
Abstract
The calcium, magnesium, nickel and zinc contents in seven Traditional Chinese Medicines (TCM) and four Ayurvedic Medicines (AM) purchased locally were determined using flame atomic absorption spectroscopy following five different digestion methods: four open wet hot plate with various mixtures of acids and/or H2O2, and microwave oven (MWO) with conc HNO3 and H2O2. Sodium and potassium levels were analysed using flame photometry after MWO digestion. Potassium had the highest mean level among the six metals analysed. MWO was found to be more effective for Mg, method M1 [conc HNO3 + H2O2 (30 %)] for Ca and Zn, and method M4 (aqua regia) for nickel. From replicate measurements, the inter-day precision of the flame photometric measurements for sodium and potassium was found to be 3.0–9.0 % and 1.3–9.0 % respectively. Comparison of results obtained from standard calibration curves and standard addition indicated that the percentage difference of sodium content in the TCM Niuhuangchiehdu Pien and the potassium content in AM, Diabecon was 3.9 % and 0.22 % respectively, indicating that the matrix did not have much influence on the metal content.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
- Traditional Chinese Medicine
- Sodium Level
- Zinc Level
- Digestion Method
- Flame Atomic Absorption Spectroscopy
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
24.1 Introduction
The World Health Organisation (WHO) defines traditional medicine as: “the sum total of the knowledge, skills, and practices based on the theories, beliefs, and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement or treatment of physical and mental illness” [1].
There exist several traditional systems of medicine around the world, each with different associated philosophies and cultural origins, of which the two most prevalent are the Traditional Chinese Medicines (TCM) and Ayurvedic Medicines (AM). During the last two decades, there has been increased global interest in traditional medicines, especially those based on herbal products and extracts. These medicines contain a wide range of inorganic elements, both toxic and essential. Toxic metals of concern are mainly As, Cd, Hg and Pb. Several studies have reported potentially harmful levels of these heavy metals in both TCM and AM [2–24], thus emphasizing the need for more stringent quality standards and regulations for these products [8, 9, 21, 25, 26]. However, some authors highlighted that detailed chemical speciation be conducted to assess the effective toxicity of the medicines as the toxicity of elements varies with their chemical forms [3, 7, 10, 27].
On the other hand, TCM and AM are also known to have many essential and nutritional elements such as Ca, Cu, K, Mg, Mn, Na, Ni and Zn, whose excess or deficiency may disturb the normal biochemical functions of the human body. Several studies have reported elemental contents in traditional medicines or medicinal plant extracts [3, 11, 12, 17, 28–35].
Considering the importance of trace elements in various human metabolic processes and also their curative properties, the analysis of six essential and trace elements, namely calcium, magnesium, nickel, potassium, sodium and zinc, in 7 TCM and 4 AM commercially available in the Mauritian market was carried out.
Calcium is an essential plant nutrient and is omnipresent in all living things (animals and plants), water, soils and sediments. It is essential for healthy bones, teeth and blood. Deficiency of calcium causes rickets, osteomalacia and scurvy [36]. Magnesium is the fourth most abundant mineral in the human body and is needed for more than 300 biochemical reactions. It helps in maintaining a healthy immune system, strong bones and regulating the levels of several vitamins and minerals. Magnesium deficiency can cause amongst others cramps, muscle tension, poor memory, irritability, depression, and can result in low levels of calcium and potassium in the blood [37]. Nickel, despite being toxic, is found in minute amounts in the human body and is believed to play a role in the stabilisation of the RNA molecule, in the normal bone functioning, in the breakdown of glucose and human breast milk production. Deficiency of nickel is normally rare but can lead to liver, skin and kidney diseases. However, at high levels of accumulation, nickel is capable of causing serious health problems such as paralysis of the spinal column, tumours, thyroid and heart diseases [38]. Zinc is an essential element for the body and is involved in numerous aspects of cellular metabolism. Zinc plays important roles in normal growth and development during pregnancy, childhood and adolescence, and nearly 100 specific enzymes depend on zinc for their catalytic activity. Severe zinc deficiency can result in the slowing of growth and development, delayed sexual maturation, chronic and severe diarrhea, immune system deficiencies, impaired wound healing, reduced appetite, impaired taste sensation and night blindness [39]. Both potassium and sodium are essential body minerals. The body depends on the electrolytic properties of potassium for conduction of nerve impulses, muscle contractions and regulation of balance of acids and bases in the blood. Potassium is also involved in various biochemical processes in the human body. Some common problems associated with low potassium levels include hypertension, congestive heart failure, cardiac arrhythmia, fatigue and osteoporosis [40]. On the other hand, the body uses sodium to regulate blood pressure and blood volume. Sodium is also essential for the transmission of nerve impulses, heart activity, and certain metabolic functions. Low sodium levels (hyponatremia) are uncommon but can occur whenever there is an increase in the amount of body water relative to sodium. On the contrary, hypernatremia (high sodium levels) is common, caused principally with high sodium content in food. Other causes include kidney diseases, low water intake, severe diarrhea and vomiting [41].
