
Abstract
Urolithiasis has been known for a very long time. Although pediatric urolithiasis is common, there is great variation in the incidence, prevalence, stone composition, and etiological factors, leading to a complex pathogenesis. This review examines pediatric urolithiasis in a developing country, highlighting the epidemiology and clinical presentations (including stones in infancy), including patients presenting without having been previously treated and with renal failure. Stone composition shows a predominance of ammonium hydrogen urate (AHU). Dietary and metabolic evaluations identified the risk factors in many of these patients. The majority of these patients can be managed by minimally invasive surgery, including extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and ureterorenoscopy (URS). However, open surgical procedures still have a limited, although important, role for patients with anatomical abnormalities and large stone burdens with sepsis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Minimally Invasive Surgery
- Calcium Oxalate
- Stone Disease
- Extracorporeal Shock Wave Lithotripsy
- Ureteric Stone
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Urolithiasis has been known for a very long time, with the first evidence found in Egyptian mummies [1]. Hippocrates was perhaps the first to describe stone disease [2, 3], yet it is still a mysterious pathology involving multiple etiological factors, including genetics, anatomy, diet, environment, and infection, which may work alone or in combination, thus giving stone disease its complex pathogenesis [4]. In simple terms, stones are endemic or idiopathic, genetic (metabolic), or infective. Nevertheless, there is still large gap in our knowledge. For example, with cystine or xanthine stones, a kidney with no obvious or visible anatomical defect forms recurrent stones, while the contralateral kidney remains stone free. Therefore, the focus of the chapter has been on management rather than etiology. There have been tremendous advances in technology for diagnostic imaging. In addition, small-size pediatric endoscopic instruments can be used to manage or remove stones by various minimally invasive surgical procedures. Unfortunately, the same level of progress has not been achieved in understanding the etiology of the disease, such as why stones form and why they recur.
This review provides a perspective from a developing country, with an overview of the present understanding of the disease, as well as the principles and rationale of current management options.
2 Epidemiology
There is great variation in the incidence and prevalence of stone disease in different regions of the world. Variation is also found in age, gender, presentation, and stones composition. In Europe, infective stones prevail while in Pakistan, ammonium hydrogen urate (AHU) stones are predominant [5] – upper tract stones in the developed world and lower tract stones in the developing world [5, 6]. However, historically, a comparison of stone types in the McCarrison study in 1931 interestingly showed the same stone types in both the United Kingdom and India, where the main reason is malnutrition and dietary risk factors [7].
Recently there has also been a progressive increase in the incidence of pediatric urolithiasis, especially in the developed world – the so-called “stone wave” – with reports of a fivefold increase in stone disease in North America and Turkey [8].
The Afro-Asian stone belt region, with high incidence and prevalence of stone disease, extends from Sudan and Egypt in Africa to Saudi Arabia, Iran, Turkey, Pakistan, and India in Asia, extending as far east as the Philippines in the Far East [7–10]. In our experience, urolithiasis amounts to 60 % of the pediatric urology workload (Fig. 30.1) [11].

Pediatric urological workload at SIUT from 1998 to 2013 (n = 17,629)
Advances in imaging techniques, improved socioeconomic conditions, obesity, and increased consumption of protein-rich diets and dairy products are some of the factors contributing to the increased incidence in the West, where a chronically inadequate dietary intake of proteins (malnutrition), dehydration, and diarrheal disease have long been known and still remain the major contributory factor to the high prevalence of the disease in developing countries [9].
3 Demography of Stone Patients
In all, 10,929 patients were seen in the period 1998–2013, with a mean age at the time of presentation of 6.5 ± 3.5 years (range <1–15 years). There was a slight male to female predominance of 2.5:1. Two hundred and nine patients presented in infancy (<1 year), with a male to female ratio of 5:1 (Fig. 30.2). The youngest patient presented to us at the outpatient clinic was 53 days old; however, there are reports of picking up urolithiasis prenatally using ultrasonography [12, 13].

