from chronic degenerative diseases health systems have to prepare for additional and increasing costs of treatment. Families may face rising and lasting contributions to health costs (out of pocket spending) and an increasing need to care for family members in old age will become a reality with an ageing population prone to e.g. dementia or Alzheimer’s disease. As a consequence of rural to urban migration in many developing countries (urbanization) and smaller families, traditional familial support networks for those in ill health and old age are in need to be supplemented by other forms of support and care. Finally health systems in developing countries have to deal with the increasing impact of life-style risk factors like e.g. smoking, unhealthy diet, physical inactivity and the harmful use of alcohol (Frenk et al. 1991; UN 2011c: 22–26, 2012a; Vallin and Meslé 2004).
Life Expectancy at Birth
The long-term global trend in life expectancy at birth reflects an increase in physical health and its contribution to wellbeing through the general decrease of mortality over the life cycle (UN Population Division 2012). From 1950/55 to 2010/15, the life expectancy improved from 47.7 to 69.3胢years. This equals a growth of 21.6胢years or an increased life expectancy of 4.3胢months every year during this period. The subsequent period of the decades up to 2060/65 will see an additional gain in life expectancy of 8.2胢years to an average of 77.5胢years or a growth of 1.9胢months per year, according to the assumptions of the UN World Population Prospects. The further development up to 2100 shown in Fig.胢2.15 follows the general convergence paradigm underlying the UN Population Divisions projection assumptions (Bongaarts and Feeney 2002). When less and least developed countries will be reaching higher life expectancies at birth in the future, the further increase will level out, and as these regions gain more weight in the world population, they will more and more determine the growth path, with a life expectancy of the world population of more than 80胢years in 2100. The difference in life expectancy between the less developed regions as well as the least developed countries compared to the leading more developed industrialised countries decreased from 22.9 to 28.7胢years in 1950/55 to 8.4 and 19.1胢years in 2010/15 and if the trend continues, it is expected to decrease further. By 2060/65 the difference will be only 5.4 and 12.2胢years. Catching up the gap in life expectancy, the least developed countries are expected to exceed 70胢years around mid-century and the less developed regions will surpass today’s life expectancy of the developed regions during the last quarter of the century.

Life expectancy at birth, both sexes by level of development 1950–2100 (Source: UN World Population Prospects 2010 Revision, Medium Variant)
The fastest growth in life expectancy since 1950/55 took place in Asia, while Africa also improved its life expectancy up to the 1980s, when further development was increasingly affected by HIV/AIDS related growth in mortality. The effect can be analysed using the difference in life expectancy between the less developed regions and the least developed countries. The latter include most countries with a high HIV/AIDS prevalence. The difference was at a moderate level of 5.8胢years in the beginning of the 1950s and developed to 10.5胢years 2010/15. Over the next 50胢years the difference is expected to shrink and fall below the 1950s level with 5.4胢years in 2060/65.
The spatial patterns of the increase in life expectancy depicted in Fig.胢2.16 resemble the image gathered from analysing the indicators presented in the previous sub-sections. Living conditions, health and therefore life expectancy at birth will increase in most parts of the world. Developed regions are expected to reach a life expectancy of more than 80胢years by 2060/65. The same is true for most parts of Latin America, Northern Africa and the Near East as well as for China. Other parts of the developing world are improving too, and reaching values of more than 70胢years, such as India, which will develop at a pace with the trend expected for the countries of the former Soviet Union. An exception of the positive general outlook is Sub-Saharan Africa. Here, different trajectories have to be considered, reflecting the prevalence of armed conflicts and HIV/AIDS. Those countries with a high prevalence of HIV/AIDS and thus a low life expectancy today are assumed to profit most from the anticipated future success in fighting mortality from HIV/AIDS (see section “HIV/AIDS”).

Life expectancy at birth, both sexes 2010/15 and 2060/65 (Source: UN World Population Prospects 2010 Revision, Medium Variant, Map: ESRI, Cartography: F. Swiaczny and N. Ahmed)
Despite the shortcomings in reaching major health related development targets such as extreme poverty and malnutrition, set by the Millennium Development Goals, the general improvement of health conditions and development on a global scale has led to an unprecedented level of life expectancy. Even in Sub-Saharan Africa, which saw the least improvement of life expectancy among all regions since 1950/55, the life expectancy increased from 37.1胢years in 1950/55 by 17.9胢years to 55胢years in 2010/15, which is equal to the level of Turkey at the end of the 1970s.
