
Abstract
Anhedonia is the reduced ability to experience pleasure emotion and has been considered a key symptom in schizophrenia spectrum disorders. However, little is known about the hedonic capacity and related neural basis for individuals prone to develop psychosis such as people with schizotypal personality traits. On the other hand, anhedonia is a complex, multidimensional construct that is important for social interaction and functioning in both healthy individuals and people with neuropsychiatric disorders. However, most measures of anhedonia are limited to clinical rating and self-report checklists that adopt a unitary concept. Increasing interest has emerged in the past decade to subdivide this construct into anticipatory and consummatory experience of pleasure. This book chapter will examine these two facets of anhedonia in individuals with schizotypal personality traits using a multi-pronged approach, including self-report questionnaires, computerized tests, and neuroscientific measures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Emotional impairments have been considered core features of negative symptoms of schizophrenia and one of the most critical determinants of functional outcome of this clinical group [1, 2]. Anhedonia is defined as the diminished ability to experience pleasure, whereas avolition is defined as the diminished motivation to seek and sustain in goal-directed behaviour driven by positive or desirable events or the possibility of these events happening [3, 4]. Negative symptoms in schizophrenia present great challenge to available treatments [5, 6] and have significant bearings on prognosis. The reason which could account for the difficulties in finding effective treatment is that the nature (especially the neural mechanism) of anhedonia in schizophrenia remains unclear. However, even though the clinical understanding of anhedonia in schizophrenia is not completely clear, it is commonly acknowledged that there is an “emotional paradox” observed in this clinical group. Patients with schizophrenia demonstrate intact pleasurable experience when they are presented with evocative stimuli in laboratory-based assessments when compared to their self-reported pleasure experience [7–11]. Moreover, the study of anhedonia has been extended to at-risk individuals before the development of the disorder such as individuals with schizotypal personality disorder (SPD) traits. In Meehl’s [12] model of schizophrenia, he considers anhedonia as an important marker of genetic vulnerability for schizophrenia which can also be observed in individuals at risk of developing the illness such as those exhibiting SPD traits. Studying anhedonia in these medication-free individuals with SPD traits can help us understand the nature of hedonic capacity in patients with schizophrenia.
In an effort to address the complex nature of anhedonia in schizophrenia spectrum disorders, the present chapter summarizes up-to-date findings of anhedonia in individuals with SPD traits. We begin with the conceptualization of SPD and its relationship with schizophrenia spectrum disorders, and the current constructs of hedonic capacity. We emphasize how important the current view and conceptualization of hedonic capacity (or anhedonia) is in understanding the aforementioned emotion paradox observed in this clinical group. In particular, we focus on the two distinct components of pleasure experience, namely anticipatory and consummatory pleasure, and their relationships to the objective laboratory-based assessments of hedonic capacity in individuals with SPD traits.
2 Conceptualizaiton of SPD and Its Relationship with Schizophrenia Spectrum Disorders
Meehl [12] proposed that schizotaxia, a genetic liability, predisposes an individual to develop some form of disorganization termed schizotypal behaviours which in turn will form a predisposition to schizophrenia. However, he also pointed out that this genetic risk alone is not sufficient for the development of schizophrenia. This implies that individuals with schizotypal traits can have behavioural manifestations that range from nearly normal to clinically abnormal presentation. Since then, Paul Meehl’s theory has evolved into two separate but related lines of research. The first one focuses on schizotypy traits that comprise cognitive slippage (mild associative loosening), anhedonia (pleasure-capacity deficit), ambivalence, and interpersonal aversiveness (social fear) [13, 14]. The second one focuses on the constellation of symptoms indicating the presence of schizotypy. The DSM-IV [15] adopts such a construct to diagnose SPD as part of the personality disorders on Axis II, which is characterized by positive (e.g., magical thinking, Ideas of reference) and negative (e.g., social withdrawal, anhedonia) symptoms [16]. However, more recent work suggests that SPD is better conceptualized as an attenuated form of schizophrenia [17]. SPD has also been considered to be one of the operational criteria for the schizophrenia prodrome [17]. An SPD diagnosis encompasses subclinical positive and negative symptoms of schizophrenia. The conversion rate of prodrome to full-blown psychosis is roughly between 25 and 45 % 1 year after the diagnosis of schizophrenia prodrome [18]. The prevalence of SPD in the general population is about 3 % (DSM-IV, 2000). Biological relatives of patients with schizophrenia have a higher prevalence of SPD [19]. Researchers have suggested a continuum concept of psychosis with SPD and schizophrenia lying on the extremes, ranging from nearly normal functioning to psychotic disorders [20]. Empirical evidence has also demonstrated that SPD traits are commonly distributed in the general population [21, 22].
In this chapter, we operationally define SPD traits as the traits generally covering the concepts of both Paul Meehl’s theory of schizotypy and the DSM-IV-based construct of attenuated form of schizophrenia. However, it should be noted that the original conceptualization of schizotaxia or schizotypy proposed by Meehl [23] does not exactly match the DSM-IV diagnosis of schizotypal personality disorder. In Meehl’s viewpoint, schizotypy refers to a latent personality organization and is essentially a broader construct linked to a developmental theory, whereas the SPD in DSM-IV is an atheoretical categorization or aggregation of a set of observable signs and symptoms. Moreover, individuals with SPD traits, like their clinical counterparts, may also demonstrate subtypes of behavioural manifestations, i.e., dominant with negative-like and positive-like symptoms. Lastly, we have included both clinically diagnosed SPD and psychometrically defined SPD in the discussion in the present chapter.
3 Current Construct of Hedonic Capacity and Its Underlying Neural Mechanisms
Anhedonia is commonly defined as the inability to experience pleasure and is a core feature of schizophrenia and depression [24, 25]. Traditionally it is conceptualized as a unitary construct of diminished momentary pleasure experience [26–31]. For example, Rado [32] posited that anhedonia is the inherited predisposition to schizophrenia as a result of the inability to experience pleasures and a lack of motive to engage in rewarding activities. It has then been incorporated into Meehl’s construct of schizotypy [12, 23] and subsequent assessment of physical and social anhedonia in schizotypy [33]. However, although the current literature demonstrates a consistent pattern of emotional deficits in schizophrenia spectrum disorders, recent findings have highlighted the presence of an “emotional paradox” in patients with schizophrenia [7, 8, 34]. While patients with schizophrenia could report experiencing strong emotions (including pleasant emotion) in response to emotional material, they do not often report experiencing strong pleasant emotions in naturalistic situations [34]. These findings were not confounded by the corresponding cognitive and language disturbances that often accompany schizophrenia and convergent evidence indicates that these patients are able to provide reliable and valid reports of emotional experience [7, 9, 35].
