
Abstract
The incidence of breast cancer has increased all over the world, which can be a result of social-demographic changes and access to health care services. Despite the increase in the incidence of breast cancer, an increase in mortality rate in developed countries has not been observed. Mammography is currently the most important method in breast evaluation. Other diagnostic methods, such as ultrasonography, magnetic resonance imaging, scintigraphy, and PET–CT, are used as auxiliary methods in the diagnosis of breast cancer and they are chosen according to the characteristics of the lesion that will be evaluated. There are two different levels of approach for breast evaluation, and these have an influence on the choice of imaging methods: asymptomatic patient evaluation for breast cancer screening and symptomatic patient evaluation to diagnose either a benign or a malignant tumor. Indications and limits are described here to help surgeons in their decisions and surgical planning.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
1 Introduction
The incidence of breast cancer has increased all over the world, which can be a result of social-demographic changes and access to health care services. Holland is the country with the highest incidence, and its rate adjusted by age is 90.2/100,000. In the USA the rate is 86.9/100,000. High rates are also found in other European countries, as well as in Australia, New Zealand, and South America, and especially in Uruguay and Argentina. Most populations in Africa and Asia have low rates of the disease. Incidence rates increase with age, and reach a peak in the age range between 65 and 70 years [1–3].
Despite the increase in the incidence of breast cancer, an increase in mortality rate in developed countries has not been observed. Up until 1987, breast cancer was the main cause of death by cancer among women in the USA, and then it was surpassed by lung cancer. That occurred because breast cancer had a lower mortality rate, mainly due to mammographic tracking, whereas lung cancer had a growing incidence among women because of tobacco smoking [4].
In Brazil, of cancers, breast cancer has the incidence among women. The highest incidence is observed in the south and southeast regions (the rates are 71/100,000 and 73/100,000, respectively). However, contrary to what is observed in developed countries, there has been an increase in the gross mortality rate in the past few decades, from 5.77 per 100,000 women in 1979 to 9.70 per 100,000 women in 1998. For that reason, breast cancer is still the main cause of death by cancer among women [5].
2 Diagnostic Methods in Breast Cancer
Mammography is currently the most important method in breast evaluation. Other diagnostic methods, such as ultrasonography, magnetic resonance imaging (MRI), scintigraphy, and PET–CT, are used as auxiliary methods in the diagnosis of breast cancer and they are chosen according to the lesion that will be evaluated [6].
There are two different levels of approach for breast evaluation, and these have an influence on the choice of imaging methods: asymptomatic patient evaluation for breast cancer screening and symptomatic patient evaluation to diagnose either a benign or a malignant tumor.
2.1 Breast Cancer Screening
The aim of breast cancer screening is to spot the tumor at an early stage, before its clinical manifestation, increasing the chances of extended the patient’s life. Mammography was the only method that pointed to an absolute reduction in mortality rate (between 25 % and 30 %) among patients undergoing regular screening owing to detection of ductal carcinomas in situ and infiltrating carcinomas of a smaller size and lower staging when compared with the group of nontracked patients [7–15]. Ultrasonography and MRI appear to be useful in specific groups of patients; however, no long-term study has been conducted to determine the impact on mortality.
Mammography can detect five to seven cancer cases in every 1,000 asymptomatic women undergoing the first examination and two to three cases in every 1,000 women undergoing annual screening [16]. The Health Insurance Plan Study provided the first evidence for the potential of mammography to reduce the mortality rate. In this study, performed in the 1960 s, around 6,000 women were randomized in two groups, a control one and another one undergoing physical examinations and mammograms. After a 7 year follow-up, a 30 % mortality rate reduction in the group of women that underwent screening [17–19] was noticed. After that study, mammography began to be widely used for screening breast cancer. By the end of the 1980 s, a variety of other studies confirmed a reduction of the mortality rate of patients aged 50 years and older undergoing regular screening [7–15]. There are also benefits, although not so evident, for women between 40 and 50 years old. Although no study has demonstrated an association between self-examination of the breasts and lower mortality rate, this type of test still has to be encouraged.
Ultrasonography is not appropriate as an initial method for tracking, mainly owing to its limited ability to evaluate microcalcifications, which are the early manifestations of cancer in 50 % of cases. Some studies have proposed the use of ultrasonography as the method for screening of asymptomatic patients with negative mammographic findings but high breast density [Breast Imaging Reporting and Data System (BI-RADS®) density categories 3 and 4) [20]. Kolb et al. [21] published a study performed with 11,130 asymptomatic patients undergoing mammography and ultrasonography which shows that additional ultrasonography and mammography increased the detection of breast cancer in dense breast patients by 42 %. Nevertheless, so far there are not enough randomized studies showing a decrease in mortality rate among this group of patients, which is a requirement for application of the method as a screening method in large populations.
MRI appears to be the most sensitive method for detecting breast cancer among high-risk patients, mainly for those with identified genetic alterations (BRCA1 and BRCA2) or a marked family history [16, 22, 23]. Krieger et al. [22] followed up 1,909 women with marked family history or with BRCA1 and/or BRCA2 mutations for an average period of 2.9 years, and found 33.3 % sensitivity for mammography and 79.5 % for MRI. Kuhl et al. [24] evaluated 529 asymptomatic women with marked family history or genetic mutation, for a period of 5.3 years, and they found 33 % sensitivity for mammography, 40 % for ultrasonography, and 91 % for MRI. However, randomized prospective studies are required to establish the impact of mortality on these new tracking methods.
In Brazil, the Ministry of Health in association with INCA and the Brazilian Society of Mastology designed a consensus document with recommendations on breast cancer control to be implemented by the end of 2003. The recommendations for detection of cancer at an early stage are as follows [25]:
-
1.
Clinical examinations of the breast for all women above 40 years of age, performed annually
-
2.
Mammography for all women between 50 and 69 years old, with a maximum interval of 2 years between examinations
-
3.
Breast examinations and an annual mammogram for women from 35 years old with high risk of breast cancer
-
4.
Guarantee of access to diagnosis, treatment, and follow-up for all women with alterations found in the examinations performed.
2.2 Evaluation of Symptomatic Patients
All imaging methods are useful for the evaluation of a patient with symptoms or signs that point to breast cancer. The combination of mammography and ultrasonography is particularly useful in this group of patients. Moy et al. [26] reported that only 2.6 % of patients from a group of 374 symptomatic women with breast cancer did not have symptoms or signs on mammography and ultrasonography. Kolb et al. [21] also reported that mammography itself diagnosed only 48 % of the tumors in patients with dense breasts, whereas mammography and ultrasonography together detected 97 % of the cases. The possibility of a patient presenting with a tumor after negative findings on mammography and ultrasonography is 3 %.
The choice of an initial method for a symptomatic patient may be influenced by the patient’s age range. If the patient is young (below 35 years old), ultrasonography is the method chosen for initial evaluation, considering that most patients will show dense breasts. For patients aged 35 years and above, an initial evaluation by mammography is recommend, and complementary ultrasonography or MRI applies for patients in which clinical suspicion is maintained [25].
If there are suspicious findings on a physical examination, no test or group of tests is able to guarantee that a patient does not have breast cancer. The final course of action in this group of patients must be based mainly on clinical parameters.
3 Breast Imaging Reporting and Data System (BI-RADS®)
BI-RADS® is the result of a mutual effort between members of the American College of Radiology and the National Cancer Institute, Centers for Disease Control and Preventions, Food and Drug Administration, American Medical Association, American College of Surgeons, and College of American Pathologists. This system is designed to standardize the medical report, reduce misunderstandings in the interpretation of images, and make follow-up of patients easier, besides allowing internal quality auditing. It should be used in mammography, ultrasonography, and MRI [6].
After evaluation of images, the medical report must be written in a clear and concise way so it can give the professional who requested the test a good idea of what was diagnosed as well as the recommended course of action. The medical report must contain the following five parts:
-
1.
Indication for examination (a brief description of the reason for the examination)
-
2.
Breast composition (description of the breast standard, this indicates the risk of a lesion being obscured by normal mammary tissue)
-
3.
Findings (an accurate description of the findings according to established terms and standards must be given)
-
4.
Comparison with previous studies (important in cases of dubious findings, and less important in cases of mammograms which reveal either negative findings or benign lesions)
-
5.
Overall assessment (classification of the examination in one of the system categories, and recommendation for the course of action; see Table 3.1)
Table 3.1 BI-RADS® categories
BI-RADS® category 0 must be reserved for cases in which an additional evaluation has to be performed, such as additional mammographic views with local compression or magnification, or even the complementary use of other tests (e.g., ultrasonography or MRI). It can also be used in cases where a comparison with previous tests is important, before a final impression is reached.
Cases classified as negative (category 1) or with benign findings (category 2) are followed up through annual routine tests.
In cases of probably benign lesions (category 3) which show a risk of malignancy lower than 2 %, a semester follow-up is recommended until 2–3 years has elapsed (according to the lesion) with the aim of determining the stability of the lesion. After such a period, if no alteration in the lesion is noticed, it is classified as category 2, and returns to the annual tracking group.
For lesions classified as category 4, the subdivision into categories 4A, 4B, and 4C is optional, but strongly recommended. Category 4A must be used when the risk of malignancy is low and a 6 month control period after biopsy or negative cytological findings is indicated. Category 4B indicates an intermediate risk of malignancy, so a good anatomic–radiological co-relation is needed. Category 4C includes findings of moderate suspicion in which malignancy is expected.
Lesions classified as highly suggestive of malignancy (category 5) have a risk of malignancy higher than 95 %. This group must be reserved for the group of classic tumor lesions such as spiculated masses, pleomorphic calcifications, and ductal calcifications in which a malignant lesion can only be ascertained after surgical evaluation of the region in question.
Category 6 is reserved for the group of lesions that are already diagnosed as being cancerous, and for which neoadjuvant chemotherapy or a second opinion is required. This category is not appropriate in cases of follow-up after breast-conserving surgery.
4 Mammography
4.1 Normal Mammographic Findings
There is a big variation in the appearance of a normal breast in a mammogram, mainly as to the size, shape, and composition of the parenchyma. The composition of the parenchyma may vary from almost totally substituted to extremely dense, and the sensitivity of mammography is directly related to this composition.
Liposubstituted breasts have excellent background tissue for tumor visualization, whereas high density can obscure tumor visualization.
The BI-RADS® composition of the breast is divided into four categories [6]:
-
1.
Category 1: breasts with severe adipose substitution (less than 25 % glandular tissue) (Fig. 3.1a)
Fig. 3.1 
Mammographic patterns of mammary density according to BI-RADS®: severe adipose substitution (a), sparse fibroglandular densities (b), heterogeneously dense (c), and extremely dense (d)
-
2.
Category 2: breasts with sparse fibroglandular densities (25-50 % glandular tissue) (Fig. 3.1b)
-
3.
Category 3: heterogeneously dense breasts, which can obscure the detection of small lesions (approximately 51-72 % glandular tissue) (Fig. 3.1c)
-
4.
Category 4: extremely dense breasts, which can reduce the sensitivity of mammography (over 75 % fibroglandular tissue) (Fig. 3.1d)

