
Abstract
Natural killer (NK) cell-derived neoplasms are a group of uncommon, heterogeneous and highly aggressive malignancies mainly seen in Asian and South American populations. The involvement of children is less common compared to adults and hence exclusive pediatric data is lacking and many management decisions are based on adult data. They are classified by the World Health Organization (WHO) into extranodal NK/T-cell lymphoma (nasal and extranasal) (ENKL) and aggressive NK cell leukemia (ANKL). NK cell lymphoblastic lymphoma and chronic lymphoproliferative disorder of NK cell are included in provisional category. While myeloid/NK cell leukemia is considered as a type of AML and Hematodermic NK cell neoplasm is considered dendritic cell neoplasm. NK cell neoplasm is characterized by polymorphic neoplastic infiltrate, angioinvasion and/or angiodestruction, cytoplasmic azurophilic granules, CD2+/surface CD3−/cytoplasmic CD3ε+/CD56+ phenotype and Epstein-Barr virus (EBV) infection. Cytogenetic study shows recurrent aberrations of 6q, 11q, 13q, and 17p. T cell receptor (TCR) genes are always in germline configuration. Mutations of p53, C-KIT, FAs gene and B-catenin are frequently seen. NK-cell neoplasms are often resistant to conventional combination chemotherapy due to p-glycoprotein expression and associated multidrug resistance. L-asparaginase based chemotherapy gives better outcome. The prognoses of both localized and advanced stages of NK-cell malignancies are worse than majority of other lymphoid malignancies. Stem cell trans-plantation is recommended for the advanced/ relapsed disease. Studies are currently underway to assess the safety, efficacy and outcomes of chemotherapy, molecular pathway inhibitors and monoclonal antibodies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Natural Killer Cell
- Hematopoietic Stem Cell Transplantation
- Allogeneic Hematopoietic Stem Cell Transplantation
- Autologous Hematopoietic Stem Cell Transplantation
- Large Granular Lymphocyte
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Natural killer (NK) cells constitute < 5% of peripheral blood lymphocytes that mediate lysis of tumor cells and bacteria- or virus-infected cells and the production of immunomodulatory cytokines. NK cells are derived in the bone marrow from CD34+ hematopoietic progenitor cells (HPCs) through the intermediate developmental stages of lymphoid stem cells, bipotential T/NK progenitor cells and committed NK progenitor cells (Liang and Graham 2008). Morphologically, mature NK cells are large granular lymphocytes (LGLs), with germ line T cell receptor (TCR) and immunoglobulin gene configurations. NK cells have abundant pale cytoplasm with azurophilic granules containing cytolytic molecules such as perforin, granzyme B, and TIA-1. NK cells show a variable expression of the T lineage-associated antigens, such as CD2, CD7 and CD8. They are typically negative for surface-CD3 and myeloperoxidase (MPO) and express cytoplasmic CD3ε chain. CD16, CD56, and CD57 are NK-associated markers, out of which, CD56 (neuronal cell adhesion molecule [N-CAM]) is the most consistently expressed. However, CD56 can also be expressed on cytotoxic T lymphocytes, neural/neuroendocrine tissues and skeletal muscle (Siu et al. 2002; Liang and Graham 2008).
Neoplasms of the NK cells and NK-like T cells are uncommon and are prevalent in Asian and Central and South American populations (Schwartz et al. 2008). The peripheral T-cell and NK/T-cell neoplasms comprise 5–10% of all Non-Hodgkin lymphoma (NHL) in Western countries and 15–20% of NHL in Asia. EBV infection is believed to be responsible for NK cell neoplasm as EBV encoded RNA (EBER) in a clonal episomal form is consistently demonstrated by in situ hybridization (ISH) (Siu et al. 2002). In fact, demonstration of EBV in the neoplastic cells is a diagnostic requisite in WHO classification of NK-/T-cell lymphoma (Chan et al. 2008).
Classification of NK Cell Neoplasm
In the 1994 Revised European-American Lymphoma (REAL) classification, NK cell malignancies were included within the categories of large granular lymphocytic leukemia and angiocentric lymphoma (Harris et al. 1994). Their distinct nature was formally acknowledged at a slide workshop on nasal and related extranodal angiocentric T/NK cell lymphomas by Jaffe et al. (1996), who classified NK cell neoplasm into three categories: precursor NK cell leukemia, nasal and nasal-type NK cell lymphoma, and aggressive NK cell leukemia. The new World Health Organization (WHO) classification encompasses three distinct entities of NK cell neoplasms: extranodal NK/T-cell lymphoma (nasal and extranasal) (ENKL) and aggressive NK cell leukemia (ANKL) (Chan et al. 2001). Aggressive NK cell leukemia and extranodal NK cell lymphoma, nasal types originate from mature NK cells (Liang and Graham 2008). Chronic lymphoproliferative disorder of NK cell and NK/lymphoblastic lymphoma are included in provisional category. While myeloid/NK cell leukemia is considered as a type of AML and Hematodermic NK cell neoplasm is considered a dendritic cell neoplasm.
Extranodal NK/T-cell lymphoma (angiocentric lymphoma in the REAL classification) constitutes most cases of NK cell neoplasms. The term “nasal” is used when the primary site of involvement is the nasal cavity and the upper aerodigestive tract, while “extranasal” or “nasal-type” represent the counterpart of nasal NK cell lymphomas and involve any other part of the body. Nasal NK cell lymphoma must be excluded by CT scan and/or multiple biopsies from nasal septum before diagnosing extranasal type.
An aggressive NK cell leukemia is an uncommon, aggressive, systemic proliferation of NK cells with more than 30% blasts of NK cell origin with rapidly declining clinical course and poor prognosis.
Hematodermic neoplasm (blastic NK cell lymphoma) is now considered a dendritic cell neoplasm rather than NK cell neoplasm due to following observations (1) This tumor is CD4+/CD56+ and also expresses CD68 and CD123 (the interleukin [IL]- 3 receptor) (Chan et al. 2001) . CD 123 is dendritic cell marker (2) absence of EBV, TIA-1, granzyme B and perforin (all NK cell markers). Skin infiltration of hematodermic neoplasm, NK cell lymphoma and myelomonocytic leukemia are CD4+/CD56+ but skin infiltration of hematodermic neoplasm lacks angiodestruction and necrosis unlike NK cell lymphoma while skin infiltration of Hematodermic neoplasm is esterase/peroxidase/T cell lymphoma one antigen negative unlike skin infiltration due to AML-M4.