24.2 Methodology
24.2.1 Materials and Reagents
7 TCM (Jin Qian Chao, Leung Pui Kee, Po Chai Pills, Quiang Li Tien-Ma, Saplingtan, Watermelon Frost and Niuhuangchiehdu Pien) imported from China and 4 AM (Diabecon, Pilex, Septilin and Softovac) imported from India were purchased locally.
The standard stock 1,000 ppm solutions of potassium and sodium were bought from Sherwood Scientific Ltd, calcium and zinc from Fisher Scientific, magnesium and nickel from Fisons Scientific. Concentrated HNO3, HCl and H2SO4 were obtained from SD Fine Chemicals Ltd while H2O2 (30 %) from Fisons Scientific.
All glassware used (burettes, pipettes, volumetric flasks, beakers) were of grade A. Prior to use, all glassware were acid-washed.
24.2.2 Sample Preparation
The traditional medicines which were mostly in the form of pills were ground using a mortar and pestle in order to obtain fine and homogeneous solids.
24.2.3 Microwave Oven Digestion
The samples were digested using the microwave digester Milestone High Performance Microwave Unit mls 1,200 M. Prior to use, the Teflon flasks were acid washed. Approximately 1 g of each powdered sample was weighed in duplicate in dry labelled Teflon flasks to which were added 7 ml of concentrated nitric acid (72 %) followed by 5 ml of H2O2 (30 %). The samples were digested using the program shown in Table 24.1.
After cooling for about 30 min, the resulting digested samples were filtered through fluted filter paper into 25 mL volumetric flasks and the filtrates were made up to the mark with distilled deionised water. The resulting clear solutions were then transferred to clean acid-washed labelled plastic bottles.
24.2.4 Wet Open Digestions
Wet open digestion of the samples was performed using four different methods as given in Table 24.2.
Approximately 1 g of the ground medicine was weighed in duplicate into separate 50 mL conical flasks. The appropriate reagents as detailed in Table 24.2 were pipetted into each of the flasks. The solutions were heated to boiling on a hot plate in a fume hood for 4 h before filtration into 25 mL volumetric flasks and making up to the mark with distilled deionised water. The contents were finally transferred to clean well-labelled plastic bottles.
Reagent blanks were prepared for both microwave and wet open digestions under similar conditions as those used for the medicinal samples.
24.2.5 Determination of Metal Contents
The standard calibration solutions were prepared daily from the stock solutions by proper dilution with distilled deionised water. The levels of potassium and sodium in the medicines were determined using a CIBA Corning Model 410 flame photometer whereas calcium, magnesium, nickel and zinc contents were analysed by a GBC Avanta flame atomic absorption spectrometer using air/acetylene. Table 24.3 lists the concentrations of the prepared standard solutions and wavelength used for the metals.
24.2.6 Standard Addition
24.2.6.1 Determination of Potassium Content in Diabecon
5 ml of the microwave oven digested medicinal sample Diabecon was diluted 20 times. 5 ml of this diluted sample was then transferred to each of five 25 mL volumetric flasks. To the five volumetric flasks, 0, 0.5, 1, 1.5 and 2 ml of 100 ppm potassium standard solution was respectively added. The resultant solutions were then made up to the mark with distilled deionised water and analysed by flame photometry. The concentration of the added standard for each flask was determined and a plot of emission against concentration of added standard was drawn. The concentration of potassium in the diluted sample corresponds to the x-intercept obtained by extrapolation. The concentration of potassium in the undiluted sample is then calculated by taking into consideration the dilution performed.