Younger women tend to have a greater amount of fibroglandular tissue, although there is considerable variation within the same age range. As the age range increases or when the woman breastfeeds, the fibroglandular tissue tends to be replaced by fat. The replacement always occurs from the posterior region to the anterior region and from medial to lateral, in a symmetric way. An increase in mammary density can be observed during pregnancy and owing to the use of hormone-replacement therapy (HRT).
4.2 Abnormal Mammographic Findings
Masses and calcifications are the commonest abnormal findings in mammography. Other lesions that have been observed are architectural distortion, focal asymmetry, global asymmetry, retraction or cutaneous thickening, mammillary retraction, and axillary lymphadenomegaly.
4.2.1 Masses
Masses are described as lesions occupying space that is seen in at least two views. They are described according to shape, margin, and density [6].
The shapes can be round, oval, lobulated, or irregular (Fig. 3.2). Whereas oval and round shapes are usually related to benign lesions, an irregular shape is more associated with malignant lesions.

Shapes of masses screened: round (a), oval (b), and irregular (c)
Margins are also an important indicator of malignancy, and they are described as circumscribed, microlobulated, obscured, indistinct, or spiculated (Fig. 3.3). Circumscribed lesions are defined as lesions that show at least 75 % of the margins as well defined, and they are associated with a possibility of malignancy lower than 2 % [32, 33]. These lesions are classified as probably benign (BI-RADS® 3 category) and it is recommended that a semester control is done. Microlobulated lesions and indistinct ones have a higher risk of malignancy, whereas spiculated ones are highly suggestive of malignancy.

Margins of masses screened: circumscribed (a), obscured (b), indistinct (c), and spiculated (d)
The density of masses may also point to their origin, being described as high density, low density, isodense to parenchyma, and fat density (Fig. 3.4). Generally, benign lesions tend to be less dense than malignant ones, although this is not always true. The existence of fat density inside the mass confirms its benign nature.

Density of masses screened: low density (a), isodense (b), high density (c), and fat density (d)
Finding associated lesions may help define the nature of lesions, such as gross calcifications (associated with fibroadenoma in involution) and pleomorphic calcifications (related to malignant lesions), cutaneous retraction, and mammillary retraction.
4.2.2 Calcifications
Calcifications are described according to their morphology and distribution. Morphology shows a good correlation with the nature of calcifications, and they can be classified as [6]:
-
1.
Typically benign: skin calcifications (lucent-centered), vascular calcifications (parallel lines associated with vascular structures), “popcorn”-type calcifications (coarse and associated with mass images, corresponding to fibroadenoma in involution), gross tubular calcifications (associated with duct ectasia), round (frequently formed in acini and lobes), rodlike calcifications (lucent-centered), “eggshell” calcifications (calcium deposit on the cyst walls or of fat necrosis), “milk of calcium” calcifications (sediment calcifications inside the cysts), suture calcifications (formation of calcium around the sutures), dystrophic calcifications (in irradiated breasts and those undergoing traumas) (Fig. 3.5).
Fig. 3.5 
Typically benign calcifications: “milk of calcium” (a); dystrophic (b), round and rodlike (c); gross tubular (d), “popcorn” type (e), and vascular (f)
-
2.
Of intermediate concern: amorphous or indistinct calcifications (frequently small and with morphology that is difficult to define, commonly mistaken for benign calcifications; when grouped they should be correlated with biopsy findings); heterogeneous calcifications (they are larger and tend to coalesce, so they can be associated with malignancy or with an initial phase of dystrophic calcifications of fibrosis, fibroadenoma or trauma) (Fig. 3.6).
Fig. 3.6 
Microcalcifications of intermediate concern: amorphous (a) and heterogeneous (b)
-
3.
Higher probability of malignancy: fine pleomorphic calcifications (they show a wide variety of shapes and sizes, generally less than 0.5 mm) and ductal calcifications (fine and irregular calcifications on the duct tracks, which suggest that there is participation of the duct through the tumor) (Fig. 3.7).
Fig. 3.7 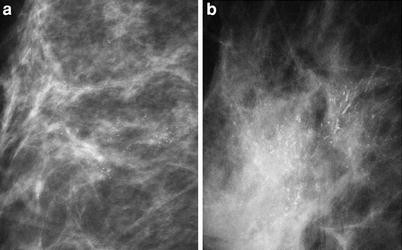
Microcalcifications of higher probability of malignancy: fine pleomorphic (a) and ductal (b)



We can describe the distribution of calcifications as follows:
-
1.
Diffuse: distributed at random in the breasts, generally found in benign calcifications.
-
2.
Regional: found in a broad area of the breast, but with no duct track. One or more quadrants may be involved, and the risk of malignancy is associated mainly with calcification morphology.
-
3.
Clustered: they is used when at least five calcifications occupy a small volume of the breast, and there is high risk of malignancy.
-
4.
Linear: this points to a ductal distribution, increasing the risk of malignancy.
-
5.
Segmental: this point to damage to the ducts and their branches in an area of the breast, also increasing the risk of malignancy.
4.2.3 Architectural Distortion
Architectural distortion is defined when normal architecture of the breast is altered; however, there is no evident mass (Fig. 3.8). When there are no records of trauma or surgery, distortion leads to a condition highly suspicious of malignancy or a radial scar; therefore, histological evaluation is recommended [6].