Myeloid/NK-cell precursor acute leukemia is CD 56+/CD 33+ and is now considered as AML and not NK cell neoplasm. This leukemia affects young population and has frequent extramedullary infiltration. Precursor NK-cell acute lymphoblastic leukemia and chronic NK-cell lymphoproliferative disorders are included in probable category of NK cell neoplasm. Myeloid/NK-cell precursor acute leukemia and Precursor NK-cell acute lymphoblastic leukemia have poor prognosis. Chronic NK-cell lymphoproliferative disorder is less aggressive and has an indolent course in concordance with the T-cell large granular lymphocytic leukemia.
Chronic lymphoproliferative disorder of NK-cells, previously designated as chronic NK-cell lymphocytosis, chronic NK-large granular lymphocyte lymphoproliferative disorder and NK-cell LGL lymphocytosis, are characterized by a persistent (≥ 6 months duration) increase in peripheral blood NK-cells (> 2 × 109/L) without an identifiable cause. Since reactive and neoplastic proliferations are difficult to distinguish, it is currently a provisional entity within the WHO classification. NK-cells are surface CD3-, cytoplasmic CD3ε +; CD16 + with weak CD56 expression. Markers of cytotoxic T cells such as TIA1, granzyme B and granzyme M are positive. The expression of CD2, CD7, and CD57 may be reduced or absent while aberrant co-expression of CD5 and CD8 can be seen. Expression of the KIR family of NK cell receptors is either restricted to one isoform or completely lacking. Immunoglobulin and TCR genes are in germ line configuration and karyotype is normal in most cases. In contrast to aggressive NK-cell leukemia, EBV is negative. There is expression of Fas ligand by the neoplastic cells with elevated serum levels (Lim et al. 2009).
Clinical Presentation
ENKL shows a predilection for Asians, Mexicans, Central and South Americans. It represents 3.3% of all non-Hodgkin’s lymphoma in Japan, 6% in Hong Kong, 8% in Korea and 5% in Taiwan (Suzuki 2005). The median age is 53 years and the male to female ratio is about 3:1 (Cheung et al. 2003).
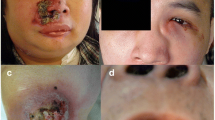
Nasal NK/T-cell lymphoma is the predominant histologic type of primary lymphoma of the nasal cavity in the Asian population. The patients present with a mass or progressive ulceration and destruction of the midline facial structures involving the nasal cavity, nasopharynx, paranasal sinuses, tonsils, hypopharynx and larynx. The common symptoms include nasal discharge, nasal obstruction, purulent rhinorrhea, epistaxis and local swelling of the nasal bridge. In patients with more advanced disease, there may be erythema, swelling of the face, proptosis, nasal septal perforation and impairment of extraocular movement. Erosion of the floor of the nasal cavity may result in the destruction and perforation of the hard palate. In about 10% of patients, hemophagocytic syndrome complicates the disease characterized by fever, rapidly developing pancytopenia, hemophagocytic histiocytes in the bone marrow, coagulopathy, and rapid deterioration in liver function. Lymph node involvement at presentation is uncommon and there is rare involvement of distant sites such as the skin, liver, lung, gastrointestinal tract and testis. Thus, most patients (∼ 82%) have an early stage disease (stage I/II) at presentation (Siu et al. 2002).
Extranasal NK cell lymphomas (“non-nasal” or “nasal-type” NK/T cell lymphomas) represent the counterpart of nasal NK cell lymphomas involving sites other than the nasal cavity and nasopharynx. The median age of presentation and male predominance is similar. Most patients have involvement of multiple anatomic sites at presentation, in the absence of superficial lymphadenopathy. The predominant sites are skin, upper aerodigestive tract (such as palate and larynx), gastrointestinal tract, salivary glands, spleen, testis, soft tissues, (especially muscle), central nervous system, lungs and liver. Isolated nodal involvement is highly unusual. The primary sites of non-nasal NK-cell lymphomas are also the areas where nasal NK-cell lymphomas tend to disseminate (Cheung et al. 2003). Therefore, the diagnosis of extranasal NK cell lymphoma requires the exclusion of nasal involvement at presentation. The skin lesions may be nodules, plaques with ulceration and necrosis or diffuse erythematous swelling. Intestinal perforation due to necrosis may be seen unlike bowel obstruction in conventional intestinal lymphomas. Common systemic symptoms include fever, malaise and weight loss. Additional sites of the disease are often identified on staging. Hemophagocytic syndrome presents with rapidly developing pancytopenia. The disease is highly aggressive. Chan et al. have reported only 10% 2-year disease-free survival (Chan et al. 1997). The worse prognosis may be because most patients were in stage III or IV, had higher International Prognostic Index, lactate dehydrogenase levels (LDH), low hemoglobin and platelet levels compared with nasal NK/T-cell lymphoma (Cheung et al. 2003).
Aggressive NK cell leukemia, first characterized by Imamura et al. (1988) is often designated as “leukemia/lymphoma” because of the concomitant features of both forms. This is a catastrophic, systemic disease and is more prevalent in Asians than in Caucasians (Chan et al. 2001). The disease is characterized by more than 30% of neoplastic NK cells in the peripheral blood or bone marrow. In contrast to ENKL, there is no gender preference and early age of presentation (median being the third decade). Patients typically are very ill at presentation with fever, liver dysfunction, hepatosplenomegaly, systemic lymphadenopathy, leukemic blood picture and sometimes accompanied by a reactive hemophagocytosis. Coagulopathy and multi-organ failure are common. Serum lactate dehydrogenase and Fas ligand are elevated. In contrast to ENKL, skin lesions are uncommon (Cheung et al. 2003; Ishida and Kwong 2010).
Chronic NK- lymphocytosis (CNKL) is characterized by a chronic expansion of mature looking peripheral blood NK cells (≥ 600/mL) without lymphadenopathy or organomegaly for ≥ 6 months. The median age of presentation is 60.5 years (range, 7–77 years) without sex predominance. CNKL has a chronic, indolent course. It can present with neutropenia, pure red cell aplasia, vasculitis and fever with unknown origin. Most patients have an indolent course but some may progress with increasing lymphocytosis and/or worsening of cytopenias. Rarely, patients may transform to an aggressive NK-cell disorder (Greer and Mosse 2009). CNKL may be reactive to viral infections or underlying solid tumors, careful search for infection and solid tumor is recommended (Suzuki 2005).