24.2.6.2 Determination of Sodium Content in Niuhuangchiehdu Pien
The experimental procedure is similar to that applied in section “Determination of Potassium Content in Diabecon ” except that 5 ml of the undiluted microwave digested Niuhuangchiehdu Pien sample was pipetted in the five volumetric flasks.
24.3 Results and Discussion
24.3.1 Metal Levels in TCM and AM
24.3.1.1 Calcium
Table 24.4 gives the calcium levels obtained in the 7 TCM and 4 AM following the five methods of digestion.
All the 11 medicinal samples analysed exhibited detectable calcium levels. The highest calcium level is observed in Niuhuangchiehdu Pien irrespective of the applied method of digestion. The elevated concentration of calcium found in Niuhuangchiehdu Pien can be accounted by the presence of the gypsum selenite (26.64 %) in its formulation. Excluding the TCM Niuhuangchiehdu Pien, the calcium content in the four AM is higher than in the remaining six TCM. Diabecon, Pilex and Softovac have the highest amount of calcium amongst the AM. However, the calcium contents were considerably lower than those analysed by Giacomino et al. [12] in five products of the Parpati family where Ca was present in all the medicines with a range of 738–8,439 μg/g. Two main ingredients namely Shilajit and Pterocarpus marsupium present in Diabecon contain high calcium levels. Shilajit is an exudate that is pressed out from rock layers in sacred mountains in Nepal and other high mountains and is rich in minerals and metals such as calcium, zinc, sodium and magnesium [42]. On the other hand, Pterocarpus marsupium also known as the Indian Kino tree contains 10–20 % of calcium sennoside which is a big molecule with molecular formula C42H36CaO20.
Comparison between the various digestion methods showed that M1 digestion resulted in the highest calcium levels for 10 out of the 11 medicinal samples analysed in this study, except for the TCM Niuhuangchiehdu Pien in which the highest calcium content was detected following digestion method M2. MWO digestion gave the next highest calcium levels for the medicines analysed. Least calcium level was observed in seven medicines (Diabecon, Pilex, Softovac, Jin Qian Chao, Leung Pui Kee, Po Chai Pills and Saplingtan) following digestion method M3, in three medicines (Septilin, Quiang Li Tien-Mo and Niuhuangchiehdu Pien) from digestion method M4 and in one medicine (Watermelon Frost) from digestion method M2.
The statistical two-tail student’s t-test method was applied to compare the different digestion methods to investigate whether there are any significant differences between the results obtained from all the ten possible pairs (Table 24.5). By analysing the calculated t-values (t calc ) with the t crit value (2.23), it is observed that for six pairs of digestion methods, namely M1/M2, M1/M3, M1/M4, M1/MWO, M3/MWO and M4/MWO, the results are significantly different from each other at 95 % confidence level. The results obtained following the digestion method M1 are thus significantly different from those obtained from the other four digestion methods. Similarly, calcium levels obtained following MWO digestion are significantly different from all the other digestion methods except M2. On the other hand, it can be concluded that the values obtained from digestion methods M2, M3 and M4 are comparable and hence are not significantly different.
24.3.1.2 Magnesium
The magnesium levels obtained in the 7 TCM and 4 AM following the five methods of digestion are shown in Table 24.6.
All the traditional medicines analysed were found to contain magnesium. The highest magnesium level was found in the AM Pilex which is due to the presence of the ingredients Guggul and Shilajit. Guggul is composed of a mixture of organic compounds, inorganic ions and minerals which consist mostly of calcium, magnesium and iron [43]. On the other hand, Shilajit is a rich source of naturally occurring minerals like magnesium [42]. The lowest magnesium level in the AM was found in Softovac. For the TCM, Jin Qian Chao was found to have the highest magnesium content. Magnesium is well-known for its calcium channel blocking effect and can reduce the formation of calcium oxalate which is the main cause for stones in body. Herba Lysmachiae, the only ingredient of Jin Qian Chao, is very effective in dissolving kidney, liver and gall stones [44] and this can explain the high level of magnesium obtained in this TCM. The range of magnesium levels obtained in this study for AM corresponds to only a certain extent to the range observed by Giacomino et al. [12] (201–4,236 μg/g). For the TCM, the range observed was within that obtained by Wang et al. [11] (ND-2,031 μg/g). The lowest magnesium levels were found in the TCM Saplingtan and Watermelon Frost.