Urolithiasis in infancy
4 Clinical Presentation
The commonest presentation is abdominal pain, vague in young children, and more localized flank pain in older children. Other features include hematuria, fever, lower urinary tract symptoms such as frequency, urgency, and dysuria, with or without urinary tract infections [14, 15]. Occasionally stones are identified as an incidental finding on ultrasounds carried out for other pathologies. Some patients present with renal or ureteric colic, and others with strangury because of vesical calculi and even with acute retention of urine, secondary to small stones getting stuck in the urethra.
In our setting, many children present with calculus oligo-anuria with advanced renal failure, fever, tachypnoea, hypotension, severe acidosis, and uraemia, secondary to bilateral obstructing stones or solitary kidney with obstruction [15]. These children develop chronic renal stone disease, caused by neglect and delay in seeking treatment, where they develop a large stone burden with pyeonephrosis, xanthogranulomatous pyelonephritis, renal cortical atrophy, chronic renal failure, advanced uraemia, and even ESRD (end stage renal disease) [15]. Many require resuscitation and urgent renal replacement therapy for stabilization, and further management of the stone disease.
5 Diagnostic Investigation
Baseline investigation includes ultrasound and x-ray KUB complete blood picture, urea, creatinine, electrolytes, urine analysis and culture and sensitivity depending on the associated clinical conditions, i.e., renal failure, advanced uraemia, or urosepsis. The following investigations are undertaken on a case–by-case basis: arterial blood gases (ABGs), blood culture, serology of hepatitis B and C, clotting profile, and chest X-ray.
6 Evaluation and Management
6.1 Evaluation
All the patients presenting to our outpatient department or emergency are evaluated according to protocol (Fig. 30.3).

Evaluation protocol for pediatric stone formers
6.1.1 Metabolic Risk Factors
Metabolic analyses identify abnormalities which contribute to the risk of urolithiasis. This analysis is especially important in children because the risk factors identified are corrected to prevent recurrence. Our protocol includes blood tests for urea, creatinine, electrolytes, calcium, phosphate, uric acid, and magnesium. A 24-h urine sample is evaluated in all children to determine volume, pH, protein, electrolytes, magnesium, phosphate, calcium, uric acid, citrate, and oxalate. It is a cumbersome procedure as compliance is poor in children, particularly because of involuntary voiding. In some cases we place an indwelling catheter and in others we collect timed urine or spot urine, and calculate levels by solute to creatinine ratio. Metabolic studies in 2563 children are given in Table 30.1. A separate analysis is also given for the predominant stone types AHU and calcium oxalate (CaOx).
In our population, we were able to identify some predominant factors which contributed to stone formation including hyperoxaluria, hypocitraturia, hypovolemia, and hyperuricosuria.
Calcium levels in our population are not as high as seen in the West because of low dietary intake of dairy products, and this contributes to the high urinary oxalate levels, as little calcium is available to chelate the dietary oxalate, leading to high levels of oxalate excretion.
Hypocitraturia is found in 87 % of the stone-forming children. In a prospective analysis we compared the urinary citrate levels of our stone-forming children with their non-stone-forming siblings and found that 79 % of these siblings have lower levels of citrate. Hypocitraturia is reported from other developed countries [16], although it remains to be determined whether hypocitraturia has a genetic or dietary origin in our region.
Hypovolumia is a significant contributing factor, as nearly half of the children with AHU stones had low urinary volumes with low sodium levels.
Urinary uric acid levels are the fourth most important contributing factor. Uric acid levels are higher, due to the high intake of legumes and wheat grain. Other than the dietary effect, the role of metabolic derangement cannot be ruled out in uric acid stone formers. In our experience, a properly collected urine specimen can identify the risk factors in more than 90 % of stone-forming children with idiopathic stones. Dietary and medicinal intervention normalizes the risk factors in more than 70 % of these children.
6.1.2 Stone Analysis
Chemical composition of stones is the hallmark of studies on etiology, risk factors, and management strategies. Stone analysis is undertaken by Fourier Transformation Infrared Spectroscopy (FTIR), depending on the size of the stone and the fragments available by minimally invasive surgery (MIS) or open surgery. Separate analysis of the core and surface is undertaken whenever possible.
Of 4,648 stone analyzed, 1,794 (38.6 %) were pure stones with single constituent and 2,854 (61.4 %) were mixtures. The frequency of compounds in stones from different sites is given in Table 30.2. Calcium oxalate is the main component in 69–72 % of the stones, followed by ammonium hydrogen urate in 52–55 %. The frequency of compounds in pure stones shows an interesting variation with age (Fig. 30.4).

