
Abstract
Acute knee dislocations, though uncommon, are among the most serious injuries encountered by the orthopedic surgeon. Many knee dislocations spontaneously reduce prior to presentation to the hospital; thus, a keen understanding of the characteristic injury mechanism and a high clinical suspicion are necessary to appropriately identify and treat this patient population. Once a knee dislocation is identified, the physical examination of the affected lower extremity is crucial to delineate the extent of the osseous and soft tissue injury, as well as prevent limb-threatening neurovascular complications. Appropriate diagnostic testing should assist in guiding immediate and delayed treatment. Neurovascular and open injuries should be addressed immediately, while fractures should be stabilized early in the post-dislocation period. There is no consensus regarding the most appropriate treatment for the multiligamentous injury that accompanies a knee dislocation. Injury pattern, patient-specific factors, and surgeon factors should all be considered when treating the ligamentous injuries associated with a knee dislocation. This chapter provides a comprehensive review of the literature alongside our current approach to the management of the acute knee dislocation and the associated multiligamentous knee injury.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Anterior Cruciate Ligament
- Anterior Cruciate Ligament Reconstruction
- Knee Flexion
- Posterior Cruciate Ligament
- Medial Collateral Ligament
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
14.1 Introduction
Acute knee dislocations are infrequent injuries; however, the sequelae may be quite severe and potentially limb threatening. Furthermore, the incidence of acute knee dislocations has been rising. The increased incidence may be a by-product of escalated involvement in contact athletics coupled with an increased participation in nontraditional sporting and recreational activities such as the riding of motorbikes, snowmobiles, and all-terrain vehicles. Although there is a rise in the incidence of knee dislocations, there is a lag in high-level-of-evidence studies from which a consensus statement on the treatment of these injuries may be derived. However, from the available prospective studies and systematic reviews in conjunction with our senior author’s expert opinion, we have compiled this guide to the treatment of the acutely dislocated knee.
14.2 Definition
The definition of a knee dislocation is most simply the complete disruption of the tibiofemoral articulation. Following the acute event, the knee may spontaneously reduce or it may remain dislocated. The dislocation event is always coupled with a multiligamentous knee injury of variable degree. The definition of a multiligamentous knee injury is the rupture of two or more of the major ligaments/ligamentous complexes of the knee: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), medial collateral ligament (MCL), posteromedial corner (posterior oblique ligament, semimembranosus expansions, oblique popliteal ligament; PMC), lateral collateral ligament (LCL), or posterolateral corner (LCL, popliteus, and popliteofibular ligament; PLC). Most commonly, an acute dislocation results in rupture of both cruciates (ACL and PCL) and one additional ligamentous structure [1–5]. Less frequently, but described in the literature, is the occurrence of an acute knee dislocation with a resultant ligamentous injury that spares the PCL, the so-called PCL-intact knee dislocation [4, 6, 7].
14.3 Epidemiology and Mechanism
Knee dislocation is a relatively rare injury, constituting 0.02–0.2 % of all orthopedic injuries [8–11]. However, some authors suggest the incidence of knee dislocation may be significantly higher because the vast majority of dislocations spontaneously reduce prior to hospital presentation. The patient demographic tends to be young males, with a male-to-female ratio of 4 to 1. These injuries are most frequently (50 %) caused by a high-velocity mechanism such as a motor vehicle accident, motorcycle collision, or all-terrain vehicle. One of the most typical mechanisms of dislocation in the high-energy cohort is a posteriorly directed force on the tibia as it strikes the dashboard or steering wheel during a crash [1, 12]. High-energy knee dislocations are present as a component of the polytraumatized patient in 14–44 % of cases. Although the likelihood of bilateral knee dislocations is quite low at 5 %, the rate of open injury associated with a knee dislocation ranges from 5 to 17 % in the literature [13].
An additional one-third of knee dislocations are secondary to low-velocity sports injuries, while one-tenth of all dislocations are due to a fall [14]. Shelbourne presented a case series of low-velocity knee dislocations secondary to football, wrestling, and running injuries [14]. The characteristic mechanism of injury in the athletic knee dislocation is a contact or collision that forces the knee into hyperextension combined with excessive varus or valgus force. It is important for the team physician to distinguish this mechanism from that of an isolated ACL rupture, which is typically sustained via a noncontact injury mechanism. An additional mechanism of injury, as described in the literature, is the “spontaneous” dislocation in the morbidly obese patient [15, 16].
14.4 Classification
The original knee dislocation classification system was proposed by Kennedy in 1963 and was purely descriptive in nature based upon the direction of the dislocation [12]. The five categories based on direction were anterior, posterior, medial, lateral, and rotatory. Based on direction, anterior dislocation is the most common followed by posterior dislocation. Rotatory dislocation is the least common [12, 17]. A limitation of this system was that it could not be used in cases of dislocation followed by spontaneous reduction. Schenck proposed a modified classification system that accounts for the pattern of injury and is thus anatomically based (Table 14.1) [18]. The anatomic classification of knee dislocations helps to guide treatment and provides a “common language” to compare outcomes for different injury patterns and across different studies in the literature.
14.5 Initial Evaluation and Management
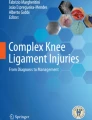
Identification of a knee dislocation is relatively easy if the knee remains dislocated at the time of presentation; however, a high index of suspicion is necessary in cases of dislocation followed by spontaneous reduction in the field. The clinician should be highly suspicious for knee dislocation if there is misalignment of the affected lower extremity, deformity of the knee, massive soft tissue swelling, or disproportionate pain (Fig. 14.1a). The absence of a joint effusion may be a misleading and false sense of comfort as high-energy dislocations can result in capsular damage, which will allow the knee effusion to diffuse into the surrounding soft tissue.