Highest levels of magnesium were observed after MWO or M1 digestion for all the 11 medicines. Digestion method M2 gave the least amount for all the medicines analysed. The following order of extractability of magnesium was observed: M2 < M3 ~ M4 < M1 ~ MWO. From Table 24.7, it was observed that the t calc was greater than the t crit (2.23) for all pairs of digestion methods except M3/M4.
24.3.1.3 Nickel
Table 24.8 gives the nickel levels obtained in the 7 TCM and 4 AM following the five methods of digestion.
Nickel was detected in all the 11 medicines. Highest level was observed in the TCM Leung Pui Kee. The latter is based mainly on constituents of plant origin and the only mineral present is talc (1 %). A potential source of nickel apart from talc is soils and sediments. Plants grown in soils rich in nickel absorb the metal which is then incorporated into the medicine. The plant Aster tataricus used in the preparation of Leung Pui Kee is native from the northern part of China and is grown in meadows and wetlands which are rich in minerals and metals due to the anthropogenic activities in the vicinity. The presence of nickel in the other medicines can also be explained from soil contribution.
The nickel levels in the 11 medicines were all found in a small range (3.2–13.1 μg/g) and are comparable to those observed by Wieckowski and Mezyk [45] in TCM (1.6–11.3 μg/g), and by Akhtar et al. [46] (0.94–4.35 μg/g) in AM.
Comparison between the five different methods of digestion for nickel revealed that methods M4 and MWO were the best acid mixtures for the medicinal samples analysed in this study. Highest deviations between the digestion methods MWO and M4 were observed for Leung Pui Kee (−46.4 %), Saplingtan (−22.8 %) and Po Chai Pills (+20.0 %). The two-tail student’s t-test was applied to compare the results obtained from all the different pairs of digestion methods and the results are shown in Table 24.9.
It can be observed that for six out of ten combinations analysed, the t calc is greater than the t crit (2.23). Results following digestion methods M4 and MWO are thus significantly different at the 95 % confidence level from those obtained after digestion methods M1, M2 and M3. On the other hand, no significant difference was observed between the three methods of digestion M1, M2 and M3 and between M4 and MWO indicating that the values obtained were comparable.
24.3.1.4 Zinc
The zinc levels obtained in the 7 TCM and 4 AM following the five methods of digestion are given in Table 24.10.
Zinc was detected in all the 11 traditional medicines analysed. The highest zinc level observed was in Po Chai Pills for the TCM and in Diabecon for the AM. The zinc level in the TCM Po Chai Pills can be explained by the presence of the ingredient Cortex Magnolia Officinalis which is rich in a number of trace elements including zinc [47]. On the other hand, the zinc content in Diabecon is mainly due to two of its constituents, namely Yashad Bhasma and Shilajit. Yashad Bhasma also known as zinc calx, is processed zinc which is obtained from the calcination of Rasaka satva which is a metallic extract of zinc carbonate/zinc oxide [48]. On the other hand, Shilajit is a rich source of essential and trace minerals including zinc [42]. The range for zinc in the TCM was found to be within that obtained by Shao et al. [49] (3.2–86.2 μg/g). Similarly, the range of zinc found in the AM is within the range (4–109 μg/g) observed by Al-Omari [17].
The wet digestion M1 using HNO3 and H2O2 was found to result in the highest zinc levels followed by M3. Digestion method M4 gave the least zinc level for seven out of the eleven medicines analysed. Using t-test, it was found that the t calc was greater than the t crit (2.23) at 95 % confidence for the following digestion pairs: M1/M2, M1/M3, M1/M4, M1/MWO, M3/M4 and M3/MWO (Table 24.11), inferring that there is a significant difference between the results obtained after M1 digestion method and the other digestion methods (M2, M3, M4 and MWO).
24.3.1.5 Potassium and Sodium
Table 24.12 gives the potassium and sodium levels obtained in the 7 TCM and 4 AM by flame photometry following MWO digestion.