Diagnostic Work-Up
The diagnoses of NK cell neoplasm requires: expression of at least one NK cell marker (CD56, CD16, or CD57); lack of expression of surface CD3, B-cell antigens (CD19 and CD20), MPO and other lineage markers; and/or germline configuration of TCR and Ig genes. EBV status provides the supportive evidence. It is important to distinguish T-cell neoplasms, myelomonocytic neoplasms and myeloid neoplasms with CD56 expression and hematodermatic neoplasm from true NK cell neoplasms (Liang and Graham 2008).
Examination of the nasal tumor by nasal panendoscopy and biopsy of every involved or suspicious area should be done in a case of suspected NK cell lymphoma. The specimen should be as sizeable as possible to avoid including just the necrotic areas, because tumor zonal necrosis is characteristic of NK-cell lymphomas. The specimens should not be fixed in formalin and should be sent fresh to the laboratory for cryostat sectioning or flow cytometric analysis. This will enable the detection of surface CD3, which distinguishes between T and NK cell lymphomas. NK cell lymphoma lacks surface CD3 while T cell neoplasm shows surface CD3. Surface CD3 is positive in NK cell neoplasm if the tissue is preserved. However, if fresh tumor biopsies are not available, TCR gene rearrangement study helps. TCR genes are germline in NK-cell lymphomas but are clonally rearranged in T-cell lymphomas (Ishida and Kwong 2010; Kwong 2011).
The histological features are similar for nasal and extranasal NK cell lymphoma irrespective of the involved sites. The tumors are characterized by mucosal ulcerations, dense abnormal lymphoid cells infiltration, angiocentric and angiodestructive growth and fibrinoid changes in the blood vessels, coagulative necrosis and apoptosis. Tumor cells may be predominantly small (8% of cases); mixed small and large cells (49% of cases); or predominantly large cells (43% of cases) with moderate amount of pale to clear cytoplasm, irregular or elongated nuclei, granular or vesicular chromatin, and inconspicuous, small nucleoli. Mitotic figures are frequent. Giemsa-stained cytologic preparations show azurophilic granules in the cytoplasm. In some patients, inflammatory cells comprising of small lymphocytes, plasma cells, histiocytes and eosinophils are also seen (Siu et al. 2002; Cheung et al. 2003).
Extranodal NK/T-cell lymphoma are CD2+, surface CD3−, cytoplasmic CD3+ and CD56+ (Ho et al. 1990). Nasal CD3+/CD56− lymphomas are also currently categorized as NK/T-cell lymphoma if they express cytotoxic molecules and harbor EBV. If cytotoxic molecules and EBV are negative, they are labeled as peripheral T-cell lymphoma unspecified. The clinical and histologic features of the CD56− subgroup of NK/T-cell lymphoma are indistinguishable from the CD56+ subgroup. The T-cell receptor genes are in germline configuration in NK cell neoplasms and EBV is nearly always positive. EBV association is strong in Oriental patients, but less consistent in Caucasians. The most commonly observed cytogenetic changes in nasal type NK cell lymphoma are del (6) (q21–q25), del (17) (p12–p13), del (13) (q14–q34), and gain of 1p32-pter (Cheung et al. 2003).
Radiologic imaging of NK cell lymphomas is an essential initial evaluation for staging. Computerized tomographic (CT) scan is better for detection of bony involvement; magnetic resonance imaging (MRI) is superior for soft tissue infiltration. Positron emission tomography (PET) is very useful for other systemic sites. NK cell lymphomas are moderately 18- fluorodeoxyglucose (FDG) avid, with an approximate standardized uptake value of about 5–10. A routine lumbar puncture is not necessary as CNS involvement is uncommon (Ishida and Kwong 2010).
The nasal and upper aerodigestive tract must be thoroughly examined and biopsies taken for patients presenting with the disease at non-nasal sites to exclude nasal NK cell lymphoma with involvement of distant organs. PET scans are useful to detect occult tumors.
An increase in circulating plasma EBV DNA is observed, possibly due to the release of viral DNA following apoptosis of proliferating tumor cells. Therefore, the quantification of circulating plasma EBV DNA in plasma or whole blood by real-time quantitative polymerase chain reaction (Q-PCR) may be a potential surrogate tumor marker in NK cell neoplasm (Ishida and Kwong 2010; Kwong 2011). EB virus encoded RNA-1 in situ hybridization should always be done from bone marrow in NK cell lymphoma as its presence suggests marrow infiltration and poor outcome. CD 56 + cells are known to be lost in marrow and hence immunohistochemical stain for CD 56 is not useful to demonstrate marrow involvement (Lee et al. 2007) .
The leukemic cells may be typical large granular lymphocytes or lymphocytes with enlarged, convoluted nuclei, condensed chromatin, distinct nucleoli, and abundant pale blue cytoplasm containing fine or coarse azurophilic granules. In tissue specimens, the neoplastic infiltrate is diffuse, destructive and permeative. The lymphoid cell population appears monomorphous, but can sometimes be polymorphous. Apoptotic bodies, areas of zonal cell death, necrosis, angioinvasion and angiodestruction are common (Liang and Graham 2008).
Immunophenotypically, these leukemias are similar to extranodal NK/T-cell lymphomas (CD56 +, CD2+, CD7+, cytoplasmic CD3ε +, surface CD3−). CD16 is expressed in half of the aggressive NK-cell leukemias, unlike extranodal NK/T-cell lymphomas. The T- cell receptor gene is in germline configuration and EBV is always expressed (Siu et al. 2002). Like ENKL, the most common cytogenetic abnormalities observed in aggressive NK-cell leukemia are deletion of 6q21–q25 and loss of 17p13 (Greer and Mosse 2009).
In CNKL, bone marrow infiltration by small lymphocytes is interstitial or intrasinusoidal. Occasionally, patients present with slow progressive increase of peripheral blood NK cells with organ involvement. EBV is not usually associated with CNKL. The circulating neoplastic cells are morphologically large granular lymphocytes. Moderate amount of pale cytoplasm containing ≥ 3 azurophilic granules are also observed. The NK cells are CD2+, surface CD3–, cytoplasmic CD3ε+, CD16+ and CD56+ with variable expression of CD57. Bright, uniform CD94 and decreased CD161 expression may be seen. Cytotoxic markers including TIA-1, granzyme B and granzyme M are positive. Altered expression of NK-associated KIR (killer-immunoglobulin like receptors), C-type lecithin-like receptors and natural cytotoxicity receptors have also been described.