The advance of neuroscience in both animal and human research now suggests that anhedonia is a multidimensional construct that comprises at least two components, namely consummatory and anticipatory pleasure [36–39]. Consummatory pleasure is the ability to experience momentary pleasure (i.e., the feeling of liking) when an individual is directly engaging in an enjoyable activity; whereas anticipatory pleasure is the ability to experience a motivated and goal-directed behaviour (i.e., the feeling of wanting) for a future pleasant event [40, 41]. Motivation is always accompanied by hedonic experience, especially anticipatory experience of pleasure (appetitive pleasure) [36, 37, 40, 41]. Berridge and Robinson [41, 42] argue that “wanting” (anticipatory) behaviour is equivalent to approach motivation and is closely associated with appetitive pleasure in animals. Knutson’s anticipatory affect model further posits that the neural response of the nucleus accumbens correlated with anticipatory pleasure (arousal) predicts motivated behaviour in the future [36]. Studies on the dopamine system have shown that dopamine in the reward process is classically linked to the anticipatory experience of pleasure [43], and data suggest that the dopamine system also plays a motivational role [41]. Neuroanatomical hotspots have also been linked up with hedonic capacity [43, 44]. For example, the orbitofrontal and cingulate cortices as well as the insular cortices contribute to experiences of pleasure. Subcortical areas such as the dorsal and ventral striatum and the amygdala have also been implicated in the processing of positive emotional or reward stimuli. In particular, the orbitofrontal cortex takes up an important role in linking reward to hedonic experiences [45]. Patients with schizophrenia have been found to have hypoactivation at the ventral striatum and orbitofrontal cortex when compared with healthy controls, although it is still not clearly known whether schizophrenia is associated with impaired reward valuation and motivation rather than a diminished processing of hedonic capacity [4, 9, 46].
The outstanding issue of hedonic capacity in general and anhedonia research in schizophrenia in particular is that the nature of the subjective experience of pleasure is still not fully understood. The study of anhedonia in schizophrenia is further complicated by the impact of clinical symptoms, medications, as well as the associated impairment of cognitive functioning and insight. Despite these challenges, the question of anhedonia in SPD can still be approached using a multi-pronged approach, utilizing findings from self-reported, behavioural and imaging work.
4 Self-Reported Anticipatory and Consummatory Pleasure in Individuals with SPD Traits
The current literature suggests that all but one self-reported measure of experiential pleasure were based on the unitary construct of pleasure. The Temporal Emotional Experience of Pleasure Scale (TEPS) [3] is an 18-item checklist that captures both the anticipatory (10 items) and consummatory (8 items) components of pleasure experience in schizophrenia research. Satisfactory construct validity, internal consistency, test-retest reliability and clinical discrimination have been demonstrated [3, 38, 47–49]. The TEPS can serve as an important tool to evaluate the subjective experience of individuals with SPD traits.
Martin et al. [50] were among the first few researchers to adopt the two-facet perspective of pleasure experience to study individuals with SPD traits. They first screened and recruited their potential participants using the Revised Social Anhedonia Scale [51] and Perceptual Aberration/Magical Ideation scale [52, 53]. Then they compared these two facets of experiential pleasure using the TEPS. Their findings showed that individuals with negative SPD traits (elevations in social anhedonia score) had significantly lower scores on both the anticipatory and consummatory subscales of the TEPS. However, no significant difference was found between individuals with positive SPD traits (elevations in magical ideation and perceptional aberrations) and healthy controls.
Gooding et al. [49] administered the TEPS to specifically examine the experience of pleasure in individuals with and without SPD traits using the TEPS. They further classified the participants into negative SPD traits and positive SPD traits, and healthy controls without these traits. Their results showed that only the subtype of SPD traits characterized by social anhedonia but not the subtype characterized by positive symptom-like behaviour reported deficits in both anticipatory and consummatory pleasure when compared with the individuals without SPD traits. These authors also found that working memory was differentially associated with the anticipatory and consummatory components of experiential pleasure. That is, significant association was only found between the consummatory components of the TEPS and working memory. These findings suggest that individual with negative SPD traits (socially anhedonia) share similar diminished anticipatory and consummatory pleasure reported in patients with schizophrenia.
Shi et al. [54] screened out a sample of 1,039 college students from an extended pool of participants in a mentally at-risk study using the Schizotypal Personality Questionnaire [55, 56] and recruited 117 individuals with SPD traits and 116 individuals without SPD traits. They then classified their SPD sample into positive and negative SPD using cluster analysis. They found that individuals with negative SPD traits demonstrated significantly lower TEPS anticipatory subscore than healthy controls. However, the two groups did not differ significantly in terms of consummatory subscore and total TEPS score. In contrast, individuals with positive SPD traits had significantly higher anticipatory and consummatory subscores as well as total TEPS score than both negative SPD and healthy controls. These findings are consistent with those demonstrated in patients with schizophrenia. In particular, the negative SPD group reported diminished anticipatory pleasure but relatively intact consummatory pleasure compared to healthy controls. Interestingly, Shi et al. [54] also found that individuals with negative SPD traits showed the least emotional expression and reported the highest levels of problems with memory as well as other depressive symptoms compared to controls. The pattern seems to be reversed in individuals with positive SPD traits with heightened pleasure experience compared to healthy controls. However, there was no significant difference between the two groups of participants in terms of emotion expression. These findings have been cross-validated by another independent study [57] showing that SPD traits could be clustered into subtypes, and with the negative group reported the lowest emotional experience ability on both anticipatory and consummatory pleasure experience than the positive and low SPD groups.