Distribution of pure renal stones in different age groups (n = 1,009)
Children younger than 5 years have predominantly AHU stones, whereas those older than 6 years have mostly CaOx stones. Many of the children younger than 5 years present with malnutrition, diarrheal disease, and dehydration, known risk factors for AHU stone formation (Table 30.2, Fig. 30.5).

Model of ammonium hydrogen urate stone formation
High urinary ammonium content is caused by a diet rich in wheat and intracellular acidosis. Low citrate and potassium in the presence of high urate levels leads to AHU stone formation. In contrast, older children without these risk factors form calcium oxalate stones. Separate analysis of the core and surface of the stones showed that stones starting as AHU later grow by addition of calcium oxalate.
6.1.3 Role of Diet in Urolithiasis
Diet plays an important role in the pathogenesis and management of pediatric urolithiasis. Stone formers routinely undergo anthropometry and dietary evaluation, and are given dietary protocol to reduce the risk factors.
We use a 7-day food diary and a food frequency questionnaire to obtain information about children’s intake of food associated with urolithiasis. These include animal protein, calcium, oxalate, phosphates, purine, sodium, potassium, and refined sugar [17]. Twenty-four-hour fluid intake is assessed by number of glasses consumed. Criteria to analyze fluid intake depends on milliliters per kilogram as recommended.
Anthropometric and dietary analysis. Anthropometric data from 2,372 children with urolithiasis revealed growth deficit and malnutrition in our patient population [15]. The normal Z-score for height and weight, i.e., >−1, was observed in 35 and 24 % of the children, respectively. Of those remaining, 17 % for height and 9 % for weight were severely deficient (Z <−3).
Food frequency questionnaires and dietary recall were analyzed for 2,176 patients and showed low intake of proteins (74 %), potassium (43 %), fiber (48 %), calcium (55 %), and fluids (55 %). High consumption of oxalate in 57 %, sodium in 39 %, purine in 42 %, and refined sugar in 41 % was observed. More than half (60 %) of the population was taking less than the recommended calories [15].
6.1.4 Imaging
6.1.4.1 Ultrasonography
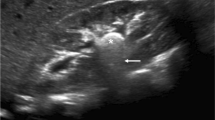
Ultrasound KUB (kidney, ureter, and bladder) is considered as part of the extended physical examination in urology, and the same is true for urolithiasis. It has high sensitivity and specificity for both opaque and non-opaque stones. Stones present as hyperechoic areas in the pelvicalyceal system with negative anechoic areas behind them (posterior acoustic shadowing). Ultrasonography gives an added advantage, in that it can tell us about kidney size and thickness of the cortex, echogenicity of the cortex, hydronephrosis, and any associated hydroureter. Repeat ultrasonograms can be performed for follow-up of the disease.
6.1.4.2 X-Ray
Plain X-ray KUB was the very first investigation in the evaluation of urolithiasis, although alone it has low sensitivity and specificity. However, this increases to >90 % when sonography and X-ray KUB are combined, and this combination is the only required diagnostic imaging for most of our cases.
6.1.4.3 IVU
The old time gold standard IVU (intravenous urogram) is now performed in selective cases only with normal renal functions where information regarding the pelvicalyceal system (PCS) is required in greater detail, and where computerized tomography (CT scan) is not available or when CT scan requires general anesthesia. IVU has certain requirements, such as extensive preparation of the bowel, as in children bowel gases obscure key information regarding the stone site and pelvicalyceal anatomy. There is also a risk of allergic reactions and nephropathy. It is also unable to delineate the anatomy of the PCS in renal dysfunction or severe obstruction, and radiation hazards are also a disadvantage.
6.1.4.4 Non-contrast Computerized Tomography
When any further imaging is required, non-contrast computed tomography has replaced IVU, and it provides extensive details of the stone size, the site, and the anatomy of the PCS. It is the investigation method of choice for patients with ureteric colic, where it identifies ureteric stones, especially mid-ureteric stones, which are almost impossible to detect by USG, X-ray KUB, and IVU together.