Architectural distortion in mammography
4.2.4 Special Cases
Some alterations can be seen through mammography, and they are described as follows [6]:
-
1.
Isolated duct dilation: If not associated with other relevant clinical suspicious findings, it is not considered important.
-
2.
Intramammary lymph nodes: They are usually smaller than 10 mm, they have a fatty hilum, and have a reniform shape. They can appear in any breast region, although they are mainly found in lateral quadrants.
-
3.
Global asymmetry: This generally represents an anatomic variation, which is identified during the comparison with the contralateral breast. It cannot be associated with the palpable mass, the architectural distortion area, masses, or microcalcifications.
-
4.
Focal asymmetry: This is defined as a lesion that cannot fill the criteria of mass required, and is visualized in both views as similar shapes. It may represent a normal parenchyma island; however, often it has nonspecific characteristics, so it demands additional investigation.
-
5.
Related findings: Some findings may increase the suspicion of malignancy when identified together with the suspicion of a lesion, represented by skin retraction, nipple retraction, skin thickening, and axillary lymphadenomegaly among others.
5 Ultrasonography
Mammary ultrasonography is a diagnostic method that aids in the characterization of alterations detected either in clinical or mammographic examinations [27, 28]. Besides allowing differentiation of solid masses and cystic ones, it supplies additional data to characterize lesions as benign or malignant; it also aids in the analysis of dense breasts through mammograms and it guides percutaneous procedures.
5.1 Normal Ultrasonographic Findings
As in mammography, the ultrasonographic aspect of the breast also varies according to its composition. The mammary echotexture results from the combination of the fibroglandular tissue (echogenic), fat (hypoechoic), and connective tissue (ligaments of Cooper, echogenic). These echotexture patterns may affect the sensitivity for lesion detection, therefore reducing the sensitivity for solid mass detection in very liposubstituted breasts, or even simulate alterations in cases of heterogeneous breasts, which must be evaluated and differentiated in real time throughout the examination.
Three echotexture patterns are described according to BI-RADS® [6]:
-
1.
Homogeneous—fat (Fig. 3.9a)
Fig. 3.9 
Echotexture patterns in ultrasonography according to BI-RADS®: homogeneous—fat (a), homogeneous—fibroglandular (b), and heterogeneous (c)
-
2.
Homogeneous—fibroglandular (Fig. 3.9b)
-
3.
Heterogeneous—fibroglandular elements, fat elements, connective tissue and ducts, interspersed; a pattern of younger breasts with little liposubstitution (Fig. 3.9c)

5.2 Abnormal Ultrasonographic Findings
The evaluation of masses detected both through mammography and through physical examinations is the most frequent indication for ultrasonography. Calcifications are poorly evaluated through this method, as their detection becomes more difficult, and their morphological evaluation is not possible.
5.2.1 Masses
Masses must be detected and analyzed on more than one view to differentiate them from normal anatomic structures. They are echographically described according to shape, orientation, margins, transition with mammary tissue, echogenicity pattern, posterior acoustic aspect, and relations with and effects on the adjacent tissue [6, 28].
The shape can be defined as round, oval, or irregular (Fig. 3.10). When it is oval, it is called macrolobulated if it has up to three lobulations. Interpretation of the examination concerning benignity and malignancy of the mass is similar to that for mammography, and irregular masses are the most suspicious.

Shape of masses screened through ultrasonography: round (a), oval (b), and irregular (c)
Orientation is a particular aspect of ultrasonography (Fig. 3.11). Masses that are parallel to the skin, that is, wider than higher, are generally benign. When the orientation is vertical, that is, higher than wider, this is more suggestive of malignancy, as it represents a growth through normal tissue planes.

Orientation of masses in ultrasonography: parallel to the skin (a) and perpendicular to the skin (b)
Margins are described as circumscribed, indistinct, spiculated, angular (projections forming acute angles), and microlobulated (various small lobulations of 1–2 mm) (Fig. 3.12). Except for the circumscribed margin, the various aspects are suggestive of malignancy. The spiculated margins and/or microlobulated margins are the ones that have the highest predictive value for malignancy [28, 29].

Margins of masses in ultrasonography: circumscribed (a) indistinct (b), and spiculated (c)
The transitional zone with the adjacent mammary parenchyma is described as defined or undefined. The well-defined transition or that with an echogenic halo indicates benignity, as it shows a lesion of slow growth compressing the parenchyma around and not infiltrated. The transition without defined demarcation is associated with some carcinomas and abscesses. The finding of an echogenic pseudo-capsule around the lesion must be interpreted together with the lobe shape (oval or slightly lobulated) to reinforce the sureness of benignity [28].
The echogenicity pattern aids primarily with the differentiation between cystic mass (anechoic) and solid mass (hypoechoic, isoechoic, and hyperechoic), defined in relation to fat (Fig. 3.13). Homogeneously hyperechoic masses are considered of higher predictive value for benignity. Solid hypoechoic and isoechoic masses need other characteristics for evaluation concerning malignancy. Complex masses have mixed echogenicity, with both anechoic and echogenic components [28].

Echogenicity patterns of masses in ultrasonography: anechoic (a), hypoechoic (b), isoechoic (c), and hyperechoic (d)
The posterior acoustic phenomena result from attenuation of the mass (Fig. 3.14), except for posterior peripheral shadow, which occurs as a result of an alteration of the speed of the acoustic beam at the curved edges in either oval or round masses. These phenomena include acoustic reinforcement, that is, more echogenic posterior area, which is found mainly in cysts. Also, an acoustic shadow has been observed, that is, a darker central posterior area, which is associated with calcifications, fibrosis, or neoplasia with high desmoplastic reaction. Some masses do not cause an alteration of the acoustic beam through the mass. These aspects are not reliable for the definition of benignity or malignancy and they must be considered in co-relation with other aspects [28, 29].

Acoustic phenomena of masses in ultrasonography: acoustic reinforcement (a), no alteration of the acoustic beam (b), and acoustic shadow (c)
Masses may have some effects on adjacent mammary parenchyma. Benign lesions tend to produce fewer alterations, such as compression. More aggressive and infiltrating lesions may obliterate the adjacent tissue planes, pull or thicken Cooper’s ligaments, and cause edema or architectural distortion of the parenchyma, as well as rupture of the regular anatomic planes. The ducts may be pulled and dilated, and the skin may have focal or diffuse thickening (normal is 2 mm or less), retraction, and irregularity.
5.2.2 Calcifications
Ultrasonography has very low sensitivity for the detection of calcifications, especially microcalcifications. It also does not allow their morphological analysis, which is important for characterization of malignancy. Among other factors, the low sensitivity results from heterogeneous breast echotexture and from the small size of the microcalcifications (less than 0.5 mm), with no typical posterior acoustic shadow [6, 28].
5.2.3 Special Cases
Some alterations exhibit characteristic findings [6]:
-
1.
Clustered microcysts: These are defined as small anechoic clustered images (less than 2-3 mm) with thin septations inside (less than 0.5 mm), with no associated solid component. When not palpable, they are considered as probably benign lesions (category 3). This finding occurs mainly with fibrocystic alterations and in the apocrine metaplasia (Fig. 3.15a).
Fig. 3.15 
Special cases observed through ultrasonography: clustered microcysts (a), complicated cysts (b), and foreign body related to draining (c)
-
2.
Complicated cysts: These are cysts that have thin echoes inside the fluid level or even mobile debris, with no solid component attached to the wall. These are also considered as probably benign lesions (category 3) (Fig. 3.15b).
-
3.
Skin masses: These are the so-called epidermal and sebaceous inclusion cysts, keloids, neurofibromas, and accessory nipples. They are classified as benign lesions (category 2).
-
4.
Foreign bodies: These may correspond to surgery marking clips, threads, catheters, silicone, metal, or glass from trauma. Clinical history is very important for differentiation. Free silicone in the parenchyma has a typical aspect of a “snowstorm,” that is, an echogenic area that causes a marked acoustic shadow, obscuring the deep structures (Fig. 3.15c).
-
5.
Intramammary lymph nodes: These are described as oval masses, circumscribed, with an echogenic center and a hypoechoic periphery. They are located mainly in the upper quadrants and sides of the breast, and their size ranges from 0.3 to 1 cm.
-
6.
Axillary lymph nodes: The aspects are similar to those of the intramammary lymph nodes, and they can measure more than 2 cm. When they are too big (above 4 cm) or with a hypoechoic center, they must be evaluated so the possibility of a metastatic disease is not ignored.