Extending the line of continuum of psychosis proposed by van Os et al. [21], Chan et al. [48] demonstrated that anhedonia, as measured by the Chapman Scales for Physical and Social Anhedonia [51], could serve as an enduring trait similar to psychotic symptoms distributing along the non-clinical sample. Significant correlations were found between SPD traits, physical and social anhedonia. More importantly, the anticipatory and consummatory subscores as well as the total TEPS score were all inversely and significantly correlated with physical and social anhedonia. However, when the sample was split into individuals with and without SPD traits, individuals with SPD traits did not report diminished experiential anticipatory and consummatory pleasure as assessed by the TEPS. These findings may be due to the heterogeneity of SPD traits similar to that of schizophrenia patients. It is likely that only the negative subtype of SPD trait is associated with subjective pleasure experience impairment. Unfortunately, Chan et al. [48] did not report any subtype comparison in their study. The inconsistent findings might have also been due to the variability of the reported TEPS scores among different studies. Strauss et al. [58] suggest that it is likely that self-reported anticipatory and consummatory pleasure may be influenced by demographic differences (e.g., ages, gender, education, and ethnicity).
Taken together, the above findings suggest that individuals with SPD traits show a similar pattern of self-reported anticipatory and consummatory pleasure with patients with schizophrenia. However, it is necessary to examine negative and positive SPD traits as separate entities to avoid confusion and misunderstanding in their emotional manifestations.
5 Experimental Tasks for Anticipatory and Consummatory Pleasure in Individuals with SPD Traits
Experimental studies of anhedonia in individuals with SPD traits were mainly limited to a unitary construct of anhedonia. The literature in this area suggests that individuals with SPD traits may experience a reduction in self-reported pleasure in response to experimental stimuli [59, 60] although there has also been studies showing no such difference [61]. Few studies have adopted an experimental paradigm to examine the anticipatory and consummatory components of pleasure experience in individuals with SPD traits. Yan et al. [62] conducted two experiments to examine specifically approach motivation based cognitive function and perceptual function in individuals with SPD traits, respectively. In their first experiments, they administered a memory probabilistic reward task based on signal detection theory to capture approach motivation. In this task, participants were first required to learn 15 pictures of sign language and were then asked to recognize the pictures that they had seen from 90 pictures comprising pictures that they had learned and not learned. Participants were informed that correct recognition of the pictures that they had learned would be accompanied by more reward. Three blocks with varied amount of reward (0, 5, 10 points) were administrated to each participant. They found that participants would increase their approach motivation along the increment of reward. Although demonstrating elevated level of anhedonia, individuals with SPD traits (n = 20) did not differ in their response bias (log b) when compared with individuals without SPD traits (n = 20) during the recognition phase, indicating that approach motivation may be intact in these individuals. In their second study, participants from another sample pool were asked to perform a perceptual probabilistic reward task. In each block of this task, participants were presented with two types of stimuli: a face with a long mouth and a face with a short mouth, and they were required to judge whether the mouth was long or not. The face with a long mouth was accompanied by more reward than the face with a short mouth. Feedback followed the participants’ judgment. Each participant was asked to perform three blocks. They observed that individuals with SPD traits (n = 24) did not display attenuated approach motivation. On the contrary, they showed a trend of enhanced approach motivation compared to individuals without SPD traits (n = 24) (p = 0.06). Taken together, these two experiments suggest that individuals with SPD traits tend to report higher levels of anhedonia, especially experiential pleasure in anticipation of future events, than healthy controls. However, no impairment was found in the approach motivation in these individuals using either the memory or the perceptual signal detection task. These authors postulated that the insignificant findings in approach motivation might be due to the fact that SPD individuals needed no additional effort to gain the reward similar to healthy controls in smoking motivation [63].
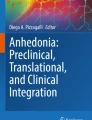
However, it is not known whether reward learning is stable or not over time and the effect of stress on reward response in these individuals. We adopted a probabilistic reward learning task developed by Bogdan and Pizzagalli [64] to a group of individuals with and without SPD traits. We modified this task by making the stimuli conditions transparent to the participants during the reward learning task, hence allowing the participants to make an informed discrimination between the two possible stimuli (reward asymmetry). This modified task has been successfully applied to discriminate patients with major depression from healthy controls [65]. However, our unpublished data on SPD showed that there was no significant difference in all parameters of this reward learning task between individuals with (n = 31) and without (n = 31) SPD traits. Figure 10.1 shows that the main effect of block was significant (F (2, 59) =19.316, p < 0.001, partial η 2 = 0.244) with a diminished response bias over time (Block 1 > Block 2 > Block 3, all ps < 0.01). The interaction among condition, block and group was also significant (F (2, 59) = 3.205, p < 0.044, partial η 2 = 0.051). However, no other significant effects were found except for block effect in each group. When we further examined whether introducing stress would change the response bias in individuals with SPD traits, we found that there was only a trend of interaction between condition and block (F (1, 60) = 3.661, p = 0.060, partial η 2 = 0.058) (Fig. 10.2). Moreover, a check on the discriminability between individuals with and without SPD traits showed that there was only a main effect of Block (F (2, 59) = 10.139, p < 0.001, partial η 2 = 0.145) with a diminished response bias (Block 1 < Block 2, Block 1 < Block 3, all ps < 0.005). Other variables were all non-significant (all Fs < 3.876; all ps > 0.054). These findings suggest that individuals with SPD traits did not demonstrate any difficulties in maintaining positive affect to appetitive stimulus and possess intact ability to experience consummatory pleasure (Fig. 10.3).

The response bias in the individuals with SPD traits group and health control group from block 1 to block 3 under the stress condition and no stress condition

The change of a response bias in the individuals with SPD traits and health control under the stress condition and no stress condition

The discriminability in the individuals with SPD traits group and health control group from block 1 to block 3 under the stress condition and no stress condition
Lui et al. [66] conducted two experiments to examine emotion-volition decoupling in patients with first-onset schizophrenia and healthy controls, as well as individuals with and without SPD traits. They adopted a task developed by Heerey and Gold [67] to examine the anticipation and consummation of experiential pleasure. They found that both patients with first-onset schizophrenia and individuals with SPD showed similar affective experiences as their controls but their experiences were significantly less predictive of their behaviour. This emotion-volition decoupling was more impaired in anticipatory than in consummatory pleasure experience for patients with schizophrenia. These findings suggest that emotion-volition decoupling can be demonstrated in patients with few negative symptoms in the early course of schizophrenia and in individuals with SPD traits. However, the latter seems to show a milder form of impairments when compared with the clinical group.