The ranges observed for potassium were 6,200–21,143 μg/g and 31.7–26,416 μg/g for the AM and TCM respectively. The highest potassium content was found in the TCM Jin Qian Chao (26,416 μg/g) followed by the AM Diabecon (21,143 μg/g). As Jin Qian Chao is composed solely of Herba Lysimachiae, the high potassium content of the TCM may be due to the presence of inorganic potassium chloride absorbed from the soil in the herb [44]. On the other hand, the high amount of potassium in Diabecon results from the ingredients Shilajit and Abhrak Bhasma. Shilajit is obtained from the Himalayan Mountains and is composed of a large number of essential metals in the ionic form including potassium [42]. Bhasmas are prepared by calcination of metals and Abhrak Bhasma contains trace amounts of potassium [48]. The highest level in the TCM observed by Wang et al. [11] was 11,054 μg/g which is lower than that observed in the present study (26,416 μg/g). The lowest potassium contents were observed in two TCM, namely Saplingtan (31.7 μg/g) and Watermelon Frost (70.5 μg/g). On the other hand, the range of potassium levels observed in the AM was within that obtained by Giacomino et al. [12] (44.5–21,440 μg/g).
The sodium levels observed ranged from 1,099 μg/g in Po Chai Pills and Niuhuangchiehdu Pien to 6,191 μg/g in Watermelon Frost. In Saplingtan, the sodium level was below the detection limit of the apparatus. The highest sodium level was observed in Watermelon Frost (6,191 μg/g) which is used for the treatment of throat diseases, general wounds with bleeding, toothache, burns and scald, and can be accounted by the presence of the ingredient Mirabilite (also known as Glauber’s salt, Na2SO4·10H2O) in its formulation. Due to its anti-bacterial property, sodium is also present in high amount in Septilin (3,500 μg/g) which is mainly used as an anti-infective therapy for the treatment of sinusitis. The high sodium level observed (5,173 μg/g) in Diabecon can be accounted by the presence of Shilajit, a major ingredient rich in various metallic salts including sodium [42].
To investigate the matrix effect in the medicines, the potassium level in the AM, Diabecon and the sodium level in the TCM Niuhuangchiehdu Pien, were determined by the method of standard addition and the results obtained compared with those obtained from standard calibration curves. The plots obtained for potassium level in Diabecon and sodium level in Niuhuangchiehdu Pien are depicted in Figs. 24.1 and 24.2 respectively.

Plot of corrected emission against concentration of added potassium for Diabecon

Plot of corrected emission against concentration of added sodium for TCM Niuhuangchiehdu Pien
The potassium and sodium levels obtained from both standard calibration curve and standard addition are shown in Table 24.13.
It is observed that the sodium and potassium concentration obtained from standard addition are close to those obtained from standard calibration curves with a CV of 0.22–3.9 %. It can thus be deduced that the matrix did not have much influence on the sodium or potassium content.
24.3.2 Precision of Flame Photometric Method
In this study, intra-day precision, also known as repeatability, was determined for the potassium content in the TCM Po Chai Pills and inter-day precision for the potassium and sodium content for all the medicines. The precision of an analytical procedure is usually expressed as the % relative standard deviation (%RSD) of a series of measurements. Precision is concentration dependent and the acceptable precision (%RSD) for concentration (≥ 100 ppm) is 15 % [50].
24.3.2.1 Intra-Day Precision
Intra-day precision expresses the precision under the same operating conditions over a short interval of time within the same day and was determined for the potassium content by flame photometry in the TCM Po Chai Pills by measuring the same sample ten times at 15 min’ time interval. The results are shown in Table 24.14.
The repeatability of the analytical method for the TCM Po Chai Pills was excellent as the %RSD was found to be 0.91 %.
24.3.2.2 Inter-Day Precision
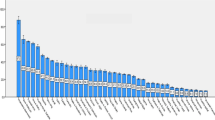
The inter-day precision of the photometric analyses and the method validity were assessed by analysing the microwave-digested samples of the 11 medicines on five different days: day 1, day 2, day 3, day 8 and day 15 for potassium and sodium. The results are shown in Table 24.15 and Fig. 24.3 respectively.