To summarize, diagnosis of NK cell neoplasm depends on following data (although not all are required to make a complete diagnosis): (1) a thorough clinical history and physical examination (2) expression of CD56 and the lack of expression of T cell specific antigens. Absence of surface CD3 and presence of cytoplasmic CD3 (3) expression of cytotoxic granule proteins, such as TIA-1, granzyme, and/or perforin; (4) in situ hybridization for EBER to demonstrate EBV positivity; and (5) germline configuration of T cell receptor/Vb chain (Hasserjian and Harris 2007).
Treatment Protocols
The treatment strategy for NK cell neoplasm has not been fully standardized due to recent recognition of these disease entities, their low frequencies and lack of controlled trials. For nasal NK cell lymphomas, combined-modality therapy (radiation and chemotherapy) serves as the best treatment regimen. On the other hand, chemotherapy is the mainstay of treatment for patients with non-nasal NK cell lymphoma and aggressive NK cell leukemia/lymphoma. Unlike conventional lymphomas, anthracyclines are less effective (Kwong 2011). Frontline high dose chemotherapy and hematopoietic stem cell transplantation (HSCT) needs to be evaluated on an individual basis (Kwong 2009). Novel treatment strategies under investigation such as chemotherapy, inhibitors of molecular pathways and monoclonal antibodies are needed to improve the outcome of patients with advanced diseases.
Nasal NK Cell Lymphoma in the Upper Aerodigestive Tract
ENKL is uncommon in children and hence there is little data for children compared to adults. However from the data available, management and outcome of pediatric ENKL is comparable with adults (Wang et al. 2009). Since more than 70% of NK-cell lymphomas develop in the nasal area, much of the clinical data exists for the nasal NK-cell lymphomas. Cure occurs in approximately half of the patient population (Ishida and Kwong 2010). For localized stage I/II nasal NK cell lymphoma, radiotherapy used to be considered as the primary treatment. However, systemic failure occurred in at least 30% of patients which was attributed to the sub-clinical dissemination. Primary chemotherapy was associated with treatment failure in about 40% of localized stage I/II nasal NK cell lymphoma. Therefore, combined chemotherapy and radiotherapy is preferred.
In contrast to other lymphomas that are usually treated with 30 Gy, the radiation dose is typically 50–54 Gy here. A smaller radiation dose has been associated with inferior outcomes when used alone, even after a complete response (CR) has been reached. The radiation field should include the adjacent areas, such as the paranasal cavity, nasopharynx, palate, tonsils, larynx, or any involved cervical lymph nodes, depending on the primary lesions. Optimal margin should be at least 1 cm from the tumor. However, an intensity-modulated radiation therapy (IMRT) with helical tomography in addition to MRI gives more promising results than 3D conformal radiation therapy (3D-CRT) in terms of a significantly better planning target volume (PTV) coverage and equivalent or slightly better organs at risk (OAR) avoidance. Whether the dose of radiotherapy can be decreased with concomitant chemotherapy or radio-sensitizer is not known. Early initiation of radiation, concomitantly or sequentially with chemotherapy, gives better results. Adverse effects of radiation include dermatitis, oral mucositis, taste disturbance and nasal bleeding and discharge. Massive bleeding with mortality due to rapid necrosis of tumors has been reported occasionally.
A phase I/II study of concurrent radiotherapy (50 Gy) and three courses of dexamethasone, etoposide, ifosfamide, and carboplatin (DeVIC) in patients with a newly diagnosed stage IE or contiguous IIE localized nasal natural killer (NK)/T-cell lymphoma showed 77% complete response (CR) with a 2-year overall survival (OS) of 78% compared to 45% with the historical control of radiotherapy alone. The most common grade 3 non-hematologic toxicity was mucositis (30%) with no mortality (Yamaguchi et al. 2009).
A phase II trial of concurrent chemoradiotherapy (CCRT) followed by three cycles of etoposide, ifosfamide, cisplatin, and dexamethasone (VIPD) was conducted in newly diagnosed stages IE to IIE nasal ENKL. The overall response rate and the CR rate were 83.3% and 80.0% respectively. The estimated 3-year progression-free and overall survival rates were 85.19 and 86.28% respectively. Only one patient experienced grade 3 toxicity during CCRT (nausea), whereas neutropenia was seen in 12 out of 29 patients (Kim et al. 2009). Controlled trials of concurrent chemoradiotherapy compared with radiotherapy alone or sequential chemotherapy and radiotherapy are required before drawing definite conclusions.
Unlike other lymphomas, very late relapses of early-stage nasal NK cell lymphoma have been described up to 30 years. Half of the relapses arose from local failure and the rest presented with dissemination or distant lesions. Therefore, life-long follow up is advisable (Kwong 2011).
The use of non-invasive diagnostic technique such as [18F]-fluorodeoxyglucose positron emission tomography (FDG-PET) and the detection of EBV-positive lymphoma cells by EBV-encoded RNA (EBER) in-situ hybridization (ISH) in bone marrow, a site relatively insensitive to FDG-PET, will enable more precise tumor staging and facilitate therapy monitoring. However, more systemic approach is to be adopted for distant or disseminated relapse rather than using simple local radiotherapy (Ishida and Kwong 2010).
In nasal NK-cell lymphoma, responses to radiotherapy or chemotherapy might be affected by the site of the primary lesion. For instance, patients with nasal natural killer (NK)/T-cell lymphoma (N-NKTL) were associated with a lower overall response (54% versus 89%) and higher persistent or progressive disease after initial chemotherapy (46% versus 11%; P = 0.000) as compared to those with Waldeyer ring NK/T-cell lymphoma (WR-NKTL). The 5-year overall survival and progression-free survival rates were 67 and 56% for N-NKTL and 65 and 47% for WR-NKTL, respectively. Patients with stage II WR-NKTL showed favorable prognosis compared to those with stage II N-NKTL. Compared with radiotherapy alone, patients with early-stage WR-NKTL that received radiotherapy and chemotherapy showed a superior progression-free survival and improved overall survival (Li et al. 2009). However, treatment options for stage I/II NK-cell lymphomas at different sites in the upper aerodigestive tract are not markedly different (Ishida and Kwong 2010). The destruction of the orbital bones or palate can lead to functional disabilities, persistent discomfort or cosmetic problems. Reconstructive plastic surgery may be needed.
Localized NK-Cell Lymphomas at Other Areas
Skin is the second most common site of involvement for limited-stage NK-cell lymphomas following upper aerodigestive area. The condition is typically characterized by multiple lesions, resistance to cyclophosphamide, adriamycin, vincristine and prednisolone (CHOP) therapy with the survival usually less than a year. Persistent CR has been achieved through a combination of INF-α, dexamethasone and narrow-band ultraviolet B phototherapy for skin lesions (Tai et al. 2009).