Strauss et al. [68] examined specifically both state and trait anhedonia between patients with schizophrenia, individuals with psychometric schizotypy, and healthy controls. They administered the Positive and Negative Affect Schedule (PANAS) [69] to examine the trait affect in these participants and found that individuals with schizotypy did not show significant differences from patients. However, for state affect, which was assessed by a mood-induction task that asked participants to evaluate their affective state (pleasant and unpleasant, separately) followed by seeing neutral/good/bad affective images, individuals with schizotypy reported lower pleasant ratings on each conditions than the other three groups, but no significant difference was found on unpleasant emotion ratings. They also showed that the negative subscale scores in schizotypy were negatively correlated with pleasant emotion ratings, whereas blunted affect was found to be inversely associated with pleasant ratings in patients with schizophrenia. These findings suggest that there might be another paradox in the schizophrenia spectrum in that for state anhedonia, individuals with schizotypy demonstrated diminished pleasure, whereas schizophrenia patients did not.
6 Neuroimaging Findings of Anhedonia in Individuals with SPD Traits
Substantial evidence from structural brain imaging studies indicates that individuals with SPD traits, particularly clinically diagnosed individuals with SPD, often exhibit a wide range of brain abnormalities including a reduction in grey matter volume in the temporal lobe, the frontal lobe, the parietal lobe, the basal ganglia [70] and the posterior cingulate cortex [71]. However, most of these studies focused on positive-like symptoms rather than negative symptoms. More recently, Asami et al. [72] adopted the voxel-based morphometry method to examine 54 clinically diagnosed SPD individuals and 54 healthy controls and found that there was a significant reduction in grey matter volume in individuals with SPD in the left superior temporal gyrus and widespread frontal, frontolimbic and parietal regions compared to healthy controls. More importantly, reduction in grey matter volume in these regions was significantly correlated with negative symptoms. However, it should be noted that neither a unitary construct nor a two-facet construct of anhedonia was specifically examined in this clinically diagnosed SPD sample.
Harvey et al. [73] were among the first to examine the enduring trait of anhedonia using both structural and functional imaging methods in a group of college students. The optimized Voxel Based Morphometric (VBM) analysis was adopted for structural images preprocessing and the structural correlates of trait anhedonia, assessed by the Chapman Physical Anhedonia Scale [33], was examined by regression analysis. The results showed that the grey matter volume of bilateral anterior caudate was inversely correlated with trait anhedonia. In the same study, they also examined brain activity during the viewing of positive pictures compared to neutral pictures and its relationship with trait anhedonia. Positive associations between trait anhedonia and brain activity of the ventromedial prefrontal cortex, the middle and superior found during the processing of positive information. These findings suggest a specific kind of vulnerability for the development of affective disorders and suggest that trait anhedonia may be linked to a volumetric reduction in the basal ganglia and to a prefrontal functional abnormality during hedonic processing. However, it should be noted that the authors did not attempt to discriminate individuals with SPD traits from those without SPD traits. These authors did not find any significant inverse association between trait anhedonia severity and functional activation in subcortical regions. These might be due to the fact that the authors did not use a selection method to divide the participants into those with SPD and without SPD traits. Moreover, anhedonia was only defined by the physical domain of the Chapman Physical Anhedonia Scale [33] and did not take into the consideration of the social domain, and more importantly, the two-facet component of anhedonia. Future research should adopt a reward-based paradigm that could specifically characterize the subtle relationship between the structural and functional correlates of anhedonia in different contexts.
Empirical findings on neural network associated with pleasure may provide insight into the study of anhedonia in individuals with SPD traits. For example, individuals with anhedonia in social interaction have been found to have less neural activity in facial expression discrimination regions such as the medial prefrontal cortex, the right superior temporal gyrus, and the left somatosensory cortex [74]. Interpersonal relationship of individuals with SPD traits has been particularly shown to correlate with reduced accuracy on the facial expression recognition task [75]. However, very few studies have been conducted to examine the neural activities of individuals with SPD traits in a social interaction situation. Huang et al. [76] developed a dyadic conversation paradigm to examine dynamic happy facial expression processing in different social interaction contexts in individuals with and without SPD traits. Their findings showed that bilateral activation of the prefrontal cortex during the contrast of happiness appearing and disappearing. More regions such as the right parahippocampal gyrus and the right insula were activated when contrasting the “praise”-“blame” cues. Individuals with SPD traits were found to exhibit less deactivation to the happiness disappearing faces than healthy controls in the rostral anterior cingulate. These SPD individuals also showed more deactivation than healthy controls in the left prefrontal cortex and the rostral superior temporal gryus with “blame” cues. However, the two groups did not differ in the contrast of incongruent and congruent conditions. If we merged the data from the two groups, we found two cortical regions (the right superior frontal gyrus and the left inferior occipital gyrus) which were sensitive to the incongruence between dynamic facial expression and social interaction context. When we re-analyzed the data with the TEPS score retrospectively, we found that the beta value of activation in the right superior frontal gyrus in the happiness appearing of blame context was significantly correlated with TEPS total score while the left inferior occipital gyrus was not. This might suggest that the right superior frontal region was involved in both processing the context-face incongruence and pleasure experience. Taken together, these findings suggest individuals with SPD traits have different neural inhibition mechanisms when processing the happiness disappearing stimuli with “blame” cues.
Recently, in addition to the conventional univariate analysis, novel multivariate approaches for the analysis of fMRI data are emerging. Unlike the univariate approach detecting the averaged activation differences in the brain [77], multivariate approach can detect fine-grained changes in neural representations and reflect more information in neural activation pattern than mean activation [78–80]. In Modinos et al.’s recent study, the Community Assessment of Psychic Experiences questionnaire [81] was used to identify participants with psychosis-proneness/SPD [82]. Each participant was required to view the neutral and negative valenced pictures from the International Affective Pictures System during scanning. Multivariate pattern analysis was employed to distinguish individuals with SPD traits from those without SPD traits during negative emotion processing. A unique pattern of activation was found between these two groups in the amygdala, the insula, the anterior cingulate cortex, the orbital frontal cortex, and the medial prefrontal cortex, while the conventional univariate analysis could not detect such differences. Our unpublished imaging data further suggest an altered medial orbitofrontal activation pattern during the experience of consummatory pleasure in individuals with SPD traits. Specifically, individuals with SPD traits could not differentiate the activation pattern of consummatory pleasure from consummatory negative emotion at the medial orbitofrontal cortex.