Summary
In this chapter, the world’s population processes and their correlation with胢health indicators is investigated based on recent data and projections. Global population developments are in general determined by decreasing levels of fertility and increasing life expectancy due to shrinking levels of mortality. Both processes are related to the patterns of demographic change predicted by the model of demographic transition. They are also essentially linked to the positive development of the worldwide quality of life, which has been reported for a long time. During the demographic transition the world population is undergoing structural changes, too. The age distributions are shifting towards older cohorts and the median age is also increasing with relevant implications for the health conditions of such ageing populations. The population growth rate is currently declining and if fertility levels are continuing to decline as expected, based on current trends, the replacement fertility will lead to a stabilisation of the world population around the turn of the twenty-first century. If this future becomes true even the currently still fast growing least developed countries will face a “Demographic Dividend” which can contribute to development and higher quality of life in the poorest regions.
Improving health indicators are contributing to this development by reducing mortality, which is the cause for the rise in global life expectancy. A large share of the improvement of global health conditions is based on the reduction of a limited number of major causes: infant mortality, maternal health, the unmet need for family planning and the prevalence of communicable diseases (among others HIV/AIDS). Together, they contribute significantly to the reduction of the mortality in the developing regions and especially the least developed countries and are causal to the reduction of the still existing gap in life expectancy and gender disparity compared to the developed regions. Consequently these issues are core targets of the UN MDGs. Ageing on a global scale is a result of this demographic change, and ageing societies are also experiencing shifts in the health conditions because older populations are more prone to risks of chronic or degenerative diseases. They gain in significance, as with rising development the epidemiological transition leads to a shift in the causes of the burden of disease and death. Moreover, hand in hand with socioeconomic and societal development, improving survival conditions of children has a limiting effect on the desired fertility too, and the access to family planning methods provides the means to reduce the number of children.
In this chapter, it could be shown that the nexus between the growth of a population, its ageing and the related human development is not a limiting condition to the improvement of global health. Life expectancy at birth as a reliable indicator of physical health has reached an unprecedented level, and regional disparities are in general declining steadily. That population growth is, at least overall, not a limiting factor for health improvements is supported by the example of the poorest least developed countries in Sub-Saharan Africa. Despite the high growth rates and low human development there, efforts to fight communicable diseases (e.g. HIV/AIDS) have been proven successful in reducing mortality and increasing the life expectancy (again). Nevertheless, targets set by the MDGs are not yet fully met, and there is a need for further improvement in development on a global scale. While physical health conditions are improving in many countries and life expectancy is reaching ever higher levels, future development targets will have to shift the focus to broader dimensions of health. The definition proposed by WHO, which was a milestone on the way to improve quality of life and wellbeing, stated that health is more than the absence of disease and infirmity. Many developed countries, ahead in the epidemiological transition, have already shifted their implementation to a broader definition of health. Developing regions are expected to follow this example in order to reduce their burden of disease further and allow their population the “enjoyment of the highest attainable standard of physical and mental health” (article 12 of the International Covenant on Economic, Social and Cultural Rights).
References
Bloom, D. E., et al. (2003). The demographic dividend. A new perspective on the economic consequences of population change. Santa Monica/Arlington: Rand.
Blue, L., & Espenshade, T. J. (2011). Population momentum across the demographic transition. Population and Development Review, 37(4), 721–747.
Bongaarts, J. (1994). Population policy options in the developing world. Science, 263(5148), 771–776.
Bongaarts, J. (2003). Completing the fertility transition in the developing world. The role of educational differences and fertility preferences (Population Council PRD Working Papers, 177). Washington, DC: Population Reference Bureau.
Bongaarts, J. (2008). Fertility transitions in developing countries. Progress or stagnation? Studies in Family Planning, 39(2), 105–110. doi:10.1111/j.1728-4465.2008.00157.x.