Non-contrast CT (NCCT) also provides information about the surrounding tissue, excluding any other pathology, as the cause of acute pain in the surrounding viscera. NCCT can also be helpful in the assessment of stone composition, and can easily differentiate between calcium and non-calcium stones on the basis of attenuation values i.e. Hounsfield units (HU) (Fig. 30.6).

Mean Hounsfield units (HU) in different stone types
6.1.4.5 Isotope Scan
An isotope scan, especially using DMSA (dimercaptosuccinic acid – a radioactive tracer), is used to assess the relative function of the kidney.
6.2 Management
6.2.1 Medical Management
Medical expulsive therapy with alpha blockers is prescribed for ureteric stones and post–ESWL (extracorporeal shock wave lithotripsy). Adequate hydration for the whole 24 h is one of the best measures to prevent kidney stone formation, and therefore we encourage good hydration in our patients on a milliliter per kilogram basis and keep a watch on the urine color to ensure it remains white or light yellow. Two servings of lemon juice daily are recommended to provide a good oral citrate source. Potassium citrate-containing syrup is provided from the hospital for patients with calcium oxalate, cystine, xanthine, and urate stones to maintain adequate urinary alkalinization, and urinary pH is checked with litmus paper. Specific medical therapy is advised on an individual basis.
6.2.2 Surgical Management of Urolithiasis in Children
Historically, all patients are managed by open surgery. Advances in technology and invention of pediatric-size endoscopic instruments have created a paradigm shift from open surgical procedures to minimally invasive surgery (MIS) [18]. These include extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), retrograde intrarenal surgery (RIRS), ureterorenoscopy (URS) and laparoscopy for renal and ureteric stones, and per urethral and percutaneous cystolithoclast (PUCL/PCCL) for vesical calculi [14]. In developed countries, over 95 % of patients are managed by MIS. Although our experience is similar, we still treat 28 % of patients with open surgery. The main reasons for this, besides anatomical abnormalities, are complex and large stones with atrophic cortices (Fig. 30.7), neglected stones with renal failure, and/or sepsis. Furthermore, many patients come from far-off places where repeat visits are not possible. This compels us to perform the maximum possible clearance in one go with open surgery, with the shortest possible stay in hospital. From 2009 to 2012, 3,434 surgical procedures for stone disease were carried out on 2,861 patients, with a mean age of 6.5 ± 3.5 years (range 2 months to 15 years) (Table 30.3) [19].

Stone burden: large stones at multiple sites
6.2.2.1 Minimally Invasive Surgery: Our Experience
6.2.2.1.1 Extracorporeal Shock Wave Lithotripsy (ESWL)
Since the first clinical report of ESWL in children by Newman et al in 1986, large size stones and even staghorn calculi have been treated with ESWL [11, 20]. Stone-free rates range from 44 to 84 % in different series but these data are difficult to interpret because of discrepancies in the available data with regard to the number of shock waves administered, retreatment rates, stone-free status, and size of residual fragments. ESWL outcome depends on type of lithotripter, operator skills, ESWL protocol used, stone characteristics including location, size, multiplicity, and composition [21].
Our initial experience with ESWL published in 2003, was very satisfactory and showed a stone-free rate of 84 %, with a mean 1.4 sessions given to a stone size ranging from 1.5 to 2.5 cm [11].
In a recent audit of our pediatric renal stones treated with ESWL, we analyzed clearance with renal units treated with ESWL in different stone positions and stone load. In the single stone group of 158 renal units with mean size of 10 ± 2.5 mm, 121 renal units (76 %) cleared in a single session, and 21 units cleared in the second session, giving an overall clearance rate of 89 % in a mean of 1.14 sessions.
In the second group of 58 units comprising multiple stones having a mean size of 17 ± 5.3 mm, 46 % (27 units) cleared in a single session, 32 %(19 units) cleared in the second session, and 7 % (4 units) cleared in the third session, giving an overall clearance rate of 86 % in a mean of 1.54 sessions. These results showed an increase in mean ESWL sessions with an increase in stone burden.