(a) Anteroposterior and (b) lateral radiographs demonstrating an anterior knee dislocation. (c) Anteroposterior and (d) lateral radiographs demonstrating an adequate reduction of previous anterior knee dislocation
Patients presenting with knee trauma should be treated like any other traumatized patient, and the first step should always be implementation of the Advanced Trauma Life Support (ATLS) protocol [19]. Following ATLS protocol, and assuming the patient is without more pressing injuries, a dislocated knee should be reduced. In cases of high-energy knee dislocations, a portable “spot shot” radiograph of the knee should be taken prior to reduction to confirm the absence of major fractures. If fractures of the distal femur or proximal tibia are present, the clinician may opt to reduce the knee if the fractures appear relatively stable. In cases of low-energy trauma, such as knee dislocations sustained on the playing field, immediate reduction should be attempted prior to imaging studies. Post-reduction radiographs should always be obtained to confirm a concentric reduction of the tibiofemoral articulation (Fig. 14.1b). The knee should be initially inspected for any evidence of an open injury that would necessitate a formal irrigation and debridement in the operating room.
14.6 Vascular Evaluation and Management
Following confirmed reduction of the knee, a thorough vascular examination should be completed. The incidence of popliteal artery injury associated with knee dislocation has been reported to range from 4.8 to 65 %, with posterior knee dislocations having the highest rate of injury [8, 20, 21]. Vascular injuries are not solely associated with high-energy knee dislocations. Low-energy and spontaneous knee dislocations can cause vascular occlusion or intimal tearing [17, 22]. This examination should begin with inspection of the color, temperature, and capillary refill of the affected leg. Distal arterial flow in the dorsalis pedis, posterior tibial, and peroneal arteries should be interrogated first manually and secondarily with Doppler ultrasound if necessary. The clinician should be cognizant that a normal physical examination and palpable distal pulses do not exclude serious vascular injury, such as an intimal tear to the popliteal artery [23]. The ankle-brachial index (ABI) should be calculated using Doppler ultrasound and a blood pressure cuff if there is any concern for the vascular status. The ratio of systolic blood pressure in the affected ankle is compared to the unaffected upper arm. In a knee dislocation cohort, Mills reported 100 % sensitivity, specificity, and positive predictive value of a significant arterial injury requiring surgical attention if the ABI is below 0.90 [23]. Absent pulses or diminished ABIs are indications for involvement of a vascular surgeon. It is important to involve vascular surgery colleagues in an expeditious fashion, as warm ischemia time of greater than 6–8 h is associated with a higher rate of amputation [17, 24]. Additional studies or interventions that are frequently requested by a vascular surgeon include computed tomography angiogram (CTA) and formal angiography (Fig. 14.2). An abnormal CTA will necessitate a formal angiogram with either endovascular or open vascular intervention. At our institution a formal angiogram with or without intervention is accompanied by external fixation performed by an orthopedic surgeon to stabilize the knee, provide access for additional vascular procedures (the external fixation eliminates the need for a splint), and permit serial examinations of the affected limb postoperatively.

Representative angiogram demonstrating lack of significant distal flow beyond the popliteal hiatus (popliteal artery) secondary to a knee dislocation. Arrow indicates significant obstruction
14.7 Neurologic Evaluation and Management
The incidence of nerve injury with acute knee dislocation is approximately 20 % [12, 25]. The most commonly injured nerve is the common peroneal nerve rather than the tibial nerve. The explanation for the higher incidence of peroneal nerve injury is its anatomic course adjacent to the proximal fibula, the decreased compliance compared to the tibial nerve, and the mechanism of knee dislocation. Lateral and posterolateral dislocations can significantly stretch the peroneal nerve. To identify these injuries, the clinician should perform an initial tactile exam of the patient’s sensation in all nerve distributions of the lower extremity. Graded motor strength with ankle dorsiflexion, ankle plantar flexion, ankle inversion, ankle eversion, and great toe dorsiflexion should be documented. There is no acute treatment for neurologic deficits following knee dislocation, and the overall prognosis for neurologic recovery remains low [26]. Chronic neurologic injuries such as foot drop may be treated with an ankle foot orthosis or a posterior tibial tendon transfer.
14.8 Ligamentous Evaluation
A thorough ligamentous examination should be performed on all patients with a suspected knee dislocation. The initial examination may be limited due to pain, hematoma, or associated injuries; however, gross laxity or instability should be documented to the best of the examiner’s abilities. It is important for the examiner to comment on the integrity of the main ligamentous stabilizers, including the ACL, PCL, MCL, LCL, and PLC. A brief review of the basic ligamentous examination is presented here.
The anterior drawer and Lachman examinations are performed to evaluate for laxity in the ACL, the latter of which is considered the more accurate maneuver [27]. Both examinations grade the magnitude of anterior-posterior (A-P) translation of the tibia in relation to the femur and the presence or absence of a firm endpoint of that motion. The presence of an ACL tear is typically apparent due to increased translation and a lack of a firm endpoint compared to the contralateral knee. A caveat for these maneuvers in the setting of an acute knee dislocation is that it may be difficult or impossible to flex the affected knee to 90° to perform the anterior drawer test secondary to pain, swelling, or fracture. In addition, both examination maneuvers take advantage of the normal anatomic resting position of the tibia in relation to the femur as the “starting point” for the examination of the magnitude of A-P translation. Typically the tibia lies anterior to the femur; however, if the PCL is disrupted, the tibial “starting point” may be translated posteriorly rendering the motion appreciated difficult to associate with ACL laxity rather than PCL laxity.
The third ACL examination maneuver is the pivot-shift test. This is the senior author’s preferred test for grading ACL laxity during an examination under anesthesia; however, it is difficult to perform on the awake patient due to the inability to control hip and leg position. In addition, the pivot-shift test requires an intact iliotibial band (ITB) for accurate results. In the acute knee dislocation, there may be tearing or disruption of the ITB. Lastly, pain, swelling, and fracture are additional reasons this examination maneuver may be difficult to perform in the setting of an acute knee dislocation.