In summary, anhedonia is the reduced capacity to experience pleasure and is one of the negative symptoms in schizophrenia. Anhedonia is also one of the main symptoms confounding the functional outcome of patients with schizophrenia. Reduced hedonic capacity can also be measured as an enduring trait in non-clinical subjects. Such altered hedonic capacity is likely the result of a basic neuropsychophysiological dysfunction and a vulnerability marker that potentially precedes and contributes to the liability of developing psychotic disorders. It is crucial to the psychopathology of schizophrenia spectrum disorders. However, most previous studies were limited by recruiting only patients with clinically diagnosed psychotic disorders, behavioural rating of anhedonia, and the adoption of a unitary concept of anhedonia. Currently, no study in the literature has examined the neural basis of anhedonia in individuals with SPD traits, and little is known about the relationship between motivation and anhedonia.
7 Conclusions and Future Directions
Anhedonia is a symptom manifestation not only observed in patients with schizophrenia but also can be observed in individuals at-risk of psychosis as well as individuals with SPD traits. Studying anhedonia in individuals with SPD traits may provide better understanding of the problem because these individuals are not influenced by the course of illness and medication effects. However, this kind of study is surprisingly rare. One the one hand, the limited literature suggests that individuals with SPD traits exhibit a similar pattern of self-reported anticipatory and consummatory pleasure to patients with schizophrenia. On the other hand, it is surprising that the study of anhedonia is no simpler than patients with schizophrenia. Although most of the self-reported findings suggest that these individuals demonstrate impairment in anticipatory and consummatory pleasure as compared to healthy controls, some suggest it is the reverse. The picture is even more complicated when findings from laboratory-based studies were taken into consideration. A large proportion of empirical findings suggest that individuals with SPD traits do not show impairment in pleasure. Taken as a whole, it seems that there is another emotion paradox, namely the state anhedonia paradox, in this at-risk group [83]. That is, by definition, it is paradoxical in the sense that schizophrenia is much more severe in virtually every illness-related aspect as compared with individuals with SPD traits. Cohen et al. [83] argue that this situation does not always apply to the whole spectrum of the disorder. However, the underlying mechanism is largely unknown. Therefore future study should focus more on this state anhedonia paradox.
It is noteworthy that Strauss and Gold [58] postulate that observed anhedonia may not be merely due to diminished experiential pleasure but also the belief system endorsed by patients with schizophrenia. According to these authors, there are three components interacting with one another in influencing the corresponding anhedonia observed in these clinical patients. These components include (1) low pleasure beliefs and a lack of prospective or retrospective overestimation of positive emotion; (2) reduced pleasure-seeking behaviour, and (3) elevated negative symptoms. However, this speculation is totally based on empirical findings from patients with schizophrenia. Given the state-anhedonia-paradox mentioned above, it is not fully known whether this speculation is applicable to individuals with SPD traits. Nevertheless, our unpublished findings on time perspective scale [84] revealed that individuals with SPD traits reported significantly lower score in past positive but higher scores in past negative as well as present fatalistic perspectives than healthy controls. Given such a negative past experience and uncertain current situation, individuals with SPD traits were found to be scoring significantly higher on present hedonistic perspective. These preliminary findings suggest that individuals with SPD traits may possess a set of cognitive style or belief system that may determine their observed hedonic behaviour. However, further systematic research is needed to verify this interesting paradox observed across the spectrum of schizophrenia. It is also necessary to examine negative and positive SPD traits as separate entities to avoid confusion and misunderstanding in their emotional manifestations.
The aforementioned studies of the two-facet experiential pleasure construct were all cross-sectional in design. No longitudinal study has been undertaken to specifically track the changes of anticipatory and consummatory experiential pleasure over time and their predictive validity in individuals with SPD traits. However, empirical findings using the Chapman Scales of Physical and Social Anhedonia [33] indicate that individuals characterized by social anhedonia were associated with elevated SPD traits and psychotic-like experiences [35, 85, 86]. It will be interesting to examine whether the anticipatory and consummatory components would change similarly or differentially over time in these individuals. In particular, it will be important to identify whether there is any predictive validity of the changes of these two facets of experiential pleasure from prodrome to full-blown psychosis.
The advance of neuroimaging technologies may provide better ways to investigate the underlying neural mechanism of anhedonia in individuals with SPD traits. Neuroimaging allows us to examine the neural substrates and their connectivity with specific areas. A related potential implication of neuroimaging technologies is to pave the way for the possibility of non-invasive way treatment for anhedonia, which is currently considered an enduring feature of schizophrenia. For example, meta-analyses of the effects of repetitive transcranial magnetic stimulation have reported medium to large effect size in improving negative symptoms of schizophrenia [87, 88]. The application of neuroimaging has been extended recently from being used as an evaluation tool to an intervention tool such as real-time imaging neurofeedback [89, 90]. There have been initial reports of success in helping patients to regulate negative emotions such as pain perception [91]. Given its promising effect of manipulating a specific brain region, it is possible that real-time imaging neurofeedback may also allow us to examine how mental strategy can regulate the hotspots of hedonic capacity such as the orbitofrontal cortex, the rostral anterior cingulate cortex and the insula.
On the other hand, Favrod et al. [92] adopted an innovative cognitive-sensory intervention to improve the anticipatory experiential pleasure in five patients with anhedonia as measured by the TEPS. These individuals were trained to enter a state of relaxation to anticipate pleasure from potential enjoyable activities and to experience the sensation of the pleasure in their bodies. The intervention has been effective in improving the anticipatory pleasure subscore of the TEPS, but did not have an effect on the consummatory pleasure subscore. Despite the preliminary nature of the study, these findings suggest that cognitive-sensory interventions may be specific to anticipatory experiential pleasure through multimodalities simulation. This kind of approach together with real-time imaging neurofeedback may have advantages over conventional medical interventions especially for individuals with SPD traits who are not clinically diagnosed patients.
Taken together, the existing literature suggests that anhedonia is not limited to patients with established schizophrenia but also extends to individuals prone to psychosis such as those with SPD traits. However, the study of anhedonia in individuals with SPD traits remains preliminary. There are a number of unresolved issues in this area and its relationship with schizophrenia spectrum disorders remains unclear. Nevertheless, a potentially fruitful avenue is the use of the two-facet construct (i.e., anticipatory and consummatory) of pleasure experience and a combination of hedonic capacity measures to provide a comprehensive approach to anhedonia evaluation in individuals with SPD traits. These will facilitate a clearer understanding on whether anhedonia may serve as a vulnerability maker for schizophrenia and contribute to the development of potential intervention for this deficit.