The relationship between stone location and clearance showed that the best clearance rates following a single session of ESWL were found for the upper calyx (87 %) and pelvis (84 %), and the poorest for the lower calyx (67 %). The mean numbers of sessions required for clearance in the upper calyx, pelvis, and middle calyx were 1.1, 1.2, and 1.3, respectively, as compared to the figure for the lower calyx of 1.5.
In a small study of 58 renal units, where we assessed the relationship between the stone densities i.e. hounsefield unit (HU on NCCT) and ESWL, the outcome showed that a lower HU is associated with good clearance for the same size of stone.
ESWL in the pediatric population is carried out under general anesthesia to minimize pain and stone mobility. To avoid repeated anesthesia and to allay the concern of renal damage in the developing kidney and hypertension, we limit our patient population for ESWL to only those cases where complete clearance is expected in a single session. We therefore recommend a maximum stone size of 1.5 cm for a renal stone and, as the lower calyceal anatomy hinders clearance of a stone, a size of 1 cm for lower calyceal stones being managed by ESWL.
6.2.2.2 Percutaneous Nephrolithotomy (PCNL)
Fernström and Johansson (1976) reported the first case of PCNL carried out in an adult [22]. Its safety and efficacy in the adult population is well established. Parenchymal damage, radiation exposure in children with its effect on the growth of the child, bleeding, and risk of sepsis were serious considerations in the pediatric age group. Woodside and associates in 1985 were the first to present PCNL in the pediatric population with adult instruments [23]; we also initially started off with adult sized instruments.
Miniaturization of the PCNL instruments have facilitated its use in all age group. We usually use a nephroscope of 15, 18, and 20 Fr for PCNL. We have successfully performed more than 1,600 PCNL in children with a mean age of 7.4 ± 3.41 years, 35 % of whom were up to 5 years of age and 10 % were less than 2 years of age.
Although instruments as small as 11 Fr “Mini-Perc” have been reported to be used [24], they go on to the other side of the spectrum and are only for selected cases. Minimal tract dilatation decreases blood loss, allows for increased maneuverability of the instruments, and leads to shorter hospital stays. However, use of these pediatric nephroscopes has to be individualized on the basis of stone location and burden to balance the benefits of small scopes against the concerns of impaired visualization, limitation with the size of grasping forceps, lower irrigation fluid flow, and prolonged operative time.
Our indications for PCNL are stone sizes of 1.5 cm or more with favorable anatomy, previous open surgery on the respective side, failed ESWL, or stones where more than one session of ESWL is expected. All the patients should undergo the proposed evaluation mentioned earlier. Active or untreated UTIs, sepsis, and bleeding diathesis are the few contraindications which should be mentioned. Spinal deformity such as scoliosis and kyphosis should be elucidated prior to surgery.
PCNL is carried out under general anesthesia, and operative considerations include negative urine culture, prophylactic antibiotics, proper draping, isotonic irrigation fluid at body temperature to avoid hypothermia and hyponatremia, and short operative time. The patient is placed in a lithotomy position first for the placement of a ureteric catheter, and then turned prone, taking care of the pressure points and ventilation.
The puncture site is chosen on the basis of the stone location, bulk, and pelvicalyceal anatomy. We prefer subcostal posteriosuperior calyceal punctures when suitable, as this gives access to the majority of the calyces with little torque on the kidney, and also allows access to the pelviureteric junction and lower calyces in the case of stone migration.
In certain situations, the supracostal approach also has be utilized with marginal risks of hydropneumothorax, which can also be avoided in experienced hands.
The procedure involves puncturing of the collecting system through the fornix, along the direction of the infundibulum, to avoid blood vessels adjacent to the infundibulum under ultrasonography or fluoro guidance using C-arm. We occasionally make multiple tracts to clear stones in inaccessible calyces or blind calyces (Table 30.4).
At our center we use an ultrasonic burr and pneumatic lithoclast for stone fragmentation, both being cost effective and reusable (Fig. 30.8). They are used either alone or in combination, depending on the size and hardness of the stone. The holmium:YAG laser is only occasionally used, with deflecting flexible nephroscope, where the stone is found at an acute angle or in calyceal diverticulum with narrow infundibulum. Electrohydraulic Lithoclast (EHL) is known to be very traumatic and therefore has not been used at our centre. We ensure complete stone clearance by checking both fluoroscopically and endoscopically (Fig. 30.9).