Chemotherapy for Localized NK-Cell Lymphoma at Sites Other Than Upper Aerodigestive Area
Chemotherapy is the mainstay of treatment for advanced stage NK cell lymphomas. Oncologists frequently used the CHOP or CHOP like regimens as they are frequently used for Non-Hodgkin’s lymphoma but CR rate was < 20%. The reason may be high expression of the multi-drug resistance 1 (MDR-1) gene, leading to high levels of ABC transporters such as P-glycoprotein in NK lymphoma cells and thereby facilitating the active export of many chemotherapeutic drugs including anthracyclines. Hence, non-anthracycline containing regimens may actually be more effective in these patients.
Dose-intensified CHOP (DI-CHOP) (1,250 mg/m2 of cyclophosphamide, 75 mg/m2 of doxorubicin, 1.4 mg/m2 of vincristine (maximum 2 mg) on day 1 and 100 mg/day of prednisolone for 5 days) and involved-field radiotherapy (44 Gy, within 4–6 weeks after the DI-CHOP) improved the results with the CR rate of 76% and the 3-year OS rate of 67%. The combination of methotrexate, etoposide, an alkylating agent (cyclophosphamide or ifosfamide) and a corticosteroid (prednisolone or dexamethasone) [ifosfamide 1.5 g/m2 (days 1–3), methotrexate 30 mg/m2 (days 3–10), etoposide 100 mg/m2 (days 1–3) and prednisolone 120 mg (days 1–5)] with or without subsequent radiation showed a CR rate of 55–65% in limited-stage disease. High-dose radiotherapy at 50 Gy with a range of 15–61 Gy, at a dose per fraction of 1.8–2 Gy is considered to be equally beneficial in younger patients and adolescents, but with substantial late complications (Ishida and Kwong 2010).
Advanced-Stage Nasal and Non-nasal NK Cell Lymphoma
The SMILE regimen (comprising of methotrexate 2 g/m2 on day 1, ifosfamide 1,500 mg/m2, etoposide 100 mg/m2 and dexamethasone 40 mg from days 2 to 4, and L-asparaginase 6,000 U/m2 every other day from day 8 to day 20, repeated every 28 days) was designed to address the limitations of MDR phenotypes. Neoplastic NK cells lack asparagine synthase activity and hence L-asparaginase has been shown to induce apoptosis of tumoral NK cells in vitro. Phase I and II studies have confirmed the effectiveness of the SMILE regimen in refractory and relapsed NK/T-cell lymphoma patients, approximately half of whom were in stage IV disease (Ishida and Kwong 2010; Kwong 2011). The overall response rate was 67% and the complete response rate was 50% in the Phase I study, while that in Phase II was 74 and 38% respectively. Because of the profound myelotoxicity, granulocyte colony-stimulating factor support is required.
Unpublished data by Tse and Kwong (2010) showed that 100% of patients with stage I-II disease achieved a durable complete remission when treated with a total of six courses of SMILE chemotherapy supplemented with field radiotherapy after the initial three courses. For patients with advanced-stage disease, a total of six courses of SMILE chemotherapy are usually given. Allogeneic hematopoietic stem cell transplantation should be considered to maintain the remission. High dose chemotherapy with autologous hematopoietic stem cell rescue does not appear to offer substantial benefit. CNS prophylaxis is helpful in NK cell prognostic index group III/IV lymphoma (Kim et al. 2010).
Salvage Treatment of NK-Cell Lymphomas
Patients with relapsed or refractory disease have a very poor outcome. The administration of L-asparaginase in monotherapy or in combination chemotherapy has resulted in favorable responses. Small retrospective studies have observed very good response and survival rates in patients treated with L-asparaginase, combined with vincristine, vinblastine, dexamethasone or methotrexate. A multi-centric open-label French prospective phase II trial in 19 patients confirmed the excellent activity of L-asparaginase-containing regimens with CR in 61%. The median OS and response duration were 1 year. The main adverse events were hepatitis, cytopenia, and allergy. A significantly better outcome was probably due to the absence of anti-asparaginase antibodies and the disappearance of Epstein-Barr virus serum DNA (Jaccard et al. 2011). Various L-asparaginase preparations (Escherichia coli-derived, Erwinia-derived and pegylated forms) appear to have similar treatment results (Kwong 2011).
Aggressive NK-Cell Leukemia/Lymphoma
Few treatment successes have been reported for aggressive NK-cell leukemia/lymphoma, considering its rarity and devastating prototype (Patel et al. 2010). Treatment results of anthracycline-based regimens have been unsatisfactory. Only three of 13 patients achieved CR and extension of survival for several weeks only (Ishida and Kwong 2010). L-asparaginase containing chemotherapy with or without allogeneic hematopoietic stem cell transplantation (HSCT) had resulted in prolonged survivals in a few cases, although the approach still needs to be validated (Ishida and Kwong 2010).
Hematopoietic Stem Cell Transplantation (HSCT)
Because of unsatisfactory outcome in advanced staged ENKL, primary-refractory or relapsed pati-ents and aggressive leukemia, the role of autologous and allogeneic HSCT has been explored. Prospective studies are lacking and most reports are retrospective (Ishida and Kwong 2010).
Autologous HSCT
A recent retrospective multicentric analysis compared NK cell lymphoma patients receiving an autologous HSCT at a median of 8.5 months from diagnosis with a historical control group, treated with chemotherapy or radiotherapy only (Lee et al. 2008). The disease status before HSCT was the most important factor affecting the outcome. Patients with early-stage disease had better outcome than those with advanced or refractory disease but the OS did not differ. Therapy-related mortality was 8.5% in the HSCT group, mainly due to infections. HSCT confers a survival benefit in patients who attained CR on post-remission consolidation therapy. Therefore, for patients in CR with high NK/T cell lymphoma International Prognostic Index (NKIPI), HSCT should be considered.
On the contrary, patients with early stage disease limited to the upper aerodigestive area are potentially curable with combined radiotherapy and chemotherapy. The addition of autologous HSCT would probably not improve survival. The role of autologous HSCT in relapsed or advance stage in CR needs to be explored. Although conditioning regimens CBV (etoposide, carmustine and cyclophosphamide), and BEAM (carmustine, etoposide, cytarabine and melphalan) have been frequently used as they are extensively used in NHL and Hodgkin’s disease, the optimal conditioning before HSCT will need to be defined (Ishida and Kwong 2010; Kwong 2011).