Abbreviations
- DSM-IV:
-
Diagnostic and Statistical Manual of Mental Disorders Fourth Edition
- fMRI:
-
Functional magnetic resonance imaging
- SPD:
-
Schizotypal Personality Disorder
- TEPS:
-
The Temporal Experience of Pleasure Scale
- VBM:
-
Voxel Based Morphometry
References
Herbener ES, Harrow M, Hill SK. Change in the relationship between anhedonia and functional deficits over a 20-year period in individuals with schizophrenia. Schizophr Res. 2005;75:97–105.
Kirkpatrick B, Fenton WS, Carpenter WTJ, Marder SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull. 2006;32:214–9.
Gard DE, Kring AM, Gard MG, Horan WP, Green MF. Anhedonia in schizophrenia: distinctions between anticipatory and consummatory pleasure. Schizophr Res. 2007;93:253–60.
Foussias G, Remington G. Negative symptoms in schizophrenia: avolition and Occam’s razor. Schizophr Bull. 2010;36:359–69.
Silver H, Chertkow Y, Weinreb O, Danovich L, Youdim M. Multifunctional pharmacotherapy: what can we learn from study of selective serotonin reuptake inhibitor augmentation of antipsychotics in negative-symptom schizophrenia? Neurotherapeutics. 2009;6(1):86–93.
Lewis SW, Barnes TRE, Davids L, Murray RM, Dunn G, Hayhurst KP, Markwick A, Lloyd H, Jones PB. Randomized controlled trial of effect of prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull. 2006;32(4):715–23.
Horan PH, Kring AM, Blanchard JJ. Anhedonia in schizophrenia: a review of assessment strategies. Schizophr Bull. 2006;32:259–73.
Cohen A, Minor K. Emotional experience in patients with schizophrenia revisited: meta-analysis of laboratory studies. Schizophr Bull. 2010;36:143–50.
Kring AM, Moran EK. Emotional response deficits in schizophrenia: insights from affective science. Schizophr Bull. 2008;34(5):819–34.
Cohen AS, Najolia GM, Brown LA, Minor KS. The state-trait disjunction of anhedonia in schizophrenia: potential affective, cognitive and social-based mechanisms. Clin Psychol Rev. 2011;31(3):440–8.
Yan C, Cao Y, Zhang Y, Song LL, Cheung EF, Chan RC. Trait and state positive emotional experience in schizophrenia: a meta-analysis. PLoS One. 2012;7:e40672.
Meehl PE. Schizotaxia, schizotypy, schizophrenia. Am Psychol. 1962;17:827–38.
Lenzenweger MF. Psychometric high-risk paradigm, perceptual aberrations, and schizotypy: an update. Schizophr Bull. 1994;20(1):121–35.
Chapman LJ, Chapman JP, Kwapil TR, Eckblad M, Zinser MC. Putatively psychosis-prone subjects 10-years later. J Abnorm Psychol. 1994;103(2):171–83.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000.
First MB, Spitzer RL, Gibbon M, Williams JBW, Benjamin L. Structured clinical interview for DSM-IV axis II personality disorders (SCID-II, version 2.0). New York: NY State Psychiatric Institute; 1994.
Woods SW, Addington J, Cadenhead KS, Cannon TD, Cornblatt BA, Heinssen R, Perkins DO, Seidman LJ, Tsuang MT, Walker EF, McGlashan TH. Validity of the prodromal risk syndrome for first psychosis: findings from the North American Prodrome Longitudinal Study. Schizophr Bull. 2009;35(5):894–908.
Yung AR, Phillips LJ, Yuen HP, Francey SM, McFarlane CA, Hallgren M, et al. Psychosis prediction: 12-month follow up of a high-risk (“prodromal”) group. Schizophr Res. 2003;60(1):21–32.
Tienari P, Wynne LC, Laksy K, Moring J, Nieminen P, Sorri A, et al. Genetic boundaries of the schizophrenia spectrum: evidence from the Finnish Adoptive Family Study of Schizophrenia. Am J Psychiatry. 2003;160:1587–94.
Johns LC, van Os J. The continuity of psychotic experiences in the general population. Clin Psychol Rev. 2001;21(8):1125–41.
van Os J, Linscott RJ, Myin-Germeys I, Delespaul P, Krabbendam L. A systematic review and meta-analysis of the psychosis continuum: evidence for a psychosis proneness-persistence-impairment model of psychotic disorder. Psychol Med. 2009;39(2):179–95.
Chan RCK, Li X, Lai M, Li H, Wang Y, Cui J, Deng Y, Raine A. Exploratory study on the base-rate paranoid ideation in a non-clinical Chinese sample. Psychiatry Res. 2011;185(1–2):254–60.
Meehl PE. Toward an integrated theory of schizotaxia, schizotypy, and schizophrenia. J Personal Disord. 1990;4:1–99.
Pelizza L, Ferrari A. Anhedonia in schizophrenia and major depression: state or trait? Ann Gen Psychiatry. 2009;8:22.
Romney DM, Candido CL. Anhedonia in depression and schizophrenia: a reexamination. J Nerv Ment Dis. 2001;189:735–40.
Katsanis J, Iacono WG, Beiser M. Anhedonia and perceptual aberration in first-episode psychotic patients and their relatives. J Abnorm Psychol. 1990;99:202–6.
Clementz BA, Grove WM, Katsanis J, Iacono WG. Psychometric detection of schizotypy: perceptual aberration and physical anhedonia in relatives of schizophrenics. J Abnorm Psychol. 1991;100:607–12.
Grove WM, Lebow BS, Clementz BA, Cerri A, Medus C, Iacono WG. Familial prevalence and coaggregation of schizotypy indicators: a multitrait family study. J Abnorm Psychol. 1991;100:115–21.
Blanchard JJ, Collins LM, Aghevil M, Leung WW, Cohen AS. Social anhedonia and schizotypy in a community sample: the Maryland longitudinal study of schizotypy. Schizophr Bull. 1998;37(3):587–602.
Lubin B, Van Whitlock R, Zuckerman M. Affect traits in differential diagnosis of anxiety, depressive, and schizophrenic disorders using the multiple affect adjective check list-revised. Assessment. 1998;5:309–19.