The PCL may be evaluated by assessing the posterior sag and the posterior drawer. The posterior sag test, performed with the knee and hip flexed to 90°, evaluates the position of the proximal tibia in relation to the distal femoral condyles. In the presence of a PCL tear, the proximal tibia will sag (posterior translation) relative to the distal femoral condyles as compared to the contralateral side. The posterior drawer test is performed in 90° of flexion by applying a posteriorly directed force on the proximal tibia with the thumbs on the joint line to quantify the distance of posterior translation. A grade III injury (greater than 10 mm of posterior translation) indicates a combined PCL and PLC injury [28].
Collateral ligament testing is performed with valgus (MCL) and varus (LCL) force on the knee. The testing is performed with the knee in 30° of flexion to isolate the collateral ligaments. The test is then repeated in full knee extension. Laxity at both 30° of flexion and full extension suggests disruption of additional structures. On the lateral side, laxity with varus stress in full extension suggests injury to the cruciate ligaments and the PLC in addition to the LCL [29]. On the medial side, laxity with valgus stress in full extension suggests injury to the cruciate ligaments and medial capsule in addition to the MCL.
The PMC is examined with maneuvers that place external rotation stress with the knee in various degrees of flexion. These tests help define the degree of anteromedial rotatory instability. The most common test is performed with the knee in 30° of flexion. A valgus stress is imposed while the foot is externally rotated [30, 31]. If this test elicits an increase in anteromedial external rotation as compared to the contralateral side, then a PMC injury has been sustained. In addition, if a combined PMC-PCL injury has been sustained, the magnitude of posterior translation of the tibia in the posterior drawer test will be exaggerated or unchanged with internal rotation of the tibia. In a PCL-deficient knee with an intact PMC, the magnitude of posterior tibial translation with the tibia internally rotated during the posterior drawer will be diminished [32, 33].
The PLC can be directly assessed with the dial test. The structures interrogated with this test include the LCL, popliteus tendon, and popliteofibular ligament [34]. With the patient prone, the knees are flexed to 30° and a symmetric, external rotation force is placed on both feet. The thigh-foot angle is measured and the test is again repeated at 90° of knee flexion. A difference in thigh-foot angle of greater than 10° side to side is considered a positive test. An increased thigh-foot angle at 30° of knee flexion but not at 90° is consistent with an isolated PLC injury, while increased thigh-foot angle at both 30 and 90° of knee flexion is consistent with a combined PCL and PLC injury. An isolated increase in thigh-foot angle at 90° of knee flexion suggests an injury to the PCL. The examiner should also be aware that increased thigh-foot angle rotation at 30 and 90° of knee flexion may signify an injury to the anteromedial aspect of the knee rather than the PLC [35].
14.9 Diagnostic Imaging
Radiographs of the knee in two planes (anteroposterior and lateral) should be performed to characterize the direction of dislocation (Fig. 14.1a, b). Initial radiographs are also important to assess for associated fractures, either large osseous injuries to the tibial plateau and distal femur or subtle fractures such as a Segond fracture or PCL avulsion. As mentioned previously, in low-velocity knee dislocations (sports injuries), a reduction should be attempted prior to the initial radiographs and ideally on the field if trained medical personnel are present. This is due to the low likelihood of significant fractures. However, in high-velocity knee dislocations (e.g., automobile accidents), the likelihood of significant fractures is much greater and thus plain radiographs should be performed prior to a reduction attempt. In either scenario, post-reduction radiographs should be obtained to confirm a concentric reduction (Fig. 14.1c, d). If there is concern for a PCL injury, stress radiographs of the bilateral knees may be performed with the knees flexed 80° and weight applied to the anterior tibia [36]. Stress radiographs may be more appropriate in the preoperative planning phase rather than acutely following a knee dislocation.
Once the knee is stabilized and vascular injuries have been ruled out, a computed tomography (CT) scan may be appropriate if fractures are present, and a magnetic resonance image (MRI) should be obtained to assess the extent of the ligamentous injury (Fig. 14.3). The MRI will also assist with preoperative planning in the case of damage to the chondral surfaces, menisci, and capsule. Bone bruising is common following acute knee dislocation and present 75 % of the time [37], while 25 % of knee dislocations have concomitant meniscal injuries [37]. Furthermore, if fractures accompany the knee dislocation, the timing of MRI is crucial. Obtaining an MRI in the early phase of treatment, prior to open reduction and internal fixation of fractures, facilitates evaluation of ligamentous integrity without being obscured by the signal artifact of implanted hardware.

(a) Sagittal magnetic resonance image (MRI) with arrow demonstrating complete disruption of the anterior cruciate ligament. (b) Sagittal MRI with arrow demonstrating complete disruption of the posterior cruciate ligament. (c) Coronal MRI with arrow demonstrating disruption of the lateral collateral ligament and posterolateral corner. (d) Coronal MRI with arrow demonstrating disruption of the medial collateral ligament
14.10 Initial Treatment
The initial care for a knee dislocation is dictated by a number of factors, including the open injury status, neurovascular status, fracture status, and ability to reduce the knee. If the dislocation is reduced, there is no fracture or open injury, and there is no concern for neurovascular compromise, then initial treatment may consist of a long-leg splint in 20° of knee flexion, lower extremity elevation, and serial neurovascular examinations. Twenty degrees of knee flexion is classically taught as the position for long-leg splinting; however, it is our experience that maintaining the knee in flexion for more than 3–5 days may compromise the ability to restore full extension long term. The treating surgeon should be cognizant of this during the initial management. If the knee dislocation is complicated by significant femoral condyle or tibial plateau fractures, an open injury, or a vascular injury or the knee is irreducible, then the complicating factor should be addressed in the operating room. Each of these complicating factors should also prompt the treating surgeon to consider concomitant application of external fixation rather than a splint at the conclusion of the operating room session. Stabilization of the dislocated knee with external fixation should also be considered in cases initially treated in a splint but with post-splinting films that demonstrate persistent tibiofemoral subluxation. Two important considerations when placing an external fixator following knee dislocation are that the hardware should be MRI compatible and the knee-spanning pins should be safely outside the knee joint and sufficiently away from future graft tunnel or fixation hardware sites. This “safe zone” for pin placement is roughly 10 cm proximal and distal to the knee joint line [38]. Lastly, if there is any clinical concern for compartment syndrome preoperatively or intraoperatively, the treating surgeon should have a low threshold for performing fasciotomies.