Bongaarts, J. (2009). Human population growth and the demographic transition. Philosophical Transactions of the Royal Society, B: Biological Sciences, 364(1532), 2985–2990. doi:10.1098/rstb.2009.0137.
Bongaarts, J., & Feeney, G. (2002). How long do we live? (Population Council Policy Research Division Working Papers, 156). New York: Population Council.
Büttner, T., & Zlotnik, H. (2005). Prospects for increasing longevity as assessed by the United Nations. Genus, LX(1), 213–233.
Caldwell, J. C. (2004). Demographic theory. A long view. Population and Development Review, 30(2), 297–316.
Caldwell, J. C., & Schindlmayr, T. (2002). Historical population estimates. Unravelling the consensus. Population and Development Review, 28(2), 183–204.
Camfield, L., & Skevington, S. M. (2008). On subjective well-being and quality of life. Journal of Health Psychology, 13(6), 764–775.
Canning, D. (2011). The causes and consequences of demographic transition. Population Studies, 65(3), 353–361.
De Souza, R.-M., et al. (2003). Critical links. Population, health, and the environment. Population Bulletin, 58(3), 3–43.
Dyson, T. (2010). Population and Development. The demographic transition. London/New York: Zed Books.
Frenk, J., et al. (1991). Elements for a theory of the health transition. Health Transition Review, 1(1), 21–38.
Gaziano, T. (2011). Prevention and treatment of chronic diseases in developing countries (Population Division Expert Paper, 2011/2). New York: UN DESA.
Glatzer, W. (1991). Quality of life in advanced industrialized countries. The case of West Germany. In F. Strack et al. (Eds.), Subjective well-being. An interdisciplinary perspective (International series in experimental social psychology, Vol. 21, pp. 261–279). Oxford/New York: Pergamon Press.
Goldstein, J. R., et al. (2009). The end of “lowest-low” fertility. Population and Development Review, 35(4), 663–699.
Gould, W. T. S. (2009). Population and Development. Oxon: Routledge.
Haupt, A., & Kane, T. T. (2004). Population Reference Bureau’s population handbook (5th ed.). Washington, DC: Population Reference Bureau.
Hotez, P. J. (2011). The development impact of the neglected tropical diseases (NTDs) (Population Division Expert Paper, 2011/1). New York: UN DESA.
Institute for Health Metrics and Evaluation. (2012). The global burden of diseases, injuries, and risk factors study 2010. Online Database. www.healtmetricsandevaluation.org/gbd/visualizations. 21 Jan 2012.
Institute for Health Metrics and Evaluation. (2013). The global burden of diseases. Generating evidence, guiding policy. Washington: University of Washington.
Klein Goldewijk, K. (2005). Three centuries of global population growth. A spatial referenced population density database for 1700–2000. Population and Environment, 26(4), 343–367. doi:10.1007/s11111-005-3346-7.
Kremer, M. (1993). Population growth and technological change. One million B.C. to 1990. Quarterly Journal of Economics, 108(3), 681–716.
Maddison, A. (2001). The World Economy. A millennial perspective. Paris: OECD.
McEvedy, C., & Jones, R. (1978). Atlas of world population history. Harmondsworth: Penguin Books.
McFalls, J. A. (2003). Population. A lively introduction (4th ed.). Population Bulletin, 58(4), 3–40.
Mendez, M. A., Monteiro, C. A., & Popkin, B. M. (2005). Overweight exceeds underweight among women in most developing countries. American Journal of Clinical Nutrition, 81, 714–721.
Molinas, J. R., et al. (2009). Measuring inequality of opportunities in Latin America and the Caribbean. Washington, DC: Palgrave/World Bank.
Molinas, J. R., et al. (2010). Do our children have a chance? The 2010 human opportunity report for Latin America and the Caribbean. Washington, DC: World Bank.
Morris, M. D. (1979). Measuring the condition of the world’s poor. The physical quality of life index. New York: Pergamon.
Moultrie, T., Sayi, T. S., & Timaeus, I. M. (2012). Birth intervals, postponement, and fertility decline in Africa. A new type of transition. Population Studies, 66(3), 241–258.
Notestein, F. W. (1950). The population of the world in the year 2000. American Statistical Association Journal, 45(251), 335–349.