5.2.4 Vascularity
This is an additional piece of data for the evaluation of masses or suspicion areas, although with limited value. The complete absence of vascularity is usually observed in cysts. A rather increased vascularity may be suggestive of neovascularity and it is usually observed not only inside the mass but also in the peripheral area of a lesion, or diffusely in the surrounding tissue [6].
6 Magnetic Resonance Imaging
MRI is the most accurate method for the detection of breast cancer and it is indicated in selected cases to increase the sensitivity that results from traditional methods (mammography and ultrasonography). The method has the advantage of showing a three-dimensional view of the breast, with high sensitivity and no use of ionizing radiation. Among the disadvantages are the high cost of the procedure and its low specificity [30].
MRI analysis must be made through images obtained from the dynamic technique during the endovenous injection of paramagnetic contrast material (gadolinium), associated with enhancement kinetics. Then, images are obtained with spatial high resolution for a detailed morphological evaluation of the lesion with the aim of detecting characteristics of suggestive malignancy. Interpretation of MRI findings must consider the clinical history data (including physical examinations—palpation of the masses, skin appearance, scars; surgical antecedents of those of biopsies; menstrual cycles; HRT; radiotherapy) and comparison with the findings of previous examinations (mammography and ultrasonography—identification of areas with suggestive lesions, mainly microcalcifications, evaluation of temporal stability, or the appearance of new lesions, among others).
6.1 Normal Magnetic Resonance Imaging Findings
Breast anatomy is thoroughly demonstrated through MRI, by which not only the parenchyma can be evaluated, but also vessels, lymph nodes (intramammary and those from axillary prolongations), the retromammary area, and the thoracic wall; these latter are difficult to access through other imaging methods.
The parenchyma is characterized and described according to BI-RADS® criteria [6]:
-
1.
Severe adipose substitution
-
2.
Disperse fibroglandular density
-
3.
Heterogeneously dense
-
4.
Extremely dense
Contrary to what occurs in mammography, dense breasts are not difficult to diagnose through MRI, which minimizes the overlapping effect of the parenchyma, and also through contrast material, which makes lesions appear more evident. On the other hand, hormone variations have an influence on the interpretation of images, mainly considering enhancement and parenchyma edema. In premenopause breasts, parenchyma enhancement varies according to the menstrual cycle, so incidental points of enhancement (uniform, diffuse, or scattered in some areas) are common and more evident in the first and fourth weeks. Some of these points may appear as quick and intense enhancement as in malignant lesions, being differentiated only when they disappear in subsequent examinations in a different phase of the menstrual cycle. The examination must be performed, preferably, in the second week of the cycle (between 7 and 14 days), when the number of points (foci) and speed of enhancement are the lowest when compared with the other phases [31, 32].
In the postmenopause period, the use of combined (estrogen/progesterone) HRT can cause reversion of the usual atrophy in the period and result in an aspect similar to that in the premenopause period, and even appearing to be a parenchyma edema and a regular edema. When there is any doubt in interpretation, it is recommended that a reevaluation be made after HRT has been suspended for 6–8 weeks. In cases of therapy with selective modulators of estrogen receptor (tamoxifen), there is no hormone stimulation, which reduces the vascularity and density of parenchyma. Enhancement foci in breasts of patients using tamoxifen cannot be considered usual, because their hormone activity is blocked. Pregnant patients and lactating ones may also experience an increase of breast density and enhancement, owing to an increase in vascularity.
Breast vascularity is important and it defines a geographic pattern of normal parenchyma enhancement. There is a preferable enhancement in the external upper quadrant and in the inferior portion as well, as the center of the breast is the last part to be enhanced owing to the existence of a different vascular supply. This geographic pattern of the normal parenchyma enhancement occurs symmetrically in both breasts.
The larger ducts that converge below the nipple and drain out of each segment are about 2 mm in diameter. Dilated ducts with proteinaceous contents or with hemorrhagic debris can be seen in weighted sequences in precontrast T1 analysis as increased signal, and the postcontrast analysis can be done through images with subtraction to not obscure the area with enhancement.
Lymph nodes are easily detected and characterized through their reniform shape with a fatty hilum (high signal in weighted sequences in precontrast T1 images, with no fat saturation), besides having a strong enhancement after the use of intravenous contrast material. The T2-weighted images are also useful for characterizing lymph nodes, as they produce increased signal intensity when compared with the normal parenchyma.
Pectoralis muscles and the thoracic walls are considered anatomically distinctive and the evaluation of isolated neoplasic involvement of one of these structures or both of them influences the staging and surgical treatment. Deep tumors may produce retraction of the pectoralis muscles or get too close and obliterated fat planes, but with neoplasic involvement there is an irregular enhancement through contrast material in damaged areas of the muscle. The thoracic wall is made up of the serratus anterior muscle, the intercostal muscles, and the ribs. Neoplasic involvement in these structures will also be highlighted as abnormal on MRI.
6.2 Abnormal Magnetic Resonance Imaging Findings
MRI findings are evaluated not only through morphological characterization of lesions, but also through the type of enhancement by means of contrast and the dynamic characteristics, which may occur not only in three-dimensional lesions, such as masses, but also in areas of the parenchyma. Microcalcifications are not demonstrated through MRI, and they must be spotted in conventional mammograms for the correlation with magnetic resonance images and detection of suggestive enhancement in the area.
The main visualized alterations on MRI are described according to BI-RADS® [6] as in the following sections.
6.2.1 Focus
This is a tiny nonspecific enhancement area (less than 5 mm) which is too small to be characterized. It does not necessarily represent a lesion that occupies some space, such as a mass. The foci may occur as multiple areas or as enhancement dots, separated by a normal parenchyma or by fat, spread in the breast (Fig. 3.16). The foci were known as unidentified breast objects, bright unidentified breast objects, or incidental enhanced lesions, and they do not have any importance for clinical practice when identified in isolation.

Foci: a maximum intensity projection (MIP) reconstruction showing an isolated focus (arrow) in a patient with a benign functional alteration; b MIP reconstruction showing diffuse foci, also in a patient with a benign functional alteration
6.2.2 Masses
These are described as three-dimensional lesions that occupy some space. They can be morphologically evaluated (shape and margins) and can also be evaluated through their enhancement patterns (Fig. 3.17).