Loas G, Boyer P, Legrand A. Anhedonia in the deficit syndrome of schizophrenia. Psychopathology. 1999;32:207–19.
Rado S. Psychoanalysis of behavior; collected papers. New York: Grune and Stratton; 1956.
Chapman LJ, Chapman JP, Raulin ML. Scales for physical and social anhedonia. J Abnorm Psychol. 1976;85(4):399–407.
Kring AM. Emotion in schizophrenia: old mystery, new understanding? Curr Dir Psychol Sci. 1999;8(5):160–3.
Blanchard JJ, Mueser KT, Bellack AS. Anhedonia, positive and negative affect, and social functioning in schizophrenia. Schizophr Bull. 1998;24:413–24.
Knutson B, Greer SM. Anticipatory affect: neural correlates and consequences for choice. Philos Trans R Soc Lond B Biol Sci. 2008;363(1511):3771–86.
Kringelbach ML, Bridge KC. Towards a functional neuroanatomy of pleasure and happiness. Trends Cogn Sci. 2009;13(11):479–87.
Gard DE, Gard-Germans M, Kring AM, Oliver JP. Anticipatory and consummatory components of the experience of pleasure: a scale development study. J Res Personal. 2006;40:1086–102.
Treadway MT, Zald DH. Reconsidering anhedonia in depression: lessons from translational neuroscience. Neurosci Biobehav Rev. 2011;35:537–55.
Klein D. Depression and anhedonia. In: Clark DC, Fawcett J, editors. Anhedonia and affect deficit states. New York: PMA Publishing; 1984. p. 1–14.
Berridge KC, Robinson TE. What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Rev. 1998;28:309–69.
Bridge KC, Robinson TE. Parsing reward. Trends Neurosci. 2003;26:507–13.
Der-Avakian A, Markou A. The neurobiology of anhedonia and other reward-related deficits. Trends Neurosci. 2012;35(1):68–77.
Kringelbach ML. The hedonic brain: a functional neuroanatomy of human pleasure. In: Kringelbach ML, Bridge KC, editors. Pleasures of the brain. Oxford: Oxford University Press; 2010. p. 202–21.
Kringelbach ML. The human orbitofrontal cortex: linking reward to hedonic experience. Nat Rev Neurosci. 2005;6:691–702.
Gold JM, Waltz JA, Prentice KJ, Morris SE, Heerey EA. Reward processing in schizophrenia: a deficit in the representation of value. Schizophr Bull. 2008;34(5):835–47.
Chan RCK, Wang Y, Huang J, Shi Y, Wang Y, Hong X, Ma Z, Li Z, Lai MK, Kring AM. Anticipatory and consummatory components of the experience of pleasure in schizophrenia: cross-cultural validation and extension. Psychiatry Res. 2010;175:181–3.
Chan RCK, Shi YF, Lai MK, Wang YN, Wang Y, Kring AM. The Temporal Experience of Pleasure Scale (TEPS): exploration and confirmation of factor structure in a healthy Chinese sample. PLoS One. 2012;7(4):e35352.
Gooding DC, Pflum MJ. The nature of diminished pleasure in individuals at risk for or affected by schizophrenia. Psychiatry Res. 2012;198:172–3.
Martin EA, Becker TM, Cicero DC, Cocherty AR, Kerns JG. Differential associations between schizotypy facets and emotion traits. Psychiatry Res. 2011;187:94–9.
Eckblad ML, Chapman LJ, Chapman JP, Mishlove M. The revised social anhedonia scale. 1982.
Chapman LJ, Chapman JP, Raulin ML. Body-image aberration in schizophrenia. J Abnorm Psychol. 1978;87(4):399–407.
Eckblad M, Chapman LJ. Magical ideation as an indicator of schizotypy. J Consult Clin Psychol. 1983;51(2):215–25.
Shi YF, Wang Y, Cao XY, Wang Y, Wang YN, Zong JG, Xu T, Tse VWS, Hsi XL, Stone WS, Lui SSY, Cheung EFC, Chan RCK. Experience of pleasure and emotional expression in individuals with schizotypal personality features. PLoS One. 2012;7(5):e34147.
Raine A. The Schizotypal Personality Questionnaire (SPQ): a measure of schizotypal personality based on DSM-III-R criteria. Schizophr Bull. 1991;17:555–64.
Chen WJ, Hsiao CK, Lin CCH. Schizotypy in community samples: the three-factor structure and correlation with sustained attention. J Abnorm Psychol. 1997;106:649–54.
Wang Y, Neumann D, Shum DHK, Chan RCK. A cross-validation study of clustering of schizotypy using a non-clinical Chinese sample. Psychiatry Res. 2012;1(30):55–8.
Strauss GP, Gold JM. A new perspective on anhedonia in schizophrenia. Am J Psychiatry. 2012;169(4):364–73.
Cohen AS, Iglesias B, Minor KS. The neurocognitive underpinnings of diminished expressivity in schizotypy: what the voice reveals. Schizophr Res. 2009;109:38–45.
Kerns JG, Docherty AR, Martin EA. Social and physical anhedonia and valence and arousal aspects of emotional experience. J Abnorm Psychol. 2008;117(4):735–46.
Gooding DC, Davidso RJ, Putnam KM, Tallent KA. Normative emotion-modulated startle response in individuals at risk for schizophrenia-spectrum disorders. Schizophr Res. 2002;57:109–20.
Yan C, Liu WH, Cao Y, Chan RCK. Self-report pleasure experience and motivation in individuals with schizotypal personality disorders proneness. East Asian Arch Psychiatry. 2011;21:115–22.
Joseph S, Manafi E, Lakovaki AM, Cooper R. Personality, smoking motivation, and self-efficacy to quit. Personal Individ Diff. 2003;34:749–58.
Bogdan R, Pizzagalli DS. Acute stress reduces reward responsiveness: implications for depression. Biol Psychiatry. 2006;60:1147–54.
Liu WH, Chan RCK, Wang LZ, Huang J, Cheung EFC, Gong QY, Gollan JK. Deficits in sustaining reward responses in subsyndromal and syndromal major depression. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35:1045–52.
Lui SSY, Shi YF, Li Z, Liu ACY, Chan CKY, Leung MMW, Chui WWH, Tsang CCM, Wang Y, Yan C, Heerey EA, Cheung EFC, Chan RCK. Affective experience and motivated behaviour in schizophrenia spectrum disorders: Convergent evidence from clinical and non-clinical samples. Submitted.