Allogeneic HSCT
A review of case reports indicates that the majority of patients who received allogeneic HSCT had nasal NK-cell lymphoma and, at the time of transplantation, 69% had recognizable or refractory diseases. Half of the patients were alive after HSCT, with 25% transplantation-related mortality and the rest 25% mortality from progressive lymphoma. In one of the largest retrospective series till date, 32% of the patients with active disease at allogeneic HSCT showed 40% 2 year OS. A graft-versus lymphoma effect was evident when a patient relapsed after allogeneic HSCT achieved a durable remission with discontinuation of immunosuppression. Thus, theoretically, reduced-intensity allogeneic HSCT may significantly reduce treatment-related complications while conserving the benefits of graft-versus lymphoma effect. The potential benefit of allogeneic over autologous HSCT is theoretical graft-versus-lymphoma effect, which is of particular significance as NK-lymphoma cells express EBV viral antigens, which may be targeted by donor derived cytotoxic T cells. Heterogeneity of these retrospective trials affect accurate interpretation: differences in donor source (such as HLA-matched siblings, unmatched donors, or cord blood), conditioning regimens (presence or absence of total-body irradiation), and timing of HSCT (at remission, during relapse or refractory disease) (Ishida and Kwong 2010; Kwong 2011). Further international collaborative trials are required to decide the optimal role of allogeneic HSCT in NK cell malignancies.
Novel Treatment Approaches
High P-glycoprotein expression by NK cell neoplasm contributes to the resistance to anthracycline based treatment regimens. Novel agents that bypass P-glycoprotein may improve prognosis. However, new studies are hampered by the rarity of the diseases, the geographic variation and the lack of international cooperation (Greer and Mosse 2009).
Gemcitabine, a pyrimidine analogue, and the purine analogues pentostatin, fludarabine, cladribine and forodesine have shown activity as single agents in peripheral NK/T-cell lymphomas and are currently being combined with other agents. Preclinical and clinical studies on pralatrexate, a novel folate analog inhibitor of dihydrofolate reductase, designed to have high affinity for the reduced folate carrier type 1, have demonstrated greater intracellular accumulation and high response rate in peripheral T-cell lymphomas (Greer and Mosse 2009). Mucositis, the dose-limiting toxicity for pralatrexate could be abrogated with folic acid and vitamin B12 supplementation. The combination of pralatrexate followed by gemcitabine has exhibited synergistic activity in vitro and is currently in clinical trials.
Histone deacetylase (HDAC) inhibitors induce histone hyperacetylation and chromatin remodeling and can modify gene expression in cancer cells by changing the conformation of DNA and thus alter gene interaction with transcription factors. Vorinostat and romidepsin (depsipeptide) have been shown to increase histone acetylation and to restore expression of tumor-suppressor and/or cell-cycle regulatory genes—inducing cell-cycle arrest and apoptosis in cutaneous T-cell lymphoma (CTCL). Panobinostat is well tolerated and down regulates genes affecting angiogenesis in CTCL patients thereby inducing clinical responses. Recent data indicates that HDAC inhibitors may up regulate IL-2 receptor expression on malignant T cells, resulting in enhanced susceptibility to killing by agents targeting IL-2, such as denileukin diftitox (Greer and Mosse 2009).
The activation of nuclear factor (NF)-kappaB/Rel proteins plays an important role in the development/progression of B and T cell lymphoid malignancies. NF-κB influences the activation of genes that encodes anti-apoptotic proteins and proteins that affect cell-cycle progression and is mediated by the ubiquitin-proteasome pathway. Bortezomib inhibits the canonical nuclear factor (NF)-κB pathway by preventing proteasome mediated degradation of inhibitor of κBα (IκBα) as well as the alternative processing pathway of the p-100 subunit (Greer and Mosse 2009).
EBV-positive ENKL cell lines, Hank-1, NK-YS, and NK-L, have high Fas surface expression but are resistant to Fas-mediated apoptosis induced by anti-Fas antibodies. Co-treatment of Hank-1 with cycloheximide, a protein synthesis inhibitor, markedly sensitized cells to Fas-mediated apoptosis, activated caspase 8 and downregulated c-FLIP(L) (cellular FLICE inhibitory protein long form) (Greer and Mosse 2009).
Four courses of a farnesyl transferase inhibitor tipifarnib has been found to improve elevated pulmonary artery pressure and erythroid differentiation after disrupting the NK-receptor signaling pathway in large granular lymphocyte leukemia which has poor hematopoiesis (Epling-Burnette et al. 2008).
Various monoclonal antibodies against NK cell or NK-related cells are now available, although there is no ubiquitous marker similar to CD20 in B-cell lymphomas. Alemtuzumab, a humanized anti-CD52 antibody, is highly active in T-prolymphocytic leukemia, but the level of CD52 expression varies widely in T/NK-cell neoplasms. Case reports have suggested responses to bevacizumab, a monoclonal antibody against VEGF, in angioimmunoblastic T-cell lymphoma with a prominent vascular component. Ongoing trials are investigating the role of denileukin diftitox, alemtuzumab and bevacizumab with combination chemotherapy regimens for NK/T-cell lymphomas (Greer and Mosse 2009).
A phase I dose-escalation trial of siplizumab, a humanized monoclonal antibody to CD2 in patients with T-cell malignancies, resulted in decreased expression of CD2 and depletion of CD4+, CD8+ T cells and NK cells. Although initial responses were encouraging, 13.7% of the patients developed EBV-positive lymphoproliferative disease and the trial was terminated. Another phase I study demonstrated the potential efficacy and tolerance of KW-0761, a defucosylated humanized anti-CC chemokine receptor 4 (CCR4) antibodies, in patients with relapsed CCR4-positive adult T-cell leukemia-lymphoma (ATLL) or peripheral T-cell lymphoma (PTCL). CCR4 receptor is also expressed by a subset of NK cell neoplasm and hence KW 0761 may be useful in NK cell neoplasm also (Greer and Mosse 2009).
NK cell neoplasm is EBV positive but antiviral drugs are not effective as thymidine kinase is not expressed. Arginine butyrate, a short chain fatty acid, induces EBV thymidine kinase expression so that anti-viral drugs can act on these cells. Arginine and gancyclovir have been used in refractory cases with significant anti-tumor activity in 66% of cases (Perrine et al. 2007).