Masses: a sagittal short τ inversion recovery image showing a round mass with regular margins (arrow) (simple cyst); b sagittal fast spin echo (FSE) T1 postcontrast image showing an oval mass with regular margins and a hypoenhanced septum (arrow) (fibroadenoma); c sagittal FSE T1 postcontrast image showing an irregular mass with indistinct margins and heterogeneous enhancement (arrow) (invasive ductal carcinoma); d sagittal FSE T1 postcontrast image showing an irregular mass with spiculated margins and peripheral enhancement (arrow) (steatonecrosis)
They may be round, oval, lobulated, or irregular. As in the other methods, a round shape is the shape most related to benignity, whereas an irregular shape is related to malignancy.
The analysis of the margins depends on the spatial resolution of the images. The margin is described as regular (circumscribed), irregular (“serrated,” or even indistinct), or spiculated (linear projections irradiate from the mass). Irregular margins and spiculated ones are the most suggestive of malignancy.
As data additional to the morphological analysis, the characteristics of the internal enhancement contribute to the differentiation of benign masses from malignant ones. The enhancement pattern can be described as homogeneous (uniform and confluent—more suggestive of benignity) or heterogeneous (there are variable signal intensities inside the mass). The enhancement can also be described as peripheral, with dark internal septations and with internal and central septation enhancement. The heterogeneous aspect is the most suggestive of malignancy, mainly when it is peripheral, although septation enhancement and central enhancement are also suggestive. Inflammatory cysts may have their own enhancement, but they are hyperintense in the T2-weighted images, owing to their fluid content. Fat necrosis may also have a peripheral enhancement with a dark center, but it can be differentiated through the clinical record, through mammographic characteristics, and through the signal in the sequences with fat saturation through MRI. These two lesions are described as false-positive potentials in the analysis of lesions with peripheral enhancement, which is typical of malignancy. The enhancement pattern with dark internal septations is highly suggestive of fibroadenoma and it is an indicator of benignity [33]. Masses without enhancement are also suggestive of fibroadenoma with a high fatty hilum content.
6.2.3 Non-mass-like Enhancement
Non-mass-like enhancement describes an area of enhancement that can be classified neither as mass nor as a focus. This includes patterns that can extend over a region of various sizes according to a specific distribution and, except for the internal homogeneous pattern, there will always be areas of normal mammary fat tissue interspersed in the enhancement areas.
The distribution is described as focal (it generally occupies less than 25 % of the volume of a quadrant), linear (it can seem like a plane in other views and it does not follow the duct track), ductal (it follows the duct track toward the nipple, with ramifications), segmental (triangular region or in a cone, with an apex to the nipple, which resembles a duct and its branches), regional (it encompasses a huge tissue volume, with a geographic aspect and with no relation to the distribution of one duct system), and multiple regional and diffuse (equal all over the extension of the breast) (Fig. 3.18). Regional distribution patterns, in multiple regions and in a diffuse way, are the most suggestive of benign disease, such as proliferative alterations, whereas the ductal and the segmental patterns are highly suggestive of malignancy (ductal carcinoma).

Non-mass-like enhancement: a sagittal FSE T1 postcontrast image showing focal enhancement (arrow) (benign functional alteration); b sagittal FSE T1 postcontrast image showing linear enhancement (arrow) (scar); c sagittal FSE T1 postcontrast image showing ductal enhancement (arrow) (intraductal carcinoma); d sagittal FSE T1 postcontrast image showing segmental enhancement (arrows) (invasive ductal carcinoma); e sagittal FSE T1 postcontrast image showing regional enhancement (arrows) (benign functional alteration)
Internal enhancement patterns can be described, as a whole, as homogeneous or heterogeneous, symmetric (in both breasts like an image in the mirror) or asymmetric. An additional description can be added when the aspect of the heterogeneous enhancement is considered. A dotted pattern describes similar tiny dots (1–2 mm) spread and not following the ductal distribution, more in accordance with the normal variety of mammary parenchyma enhancement or with fibrocystic alterations. An agglomerated pattern represents a cluster of enhancement foci in one area, being either confluent with a “cobblestone-like” appearance or in “string of pearls” when it is linear (suggestive of ductal carcinoma in situ). The dendritic or reticular pattern occurs mainly in partially involuted breasts, where there are glandular parenchyma extensions, interspersed with stretches of fat tissue.
6.2.4 Associated Findings
The associated findings may increase suspicion of breast cancer and they are considered important because some of them influence the surgical treatment and the staging. The associated findings include [6]:
-
1.
Skin retraction or nipple retraction.
-
2.
Skin thickening: focal or diffuse (normal thickness up to 2 mm).
-
3.
Skin invasion: There is an abnormal enhancement of the skin, which is also thick in most cases.
-
4.
Edema: There is a trabecular thickening with or without associated skin thickening.
-
5.
Lymphadenomegaly: There are enlarged and round lymph nodes with loss of fatty hilum signal; they are highly suggestive.
-
6.
Pectoralis muscle or thoracic wall invasion: There is abnormal enhancement stretching to the pectoralis muscle with or without retraction, as well as to ribs and intercostal spaces.
-
7.
Hematoma: There is an increase of the signal in the weighted sequence in precontrast T1 images.
-
8.
Abnormal signal void: This occurs because of a magnetic object, and is caused by metal (as occurs with surgical clips).
-
9.
Cyst: This is described as a well-circumscribed structure filled with fluid; it can be round or oval and with an imperceptible wall. In the weighted margins in T1 images, the cysts appear with a hypointense signal with respect to the adjacent tissue, except for cysts with protein content due to blood products. In precontrast sequences, only the inflammatory cysts will exhibit peripheral enhancement.
6.3 Kinetic Curve
The kinetic curve is obtained from a dynamic sequence performed with intravenous injection of contrast material (gadolinium) and it describes the enhancement characteristics of a specific region determined by the region of interest. This region must be the one with the largest and fastest enhancement or the most suggestive area.
The physiopathological basis has not been properly elucidated yet, but it is known that the intensity of enhancement depends not only on the increase of vascularity and the permeability of the vessels, as commonly found in malignant lesions, but also on the interaction of the contrast material with the lesion tissues.
Considering the enhancement pattern in dynamic series, we can distinguish two phases according to BI-RADS®: the initial phase (the period between the injection of the constant material and the second minute after injection) and the delayed phase (the period that starts 2 min after injection of the contrast material). Fischer et al. [34] consider the initial phase to be the phase up to the third minute after the intravenous injection of contrast material, and the delayed phase to be the phase between 3 and 8 min.
In the initial phase, signal intensity after injection of contrast material is quantitatively evaluated and the speed of enhancement is classified as slow, medium, or rapid. Mainly in malignant lesions, the maximum intensity of enhancement tends to be reached in the initial phase. Kuhl et al. [35] evaluated 266 lesions with mean enhancement for malignant lesions of 104 % ± 41 and for benign lesions of 72 % ± 35, with a sensitivity of 91 % and a low specificity of 37 %. Low specificity was attributed to the fact that benign lesions can also have fast and intense enhancement.
The delayed phase is evaluated in a qualitative way through the morphology curve. Visual classification is made as follows:
-
1.
Type 1 curve (persistent)—signal intensity increases throughout the dynamic series and the highest point is obtained in the last postcontrast series (Fig. 3.19a). According to Fischer et al. [34], signal intensity in the delayed phase increases to 10 % above the peak value of the initial rise by 3 min.
Fig. 3.19 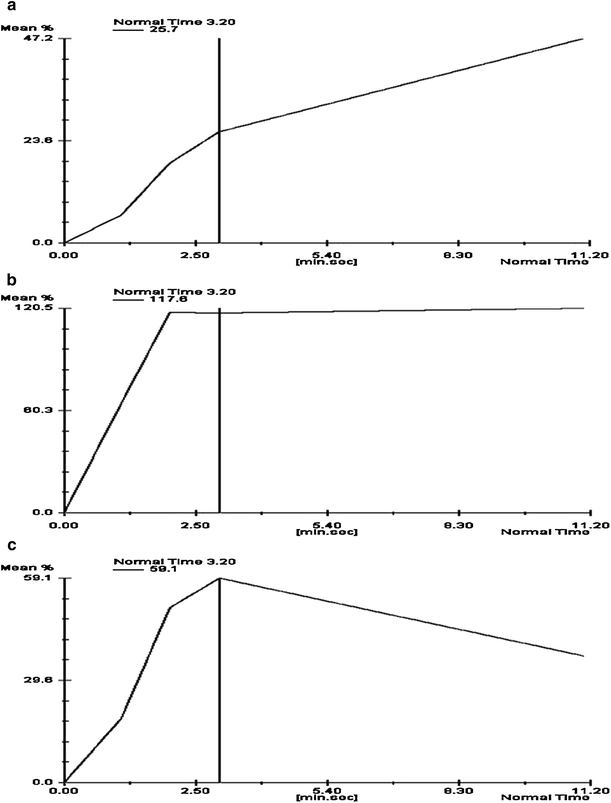
Types of kinetic curve for dynamic magnetic resonance imaging (MRI) evaluation: pattern type I (a), pattern type II (b), and pattern type III (c)
-
2.
Type 2 curve (plateau)—signal intensity reaches a plateau after the initial phase and it does not vary significantly in the subsequent phases (Fig. 3.19b). The maximum signal intensity is reached after 2 or 3 min. A variation of signal intensity of ± 10 % of the peak value of the initial rise at 3 min is acceptable [34].
-
3.
Type 3 curve (washout)—signal intensity decreases immediately after it reaches its highest point, usually on the first or second postcontrast sequence (Fig. 3.19c). According to Fischer et al. [34], the signal intensity in the late phase reduces by over 10 % of the initial peak value by 3 min.