Notestein, F. W. (1952). The economics of population and food supplies. Proceedings of the 8th Conference of Agricultural Economists, 1952(8), 13–31.
Oeppen, J., & Vaupel, J. W. (2002). Broken limits to the life expectancy. Science, 296(5570), 1029–1031.
Olshansky, J. S., & Ault, B. (1986). The fourth stage of the epidemiologic transition. The age of delayed degenerative diseases. The Milbank Quarterly, 64(3), 355–391.
Omran, A. R. (1971). The epidemiologic transition: A theory of the epidemiology of population change. The Milbank Memorial Fund Quarterly, 49(4), 509–538.
Omran, A. R. (1998). The epidemiologic transition theory revisited years later. World Health Statistics Quarterly, 53(2–4), 99–119.
O’Neill, B., & Balk, D. (2001). World population futures. Population Bulletin, 56(3), 3–40.
O’Neill, B., et al. (2001). A guide to global population projections. Demographic Research, 4, 203–288.
Pearce, F. (2010). Peoplequake. London: Eden Project Books.
Population Reference Bureau. (2004). Transition in world population. Population Bulletin, 59(1), 3–40.
Preston, S. H., et al. (2001). Demography. Measuring and modelling population processes. Oxford: Blackwell.
Reher, D. S. (2007). Towards long-term population decline. A discussion of relevant issues. European Journal of Population, 23(2), 189–207.
Rowland, D. T. (2006). Demographic methods and concepts. Oxford: Oxford University Press.
Rowland, D. T. (2012). Population ageing (International perspectives on aging, 3). Dordrecht: Springer.
Salomon, J. A., & Murray, C. J. (2002). The epidemiologic transition revisited. Compositional models of causes of death by age and sex. Population and Development Review, 28(2), 205–228.
Salomon, J. A., et al. (2012, December 13). Healthy life expectancy for 187 countries, 1990–2010: A systematic analysis for the Global Burden Disease Study 2010. The Lancet, 380, 2144–2162. [Publication Summary http://www.healthmetricsandevaluation.org/gbd/publications /healthy-life-expectancy-187-countries-1990-2010-systematic-analysis-global-bu. 30 Jan 2013]
Sen, A., & Nußbaum, M. (Eds.). (1993). The quality of life. Oxford: Clarendon.
Schoumaker, B. (2009). Stalls in fertility transition in Sub-Saharan Africa. Real or spurious? (Document de Travail, Dept. des Sciences de la Population et du Développement Louvain, 30). Louvain: Dept. des Sciences de la Population et du Développement Louvain.
Shetty, P., & Schmidhuber, J. (2011). Nutrition, lifestyle, obesity and chronic disease (Population Division Expert Paper, 2011/3). New York: UN DESA.
Singh, S., & Darroch, J. (2012). Adding it up: Costs and benefits of contraceptive services. Estimates for 2012. New York: Guttmacher Institute, UNFPA.
Strack, F., et al. (Eds.). (1991). Subjective well-being. An interdisciplinary perspective (International series in experimental social psychology, 21). Oxford/New York: Pergamon Press.
Streeten, P., et al. (1981). First things first. Meeting basic human needs in the developing countries. New York/Oxford: Oxford University Press.
Swiaczny, F. (2010). Zukunft der Weltbevölkerung. In K. Husa, Ch. Parnreiter, H. Wohlschlägl (Eds.), Weltbevölkerung (Historische Sozialkunde/Internationale Entwicklung, 30, pp. 39–60). Wien: Promedia. [Future of World Population. Figures with English Glossary available at http://www.swiaczny.de/HSK30_Abbildungen_Figures.pdf].
Swiaczny, F., & Grünheid, E. (2012). Weltbevölkerung und Millennium-Entwicklungsziele. Geographische Rundschau, 64(11), 48–55.
Swiaczny, F., & Henning, S. (2011). Die Welt mit 7 Mrd. Menschen. Globalisierung und Demographischer Wandel. Geographische Rundschau, 63(9), 56–61.
UN. (1948). Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June, 1946. In Official Records of the World Health Organization 2. New York/Geneva: WHO, 100.