Heerey EA, Gold JM. Patients with schizophrenia demonstrate dissociation between affective experience and motivated behavior. J Abnorm Psychol. 2007;116:268–78.
Strauss GP, Gold JM. Response to Gooding and Plfum, “The nature of diminished pleasure in individuals at risk for or affected by schizophrenia” Anticipatory and consummatory pleasure deficits across the schizophrenia spectrum. Psychiatry Res. 2012;198:174–5.
Watson D, Tellegen A. Toward a consensual structure of mood. Psychol Bull. 1985;98:219–35.
Dickey CC, McCarley RW, Shenton ME. The brain in schizotypal personality disorder: a review of structural MRI and CT findings. Harv Rev Psychiatry. 2002;10(1):1–15.
Modinos G, Mechelli A, Ormel J, Groenewold NA, Aleman A, McGuire PK. Schizotypy and brain structure: a voxel-based morphometry study. Psychol Med. 2010;40:1423–31.
Asami T, Whitford TJ, Bouix S, Dickey CC, Niznikiewicz M, Shenton ME, Voglmaier MM, McCarley RW. Globally and locally reduced MRI gray matter volumes in neuroleptic-naïve men with schizotypal personality disorder: association with negative symptoms. JAMA Psychiatry. 2013;70(4):361–72.
Harvey PO, Pruessner J, Czechowska Y, Lepage M. Individual differences in trait anhedonia: a structural and functional magnetic resonance imaging study in non-clinical subjects. Mol Psychiatry. 2007;12:767–75.
Germine LT, Garrido L, Bruce L, Hooker C. Social anhedonia is associated with neural abnormalities during face emotion processing. Neuroimage. 2011;58:935–45.
Abbott GR, Green MJ. Facial affect recognition and schizotypal personality characteristics. Early Interv Psychiatry. 2013;7:58–63.
Huang J, Wang Y, Jin Z, Di X, Yang T, Gur RC, Gur RE, Shum DHK, Cheung EFC, Chan RCK. Happy facial expression processing with different social interaction cues: an fMRI study of individuals with schizotypal personality traits. Prog Neuropsychopharmacol Biol Psychiatry. 2013;44:108–17.
Friston KJ, Frith CD, Turner R, Frackowiak RS. Characterizing evoked hemodynamics with fMRI. Neuroimage. 1995;2:157–65.
Haxby JV. Multivariate pattern analysis of fMRI: the early beginnings. Neuroimage. 2012;62:852–5.
Kamitani Y, Tong F. Decoding the visual and subjective contents of the human brain. Nat Neurosci. 2005;8:679–85.
Kriegeskorte N, Goebel R, Bandettini P. Information-based functional brain mapping. Proc Natl Acad Sci U S A. 2006;103:3863–8.
Stefanis NC, Hanssen M, Smirnis NK, Avramopoulos DA, Evdokimidis IK, Stefanis CN, Verdoux H, Van Os J. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med. 2002;32:347–58.
Modinos G, Pettersson-Yeo W, Allen P, McGuire PK, Aleman A, Mechelli A. Multivariate pattern classification reveals differential brain activation during emotional processing in individuals with psychosis proneness. Neuroimage. 2012;59(3):3033–41.
Cohen A, Callaway DA, Larsen JT, Strauss GP. On “risk” and reward: investigating anhedonia in psychometrically defined schizotypy and schizophrenia. J Abnorm Psychol. 2012;121(2):407–15.
Zimbardo PG, Boyd JN. Putting time in perspective: a valid, reliable individual-differences metric. J Pers Soc Psychol. 1999;77(6):1271–88.
Kwapil TR. Social anhedonia as a predictor of the development of schizophrenia-spectrum disorders. J Abnorm Psychol. 1998;107:558–65.
Gooding DC, Tallent KA, Matts CW. Clinical status of at risk individuals 5 years later: further validation of the psychometric high-risk strategy. J Abnorm Psychol. 2005;114:170–5.
Dlabac-de Lange JJ, Knegtering R, Aleman A. Repetitive transcranial magnetic stimulation for negative symptoms of schizophrenia: review and meta-analysis. J Clin Psychiatry. 2010;71(4):411–8.
Freitas C, Gregni F, Pascual-Leone A. Meta-analysis of the effects of repetitive transcranial magnetic stimulation (rTMS) on negative and positive symptoms in schizophrenia. Schizophr Res. 2009;108:11–24.
deCharms RC. Applications of real-time fMRI. Nat Rev Neurosci. 2008;9(9):720–9.
Sulzer J, Haller S, Scharnowski F, Weiskopf N, Birbaumer N, Blefari ML, Bruehl AB, Cohen LG, deCharms RC, Gassert R, Goebel R, Herwig U, LaConte S, Linden D, Luft A, Seifritz E, Sitaram R. Real-tem fMRI neurofeedback: progress and challenges. NeuroImage. 2013. doi:10.1016/j.neuroimage.2013.03.033.
deCharms RC, Maeda F, Glover GH, Ludlow D, Pauly JM, Soneji D, Gabrieli JDE, Mackey SC. Control over brain activation and pain learned by using real-time functional MRI. Proc Natl Acad Sci U S A. 2005;102(51):18626.
Favrod J, Giuliani F, Ernst F, Bonsack C. Anticipatory pleasure skills training: a new intervention to reduce anhedonia in schizophrenia. Perspect Psychiatr Care. 2010;46:171–81.
Acknowledgments
This research received support from a grant from the National Science Fund China Young Investigator Award (81088001); the National Key Technologies R&D Program (2012BAI36B01); and the “Strategic Priority Research Program (B)” of the Chinese Academy of Sciences (XDB02030002).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Chan, R.C.K., Yan, C., Wang, Y., Yin, Qf., Lui, S.S.Y., Cheung, E.F.C. (2014). Anticipatory and Consummatory Anhedonia in Individuals with Schizotypal Traits. In: Ritsner, M. (eds) Anhedonia: A Comprehensive Handbook Volume II. Springer, Dordrecht. https://doi.org/10.1007/978-94-017-8610-2_10
Download citation
DOI: https://doi.org/10.1007/978-94-017-8610-2_10
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-017-8609-6
Online ISBN: 978-94-017-8610-2
eBook Packages: MedicineMedicine (R0)