As a general rule, the vast majority of benign lesions follow a persistent curve pattern and the malignant ones follow a washout pattern or a plateau one. The probability that each type of curve is associated with breast cancer was studied by Kuhl et al. [35], and the following results were found: type 3 curve—87 %, type 2 curve—64 %, and type 1 curve—6 %. In the same study it was demonstrated that the analysis of the shape of the aspect is more specific (83 %) than the quantitative analysis of the signal intensity (37 %), although both methods have the same sensitivity (91 %).
6.4 Current Clinical Applications of Magnetic Resonance Imaging
Clinical indications are still discussed in some aspects, with the best cost–benefit relationship for patients with high risk of developing breast cancer or for those proven to have cancer. In the following sections, we highlight some examples.
6.4.1 Patients with High Risk of Breast Cancer
Women considered high risk for developing breast cancer are those with documented mutations in genes BRCA1 and BRCA2, a marked family history (estimated risk over 20 % according to the risk calculation models), personal history of breast cancer, previous biopsy showing lobular carcinoma in situ or atypical ductal hyperplasia, and previous thoracic radiation between 10 and 30 years of age (Fig. 3.20) [36].

A 45-year-old patient, asymptomatic, with family history of two sisters having breast cancer. Mammography (a, b) and ultrasonography did not show abnormalities. The patient underwent MRI (c) for tracking, and the image shows a suspicious enhancement area in the right breast (arrow). On ultrasonography (d) performed after the MRI, an irregular hypoechoic area was observed (arrows). Patient undergoing a percutaneous biopsy (e), diagnosed as having invasive ductal carcinoma
The importance of mammographic tracking in this group is low, as most of the subjects will develop breast cancer during their premenopause period, a stage when the mammary parenchyma is denser. Another limiting factor is the higher radiosensitivity in this group, as reported in some studies. Kriege et al. [37] compared the accuracy of mammography, ultrasonography, and MRI for diagnosis in 1,904 patients with high risk on both genetic and family history grounds, and found sensitivities of 33 %, 60 %, and 100 %, respectively. Other multicenter studies found similar results [38–43]. The most recent study was published by Kuhl et al. [43], demonstrating sensitivity for cancer detection of 33 % for mammography, 37 % for ultrasonography, and 92 % for MRI in high-risk patients, with 98 % specificity for all methods. No case of hidden carcinoma was found, and all tumors were smaller than 1 cm (46 % invasive carcinomas and 53 % carcinomas in situ).
On the basis of these data, in 2007 the American Cancer Society published recommendations for the performance of mammography and MRI annually for all patients with confirmed mutation, first-grade patients with confirmed mutation, patients with risk of developing breast cancer above 20 %, and patients undergoing thoracic radiation for over 10 years [44]. These recommendations have been recently confirmed in a publication by the American College of Radiology and the Society of Breast Imaging [45].
6.4.2 Detection of Hidden Primary Tumor of the Breast with a Positive Axillary Lymph Node
A hidden tumor is defined in patients with axillary lymph node metastasis of breast cancer with no primary focus detected through conventional methods (mammography and ultrasonography), corresponding to less than 1 % of all breast cancer cases [46, 47]. Contrast MRI is highly sensitive for the detection of a hidden tumor, changing the course of action in relation to the treatment of some patients, even to the point of considering a conservative treatment for some selected cases (Fig. 3.21).

A 55-year-old patient with a palpable lymph node in the right axillary region. Mammography (a, b) showed a dense lymph node in the axillary region. Ultrasonography did not reveal suspicious findings in the breast. MRI (c, d) confirmed the lymph node enlarging in the axillary region (two arrows) and showed a small enhanced mass in the superolateral quadrant of the right breast (arrow), with a type 3 kinetic curve type, which was confirmed as invasive ductal carcinoma when surgery was performed
Studies so far have only been of small populations, although with interesting results on the capacity to detect primary lesions through MRI. The proportion detected was 75 % and 86 %, respectively, in the studies by Morris et al. [48] and Orel et al. [49], all of the tumors with proven histological basis. The lesions appear predominantly as a mass-like enhancement with morphology suggestive of malignancy and sizes ranging between 5 mm and 30 mm. In spite of the highly predictive negative rate, in the case of a negative MRI findings, the possibility of a primary breast lesion cannot be completely excluded.
6.4.3 Preoperative Staging of Breast Cancer
The surgical planning depends on a careful preoperative evaluation of the extension of the disease (Fig. 3.22). MRI is currently the most sensitive method to detect additional foci of multifocal disease (detecting a range of 1−20 %), multicentric disease (2−24 %), and contralateral disease (3−24 %) not found by traditional methods (mammography and ultrasonography), besides allowing an evaluation of the extension for the pectoralis muscle, the thoracic wall, and the papillary–areola complex. The main point of discussion is whether to find out these foci of neoplasia represent an increase in the extended life of the patients undergoing conservative surgery [50–52].

A 51-year-old patient with mammary prosthesis undergoing mammography (a–c), which showed pleomorphic microcalcifications in the superolateral quadrant of the right breast, with the diagnosis of invasive intraductal carcinoma confirmed by biopsy findings. MRI (d, e) for staging showed that the lesion extended to the papilla, besides having another invasive focus in the contralateral breast (arrow)
Fischer et al. [34] evaluated 463 patients with confirmed diagnosis of breast cancer and found multifocal lesions not detected by other methods in 8.9 % of cases, multicentric ones in 7.1 % of cases, and contralateral ones in 4.5 % of cases, which results in a change of attitude in therapy using MRI in 19.6 % of cases. Later, Fischer et al. [50] published another study evaluating the influence of preoperative MRI on the local recurrence rate of breast cancer and found a reduction from 6.5 % to 1.2 % among the group undergoing MRI. They associated this fact with better diagnosis of the tumor extension and better staging.
On the other hand, a study by Turnbull et al. [53] did not show any difference in the percentage of patients requiring reoperation between the group undergoing MRI (19 %) and the group that did not undergo MRI (19 %). They also demonstrated that MRI contributed to a delay in the surgical procedure and an increase in the number of mastectomies. Therefore, multicentric studies are still not considered necessary to define specific groups that could benefit from routine preoperative staging through MRI [54]. An attempt to develop a systematization was recently published by an EUSOMA working group, which recommended preoperative MRI for some specific groups, such as patients with multiple undetermined or suggestive lesions with clinical findings that diverge from those findings from screening, with significant familial or genetic risk, or with diagnosis of Paget disease or lobular histological subtype, besides those patients with indication for partial radiotherapy [55].
6.4.4 Evaluation of Response to Neoadjuvant Chemotherapy
Neoadjuvant chemotherapy is performed on patients with an advanced stage of the disease, aiming to reduce tumor staging before treatment through surgery. Adequate monitoring of the effects of the preoperative therapy is relevant to evaluate the efficacy of medication after the first cycles, which implies the continuation or change of chemotherapy scheme, besides aiding the surgical planning.
Although the response to neoadjuvant chemotherapy is traditionally assessed through clinical examination, mammography, and ultrasonography, the use of MRI for this monitoring has been shown to be more effective than conventional methods (Fig. 3.23). MRI helps differentiate fibrosis induced by chemotherapy of the tumor itself, besides being useful for the evaluation of multicentric, multifocal, and contralateral disease [56].