Instruments used for PCNL in children

PCNL in progress
Tubeless PCNL has been performed in cases with no significant bleeding, pelvicalyceal breach, and residual fragments. However, we prefer to place a 10–16 Fr nephrostomy tube postoperatively in the majority of our cases for safety reasons.
The variety of stones managed at our center with PCNL range from single pelvic or calyceal stones to partial or complete staghorn stones.
For the purpose of evaluating the results of our PCNL, we divide our stone burden into simple (81 %) and complex (19 %) stones. Simple stones (mean stone burden 2.7 ± 1.5 cm2) were single stones in the pelvis or calyx or pelvic stones with a single calyceal stone. Complex stones (mean stone burden 5.0 ± 5.8 cm2) were staghorn, partial staghorn, or stones in the pelvis with two or more calyces. The success rate of PCNL as monotherapy is higher in simple stones (89 %) than in complex stones (71.5 %). Those with residual stones required retreatment with Re-PCNL, ESWL, or URS, and stone clearance increased to 95 % in simple stones and 86 % in complex stones.
Preoperatively, patients’ mean hemoglobin was 11.1 gm/dl. Of our patients, 14 % required blood transfusion, more in complex stone cases, where more manipulation was carried out.
Our mean operative time was 64.9 min for simple and 92 min for complex stones. Our mean hospital stay was 4.1 ± 3 days. Our patients tend to overstay in hospital as they come from far-off areas, where follow-up facilities are not available.
Conversion to open surgeries (2.6 %) occurred in the early phase of our learning curve. Post-operative complications include hydrothorax in 2 % and urosepsis in 1.6 %, while intraperitoneal and perirenal collections are seen in 1.5 % of cases.
The post-operative effects on renal functions have been evaluated by measuring creatinine levels in all cases and by DMSA scans in selected cases. We did not find any significant deterioration in renal function post-operatively.
To conclude, PCNL is a safe and effective method of renal stone management in all age groups, with acceptable complication rates.
6.2.2.3 Ureterorenoscopy (URS) and Retrograde Intrarenal Surgery (RIRS)
Ureterorenoscopy and retrograde intrarenal surgery have become the standard urological techniques [14, 18, 25]. They have various diagnostic and therapeutic indications, and their main use is in the management of urolithiasis. The first ureteroscopy was performed in 1912 by Hugh Hampton Young. The first URS in children was performed by Ritchy and colleagues in 1988. With the development of fiber optics, miniaturization of the instruments took place, and thereby semi-rigid and flexible ureteroscopes were developed.
Ureterorenoscopy with a holmium YAG laser is the mainstay of treatment of ureteric stones at our institute. Semi-rigid ureterorenoscopes of size 4.5/6, 6/7.5, and 8/9.8 Fr are used depending on the age and anatomy of the patient and size of the stone, considering the therapeutic requirements. The semi-rigid ureteroscopes are more durable, can access the whole ureter even as far as the PCS, and have better visibility, faster irrigation flow, and larger working channels. In contrast, banding may be difficult and, with large psoas muscles, access to the upper ureter may be limited in comparison to flexible ureteroscopes, which we use infrequently because they are fragile and expensive. The deflectable tip of the flexible scopes is more suitable for retrograde intrarenal surgery.
After complete workup we perform URS under general anesthesia in the lithotomy position with antibiotic prophylaxis and negative urine culture. First a cystoscopy is performed, and a safety guide/glide wire is placed in the ureter under fluoroscopic guidance. Usually no ureteric (VUJ) dilatation is needed, but, in cases where we cannot negotiate the smallest of the scopes (4/6.5 Fr), we use plastic dilators over a guide wire to dilate the ureteric orifice or place a DJ stent for 2–3 weeks, which relieves obstruction and dilates the ureter for the subsequent session of stone fragmentation. Balloon dilatation is not used at our center, being controversial in children and very expensive. Isotonic saline is used at body temperature as an irrigation fluid, and may be used for hydrodilatation of VUJ with caution, taking care to prevent any stone fragment migration and extravasation.
We do not use ureteral access sheaths, which are used with flexible URS to aid in repeated entry into the ureter. The smallest diameter available is 9 Fr, which is too big for our patients.