Prognosis
Ann-Arbor staging doesn’t correlate well with prognosis in NK cell neoplasm due to various reasons: (1) NK cell lymphomas are almost exclusively extranodal (2) Ann-Arbor staging system is based on the concept of contiguous lymphatic spread and designed mainly for Hodgkin lymphoma and may not always be accurate for NK-cell lymphomas and (3) Ann-Arbor staging system does not take into account the tumor burden. Therefore, a T-staging system, originally designed for sinonasal B-cell lymphoma has been adopted to overcome this problem by taking into account the extent of local tumor involvement (Robbins et al. 1985). T1 denotes confinement to the nasal cavity. T2 indicates extension to the maxillary antra, anterior ethmoid sinus or hard palate. T3 indicates extension to posterior ethmoid sinus, sphenoidal sinus, orbit, superior alveolar bone, cheeks, or superior buccinators space. T4 indicates involvement of the inferior alveolar bone, inferior buccinators space, infratemporal fossa, nasopharynx, or cranial fossa. A number of prognostic models have been designed in this regard, including the International Prognostic Index (IPI), a clinical tool developed by oncologists to aid in predicting the treatment outcome in malignant lymphomas of different grades and subtypes. The index depends on factors like patient’s age, stage of the lymphoma, whether or not it is in organs outside the lymph system, performance status of the patient and the serum level of LDH. It allows the doctors to plan treatment better than they could just base on the type and stage of the lymphoma. It also gives patients information about the outlook for their future. The good prognostic factors include:
-
Age 60 or below
-
Stage I or II (Ann Arbor)
-
No lymphoma outside of lymph nodes, or lymphoma in only 1 area outside the lymph nodes
-
Performance Status: Able to function normally
-
Serum LDH is normal
The poor prognostic factors, on the other hand, include:
-
Age above 60 years
-
Stage III or IV (Ann Arbor)
-
Lymphoma is in more than 1 organ of the body outside of lymph nodes
-
Performance Status: Needs a lot of help with daily activities
-
Serum LDH is elevated
Each poor prognostic factor is assigned 1 point. Patients without any poor prognostic factors would have a score of 0, while those with all the poor prognostic factors would have a score of 5. The index divides patients into four risk groups:
-
Low (0 or 1 poor prognostic factors)
-
Low intermediate (2 poor prognostic factors)
-
High intermediate (3 poor prognostic factors)
-
High (4 or 5 poor prognostic factors)
Patients with IPI of one or less have been shown to have a better overall survival. Two other prognostic models based on the IPI concept have also been proposed. Considering B symptoms, stage, LDH level and regional lymph node involvement, stage I/II nasal NK cell lymphomas were found to be better stratified into different risk groups (Kwong 2011). In another prognostic model, non-nasal type, stage, performance status and number of extranodal involvement were found to be significant in predicting outcome (Suzuki et al. 2010).
In conclusion, NK cell tumors are uncommon, aggressive, and heterogeneous group of disorders with varying geographical prevalence and dismal clinical outcome. They are clinically subdivided into nasal NK-cell lymphoma, non-nasal NK-cell lymphoma and aggressive NK-cell leukemia/lymphoma. The diagnosis is based on the morphology, immunohistochemistry, demonstration of EBV and cytogenetic study. The management requires high dose local radiotherapy and non-MDR-dependent drugs due to P-glycoprotein expression. L-asparaginase based regimens like SMILE appear to be promising. Autologous and allogeneic HSCT have been recommended in selected patients with a poor prognosis. The novel agents that bypass P-glycoprotein expression or that target molecular pathways or surface receptors are under investigations.
References
Chan JK, Sin VC, Wong KF, Ng CS, Tsang WY, Chan CH, Cheung MM, Lau WH (1997) Nonnasal lymphoma expressing the natural killer cell marker CD56: a clinicopathologic study of 49 cases of an uncommon aggressive neoplasm. Blood 89:4501–4513
Chan JKC, Jaffe ES, Ralfkiaer E (2001) Extranodal NK/T-cell lymphoma, nasal type. In: Jaffe ES, Harris NL, Stein H et al (eds) Pathology and genetics, tumours of haematopoietic and lymphoid tissues. World Health Organization classification of tumours. IARC Press, Lyon, pp 204–207
Chan JK, Quintanilla-Martinez L, Ferry JA, Peh SC (2008) Extranodal NK/T-cell lymphoma, nasal type. In: Swerdlow SH, Campo E, Harris NL et al (eds) WHO classification of tumours of haematopoietic and lymphoid tissues. International Agency for Research on Cancer, Lyon, pp 285–288
Cheung MMC, Chan JKC, Wong K (2003) Natural killer cell neoplasms: a distinctive group of highly aggressive lymphomas/leukemias. Semin Hematol 40:221–232
Epling-Burnette PK, Sokol L, Chen X, Bai F, Zhou J, Blaskovich MA, Zou J, Painter JS, Edwards TD, Moscinski L, Yoder JA, Djeu JY, Sebti S, Loughran TP Jr, Wei S (2008) Clinical improvement by farnesyl transferase inhibition in NK large granular lymphocyte leukemia associated with imbalanced NK receptor signaling. Blood 112:4694–4698
Greer JP, Mosse CA (2009) Natural killer–cell neoplasms. Curr Hematol Malig Rep 4:245–252
Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML, Delsol G, De Wolf-Peeters C, Falini B, Gatter KC (1994) A revised European-American classification of lymphoid neoplasms: a proposal from the international lymphoma study group. Blood 84:1361–1392
Hasserjian RP, Harris NL (2007) NK-cell lymphomas and leukemias. A spectrum of tumors with variable manifestations and immunophenotype. Am J Clin Pathol 127:860–868
Ho FC, Choy D, Loke SL, Kung IT, Fu KH, Liang R, Todd D, Khoo RK (1990) Polymorphic reticulosis and conventional lymphomas of the nose and upper aerodigestive tract: a clinicopathologic study of 70 cases, and immunophenotypic studies of 16 cases. Hum Pathol 21:1041–1050