Variation of the sodium content of the TCM and AM on an inter-day basis
It was observed that the %RSD for all the medicines (1.3–9.0 %) for both the potassium and sodium analysis were well below the acceptable precision and thus it can be inferred that the inter-day precision for the analytical method was good.
24.4 Conclusions
In this study, 7 TCM and 4 AM purchased in Mauritius were analysed for their calcium, magnesium, nickel and zinc levels by flame atomic absorption spectroscopy after digestion by four wet open methods and MWO. The results obtained after the different methods of digestion were compared using the student’s t-test. In addition, the potassium and sodium levels in the 11 medicines were determined by flame photometry, whose validity was checked by analyzing its precision.
In both the TCM and AM, potassium was present in the highest amount. The highest calcium, magnesium, nickel, potassium, sodium and zinc level were observed respectively in Niuhuangchiehdu Pien (912 μg/g), Pilex (265 μg/g), Leung Pui Kee (13.1 μg/g), Jin Qian Chao (26,416 μg/g), Watermelon Frost (6,191 μg/g) and Diabecon (26.8 μg/g). MWO digestion was found to be more effective for Mg, method M1 [conc HNO3 + H2O2 (30 %)] for Ca and Zn, and method M4 (aqua regia) for nickel.
From replicate measurements, the precision of the flame photometric method used for the analysis of potassium was found to be good as the %RSD for both intra-day (0.91 %) and inter-day (1.3–9.0 %) precision was less than the acceptable %RSD (15 %). For sodium, the inter-day precision was found to be in the range 3.0–9.0 %.
To investigate matrix interference, standard addition was carried out on the AM Diabecon for potassium and the TCM Niuhuangchiehdu Pien for sodium. A coefficient of variation of 0.22 % and 3.9 % was observed for the potassium and sodium level respectively indicating little interference from the sample matrix.
Further study is under way for the analysis of other metals, in particular toxic ones in these TCM and AM.
References
World Health Organization (2000) General guidelines for methodologies on research and evaluation of traditional medicine. World Health Organization, Geneva, pp 1–73
Saper RB, Kales SN, Paquin J, Burns MJ, Eisenberg DM, Davis RB, Phillips RS (2004) Heavy metal content of Ayurvedic herbal medicine products. J Am Med Assoc 292:2868–2873
Wang X, Zhuang Z, Sun D, Hong J, Wu X, Lee F, Yang MS, Leung HW (1999) Trace metals in traditional Chinese medicine: a preliminary study using ICP-MS for metal determination and As speciation. Atom Spectrosc 20:86–91
Centres of Disease Control and Prevention (2004) Lead poisoning associated with use of Ayurvedic medications – five states, 2000–2003. MMWR Morb Mortal Wkly Rep 53:582–584
Ernst E (2002) Heavy metals in traditional Indian remedies. Eur J Clin Pharmacol 57:891–896
Saper RB, Phillips RS, Sehgal A, Khouri N, Davis RB, Paquin J, Thuppil V, Kales SN (2008) Lead, mercury and arsenic in US- and Indian-manufactured Ayurvedic medicines sold via the internet. J Am Med Assoc 300:915–923
Yang L-L, Gao L-R, Zhang D-Q (2003) Speciation analysis of arsenic in traditional Chinese medicines by hydride generation-atomic fluorescence spectrometry. Anal Sci 19:897–902
Chan K (2003) Some aspects of toxic contaminants in herbal medicines. Chemosphere 52:1361–1371
Koh H-L, Woo S-O (2000) Chinese proprietary medicine in Singapore: regulatory control of toxic heavy metals and undeclared drugs. Drug Saf 23:351–362
Wu X-H, Sun D-H, Zhuang Z-X, Wang X-R, Gong H-F, Hong J-X, Lee FSC (2002) Analysis and leaching characteristics of mercury and arsenic in Chinese medicinal materials. Anal Chim Acta 453:311–323
Wang C-F, Duo M-J, Chang EE, Yang JY (1996) Essential and toxic trace elements in the Chinese medicine. J Radioanal Nucl Ch Ar 211:333–347