EHL is too traumatic and cannot be used with small size URS. The pneumatic lithoclast is cost effective, but can only be used with minimum 7 Fr scopes. We use a pneumatic lithoclast in older children with large or hard stones.
Our mainstay of stone disintegration and fragmentation has been the holmium YAG laser, which has revolutionized pediatric ureteric stone management because of its safety and effectiveness in fragmentation of all stone compositions in all age groups, including infants. Its safety is ensured, as most of the laser energy is absorbed by the irrigation fluid, and thus does not damage the ureteric mucosa if the laser fiber is in line with the ureter and not in close proximity to the ureteric wall (0.5–1.0 mm). It produces a photothermal and photomechanical effect, resulting in vaporization of the stone. Typically, 200- to 400-μm fibers are utilized during ureteroscopy. The energy is mostly absorbed by the irrigating solution and the incident angle is kept constant.
We have used the Ho:YAG laser in our patients with a mean age of 6.8 ± 3.5 years, 40 % being less than 5 years of age. Our mean stone size was 8 mm (4–20 mm). The majority (80 %) is in the distal ureter with a stone free rate of 82 % in a single session and 98 % in two sessions. The complications with URS and stone disintegration include extravasation in 2.5 %, UTI in 5 %, and hematuria in 10 %.
7 Stones with Renal Failure
About 15–20 % of our pediatric stone patients present with renal dysfunction. There are two major groups of patients presenting with this:
-
First group: calculus oligo – anuric with two good kidneys or a solitary good/normal functioning kidney, which becomes acutely blocked with bilateral renal and/or mostly ureteric stones. Usually these children are younger with a mean age of 4.3 ± 2.9 years.
-
Second group: chronic calculus renal failure group, who have been harboring stones for a long period; these stones have slowly and gradually affected/damaged the kidney permanently or irreversibly because of associated chronic obstruction leading to ischemic cortical atrophy, with infection on top of this. Most of these children are in renal dysfunction for extended periods, affecting their body metabolism and growth. Many present with extremes of disease with osteodystrophy, anemia, and severe malnutrition. These children are older than those with calculus oligo/anuria, with mean ages of 6.9 ± 3.4 years.
The majority (89 %) of these patients are from poor socioeconomic backgrounds, 66 % coming from rural areas, and live far away from our health facility, with a mean travel distance of 160 ± 45 km. They therefore present late with advanced uremia, sepsis, fever, tachypnea, and respiratory distress because of fluid overload and or severe acidosis and hyperkalemia.
The initial management in many of these patients requires resuscitation, ventilatory support, and multidisciplinary intensive care management, with immediate imaging, peritoneal or hemodialysis.
Management of the calculus anuria group after evaluation is by placement of the JJ stent under general anesthesia within a few hours of their presentation. There are 24-h services for anesthesia, pediatric nephrology, and urology. This is considered to be the best form of management for these patients, as JJ placement results in relief of obstruction and urine formation. Those who cannot have a JJ stent, and have some plevicalyceal dilatation, are treated by placement of percutaneous nephrostomy.
After evaluation, the chronic calculus renal failure group undergoes immediate management with temporary angio access with double lumen catheter, hemodialysis, and some with peritoneal dialysis. In the calculus anuria group, 90 % of patients had complete recovery of renal function, compared to 54 % in the chronic calculus renal failure group, whereas there was partial recovery in 7 % of the first group and 17 % in the chronic calculus renal failure group. In the chronic calculus renal failure group, no recovery of renal function is observed in 21 %, of which 14 % are on hemodialysis, and 7 % underwent renal transplantation.