A 36-year-old patient with edema and redness of the left breast. MRI showed an extensive lesion in the left breast (a), with a type 3 enhancement curve (b), besides skin thickening and axillary lymphadenomegaly. The patient underwent neoadjuvant chemotherapy, and examination after the third cycle (c) revealed tumor regression with a small residual lesion (arrow) and a type 1 enhancement curve (d)
Even with so many advantages, MRI also has some limitations for this group. Chemotherapy drugs reduce vascularization and capillary permeability, besides producing fibrosis, necrosis, and tumor inflammation, which changes the enhancement parameters for this group. This is related to less accuracy in the evaluation of tumor volume, which may be underestimated or overestimated [56, 57].
Martincich et al. [58] showed that the integration between morphological and functional parameters can improve the precocious response to neoadjuvant treatment (after the second cycle), with a good histopathological correlation. In this study an accuracy of 93 % was obtained to predict the full pathological response, with reduction of the tumor volume and of the enhancement through contrast material. Pickles et al. [56] evaluated 68 patients before and during the precocious phases as well as after chemotherapy, and showed that quantifying the dynamic parameters of enhancement and the change of tumor volume allow differentiation between responsive and unresponsive patients.
6.4.5 Papillary Lesion with Pathological Discharge
Papillary flow can be a breast cancer manifestation. Mammography and ultrasonography are the first examinations to be performed, although often they do not detect the lesion, owing to difficulties in evaluating the retroareolar region. Ductography also helps detect the lesion, although with limitations, mainly because of the intermittent papillary flow. MRI appears to a good choice for diagnosis in this group because it is able to detect small intraductal lesions, therefore aiding surgical planning (Fig. 3.24).

A 43-year-old patient with family history of papillary brain stroke on the right. Mammography and ultrasonography did not show any abnormality. MRI showed a small dilated duct (a, arrow) with a linear enhancement area inside the duct (b, double arrow). Surgery confirmed the diagnosis of intraductal carcinoma
Morrogt et al. [59] evaluated 376 patients with papillary discharge, of which 306 had negative findings on mammography and ultrasonography. This group then underwent ductography and MRI, and 46 tumors (15 % of cases) were observed. Ductography did not detect six tumors (predictive positive value of 19 % and predictive negative value of 63 %) and MRI did not detect one tumor (predictive positive value of 56 % and predictive negative value of 87 %). The authors concluded that ductogalactography has a low predictive negative value so it may not exclude disease and that MRI can aid the surgical planning, although it does not exclude duct resection when there is suspicion of discharge. But Liberman et al. [59] concluded that MRI can be a good alternative to galactography in cases when papillary discharge suspected with negative findings on mammography and ultrasonography, as it detected the focus in 100 % of the patients evaluated. This way, concomitant evaluation with mammography and MRI is recommended for patients with suspected papillary discharge.
6.4.6 Postoperative Evaluation to Detect Local Recurrence
Recurrence occurs at an annual rate of 1–2 %, but it is uncommon during the first 18 months after the treatment [60]. Evaluation through physical examination, mammography, and ultrasonography is difficult owing to postoperative and radiotherapy changes, such as surgical scar, architectural distortion, calcifications, increase in mammary density, and fat necrosis, which can mimic the appearance of a recurring neoplasia, or even obscure it. MRI appears to be a promising method for the evaluation of local recurrence, mainly in cases of difficult evaluation through conventional methods (Fig. 3.25).

A 63-year-old patient with a history of 6-year quadrantectomy. The control mammogram (a) shows focal asymmetry of the scar topography. MRI shows asymmetry (b), but with a fat area inside (c) confirming the diagnosis of postsurgical steatonecrosis
Up until 18 months after the surgical and radiotherapy treatments, MRI has limited value, as there is still secondary enhancement of inflammation induced by the treatment both in the scar region and in the areas with normal tissue, due to radiotherapy. After this period, MRI is able to detect tumor recurrence and differentiate it from areas of secondary enhancement resulting from the treatment. Benign sequelae such as fat necrosis, seroma, and hematoma can be safely differentiated through MRI, because of their signal characteristics [30, 61].
6.4.7 Evaluation of Inconclusive Findings of Conventional Imaging Examinations
MRI shows morphological and enhancement details that allow better differentiation between benign and malignant lesions when a biopsy is not viable and the evaluation through conventional imaging methods is inconclusive. The dynamic study helps differentiate a well-circumscribed carcinoma that morphologically mimics a benign mass or a thick content cyst, as well as to characterize lobular neoplasia that mimics focal asymmetries, cases of palpable lesions that are not shown by the traditional methods, and cases of diabetic mastoplasty that simulate a carcinoma, among others. In cases of suspected microcalcifications seen on mammography, MRI cannot be used to exclude the presence of neoplasia, so there is need for a biopsy because of limited sensitivity in the evaluation of low-grade intraductal carcinomas. But in cases of high-grade intraductal carcinomas, MRI has higher sensitivity than mammography. This was demonstrated by Kuhl et al. [62], who prospectively studied 7,319 women. They found a sensitivity of 61 % for mammography and 80 % for MRI in the detection of low-grade intraductal carcinomas, whereas for high-grade intraductal carcinomas, sensitivity was 52 % for mammography and 98 % for MRI.
6.4.8 Evaluation of a Mammary Prosthesis
MRI has been more frequently used to evaluate a mammary prosthesis for aesthetic or reconstruction (after mastectomy or quadrantectomy). The aims of evaluation through MRI of women with a prosthesis range from checking implant disruption (Figs. 3.26, 3.27), to checking for neoplasia (high-risk women or those in which there is suspicion of alteration in clinical–imagiological examinations), to evaluation of extension of a confirmed neoplasia and checking for recurring tumor in reconstructed breast after mastectomy. In patients with injection of silicone in the parenchyma, for which conventional methods are limited in their evaluation capability, MRI appears to be highly efficient to differentiate siliconomas from carcinomas (Fig. 3.16). In a meta-analysis, Cher et al. [63], concluded that the use of MRI to evaluate the integrity of the prosthesis has sensitivity of 78 % and specificity of 91 %, with a positive predictive value ranging between 50 % and 100 % and a negative predictive value ranging between 70 % and 100 %. Holmich et al. [64] compared the clinical diagnosis and the MRI diagnosis of prosthesis rupture and concluded that the clinical examination focusing on the detection of a rupture had low sensitivity and specificity, detecting less than 30 % of rupture cases; only 50 % of the implants considered clinically intact through MRI were actually intact. Therefore, the FDA recommends the annual use of MRI from the third year after surgery to detect silent ruptures [65].

Signs of intracapsular rupture on MRI: a thin drops of fluid inside the prosthesis; b focal area of liquid subjacent to the capsule; c small leakage of silicone external to the capsule; d “tear drop” sign; e “linguini” sign; f “salad oil” sign