Giacomino A, Abollino O, Malandrino M, Karthik M, Murugesan V (2010) Determination and assessment of the contents of essential and potentially toxic elements in Ayurvedic medicine formulations by inductively coupled plasma-optical emission spectrometry. Microchem J 99:2–6
Dargan PI, Gawarammana IB, Archer JRH, House IM, Shaw D, Wood DM (2008) Heavy metal poisoning from Ayurvedic traditional medicines: an emerging problem? Int J Environ Health 2:463–474
Espinoza EO, Mann MJ, Bleasdell B (1995) Arsenic and mercury in traditional Chinese herbal balls. New Engl J Med 333:803–804
Kales SN, Christophi CA, Saper RB (2005) Hematopoietic toxicity from lead-containing Ayurvedic medications. Med Sci Monit 13:CR295–CR298
Au AM, Ko R, Boo FO, Hsu R, Perez G, Yang Z (2000) Screening methods for drugs and heavy metals in Chinese patent medicines. Bull Environ Contam Toxicol 65:112–119
Al-Omari S (2011) Determination of essential and toxic trace elements in ten herbal medicines using energy-dispersive XRF analysis. X-Ray Spectrom 40:31–36
Lam JC, Chan K-K, Yip Y-C, Tong W-F, Sin DW (2010) Accurate determination of lead in Chinese herbs using isotope dilution inductively coupled plasma mass spectrometry (ID-ICP-MS). Food Chem 121:552–560
Sa F, Vong WT, Chan TM, Lam CWK (2010) Determination of heavy metals in proprietary Chinese medicines by inductively coupled plasma–mass spectrometry. Clin Chim Acta 411:896 (Abstract)
Yuan X, Ling KH, Keung CW (2009) The analysis of heavy metals in Chinese herbal medicine by flow injection–mercury hydride system and graphite furnace atomic absorption spectrometry. Phytochem Anal 20:293–297
Cooper K, Noller B, Connell D, Yu D, Sadler R, Olszowy H, Golding G, Tinggi U, Moore MR, Myers S (2007) Public health risks from heavy metals and metalloids present in traditional Chinese medicines. J Toxicol Env Health 70:1694–1699
Gunturu KS, Nagarajan P, McPhedran P, Goodman TR, Hodsdon ME, Strout MP (2011) Ayurvedic herbal medicine and lead poisoning. J Hematol Oncol 4:51–56
Lavekar GS, Ravishankar B, Gaidhani S, Shukla VJ, Ashok BK, Padhi MM (2010) Mahayograj guggulu: heavy metal estimation and safety studies. Int J Ayurveda Res 1:150–158
Gair R (2008) Heavy metal poisoning from Ayurvedic medicines. BC Med J 50:105
Dobos GJ, Tan L, Cohen MH, McIntyre M, Bauer R, Li X, Bensoussan A (2005) Are national quality standards for traditional Chinese herbal medicine sufficient? Current governmental regulations for traditional Chinese herbal medicine in certain Western countries and China as the Eastern origin country. Complement Ther Med 13:183–190
Mazzanti G, Battinelli L, Daniele C, Costantini S, Ciaralli L, Evandri MG (2008) Purity control of some Chinese crude herbal drugs marketed in Italy. Food Chem Toxicol 46:3043–3047
Koch I, Moriarty M, House K, Jie S, Cullen WR, Saper RB, Reimer KJ (2011) Bioaccessibility of lead and arsenic in traditional Indian medicines. Sci Total Environ 409:4545–4552
Lokhande R, Singare P, Andhale M (2010) Study on mineral content of some Ayurvedic Indian medicinal plants by instrumental neutron activation analysis and AAS techniques. Health Sci J 4:157–168
Lokhande R, Singare P, Andhele M, Acharya R (2010) Study of some Indian medicinal plants by application of INAA and AAS techniques. Nat Sci 2:26–32
Avula B, Wang Y-H, Smillie TJ, Duzgoren-Aydin NS, Khan IA (2010) Quantitative determination of multiple elements in botanicals and dietary supplements using ICP-MS. J Agric Food Chem 58:8887–8894
Fei T, Dehong L, Fengqun Z, Junhua L, Hua T, Xiangzhong K (2010) Determination of trace elements in Chinese medicinal plants by instrumental neutron activation analysis. J Radioanal Nucl Chem 284:507–511
Mahawatte P, Dissanayaka KR, Hewamanna R (2006) Elemental concentrations of some Ayurvedic drugs using energy dispersive XRF. J Radioanal Nucl Chem 270:657–660