Imamura N, Kusunoki Y, Kajihara H, Okada K, Kuramoto A (1988) Aggressive natural killer cell leukemia/lymphoma with N901-positive surface phenotype: evidence for the existence of a third lineage in lymphoid cells. Acta Haematol 80:121–128
Ishida F, Kwong YL (2010) Diagnosis and management of natural killer-cell malignancies. Expert Rev Hematol 3:593–602
Jaccard A, Gachard N, Marin B, Rogez S, Audrain M, Suarez F, Tilly H, Morschhauser F, Thieblemont C, Ysebaert L, Devidas A, Petit B, de Leval L, Gaulard P, Feuillard J, Bordessoule D, Hermine O, GELA and GOELAMS Intergroup (2011) Efficacy of L-asparaginase with methotrexate and dexamethasone (AspaMetDex regimen) in patients with refractory or relapsing extranodal NK/T-cell lymphoma, a phase 2 study. Blood 117:1834–1839
Jaffe ES (1996) Classification of natural killer (NK) cell and NK-like T-cell malignancies. Blood 87:1207–1210
Kim SJ, Kim K, Kim BS, Kim CY, Suh C, Huh J, Lee S, Kim SJ, Cho J, Lee G, Kang KM, Eom HS, Pyo HR, Ahn YC, Ko YH, Kim WS (2009) Phase II trial of concurrent radiation and weekly cisplatin followed by VIPD chemotherapy in newly diagnosed, stage IE to IIE, nasal, extranodal NK/T-cell lymphoma: consortium for improving survival of lymphoma study. J Clin Oncol 27:6027–6032
Kim SJ, Oh SY, Hong JY, Chang MH, Lee DH, Huh J, Ko YH, Ahn YC, Kim HJ, Suh C, Kim K, Kim WS (2010) When do we need central nervous system prophylaxis in patients with extranodal NK/T-cell lymphoma, nasal type? Ann Oncol 21:1058–1063
Kwong YL (2009) High-dose chemotherapy and hematopoietic SCT in the management of natural killer-cell malignancies. Bone Marrow Transplant 44:709–714
Kwong YL (2011) The diagnosis and management of extranodal NK/T-cell lymphoma, nasal-type and aggressive NK-cell leukemia. J Clin Exp Hematop 51:21–28
Lee J, Suh C, Huh J, Jun HJ, Kim K, Jung C, Park K, Park YH, Ko YH, Kim WS (2007) Effect of positive bone marrow EBV in situ hybridization in staging and survival of localized extranodal natural killer/T-cell lymphoma, nasal-type. Clin Cancer Res 13:3250–3254
Lee J, Au WY, Park MJ, Suzumiya J, Nakamura S, Kameoka J, Sakai C, Oshimi K, Kwong YL, Liang R, Yiu H, Wong KH, Cheng HC, Ryoo BY, Suh C, Ko YH, Kim K, Lee JW, Kim WS, Suzuki R (2008) Autologous hematopoietic stem cell transplantation in extranodal natural killer/T cell lymphoma: a multinational, multicenter, matched controlled study. Biol Blood Marrow Transplant 14:1356–1364
Li XY, Liu QF, Qi SN, Wang H, Wang WH, Song YW, Lu J, Jin J, Wang SL, Liu YP, Lu N, Liu XF, Yu ZH (2009) Variable clinical presentations of nasal and waldeyer ring natural killer/T-cell lymphoma. Clin Cancer Res 15:2905–2912
Liang X, Graham DK (2008) Natural killer cell neoplasms. Cancer 112:1425–1436
Lim MS, de Leval L, Quintanilla-Martinez L (2009) Commentary on the 2008 who classification of mature T- and NK-cell neoplasms. J Hematop 2:65–73
Patel AP, Ghatak SB, Patel JA (2010) Long term survival in aggressive NK-cell leukemia. Indian Pediatr 47:807–808
Perrine SP, Hermine O, Small T, Suarez F, O’Reilly R, Boulad F, Fingeroth J, Askin M, Levy A, Mentzer SJ, Di Nicola M, Gianni AM, Klein C, Horwitz S, Faller DV (2007) A phase 1/2 trial of arginine butyrate and ganciclovir in patients with Epstein-Barr virus-associated lymphoid malignancies. Blood 109:2571–2578
Robbins KT, Fuller LM, Vlasak M, Osborne BS, Velasquez WS, Sullivan JA (1985) Primary lymphomas of the nasal cavity and paranasal sinuses. Cancer 56:814–819
Schwartz EJ, Molina-Kirsch H, Zhao S, Marinelli RJ, Warnke RA, Natkunam Y (2008) Immunohistochemical characterization of nasal-type extranodal NK/T-Cell lymphoma using a tissue microarray: an analysis of 84 cases. Am J Clin Pathol 130:343–351
Siu LLP, Chan JKC, Kwong YL (2002) Natural killer cell malignancies: clinicopathologic and molecular features. Histol Histopathol 17:539–554
Suzuki R (2005) Leukemia and lymphoma of natural killer cells. J Clin Exp Hematop 45:51–70
Suzuki R, Suzumiya J, Yamaguchi M, Nakamura S, Kameoka J, Kojima H, Abe M, Kinoshita T, Yoshino T, Iwatsuki K, Kagami Y, Tsuzuki T, Kurokawa M, Ito K, Kawa K, Oshimi K, NK-cell Tumor Study Group (2010) Prognostic factors for mature natural killer (NK) cell neoplasms: aggressive NK cell leukemia and extranodal NK cell lymphoma, nasal type. Ann Oncol 21:1032–1040
Tai WC, Li HP, Lin TY, Lin CY, Wu MT (2009) Response of extranodal natural killer/T-cell lymphoma, nasal type, to interferon-a, corticosteroid and narrow band ultraviolet B phototherapy. Clin Exp Dermatol 34:e927–e930
Tse E, Kwong YL (2010) Recent advances in the treatment of lymphomas. J Hong Kong Col Radiol 13(Suppl):S22–S24
Wang ZY, Li YX, Wang WH, Jin J, Wang H, Song YW, Liu QF, Wang SL, Liu YP, Qi SN, Fang H, Liu XF, Yu ZH (2009) Primary radiotherapy showed favorable outcome in treating extranodal nasal-type NK/T-cell lymphoma in children and adolescents. Blood 114:4771–4776
Yamaguchi M, Tobinai K, Oguchi M, Ishizuka N, Kobayashi Y, Isobe Y, Ishizawa K, Maseki N, Itoh K, Usui N, Wasada I, Kinoshita T, Ohshima K, Matsuno Y, Terauchi T, Nawano S, Ishikura S, Kagami Y, Hotta T, Oshimi K (2009) Phase I/II study of concurrent chemoradiotherapy for localized nasal natural killer/T-cell lymphoma: Japan Clinical Oncology Group Study JCOG0211. J Clin Oncol 27:5594–5600
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this chapter
Cite this chapter
Patel, A., Ghatak, S. (2013). Pediatric Leukemia of Natural Killer Cells: Diagnosis and Multi-Agent Chemotherapy. In: Hayat, M. (eds) Pediatric Cancer, Volume 4. Pediatric Cancer, vol 4. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-6591-7_14
Download citation
DOI: https://doi.org/10.1007/978-94-007-6591-7_14
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-6590-0
Online ISBN: 978-94-007-6591-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)