14.11 Definitive Treatment Considerations
Historically, the mainstay of knee dislocation definitive treatment was immobilization in plaster casts. However, as longitudinal clinical studies emerged, it became clear that patients sustaining knee dislocations and undergoing nonoperative treatment went on to develop persistent knee instability and had poor long-term functionality [39–42]. Recent studies suggest considerable benefit from surgical treatment [12, 21, 39, 41–45]. A recent systematic review comparing operative versus nonoperative treatments for multiligament knee injuries found significantly higher International Knee Documentation Committee (IKDC) scores, improved return-to-work rate, and higher rates of return to sport for patients in the cohort that underwent surgical treatment [44]. Dedmond and Almekinders [39] performed a meta-analysis of differences between operative and nonoperative treatment of acute knee dislocations. They evaluated 74 nonoperatively and 132 operatively treated knee dislocations and found significantly improved Lysholm scores in the surgically managed cohort as compared to the cohort treated nonoperatively [39]. Several other studies have corroborated these findings by comparing return to sport following acute knee dislocation and demonstrated higher success rates in those undergoing surgical reconstruction [45, 46].
14.12 Nonoperative Treatment
Despite the emerging clinical evidence that favors operative rather than nonoperative definitive care, there are some instances in which the treating clinician should opt for nonoperative management. Polytraumatized or significantly injured patients with multiorgan system injuries should not be indicated for surgery until they are able to participate in postoperative rehabilitation. Patients with open injuries and inadequate soft tissue coverage in which there are concerns for wound healing should not be indicated for surgical reconstruction. The low functional demand and morbidly obese patient populations will likely have better outcomes with nonoperative rather than operative treatment. Lastly, patients who wish to pursue nonsurgical treatment should be counseled on the pros and cons of both surgical and nonsurgical care and ultimately have their wishes granted if they choose nonoperative management.
14.13 Surgical Treatment
The objective of definitive surgical management following an acute knee dislocation is to provide a stable joint and ideally return the patient to his or her preoperative activity level. While the objective is clearly defined, there is considerable debate concerning several surgical factors, including timing of surgery, surgical approach, ligamentous repair versus reconstruction, and technique of reconstruction.
14.13.1 Timing of Surgery
The timing of surgery can be broadly classified as early (within the first 2–3 weeks following injury) or delayed (greater than 3 weeks from the time of injury). A third broad classification is a staged approach in which the medial and lateral structures are repaired or reconstructed with or without PCL reconstruction in the early window followed by delayed ACL reconstruction if deemed necessary. Although not universally implemented, the staged approach is still in practice and has been advocated by a number of authors [11, 47]. Currently, most knee surgeons advocate early surgical intervention, and this approach is widely supported by the literature [41, 44, 48, 49]. Harner reported on the subjective and objective outcomes of 31 knee dislocations, 19 of which underwent acute reconstructions [41]. Their cohort of acutely treated patients reported higher subjective scores and had increased stability compared to the delayed cohort. Conversely, authors have also reported favorable outcomes utilizing a delayed approach to ligamentous reconstruction [50–54]. Mook and colleagues performed a systematic review of multiligamentous knee injuries treated with early, late, or staged reconstructions [50]. Their analysis suggested that delayed reconstruction had the advantage of lower rates of postoperative stiffness while performing comparable to early and staged procedures in terms of knee stability. Ultimately, the decision to proceed with acute or delayed reconstruction should be based on patient-specific factors and the surgeon’s comfort level with the various surgical techniques. Lastly, regardless of the decision to operate in the early or delayed postoperative window, the surgeon should be aware that arthroscopic reconstruction in the presence of a disrupted capsule may cause fluid extravasation and result in compartment syndrome. Although this concern is greater in the immediate post-injury phase, all surgeons should be aware of this potential complication and allow 1–2 weeks of post-injury healing prior to any arthroscopic procedure.
14.13.2 Surgical Technique
A wide variety of surgical techniques have been described for the treatment of acute knee dislocations. Successful surgical intervention first requires the treating surgeon to accurately and completely identify all injuries, including those to ligaments, bone, menisci, cartilage, and adjacent soft tissues. Second, regardless of technique, the primary ligamentous restraints must be repaired or reconstructed in an anatomic and isometric fashion. A detailed discussion of all the potential techniques for the surgical care of acute knee dislocations is outside the scope of this chapter; however, a brief description of our preferred ligament reconstruction surgical techniques will follow.
Once the patient is in the operating room, the first step to a successful knee reconstruction is an examination under anesthesia (EUA). A thorough EUA takes advantage of full muscle relaxation and allows the surgeon to completely delineate the extent of the ligamentous injury. The previously described ligamentous examination is repeated, including Lachman, pivot-shift, anterior and posterior drawers, varus and valgus stress testing, and medial and lateral rotational testing. If there is any uncertainty regarding the extent of ligamentous injury after the MRI and EUA, a diagnostic arthroscopy can be performed prior to autologous graft harvest or open surgical treatment of collateral, PLC, or PMC structures. An initial arthroscopy is also beneficial for evaluation of the menisci, chondral surfaces, and joint capsule (Fig. 14.4a).