Choudhury RP, Kumar A, Reddy AVR, Garg AN (2007) Thermal neutron activation analysis of essential and trace elements and organic constituents in Trikatu: an Ayurvedic formulation. J Radioanal Nucl Chem 274:411–419
Singare P, Lokhande R, Andhale M, Acharya R (2010) Availability of essential trace elements in Ayurvedic Indian medicinal herbs using instrumental neutron activation analysis and atomic absorption spectroscopy. World J Sci Technol Sustain Dev 7:175–190
Yan Q, Yang L, Wang Q, Ma X (2012) Determination of major and trace elements in six herbal drugs for relieving heat and toxicity by ICP-AES with microwave digestion. J Saudi Chem Soc 16:287–290
Krebs J, Michalak M (2007) Calcium: a matter of life or death. Elsevier BV, Amsterdam
Office of Dietary Supplements (2009) Dietary supplement fact sheet: Magnesium. http://ods.od.nih.gov/factsheets/magnesium/. Accessed 5 Mar 2012
Haas E, Levin B (2006) Staying healthy with nutrition. The complete guide to diet and nutritional medicine. Celestial Arts, Berkeley
Office of Dietary Supplements (2011) Dietary supplement fact sheet: Zinc. http://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/. Accessed 7 Mar 2012
Elson MH (2011) Role of potassium in maintaining health. http://org/patients/potassium-health. Accessed 13 Dec 2011
Gittleman AL (2000) Understanding salt and sodium. http://curezone.com/foods/salt/understanding_salt_and_sodium.html. Accessed 26 Oct 2010
Asian Health Secrets (2010) Shilajit: Nature’s Rejuvenator. http://www.asianhealthsecrets.com/letha/?p=2386. Accessed 13 Mar 2012
Word Press (2010) Medicinal plants, herbs, spices: Guggul. Available from: http://herbtime.wordpress.com/2010/02/19/guggul-commiphora-mukul-or-balsamodendron-mukul/. Accessed 15 Mar 2012
Xu L, Wang W (2002) Jin Qian Cao. In: Chinese materia medica: combinations and applications. Donica, St Albans, p 240
Wieckowski SK, Mezyk Z (1999) Studies of trace element content in selected medical herbs. Pol J Environ Stud 8:129–130
Akhtar N, Khan SA, Khan L, Hussain I, Marwat KB (2008) Profile of heavy metals in selected medicinal plants. Pak J Weed Sci Res 14:101–110
Guo L (2012) The producing area of Chinese medicine and famous region drug research – Magnolia officinalis. In: Kuang H (ed) Recent advances in theories and practice of Chinese medicine. InTech, Shanghai, pp 453–460. www.intechopen.com/download/pdf/pdfs_id/26178. Accessed 13 Jan 2012
Himalaya Herbal Health Care (2002) Himalaya’s herbs and minerals: Yashad bhasma. http://www.himalayahealthcare.com/aboutayurveda/cahy.htm. Accessed 15 Mar 2012
Shao YY, Cai BS, Lin J, Xu JS (2007) Determination of trace elements in 13 traditional Chinese medicines in medicated diet for diabetes mellitus by ICP-MS. Zhongguo Zhong Yao Za Zhi 32:2011–2015 [Abstract]
European Medicines Agency (2009) Guidelines for the validation of analytical methods used in residue depletion studies. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/01/WC500040499.pdf. Accessed 13 Jan 2012
Acknowledgements
We are very grateful to the University of Mauritius for providing the necessary facilities to carry out the project. Thanks also to the technical staff of the Chemistry Department, in particular to Mr. V Ramsahye for assistance.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media Dordrecht
About this paper
Cite this paper
Wah, H.L.K., Ramchurn, K., Alladin, S.B. (2014). Metal Levels in Traditional Chinese and Ayurvedic Medicines. In: Gupta Bhowon, M., Jhaumeer-Laulloo, S., Li Kam Wah, H., Ramasami, P. (eds) Chemistry: The Key to our Sustainable Future. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-7389-9_24
Download citation
DOI: https://doi.org/10.1007/978-94-007-7389-9_24
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-7388-2
Online ISBN: 978-94-007-7389-9
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)