References
Shattock JG (1905) A pre- historic or pre- dynastic Egyptian calculus. Trans Pathol Soc Lond 61:275
Desnos E (1914) The history of urology. Murphy LJT (trans and ed). Paris, Doinlet Fits, pt.1
Dimopoulos C, Gialas A, Likourinas M, Androutsos G, Kostakopoulos A (1980) Hippocrates: founder and pioneer of urology. Br J Urol 52(2):73–74
Baştuğ F, Düşünsel R (2012) Pediatric urolithiasis: causative factors, diagnosis and medical management. Nat Rev Urol 9(3):138–146
Sarica K (2006) Pediatric urolithiasis: etiology, specific pathogenesis and medical treatment. Urol Res 34(2):96–101
Bakane BC, Nagtilak SB, Patil B (1999) Urolithiasis: a tribal scenario. Indian J Pediatr 66(6):863–865
McCarrison R (1931) A lecture on the causation of stone in India. Br Med J 1(3675):1009
Sharma AP, Filler G (2010) Epidemiology of pediatric urolithiasis. Indian J Urol 26(4):516–522
Romero V, Akpinar H, Assimos DG (2010) Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol 12(2–3):e86
Rizvi SAH, Naqvi SAA, Hussain Z, Hashmi A, Hussain M, Zafar MN, Sultan S, Mehdi H (2002) Pediatric urolithiasis: developing nation perspectives. J Urol 168(4):1522–1525
Rizvi SAH, Naqvi SAA, Hussain Z, Hashmi A, Hussain M, Zafar MN, Sultan S, Mehdi H (2003) Management of pediatric urolithiasis in Pakistan: experience with 1,440 children. J Urol 169(2):634–637
Rhodes C, Churchill D, Hulton SA (2005) Antenatal diagnosis of fetal renal calculus. Ultrasound Obstet Gynecol 25(5):517–518
Tannous RJ, Solhaug MJ, Bogdan D, Abuhamad AZ (2000) Prenatal diagnosis of fetal nephrolithiasis. Ultrasound Obstet Gynecol 15(4):331–332
Gnessin E, Chertin L, Chertin B (2012) Current management of paediatric urolithiasis. Pediatr Surg Int 28(7):659–665
Rizvi SA, Sultan S, Zafar MN, Ahmed B, Faiq SM, Hossain KZ, Naqvi SA (2007) Evaluation of children with urolithiasis. Indian J Urol 23(4):420–427
Kovacevic L, Wolfe-Christensen C, Edwards L, Sadaps M, Lakshmanan Y (2012) From hypercalciuria to hypocitraturia—a shifting trend in pediatric urolithiasis? J Urol 188(4):1623–1627
Hamill PVV, Drizd TA, Johnson CL, Reed RB, Roche AF, Moore WM (1979) Physical growth: National Center for Health Statistics percentiles. Am J Clin Nutr 32(3):607–629
Raju GA, Norris RD, Ost MC (2010) Endoscopic stone management in children. Curr Opin Urol 20(4):309–312
Rizvi SA, Sultan S, Ijaz H, Mirza ZN, Ahmed B, Saulat S, Naqvi SA (2010) Open surgical management of pediatric urolithiasis: a developing country perspective. Indian J Urol 26(4):573
Lottmann HB, Traxer O, Archambaud F, Mercier-Pageyral B (2001) Monotherapy extracorporeal shock wave lithotripsy for the treatment of staghorn calculi in children. J Urol 165(6):2324–2327
Jeong U, Lee S, Kang J, Han DH, Park KH, Baek M (2013) Factors affecting the outcome of extracorporeal shock wave lithotripsy for unilateral urinary stones in children: a 17-year single-institute experience. Korean J Urol 54(7):460–466
Fernström I, Johansson B (1976) Percutaneous pyelolithotomy. A new extraction technique. Scand J Urol Nephrol 10(3):257–259
Woodside JR, Stevens GF, Stark GL, Borden TA, Ball WS (1985) Percutaneous stone removal in children. J Urol 134(6):1166–1167
Jackman SV, Hedican SP, Peters CA, Docimo SG (1998) Percutaneous nephrolithotomy in infants and preschool age children: experience with a new technique. Urology 52(4):697–701
Wang AJ, Preminger GM (2011) Modern applications of ureteroscopy for intrarenal stone disease. Curr Opin Urol 21(2):141–144
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag Italia
About this chapter
Cite this chapter
Sultan, S. (2015). Urolithiasis. In: Lima, M., Manzoni, G. (eds) Pediatric Urology. Springer, Milano. https://doi.org/10.1007/978-88-470-5693-0_30
Download citation
DOI: https://doi.org/10.1007/978-88-470-5693-0_30
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5692-3
Online ISBN: 978-88-470-5693-0
eBook Packages: MedicineMedicine (R0)