(a) Diagnostic arthroscopy image assessing the articular cartilage (femoral condyle (FC) and tibial plateau (TP)) and menisci (medial meniscus (MM)). (b) Arthroscopic image with arrow denoting the drilled tibial socket of the posterior cruciate ligament (PCL). (c) Arthroscopic image with two arrows denoting the double-bundle PCL femoral tunnels. (d) Arthroscopic image of bicruciate ligament reconstruction with soft tissue grafts in place. The double-bundle PCL reconstruction is labeled by bundle: anterolateral (AL) and posteromedial (PM). The single-bundle (SB) anterior cruciate ligament reconstruction is also shown
14.13.3 Cruciate Ligament Reconstruction
Arthroscopic reconstruction of both cruciates, ACL and PCL, requires anatomic graft placement at the footprints of the native ligaments. Several techniques and graft types are acceptable, and our preferences are for arthroscopic anteromedial single-bundle ACL reconstruction and arthroscopic double-bundle tibial inlay PCL reconstruction [55, 56]. With regard to graft type, for more severe ligamentous injuries that include three or four ligaments and adjacent soft tissue trauma, we prefer to limit the additional donor-site morbidity from graft harvest associated with autograft ligament reconstruction. In this case, we prefer tibialis anterior allograft for ACL reconstruction and Achilles tendon allograft for a bifid double-bundle PCL reconstruction. Hamstring allograft is an acceptable alternative for ACL reconstruction. The potential drawbacks of allograft usage—disease transmission, increased cost, and delayed re-ligamentization—are outweighed by the decrease in operative time, lack of donor-site morbidity, decrease in skin incisions, and reduction in postoperative pain and stiffness [57, 58]. If the decision is made to utilize autograft, preference is given to the ACL. In isolated ACL reconstructions, studies suggest that autograft outperforms allograft in the young, active patient population, and this philosophy is extrapolated to our multiligament reconstructions [59]. The autograft of choice is bone-patellar tendon-bone; however, hamstring and quadriceps tendons are also viable options. If both ACL and PCL are to be reconstructed with autograft, our preference is to use ipsilateral quadriceps tendon for the double-bundle PCL graft. However, rarely do we perform autograft bicruciate ligament reconstruction secondary to the aforementioned drawbacks and potential complications. Bicruciate ligament reconstructions require precise tunnel locations, and to increase the likelihood of this occurrence, the tunnels should be drilled in a consistent and reproducible order. The PCL tibial inlay socket is created first as this is the most technically challenging (Fig. 14.4b). The ACL femoral tunnel and PCL femoral tunnels are drilled after the PCL tibial inlay socket. The ACL tibial tunnel is drilled last (Fig. 14.4c). The grafts are then passed, and the PCL graft is tensioned with the knee in 90° of flexion. The ACL graft is subsequently tensioned with the knee in full extension (Fig. 14.4d) [60]. Of note, graft tensioning should not be finalized until collateral ligament repair or reconstruction is complete.
14.13.4 Lateral Collateral Ligament and Posterolateral Corner Reconstruction
If the MRI findings (LCL attenuation) and EUA (varus opening at 30° without rotational instability) are consistent with an isolated LCL injury, then an LCL reconstruction is indicated. A lateral approach between ITB and biceps femoris is taken to expose the native LCL from origin to insertion (Fig. 14.5a). Our preferred technique is to utilize an Achilles tendon allograft. The allograft bone plug is seated in the proximal fibula and the soft tissue end whipstitched and docked in a femoral bone tunnel proximally. The reconstruction is tensioned in 30° of knee flexion with a valgus force applied. The native LCL is then imbricated or oversewn into the reconstruction.

(a) Photograph of the lateral approach to the knee with iliotibial band split and biceps femoris and lateral collateral ligament (LCL) exposed (white arrow) and tagged with suture. (b) Photograph with arrow demonstrating the LCL and posterolateral corner (PLC) elevated in a sleeve and tagged for acute repair. (c) Photograph of the drill angle (white arrow) and position of the anteroposterior tibial tunnel for recreation of the popliteus component of the PLC. (d) PLC reconstruction with popliteofibular ligament graft (black arrow), popliteus tendon graft, and LCL graft (white arrow) reconstructions
Injuries to the PLC complex affecting more than the LCL are again addressed through a lateral approach to the knee (Fig. 14.5a). A select group of PLC injuries, in which a distal soft tissue or bony avulsion has occurred, may be amenable to early repair (less than 2 weeks). The repair may be carried out with suture anchors or a screw and washer to reattach the LCL and biceps femoris to their distal attachment sites (Fig. 14.5b). Outside the 2-week window or if mid-substance attenuation exists, scarring and retraction make repair a less reliable option and we advocate surgical reconstruction. The main constituents of the PLC (LCL, popliteofibular ligament, and popliteus tendon) can be reconstructed with one Achilles tendon allograft [61]. The bone plug is secured with an interference screw at the popliteus tendon insertion. The Achilles tendon is then split into two 6–7-mm limbs starting 1–2 cm from the bone plug. The first limb is passed through a fibular bone tunnel (posterosuperior to anteroinferior) and secured with an interference screw to reconstitute the popliteofibular ligament. The residual graft material of this limb is then used to create the LCL. This is accomplished by fixing the graft at the fibular insertion of the LCL with a suture anchor and bringing the graft limb proximally to be passed through a bone tunnel at the anatomic femoral origin of the LCL. The second graft limb is used to recreate the popliteus and is thus passed through a tibial bone tunnel from posterior to anterior at the musculotendinous junction (Fig. 14.5c, d). The graft is tensioned in 30° of knee flexion with internal tibial rotation.