Signs of extracapsular rupture on MRI: a focal area of silicone leakage outside the reaction capsule; b focal silicone area in front of the pectoralis muscle; c laminar area of silicone leakage; d intermediate silicone leakage around all the reaction capsule; e extensive leakage of silicone behind the capsule; f leakage of silicone for the parenchyma
References
Veronesi U et al (2005) Breast cancer. Lancet 365:1727–1741
Jemal A et al (2005) Cancer Statistics, 2005. CA Cancer J Clin 55:10–30
Ries LAG, et al (1994) Cancer statistics review 1973–91: tables and graphs. National institutes of health publication, National Cancer Institute, Bethesda n94–2789
Kelsey JL (1990) Breast cancer epidemiology: summary and future directions. Epidemiology 131:984–986
INCA (2011) Estimativas da incidência e da mortalidade por câncer no Brasil. Disponível em: hppt://www.inca.gov.br/estimativa2011. Accessed 10 oct 2011
American College of Radiology (2003) Breast imaging reporting and data system (BI-RADS), 4th edn. American College of Radiology, Reston
Chu KC, Smart CR, Taronev RE (1998) Analysis of breast cancer mortality and stage distribution by age for the health insurance plan clinical trial. J Natl Cancer Inst 80:1125–1132
Andersson I, Janzon L (1997) Reduced breast cancer mortality in women under age 50: update results from the malmo mammographic screening program. J Natl Cancer Inst Monogr 22:63–67
Bjurstam N et al (1997) The Gothenburg breast screening trial: first results on mortality, incidence, and mode of detection for women ages 39–49 years at randomization. Cancer 80:2091–2099
Brown D (2000) Death rates from breast cancer fall by a third. BMJ 321:849
Frisell J et al (1997) Follow-up after 11 years: update of mortality results in the stockholm mammographic Screening Trial. Breast Cancer Res Treat 45:263–270
Jackman VP (2002) Screening mammography: controversies and headlines. Radiology 225:323–326
Miller AB et al (1992) Canadian national breast screening study I: breast cancer detection and death rates among women aged 40–49 years. Can Med Assoc J 147:1459–1476
Miller AB et al (1992) Canadian national breast screening study II: breast cancer detection and death rates among women aged 50–59 years. Can Med Assoc J 147:1447–1488
Tabar L et al (1995) Efficacy of breast cancer screening by age: new results from the Swedish two-county trial. Cancer 75:2507–2517
Liberman L (2004) Breast cancer screening with MRI: what are the data for patients at high risk? New Engl J Med 351:497–500
Shapiro S (1977) Evidence on screening for breast cancer from a randomized trial. Cancer 39:2772
Shapiro S, Strax P, Venet L et al (1982) Ten- to fourteen-year effect of screening on breast cancer mortality. J Natl Cancer Inst 69:349–355
Shapiro S (1977) Evidence on screening for breast cancer from a randomized trial. Cancer 39:2772
Crystal P et al (2003) Using sonography to screen women with mammographically dense breast. AJR 181:177–182
Kolb TM, Lichy J, Newhouse JH (2002) Comparison of the performance of screening mammography, physical examination and breast US, and evaluation of factors that influence them: an analysis of 27,825 patients’ evaluations. Radiology 225:165–175
Kriege R et al (2004) Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. New Engl J Med 351:425–437
Warner E et al (2004) Surveillance of BRCA2 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 292:1713–1725
Kuhl CK et al (2005) Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familiar risk for breast cancer. J Clin Oncol 23:8469–8476
BRASIL (2004) Ministério da Saúde. Instituto Nacional de Câncer. Coordenação de Prevenção e Vigilância. Controle do câncer de mama: documento de consenso. Rio de Janeiro, INCA/CONPREV
Moy L, Slanetz PJ, Moore R et al (2002) Specificity of mammography and US in the evaluation of a palpable abnormality: retrospective review. Radiology 225:176–181
Sickles EA (1986) Nonpalpable, circumscribed, noncalcified solid breast masses: likelihood of malignancy based on lesion size and age of patients. Radiology 192:439–442
Stravos TM et al (1995) Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology 196:123–134
Rahbar H et al (1999) Benign versus malignant solid breast masses: US differentiation. Radiology 213:889–894
Hylton N (2005) Magnetic resonance imaging of the breast: opportunities to improve breast cancer management. J Clin Oncol 23:1678–1684
Kuhl CK et al (1997) Healthy premenopausal breast parenchyma in dynamic contrast-enhanced MR imaging of the breast: normal contrast medium enhancement and cyclical-phase dependency. Radiology 203:137–144
Muller-Schimpfle M et al (1997) Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology 203:145–149
Nunes LW, Schnall MD, Orel SG et al (1997) Breast MR imaging interpretation model. Radiology 202:833–841
Fischer U, Kopka L, Grabbe E (1999) Breast carcinoma: effect of preoperative contrast-enhanced MR imaging on the therapeutic approach. Radiology 213:881–888
Kuhl CK et al (1999) Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions? Radiology 211:101–110
Warner et al (2001) Comparison of breast magnetic resonance imaging, mammography, and ultrasound for surveillance of women at high risk for hereditary breast cancer. J Clinl Oncol 19:3524–3531
Kriege M, Brekelmans CT, Boetes C et al (2004) Magnetic resonance imaging screening study group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 351:427–437
Kuhl CK, Schrading S, Leutner CC et al (2005) Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 23:8469–8476
Leach MO, Boggis CR, Dixon AK et al (2005) Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet 365:1769–1778
Warner E, Plewes DB, Hill KA et al (2004) Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 292:1317–1325
Sardanelli F, Podo F, D’Agnolo G et al (2007) High breast cancer risk Italian trial. Multicenter comparative multimodality surveillance of women at genetic-familial high risk for breast cancer (HIBCRIT study): interim results. Radiology 242:698–715
Lehman CD, Isaacs C, Schnall MD et al (2007) Cancer yield of mammography, MR, and US in high-risk women: prospective multi-institution breast cancer screening study. Radiology 244:381–388
Kuhl C, Weigel S, Schrading S et al (2010) Prospective multicenter cohort study to refine management recommendations for women at elevated familial risk of breast cancer: the EVA Trial. J Clin Oncol 20:1450–1457
Warner E, Yaffe M, Andrews KS et al (2007) American cancer society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 57:75–89
Lee CH, Dershaw D, Kopens D et al (2010) Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol 7:18–27
Stomper PC et al (1999) Breast MRI in the evaluation of patients with occult primary breast carcinoma. Breast J 5:230–234
Schorn C et al (1999) MRI of the breast in patients with metastatic disease of unknown primary. Eur Radiol 9:470–473
Morris E et al (1997) MR imaging of the breast in patients with occult primary breast carcinoma. Radiology 205:437–440
Orel S et al (1999) Breast MR imaging in patients with axillary node metastases and unknown primary malignancy. Radiology 212:543–549
Fischer U et al (2004) The influence of preoperative MRI of the breasts on recurrence rate in patients with breast cancer. Eur Radiol 10:1725–1731
Kuhl CK, Schmiedel A, Morakkabati N et al (2002) Breast MR imaging of the asymptomatic contralateral breast in the work up or follow-up of patients with unilateral breast cancer. Radiology 217–268
Liberman L, Moris EA, Kim CM et al (2003) MR imaging findings in the contralateral breast in women with recently diagnosed breast cancer. AJR 180:333–341
Turnbull L, Brown S, Harvey I et al (2010) Comparative effectiveness of MRI in breast cancer (COMICE) trial: a randomized controlled trial. Lancet 375:563–571
Tan MP (2009) An algorithm for the integration of breast magnetic resonance imaging into clinical practice. Am J Surg 197:691–694
Sardanelli F et al (2010) Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. Eur J Cancer 46:1296–1316
Pickles M et al (2005) Role of dynamic contrast enhanced MRI in monitoring early response of locally advanced breast cancer to neoadjuvant chemotherapy. Breast Cancer Res Treat 91:01–10
Rieber A, Brambs HJ, Gabelmann A et al (2002) Breast MRI for monitoring response of primary breast cancer to neoadjuvant chemotherapy. Eur Radiolgy 12:1711–1719
Martincich L et al (2004) Monitoring response to primary chemotherapy in breast cancer using dynamic contrast-enhanced magnetic resonance imaging. Breast Cancer Res Treat 83:67–76
Morrogh M, Morris EA, Liberman L et al (2007) The predictive value of ductography and magnetic resonance imaging in the management of nipple discharge. Ann Surg Oncol 14:3369–3378
Dershaw D (2002) Breast imaging and the conservative treatment of breast cancer. Radiol Clin Am 40:501–516
Berg WA, Nguyen TK, Middleton MS, Soo MS et al (2002) MR imaging of extra-capsular silicon from breast implant: diagnostic pitfalls. AJR 178:465–472
Kuhl C, Schrading S, Bieling HB et al (2007) MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet 370:485–492
Cher DJ, Conwell JA, Mandel JS (2001) MRI for detecting silicone breast implant rupture: Meta-analysis and implications. Ann Plast Surg 47:367–380
Hölmich LH et al (2005) The diagnosis of breast-implant rupture: Clinical findings compared with findings at magnetic resonance imaging. An Plastic Surg 54:583–589
Mc Carthy MC, Pusic AL, Kerrigan CL. Silicon breast implants and magnetic resonance imaging screening for rupture: do US Food and Drug Administration recommendations reflect an evidence-based practice approach to patient care? Plast Reconstr Surg 2008; 121:1127-1134
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer-Verlag Italia
About this chapter
Cite this chapter
Urban, L., Urban, C. (2013). Breast Imaging. In: Urban, C., Rietjens, M. (eds) Oncoplastic and Reconstructive Breast Surgery. Springer, Milano. https://doi.org/10.1007/978-88-470-2652-0_3
Download citation
DOI: https://doi.org/10.1007/978-88-470-2652-0_3
Published:
Publisher Name: Springer, Milano
Print ISBN: 978-88-470-2651-3
Online ISBN: 978-88-470-2652-0
eBook Packages: MedicineMedicine (R0)