UN. (1995). Report of the International Conference on Population and Development, Cairo 5–13 September 1994 (A/CONF.171/13/Rev.1). New York: UN.
UN. (2009). World population monitoring, focussing on the contribution of the Programme of Action of the International Conference on Population and Development to the internationally agreed development goals, including the Millennium Development Goals (E/CN.9/2009/3). New York: UN.
UN. (2010). UN World Population Prospects. The 2010 revision. http://esa.un.org/unpd/wpp/index.htm. 1 July 2012.
UN. (2011a). Fertility, reproductive health and development (E/CN.9/2011/3). New York: UN.
UN. (2011b). The Millennium Development Goals report 2011. New York: UN.
UN. (2011c). United Nations expert group meeting on health, mortality and development (ESA/P/WP.218). New York: UN.
UN. (2012a). Population ageing and the non-communicable diseases. Population Facts 2012(1), 1–2.
UN. (2012b). Towards global equity in longevity. Population Facts 2012(2), 1–4.
UN. (2013). A new global partnership: Eradicate poverty and transform economies through sustainable development. The Report of the High-Level Panel of Eminent Persons on the Post-2015 Development Agenda. New York: UN.
UN Population Division. (1999). The world at six billion (ESA/P/WP.154). New York: UN.
UN Population Division. (2004a). World population in 2300. In Proceedings of the United Nations Expert Meeting on World Population in 2300 (ESA/WP.187/Rev.1). New York: UN.
UN Population Division. (2004b). World population to 2300 (ST/ESA/Ser.A/236). New York: UN.
UN Population Division. (2011a). Seven billion and growing: The role of population policy in achieving sustainability (Population Division Technical Paper 2011/3). New York: UN.
UN Population Division. (2011b). World Mortality report 2009 (ST/ESA/SER.A/315). New York: UN.
UN Population Division. (2011c). Assumptions underlying the 2010 revision. http://esa.un.org/unpd/wpp/Documentation/pdf/WPP2010_ASSUMPTIONS_AND_VARIANTS.pdf. 1 July 2012.
UN Population Division. (2012). Changing levels and trends in mortality (ST/ESA/SER.A/318). New York: UN.
UNAIDS. (2010). Report on the global AIDS epidemic. Geneva: UNAIDS.
UNDP. (1994). Human development report 1994. New York/Oxford: Oxford University Press.
UNDP. (2011). Human development report 2011. Houndmills/New York: Palgrave Macmillan.
UNFPA. (2012). 2011 annual report. Delivering results in a world of 7 billion. New York: UNFPA.
Vallin, J., & Meslé, F. (2004). Convergences and divergences in mortality. Demographic Research – Special胢collection 2, 11–44.
van de Kaa, D. J. (1987). Europe’s second demographic transition. Population Bulletin, 42(1), 1–55.
Veenhoven, R. (1996). Happy life-expectancy. A comprehensive measure of quality-of-life in nations. Social Indicators Research, 39, 1–58.
Veenhoven, R. (2005). Apparent quality-of-life in nations. How long and happy people live. Social Indicators Research, 71(1–3), 61–86.
Weeks, J. R. (2008). Population. An introduction to concepts and issues (10th ed.). Belmont: Thomson Wadsworth.
WHO. (2004). The World Health Organization Quality of Life (WHOQOL)-BREF. Geneva: WHO.
WHO. (2008). The global burden of disease. 2004 update. Geneva: WHO.
WHO. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. Geneva: WHO.
WHO, UNICEF, UNFPA, & World Bank. (2012). Trends in maternal mortality: 1990 to 2010. Geneva: WHO.
Woods, R. (1982). Theoretical population geography. London/New York: Longman.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Swiaczny, F. (2015). Demographic and Health Development in the Long Run. In: Glatzer, W., Camfield, L., Møller, V., Rojas, M. (eds) Global Handbook of Quality of Life. International Handbooks of Quality-of-Life. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-9178-6_2
Download citation
DOI: https://doi.org/10.1007/978-94-017-9178-6_2
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-9177-9
Online ISBN: 978-94-017-9178-6
eBook Packages: Humanities, Social Sciences and LawSocial Sciences (R0)