14.13.5 Medial Collateral Ligament and Posterior Medial Corner Repair and Reconstruction
Medial-sided injuries are surgically treated less frequently than lateral-sided injuries. Most cases of MCL and PMC patholaxity in the setting of multiligamentous knee injuries are treated nonoperatively with bracing and protected weight bearing followed by delayed cruciate reconstruction [10]. If, at the time of cruciate reconstruction, there is continued laxity suggestive of a nonhealing grade III injury to the MCL or combined MCL-PMC injury, then MCL-PMC repair or reconstruction is undertaken. A standard medial longitudinal incision centered over the posterior third of the medial femoral condyle is utilized to identify the native MCL. Proximal and distal avulsion injuries are whipstitched and reapproximated to the native attachment site with either suture anchors or a screw and soft tissue washer [33]. The knee is placed in 30° of flexion for appropriate MCL tensioning. The posterior oblique ligament (POL) is reapproximated to the posterior edge of the MCL with nonabsorbable suture. In cases of mid-substance MCL tears, the opposing ends of the MCL are whipstitched and reapproximated. The medial capsule may also be incorporated into the MCL repair. Likewise, the POL is imbricated into the MCL in a pants-over-vest pattern [33, 62]. Again, the knee should be placed in 30° of flexion during this procedure. Rarely will residual laxity be present with valgus stress testing; however, if valgus patholaxity persists, a soft tissue allograft can be used to supplement the native MCL. The soft tissue allograft should be secured to the native MCL origin and insertion sites with interference screws in bone tunnels or suture anchors.
Often the medial meniscus will need repair, and this can be accomplished with all-inside, inside-out, or hybrid technique. The meniscal attachments to the deep MCL and the posteromedial capsule should also be reapproximated to restore appropriate dissipation of hoop stress through the meniscus [33, 63]. This repair and reapproximation should be completed prior to addressing the MCL and POL.
14.14 Rehabilitation
The overall objective of rehabilitation is to protect the reconstructed or repaired knee in the early postoperative period and then gradually increase motion and strength of the knee over time. There are a number of rehabilitation protocols in the literature with demonstrated good to excellent results [64–66]. In the early postoperative period (33 weeks), the patient is placed in a long-leg splint or hinged knee brace locked in extension. During this time they should remain non-weight-bearing. The non-weight-bearing period may be extended to 6 weeks if fracture fixation, chondroplasty, or meniscal repair is undertaken. Additionally, the non-weight-bearing period may be lengthened due to patient compliance and muscle function. During this time period isometric quadriceps exercises are permitted and electrical muscle stimulation is used to enhance quadriceps recruitment [67]. Early passive motion is initiated between the third and sixth postoperative weeks with a goal of full extension and 90° of passive knee flexion at week six. Achievement of early passive motion goals is often assisted by the use of a continuous passive motion machine for 1 h a day.
The second phase of rehabilitation begins with partial weight bearing at 25 % of body weight. This phase characteristically begins at the sixth postoperative week but again depends on the extent of injury and the patient’s ability to demonstrate neuromuscular control of the operative extremity. Once partial weight bearing is initiated, the weight-bearing status is increased by 25 % per week until full weight bearing is resumed. The weight-bearing exercise has a beneficial effect on rebuilding atrophic muscle while providing mechanical stimulus to encourage tendon-to-bone healing in the ligament reconstructions. In a similar fashion, knee flexion is advanced weekly with the goal of 120° of flexion by the 12th postoperative week. All range-of-motion progress is made while wearing a hinged kneed brace, which provides varus/valgus stability to the healing knee. The stationary bike is also incorporated into this phase of the rehabilitation to promote increases in range of motion and quadriceps strength.
From the third to the sixth postoperative month, weight-bearing exercises are advanced and low-resistance quadriceps exercises are introduced. Resisted hamstring exercises are introduced after resisted quadriceps exercises due to the strain hamstring exercises can place on the healing PCL reconstruction. The focus is on closed-chain exercises, as open-chain exercises should be avoided. Proprioception and balance exercises are also introduced during this phase of rehabilitation. Once the quadriceps strength is greater than or equal to 70 % of the contralateral leg, activities may be gradually increased. Jogging and non-cutting activity can begin between the 6th and 9th postoperative months. Emphasis is placed on smooth and slow closed-chain endurance exercise, and jumping rope may be introduced. Plyometrics and cutting activity (sporting activity) are generally resumed between the 9th and 12th postoperative months. If pool workouts and swimming are to be used during the later phases of rehabilitation, it is important to restrict patients from frog kicking or breaststroke until rehabilitation is complete. We use isokinetic strength equivalent to 90 % of the contralateral limb and the single-leg hop test equivalent to 90 % of the contralateral limb as strict criteria prior to returning to sport. Additionally, the patient must be without pain, swelling, and significant laxity to be released to all activity.
14.15 Conclusion
Acute knee dislocations are uncommon yet serious injuries with significant potential for associated neurovascular complications. A high index of suspicion, appropriate clinical examination, and proper diagnostic modalities are paramount to the identification of the complete injury pattern. Vascular and open injuries should be addressed immediately. Osseous injuries should be addressed with open reduction and internal fixation prior to ligamentous reconstruction. The decision to proceed with multiligament reconstruction is multifactorial, and both patient-specific and surgeon factors should impact when and how the multiligamentous knee is repaired or reconstructed. The objectives of treatment and rehabilitation of the acute knee dislocation are to provide a stable, functional knee and ideally to return the patient to an acceptable activity level.
References
Brautigan B, Johnson DL (2000) The epidemiology of knee dislocations. Clin Sports Med 19(3):387–397
Levy BA, Marx RG (2009) Outcome after knee dislocation. Knee Surg Sports Traumatol Arthrosc 17(9):1011–1012
Seroyer ST, Musahl V, Harner CD (2008) Management of the acute knee dislocation: the Pittsburgh experience. Injury 39(7):710–718
Shelbourne KD, Pritchard J, Rettig AC, McCarroll JR, Vanmeter CD (1992) Knee dislocations with intact PCL. Orthop Rev 21(5):607–608, 610–601
Wascher DC, Dvirnak PC, DeCoster TA (1997) Knee dislocation: initial assessment and implications for treatment. J Orthop Trauma 11(7):525–529
Bratt HD, Newman AP (1993) Complete dislocation of the knee without disruption of both cruciate ligaments. J Trauma 34(3):383–389
Cooper DE, Speer KP, Wickiewicz TL, Warren RF (1992) Complete knee dislocation without posterior cruciate ligament disruption. A report of four cases and review of the literature. Clin Orthop Relat Res 284:228–233
Hoover NW (1961) Injuries of the popliteal artery associated with fractures and dislocations. Surg Clin North Am 41:1099–1112
Jones RE, Smith EC, Bone GE (1979) Vascular and orthopedic complications of knee dislocation. Surg Gynecol Obstet 149(4):554–558
Klimkiewicz JJ, Petrie RS, Harner CD (2000) Surgical treatment of combined injury to anterior cruciate ligament, posterior cruciate ligament, and medial structures. Clin Sports Med 19(3):479–492, vii
Yeh WL, Tu YK, Su JY, Hsu RW (1999) Knee dislocation: treatment of high-velocity knee dislocation. J Trauma 46(4):693–701
Kennedy JC (1963) Complete dislocation of the knee joint. J Bone Joint Surg Am 45:889–904
Levitsky KA, Berger A, Nicholas GG, Vernick CG, Wilber JH, Scagliotti CJ (1988) Bilateral open dislocation of the knee joint. A case report. J Bone Joint Surg Am 70(9):1407–1409
Shelbourne KD, Porter DA, Clingman JA, McCarroll JR, Rettig AC (1991) Low-velocity knee dislocation. Orthop Rev 20(11):995–1004
Pace A, Fergusson C (2004) Spontaneous non-traumatic dislocation of the knee. Acta Orthop Belg 70(5):498–501
Shetty RR, Mostofi SB, Housden PL (2005) Knee dislocation of a morbidly obese patient: a case report. J Orthop Surg (Hong Kong) 13(1):76–78
Green NE, Allen BL (1977) Vascular injuries associated with dislocation of the knee. J Bone Joint Surg Am 59(2):236–239
Schenck RC Jr (1994) The dislocated knee. Instr Course Lect 43:127–136
Collicott PE (1992) Advanced Trauma Life Support (ATLS): past, present, future–16th Stone Lecture, American Trauma Society. J Trauma 33(5):749–753
McCoy GF, Hannon DG, Barr RJ, Templeton J (1987) Vascular injury associated with low-velocity dislocations of the knee. J Bone Joint Surg Br 69(2):285–287
Meyers MH, Harvey JP Jr (1971) Traumatic dislocation of the knee joint. A study of eighteen cases. J Bone Joint Surg Am 53(1):16–29
Peck JJ, Eastman AB, Bergan JJ, Sedwitz MM, Hoyt DB, McReynolds DG (1990) Popliteal vascular trauma. A community experience. Arch Surg 125(10):1339–1343; discussion 1343–1344
Mills WJ, Barei DP, McNair P (2004) The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: a prospective study. J Trauma 56(6):1261–1265
Marin EL, Bifulco SS, Fast A (1990) Obesity. A risk factor for knee dislocation. Am J Phys Med Rehabil 69(3):132–134
Robertson A, Nutton RW, Keating JF (2006) Dislocation of the knee. J Bone Joint Surg Br 88(6):706–711
Monahan TJ (2001) Management of acute and chronic nerve injuries in the multiple ligament injured knee. Sports Med Arthrosc Rev 9(3):227–238
Jonsson T, Althoff B, Peterson L, Renstrom P (1982) Clinical diagnosis of ruptures of the anterior cruciate ligament: a comparative study of the Lachman test and the anterior drawer sign. Am J Sports Med 10(2):100–102
Sekiya JK, Whiddon DR, Zehms CT, Miller MD (2008) A clinically relevant assessment of posterior cruciate ligament and posterolateral corner injuries. Evaluation of isolated and combined deficiency. J Bone Joint Surg Am 90(8):1621–1627
Borden PS, Johnson DL (2001) Initial assessment of the acute and chronic multiple ligament-injured knee. Sports Med Arthrosc Rev 9(3):178–184
Norwood LA Jr, Hughston JC (1980) Combined anterolateral-anteromedial rotatory instability of the knee. Clin Orthop Relat Res 147:62–67
Hughston JC, Barrett GR (1983) Acute anteromedial rotatory instability. Long-term results of surgical repair. J Bone Joint Surg Am 65(2):145–153
Ritchie JR, Bergfeld JA, Kambic H, Manning T (1998) Isolated sectioning of the medial and posteromedial capsular ligaments in the posterior cruciate ligament-deficient knee. Influence on posterior tibial translation. Am J Sports Med 26(3):389–394
Tibor LM, Marchant MH Jr, Taylor DC, Hardaker WT Jr, Garrett WE Jr, Sekiya JK (2011) Management of medial-sided knee injuries, part 2: posteromedial corner. Am J Sports Med 39(6):1332–1340
Lunden JB, Bzdusek PJ, Monson JK, Malcomson KW, Laprade RF (2010) Current concepts in the recognition and treatment of posterolateral corner injuries of the knee. J Orthop Sports Phys Ther 40(8):502–516
Griffith CJ, Wijdicks CA, LaPrade RF, Armitage BM, Johansen S, Engebretsen L (2009) Force measurements on the posterior oblique ligament and superficial medial collateral ligament proximal and distal divisions to applied loads. Am J Sports Med 37(1):140–148
Garavaglia G, Lubbeke A, Dubois-Ferriere V, Suva D, Fritschy D, Menetrey J (2007) Accuracy of stress radiography techniques in grading isolated and combined posterior knee injuries: a cadaveric study. Am J Sports Med 35(12):2051–2056
Bui KL, Ilaslan H, Parker RD, Sundaram M (2008) Knee dislocations: a magnetic resonance imaging study correlated with clinical and operative findings. Skeletal Radiol 37(7):653–661
Howells NR, Brunton LR, Robinson J, Porteus AJ, Eldridge JD, Murray JR (2011) Acute knee dislocation: an evidence based approach to the management of the multiligament injured knee. Injury 42(11):1198–1204
Dedmond BT, Almekinders LC (2001) Operative versus nonoperative treatment of knee dislocations: a meta-analysis. Am J Knee Surg 14(1):33–38
Fanelli GC, Orcutt DR, Edson CJ (2005) The multiple-ligament injured knee: evaluation, treatment, and results. Arthroscopy 21(4):471–486
Harner CD, Waltrip RL, Bennett CH, Francis KA, Cole B, Irrgang JJ (2004) Surgical management of knee dislocations. J Bone Joint Surg Am 86-A(2):262–273
Sisto DJ, Warren RF (1985) Complete knee dislocation. A follow-up study of operative treatment. Clin Orthop Relat Res 198:94–101
Almekinders LC, Dedmond BT (2000) Outcomes of the operatively treated knee dislocation. Clin Sports Med 19(3):503–518
Levy BA, Dajani KA, Whelan DB et al (2009) Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy 25(4):430–438
Richter M, Bosch U, Wippermann B, Hofmann A, Krettek C (2002) Comparison of surgical repair or reconstruction of the cruciate ligaments versus nonsurgical treatment in patients with traumatic knee dislocations. Am J Sports Med 30(5):718–727
Wong CH, Tan JL, Chang HC, Khin LW, Low CO (2004) Knee dislocations–a retrospective study comparing operative versus closed immobilization treatment outcomes. Knee Surg Sports Traumatol Arthrosc 12(6):540–544
Ohkoshi Y, Nagasaki S, Shibata N, Yamamoto K, Hashimoto T, Yamane S (2002) Two-stage reconstruction with autografts for knee dislocations. Clin Orthop Relat Res 398:169–175
Liow RY, McNicholas MJ, Keating JF, Nutton RW (2003) Ligament repair and reconstruction in traumatic dislocation of the knee. J Bone Joint Surg Br 85(6):845–851
Wascher DC, Schenck RC Jr (2001) Surgical treatment of acute and chronic anterior cruciate ligament/posterior cruciate ligament/lateral sided injuries of the knee. Sports Med Arthrosc Rev 9(3):199–207
Mook WR, Miller MD, Diduch DR, Hertel J, Boachie-Adjei Y, Hart JM (2009) Multiple-ligament knee injuries: a systematic review of the timing of operative intervention and postoperative rehabilitation. J Bone Joint Surg Am 91(12):2946–2957
Fanelli GC, Edson CJ (2004) Combined posterior cruciate ligament-posterolateral reconstructions with Achilles tendon allograft and biceps femoris tendon tenodesis: 2- to 10-year follow-up. Arthroscopy 20(4):339–345
Fanelli GC, Giannotti BF, Edson CJ (1996) Arthroscopically assisted combined posterior cruciate ligament/posterior lateral complex reconstruction. Arthroscopy 12(5):521–530
Karataglis D, Bisbinas I, Green MA, Learmonth DJ (2006) Functional outcome following reconstruction in chronic multiple ligament deficient knees. Knee Surg Sports Traumatol Arthrosc 14(9):843–847
Shelbourne KD, Haro MS, Gray T (2007) Knee dislocation with lateral side injury: results of an en masse surgical repair technique of the lateral side. Am J Sports Med 35(7):1105–1116
Bedi A, Altchek DW (2009) The “footprint” anterior cruciate ligament technique: an anatomic approach to anterior cruciate ligament reconstruction. Arthroscopy 25(10):1128–1138
Kohen RB, Sekiya JK (2009) Single-bundle versus double-bundle posterior cruciate ligament reconstruction. Arthroscopy 25(12):1470–1477
Prohaska DJ, Harner CD (2001) Surgical treatment of acute and chronic anterior and posterior cruciate ligament medial side injuries of the knee. Sports Med Arthrosc Rev 9(3):193–198
Shapiro MS, Freedman EL (1995) Allograft reconstruction of the anterior and posterior cruciate ligaments after traumatic knee dislocation. Am J Sports Med 23(5):580–587
Borchers JR, Pedroza A, Kaeding C (2009) Activity level and graft type as risk factors for anterior cruciate ligament graft failure: a case–control study. Am J Sports Med 37(12):2362–2367
Sherman SL, Chalmers PN, Yanke AB et al (2012) Graft tensioning during knee ligament reconstruction: principles and practice. J Am Acad Orthop Surg 20(10):633–645
Sekiya JK, Kurtz CA (2005) Posterolateral corner reconstruction of the knee: surgical technique utilizing a bifid Achilles tendon allograft and a double femoral tunnel. Arthroscopy 21(11):1400
Hughston JC, Eilers AF (1973) The role of the posterior oblique ligament in repairs of acute medial (collateral) ligament tears of the knee. J Bone Joint Surg Am 55(5):923–940
McAllister DR, Miller MD, Sekiya JK, Wojtys EM (2009) Posterior cruciate ligament biomechanics and options for surgical treatment. Instr Course Lect 58:377–388
Edson C (2003) Postoperative rehabilitation of the multiple-ligament reconstructed knee. Oper Tech Sports Med 11(4):294–301
Edson CJ (2001) Postoperative rehabilitation of the multiligament-reconstructed knee. Sports Med Arthrosc Rev 9(3):247–254
Fanelli GC, Edson CJ (2002) Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction in the multiple ligament injured knee: 2- to 10-year follow-up. Arthroscopy 18(7):703–714
Kim KM, Croy T, Hertel J, Saliba S (2010) Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient-oriented outcomes: a systematic review. J Orthop Sports Phys Ther 40(7):383–391
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Verlag Italia
About this chapter
Cite this chapter
Weber, A.E., Sekiya, J.K. (2014). Treatment for Acute Knee Dislocations. In: Rossi, R., Margheritini, F. (eds) Knee Ligament Injuries. Springer, Milano. https://doi.org/10.1007/978-88-470-5513-1_14
Download citation
DOI: https://doi.org/10.1007/978-88-470-5513-1_14
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-5512-4
Online ISBN: 978-88-470-5513-1
eBook Packages: MedicineMedicine (R0)